Embed Size (px)
Citation preview
DRINK AND DRUGS NEWS ISSN 1755-6236 SEPTEMBER 2019
INSIDE: WHY ARE WE FAILING NEWLY RELEASED PRISONERS?
WE NEED TO BECOME HARM REDUCTION ACTIVISTS AGAIN
TIMETO MAKE
SOMENOISE

pioneering simplicity
GP
011
2_
A6
7_
03
The MySafe Plus o.ers a safe and secure containment solution for a single 1ml and 2ml syringe, with either a fixed needle or separate needle attached.
A used syringe can be safely and discreetly transport to a needle and syringe programme outlet without the risk of a needle stick injury.
Contaminated sharps are secured within a two-stage locking mechanism preventing access to used sharps once contained. Reducing the risk of needlestick injuries should injection equipment be accidentally discarded prior to disposal.For more information:
Call +44 (0)1495 235800 Email: [email protected] Website: www.frontier-group.co.uk
Frontier Medical Group, Block G Newbridge Road Industrial Estate, Blackwood, Caerphilly NP12 2YN United Kingdom.
Frontier Medical Group are market leader in the Harm Reduction sector with an excellent reputation for innovation, service and professionalism.
Due to continued growth we are looking to recruit in the South of the UK either a Sales Support Specialist or Territory Account Manager to support and grow our business across the region.
We are looking for a professional, dynamic and results orientated individual to implement and execute commercial strategies, to grow the business through education, solution selling and collaboration. Experience in a harm reduction / needle exchange setting would be an advantage.
The position comes with a competitive package, bonus, 25 days annual leave, pension, healthcare and company car. Ideal locations include Birmingham, Northamptonshire, Milton Keynes, Cambridge and Oxford.
We welcome your application.
For more information please contact:Tom Hull on 07745 861 578 or [email protected] Website: www.frontier-group.co.uk/nx-application
Introducing MySafe PlusSafe, discreet and secure containment for 1ml and 2ml syringes.
To learn more please visit our website or call us today.
new
New
Produc
t
Are you looking for a new challenge in a fast-paced and growing company?
Job Vaca
ncy

DDN is an independent publication, entirely funded by advertising.Proud to work in partnership with:
4 NEWSHighest drug death toll – again; More research needed on medicinal cannabis.
6 AGENTS OF CHANGEWe urgently need to become activists once more, says Nick Wilson.
8 NEWS FOCUS: THANKS FOR SHARINGData sharing is lagging dangerously behind in the battle to eliminate hep C.
10 A PRESCRIPTION FOR PAINPaul was prescribed OxyContin after an industrial injury. As he tells us, it was
the start of his problems.
11 POST-ITS FROM PRACTICEDr Steve Brinksman discusses his approach to prescribing opioid painkillers.
12 CRISIS POINTThoughts on how to reverse the appalling trend of drug-related deaths.
13 LETTERS & COMMENTIn her Clinical Eye column Ishbel Straker asks what we are doing to support
nurses’ health; more on the legalisation debate in letters.
13 MEDIA SAVVYThe news, and the skews, in the national media.
14 CASE DISMISSEDWhy are improvements to custody-community transitions being ignored?
16 UPPING THEIR GAMEThe sixth annual Recovery Games were the best yet, says Stuart Green.
September 2019 | drinkanddrugsnews | 3www.drinkanddrugsnews.com
ContEnts
September is a glorious opportunity to celebrate recoverymonth and we’re delighted to hear about the activitiestaking place all over the country. The Recovery Games in
Doncaster (page 16) sums up the spirit of events and we’re lookingforward to following what’s happening around the country.
But as we do so, let’s remember our common purpose. Harmreduction is not the preserve of one community – it’s all of ourbusiness and should be central to everything we do, whatever thedrug and whatever the treatment preference. Nick Wilson’s piece(cover story, page 6) is a reminder that activism is essential, andthat includes the kind of community engagement that makesrecovery messages so visible and effective. The ‘culture ofacceptance and engagement’ should be the unifying force thatpropels harm reduction to the heart of mainstream healthcare andpolicy. We have plenty of evidence for this, right down to thedepressing year-on-year increase in drug-related deaths.
The evidence is particularly clear when looking at custody-community transitions (page 14) – an area where small changes inpractice could make a vast difference to prisoners’ chances ofsuccess. As Alex Stevens points out, there’s much that can be donein the short term for a population ‘so highly vulnerable to healthproblems’. Meanwhile, in this month’s News Focus (page 8) we lookat progress on hepatitis C and find some important messages ondata sharing if we are to meet NHS England’s ambitiouselimination target of 2025.
Claire Brown, editorKeep in touch at www.drinkanddrugsnews.com and @DDNmagazine
Editor: Claire Browne: [email protected]
Advertising manager: Ian Ralphe: [email protected]
Reporter: David Gillivere: [email protected]
Designer: Jez Tuckere: [email protected]
Keep in touch with us via Facebook and Twitter!/DDNMagazine @DDNMagazine
ON THE COVERHarm reduction must rise again, p6
DDN is published by CJ Wellings Ltd,Romney House, School Road, Ashford, Kent TN27 0LT
t: 0845 299 3429
Subscriptions: e: [email protected]
website:www.drinkanddrugsnews.com
Website support bywiredupwales.com
Printed on environmentallyfriendly paper by the Manson Group Ltd
Cover by JellyPics
CJ Wellings Ltd does not acceptrespon si bility for the accuracyof state ments made by contri bu t ors or advertisers.
The contents of this magazineare the copyright of CJ WellingsLtd, but do not necess arilyrepresent its views, or those ofits partner organisations.
Editor’s lEttEr
‘Harmreduction is not thepreserve of onecommunity’ pi
c: n
igel
brun
sdon
.com

REGISTRATIONS OF DEATHS relating to poisoning(overdose) in England and Wales have once againbroken previous records, according to figures from theOffice for National Statistics (ONS). There were 4,359drug poisoning deaths in 2018, up from 3,756 theprevious year (DDN, September 2018, page 4). Thisrepresents a ‘statistically significant’ increase of 16 percent, the highest since records began in 1993.
The figures follow the announcement in July ofanother set of record drug-fatalities north of the border,at 1,187 – the fifth consecutive Scottish increase and upalmost 30 per cent from 2017’s figure of 934 (DDN,July/August 2018, page 4). The Scottish Government hassince announced an additional £20m funding over twoyears for the country’s drug services.
Two-thirds of the fatalities in England and Waleswere related to drug misuse, with male deathsincreasing significantly from 89.6 per million males in2017 to 105.4 in 2018, while the female rate increasedfor the ninth consecutive year to 47.5 per million. Whilemore than half of all drug poisonings involved anopiate, deaths involving cocaine have now risen forseven years in a row and almost doubled between 2015and 2018 – to 637. Fentanyl deaths, however, remainedstable at 74.
There were also 125 deaths involving NPS, onceagain a ‘statistically significant’ increase from the 61recorded in 2017 and a return to 2016’s levels, whichsaw 123. Synthetic cannabinoids contributed to 60 ofthe NPS-related deaths, up from 24 in 2017. As inprevious years, the North East reported significantlyhigher drug-related death rates than all other Englishregions.
Transform called the deaths ‘an avoidable tragedy’,while Release said government inaction was asignificant contributory factor. ‘For the last seven yearswe have seen drug-related deaths increase year on yearand every year we have called on the government totake action, to scale up funding for drug treatment, tosupport overdose prevention sites, to fund drugchecking facilities, and to expand heroin assisted
treatment,’ said executive director Niamh Eastwood.‘Each year they have ignored us.’
‘Drug-related deaths are preventable deaths,’ addedTurning Point’s director for public health and substancemisuse, Jay Stewart. ‘Investment in high quality, free toaccess, evidence-based treatment services is critical, notonly to protect communities from drug-related crimeand anti-social behaviour but to save lives. Nationally,funding has been reduced by 18 per cent over the pastfive years and this reduction needs to be reversed.’
Deaths related to drug poisoning in England andWales: 2018 registrations at www.ons.gov.uk
News
4 | drinkanddrugsnews | September 2019 www.drinkanddrugsnews.com
DELAYED GRATIFICATIONALCOHOL COMPANIES WILL FINALLY INCLUDE THE CMO’SREVISED DRINKING GUIDELINES on bottles and cans threeand a half years after their introduction. Portman Groupmembers – which include Diageo, Barcardi and Carlsberg –will now voluntarily display the 14 unit guidelines on theirpackaging. Institute of Alcohol Studies chief executiveKatherine Severi said that it was a victory for the publicthat the guidelines would appear ‘after three years ofdelaying tactics by alcohol companies, and at the lastminute before a government deadline to comply.But while this marks a half step forward, it showsthat the current system of alcohol industry self-regulation is failing consumers.’
HIGHEST DRUG DEATH TOLL FORENGLAND AND WALES – AGAIN
RIGHTS VIOLATIONSTHE UN HUMAN RIGHTS COUNCIL shouldopen an investigation into Rodrigo Duterte’s‘war on drugs’, says an AmnestyInternational report. The Philippinepresident’s violent anti-drugs campaignshould be investigated for gross humanrights violations and ‘possible crimes againsthumanity’, according to They just kill. Whilethe country’s government had acknowledgedat least 6,600 killings by police, ‘evidencepoints to many thousands more killed byunknown armed persons with likely links tothe police’, Amnesty states. ‘It is time for theUN, starting with its Human Rights Council,to act decisively to hold President Duterteand his government accountable,’ saidAmnesty regional director Nicholas Bequelin. Report at www.amnesty.org.uk
CYNICALEXPLOITATIONCHILDREN AS YOUNG AS SEVEN are beingexploited by county lines gangs, says aChildren’s Society report. While those in the14-17 age range are the most likely to beexploited, children of primary school age arebeing ‘increasingly targeted’, the charitywarns. The number of 10-17-year-oldsarrested outside London for intent to supplydrugs increased by 49 per cent between2015-16 and 2017-18 to more than 500,while respondents described seven andeight-year-olds receiving support from theauthorities. ‘Children are being cynicallyexploited with the promise of money, drugs,status and affection and controlled usingthreats, violence and sexual abuse, leavingthem traumatised and living in fear,’ saidChildren’s Society chief executive NickRoseveare. Counting lives: responding tochildren who are criminally exploited atwww.childrenssociety.org.uk
EFFECTIVEIMPLEMENTATIONMUP IS BEING IMPLEMENTED EFFECTIVELY,according to NHS Health Scotland. Levels ofcompliance among licensed premises arehigh, says Evaluating the impact of minimumunit pricing in Scotland on harmful drinkers.The report, which is based on interviews withtrading standards officers, police and others,found that even where issues of non-compliance were identified these were‘minor and swiftly resolved’. Pubs, clubs andrestaurants – which charge higher pricesthan off-sales premises – had been largelyunaffected, and there was also no reportedincrease in incidences of unlicensed or illegalalcohol activity since MUP’s introduction inMay last year. Report athttp://www.healthscotland.scot/
‘every year we have called onthe government to takeaction, to scale up funding fordrug treatment... each yearthey have ignored us.’
niAmh eAStwood
A victory for the publicKAtherine Severi

CHALLENGING ISSUESVULNERABLE ADULTS’ ALCOHOL USE IS BEING‘MISSED OR POORLY MANAGED’, according toa report from Alcohol Change UK, with themismanagement of severe alcohol problemsamong people with complex needsincreasing their risk of harm and even death.All professionals working with alcohol-dependent people should be fully trained torecognise the ‘complicated role that alcoholplays in adult safeguarding’, says thedocument, and stresses that a person’srefusal of care needs to be ‘constantlychallenged’. The refusal of alcohol treatmentshould not lead to someone being deemedbeyond help, it says, and treatment servicesmay need to adapt their models, for example
September 2019 | drinkanddrugsnews | 5
read the full stories, and more, onlinewww.drinkanddrugsnews.com
through the use of home visits.Learning from tragedies: an analysis ofalcohol-related safeguarding adult reviews atalcoholchange.org.uk
SHARE AWAREMANY PEOPLEDELIVERINGHEPATITIS C TESTINGor treatment do notunderstand whichdata can be shared orwith whom,according to a newreport from theLondon Joint WorkingGroup on SubstanceUse and Hepatitis C(LJWG). Clearguidance and training is needed to ensureprogress towards eliminating hep C, saysJoining the dots: linking pathways to hepatitisC diagnosis and treatment. Report atljwg.org.uk. See news focus, page 8
DRUG DELUGETHE PRISON SERVICE RESPONSE to the ‘delugeof drugs flowing into many prisons’ in recentyears has been slow and ‘neither robust norsophisticated’, according to the chief inspectorof prisons’ annual report. Last year had beenanother ‘deeply troubling’ year for parts ofthe prison estate, with many establishmentsstill ‘plagued by drugs, violence, appallingliving conditions and a lack of access tomeaningful rehabilitative activity’, the reportstates. The government has since promised a‘crime crackdown’ in prisons, with ‘airport-style’ security to tackle smuggling of drugsand weapons. ‘We cannot allow our prisons tobecome factories for making bad peopleworse,’ said Prime Minister Boris Johnson. HM chief inspector of prisons’ annual report for2018-19 at www.justiceinspectorates.gov.uk
NEXT LEVELTHE FIRST POST-INTRODUCTORY LEVELINTERPERSONAL GROUP THERAPY COURSE INTHE UK has been launched by Action onAddiction. Based on a collaborative adultlearning model, the practice-based course isdesigned to equip people with a fullunderstanding of how interpersonal grouptherapy can be effective in facilitating characterchange. Teaching takes place one Saturday permonth in Warminster from 16 Novemberonwards. Meanwhile, applications are open forthe foundation degree in addictions counsellingat University of Bath, offering a mixture ofacademic study and work-based learning.For more information [email protected]
www.drinkanddrugsnews.com
MORE RESEARCH IS NEEDED on cannabis-based medicinalproducts before they can be widely prescribed, says theNational Institute for Health and Care Excellence (NICE).Medicinal cannabis products were re-classified last yearto allow specialist doctors to prescribe them where theneeds of patients could not be met by licensed medicines.The decision followed the high-profile cases of twochildren with epilepsy whose parents were unable tolegally access cannabis oil-based medicines to preventtheir seizures (DDN, July /August 2018, page 5).
NICE has issueddraft guidance forpublic consultationon the use ofcannabis-basedproducts forpeople with severetreatment-resistant epilepsy,chronic pain,spasticity andintractable nauseaand vomiting as aresult ofchemotherapy. Theguidance makes arange ofrecommendationsfor furtherresearch based onthe ‘overall lack of clinical and cost-effectivenessevidence’ for the products. The guidance states that, otherthan pure cannabidiol (CBD) used ‘on its own in thecontext of a clinical trial’, no cannabis-based productsshould be used for treating chronic pain, while Sativexshould not be used for treating spasticity in people withmultiple sclerosis as it was not found to be cost-effectivein relation to its benefits.
NHS England has also published a review of the
barriers to prescribing the products, which states that thelack of evidence regarding their long-term safety andeffectiveness has ‘weighed heavily on prescribingdecisions’ and recommends that two major clinical trialsbe set up. It also states that ‘consistency is key’ whenmaking decisions about the use of medicinal cannabis forchildren with severe epilepsy, as without sufficient clinicaltrial evidence clinicians were ‘very reluctant’ to prescribe.
‘We heard loud and clear the concerns and frustrationthe children’s families are feeling, but theserecommendations aim to help us develop the evidencebase to understand how safe these products are, andensure education and expert advice is available tosupport clinicians across the UK,’ said chiefpharmaceutical officer at NHS England, Dr Keith Ridge.
‘We recognise that some people will be disappointedthat we have not been able to recommend the wider useof cannabis-based medicinal products,’ added director ofNICE’s centre for guidelines, Paul Chrisp. ‘However, wewere concerned when we began developing this guidancethat a robust evidence base for these mostly unlicensedproducts was probably lacking. Having now considered allthe available evidence it’s therefore not surprising thatthe committee has not been able to make many positiverecommendations about their use.’
Director of external affairs for the MS Society,Genevieve Edwards, said her organisation was ‘bitterlydisappointed’ by the guidelines. ‘NICE’s refusal torecommend cannabis for pain and muscles spasms, or tofund Sativex on the NHS, means thousands of peoplewith MS will continue to be denied an effectivetreatment,’ she said. ‘MS is relentless and painful, yet nota single person with MS has benefited from medicinalcannabis being legalised nine months ago.’
Draft guidance atwww.nice.org.uk/guidance/indevelopment/gid-ng10124/documents. NHS review atwww.england.nhs.uk/medicines/support-for-prescribers/cannabis-based-products-for-medicinal-use/
STUBBED OUTJUST 16 PER CENT OFSECONDARY-SCHOOL PUPILSHAVE SMOKED TOBACCOcompared to almost 50 per centin 1996, according to the latestfigures from NHS Digital. Almosta quarter have tried drugs,however, while 17 per cent drinkalcohol at least once a month –rising to almost 40 per cent of15-year-olds. Half of the youngpeople who had recently drunk,taken drugs or smoked cigarettesexperienced ‘low levels’ of happiness, the report adds. Smoking,drinking and drug use among young people 2018 at digital.nhs.uk
MORE RESEARCH NEEDED ONMEDICINAL CANNABIS, SAYS NICE
‘we recognise thatsome people willbe disappointedthat we have notbeen able torecommend thewider use ofcannabis-basedmedicinal products’

Agents of
The UK’s well-deserved reputation for developing gold standard harm reductionservices was the envy of many countries around the world. From modestbeginnings in the 1980s and an extraordinarily passionate and committed harmreduction community, was crafted the level of activism which ultimately broughtharm reduction into the UK’s healthcare mainstream.
Credit must also be given to the UK government who at this time, and facedwith the emerging ‘AIDS epidemic’, committed protected funding to support thegrowth and roll out of harm reduction services, most notably the provision ofneedles and syringes for people who inject drugs. Rates of HIV in the UK today(about 1 per cent of people who inject drugs) are among the lowest in the worldand testament to this partnership of activism and political pragmatism.
From the late ’80s the UK began to refine effective skills around engagementand interventions to reduce harm among people who inject drugs. The fourcornerstones of harm reduction – needle and syringe provision, substitution therapyand methadone, treatment for hepatitis C and HIV and the prevention and reversalof overdose – established our role as agents of behaviour change within thisinclusive, non-judgemental, low-threshold environment.
We have been effective at reducing the risks associated with injecting drug useand developing initiatives which deliver some of the most cost-effective healthinterventions of any kind. It is estimated that for every £1 spent on harm reduction,£4 is delivered in return in health and social gain. This was achieved by tenacity,commitment, compassion and years of activism at a time when our communitieswould rather see people who inject drugs locked up rather than understood, treatedand supported.
However, despite achieving the inclusion of harm reduction within mainstreamhealthcare, the attitudes of the public have not changed towards people who injectdrugs. Look beneath the thin veneer of acceptability for harm reduction in ourcommunities and there remain the same pernicious and ignorant views about druguse which are ill-informed but ensure that people who use drugs remain some ofthe most marginalised in our society.
This is due in part to the UK government’s insistence that drugs and drug useremain illegal and the fear and ignorance within our society that leads many tobelieve people who use drugs should be locked up rather than helped. Society doesnot see them as worthy of compassion and healthcare and resents ‘their taxes beingspent’ on injecting equipment and treatment. It’s also due to the failure of a trulyrepresentative and sustainable model of a service user involvement movement, whichwould have helped ensure service users’ views and rights were central to the planning,funding and commissioning process at both the political and service delivery level.
A PERFECT STORMSadly, since 2010, England has systematically disinvested in harm reduction. Thepolitical firestorm debate of 2008 saw the abstinence model of intervention win outover harm reduction, and the government’s new drug policy in 2010 saw a political
Cover story
www.drinkanddrugsnews.com6 | drinkanddrugsnews | September 2019
We urgently need tobecome activists oncemore, argues Nick Wilsonin his contribution to The Vision Project
shift away from harm reduction. This occurred at thesame time as a move in the commissioningresponsibility for drug services from the thenprimary care trusts to local authorities, just as theauthorities ran out of money. The ring-fencing offunding for HIV, which supported drug services,disappeared and harm reduction had to startcompeting for funding against a range of otherworthy causes within public health.
There is no doubt that many people havebenefited beyond their hopes from the opportunitiesdelivered by the recovery model, but many peoplewho use drugs are so much worse off. In the UK weare experiencing an increase in homelessness, anddrug-related deaths are higher than they have everbeen. We have now also had the worst HIV outbreakin 30 years, a fact which outside of Scotland hardlyanyone knows or talks about.
DIMINISHED SERVICEMany harm reduction services that traditionally provided a front door into treatmentservices and, no less importantly, a safety net for people who couldn’t manage thetreatment options on offer, now provide little more than the distribution of injectingequipment. The systematic disinvestment in harm reduction in England has left manypeople alone, isolated and vulnerable, without skilled harm reduction workers to dowhat they always have: engage, support and save lives.
A recent exchange on social media quoted a triage discussion with a new clientregistering at a needle and syringe programme provided by a large national charity:‘Whilst going through the triage paperwork to register he was asked his preferenceregarding administration of substances. He told the worker he was an IV user. Theworker didn’t know what that was, so he expanded saying he was an intravenoususer. The worker still didn’t know what that meant.’
Does this represent what happens in most drug services? Of course not, but it

chAnge
September 2019 | drinkanddrugsnews | 7www.drinkanddrugsnews.com
A NEED FOR VISIONDeveloping Health & Independence (DHI), a West of Englandbased social exclusion charity are marking their 20th anniversarythis year with The Vision Project. This series of articles, podcastsand events is exploring the question of how they can achievetheir vision to ‘end social exclusion by ensuring that everyonehas their basic needs met and is able to thrive by contributing tothe richness and wellbeing of their community’. All articles andpodcasts can be found at www.dhi-online.org.uk/vision-projectand you can sign up to get latest updates on the project atwww.dhi-online.org.uk/newsletter.
does happen and it absolutely should not. So many drug services now have staffcovering the needle and syringe programme who do not have the requiredknowledge, skills or even, in some cases, the appropriate attitudes to engage withsome of the most marginalised and vulnerable people in our society.
In this environment, good quality harm reduction cannot happen and we havelittle hope of reducing or ending the harms and social isolation of drug users untilthere is enough political will to develop a drug policy which truly reflects the valueof human life. Naloxone is not the answer to saving the lives of people who usedrugs. Harm reduction is, of which naloxone is one important component.
THE PROPER SUPPORTWe must celebrate the commitment and compassion of those who work in our fieldand properly educate, train, mentor and support them. This doesn’t have to cost theearth – it’s not a financial issue, it’s a cultural one. In a world increasinglydominated by pharmacy provision of syringes, we appear to have forgotten how tolike and respect people who use drugs. If we lack positive enthusiasm andoptimism, what right do we have to expect this in others?
Services must properly support our amazing colleagues to once again create theculture of acceptance and engagement, save more lives and improve the health ofpeople who inject drugs. We need to reimagine how harm reduction can work inthis austere climate and, yes, maybe this also means we need to rediscover a newstyle of activism to once again make a difference by keeping people who injectdrugs alive and well.
We must also engage with our communities in a way that encourages them toreframe their understanding of drugs and the people who use them. We have tochallenge attitudes and break down the barriers that prevent society from feelingcompassion, understanding and acceptance for people who make life choices thatcan carry risk.
We accept people who make life choices that lead to heart disease, diabetes,respiratory disease and cancer, yet condemn people who inject drugs for ‘wastingprecious health resources’ .
This health inequality is perverse and is perpetuated by a political policy whichcontinues to classify people who inject drugs as criminals, fails to support harmreduction and does nothing to challenge society’s perpetual exclusion of peoplewith genuine health needs. In the absence of any political will to address this, ouronly hope is that the field can become activists once more and bring about thechange we need.
We did it before; we can do it again.
Nick Wilson is from Exchange Supplies, a social enterprise specialising in harmreduction equipment. The Vision Project published this piece on 28 July to coincidewith World Hepatitis Day.
‘We have been effective at reducing the
risks associated with injecting drug use
and developing interventions which
deliver some of the most cost-effective
health interventions of any kind.‘
www.drinkanddrugsnews.com
News Focus
8 | drinkanddrugsnews | September 2019
THANKS FOR SHARING
NHS ENGLAND’S TARGET DATE TO ELIMINATEHEPATITIS C IS 2025 – five years ahead of theWorld Health Organization’s 2030 target. It’san ambitious objective, and one that theNHS is confident it can meet. ‘We areworking, we are curing people, the strategyis being successful,’ its clinical lead for hep C,Dr Graham Foster, told last December’sSeven years to elimination: the road to 2025conference (DDN, February, page 12). Delegates at the same event, however,
also heard the results of an evaluationproject by King’s College’s National AddictionCentre on operational delivery networks(ODNs) meeting their hep C targets. One ofthe main obstacles identified was missingdata, frequently the result of providershaving different electronic patient recordsystems – an ‘endemic problem across theNHS’, according to the National AddictionCentre’s Dr Katherine Morley.
THE IMPORTANCE OF EFFECTIVE DATA SHARINGNow a new report from the London JointWorking Group on Substance Use andHepatitis C (LJWG) is highlighting theimportance of effective data sharingprocesses if the elimination target is to bemet. Treatment and testing for hep C hasimproved dramatically in recent years, butwith more diagnoses happening at differentlocations – drugs and outreach services, GPsurgeries, prisons – it’s crucial thatorganisations have systems in place that canprocess and share patient informationefficiently. Eradicating the virus will only happen if
the many services engaged with people with
hep C ‘join up their data systems so thatpeople who are diagnosed can progressquickly and easily to treatment and care’,said LJWG co-chair and clinical director ofSouth London and Maudsley NHSFoundation Trust’s Central Acute andAddictions Directorate, Dr Emily Finch. Whilejoining up data systems might sound fairlysimple, the reality is ‘not straightforward’,the report states. Different organisationshave different IT systems and differentprocesses for sharing their diagnoses withODNs, treatment providers and PublicHealth England (PHE). ‘These issues aretechnical but they are absolutely vital inmaking the system work for patients,’ itstresses.
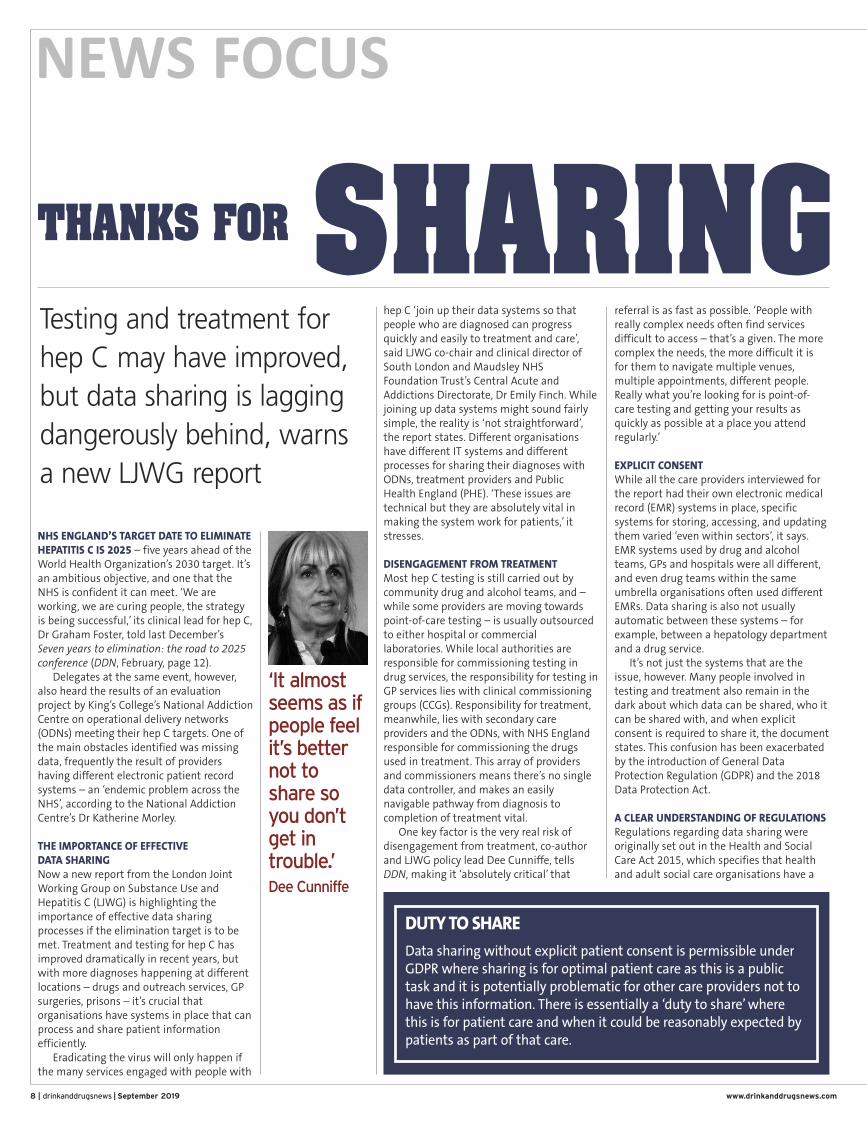
DISENGAGEMENT FROM TREATMENTMost hep C testing is still carried out bycommunity drug and alcohol teams, and –while some providers are moving towardspoint-of-care testing – is usually outsourcedto either hospital or commerciallaboratories. While local authorities areresponsible for commissioning testing indrug services, the responsibility for testing inGP services lies with clinical commissioninggroups (CCGs). Responsibility for treatment,meanwhile, lies with secondary careproviders and the ODNs, with NHS Englandresponsible for commissioning the drugsused in treatment. This array of providersand commissioners means there’s no singledata controller, and makes an easilynavigable pathway from diagnosis tocompletion of treatment vital. One key factor is the very real risk of
disengagement from treatment, co-authorand LJWG policy lead Dee Cunniffe, tellsDDN, making it ‘absolutely critical’ that
referral is as fast as possible. ‘People withreally complex needs often find servicesdifficult to access – that’s a given. The morecomplex the needs, the more difficult it isfor them to navigate multiple venues,multiple appointments, different people.Really what you’re looking for is point-of-care testing and getting your results asquickly as possible at a place you attendregularly.’
EXPLICIT CONSENTWhile all the care providers interviewed forthe report had their own electronic medicalrecord (EMR) systems in place, specificsystems for storing, accessing, and updatingthem varied ‘even within sectors’, it says.EMR systems used by drug and alcoholteams, GPs and hospitals were all different,and even drug teams within the sameumbrella organisations often used differentEMRs. Data sharing is also not usuallyautomatic between these systems – forexample, between a hepatology departmentand a drug service. It’s not just the systems that are the
issue, however. Many people involved intesting and treatment also remain in thedark about which data can be shared, who itcan be shared with, and when explicitconsent is required to share it, the documentstates. This confusion has been exacerbatedby the introduction of General DataProtection Regulation (GDPR) and the 2018Data Protection Act.
A CLEAR UNDERSTANDING OF REGULATIONSRegulations regarding data sharing wereoriginally set out in the Health and SocialCare Act 2015, which specifies that healthand adult social care organisations have a
‘It almostseems as ifpeople feelit’s betternot toshare soyou don’tget introuble.’Dee Cunniffe
Testing and treatment forhep C may have improved,but data sharing is laggingdangerously behind, warnsa new LJWG report
DUTY TO SHARE
Data sharing without explicit patient consent is permissible underGDPR where sharing is for optimal patient care as this is a publictask and it is potentially problematic for other care providers not tohave this information. There is essentially a ‘duty to share’ wherethis is for patient care and when it could be reasonably expected bypatients as part of that care.
More on hepatitis C atwww.drinkanddrugsnews.com
legal obligation to share patient informationwith each other in order to provide the bestcare possible. While GDPR and the DataProtection Act do not actually alter therequirements of this in terms of sharingdata to facilitate care, many people areunaware or unsure and tend to very mucherr on the side of caution. Clinicians, information governance
specialists and Caldicott Guardians – thepeople responsible for protecting theconfidentiality of personal health and careinformation and ensuring that it’s usedproperly, and which all NHS organisations
are required to have – were all interviewedfor the report. While the Caldicott Guardiansand information governance personnel hada clear understanding of the basis on whichdata could be shared, this had not‘penetrated all levels of clinical practice’, thereport found. Many people believed thatobtaining written consent from patients wasthe ‘best’ – or only – basis on which datacould be shared.
SHARING DATA AS PART OF CLINICAL PRACTICEThis is ‘at odds with’ the Health and Social
Care Act and GDPR, the report points out,which ‘create an obligation to share data forpatient care and provide a legal basis fordoing so that does not require explicitpatient consent’. This confusion and anxietyabout what sharing is or isn’t permissiblemeans that information often ends up notbeing shared at all, even when it wouldclearly be in the best interests of patients. ‘When we spoke to the Caldicott
Guardians and the information governancepeople the overall feeling was, “We don’tunderstand why people are doing this,”’ saysCunniffe. ‘People need to talk to theirCaldicott Guardians and IG leads and askthese questions. I think senior managerscould do with doing it as much as anybody.’ The focus should not be on consent as
the ‘sole legal basis for sharing andprocessing patient data,’ the reportcontinues. ‘GDPR has specific allowances forsharing data as part of clinical practice, bothin terms of delivering care andadministrative work, that do not requireexplicit consent.’ LJWR wants to see thedevelopment of clear guidance and training,particularly for drug service staff, aroundwhen explicit consent is needed, which datacan be shared, who it can be shared withand under what circumstances. This could beprovided by PHE or the ODNs. ‘Ever since the LJWG was established
there’s been times when people will say “wecan’t share that”, then you’ll go to anotherarea and they will,’ says Cunniffe. ‘When westarted up our pharmacy testing project(DDN, June 2018, page 5) we found thatpeople are just really edgy about sharingdata with each other. It almost seems as ifpeople feel it’s better not to share so youdon’t get in trouble.’Ultimately, a lot of these issues could be
solved by effective training, she says. ‘I thinkthere’s a real need for organisations to standup and tell their staff, “Look, you’re OK – youcan do this.” It wouldn’t take much to getthose messages out there. But we needorganisations to take a lead on it.’ DDN
Information sharing pathways between careproviders involved in hepatitis C testing andtreatment (left): The arrows indicate the flowof information to and from the different careproviders that is needed to ensure successfultesting and completion of treatment.Source: ljwg.org.uk
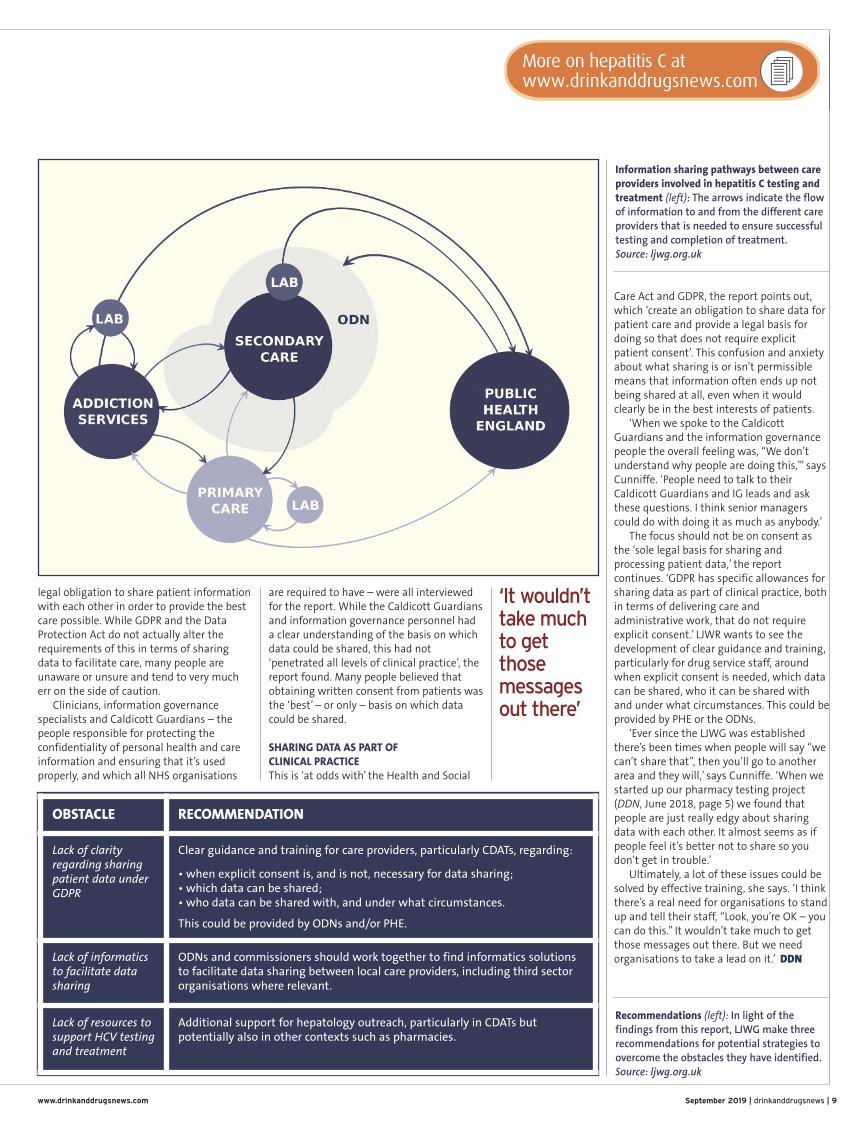
OBSTACLE RECOMMENDATION
Lack of clarityregarding sharingpatient data underGDPR
Clear guidance and training for care providers, particularly CDATs, regarding:
• when explicit consent is, and is not, necessary for data sharing;• which data can be shared;• who data can be shared with, and under what circumstances.
This could be provided by ODNs and/or PHE.
Lack of informaticsto facilitate datasharing
ODNs and commissioners should work together to find informatics solutionsto facilitate data sharing between local care providers, including third sectororganisations where relevant.
Lack of resources tosupport HCV testingand treatment
Additional support for hepatology outreach, particularly in CDATs butpotentially also in other contexts such as pharmacies.
Recommendations (left): In light of thefindings from this report, LJWG make threerecommendations for potential strategies toovercome the obstacles they have identified.Source: ljwg.org.uk
September 2019 | drinkanddrugsnews | 9www.drinkanddrugsnews.com
‘It wouldn’ttake muchto getthosemessagesout there’

Pain management
www.drinkanddrugsnews.com10 | drinkanddrugsnews | September 2019
My name is Paul.I’m 51 and live ina small markettown in the PeakDistrict. I enjoyeda happy
childhood and walked straight into afull-time job after school. At 18 I joineda local concrete manufacturingcompany and spent around ten yearshand stacking very heavy paving slabs.
One morning at work I injured myback. This was in the days whereawareness around health and safetyissues was far lower than today, and Ihad some physio and returned to worka few days later. Over the followingyears I was promoted many times, butcontinually experienced problems withsevere, debilitating lower back andneck pain.
Around ten years ago I wasdiagnosed with degenerative discdisease after MRI scans showeddamage to five discs in my back andtwo in my neck, all believed to becaused by the heavy manual job I didfor years. Numerous injections at thepain clinic offered no relief and I waseventually prescribed OxyContin.
Each time I visited the doctor the
dosage was increased as it was nolonger giving me any pain relief, until Iwas eventually prescribed 800mg perday – but taking 1,500mg per day. Iwould wake up around 2am then spendthe rest of the night thinking of excusesfor how I could collect my prescriptionearly. OxyContin was the last thing Ithought about at night and the firstthing in the morning. At this point, Iwas no longer taking this amount ofOxyContin to relieve the pain – I wastaking it simply in order to function. Irealised I had a serious problem.
One tablet was supposed to last afull 12 hours – I was taking my doseevery couple of hours. However I kepttelling myself I couldn't possibly be anaddict, as I had been prescribed this bymy doctor. There were times when Iwould run out because my GP was onholiday and the locum or other doctorsrefused to prescribe such a highamount. I would then suffer full-blownwithdrawal until I could pick up mynext prescription.
Around this time I was involved in acar accident. While lying in the hospitalbed the nurse asked me if I was takingany medication. When I told her800mg of OxyContin per day, but
actually almost double that, she said,‘You must mean 80mg.’ I replied no,and my partner confirmed the amount.
I got another, better-paid job butwas still taking around 1,500mg perday and was eventually let go. Sittingat home wondering what I was goingto do, I started to replay things in mymind – what if that car accident wasactually my fault due to the amount ofOxyContin I was taking? What if Ibelieved I was doing a good job butactually wasn't and that’s why they letme go? I decided I’d had enough andwanted my life back. I made an urgentappointment with my doctor and said Iwanted off all the OxyContin.
I was then told that there had beenseveral meetings held about me, and
my doctor had been reprimanded byother GPs at the surgery over theamount of OxyContin I had beenprescribed over such a long period. Iwas then referred to my first drugclinic, where the drug worker said theycouldn’t help me as it wasn’t heroin.Another clinic told me the same thing.
I moved back to the small town Igrew up in and registered at the localGP surgery.
The doctor drew up a taper planthat I was determined to follow. Overthe following months I stuck to it andwas doing really well, managing toreduce from the 1,500mg down to theactual prescribed level of 800mg, thengradually further until I’d droppeddown to 320mg per day.
Paul was prescribed OxyContinafter an industrial injury. But thatwas just the start of his problems
A PRESCRIFOR PAIN
Findings from the 2014/15 Crime Survey for England and Wales examinesthe extent and trends in illicit drug use among a nationally representativesample of 16 to 59 year olds resident in households in England and Wales.In 2014/15, for the first time the survey included questions relating tomisuse of prescription painkillers (use of prescription analgesics by thosefor whom they are not prescribed). Findings include:
• Overall, 5.4 per cent of adults aged 16 to 59 years had misused aprescription-only painkiller not prescribed to them
• 7.2 per cent of 16 to 24 year olds had misused a prescription-only painkillerin the last year, while 4.9 per cent of 25 to 59 year olds had done so.
• People with a long-standing illness or disability were more likely tohave misused prescription-only painkillers.
• Misuse of prescription painkillers is distributed more evenly across thegeneral population than the use of illicit drugs
• Misuse of painkillers was similar in both rural and urban areas
September 2019 | drinkanddrugsnews | 11www.drinkanddrugsnews.com
More on prescription drugs at:www.drinkanddrugsnews.com
‘I was then referred to my first drugclinic, where the drug worker said theycouldn’t help me as it wasn’t heroin.Another clinic told me the same thing.’
IPTION
THERE HAS BEEN A CONSIDERABLE INCREASE in the focus on prescribed opioidpainkillers lately, and with good reason given the alarming statistics on overdosedeaths from the US alongside massive increases in prescribing in the UK.
This has resulted in improved awareness of the risks associated with these drugs,and hopefully means that careful consideration will be given before using them for
non-cancer chronic pain and fewer patientswill continue them where there is nosubstantial benefit. However we are stillleft with a large number of patients whohave been prescribed these drugs for manyyears, and that brings us to the potentiallythorny issue of de-prescribing. How do webest approach this?
Some may advocate reducing andeventually stopping these drugs for all inwhom there is no sizeable reduction inpain, but how to assess that? For somepatients, years of taking them have blurredthe line between benefit, tolerance anddependence. Auditing prescribing data can
be a good start, and writing to patients and flagging notes to discuss at medicationreviews are useful tools as well.
Richard is a case in point. He is 70 and has been taking opioids for manyyears, originally for osteoarthritis that developed in his early 50s. He has a historyof depression and anxiety, was alcohol dependent for many years, and cares forhis wife who is slowly dying from severe COPD.
As well as his opioids he also takes regular diazepam, although over the yearsthe dose of this has come down. He is currently on a 100mcg fentanyl patch, co-codamol and Oramorph. He freely admits that he is dependent on these but asthey were started by a doctor, he doesn’t feel he should have to stop them. Isuspect this is a common scenario.
We had a lengthy consultation and I was able to explain that medical opinionwas changing, that these drugs were now felt to be less effective than we usedto believe, and that decreasing liver and kidney function could mean he was atgreater risk of overdose as he got older. We also discussed the impact on his wifeif he wasn’t around to care for her. Following our conversation we agreed that wewould reduce his fentanyl from 100 to 87mcg and in six months to 75mcg, whenwe would discuss the situation again.
This probably wouldn’t be enough for the aggressive de-prescribers, but as a GPI can hopefully take a pragmatic long-term approach. It would be better if thesituation had never arisen. However it has, and an individualised approach agreedbetween the prescriber and the patient seems to my mind the best compromise.
Steve Brinksman is a GP in Birmingham, clinical lead for SMMGP and RCGPregional lead in substance misuse for the West Midlands
Addressing long-termprescribed opioid userequires an individualisedapproach, says Dr Steve Brinksman
Post-its from Practice
But doc… I’ve Beenon them for years
‘An individualised
approach agreed
between the
prescriber and the
patient seems... the
best compromise’However, this is where my journeyto hell began, going around in circlesfrom doctor referrals to drug clinicsand pain clinics, being told the sameold story and referred back to my GP. Iwas suicidal at this point. I’d done sowell to reduce my dose, but could nolonger see any way forward. EventuallyI contacted Release who got one of thedrug clinics to agree to treat me, andafter an agonising few months,starting on a minimum dose of 30mlof methadone that didn’t even holdme for two hours, they eventually gotme to a dose of 105ml where I wasstable and no longer going throughhorrendous withdrawals. I reduced themethadone over many months until Ifinally became drug-free.
However in 2016 I was diagnosedwith severe ‘central’ sleep apnoea. Mydriving licence was revoked and I wastold after blood tests that mytestosterone level was zero. I also haveperipheral neuropathy from perniciousanaemia, where it is painful to walk
due to nerve damage in my feet, and Istill have the degenerative disc diseasein my back. However, I’m looking atalternative relief rather than the legalheroin I was given that almost tookmy life.
My main passion and purpose nowis to educate everyone about howlong-term opiate use destroys livesand actually makes pain so muchworse in the long term. Opiates dohave a very important role to play inpain relief, but only in certainsituations and only for the short term,prescribed and monitored very closely.Even though I was lucky enough tobeat my addiction, I am now having todeal with the long-term health effects.Not only did my addiction takeeverything I had, it also greatlyaffected the people who I love most.
If by telling my story and raisingawareness of what I experienced I cansave even one person from sufferingwhat I went through, it will have beenworth it.

URGENT MEASURESFirst, people whouse opiates likeheroin need easyaccess to qualitytreatment in theirown communities.This means theright dose of areplacement
medication and an experienced keyworker to support and listen to them.
Second, we need to invest more incommunity outreach. Many localservices have faced cutbacks and thereality is that outreach services barelyexist anymore.
Third, we need a national push topromote the overdose reversal drugnaloxone. It is a safe, effective, life-saving tool and we need to get peopletrained and carrying naloxone all overthe country.
Fourth, the rise in cocaine deathsshows treatment services need to domore to reach out to this group.
These are crisis measures. They areurgent and necessary. But we will onlymake real progress if we tackle povertyand disadvantage in our communities. Mike Dixon, chief executive, Addaction
STRONGER FOCUS ON PREVENTION
We believe thatdrug policy shouldbe guided by thebest availablescientific evidence,rather than byideology or political
expediency and this includes anevidence-based approach to drugsclassification. We call for a stronger focuson prevention and the root causes ofproblematic substance use. Interventionsshould be delivered by a skilledworkforce in collaboration andconsultation with peers in recovery and
professionals from other areas such asprimary care, mental health, housing andemployment support. Drug users mustalso receive equitable access to healthservices to improve their physical health.Royal Society of Public Health andFaculty of Public Health
EVIDENCE-BASEDTREATMENT
Long- term heroinusers with poorhealth, whofrequently use acocktail of differentdrugs and alcohol,are most at risk.For this group thebest way to
prevent drug-related deaths is to getpeople into treatment. Widescaledistribution of naloxone kits which canbe used to save someone’s life if theyoverdose from heroin is also key.Jay Stewart, director for public healthand substance misuse, Turning Point
A PUBLIC HEALTH CRISISWe know thatdrug-relateddeaths are linkedto age andcomplicated byhealth conditions.Poverty,deprivation,homelessness and
mental health conditions all increasethe chances of a life lost to drugs. Thatis why we need investment insubstance misuse services that supportpeople to improve their physical andmental health.
Working with our partners, we arefully committed to offeringcomprehensive care and supporting ourservice users to be healthier andhappier. This includes providingmedical help and opportunities for
housing, volunteering, training andmeaningful work.
We continue to prioritise thenational distribution of life-savingnaloxone kits. In the last year alone,more than 1,500 lives have potentiallybeen saved through naloxone.
This is a national public health crisisand action is needed. Our message toany person or organisation that canprevent another drug-related death issimple – we are ready to work with you.Mark Moody, chief executive, Change Grow Live
LOSS OF HARM REDUCTION TALENT
This report furtheremphasises theneed for a focus oneffective harmreductioninterventions as
well as a need to address key stresseson the treatment system, such asnaloxone prescribing and the overallcapacity of the workforce which has
experienced a significant loss of talent,particularly harm reduction specialists.
It is clear that the ability of thetreatment system to respond is beingstunted by ongoing budget reductions,instability in commissioningarrangements and the overall budgetavailable. When will government draw aline in the sand and decide enough isenough around drug- related deaths?NHS Substance Misuse Providers Alliance(NHS SMPA)
FOLLOW THE EVIDENCE!With thiscondition, as withmany othermedicalconditions, weneed to follow theevidence and notwhat peoplewould prefer to be
true. The evidence shows us thatopioid substitution treatment andother forms of treatment that goalongside decriminalisation, such ashas been done in Portugal – increasingwelfare, reducing punishment andproviding public health services – havebeen shown to reduce drug-relateddeaths, and that’s what we should bedoing.
Most of the people who suffer fromchronic drug use have had verydifficult lives including bereavement,trauma, abuse and neglect. Very few ofthose people who have been usingheroin for a long time do that out ofchoice – they do it because they arecaught in a situation where heroin useis the only way to reduce their pain.
[For] people that have got intoproblematic patterns of heroin use, themost effective thing we can do isprovide them with good treatmentand stop punishing them.Alex Stevens, professor in criminaljustice and joint chair of ACMD,speaking on BBC Radio 4
12 | drinkanddrugsnews | September 2019 www.drinkanddrugsnews.com
Comment
Crisis pointLast year had the highest number of drug-related deaths on record – 4,359 people, accordingto the Office for National Statistics (ONS). What should we do to reverse this appalling trend?
‘Our message toany person ororganisa tionthat can preventanother drugrelated death issimple – we areready to workwith you.’

September 2019 | drinkanddrugsnews | 13www.drinkanddrugsnews.com
THE INCREASE IN DRUG-RELATEDDEATHS hasn’t suddenly happened,deaths have been rising significantlyfor years. There has been ampleopportunity to think about how toreverse this horrendous trend. Andunusually, we know how to do it.The evidence has been collected andmade available to ministers… So ifit’s not a lack of evidence, somethingelse must be holding back politiciansfrom tackling the rise in drug-relatedmortality. It’s seductively simple topoint out the failings of politicianson this issue. But they instinctivelyfollow public opinion rather thanshape it. So the uncomfortable truthmight be that we, the electorate, areresponsible.Ian Hamilton, Independent, 15 August
FEW EXPERTS consider thatcriminalising vulnerable andmarginalised people who inject drugsis an appropriate response. The UKgovernment should stop politickingabout being ‘tough on drugs’ and acturgently to stop the harm to which its
policy contributes.Decriminalisation ofpersonal drug useallows interventionssuch as safer injectingrooms and drug testingwhere appropriate. Italso enables gatheringof evidence. What isalready clear is thatmoralising aboutperceived intrinsicwrongs in taking drugsand blaming or punishingpatients for having drug usedisorders are not effective or
ethical ways to reduce harm.Richard Hurley, BMJ, 8 August
MOST ADDICTION SERVICES are notproperly connected to wider healthand care teams, so people arebounced between addiction andmental health services or fallbetween the gaps in both. It’s notuncommon for a patient to beexcluded from mental health servicesdue to having drug or alcohol usedisorder but not be able to accessaddiction services because they havean untreated mental illness. Thisrepresents a lost opportunity toimprove outcomes for patients,reduce the harm to individuals andtheir families, as well as a staggeringwaste of limited resources. Julia Sinclair, BMJ, 23 August
AS THE SICKLY-SWEET STENCH OFMARIJUANA spreads ever furtheracross the once-civilised Westernworld, there is one universal result.There are more crazy people. Some ofthem are dangerous. Many of themare crazy because they have fried theirbrains with skunk. Some are crazierstill because baffled doctors haveadded to the cocktail with variouspoorly understood prescription drugs.But the chances that you will meetsuch a person grow daily, as ourleaders refuse to enforce the lawsagainst marijuana possession. Theywill grow still more if they are stupidenough to bow to the billionairecampaign to legalise this poison.Peter Hitchens, Mail on Sunday, 11 August
The news, and the skews, in the national media
IT WAS WITH GREAT SADNESS THAT THE KEYS TO CITY ROADS DETOX UNIT WEREHUNG UP FOR THE FINAL TIME EARLIER THIS YEAR – a service with a legacy of over40 years of supporting drug and alcohol users to reach their goals. A staff team ofexceptionally passionate people who genuinely had a heart for their clients andwho steered them towards success at every opportunity, a team who hadembraced changes where others may have crumbled under the pressure of ‘this ishow it has always been done’ and did everything in their power to uplift thisservice in the face of political adversity.
I was interested to see in the August issue of the Nursing Standard an articlediscussing the NHS England data of almost 7,000 full-time equivalent days sick leavebecause of drug and alcohol issues. The majority of these issues were related toalcohol, with staff using it as a coping mechanism to manage stress and anxiety. Thesolution wasn’t clear, other than staff needing more support in some form.
This data was between Oct 2017 and Nov 2018 and I have neither seen norheard a whisper of a measurable response. I have watched staff crumble underpressure throughout my career and it is never a surprise when a substance isbrought into the mix. I have seen colleagues become mentally unwell and I haveattended funerals of those who have committed suicide, yet the approach seemsto never change and surprise is a first response.
With the closure of City Roads and one less place in the country to supportsuch people, I find myself trepidatious about what NHS England may have up theirsleeve and would like those reading this from varying organisations to considerhow they support their staff – not just with treatment, but to have the confidenceto come forward.
Ishbel Straker is a clinical director, registered mental health nurse, independentnurse prescriber and board member of IntNSA
What are we doing to support nurses’health, asks Ishbel Straker
Crumbling under
pressure
CliniCal eye
Have your say on issues that count:www.drinkanddrugsnews.com
‘Theuncomfortabletruth might bethat we, theelectorate, areresponsible.’
MEDIA SAVVY
/DDNMagazine @DDNMagazine
www.drinkanddrugsnews.com
Letter
StrIKIng�A�BALAnCeSteve Rolles makes some valid points inhis response to my letter (DDN,July/August, page 12), and I’mencouraged by the fact that he says manyissues around legal regulation are tricky,that challenges exist, balances need to bestruck, and that there’s ‘no perfectanswer’. I’ve always been in favour ofdecriminalisation, and I’m open tohearing a well-argued case forlegalisation and regulation as well.
What antagonises me is theunquestioning certainty of much that’swritten on this subject by many mediacommentators – ‘war on drugs’ bad,legalisation good – as if it were somemagic bullet that would miraculously end
all drug harms and put the world’sorganised crime groups out of businessovernight. So it’s nice to hear somethinga bit more nuanced (and it goes withoutsaying that Transform know considerablymore about this subject than youraverage columnist).
He’s also right to say thatmephedrone’s popularity had a lot to dowith MDMA shortages, althoughevidence does suggest that a significantproportion of its users were people whohadn’t really taken many drugs beforeand did so because it was legal. One ofmy points he doesn’t address, though, isthe question of the US – a massiveincrease in legal opioid prescribing,coupled with a massive increase inopioid-related deaths.
Molly Cochrane, by email
Prisons
www.drinkanddrugsnews.com14 | drinkanddrugsnews | September 2019
Case dismissed
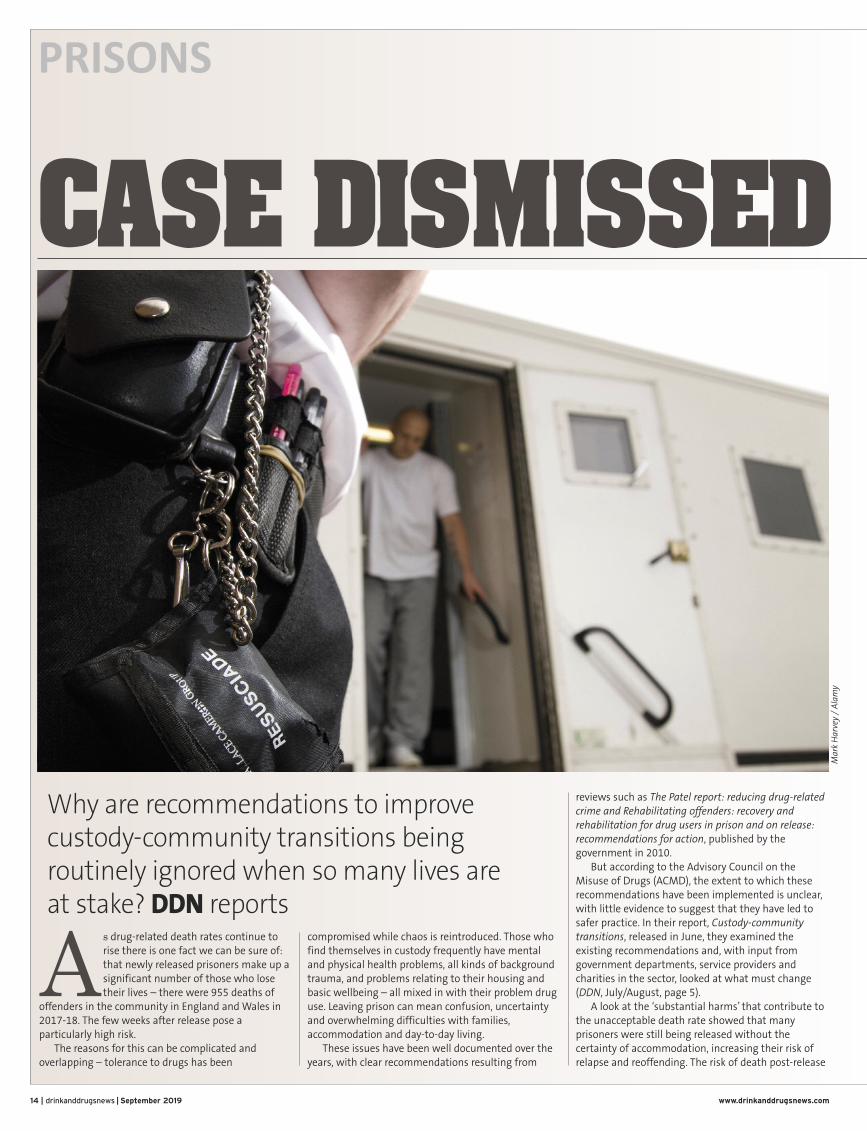
As drug-related death rates continue torise there is one fact we can be sure of:that newly released prisoners make up asignificant number of those who losetheir lives – there were 955 deaths of
offenders in the community in England and Wales in2017-18. The few weeks after release pose aparticularly high risk.
The reasons for this can be complicated andoverlapping – tolerance to drugs has been
compromised while chaos is reintroduced. Those whofind themselves in custody frequently have mentaland physical health problems, all kinds of backgroundtrauma, and problems relating to their housing andbasic wellbeing – all mixed in with their problem druguse. Leaving prison can mean confusion, uncertaintyand overwhelming difficulties with families,accommodation and day-to-day living.
These issues have been well documented over theyears, with clear recommendations resulting from
reviews such as The Patel report: reducing drug-relatedcrime and Rehabilitating offenders: recovery andrehabilitation for drug users in prison and on release:recommendations for action, published by thegovernment in 2010.
But according to the Advisory Council on theMisuse of Drugs (ACMD), the extent to which theserecommendations have been implemented is unclear,with little evidence to suggest that they have led tosafer practice. In their report, Custody-communitytransitions, released in June, they examined theexisting recommendations and, with input fromgovernment departments, service providers andcharities in the sector, looked at what must change(DDN, July/August, page 5).
A look at the ‘substantial harms’ that contribute tothe unacceptable death rate showed that manyprisoners were still being released without thecertainty of accommodation, increasing their risk ofrelapse and reoffending. The risk of death post-release
Why are recommendations to improvecustody-community transitions beingroutinely ignored when so many lives are at stake? DDN reports
Mark Harve
y / Alamy

was many times higher than in the general population,particularly in the first few weeks – yet naloxone wasnot being provided routinely to guard against fataloverdose. Furthermore, the opportunity to reduce drugproblems in custody was being squandered by thesubsequent failure to provide support on release.
In the last ten years a new challenge had alsoemerged through widespread use of syntheticcannabinoid receptor agonists such as ‘spice’ – addingnew health priorities to the continuing efforts to containblood-borne viruses, particularly HIV and hepatitis C.
So if progress has stalled, where does the failurelie? The picture from the ACMD is of fragmentedresponsibility and a lack of systematic follow-up.Continuity of care appears to be missing throughoutthe transition period – the latest PHE data shows thatonly 32 per cent of people who were assessed asneeding treatment on release were having treatmentin the community within 21 days.
Many of the deaths resulted from overdose, yet thecommunity policy of maximising access to naloxone(to reverse the effects of an opioid overdose) stillhasn’t reached English prisons. Only 12 per cent ofprisoners who were previously dependent on heroinleft prison with naloxone in 2017-18 because ofreluctance among NHS providers to fund it – asituation that could be resolved by funding throughnational NHS bodies, including NHS England.
With much to tackle, the ACMD hasmade key among itsrecommendations the need for aminister, nominated by the DrugStrategy Board, to take over-arching
responsibility for improving custody-communitytransitions for prisoners with complex health needs.
‘The fragmentation of responsibility forimplementing the previous reports andrecommendations in this area is one of the problemswe’ve identified,’ Alex Stevens, co-chair of the ACMDtold DDN. ‘This is why we’ve recommended that asingle minister be made responsible for implementingthese recommendations and previous ones, includingthe Bradley review [2009] and the Patel report [2010].’
While realistic that there could be delays inresponding ‘because of all the turmoil politically’, he ishopeful that interest shown last year by RobertBuckland MP could prove useful in terms of continuity,since he has been made minister for justice.
In the meantime, there is much that could andshould be done now. ‘Given that, from the spendingannouncements we’ve been getting from BorisJohnson, austerity seems to be officially over, there’sno reason that money shouldn’t be spent on savingpeople’s lives by distributing naloxone,’ he says.
Other recommendations have already been madebut need renewed attention – such as the
recommendation to change Friday release dates forvulnerable prisoners, to give them a fair chance ofexperiencing joined-up working between custody andcommunity. ‘This is an odd one,’ says Stevens. ‘NACROreleased a report last year arguing for reductions inFriday afternoon releases and the pushback they gotfrom the Ministry of Justice was that if this was workingproperly, it shouldn’t make a difference what day of theweek you’re released on. But all the reports from theinspectorates of both prison and probation show thatwe do not have a system that’s working properly.’
In some cases, the recommendations are anextension of existing initiatives, such as making sure
people have access to universal credit or a chance ofemployment, along with help to find somewhere tolive. ‘There are pilots going on and we’re arguing thatthese should be accelerated,’ he says. The problem –such as in the case of universal credit, where there is apartnership between the Department for Work andPensions and the Prison Service – is that they arecompeting with so many other priorities.
‘We’re arguing that more priority should be givento this population because it’s so highly vulnerable tohealth problems, but also problematic in terms of itshigh level of reoffending,’ says Stevens. ‘And so therewould be wins for public health and crime reduction ifpriority was put on meeting the needs and solving theproblems of this population.’
And while we wait for the processes ofgovernment, what should the treatment communitybe doing? The ACMD talks about the vital need foreffective community pathways and says the ‘main aim’of the planned reforms to probation should be dealingwith offenders in the community – a conclusion builton effectiveness, safety and ‘substantially cheaper’cost. That surely points to a highly proactive role forcommunity drug and alcohol services?
Stevens recommends looking at the other recentreport, by the Ex-Prisoners Recovering from AddictionGroup, chaired by Lord Patel. ‘This has developed ablueprint for pathways between custody andcommunity for people with various different types ofdrug treatment need, including those who haveachieved abstinence in prison – a group that’s often letdown when they leave prison,’ he says. ‘There arepractical steps available in that report.’
Much is being pinned on hopes for a nominatedminister, and within that person’s mandate thisindicator of progress stands out: ‘reducing thenumbers of people who die within four weeks ofleaving custody and while under supervision of theprobation services.’ Could this be the opportunity tojoin up the strands of research and recommendationthrough a clearly defined brief? DDN
September 2019 | drinkanddrugsnews | 15www.drinkanddrugsnews.com
‘If progress has stalled,where does the failurelie? The picture fromthe ACMD is offragmentedresponsibility and a lackof systematic follow-up.Continuity of careappears to be missingthroughout thetransition period.’
‘All I want is real help’I’ve spent a total of 28 years in custody and over three years in isolation. For years
I’ve searched out drugs to give me comfort. When I’m released I find myself
scoring and telling lies. I use and it fills that void and temporarily gives me the
power to be confident and feel I fit in better. Once it comes to light you’re using,
the powers that be recall you and I end up again in deeper discomfort, knocked
back again. My hope has gone. The jail’s chocka with drugs and I’m expected to
never pick up and use. My family is gone, my mother is in a care home. I’m full of
guilt and resentment and all I really want is real help and someone in my corner
encouraging me, but I’m falling short of finding good people who get me and
know how to help me. The truth is I contemplate suicide a lot.
Colin, in a letter to DDN editor

UPPING THEIR GAMEAhead of September’s Recovery Month, people fromacross Britain gathered to celebrate recovery at thesixth annual Recovery Games in Doncaster last month.The games are the brainchild of Aspire drug and alcoholservice, which is run in partnership with RotherhamDoncaster and South Humber NHS Foundation Trustand The Drug and Alcohol Service (ADS). These games celebrate the achievements, personal
journeys and overcoming of challenges faced bypeople in recovery from a drug or alcohol problem.They provide the opportunity for shared experiencesand making new friends and connections withlikeminded people who are in recovery themselves.The games symbolise that recovery is possible withthe right support and inclusive recovery communities.
This year the demand from across the UK to takepart exceeded all expectations, with 50 teams fromEngland, Scotland and Wales registering andcompeting in a day of gladiator-style games and
obstacle courses on the ground and in the water. Suchwas the demand that registrations unfortunately hadto be closed early, but plans are afoot to make the2020 Recovery Games even bigger and better. The raincouldn’t dampen the energy and enthusiasm of thecompetitors and spectators, with just short of 1,000people attending on the day.The Recovery Games represents a movement
towards inclusiveness, and this year saw a push toattract more spectators from the general public.Families with young children came along andenjoyed the carnival atmosphere, and teams madetheir own costumes or wore fancy dress to celebratecomradery. This in turn contributed to the build-up ofexcitement, creating a sense of equality by givingservice users, support groups and workers a sharedconnection and purpose.The Recovery Games is a mix of celebration,
excitement, inspiration and emotion. The minute’ssilence at the middle of the day was an opportunityfor everyone to show respect for the ‘fallen warriors’who’ve lost their battle with addiction. This wasfollowed by the spectacular ‘festival of colours’ whichcelebrated being alive – you can watch the film viathis link https://youtu.be/2FxPd6yhjL8 The overall winner this year was the ‘Greased
Lightning’ themed team from New Beginnings, aDoncaster based rehab and detox unit run by Aspire.The games were made possible by donations and theproceeds from the sale of merchandise, especially themuch-admired t-shirts which have helped secure an
important step towards funding the 2020 games.‘This year’s games were the biggest and best yet,
with the recovery community being stronger andmore vibrant than ever,’ said event organiser NeilFirbank of Aspire. ‘The event is about letting peopleknow that recovery is alive and being nurtured inmany towns across the region and the UK. Thank youto everyone who took part and supported thisamazing event.’Tim Young, chief executive of ADS, said the games
were a ‘great day of celebration. For the first time thisyear the weather wasn’t kind to us and yet the rain didnothing to dampen the magic of the event. If anythingthis year has added ‘the year of the rain’ to the legendof the Recovery Games in the same way Glastonburyhas its infamous ‘year of the mud’. A day of powerfulimages and emotions, the games once again broughtpeople together to make new connections andreinforce existing ones. The message it sends is clearand loud – “recovery is possible, and fun!”’Once again it was a fantastic day, exceeding all
expectations, with hundreds of people comingtogether to celebrate and applaud those in recoveryfrom an addiction. The event has become a recognisedmilestone in the recovery calendar. It sees people withdifferent addictions and health conditions cometogether, connect, give and learn new skills, but mostimportantly have fun without the need for substances.
Stuart Green is service manager at Aspire drug andalcohol service
More recovery activities at:www.drinkanddrugsnews.com
RecoveRy
‘...this year saw apush to attract morespectators from thegeneral public.’
16 | drinkanddrugsnews | September 2019 www.drinkanddrugsnews.com
The sixth annualRecovery Games werethe biggest and bestyet, says Stuart Green

www.drinkanddrugsnews.com September 2019 | drinkanddrugsnews | 17
Classified advertising | Training and services
Interpersonal Group TherapyIntermediate level clinical trainingfrom the Centre for Addiction Treatment Studies
The UK’s first interpersonal group therapy course beyond
introductory level, this course is suitable for those working with
people with substance and behavioural addictions and related
problems.
The clinical training will build your knowledge of, and
competency and confidence in the interpersonal group therapy
model, and increase your understanding of how it can be
effective in improvements in relationships and quality of life.
Teaching takes place one Saturday a month for nine months,
starting 16 November. The teaching is delivered by tutors
Dr Tim Leighton and Nicky Adams.
Book your place: [email protected] / 01985 843780
www.actiononaddiction.org.uk
Get in touch today to speak to our confidential, professional and friendly team of experts,
(7 days a week, 9:00am – 9:00pm)
Ashton Road, Lancaster, LA1 5AZ01524 39375 [email protected]
‘From Dependence to Freedom’
The Pavilion is a stunning residential drug and alcohol treatment centre, delivering personalised and structured detoxification programmes, personally
tailored to each individual.
Low fees
Flexible payment plans
CQC rated ‘good’
Part of a not-for-profit organisation
All rooms en-suite
Experienced medical and wellbeing professionals
oday touch tt in tGe
01524 39375
eek, 9:00am – 9:00pm)s a w(7 day
onfidential, pro our cak to spe
eek, 9:00am – 9:00pm)
esional and friendly tesofonfidential, pr
[email protected] oad, Lancon RshtA
ts,xperam of ee
ZA1 5A, Lerastoad, Lanc

c l b i e r t y s d z
x c s d f k a a s a s
h m n s v j z x c f b
humankynd®
for fair chances
A people led organisation. Our diverse staff members come from a wide range of backgrounds and careers, but all share one common belief - that all people should have the opportunity to realise their full potential.web: humankindcharity.org.uk telephone: 01325 731160
Humankind horizontal 130mm x 214mm DDN advert - a people led organisation May 2019 v1.indd 1 28/05/2019 13:38:54
www.drinkanddrugsnews.com18 | drinkanddrugsnews | September 2019
Classified advertising | Services

Classified advertising | Recruitment and services
www.drinkanddrugsnews.com September 2019 | drinkanddrugsnews | 19
*228,282 screened since inception to end April 2019. DrinkCoach is delivered by Humankind | Reg charity: 515755 | Ltd company: 1820492 Reg office: Sapphire House, Aycliffe Business Park, Horndale Ave, Newton Aycliffe, DL5 6DS humankindcharity.org.uk
Test - App - Online Coaching
MAKE ALCOHOL A PRIORITY IN YOUR AREADrinkCoach is a cost-effective way to screen residents and deliver online advice and interventions.
• Invest-to-save• Evidenced-based• Fully digital pathway• Complements local services
Visit www.drinkcoach.org.uk for more information
More than 220,000 screened
so far*
Current clinical opportunities include:
Experienced Nurses and NMP’s to work within our Substance Misuse sector in London, Leicester, Wiltshire and Rochdale & Oldham
We offer Bank and Permanent opportunitiesRunning health facilities and services on a not-for-profit basis, we invest every penny back into our care - and our people.So if you’re ambitious and focused on helping people with substance misuse issues, progress your career with us.
We support people across the UK with substance misuse issues. As a part of our clinical team, you’ll make a real difference to their lives as you go above and beyond to help them with their daily needs.
For more information please contact [email protected] or visit us at https://careers.turning-point.co.uk

Could you helppeople achievetheir potential?
Change Grow Live (CGL) Registered Office: 3rd Floor, Tower Point, 44 North Road,Brighton BN1 1YR. Registered Charity Number in England and Wales (1079327) and inScotland (SCO39861). Company Registration Number 3861209 (England and Wales).
We are an equal opportunities employer and hold theprestigious Investors in People Silver award.
Change Grow Live (CGL) offers a wide range of employee andvolunteer opportunities which can encourage behaviour change,improve health and relationships and make a real difference topeople’s lives. We currently support 66,000 people each day.
We value creativity and initiative and you will be encouraged tocontribute your ideas to the development of our substancemisuse, health and social care and criminal justice services. Wework with adults, young people and families and roles includenurses, recovery workers, service managers and team leaders.
We offer employees:
− A professional and supportive environment
− An hour a week to spend doing something positive for yourpersonal wellbeing
− A competitive salary
− 25 days annual leave (rising to 30 days per annum)
− A generous contributory pension scheme
− Personal and professional development, including training courses, mentoring programmes and time off to pursue relevant qualifications.
Volunteers can also gain valuable experience and many of ourvolunteers go on to gain paid roles.
For further information about the roles we have available please visitwww.changegrowlive.org/jobs