Embed Size (px)
Citation preview

Miles Levy
Consultant Endocrinologist
Leicester Royal Infirmary
East Midlands Acute Medicine Conference
24th February2016

� Sodium
� Calcium
� Pituitary
� Thyroid


� Mild 130-135 mmol/L
� Moderate 125-129 mmol/L
� Severe <125 mmol/L

� Mild No symptoms
� Moderate Nausea, headache, confusion
� Severe Vomiting, low GCS, seizures

� 35 year old man
� Neuro-surgical ward
� Berry aneurysm repair
� Intractable seizures
� GCS = 5

� 35 year old man
� Neuro-surgical ward
� Berry aneurysm repair
� Intractable seizures
� GCS = 5
Cerebral oedema

� Na 109 mmol/l (133-144)
� K 4.3 mmol/l (3.3-5.3)
� U 5.5 mmol/l (2.5-6.5)
� C 64 μmol/l (60-120)

� Na 109 mmol/l (133-144)
� K 4.3 mmol/l (3.3-5.3)
� U 5.5 mmol/l (2.5-6.5)
� C 64 μmol/l (60-120)
� Na 142 mmol/L yesterday

� Acute severe hyponatraemia
� No time for full investigation
� Urgent action needed
� Ring ITU

Move to a Level 2 monitored environment
Administration of hypertonic 3% saline*
150 mL IV over 15 min
Repeat after 20 min if no clinical improvement
Recheck serum [Na+] at 6, 12, 24 and 48 h for
overcorrection (no more than 10 mmol/L
in 24 h)
*Hypertonic 3% saline can also be administered at 0.5–1 mL/kg/hour with frequent monitoring every 2–4 hours.

� If life threatening situation
� Irrespective of cause hyponatraemia
� 5 mmol/L increase in first hour
� < 10mmol/ L in first 24 hours
� Must be senior decision

� If life threatening situation
� Irrespective of cause hyponatraemia
� 5 mmol/L increase in first hour
� < 10mmol/ L in first 24 hours
� Must be senior decisionOsmotic Demyelination
Syndrome (ODS)
Cerebral Oedema

� 74 year old lady
� AMU admission
� Increased confusion
� Weight loss few weeks
� Collapse at home

� Na 127 mmol/l (133-144)
� K 3.8 mmol/l (3.3-5.3)
� U 3.6 mmol/l (2.5-6.5)
� C 49 μmol/l (60-120)

� Na 127 mmol/l (133-144)
� K 3.8 mmol/l (3.3-5.3)
� U 3.6 mmol/l (2.5-6.5)
� C 49 μmol/l (60-120)
� LFTs normal
� FBC normal
� CRP 17

� Time for full investigation
� No urgent action needed
� Make a diagnosis first

HYPONATRAEMIA [Na+] <130 mmol/L
Consider the contexte.g. known cancer, polydipsia
Stop any offending medicationse.g. thiazide diuretics, SSRIs
Initial immediate investigation panel• Glucose• Lipids• Cortisol• Thyroid function
• Liver function• Plasma osmolality• Urine osmolality• Urine [Na+] + [K+]

HYPONATRAEMIA [Na+] <130 mmol/L
Consider the contexte.g. known cancer, polydipsia
Stop any offending medicationse.g. thiazide diuretics, SSRIs
Initial immediate investigation panel• Glucose• Lipids• Cortisol• Thyroid function
• Liver function• Plasma osmolality• Urine osmolality• Urine [Na+] + [K+]
• Clinical context and timeline always very important
• If clinically obvious then do not need algorithm

Assess patient’s hydration status
EUVOLAEMIAHYPOVOLAEMIA
• Reduced skin turgor• Dry membranes• Tachycardia• Low BP or postural hypotension
HYPERVOLAEMIA• Oedema• Raised JVP• LVF• Ascites

Assess patient’s hydration status
EUVOLAEMIAHYPOVOLAEMIA
• Reduced skin turgor• Dry membranes• Tachycardia• Low BP or postural hypotension
HYPERVOLAEMIA• Oedema• Raised JVP• LVF• Ascites
• Clinical assessment of volume status is difficult
• If in doubt, give saline and see what happens
• In dehydration things will improve
• In SIADH things will worsen

EUVOLAEMIA
Check urine [Na+]
Confirm hypotonic hyponatraemia
i.e. plasma osmolality <275 Osm/kg,urine osmolality >100 Osm/kg
Urine [Na+] >20 mmol/L: likely SIADH
Urine [Na+] <20 mmol/L: reconsider hypo/hypervolaemia

EUVOLAEMIA
Check urine [Na+]
Confirm hypotonic hyponatraemia
i.e. plasma osmolality <275 Osm/kg,urine osmolality >100 Osm/kg
Urine [Na+] >20 mmol/L: likely SIADH
Urine [Na+] <20 mmol/L: reconsider hypo/hypervolaemia
• If urine osmolality < 100 Osm/Kg likely primary polydipsia
• If urine osmolality > 100 Osm/Kg then check urine Na

EUVOLAEMIA
Check urine [Na+]
Confirm hypotonic hyponatraemia
i.e. plasma osmolality <275 Osm/kg,urine osmolality >100 Osm/kg
Urine [Na+] >20 mmol/L: likely SIADH
Urine [Na+] <20 mmol/L: reconsider hypo/hypervolaemia
• If urine Na > 20 mmol/L, SIADH is likely diagnosis
• If urine Na < 20 mmol/L, probably intravasular volume depletion

Investigate underlying cause: consider CT chest / abdomen / pelvis /
head
Calculate electrolyte-free water clearance using Furst formula:
Urine [Na+] + [K+]Serum [Na+]
Urine [Na+] >20 mmol/L: likely SIADH

Investigate underlying cause: consider CT chest / abdomen / pelvis /
head
Calculate electrolyte-free water clearance using Furst formula:
Urine [Na+] + [K+]Serum [Na+]
Urine [Na+] >20 mmol/L: likely SIADH
• If no clear cause, consider CT CAP and / or MRI brain
• Furst formula to estimate electrolyte-free water clearance
• Exclude hypothyroidism, ACTH deficiency

Investigate underlying cause: consider CT chest / abdomen / pelvis /
head
Calculate electrolyte-free water clearance using Furst formula:
Urine [Na+] + [K+]Serum [Na+]
Urine [Na+] >20 mmol/L: likely SIADH
• If no clear cause, consider CT CAP and / or MRI brain
• Furst formula to estimate electrolyte-free water clearance
• Exclude hypothyroidism, ACTH deficiency

� Different from primary adrenal failure
� Not mineralocorticoid deficiency

� Different from primary adrenal failure
� Not mineralocorticoid deficiency
� Cortisol needed to excrete free water
� Deficiency causes dilutional hyponatraemia

� Different from primary adrenal failure
� Not mineralocorticoid deficiency
� Cortisol needed to excrete free water
� Deficiency causes dilutional hyponatraemia
� Looks identical to SIADH

HYPOVOLAEMIA• Reduced skin turgor• Dry membranes• Tachycardia• Low BP or postural hypotension
HYPERVOLAEMIA• Oedema• Raised JVP• LVF• Ascites
Urine [Na+] <20 mmol/L: reconsider hypo/hypervolaemia
Treat with 0.9% salineTreat the underlying cause e.g. cardiac
failure, renal failure, liver cirrhosis

HYPOVOLAEMIA• Reduced skin turgor• Dry membranes• Tachycardia• Low BP or postural hypotension
HYPERVOLAEMIA• Oedema• Raised JVP• LVF• Ascites
Urine [Na+] <20 mmol/L: reconsider hypo/hypervolaemia
Treat with 0.9% salineTreat the underlying cause e.g. cardiac
failure, renal failure, liver cirrhosis
• Involve appropriate specialist for CCF, nephrotic, cirrhosis
• Loop diuretics will cause diuresis that exceeds 24h sodium loss

<0.5: commence 1.0 L fluid restrictionCalculate electrolyte-free water clearance using Furst formula:
Urine [Na+] + [K+]Serum [Na+]
0.5–1.0: commence 0.5 L fluid restriction
>1.0: fluid restriction unlikely to be effective
Assess response after 24–48 h
Re-evaluate
If poor responseConsult with Specialist e.g. Consultant Endocrinologist
Aim for target [Na+] 130 mmol/L

<0.5: commence 1.0 L fluid restrictionCalculate electrolyte-free water clearance using Furst formula:
Urine [Na+] + [K+]Serum [Na+]
0.5–1.0: commence 0.5 L fluid restriction
>1.0: fluid restriction unlikely to be effective
Assess response after 24–48 h
Re-evaluate
If poor responseConsult with Specialist e.g. Consultant Endocrinologist
Aim for target [Na+] 130 mmol/L
• Response to fluid restriction predicted by Furst formula
• If high Na / K in urine then kidneys cannot excrete free water

� Treat underlying pathology
� AVP antagonists
� Demeclocycline

� Treat underlying pathology
� AVP antagonists tolvaptan 15-30mg /day
� Demeclocycline

� Treat underlying pathology
� AVP antagonists tolvaptan 15-30mg /day
� Demeclocycline 150-300mg tds

� Treat underlying pathology
� AVP antagonists tolvaptan 15-30mg /day
� Demeclocycline 150-300mg tds
� Discuss with local sodium expert


� Pigmentation
� Hyponatraemia
� Hyperkalaemia
� Hypoglycaemia
� Hypotension

� Pigmentation
� Hyponatraemia
� Hyperkalaemia
� Hypoglycaemia
� Hypotension

� Pigmentation
� Hyponatraemia
� Hyperkalaemia
� Hypoglycaemia
� Hypotension

� Think of the diagnosis
� Reverse hypoglycaemia
� Hydrocortisone 100mg IV stat
� Treat hyperkalaemia
� Volume replacement
� Normal saline
� Fluid balance

� Not pigmented
� Hyponatraemia
� No hyperkalaemia
� Looks like SIADH

� Not pigmented
� Hyponatraemia
� No hyperkalaemia
� Looks like SIADH
� Flat cortisol response

� Not pigmented
� Hyponatraemia
� No hyperkalaemia
� Looks like SIADH
� Flat cortisol response
� Long term steroids?

� Not pigmented
� Hyponatraemia
� No hyperkalaemia
� Looks like SIADH
� Flat cortisol response
� Long term steroids?Pituitary tumour?

� Not pigmented
� Hyponatraemia
� No hyperkalaemia
� Looks like SIADH
� Flat cortisol response
� Long term steroids?
� Improvement with steroids Pituitary tumour?


� Mild 145-150 mmol/L
� Moderate 150-159 mmol/L
� Severe > 160 mmol/L

� Pure water depletion
� Hypotonic fluid loss
� Salt gain

� Pure water depletion elderly co-morbidities
� Hypotonic fluid loss
� Salt gain

� Pure water depletion elderly co-morbidities
� Hypotonic fluid loss diabetes inspidus
� Salt gain

� Pure water depletion elderly co-morbidities
� Hypotonic fluid loss diabetes inspidus
� Salt gain rarely seen



High osmolality

High osmolality
I am thirsty and need to drink and hang onto
more water

High osmolality
I am thirsty and need to drink and hang onto
more water
Anti-Diuretic Hormone

High osmolality
I am thirsty and need to drink and hang onto
more water
ADH

High osmolality
I am thirsty and need to drink and hang onto
more water
ADH

High osmolality
I am thirsty and need to drink and hang onto
more water
ADH
Water gets recycled
into blood stream

High osmolality
I am thirsty and need to drink and hang onto
more water
ADH
Water gets recycled
into blood stream

Osmolality stable again
I am thirsty and need to drink and hang onto
more water
ADH
Water gets recycled
into blood stream



Low osmolality

I am not thirsty any more and need to pee
Low osmolality

I am not thirsty any more and need to pee
ADH switched off
Low osmolality

I am not thirsty any more and need to pee
ADH switched off
Water not recycled back
into blood stream
Low osmolality

I am not thirsty any more and need to pee
ADH switched off
Water not recycled back
into blood stream
Low osmolality

I am not thirsty any more and need to pee
ADH switched off
Water not recycled back
into blood stream
Low osmolality

I am not thirsty any more and need to pee
ADH switched off
Water not recycled back
into blood stream
Osmolality stable again


ADH not produced or not working

ADH not produced or not working

ADH not produced or not working
Water cannot get recycled back

ADH not produced or not working
Water cannot get recycled back

ADH not produced or not working
Water cannot get recycled back
Osmolality dangerously high

ADH not produced or not working
Water cannot get recycled back
Osmolality dangerously high
Raging thirst and drink huge amounts

ADH not produced or not working
Water cannot get recycled back
Osmolality dangerously high
Raging thirst and drink huge amounts

� 78 year old lady
� Previous pituitary tumour

� 78 year old lady
� Previous pituitary tumour

� 78 year old lady
� Previous pituitary tumour
� Right sided weakness
� Possible chest infection

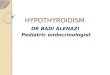
� Desmopressin 200 µg / day
� Hydrocortisone 10/5/5mg
� Thyroxine 100 µg

� Nil by mouth
� CT brain NAD
� Antibiotics
� IV fluids

� Nil by mouth
� CT brain NAD
� Antibiotics
� IV fluids
130
140
150
160
170
180
190
200
0 1 2 4 6 7 8 12 13 14 16 17 23 26
Na
Na

� Nil by mouth
� CT brain NAD
� Antibiotics
� IV fluids
� RIP130
140
150
160
170
180
190
200
0 1 2 4 6 7 8 12 13 14 16 17 23 26
Na
Na



HYPERNATRAEMIA [Na+] >150 mmol/L
Consider the contexte.g. known diabetes insipidus
Stop any offending medicationse.g lithium, demeclocycline
Initial immediate investigation panel• U&E, Glucose• Plasma osmolality• Urine osmolality• Monitor urine output

HYPERNATRAEMIA [Na+] >150 mmol/L
Consider the contexte.g. known diabetes insipidus
Stop any offending medicationse.g lithium, demeclocycline
Initial immediate investigation panel• U&E, Glucose• Plasma osmolality• Urine osmolality• Monitor urine output
• If urine output low and urine osmolality > 800 osm/Kg
• Likely cause is reduced intake with co-morbidities

HYPERNATRAEMIA [Na+] >150 mmol/L
Consider the contexte.g. known diabetes insipidus
Stop any offending medicationse.g lithium, demeclocycline
Initial immediate investigation panel• U&E, Glucose• Plasma osmolality• Urine osmolality• Monitor urine output
• If urine output high and urine osmolality low
• Consider diabetes inspidus

• Discuss with ITU if appropriate / HDU environment
• Close monitoring of fluid balance and electrolytes
• Correction of circulating volume and water deficit
• Consider diabetes inspidus

• Discuss with ITU if appropriate / HDU environment
• Close monitoring of fluid balance and electrolytes
• Correction of circulating volume and water deficit
• Consider diabetes inspidus
• If hypovolaemic, give normal saline until fluid replete
• Switch to 5% dextrose when euvolaemic
• At least 4 hourly serum Na checks
• If known DI, ensure desmopressin is administered


� Mild 2.6-3.0 mmol/L
� Moderate 3.0-3.5 mmol/L
� Severe >3.5 mmol/L

� Hyperparathyroidism or malignancy

� Hyperparathyroidism or malignancy
� High PTH = hyperparathyroidism
� Low PTH = malignancy til proved otherwise

History and clinical context
• Symptoms of hypercalcaemia
• Red flag symptoms and signs of malignancy
• Family history of calcium problems
• Relevant drugs or over the counter treatments

History and clinical context
• Symptoms of hypercalcaemia
• Red flag symptoms and signs of malignancy
• Family history of calcium problems
• Relevant drugs or over the counter treatments
Symptoms of hypercalcaemia
• Polyuria and thirst
• Anorexia, nausea, constipation
• Mood disturbance and cognitive dysfunction

History and clinical context
• Symptoms of hypercalcaemia
• Red flag symptoms and signs of malignancy
• Family history of calcium problems
• Relevant drugs or over the counter treatments
Severe hypercalcaemia
• Low GCS and coma in severe cases
• ECG changes (short QT interval)

History and clinical context
• Symptoms of hypercalcaemia
• Red flag symptoms and signs of malignancy
• Family history of calcium problems
• Relevant drugs or over the counter treatments
Relevant drugs
• Thiazide diuretics
• Calcium / Vitamin D
• Theophylline
• Lithium

Investigation of hypercalcaemia
U&E
Phosphate
PTH
Vitamin D

Investigation of hypercalcaemia
U&E
Phosphate
PTH
Vitamin D
• Renal dysfunction common in severe hypercalcaemia
• Phosphate usually low in hyperparathyroidism
• Vitamin D toxicity rare in clinical practice

� Granulomas
� Immobilisation
� Thyrotoxicosis
� Vitamin D toxicity
� Phaeochromocytoma

First line treatment
• Rehydration with normal saline 4-6L in 24h
• Monitor fluid status and urine output
• Consider IV bisphosphonate

First line treatment
• Rehydration with normal saline 4-6L in 24h
• Monitor fluid status and urine output
• Consider IV bisphosphonate
• Zolendronic acid 4mg over 15 minutes
• Pamidronate 30-90mg at 20mg/hour
• Bisphosphonates will affect PTH result

First line treatment
• Rehydration with normal saline 4-6L in 24h
• Monitor fluid status and urine output
• Consider IV bisphosphonate
Second line treatment
• Prednisolone
• Calcitonin
• Calcimimetics
• Parathyroidectomy
• Zolendronic acid 4mg over 15 minutes
• Pamidronate 30-90mg at 20mg/hour
• Bisphosphonates will affect PTH result

First line treatment
• Rehydration with normal saline 4-6L in 24h
• Monitor fluid status and urine output
• Consider IV bisphosphonate
Second line treatment
• Prednisolone
• Calcitonin
• Calcimimetics
• Parathyroidectomy
• Steroids if lymphoma or granuloma
• Cinacalcet (calcimimetic)

� If young or recurrent consider MEN-1
� If severe consider parathyroid carcinoma
� If mild and family history exclude FHH


� Mild Ca > 1.9 mmol/L no symptoms
� Severe Ca < 1.9 mmol/L symptoms

� Can be life threatening
� Rate of change very important
� IV calcium mainstay of inpatient treatment

Peri-oral and digital parasthesia
Trousseau’s / Chvostek’s sign
Tetany and carpo-pedal spasm
Laryngospasm
ECG changes (prolonged QT interval)
Seizures

Peri-oral and digital parasthesia
Trousseau’s / Chvostek’s sign
Tetany and carpo-pedal spasm
Laryngospasm
ECG changes (prolonged QT interval)
Seizures
Commonest cause disruption of parathyroids post-thyroidectomy
May be temporary or permanent

Peri-oral and digital parasthesia
Trousseau’s / Chvostek’s sign
Tetany and carpo-pedal spasm
Laryngospasm
ECG changes (prolonged QT interval)
Seizures
Commonest cause disruption of parathyroids post-thyroidectomy
May be temporary or permanent
Consider other causes of hypocalcaemia
Severe Vitamin D deficiency
Hypomagnesaemia

Acute severe hypocalcaemia (<1.9) with symptoms • Ensure airway stable and cardiac monitor
• 10-20ml 10% calcium gluconate in 50-100 mls 5% dextrose over 1o mins
• Continuous calcium gluconate infusion (100ml 10% in 1 L saline)*
*Infuse initally at 50-100ml per hourTitrate by clinical and biochemical response

Acute severe hypocalcaemia (<1.9) with symptoms • Ensure airway stable and cardiac monitor
• 10-20ml 10% calcium gluconate in 50-100 mls 5% dextrose over 1o mins
• Continuous calcium gluconate infusion (100ml 10% in 1 L saline)*
On-going management once stabilised• Reversal of underlying cause of hypocalcaemia
• 1-α calcidol 0.25-0.5µg/day
• Sandocal 1000 1 tablet twice daily
• Ensure specialist follow up
*Infuse initally at 50-100ml per hourTitrate by clinical and biochemical response

� Functional hypoparathyroidism
� Proton pump inhibitors
� Gastro-intestinal loss
� Cytotoxic drugs
� Alcohol

� Functional hypoparathyroidism
� Proton pump inhibitors
� Gastro-intestinal loss
� Cytotoxic drugs
� Alcohol
Remove cause and give IV MgSo4 24mmol/24 hours


� 32 year old man
� Thunderclap headache
� Double vision
� 3rd nerve palsy

� 32 year old man
� Thunderclap headache
� Double vision
� 3rd nerve palsy

� Na 129 mmol/l
� K 3.8 mmol/l
� Urea 5.6 mmol/l
� Cr 88 μmol/l
� Gl 5.7 mmol/l
� WBC 11.8 x 109/l
� CRP < 5 mg/l

� Na 129 mmol/l
� K 3.8 mmol/l
� Urea 5.6 mmol/l
� Cr 88 μmol/l
� Gl 5.7 mmol/l
� WBC 11.8 x 109/l
� CRP < 5 mg/l
� LP normal

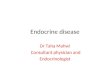
sagittal coronal

sagittal coronal

sagittal coronal

sagittal coronal



� Pituitary apoplexy
� Vascular event within a pituitary tumour

• Basic resuscitation, analgesia, fluid balance
• Consider cortisol status
• Assess visual fields
• Pituitary hormone screen
• Basic resuscitation, analgesia, fluid balance
• Consider cortisol status
• Assess visual fields
• Pituitary hormone screen

• Basic resuscitation, analgesia, fluid balance
• Consider cortisol status
• Assess visual fields
• Pituitary hormone screen
• Basic resuscitation, analgesia, fluid balance
• Consider cortisol status
• Assess visual fields
• Pituitary hormone screen
• Check random cortisol (< 100 nmol/L diagnostic)
• If unwell give hydrocortisone 100mg IV
• T4, TSH, Prolactin, IGF-1, LH, FSH, Testo / E2
• Check random cortisol (< 100 nmol/L diagnostic)
• If unwell give hydrocortisone 100mg IV
• T4, TSH, Prolactin, IGF-1, LH, FSH, Testo / E2

• Basic resuscitation, analgesia, fluid balance
• Consider cortisol status
• Assess visual fields
• Pituitary hormone screen
• Basic resuscitation, analgesia, fluid balance
• Consider cortisol status
• Assess visual fields
• Pituitary hormone screen
• Check random cortisol (< 100 nmol/L diagnostic)
• If unwell give hydrocortisone 100mg IV
• T4, TSH, Prolactin, IGF-1, LH, FSH, Testo / E2
• Check random cortisol (< 100 nmol/L diagnostic)
• If unwell give hydrocortisone 100mg IV
• T4, TSH, Prolactin, IGF-1, LH, FSH, Testo / E2
• Medical stabilisation most important thing
• Conservative management usually sufficient
• Deteriorating vision / reduced GCS may need surgery
• Needs specialist endocrinology / pituitary surgeon
• Medical stabilisation most important thing
• Conservative management usually sufficient
• Deteriorating vision / reduced GCS may need surgery
• Needs specialist endocrinology / pituitary surgeon




� Consider in all SVT
� High T4, TSH < 0.05

� Consider in all SVT
� High T4, TSH < 0.05

� Thyroid storm vanishingly rare
� High output pulmonary oedema (ITU)

� Thyroid storm vanishingly rare
� High output pulmonary oedema (ITU)
� Agranulocytosis with carbimazole
� Cytopaenias common in hyperthyroidism

� Consider in hypothermia
� Low T4, TSH > 100

� Consider in hypothermia
� Low T4, TSH > 100

� Very high mortality (ITU)
� Supportive treatment
� Thyroxine replacement
� Pericardial effusion
� Adrenal crisis

� Sodium
� Calcium
� Pituitary
� Thyroid