Embed Size (px)
Citation preview
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh Sr. Lecturer Dept. of Pediatric & Preventive Dentistry
Dr. Shruti Singh, Subharti Dental College, SVSU

Introduction
Embyological aspects
Etiology and Diagnosis
Classification of cleft lip and palate
Types of clefting
Facial growth in unrepaired CLP cases
Orthodontic management of CLP
- Infant orthopedics
- Primary dentition period
- Mixed dentition period
- Permanent dentition period
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

“ ORO - FACIAL DEFORMITY ”
Dr. Shruti Singh, Subharti Dental College, SVSU

1 in 600 – 1000 live births
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Failure of fusion
Dr. Shruti Singh, Subharti Dental College, SVSU

HANDICAPPING MALOCCLUSION AND
HANDICAPPING DENTOFACIAL DEFORMITY
- J.A.Salzmann
Definition : conditions that are harmful to the physical,
psychodynamic and social well-being of the person by
adversely affecting the health, function and esthetics
of the facio-oro-dental tissues.
Am . J . Orthodontics, March 1966
Dr. Shruti Singh, Subharti Dental College, SVSU

The cleft can be diagnosed by high resolution
ultrasound at 18 weeks of gestation.
Diagnosis is otherwise made after delivery.
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU
Defective muscular supply to the area involved
Mechanical disturbance in which the size of the
tongue may prevent the union of the parts
Circulating substances like alcohol and certain drugs
and toxins
Infections
Lack of inherent developmental force
Dr. Shruti Singh, Subharti Dental College, SVSU

Hereditary/Polygenic Syndromic/Manogenic
Dr. Shruti Singh, Subharti Dental College, SVSU
MSX 1
TGFA
TGFB 1
TGFB 2
IRF 6
BCL 3
BMP 4
BMP 3
PAX 7
PAX9
Seminars in Orthodontics June 2008
Dr. Shruti Singh, Subharti Dental College, SVSU
Dr. Shruti Singh, Subharti Dental College, SVSU

Davis and Ritch classification :
Group I – Pre alveolus clefts (clefts involving only lip)
Unilateral
Bilateral
Median
Dr. Shruti Singh, Subharti Dental College, SVSU

Group II – Post Alveolar Clefts
- comprises of different degrees of hard and soft
palate clefts that extend upto the alveolar ridge.
Unilateral
Bilateral
Median
Dr. Shruti Singh, Subharti Dental College, SVSU

Group III – Alveolar clefts :
Complete clefts involving the
- palate
- alveolar ridge
- lip
Dr. Shruti Singh, Subharti Dental College, SVSU

Group I : Clefts involving only the soft palate
Group II : Clefts of hard and soft palate extending
upto the incisive foramen.
Dr. Shruti Singh, Subharti Dental College, SVSU

Group III : Complete unilateral cleft involving the
soft palate, hard palate, lip and alveolar
ridge.
Group IV : Complete bilateral clefts affecting the soft
palate, hard palate, lip and alveolar ridge.
Dr. Shruti Singh, Subharti Dental College, SVSU

Group I Group II Group III
- lip - lip and palate - clefts of
palate
unilateral unilateral
bilateral bilateral
Dr. Shruti Singh, Subharti Dental College, SVSU

Group I
Clefts of lip only
Group II
Clefts of palate only
(2o)
Group III
Clefts of lip,
alveolus, palate
Group IV
Clefts of lip and
alveolus
(primary cleft
palate and lip) Group V
Miscellaneous
Dr. Shruti Singh, Subharti Dental College, SVSU

1 and 4 - Lip
2 and 5 - Alveolus
3 and 6 - Hard palate anterior
to incisive foramen
7 and 8 - Hard palate posterior
to incisive foramen
9 - Soft palate Dr. Shruti Singh, Subharti Dental College, SVSU

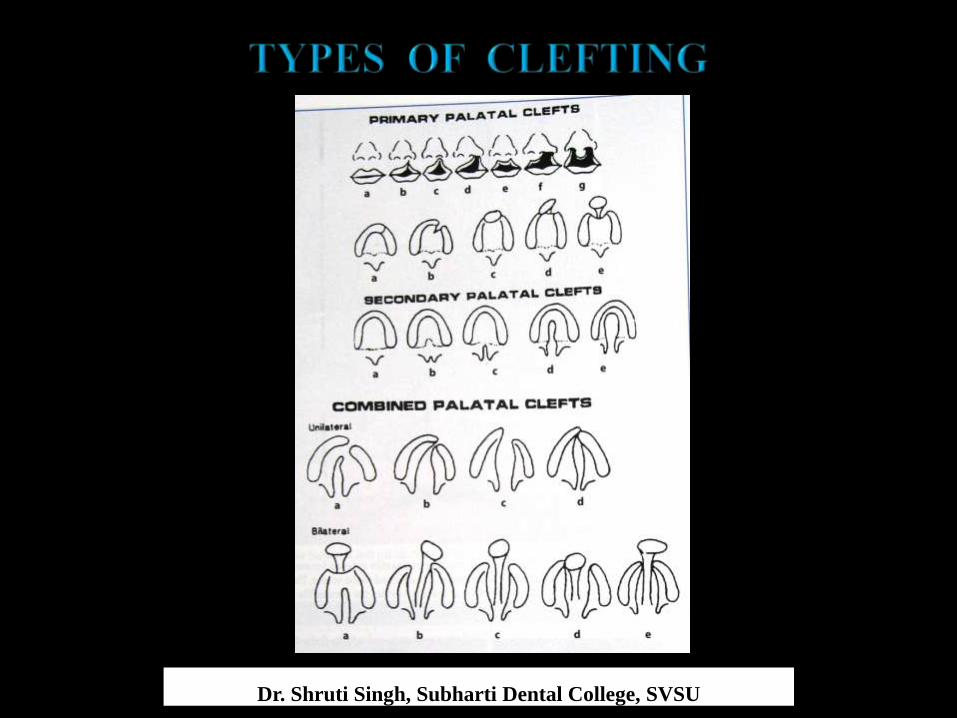
Clefts of primary palate ( unilateral and bilateral )
Clefts of primary and secondary palate
Clefts of secondary palate
Dr. Shruti Singh, Subharti Dental College, SVSU
Dr. Shruti Singh, Subharti Dental College, SVSU

SKELETAL GROWTH :
Facial width :
- Generalised increase in width of facial strucutres
which appears to persist throughout growth.
- Head width is relatively greater than head length.
Dr. Shruti Singh, Subharti Dental College, SVSU

- Orbits are further apart than in normal.
- Maxilla which was wider in infancy remains wide.
Dr. Shruti Singh, Subharti Dental College, SVSU

- Palatal shelves are deficient in width.
Dr. Shruti Singh, Subharti Dental College, SVSU

- Clubbing of the shelf ends suggest that the growth is
being distorted probably by the tongue.
- The buccolingual occlusion of the posterior teeth is
invariably excellent.
Dr. Shruti Singh, Subharti Dental College, SVSU

- Mild deficiency of maxillary bone if present is
compensated for by an adjustment in the direction of
dental eruption and alveolar apposition.
- Anterior nasal spine is markedly deviated to the non
cleft side.
Dr. Shruti Singh, Subharti Dental College, SVSU

Facial height :
- Maxillary height in unilateral clefts
slightly less on the cleft side than on non-cleft side.
- Height of nasal cavity may be less in infants but greater
in adults .
Dr. Shruti Singh, Subharti Dental College, SVSU

Facial depth :
Infants with unilateral CLP or isolated cleft palate
Maxilla is more retrusive
Older children and adults
Maxilla is in a normal position
Dr. Shruti Singh, Subharti Dental College, SVSU

Pre-maxillary area
rotated forward and laterally in unilateral clefts
advancing the nasal spine maxillary protrusion
Dr. Shruti Singh, Subharti Dental College, SVSU

Pterygoid process
abnormal in size and direction of growth
adults with cleft palate and unilateral CLP
Dr. Shruti Singh, Subharti Dental College, SVSU

Growth of Nose :
- Tip of nose retrusive (all types of clefts)
Dr. Shruti Singh, Subharti Dental College, SVSU

- Nasal bones distorted (infants with UCL)
- Nasal bone flattened on cleft side
- Short columella + nasal tip is slumped and blunted.
bilateral clefts
Dr. Shruti Singh, Subharti Dental College, SVSU

Musculature :
Bilateral case
severe under-development and atrophy of prolabium
Unilateral cases
upper lip less protrusive
lower lip protrusive
Dr. Shruti Singh, Subharti Dental College, SVSU

Dental occlusion :
Maxillary buccal teeth
usually in normal buccolingual r/s with mandibular teeth
(in CLP cases)
Maxillary incisors protrusive ( bi CLP)
Mandibular incisors less protrusive
Interincisal angle is normal.
Dr. Shruti Singh, Subharti Dental College, SVSU

In unilateral cleft lip and palate:
- maxillary incisors tip towards the cleft
- occasionally an open bite in the incisor region
- maxillary cuspids generally incline towards the cleft
and displaced medially
- posterior occlusion is invariably quite acceptable
Dr. Shruti Singh, Subharti Dental College, SVSU

Jaw and tooth relations :
Retrusion of maxillary basal bone in CP and uni CLP
balanced by
rotation of the mandible and consequent retrusion of chin
Antero posterior jaw r/s :
- young children : satisfactory
- older children : progressively worsen
Dr. Shruti Singh, Subharti Dental College, SVSU

MULTIDISCIPLINARY CLEFT MANAGEMENT
Cleft lip and palate
commonest craniofacial anomaly
INTERDISCIPLINARY TEAM OF SPECIALISTS
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Pre surgical infant
orthodpedics : 0-4 weeks
Lip closure : 8-12 weeks
Palate closure : 18-24 months
Speech therapy : 6-11 years
Early orthodontics : 7-8 years
Dr. Shruti Singh, Subharti Dental College, SVSU

Alveolar grafting : 6-10 years
Comprehensive orthodontics : 11-14 years
Pharyngeal flap surgery : 9-19 years
Orthognathic surgery : 17-19 years
Fixed Prosthodontics : 17-19 years
Dr. Shruti Singh, Subharti Dental College, SVSU

They can be broadly classified as :
a) Dental
b) Esthetic
c) Speech and Hearing
d) Psychologic.
Dr. Shruti Singh, Subharti Dental College, SVSU

Congenitally missing teeth (upper lateral)
Presence of natal or neonatal teeth
Ectopically erupting teeth
Anomalies of tooth morphology.
Enamel hypoplasia
Microdontia
Dr. Shruti Singh, Subharti Dental College, SVSU

Fused teeth
Macrodontia
Mobile and early shedding of teeth
( poor periodontal support )
Posterior and anterior cross bite
Protruding premaxilla
Deep bite
Spacing or crowding.
Dr. Shruti Singh, Subharti Dental College, SVSU

Facial disfigurement
Malformed oro-facial structures
Congenitally missing oro-facial structures
Deformities of nose
Dr. Shruti Singh, Subharti Dental College, SVSU

CLP
disorders of the middle ear
affect hearing
difficulties in language uptake and speech
Dr. Shruti Singh, Subharti Dental College, SVSU
CLP
lot of psychological stress
- Due to their abnormal facial appearances
- Put up with staring, curiosities, pity etc.
- Problems in obtaining job and making friends
- Fare badly in academics
Dr. Shruti Singh, Subharti Dental College, SVSU

Presurgical orthopedics : 0-3 months
Interceptive orthopedics : 6-7 yrs
Alignment of maxillary incisors prior to secondary
alveolar bone grafting
Dr. Shruti Singh, Subharti Dental College, SVSU

Secondary alveolar bone grafting of the cleft alveolar
process
Conventional orthodontics in the permanent dentition
Prosthodontic or orthognathic surgery : 17-19yrs
Dr. Shruti Singh, Subharti Dental College, SVSU

By C. Kerr McNeil
Performed on new born before surgical repair of lip.
Rationale...realignment of the collapsed segments
before surgery.
Dr. Shruti Singh, Subharti Dental College, SVSU

In bilateral CLP – maxillary alveolar segments are
displaced at the time of birth.
In unilateral CLP - premaxillary segment likely to be
displaced facially adjacent to cleft
Dr. Shruti Singh, Subharti Dental College, SVSU

Displacement of bony segments
separation of the soft tissue segments
lip repair more difficult
Dr. Shruti Singh, Subharti Dental College, SVSU

To achieve a more normal skeletal base under the lip
and nose
Maxilla becomes more symmetrical.
Lip fissure is narrowed considerably.
There may be slight advancement of the smaller
maxillary segment.
Dr. Shruti Singh, Subharti Dental College, SVSU

TYPES OF NEONATAL MAXILLARY ORTHOPEDIC
APPLIANCES
Pin-retained active appliances and passive appliances
- Active
- Semi-active
- Passive
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Control and modify the postnatal development of the
maxilla
Stimulate palatal shelf growth
Aids the plastic surgeon
Prevents tongue distortions
Prevents nasal septum irritation
Dr. Shruti Singh, Subharti Dental College, SVSU
Decreases the number of ear infections
Expands the collapsed maxillary segments
Repositioning of pre maxilla
Aids in nursing
Helps the mother psychologically.
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

NASOALVEOLAR MOULDING
- Grayson et al,. ( 1993 )
Reduces the severity of the initial cleft alveolar and
nasal deformity.
Dr. Shruti Singh, Subharti Dental College, SVSU

Improved long term esthetics
A reduced number of nasal surgical procedures
A reduced need for secondary bone grafts
No larger growth disturbance than is found for other
well-established procedures.
Savings in cost
Dr. Shruti Singh, Subharti Dental College, SVSU

Intra oral moulding plate
with nasal stents
to mould the alveolar ridge and nasal cartilage concurrently
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Reduce the severity of the original cleft deformity
better repair of the alveolus, lip and nose
( by the surgeon )
better and more predictable surgical results
Dr. Shruti Singh, Subharti Dental College, SVSU

NAM technique
also eliminated surgical columella reconstruction
resultant scar tissue in bilateral cleft lip and palate
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU
Orthodontic management of CLP
- Primary dentition period
- Mixed dentition period
- Permanent dentition period
Goslon yardstick
Stem cell therapy for CLP
Conclusion
Dr. Shruti Singh, Subharti Dental College, SVSU

2-3 yrs
classification of the type of developing malocclusion
DIAGNOSTIC REGIMEN
skeletal and dental components
IDENTIFIED
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU
primary incisors more upright
anterior crossbite unilateral / bilateral
with / without functional shift
of mandible
Dr. Shruti Singh, Subharti Dental College, SVSU

To eliminate mandibular shifts
ORTHODONTIC TREATMENT
maxillary anteriors ( anterior crossbite ) /
expansion of posterior segments
to eliminate posterior crossbite
Dr. Shruti Singh, Subharti Dental College, SVSU

If dental crossbite a continuing problem
reflects underlying skeletal discrepancy
Growth modification and redirection
“FACIAL MASK”
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Orthopedic forces for maxillary protraction
350-500 gm per side over 10-12 hr/day
average of 12-15 months
Dr. Shruti Singh, Subharti Dental College, SVSU
Stability…….(Questionable)
Because of two reasons
Counter pressure of a tight lip on the maxilla
which inhibits its growth
Scarring in the pterygo maxillary region after
extensive tissue mobilization for palatal closure
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Child co-operation
Severity of the malocclusion
Timing of secondary bone grafts
Need for future orthodontic treatment in early mixed
or permanent dentitions
Dr. Shruti Singh, Subharti Dental College, SVSU

Transition to mixed dentition : 6 to 7 yrs
Further growth of the craniofacial complex
accentuates
previously mild skeletal discrepancy
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU
Elimination of the residual cleft
ALVEOLAR BONE GRAFTING
major advance in contemporary management
cleft maxilla
Dr. Shruti Singh, Subharti Dental College, SVSU

PRIMARY ALVEOLAR BONE GRAFTING
at the time of lip closure
10-12 weeks ( in 1950’s )
- Causes hinderance in maxillary growth
Dr. Shruti Singh, Subharti Dental College, SVSU
Performed after primary lip repair
- Early secondary bone grafting ( 2-5 yrs )
- Intermediate or secondary bone grafting ( 6-15 yrs)
- Late secondary bone grafting ( adolescene to adulthood)
Dr. Shruti Singh, Subharti Dental College, SVSU

Provides bone support for unerupted teeth and those
teeth adjacent to the cleft
Closure of the oronasal fistulae
Dr. Shruti Singh, Subharti Dental College, SVSU

Support and elevation of the alar base on the cleft side
Construction of a continuous arch form and alveolar
ridge
Achieve stabilization and some repositioning of the
premaxilla in those patients with a bilateral cleft
Dr. Shruti Singh, Subharti Dental College, SVSU
TIMING
depends on dental development than on
chronological age
Ideally : permanent canine root should be half to
two thirds formed at the time graft is placed
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU
SEQUENCING
Most appropriate time for grafting
INTERMEDIATE PERIOD ( 6-15 yrs)
greatest benefits and least risk for interfering with
Midfacial and skeletodental growth and development
Dr. Shruti Singh, Subharti Dental College, SVSU

Decayed teeth adjacent to the cleft to be restored
Good oral hygiene practices
Reposition maxillary teeth that are in traumatic
occlusion
Expand a severely constricted maxilla
Erupted teeth adjacent to cleft with poor periodontal or
endodontal prognosis to be extracted atleast 2 months
in advance Dr. Shruti Singh, Subharti Dental College, SVSU

Transverse dimension
Incisor alignment
Eruption of maxillary canines
Dr. Shruti Singh, Subharti Dental College, SVSU

- Transverse dimension
Retention of corrected crossbite
orthodontic appliances post-surgically
Because bone graft is unlikely to stabilize the expansion
Dr. Shruti Singh, Subharti Dental College, SVSU

- Incisor alignment
- If appliances have been placed presurgically
orthodontic tooth movements delayed until
3-6 weeks following bone grafting
Dr. Shruti Singh, Subharti Dental College, SVSU

- Eruption of the maxillary canine
orthodontic tooth movement
space is created in the arch
canine erupts successfully
Dr. Shruti Singh, Subharti Dental College, SVSU

AUTOGENOUS GRAFTS :
- Iliac
- Tibia
- Rib
- Cranial bone
ALLOGENOUS GRAFTS :
- Freeze dried bone
Dr. Shruti Singh, Subharti Dental College, SVSU
With eruption of canines and premolars
Permanent dentition is established
Adolescent growth spurt and onset of puberty occur
Dr. Shruti Singh, Subharti Dental College, SVSU

Skeletal discrepancy
accentuated
Facial appearance +
occlusal relationships
deteriorate
Dr. Shruti Singh, Subharti Dental College, SVSU
Medial displacement of the maxillary segment giving
buccal cross bite
Relative maxillary retrognathism, giving reversed
incisal overjet.
Deficiency of vertical growth of the upper jaw –
REDUCED FACIAL HEIGHT
Dr. Shruti Singh, Subharti Dental College, SVSU

Rotation, malposition and hypodontia of teeth.
Supernumerary teeth
Accentuated curve of spee in maxilla
Collapsed arch forms
Poor oral hygiene and caries
Dr. Shruti Singh, Subharti Dental College, SVSU
Full fixed appliance
GOALS :
- Achieve alignment and arch form
- Resolve anterior and or posterior cross-bite tendencies
Dr. Shruti Singh, Subharti Dental College, SVSU

Expansion appliance
Quad Helix Rapid Maxillary Expansion (RME)
Dr. Shruti Singh, Subharti Dental College, SVSU

Close the lateral incisor space by substituting canines
brings the posterior segments into a class II r/s
or make compensatory extractions in madibular arch
Dr. Shruti Singh, Subharti Dental College, SVSU

Maintain or create space for prosthetic build up or
replacement of the missing lateral incisor
Class I molar r/s and a non extraction approach
to the lower arch
Dr. Shruti Singh, Subharti Dental College, SVSU

If growth deficiency is mild
orthodontic treatment
If growth deficiency is severe
orthognathic surgery at the end of growth
Dr. Shruti Singh, Subharti Dental College, SVSU

Due to severe skeletal discrepancy
deterioration of esthetics and occlusion
Orthodontic and Orthognathic approach
Dr. Shruti Singh, Subharti Dental College, SVSU

Size and position of maxilla is often a problem
Thus maxillary advancement and occasional grafting
needs to be performed.
To correct the transverse problem multiple segment
Lefort I osteotomies may be required.
Dr. Shruti Singh, Subharti Dental College, SVSU

For bilateral CLP
three-piece maxillary surgery
( allows rotation of segments also )
For unilateral CLP
two-piece maxillary surgery
( Vlachos 1996 )
Dr. Shruti Singh, Subharti Dental College, SVSU
Usually requires 12 months
Multiple segment maxillary osteotomies requires
segmental treatment.
The bracket positions are altered for teeth adjacent
to the osteotomy site.
Dr. Shruti Singh, Subharti Dental College, SVSU

Proffit recommends overcorrecting the anterior
crossbite - compensate for post surgical relapse.
Cases with overjet of more than 8mm - Mandibular
surgery (BSSO) also must be considered.
If not , over advancement of maxilla – unstable and
speech defects.
Dr. Shruti Singh, Subharti Dental College, SVSU

Post surgical orthodontics:
- Detailing of occlusion
- Closure of residual spaces
- Maintenance of transverse dimension
- Lasts for 4-6 months.
Dr. Shruti Singh, Subharti Dental College, SVSU

RETENTION :
Retainers to be placed immediately after removal of
appliance
Soldered lingual arch preferred
Dr. Shruti Singh, Subharti Dental College, SVSU

TIMING :
Never indicated in active facial growth
Ideal time : 18-19 yrs
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Gavril ( 1903 )
Types :
- external distractors
- internal distractors
Dr. Shruti Singh, Subharti Dental College, SVSU

Advantage : direction of force is well controlled
Disadvantage : cranial surgery is required
esthetics are compromised
Dr. Shruti Singh, Subharti Dental College, SVSU

Advantage:
• Esthetics
• Psychological relief
Disadvantage:
• Difficult to control the
direction of force
Dr. Shruti Singh, Subharti Dental College, SVSU

Replacement of missing teeth
Removable or fixed appliances
improves speech and esthetics
Dr. Shruti Singh, Subharti Dental College, SVSU

A new system of assessing dental arch relationships
in children with unilateral clefts of lip and palate
The GOSLON ( Great Ormond Street London and
Oslo ) Yardstick is a clinical tool that allows
categorization of the dental arch relationships in the
late mixed and or early permanent dentition stage into
five discrete categories
Dr. Shruti Singh, Subharti Dental College, SVSU

Cases are allocated to these categories on a value
judgement basis by reference to the anchor groups of
the Goslon yardstick
The clinical features that are considered most
important in characterizing malocclusions in the early
permanent dentition stages of children with unilateral
clefts of lip and palate are :
Dr. Shruti Singh, Subharti Dental College, SVSU

Anteroposterior arch relationships
Vertical labial segment relationships
Transverse relationships
Dr. Shruti Singh, Subharti Dental College, SVSU

Severe class III incisor relationship - least satisfactory
Class II division 1 relationship - most favourable
Pre-existing dentoalveolar compensation in the
presence of a reverse overjet - not favourable
Dr. Shruti Singh, Subharti Dental College, SVSU

Deep overbite preferable to a reduced overbite
which, in turn , was considered a better situation
than an open bite.
Dr. Shruti Singh, Subharti Dental College, SVSU

Canine cross-bites of the smaller segment were
considered worse than molar cross-bites
The degree of transverse arch narrowness, rather
than the number of teeth in crossbite, is the critical
factor
Dr. Shruti Singh, Subharti Dental College, SVSU

Anteroposterior relationships
greatest clinical importance
Generalised crowding and irregularity
relatively unimportant
Dr. Shruti Singh, Subharti Dental College, SVSU

GROUP 1 - Excellent
GROUP 2 - Good
GROUP 3 - Fair
GROUP 4 - Poor
GROUP 5 - Very poor
Dr. Shruti Singh, Subharti Dental College, SVSU

Groups 1 and 2 - Orthodontic treatment/ none
Group 1 - Complex orthodontic treatment with
good results
Group 4 - limitations of orthodontic treatment
without orthognathic surgery
Group 5 - Orthognathic surgery
Dr. Shruti Singh, Subharti Dental College, SVSU

Highly reliable
Capable of discriminating among the quality of
results at different centres
Dr. Shruti Singh, Subharti Dental College, SVSU

Platelet-rich-plasma (PRP) extracted from autologous
whole blood is known to have a number of different
growth factors in high concentration
PRP is a safe and a cost-effective source of growth
factors .
Enhance osteogenesis of alveolar bone grafting in CLP
patients
Dr. Shruti Singh, Subharti Dental College, SVSU

Muscle derived stem cells have potential for alveolar
bone reconstruction in CLP patients :
Study has shown that cells from orbicularis oris
muscle have phenotypic and behavior characteristics
similar to other adult stem cells, both in vitro and in
vivo.
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU

• CRANIOFACIAL DEVELOPMENT- Sperber
• Surgical orthodontic treatment- Proffit and White
• Grayson etal, Pre surgical naso alveolar molding, cleftliip- craniofacial journal 1999:35
• Cleft Lip and Palate, Diagnosis and Management – Samuel Berkowitz 2nd edition
• Graber. Vanarsdall . Vig – Current Principles and Techniques 4th editionAdvances in management of cleft palate: Edwards and Watson
• Cleft lip and palate, Seminars in Orthodontics
• Baik et al. surgical orthodontic treatment in patients with clcp: conventional surgery vs maxillary distraction, world J Orthod;2:331-40
Dr. Shruti Singh, Subharti Dental College, SVSU

Dr. Shruti Singh, Subharti Dental College, SVSU