-
8/9/2019 Drama as an Experiential Technique
1/14
Teaching in Higher Education, Vol. 6, No. 1, 2001
Drama as an Experiential
Technique in Learning How toCope with Dying Patients and
theirFamiliesPAT DEENY, ALPHY JOHNSON*, JENNIFER BOORE,CATHERINE
LEYDEN & ELLIS McCAUGHAN
Centre for Nursing Research, University of Ulster, Coleraine,
County Londonderry,BT52 1SA, and *School of Nursing and Midwifery,
The Queens University of
Belfast, 13 College Park East, Belfast, BT7 1LQ, UK
ABSTRACT This paper discusses a teaching experiment in which
participation and observation
of a drama helped rst year nursing students to consider ways of
dealing with death and dying.
Workshops included dramatised scenarios of critical incidents
demonstrating different peoples
experiences of the death of a ctional patient in hospital. Two
nurse teachers performed a
two-part drama about the experiences of a patient just diagnosed
with terminal cancer. Live
performances were presented to large groups of students and
followed by small group discussions.
Drama as a teaching method was well received, and the
combination of drama and group
discussion was considered very effective by students, who
requested more similar sessions. Drama
appears highly satisfactory for achieving learning in the
affective domain, and can be added to
teaching methods for improving communication skills and coping
strategies with nursing
students who will be caring for the dying. However, further
research is necessary.
Introduction and Literature Review
Caring for dying patients can be an emotionally painful,
distressing, and sometimes
threatening experience for nurses and other health care
professionals as the illness is
incurable and death imminent; nurses may feel powerless to help
the patients
distress and suffering. Often this generates feelings of anger,
guilt, fear and loss of
control (Mandel, 1981). Nurses may worry about what to say or
do, and feel
ill-equipped to give the sympathy and support which patients and
relatives need(Ferszt, 1984; Hurtig & Stewin, 1990; Servaty et
al., 1996; OGorman, 1998). They
may feel anxious and this is strongly linked to fear of their
own death (Popoff, 1975;
OGorman, 1998). Nurses may not have learnt to deal with their
own feelings in
Correspondence: Mr P. Deeny, University of Ulster, Cromore Road,
Coleraine, Co. Londonderry
BT52 1SA, UK. E-mail: PG.Deeny @ulst.ac.uk
ISSN 1356-2517 (print)/ISSN 1470-1294 (online)/01/010099-14 2001
Taylor & Francis LtdDOI: 10.1080/13562510020029635
-
8/9/2019 Drama as an Experiential Technique
2/14
100 P. Deeny et al.
relation to death and dying, and may resort to coping strategies
such as distancing
themselves emotionally and physically from their dying patients
(Ross, 1978). These
problems can be avoided if nurses are helped to face their own
personal concerns
with death and dying, and are taught ways to relate to dying
patients and their
families. This should begin early in nurse education to promote
personal awareness
of death-related fears so that anxieties can be dealt with
before caring for thesepatients and their families.
Despite possible inner turmoil, nurses assume important roles
with dying
patients in providing practical and emotional care
(Haiseld-Wolfe, 1996). They are
also expected to provide support for patients families, helping
to maintain
emotional well-being of all involved. This is only possible if
nurses are educationally
prepared, and possess good interpersonal skills and personal
coping strategies.
Nurse educators must nd teaching processes that stimulate
learning in the affective
domain, that is, facilitating students understanding about
emotional aspects of thesubject and the feelings and fears of all
involved (Hurting & Stewin, 1990; Sawatzky,
1998).
Within the affective domain of learning Bloom (1955) described a
hierarchy of
ve levels, in ascending order: receiving or attending,
responding, valuing, organis-
ing (or conceptualising) and internalising. It is recognised as
an area in which setting
and evaluating achievement of objectives is difcult (Mellish
& Brink, 1990). Within
nursing education relatively little work has been undertaken
which evaluates meth-
ods of enhancing learning within this domain, and none that
assesses the intensity
and long-term stability of affective change in relation to death
and dying. However,experiential learning methods are commonly
recommended (Wise, 1974; Parkes,
1985; Lyons, 1988), and are reported as particularly valuable
when teaching
interpersonal communication and human skills such as empathy and
understanding,
as students are able to explore personal views and reactions
(Ferszt, 1984; Burnard,
1985; Quinn, 1997).
Evaluation of Education Related to Death and Dying
Education about death and dying has been criticised as
inadequate (Birch, 1983;
Whiteld, 1983) with nurses being prepared to give physical, but
not psychological
or spiritual care (Doyle, 1982). Several authors (Birch, 1983;
Hockley, 1989;
Frommelt, 1991) reported students and registered nurses
criticism of their teaching
on the subject, and suggested that instruction was inadequate to
prepare them for
the real situation. Mackay (1989) reported that death was a
common fear of learners
entering nursing, but by their second ward experience initial
apprehensions had
diminished, although students still found their early
experiences trying. Where
education was adequate, there was still disparity between theory
and practice (Field& Kitson, 1986; Johnson, 1994).
Stress is common when students anticipate situations concerning
death or
suffering of a patient (Kieger, 1993; Rhead, 1995). Dealing with
death and dying is
the second most frequently cited stressor among nurses of all
levels (Lees & Ellis,
1990). In particular, seeing and handling a corpse, and the idea
of losing a much
-
8/9/2019 Drama as an Experiential Technique
3/14
Drama as an Experiential Technique 101
cared for patient were considered to be most distressful. Kieger
(1994) reported that
at the commencement of training students expressed feelings of
dread, uncertainty
and concern about the nature of the dying process, especially
how it would affect
them. Much of this concern grew out of their relative
inexperience with death and
fear of being unable to cope with emotional care, the pain of
seeing suffering, shock
of seeing a dead body and difculty of dealing with bereaved
relatives.This theme of personal inadequacy and fear of mistakes is
frequently cited in
literature about stress in nursing students (McKay, 1978;
Pagana, 1988; Lindrop,
1991; Sawatzky, 1998) and is not unique in caring for dying
patients. Some studies
reported good and bad experiences with death where students
reected upon and
discussed both satisfying and negative aspects of caring for a
dying patient and their
relatives (Johnson, 1994; Kieger, 1994). Regardless of students
preconceived ideas
about death, the learning through experience of caring for dying
patients remained
a particular challenge.Kieger (1993) stressed the difference
between knowing about and knowing.
Inevitably, there will be a disparity between the students
expectations and their
experience since they cannot really know nursing until they have
experienced it.
Despite perceived inadequacies about the care they deliver to
the dying person and
family, many will form deep personal and emotional bonds with
patients, and gain
satisfaction from providing high quality care (Melia, 1983;
Kieger, 1994). How well
they then cope with death of the patient depends on numerous
factors, including
personal coping resources (Sawatzky, 1998), previous experiences
of death
(OGorman, 1998), support by colleagues (Mackay, 1989) and their
educationalpreparation. Education which develops their emotional
resources to deal with this
stressful experience will provide a foundation for continuing
enhancement of the
necessary caring skills. Development of interactive abilities
and knowledge about
dying must be preceded by dealing with fears and emotional needs
about the
subject.
Experiential Learning about Death and Dying
In teaching about death and care of the dying patient, nurse
educators must
challenge societal perceptions of death and dying, and
facilitate nursing students in
developing a deeper insight into individual responses.
Programmes that promote
affective learning, that is interpersonal awareness and empathy
with others, are
fundamental (Burnard, 1996). A teaching method that increases
students interest
and involvement, and helps them to see connections between
abstract ideas and
concrete phenomena is needed.
Students learn from experiencing and participating, and learning
is enhanced if
students can process their recent experience by reecting,
describing, talking aboutand analysing what they have seen and done
(National Society for Experiential
Education, 1997). The experiential learning cycle consists of
four stages that actively
engage the participants to stimulate learning: experiencing,
reecting, generalising
and applying. After a practical exercise, a skilled facilitator
guides students through
a reective process which helps them improve their ability to
learn and internalise
-
8/9/2019 Drama as an Experiential Technique
4/14
102 P. Deeny et al.
knowledge. Reection used wisely in group or one-to-one
discussions, can enliven
and sharpen the learning experience for students (Greenaway,
1999). Ideas, experi-
ences and feelings are discussed, and linked to abstract
concepts so that theoretical
knowledge can be integrated with practical experience. Thoughts
and insights are
transformed into generalisations, and then applied to real life
situations in the
clinical area. The cycle begins again as students reect upon how
well thesegeneralisations test in reality.
A range of methods can be used for experiential learning to help
students get in
touch with their own feelings and fears about the subject, and
provide opportunities
for discussion about death and reactions to it (Hurtig &
Stewin, 1990). Lessons
learned can facilitate the transition to practical application
in the clinical setting
(Wise, 1974). Role play can improve communication skills, and
promote interaction
with patients and their families (Parkes, 1985), while role
play, drama and small
group exercises can promote skill-building and self-learning
(Lyons, 1988; Kalisch,1974). Wise (1974) and Lewis (1977) described
positive results from simulation and
drama techniques.
Use of Drama as a Method for Teaching Death and Dying
Drama facilitates affective learning about death and dying
because it provides
opportunities for self-exploration and personal reection
(Ferszt, 1984), and enables
practice and development of effective interactional skills
(Parathian & Taylor,
1993). Participation in drama, as an actor or viewer, can foster
empathy: as actorsexpress characters innermost thoughts and
feelings, so viewers gain a deeper
appreciation of how the patient and family may feel. This
fosters creative thinking
in the following discussion, as students learn new ways of
interacting with patients
and relatives (Kalisch, 1974). Drama can put students in touch
with their feelings
about death (Lewis, 1977), promote interpersonal learning
(Ferszt, 1984), increase
self-awareness, and assist in personal growth and development
(Weil & McGill,
1989).
Fundamental to the value of this experience is the process of
reection. Thiscan take place: within the drama; in class discussion
following the drama; in written
work arising out of the drama; in compiling statements of
insights achieved during
the drama to be shared with others; or in further reading and
thinking (ONeill et al.,
1976). Through reection, individuals can arrive at personal
understanding of
themselves or the world around them, and may be able to transfer
learning to similar
situations or propose alternative actions.
Drama in education is a mode of experiential learning which
involves students
in active participation through identication with imagined roles
and situations
(ONeill & Lambert, 1984). It builds upon the knowledge,
skills and experiencesthat students bring to the learning situation
in order to enrich their knowledge of a
subject. The teacher engages in creating and sharing the process
of learning with
students (ONeill et al., 1976). It raises awareness of facts and
issues surrounding
the care of a dying patient. It is particularly benecial for
dealing with emotive issues
such as death in a non-threatening way in which students rst
experience this
-
8/9/2019 Drama as an Experiential Technique
5/14
Drama as an Experiential Technique 103
emotive topic in relation to the lives of ctional characters.
Advocates suggest that
drama facilitates the education of the emotions by allowing
students to develop
empathy with characters, mood, situation and content (OHara,
1984). The result-
ing learning helps students to order and control their emotions
(Allen, 1975),
assisting them towards appropriate and creative forms of
expression with patients
and relatives.Because drama in education is designed to help
students connect with sensitive
and sometimes complicated human issues, and can expose students
to new,
emotional, intensive, confusing or complex experiences, not all
students will be
comfortable with this situation. Therefore, drama workshops need
to be handled
with sensitivity and care, with experienced staff present to
lead discussions and
debrieng sessions. Students may be anxious about feeling safe,
especially in
relation to self-disclosure of emotions and feelings and the
threat of ridicule from
other students (Burnard, 1996). When facilitating reective
discussion, educatorsmust channel reection towards establishing
facts and exploring, examining and
expressing feelings in a safe environment for students
(Greenaway, 1999). While
expression of opinions is to be encouraged, ground rules must
clearly state that
language used must be non-threatening and non-offensive to
others. Staff need to be
alert for volatile areas especially when dealing with ethnic,
racial and ethical issues
(Bontempo, 1995)
Research Problem
Research into the effectiveness of drama in learning has been
undertaken in the
context of general education (Brossell, 1975) and the use of
drama in nursing
education has been described (Hurst, 1993). However, there is
little evidence of
attempts to evaluate the effectiveness of drama as a teaching
method in nursing
education.
This study arose from evaluations by previous student groups who
received
traditional lecture-and seminar-based teaching about death and
dying. As in the
literature previously discussed, they reported difculty in
coping with situations inthe ward and stated we need more. Thus,
this study aimed to enhance student
understanding of this subject area, while also beginning to
address the decit in
evaluation of drama as a teaching method in nursing
education.
Research Methodology
Research Method
The aim of the dramatic intervention was to highlight the types
and range ofemotional responses experienced by patients, families
and professionals associated
with dying. Two acts of approximately 10 minutes each were
presented (see Boxes
1 and 2). Both acts presented scenarios dealing with issues and
feelings related to
open/closed awareness, power, ownership of information,
patientprofessional rela-
tionships, touch and spirituality. Stage props were used to
create atmosphere and
-
8/9/2019 Drama as an Experiential Technique
6/14
104 P. Deeny et al.
Box 1. Act one
This act emphasises how nursing students may feel isolated
within the ward team and bereft
of information, even though most of their day is spent giving
direct patient care. Personal and
professional conicts in this situation are explored. Beginning
with the patient being told not
that he has cancer, but a suspicious growth, act one shows the
nursing student is in the middle
of a communication nightmare. The patient knows he has cancer,
he also knows that the nursesknow he has cancer, the student knows,
but no-one except the student is talking with the
patient. The student cannot disclose what he knows because of
fear of being rebuked by the
Ward Sister. The student wants to support the patient, but is
very clumsy in interaction, being
more evasive than helpful. Both student and patient are left
feeling uncomfortable. In
particular, the patient was confused, bewildered and ultimately
neglected.The nursing student
is lled with self-blame and guilt. The rst act points up the
conict within the team. Failure
to recognise the learning needs of the student and the
conspiracy of silence around cancer
diagnosis are presented. The handmaiden role of the nurse in
relation to not giving
information unless instructed by the doctor or merely rephrasing
the words of the doctor is
also explored.
Box 2. Act Two
The second act progresses to a stage when the nursing student
has become a staff nurse. One
year after the diagnosis of cancer the patient returns to the
ward to die. At the beginning of
Act Two, a powerful soliloquy by the patient reminds the
audience of what it is like to have
a fatal diagnosis. Thepatient reminds us of the denial, despair,
anger, depression and aggressiveoutbursts with the family. The
nurse has established a close emotional bond with the patient
and nurse and patient relate to each others needs within a
meaningful human relationship.
The intimacy that develops is emphasised. The family, in
particular the wife, is unable to deal
with the death of her husband, refuses to visit and keeps the
two children at home. The nurse
acts as intermediary conversing with the wife and the children
by telephone. As the patient
draws near death the nurse lights a candle and prays. The
patient dies. After a short silence
the nurse reects on the loss. The nurse then begins the
bereavement process in a melancholic
way whilst listening some music which was a favourite of the
patient. In an angry manner the
nurse then appeals to the audience (as nurses) to attend more
closely to the needs of dying
people and those who care for them.
help the audience focus on elements with signicant meaning
within the drama. A
short piece of music, a bed, bedside cabinet, a family
photograph, a scented lighted
candle, a crucix and a bible were used to create the atmosphere
around the
death-bed.
After the drama, students were divided into small groups, and
asked to share
feelings and discuss issues raised. Teachers were available
afterwards for one-to-onediscussion if needed. The effectiveness of
this as an educational method to illumi-
nate the topic of death and dying was evaluated by using a
questionnaire to obtain
student views, attitudes and opinions. Students were asked to
complete the ques-
tionnaire 1 week later, having had time to assimilate learning
and share feelings with
peers.
-
8/9/2019 Drama as an Experiential Technique
7/14
Drama as an Experiential Technique 105
Sample
The research sample was drawn from the total population of rst
year nursing
students within Northern Ireland undertaking the Common
Foundation Pro-
gramme of a Project 2000 Diploma or Degree. An important issue
for consideration
was the religious mix of the sample as the scenarios presented
included somereligious symbolism which could have different
implications for those from Catholic
or Protestant backgrounds. Thus, it was decided to ensure that
the ample ade-
quately represented students from both communities.
A cluster sampling technique was used: from a total of six nurse
education
establishments within Northern Ireland, three were selected.
Group A (n5 35) was
based within a predominantly Catholic and the other (Group B, n5
75) within a
mainly Protestant catchment area. These groups were used for the
main study. The
third group (n5 25), which was used for the pilot study, had
substantial numbers of
students from both communities. The ages of participants ranged
from 19 to 30(mean 21) and most of the sample were female
(91%).
The Questionnaire
The questionnaire (Table I) was developed from issues identied
in the literature.
It consisted of 21 questions, comprising two items related to
biographical details, 18
items which explored students opinions and feelings about the
scripted drama, and
one open-ended question which allowed respondents to comment on
the drama.Students were asked to rate their response to each of the
18 questions along a Visual
Analogue Scale, indicating their response by placing a mark
through the point of the
line which best reected their perception (see Table I).
The Visual Analogue Scale provides interval-level data with ne
discrimination
of values (Burns & Grove, 1987), and is particularly useful
for scaling attitudes and
feelings (stimuli) as it discourages the respondent from always
choosing the extremes
of a scale (Lodge, 1981). The scale is a line exactly 100 mm in
length, with the
extremes of the response placed at each end of the line.
Respondents are asked toplace a mark through the line to indicate
the intensity of the stimulus. A ruler is then
used to measure the distance between the left end of the line
and the mark placed
by the respondent, for example, if the mark is at 67 mm then
this response is given
a score of 6.7.
The scripted drama and the questionnaire were piloted with a
group of 25
nursing students not used in the main study. This enabled the
actors to practice the
drama and identied errors in the questionnaire such as
presentation, typographical
errors, overlapping response sets and ambiguity (Litwin, 1995).
A few amendments
were made to clarify ambiguities.Content and face validity were
established through scrutiny by a panel of nurse
educators and practitioners (Litwin, 1995). The questionnaire
provided consistent
and accurate data, and tests of internal consistency were
undertaken with the main
data set to determine the questionnaires reliability. Analysis
demonstrated a high
internal consistency (Cronbachs a coefcient5 0.835).
-
8/9/2019 Drama as an Experiential Technique
8/14
106 P. Deeny et al.
TABLE I. Questionnaire for evaluation of Drama for teaching
about death and dying
Foreach question respondents were asked to insert a mark on that
position on the line which reected
their response (as indicated).
Not at all A great deal u1. I enjoyed the drama as a method for
teaching me about death and dying
2. The drama encouraged me to read the handout about death and
dying
3. The drama helped me understand my own feelings about death
and dying
4. The drama helped me understand how a patient might feel about
death and dying
5. The drama helped me understand how a member of the family may
feel
6. The drama helped me to understand how nurses might feel about
caring for a dying patient
7. During the drama I felt emotional
8. I think the drama will help me prepare for the real
situation
9. The drama dealt with death and dying in a sensitive way
10. The use of props and aids helped me to attend to the
drama
11. I found the drama helped learning
12. The drama helped me identify the need for emotional support
for nurses
13. I thought about the drama afterwards
14. The drama will help me to use touch to express feelings
towards dying patients
15. The drama will help me talk with patients who are dying
16. The drama made me think about my own attitudes to death and
dying
17. The drama raised more questions than provided answers
18. The drama showed me the need for peer support from fellow
nursing students
19. Please comment on the drama
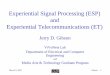
Results
Overall, results from this study demonstrate very positive
feedback from students
regarding drama as a method of teaching students about death and
dying (see
Figure 1) with scores ranging from 5 (i.e. half-way along the
continuum from not at
all to a great deal) to 9 (90% of the way along that continuum).
Results from Group
A (n5 35) (predominantly Catholic) and Group B (n5 75) (mainly
Protestant)
were compared using t-tests and no signicant differences were
noted in any of the
items. There were no age or gender differences in responses.
Eighty-four per cent of the students in Group A and 80% of those
in group B
perceived that the drama helped them to learn about death and
dying, and gain
insight into the patients perspective. Qualitative comments
supported this:
The drama presented a life-like situation and it made me think
about how
I would cope with someone who is dying and how I would
communicate
with them.
It made me understand more as it was the actual patient who was
talking
about his feelings and the family.
made me realise how a dying patient feels as they approach
death. Since
they are in a strange hospital environment it makes it all the
more
frightening and lonely. It is the nurse who must provide
company.
-
8/9/2019 Drama as an Experiential Technique
9/14
Drama as an Experiential Technique 107
FIG. 1. Results from questionnaire on drama about death and
dying.
I thought the drama was a very easy-to-follow and simple way to
under-
stand death and bereavement.
Students also indicated that the drama helped to raise their
awareness of the
emotional aspects of caring for dying patients, especially how
patients, families and
nurses feel. Most of the qualitative comments referred to how
they could identify
with patients and families much more after the drama.
I found it very useful because it got me into contact with my
emotions/
feelings. It brought back memories of loved ones on their
deathbed.
It provoked a lot of emotion and was very effective in raising
issues
concerning death and terminal illness.
Very good, very emotional where a video or other approach would
not getacross the same feelings.
Findings also indicate a heightened awareness of the need for
support for nurses
(Group A 89%, Group B 90%). Qualitative comments such as:
I thought the drama was very powerful. It brought across how the
nurse
feels in this situation. It prepared me for what is to come and
gave me an
idea on how I might cope.
I found the drama very interesting, and it proved how difcult it
can be forstudent nurses to discuss death with senior nurses and
other members of
the team.
The drama clearly demonstrated the difference between the role
of the
student and the staff nurse. It hit me how the student wasnt
able to answer
the questions. This is how I feel sometimes.
-
8/9/2019 Drama as an Experiential Technique
10/14
108 P. Deeny et al.
However some of the qualitative comments highlighted
dissatisfaction with the
drama:
I felt that it was not realistic, it was a bit fake I
thought.
It was good but afterwards I felt very unsure, I would still be
insecure in
dealing with this situation.
I thought that the drama was good but I found it difcult to hear
the
patient at times. I would have liked more emphasis on the
family, perhaps
some actors doing the family would have helped.
I felt that the drama was too short in duration. The death was
too quick.
A few students had difculty with the symbolic meaning behind
various props used
in the drama. For example:
I thought that this was very Catholic, the crucix and all. They
should have
been less provocative.
We do not have candles at the death. I think that this was too
Roman
Catholic.
These last two comments came from the predominantly Protestant
students (group
B). Interestingly, issues related to the religious symbolism did
not arise as a problem
within the pilot study with the mixed religious group.
Discussion
Learning about Dying
The ndings in this study support the use of drama as an
experiential method in
teaching nursing students about death and dying. As intended,
the drama caused an
emotional response in students and enabled them to reect on how
they might feel
and cope in the real situation, similar to the ndings of Hurtig
& Stewin (1990).Drama taking place in a group setting results
in participants sharing their experi-
ences with others, and discovering that they all feel and
respond in similar ways.
This engenders feelings of support and afrmation from colleagues
identied by
Mackay (1989) as one of the factors which inuence the ability to
cope with the
death of a patient.
The evidence from the questionnaires suggest that the drama and
discussion
resulted in affective learning as the students perceived it as
being benecial in
understanding how others feel. However, whether it will enable
students to respond
in a more empathetic manner to dying patients in their clinical
placements can onlybe evaluated by undertaking a follow-up study
with the same students. Some
informal feedback from these students at a later date has
indicated that it did help
them in practice through enhancing their understanding of how
the patient, family
and nurses might feel.
Educational preparation to care for dying patients and their
families needs to be
-
8/9/2019 Drama as an Experiential Technique
11/14
Drama as an Experiential Technique 109
combined with supportive clinical experiences. Johnson (1994)
highlighted that
students considered that only some aspects of death and dying
can be taught in
college. Other aspects, such as how they will feel when faced
with the situation of
caring for dying patients and development of coping strategies,
can only be devel-
oped fully within a supportive clinical environment and this was
reinforced by
student feedback. However, the approach discussed in this paper
may help to bridgethe gap between academic and clinical settings,
particularly when followed by
experience with effective clinical role models, and the
opportunity to reect on
practice with nursing colleagues and/or academic tutors.
The affective domain within Blooms Taxonomy (1956) is a difcult
area in
which to evaluate the effectiveness of learning opportunities
provided. Within this
example, it was clear from the students responses to the
questionnaire that learning
at the rst two levels (receiving or attending, and responding)
was achieved. The fact
that over 80% of students responded positively to the statement
that the drama mademe think about my own attitudes to death and
dying indicates that it is likely that many
also achieved the third level (valuing). The discussion
following the drama was
intended to facilitate them in reaching towards the fourth level
in which they would
be able to conceptualise their knowledge and experiences.
However, at this stage in
their programme, this penultimate stage and the nal level, in
which they will
internalise their new understanding, are unlikely to have been
achieved. It is
predicted that relevant experience in practice with appropriate
support, as described
by Mackay (1989), will build on this initial introduction to
enable achievement at all
levels in this hierarchy.
Limitations and Difculties of Educational Method
There are some issues related to the method and the rigour of
the research that merit
discussion. This study used a relatively weak experimental
design with an interven-
tion or independent variable (the drama and discussion) followed
by measurement
of the dependent variable (students attitudes and opinions) 1
week later. It wouldhave been improved by some measurement of these
before the intervention. Simi-
larly, the study would have been enhanced by including a
comparison group who
received a more conventional educational input on death and
dying. This would
have eliminated the possible inuence of the Hawthorne effect in
increasing the
positive results obtained. Nevertheless, the students own
evaluation of their learning
through this activity cannot be discounted.
Students in this study were asked to complete the questionnaire
1 week after the
drama. The rationale for this approach was that they required
time to assimilate the
knowledge and emotional experience and discuss the experience
with their peers. Italso means, however, that there is a
possibility of diffusion of ideas and positive
perceptions of the drama that may bias the evaluation, and (with
the Hawthorne
effect) explain the overly positive response. The two groups in
the study had no
contact with each other and the similarity in responses
reinforces the reliability of the
ndings. To elucidate students views, attitudes and opinions a
self-report question-
-
8/9/2019 Drama as an Experiential Technique
12/14
110 P. Deeny et al.
naire was the only feasible method, but does not assess the
inuence on their
professional practice of the learning they have achieved.
Respondents comments that props used during the drama, such as a
crucix
and lighted candle, were too Roman Catholic were made within
Northern Ireland,
a divided society with many having strong afliations to either
the Protestant or the
Catholic community. These comments, not surprisingly, were
mainly from thepredominantly Protestant group. Nurse educators
responses to these type of state-
ments need to be carefully considered. On one hand, it is easy
to be critical of some
individuals unwillingness to appreciate cultures other than
their own. Conversely,
it also highlights the need for educators to avoid ethnocentrism
and offence
(Bontempo, 1995).
However, symbols and rituals of death and mourning are an
important part of
the process of grieving for families (OGorman, 1998).
Presentation of such symbols
to students in the context of teaching about death and dying is
crucial if they are toreect on how they might deal with these in a
respectful manner within the patient
care situation. The issue that this study raised is how do nurse
educators, knowing
that such prejudicial perceptions may exist in groups of nursing
students, incorpor-
ate these into their teaching without causing offence. In this
situation the issue was
not foreseen, but in the future when such symbols are introduced
in any form of
teaching they should reect the diversity within the particular
society and should not
cause offence to any. When using drama, educators need to
carefully consider
students ethnic and cultural backgrounds, and endeavour to
integrate a diversity of
traditions and there should be open discussion on the topic.
Indeed, the introduc-tion of such symbols could act as a catalyst
for reective discussion on prejudicial
perceptions and attitudes.
Potential Value of Drama in Professional Education
The use of drama as a teaching method was well received, and the
combination of
drama and group discussion was considered very effective by the
students. Drama
was found a highly satisfactory method for enabling nursing
students to reect ontheir understanding of the emotional aspects of
death and dying in hospital. This
method has considerably wider application than nursing
education. Many health
professionals have to confront similar situations and this
method of introducing the
topic and enabling students to begin to consider possible coping
strategies could be
used with all such groups. If undertaken within
multi-professional groups, it would
have the additional advantage of enhancing inter-professional
understanding and
thus enhancing patient care.
In addition to the topic of death and dying, there are many
other difcult
situations which health and social care professionals encounter.
Drama is a viablemethod of enabling students to begin to think
about and come to terms with such
issues, and could be used much more widely to provide
opportunities for students
to practice the affective skills needed.
While this study was carried out in Northern Ireland,
considerations similar to
those discussed above would apply in other situations where
different cultures meet,
-
8/9/2019 Drama as an Experiential Technique
13/14
Drama as an Experiential Technique 111
including many other parts of the United Kingdom. Use of this
teaching method
would enhance students abilities in working empathetically with
patients from
cultures other than their own.
Acknowledgements
The authors gratefully acknowledge the National Board For
Nursing, Midwifery and
Health Visiting for Northern Ireland for second-line research
funding related to this
project.
REFERENCES
ALLEN, J. (1975) Notes on a denition of drama, in: J. HODGSON
& M. BANHAM (Eds) Drama in
Education 3 (London, Pitman).
BIRCH, J. (1983) Anxiety and conict in nurse education, in: B.
DAVIS (Ed.) Research in Nurse
Education (London, Croom Helm).
BLOOM, B.S. (1956) Taxonomy of Educational Objectives (New York,
McKay).
BONTEMPO, B. (1995) Exploring Prejudice in Young Adult
Literature through Drama and Role Play.
http://scholar.lib.vt.edu/ejournals/ALAN/spring95/Bontempo.html
BROSSELL, G. (1975) Researching drama: a humanistic perspective,
in: N. STEPHENSON & D.
VINCENT (Eds) Teaching and Understanding Drama (London, National
Foundation for
Educational Research).
BURNARD, P. (1985) Learning Human Skills (Oxford,
Heinemann).
BURNARD, P. (1996) Acquiring Interpersonal Skills: a handbook of
experiential learning for health
professionals, 2nd edn (London, Chapman and Hall).
BURNS, N. & GROVE, S. (1987) The Practice of Nursing
Research: conduct, critique and utilization
(Philadelphia, PA, W.B. Saunders).
DOYLE, D. (1982) Nursing education in terminal care, Nurse
Education Today, 2, pp. 46.
FERSZT, G. (1984) Drama as an educational tool, Oncology Nursing
Forum, 11, pp. 6466.
FIELD, D . & K ITSON, C. (1986) Formal teaching about death
and dying in United Kingdom
nursing schools, Nurse Education Today, 6, pp. 270276.
FROMMELT, K. (1991) The effect of death education on nurses
attitudes towards caring for
terminally ill persons and their families, American Journal of
Hospice and Palliative Care, 8(5),
pp. 3743.
GREENAWAY, R. (1999) Reviewing Skills Training. Reviewing and
Debriefing: what, why and how?http://www.user.globalnet.co.uk/ ,
rogg/review.htm
HAISFIELD-WOLFFE, M. (1996) Cancer nursing perspectives.
End-of-life care: evolution of the
nurses role, Oncology Nursing Forum, 23, pp. 931935.
HOCKLEY, J. (1989) Caring for the dying in acute hospitals,
Nursing Times, 85(39), pp. 4750.
HURST, B. (1993) Drama class, Nursing Times, 89(1), pp.
3031.
HURTIG, W . & STEWIN, L. (1990) The effect of death
education and experience on nursing
students attitude towards death, Journal of Advanced Nursing,
15, pp. 2934.
JOHNSON, G. (1994) The phenomenon of death: a study of Diploma
in Higher Education nursing
students reality, Journal of Advanced Nursing, 19, pp.
11511161.
KALISCH, B. (1974) Summer theatre: another way to learn, Nursing
Outlook, 22, pp. 3134.KIEGER, A. (1993) Accord and discord in
students images of nursing, Journal of Nursing
Education, 32, pp. 309317.
KIEGER, A. (1994) Student nurses involvement with death: the
image and the experience, Journal
of Advanced Nursing, 20, pp. 679686.
LEES, S. & ELLIS, N. (1990) The design of a
stress-management programme for nursing
personnel, Journal of Advanced Nursing, 15, pp. 946961.
-
8/9/2019 Drama as an Experiential Technique
14/14
112 P. Deeny et al.
LEWIS, F. (1977) A time to live and a time to die: an
instructional drama, Nursing Outlook, 25,
pp. 762765.
LINDROP, E. (1991) Individual stress among nurses in training:
why some leave while others stay,
Nurse Education Today, 11, pp. 172179.
LITWIN, M. (1995) The Survey Kit, Volume 7: how to measure
survey reliability and validity
(Thousand Oaks, CA, Sage Publications).
LODGE, M. (1981) Magnitude Scaling: quantitative measures of
opinions (Beverly Hills, CA, SagePublications).
LYONS, G. (1988) Bereavement and death education: a survey of
nurses views, Nurse Education
Today, 8, pp. 168172.
MACKAY, L. (1989) Nursing a Problem (Buckingham, Open University
Press).
MCKAY, S. (1978) A review of student stress in nursing education
programmes, Nursing Forum,
17, pp. 376379.
MANDEL, H. (1981) Nurses feelings about working with death and
dying, American Journal of
Nursing, 81, pp. 11941197.
MELIA, K. (1983) Students views of nursing. Nursing in the dark
students are often left short
of information, Nursing Times, 79(21), pp 6263.MELLISH, J.M.
& BRINK, H. (1990) Teaching the Practice of Nursing: a text in
nursing didactics, 3rd
edn (Durban, Butterworths)
NATIONAL SOCIETY FOR EXPERIENTIAL EDUCATION (1997) Foundations
of Experiential Education.
http://www.nsee.org/round.htm
OGORMAN, S. (1998) Death and dying in contemporary society: an
evaluation of current
attitudes and the rituals associated with death and dying and
their relevance to recent
understandings of health and healing, Journal of Advanced
Nursing, 27, pp. 11271135.
OHARA, M. (1984) Drama in education: a curriculum dilemma,
Theory into Practice, XX111(4),
pp. 315320.
ONEILL, C. & LAMBERT, A. (1984) Drama Structures: a
practical handbook for teachers (London,
Heinemann).ONEILL, C., LAMBERT, A., LINNELL, R. & WARR-WOOD,
J. (1976) Drama Guidelines (London,
Heinemann).
PAGANA, K. (1988) Stresses and threats reported by baccalaureate
students in relation to initial
clinical experience, Journal of Nursing Education, 27, pp.
418424.
PARATHIAN, A. & TAYLOR, F. (1993) Can we insulate students
from exposure to bad practice? A
study of role play in communicating bad news to patients,
Journal of Advanced Nursing, 18,
pp. 801807.
PARKES, K. (1985) Stressful episodes reported by rst-year
student nurses: a descriptive account,
Social Science and Medicine, 20, pp. 945953.
POPOFF, D. (1975) What are your feelings about death and dying?
Nursing 75, 5, pp. 1624.QUINN, F. (1997) The Principle and Practice
of Nurse Education, 3rd edn (London, Chapman and
Hall).
RHEAD, M. (1995) Stress among student nurses: is it practical or
academic? Journal of Clinical
Nursing, 4, pp. 369376.
ROSS, C. (1978) Nurses personal death concerns and responses to
dying patient statements,
Nursing Research, 27, pp. 6468.
SAWATZKY, J. (1998) Understanding nursing students stress: a
proposed framework, Nurse
Education Today, 18, pp. 108115.
SERVATY, H., KREJCI, M. & HAYSLIP, B. (1996) Relationships
among death anxiety, communi-
cation apprehension with the dying, and empathy in those seeking
occupations as nurses
and physicians, Death Studies, 20, pp. 149161.
WEIL, S. & MCGILL, I. (Eds) (1989) Making Sense of
Experiential Learning (Buckingham, Open
University Press).
WHITFIELD, S. (1983) A descriptive study of student nurses ward
experiences with dying patients
and their attitudes towards them, in: C. COX (Ed.) Sociology: an
introduction for nurses,
midwives and health visitors (London, Butterworth).
WISE, D. (1974) Learning about dying, Nursing Outlook, 22, pp.
4244.