Embed Size (px)
Citation preview
1
Duke Radiation Safety Manual Site-Specific Excerpts Duke University Hospital: Department of Radiology
Origination Date: 01/01/2019
Review/Revision Dates: 01/01/2019
Introduction
This document is a collection of excerpts from the Radiation Safety Manual for Duke University and Medical Center (RSM) that are pertinent to the radiation protection issues encountered in the Department of Radiology at Duke University Hospital. The most current version of the complete RSM is available on the Occupational and Environmental Safety Office’s web site (https://www.safety.duke.edu/) under Policies/Manuals.
For convenience, these excerpts are arranged in order of applicability to radiology and nuclear medicine practice, and are cross-referenced to the contents in the institutional RSM. Passages highlighted in yellow with footnotes address important issues that are commonly encountered in practice. A set of facsimiles of pages from the Radiation Safety Division’s web site that address various radiation emergency scenarios is included at the end of this document.
Contents GUIDELINES FOR THE SAFE USE OF X-RAY EQUIPMENT ............................................................................... 2
CLINICAL RADIATION SAFETY PROCEDURES [Nuclear Medicine] ................................................................. 3
MEDICAL X-RAY DOSIMETRY ......................................................................................................................... 7
THYROID BIOASSAYS ..................................................................................................................................... 8
REPRODUCTIVE HEALTH POLICY ................................................................................................................. 10
SEALED SOURCES ........................................................................................................................................ 11
MEDICAL CENTER AND CAMPUS X-RAY MACHINES ................................................................................... 12
AUTHORIZATION FOR MEDICAL USE OF RADIOACTIVE MATERIAL IN HUMANS: PHYSICIANS, MEDICAL PHYSICISTS AND NUCLEAR PHARMACISTS.................................................................................................. 14
INFORMED CONSENT FOR PROCEDURES INVOLVING IONIZING RADIATION IN CLINICAL INVESTIGATIONS .................................................................................................................................................................... 16
2
GUIDELINES FOR THE SAFE USE OF X-RAY EQUIPMENT The following policies pertain to the safe use of x-ray producing equipment. Such equipment includes, but is not limited to, digital and fixed plain-film radiographic equipment, bone densitometers, mobile (portable) units, CT scanners and fluoroscopy units. Other provisions set forth in pertinent subsections of the North Carolina Administrative Code, Title 10A, Chapter 15, Section .0600 shall also apply.
a. Individuals who will be operating the x-ray equipment shall be instructed in the safe operating procedures and use of the equipment, and demonstrate an understanding of such procedures.
b. Written safety procedures and rules shall be established and made available to each individual who operates x-ray equipment. All operators shall be familiar with these rules.1
c. Only the professional staff and ancillary personnel required for the medical procedure or for training shall be in the room during the radiographic exposure. “Ancillary personnel” may include parents of pediatric patients assisting with x-ray procedures for the purpose of avoiding sedation.
d. All individuals shall be positioned so that any part of the body (including the extremities) which may be exposed to the primary (useful) beam is protected by 0.5 mm lead equivalent.
e. Personnel not protected by shielding aprons shall avoid exposure to the primary beam, and should remain at least six feet away from the x-ray tube in order to minimize exposure to scattered radiation.
f. Professional staff and ancillary personnel shall be protected from direct scatter radiation by protective aprons or whole body protective barriers of at least 0.25 mm lead equivalent.
g. Mechanical holding devices shall be used whenever medical circumstances permit. If a human holder is required, the hand or other parts of the body that might be exposed to the primary beam shall be protected by 0.5 mm lead equivalent. No individual shall be used routinely to hold patients or film. Pregnant women and minors shall not hold patients or film during exposures.
h. Gonad shielding of at least 0.5 mm lead equivalent shall be used for potentially procreative patients during radiographic procedures in which the gonads are within the primary beam, except when doing so would interfere with the diagnostic procedures.2
i. No individual shall be exposed to x-rays for purposes of education, demonstration, training, research or any other purpose not related to the healing arts, unless the individual is participating in clinical research approved by the Duke Institutional Review Board.
RSM Reference: Chapter XI, Section E, Subsection 2
1. This refers to the “Written Radiation Safety Program” that is required by North Carolina regulations. Compliance with this requirement is via mandatory annual completion of an on-line module available on the OESO Training web site.
2. Gonadal shielding is not required when the FOV does not include the gonads. Although shielding the gonads when they are not in the FOV is common practice, the questionable benefit must be weighed against the risks of heavy metal toxicity (shields may contain lead) and spread of infection from infrequently-cleaned vinyl covers.

3
CLINICAL RADIATION SAFETY PROCEDURES [Nuclear Medicine] The purpose of this Chapter is to provide radiation protection information to nursing staff and other hospital personnel who may come in contact with patients who have received diagnostic or therapeutic amounts of radioisotopes or with radiation-producing devices such as portable x-ray machines.
Specific information on radiological protection for employees of the Radiology, Nuclear Medicine and Radiation Oncology Departments may be found in the Radiation Safety Procedures documents located in those departments.
A.NURSING CARE OF PATIENTS TREATED WITH RADIOPHARMACEUTICALS
Radiation hazards to nursing staff, ancillary personnel and visitors are due to (a) irradiation by emissions from radioactive isotopes in the patient, (b) accidental contamination of the skin by radioactive material, and (c) accidental ingestion of radioactive material. The following policies are intended to minimize the hazard associated with the therapeutic use of radiopharmaceuticals.
1. Patients requiring hospitalization for treatment with radiopharmaceuticals who cannot be released under the conditions of 10 CFR 35.75 or the applicable North Carolina regulations shall be provided with a private room with private bathroom facilities.
2. Before the patient is admitted to the room, the floors, and sink may be covered with a suitable removable protective material, if indicated by circumstances and consistent with patient safety. The Radiation Safety Division is responsible for the preparation of rooms used to house in-patients being treated with radiopharmaceuticals. Appropriate radioactive trash disposal containers will be placed in the room by Radiation Safety Division personnel.
3. Once the radioactive material has been administered to the patient, the patient will be considered to be restricted under "Radiation Precautions". The rooms occupied by these patients shall be posted with a sign bearing the standard radiation symbol (a black or magenta tri-blade on a yellow background) and the words "Caution: radioactive material". Ancillary personnel should not enter these rooms without consulting medical, nursing or the Radiation Safety Division.
4. “Radiation Precautions” shall be ordered by the Radiation Safety Officer or his/her designee for radiation therapy patients who fulfill the regulatory criteria for radiation isolation. Radiation precautions include, but are not limited to, restricting the patient to his/her private room and bath facilities, restricting public access to doorways and corridors adjacent to the room if dose rates exceed applicable regulatory limits, limiting visitors, removal of bodily fluids and trash by Radiation Safety Division personnel, and exclusion of pregnant women or nursing mothers from the room. Radiation precautions shall be discontinued only by order of the Radiation Safety Officer or his/her designee, and only when the patient has fulfilled the regulatory criteria for the discontinuation of radiation isolation.
5. Patients not being treated with radionuclides shall not occupy a room previously used for radionuclide treatment until that room has been cleaned and surveyed for residual contamination. Protective coverings and waste disposal containers located in patient rooms shall not be removed unless so directed by personnel of the Radiation Safety Division. These materials will generally be removed when radiation precautions have been discontinued and the patient has been discharged from the room. However, in the event that it is necessary for the patient to remain hospitalized after radiation

4
precautions have been discontinued, any protective covering materials may be left in place at the discretion of the Radiation Safety Division.
6. Clinical specimens of urine or blood required for patient care should be obtained at the minimum frequency consistent with appropriate patient care. Hospital phlebotomists or clinical laboratory staff who obtain, transport and process clinical material shall do so while following the applicable policies and procedures of the Clinical Laboratory Service.
7. The body of a patient who dies while undergoing systemic radionuclide therapy should not be removed from the room until such transport has been approved by staff of the Radiation Safety Division.
8. Personnel shall not eat, drink or smoke in areas where unencapsulated radioactive material is used in patient treatment or if the possibility of contamination of the hands exists. Skin contamination, ingestion or inhalation of radioactive material can be avoided by wearing appropriate personal protective equipment (PPE) and frequent hand washing. In general, the protective principles based on the Standard Precautions for Blood and Body Fluids shall be followed.
9. Time spent close to patients should be limited to the minimum amount of time required to perform duties consistent with effective patient care. The Radiation Safety Division may issue special instructions, depending upon the nature of the treatment and any specific hazards associated with it.
10. For high-dose radioiodine treatments, protective gloves and shoe covers shall be worn upon entering a patient's room. Hands shall be washed with soap and water after leaving a patient's room. Contaminated materials, including urinals, bedpans, basins paper handkerchiefs, gauze sponges, shoe covers and gloves, shall be discarded into the non-porous garbage bags provided in the room and transported by the Radiation Safety Division for storage and decay. Sharps shall be disposed in the appropriate sharps disposal containers. Articles or utensils suspected of being contaminated, including the patient's personal effects, shall be monitored by the Radiation Safety Division prior to final disposition.
11. Linen which may be contaminated by vomiting, incontinence, or profuse perspiration shall be disposed in the box with the trash.
12. Protective gloves shall be worn while cleaning possibly contaminated equipment. In the case of radioiodine-131 therapy, patient urine will be collected in containers placed within special shields provided by the Nuclear Medicine Division, unless such collection would lead to unsafe conditions for personnel. These containers will be removed by Radiation Safety Division personnel. The patient is to be encouraged to take responsibility for his/her own urine collection, if possible. Stool may be disposed of via the sanitary sewer unless collection is specifically requested.
13. If there has been a spill of urine or other contaminated material, the Radiation Safety Division or Nuclear Medicine personnel shall be notified immediately.
B. VISITING POLICY FOR FAMILIES OF PATIENTS UNDERGOING SYSTEMIC RADIONUCLIDE THERAPY
The purpose of this policy is to enable patients being treated with systemic radionuclides such as radioiodine-131 to spend brief periods of time with family members during protracted hospitalization. Visit duration and frequency are intended to ensure that dose rates to the hospital staff and visitors are maintained below the applicable statutory limits on exposure to the general public.
5
1. No provision contained in this policy shall be construed to override a physician's written order that prohibits visitors, or hospital policies intended for infection control.
2. Children under age 18 or visitors who are pregnant shall not visit.
3. Visits shall not exceed 30 minutes.
4. Two visits per day per visitor are permitted, separated by one hour or more.
5. No more than two people may visit at a time.
6. The patient and the visitors should be positioned in the room so that the maximum practical distance is maintained between the patient and the visitors.
7. Visitors are to remain in the area of the room closest to the door. The door must remain closed during the visit.
8. Visitors must wear shoe covers and gloves while in the room, and should dispose of them in the box provided within the room. Visitors must not use the patient's bathroom or eat from the patient's food tray.
9. For patients housed in the shielded rooms on DHN Division 9300, visitors will not be permitted during the first 24 hours following administration of radioiodine-131, except under circumstances as approved by the Radiation Safety Division.
C. RELEASE OF PATIENTS TREATED WITH RADIONUCLIDES FROM RADIATION PRECAUTIONS
Federal and North Carolina State regulations and the Duke University Medical Broad Scope Medical License conditions permit Duke University Medical Center to release patients from radiation precautions when certain conditions are met. The patient may be released from radiation precautions when:
1. The patient is continent of urine and is capable of an appropriate degree of self-care; and:
2. The exposure rate at one meter from the patient does not exceed seven (7) milliroentgens per hour; or
3. The iodine-131 radioactivity retained in the patient does not exceed 33 millicuries; or
4. Computations performed in accordance with Nuclear Regulatory Commission NUREG 1556, Volume 9, Revision 2, Appendix U determine that the estimated dose to a member of the general public consequential to release of the patient will not exceed 500 millirem (5 mSv) in one calendar year. If the calculation of estimated dose to the general public is based in part on tissue shielding, biological elimination and / or an occupancy factor less than 0.25 at one meter, then the release shall be documented and the record retained for three years. Instructions to patients regarding measures to ensure that dose to the public is ALARA, and instructions to women breast-feeding infants and children, shall be issued to patients in accordance with NUREG 1556.
Duke Radiation Safety personnel may release patients from Radiation Precautions whenever the applicable criteria are met. This "release from radiation precautions" shall not be construed as an order to discharge the patient from the hospital. At their discretion, Radiation Safety personnel may continue to require that patient waste be confined to the patient's room until it is removed by Radiation Safety.
6
D. PATIENTS TREATED WITH SEALED SOURCES (BRACHYTHERAPY IMPLANTS)3
The following practices are intended to minimize the hazards associated with sealed brachytherapy sources.
1. Should an implant become dislodged during treatment, it must never be touched with the bare hand. Long tongs, forceps or other devices should be used to return it to an appropriate shielded container.3 Appropriate on-call medical staff, including the Radiation Oncology resident on call shall be notified immediately in the event an implant becomes dislodged. The Radiation Safety Division should also be contacted as soon as possible. Loss of a brachytherapy source shall be reported immediately to the Radiation Safety Officer of his/her designee.
2. Intact sealed sources do not usually present a contamination hazard. However, personnel must always be alert to the possibility that the integrity of any sealed source may be compromised in the event that it is damaged or mishandled. If this is suspected, notify personnel from the Radiation Safety Division immediately.3
3. For temporary (removable) implants, patients shall be confined to their rooms until the implant is removed, unless otherwise authorized by the Radiation Safety Division. After the implant is removed, the patient poses no radiation hazard. While the implant is in place, the room will be posted with a "Caution: Radioactive Material" or "Caution: Radiation Area" sign until precautions are removed. Personnel or visitors should not enter these rooms without consulting medical or nursing staff, or the Radiation Safety Division.
4. Radiation exposure to personnel may be minimized by (a) working within the room as quickly as feasible, consistent with effective care, and by (b) spending as much time as possible behind any movable lead shields that may be placed around the bedside.
The body of a patient who dies while undergoing implant therapy should be removed from the room until such transport has been approved by the staff of the Radiation Safety Division.
RSM Reference: Chapter X, Sections A-D
3. This section is pertinent to the use of radioactive “seeds” to localize non-palpable breast tumors or lymph nodes. Seeds may migrate along the needle track and become dislodged, remain in the needle or otherwise be subject to loss. “Reverse-action” forceps are recommended for handling a dislodged seed. The Mammography Division is equipped with a Geiger-Mueller (GM) detector to aid in the location of a misplaced seed. Although the low-energy photons from the radioactive material in the seeds is detectable externally by a GM detector, the doses rates from the seeds present no significant risk, even when no shielding is used. The benefit of using x-ray shielding PPE in settings other than mammography-guided seed placement is minimal, and must be weighed against the risk due to the clumsiness of the PPE.
7
MEDICAL X-RAY DOSIMETRY 1. Personnel operating portable x-ray machines and fluoroscopic units shall wear whole-body dosimeters at the collar level, as directed by the Radiation Safety Officer. Dosimeters shall be worn outside any shielding aprons or other shielding personal protective equipment, unless specified otherwise. In these cases, assigned personnel dose will be equal to the values of deep dose equivalent and shallow dose equivalent calculated by the dosimetry vendor, or as directed by the Radiation Safety Officer.
2. Two additional methods are available for determining personnel dose in instances where there is significant exposure to high x-ray fluoroscopic workloads and where personnel can demonstrate the routine use of shielding aprons as personal protective equipment. In the first method (designated as EDE-2), the radiation dose from a single external monitor is used to compute effective dose equivalent (EDE). In the second method (designated as EDE-1), two external monitors are used to compute EDE.
a. For personnel monitored using the EDE-2 calculation, the single dosimeter shall be worn outside the shielding apron at collar level.
b. For personnel monitored using the EDE-1 calculation, one dosimeter shall be worn outside the shielding apron at collar level. A second dosimeter shall be worn underneath the shielding apron at waist level. Wearing the two dosimeters consistently in the proper locations is important. The proper placement of each dosimeter in the EDE-1 system is depicted on the face of each badge.4
3. Special Dose Calculations: The choice of method used to compute EDE for personnel who work with high-dose fluoroscopy (EDE-1 or EDE-2) will be determined by the Radiation Safety Officer on a case-by-case basis, and for individuals exceeding 25% of the annual whole-body dose limits.
a. Algorithms for the EDE-1 and EDE-2 computations will be employed as directed by the appropriate regulatory and advisory agencies (US NRC, Regulatory Issue Summary 2002-06, “Evaluating Occupational Dose for Individuals Exposed to NRC-Licensed Material and Medical X-rays).
b. Effective dose to the lens of the eye or other organ dose weighting factors for external exposure will be evaluated and assigned to individuals by the Radiation Safety Officer on a case-by-case basis when reliable, accurate and predictable estimates of effective dose equivalent are possible, given the conditions of exposure, and are based upon methods that are acceptable to the Radiation Protection Section of the North Carolina Department of Health and Human Services.
RSM Reference: Chapter V, Section B
4. This refers to the so-called “double-badge system”. The double-badge system may be used in interventional settings and gives a much better estimate of EDE than the single “outside the lead” value. The two badges must be (a) diligently worn and (b) worn consistently in the correct locations. Failure to pay attention to these details may lead to an incorrect assessment that the EDE has exceeded the occupational limit and may lead to termination of performing procedures.
8
THYROID BIOASSAYS 1. APPLICABILITY
a. Individuals directly involved* in clinical radioiodine therapy using unencapsulated material shall obtain a thyroid burden measurement not to exceed seven (7) days following administration of the therapy dose. The Director of Nuclear Medicine, in consultation with the RSO, determines the assay time window.
*Definition of individuals who are "directly involved" with radioiodine therapy:
i. For unsealed solutions of iodine-131 (I-131) sodium iodide for oral administration: The patient self-administers the material. Other individuals "directly involved" include the person who removes the lid from the vial, the person who holds the vial and straw while the patient ingests the solution, the person who rinses the vial to permit full ingestion and the person who handles the radioactive waste.
ii. For closed-system intravenous or intrathecal administrations of bound forms of I-131: Individuals "directly involved" include the person who connects the I-131 syringe to the closed injection system, the person dispensing the radiopharmaceutical into the closed system, the person who manipulates any three-way stopcocks or other manual valves (or the connections to the intravenous or intrathecal lines during the administration), the person(s) who dismantles the closed system and the person who handles the radioactive waste.
iii. Individuals excluded from the "directly involved" requirements are observers who are not physically contacting the patient, the administration paraphernalia or the radioactive waste.
b. Individuals directly involved in the handling of stock vials and radioiodination procedures in the Radiopharmacy shall obtain a thyroid burden measurement not to exceed than seven (7) days following the procedure. Required bioassay time windows may vary depending on the nature of the procedure and the amount of radioiodine employed. The Director of Radiopharmacy, in consultation with the Radiation Safety Officer, determines the time window for each procedure involving radioiodine.
c. Individuals directly involved in radioiodinations performed in authorized research laboratories shall obtain a thyroid burden measurement not to exceed than seven (7) days following the procedure. The amount of radioactivity and the conditions under which the procedure is performed are subject to the limits and conditions set forth in Table 2 below.
2. SPECIFIC RECOMMENDATIONS
Based on the biokinetics of radioiodine, it is generally recommended that thyroid monitoring be performed between 24 and 72 hours following a therapeutic administration or other procedure whenever practical. Individuals who are unable to comply with the requirements outlined in "Applicability" above should defer participation in procedures to others.
9
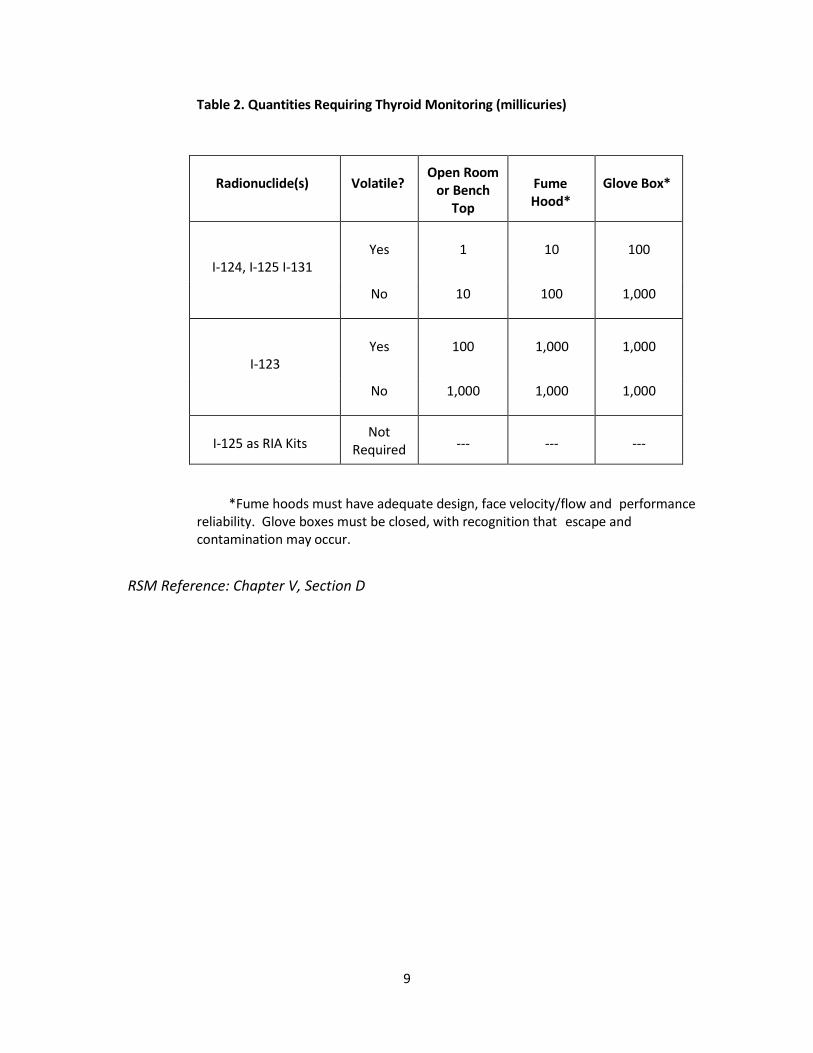
Table 2. Quantities Requiring Thyroid Monitoring (millicuries)
Radionuclide(s)
Volatile?
Open Room or Bench
Top
Fume Hood*
Glove Box*
I-124, I-125 I-131
Yes
1
10
100
No 10 100 1,000
I-123
Yes
100
1,000
1,000
No 1,000 1,000 1,000
I-125 as RIA Kits
Not Required
---
---
---
*Fume hoods must have adequate design, face velocity/flow and performance reliability. Glove boxes must be closed, with recognition that escape and contamination may occur.
RSM Reference: Chapter V, Section D
10
REPRODUCTIVE HEALTH POLICY Recognizing the need for the safety and well-being of the fetus during pregnancy, Federal and North Carolina State regulations and the Duke ALARA policy proscribes that the total dose equivalent to the embryo or fetus of a declared pregnant woman shall not exceed 5 mSv (500 millirem) during the period of gestation. Employees who become pregnant and must work with radioactive material or radiation sources during their pregnancy should contact Duke Employee Occupational Health and Wellness and complete a confidential Declaration of Pregnancy form. After declaring her pregnancy, the employee will then receive:
1. an evaluation of the radiation hazard from external and internal sources;
2. counseling from personnel of the Radiation Safety Division regarding modifications of technique that will help minimize exposure to the fetus;
3. a fetal dosimeter, if appropriate.
Employees who are not declared pregnant workers will not be issued a fetal dosimeter.
An employee who has declared her pregnancy shall inform the Employee Occupational Health and Wellness and the Radiation Safety Division if her pregnancy has ended for any reason.
RSM Reference: Chapter VI
11
SEALED SOURCES5 A. The Radiation Safety Officer shall ensure that leak tests and physical inventories are performed on those sealed sources specified and at the intervals specified in the applicable radioactive material license condition or applicable regulations.
B. The responsible Authorized User shall ensure that:
1. the Radiation Safety Officer is notified prior to the acquisition, transfer, relocation, destruction or disposal of any sealed source;
2. the Radiation Safety Officer shall be notified immediately upon the loss or suspected theft of any sealed source;
3. all sealed sources under the Authorized User's control are secured against unauthorized access or removal;
4. a complete inventory of all sealed sources under the Authorized User's control is maintained and kept available for inspection by Radiation Safety.
RSM Reference: Chapter IX
5. This section is pertinent to “radioactive seed localization” procedures. The seeds must be stored in an area that is secure from public access, and, if practical, kept in a locked cabinet. Every seed must be accounted for using the appropriate on-line software or other accounting mechanism. If a seed is misplaced during a procedure, on-site staff should restrict access to the area, begin the search for the seed using the GM detector and contact Radiation Safety immediately for assistance.
12
MEDICAL CENTER AND CAMPUS X-RAY MACHINES The State of North Carolina requires that all users of x-ray producing equipment register their x-ray machines with the North Carolina Division of Radiation Protection within thirty days of first use (North Carolina Administrative Code, Title 10A, Chapter 15, Section .0200).
1. ACQUISITION AND INSTALLATION OF X-RAY EQUIPMENT
The following policies pertain to the acquisition and installation of x-ray equipment facilities at the Duke University Medical Center or participating entities within the Duke University Health System.
a. The Department or clinical entity responsible for the x-ray equipment shall notify the Duke Radiation Safety Officer prior to the new construction or the renovation of existing facilities that house x-ray producing equipment.6 To ensure that shielding calculations and other recommendations are compliant with radiation dose limits to the public, a review of the proposed floor plans and shielding will be completed and submitted to the North Carolina Radiation Protection Section for approval. Installation or relocation of x-ray equipment shall not take place until an acknowledgement letter from the North Carolina Radiation Protection Section is received.6
b. The Radiation Safety Division shall be notified immediately following purchase, acquisition or installation of any x-ray producing equipment.6
c. Upon completion of construction and/or renovations, a shielding continuity survey should be performed for the area covered in the shielding calculation report.
d. Upon completion of the x-ray equipment installation, an environmental radiation protection survey of those unrestricted areas included in the shielding report shall be performed within thirty days of first use.7
e. All x-ray equipment, stationary and mobile, shall be added to the applicable registration with the State of North Carolina. All documentation will be kept on file at the offices of the Radiation Safety Division and a copy sent to the appropriate department manager.8
13
f. X-ray shielding aprons and other articles of x-ray shielding personal protective equipment shall be periodically inspected for integrity by each department. Results shall be submitted to the Radiation Safety Division via the Shielding PPE Registry Website: http://vmw-oesoapps.duhs.duke.edu/radsafety/aprons/ .
RSM Reference: Chapter XI, Section E, Subsection 1
6. The use of “shall” in (1a) and (1b) indicates “this is mandatory”. Acquiring x-ray equipment, or constructing/renovating x-ray facilities without prior notification of the Radiation Safety Division is a violation of Duke policy, and has resulted in Notices of Violation being issued to Duke by North Carolina regulators. Shielding designs by architects or outside consultants are not valid until they have been reviewed by Duke Radiation Safety, formally submitted to our State regulatory agency by Duke Radiation Safety, and an acknowledgement letter has been received by Duke Radiation Safety.
7. Important Note: Although North Carolina regulations require that a shielding continuity (integrity) survey be performed within 30 days of first clinical use, The Joint Commission’s standards require that the survey be performed prior to any clinical use. Contact Radiation Safety for a shielding integrity survey before using the equipment on patients.
8. In addition to the requirement for new equipment being added to a registration, old fixed equipment that is disassembled, moved and re-assembled must be re-registered. Notify the Radiation Safety Division before moving x-ray equipment to ensure that the proper FDA forms are obtained and the equipment is properly re-registered with the State. Similarly, equipment that is donated, sold, disposed or otherwise leaves Duke must be removed from its registration.
14
AUTHORIZATION FOR MEDICAL USE OF RADIOACTIVE MATERIAL IN HUMANS: PHYSICIANS, MEDICAL PHYSICISTS AND NUCLEAR PHARMACISTS The administration of radioactive material or therapeutic radiation to patients or research subjects at Duke University Medical Center is regulated by the US NRC, the US Food and Drug Administration (FDA), the State of North Carolina and the Medical Center Committee. In order to participate in the human use of radioactive material or accelerators, the applicant must provide evidence of training and experience that reflect those set forth in 10 CFR 35 and equivalent North Carolina regulations. These requirements generally involve (1) training in basic radioisotope handling techniques, (2) supervised clinical training in an institutional radiology, nuclear medicine or radiation oncology program, and (3) relevant experience.
The physician applicant for clinical use of radioactive material or accelerators must fulfill all of the following conditions:
1. Hold an active license to practice medicine in the State of North Carolina, as issued by the North Carolina Medical Board.
2. Have training and experience commensurate with the types and amounts of radioactive material applied for, as set forth in 10A NCAC 15.0318(c). Applicants may demonstrate fulfillment of the requirements either by (a) a combination of specialty board certification, documentation of alternative training and experience and by preceptor attestation; or (b) by having previously been named as an Authorized User on an NRC or Agreement State license for the clinical use of radioactive material.
3. Have contacted the Secretary of the Radiation Safety Committees or the Radiation Safety Officer, through his/her Departmental Chair or other individual designated by the Department. The applicant should submit a copy of the licensee’s registration certificate issued by the North Carolina Medical Board documenting current active licensure, a curriculum vitae, a copy of the applicant’s specialty board certificate, or letter of intent to certify from the specialty board and a letter of attestation (if applicable). If Authorization is sought through preceptor attestation in lieu of board certification, a preceptor attestation form as provided by the North Carolina Radiation Protection Section, or equivalent Agreement State or USNRC form (e.g. Form 313a), is required.
The medical physicist applicant must fulfill all of the following conditions:
1. Have training and experience commensurate with the clinical activities applied for, as set forth in 10A NCAC 15.0318(a). Applicants may demonstrate fulfillment of the requirements either by specialty board certification, or by preceptor attestation.
2. Apply to the Secretary of the Radiation Safety Committees or the Radiation Safety Officer through his/her Departmental Chair or other individual designated by the Department. The application must be accompanied by a curriculum vitae and a copy of the applicant’s specialty board certificate, or letter of intent to certify from the specialty board. If Authorization is sought through preceptor attestation, a complete, signed preceptor attestation form is required.
The nuclear pharmacist applicant for clinical use of radioactive material must fulfill all of the following conditions:
1. Hold an active license to practice pharmacy in the State of North Carolina, as issued by the North Carolina Board of Pharmacy.

15
2. Have training and experience commensurate with the types and amounts of radioactive material applied for, as set forth in 10A NCAC 15.0318(b). Applicants may demonstrate fulfillment of the requirements either by specialty board certification, or by preceptor attestation.
3. Make application to the Secretary of the Radiation Safety Committees or the Radiation Safety Officer. The application must be accompanied by a copy of the licensee’s registration certificate issued by the North Carolina Board of Pharmacy as documentation of current active licensure, a curriculum vitae and a copy of the applicant’s specialty board certificate, or letter of intent to certify from the specialty board. If Authorization is sought through preceptor attestation, a complete, signed preceptor attestation form is required.
Once all the application materials are received by the Secretary, the applicant may be granted provisional approval as an Authorized User by the Human Use Subcommittee. Formal approval will be granted by vote of the full Medical Center Committee at its next scheduled meeting. Authorized User status terminates if either (a) the Authorized User leaves Duke University Medical Center, (b) the applicant does not maintain active licensure with the applicable North Carolina licensing board or (c) the Authorized User’s clinical privileges at Duke University Medical center are suspended or terminated.
BASIC HUMAN RESEARCH AND THE RADIOACTIVE DRUG RESEARCH COMMITTEE
“Basic human research” means research intended to obtain basic information regarding the metabolism (including kinetics, distribution and localization) of a radioactively labeled drug or regarding human physiology, pathophysiology or biochemistry; but not intended for immediate therapeutic, diagnostic or similar benefit. For such studies, application must be made to the Duke University Medical Center Radioactive Drug Research Committee (RDRC). The RDRC reports to the US Food and Drug Administration (FDA). Investigators who wish to conduct basic human research on radioactive drugs shall make an application to the RDRC, consistent with the requirements of 21 CFR 361. Requirements include, but are not limited to, the following:
a. the amount of active pharmaceutical ingredient or combination of pharmaceutical ingredients to be administered shall be known not to cause any clinically detectable pharmacological effect in human beings, and
b. the radiation dose shall be the smallest practical to perform the study. Under no circumstances shall the whole body effective dose equivalent exceed a yearly cumulative value of 5 rem (50 mSv), or a single-exposure value of 3 rem (30 mSv). The total critical organ dose shall not exceed 15 rem (150 mSv) annually. For research subjects who have not reached 18 years of age, the maximum permissible whole body and critical organ exposure limits are 10 percent of the foregoing. A female research subject of childbearing potential shall state in writing that she is not pregnant, or shall be given a pregnancy test before participating in any study.
c. Approval of a protocol by the RDRC does not relieve the applicant of obtaining the approval of other entities, including the Duke Institutional Review Board, prior to conducting research in humans.
RSM Reference; Chapter IV, Section D, Subsection 1

16
INFORMED CONSENT FOR PROCEDURES INVOLVING IONIZING RADIATION IN CLINICAL INVESTIGATIONS Investigators supervising clinical trials that are subject to oversight by the Duke Institutional Review Board (IRB) must inform research subjects of any exposure to ionizing radiation consequential to participation in a clinical study (a) where the exposure exceeds the standard of care for the condition that is the subject of the study, or (b) as a normal volunteer. The IRB requires that such protocols undergo “Specialty Committee” review and approval. The Medical Center Committee acts as the Specialty Committee for protocols involving ionizing radiation. The Committee has adopted the following requirements relative to expressing radiation dosage to patients or research subjects who are participating in clinical or basic human research.
a. The investigator or his/her designee shall determine the types and numbers of radiological or nuclear medicine examinations that are required for participation in the clinical trial, which are beyond the “standard of care”.
b. The investigator or his/her designee may use the Duke Radiation Safety Committee’s web site (http://vms-oeseapps.duhs.duke.edu/radsafety/consents/default.asp) to compute the total effective radiation dose consequential to all procedures, and to use the resulting expression of risk in the “Risks and Discomforts” section of the informed consent document for the protocol. Benchmarks and wording formats suggested by the Web site include comparison to events encountered in daily living, such as airplane travel, and the annual natural background. The expression of risk is not restricted to the preceding formats. However, any expression of radiation dose must assist the subject in making an informed value judgment as to the magnitude of the risk attributable to ionizing radiation.
RSM Reference; Chapter IV, Section D, Subsection 2
Responses to Incidents Involving Radiation or Radioactive Materials
Radiation Safety Division
Duke University Medical Center
List of Incidents and Responses
• Emergency Contact Information for Radiation Safety • Spills Involving Radioactive Materials • Code Blue -- Emergency Involving a Radioactive Patient • Injuries Involving Radioactive Materials • Radioactive Seed Localization Procedure: Seed Loss or Transection • Inadvertent Exposure to Radiation While Pregnant • Radioactive Patients In the Hospital, or Coming to the Hospital • Loss or Theft of Radioactive Materials or Therapy Sources • Death of a Patient Containing Radioactive Materials
Emergency Contact Information for Radiation Safety
Emergency (24/7): Dial 911 and Request the Duke Radiation Safety On-call Responder
Patient Pager (Business hours): 970-9703
Web: www.safety.duke.edu/radsafety; click on EMERGENCIES link
684-2794684-2194
Spills Involving Radioactive MaterialsRadiation Safety Division -- OESO
Duke University and Duke University Medical Center
What You Should Do Immediately
(1) Prevent access to the spill to prevent personnel exposure and the spread of radioactive contamination. Cordon off the area. Put on a lab coat or disposable gown, shoe covers and protective gloves.
(2) DO NOT activate the HEICS 'Code Orange' process before consulting Radiation Safety.
(3) Notify the Radiation Safety Division, using any of the means on the "Contact Us" link on the Main Page.
(4) Contain the spill. Cover copiously with absorbent paper; do not wipe up.
How Radiation Safety Will Respond
(1) Assist in cleaning up the spill and decontamination procedures.
(2) Assist in surveying the area to ensure that residual contamination levels are acceptable.
(3) Notify State authorities if required.
Code Blue -- Emergency Involving a Radioactive Patient
Radiation Safety Division -- OESO
Duke University and Duke University Medical Center
What You Should Do Immediately
(1) Code procedures should be performed so as NOT to compromise the patient's chances for recovery. Radiation exposure should NOT be a consideration during the initial critical minutes of the code. As the code progresses and becomes more organized, measures can be taken to reduce personnel exposure.
(2) The patient should be BAGGED ONLY. Mouth-to-mouth breathing assistance should be avoided if at all possible.
(3) Face protection should be used by those at risk for splash exposure by saliva, respiratory secretions or vomitus. Gloves and gowns should be employed as usual. Universal precautions should be employed as usual.
(4) If time permits, portable shields may be employed. They can reduce the gonadal exposure of people who are in close. Lead aprons should NOT be sought out or worn. They are ineffective.
(5) Personnel assisting in procedures should maintain the maximum distance consistent with effective care.
(6) After the situation has resolved, staff should dispose of gowns, gloves, etc. in the box on the patient's room. Such materials should not be removed from the room. Other equipment (defibrillators, etc.) should be checked for contamination by Radiation Safety before they are removed from the room, unless they need to accompany the patient to an intensive care unit. Personnel should perform thorough handwashing.
(7) Radiation Safety personnel should be contacted when the situation stabilizes to assist in transfer of the patient to intensive care (beeper 970-9703, or Duke Police at 911). Transfer to the intensive care unit should be performed irregardless of whether the patient has been removed from "radiation precautions", if medically indicated. It

may be necessary to transfer other patients in Intensive Care to minimize their exposure.
(8) Personnel who experienced exposure to blood or body fluids should contact Radiation Safety within 24 hours to have thyroid monitoring performed.
How Radiation Safety Will Respond
Radiation Safety Staff are available for consultation regarding personnel surveys (including assistance with thyroid bioassays) and dose reconstruction.
Injuries Involving Radioactive Materials
Radiation Safety Division -- OESO
Duke University and Duke University Medical Center
What You Should Do Immediately
(1) For minor injuries (scalpel cuts, needle-sticks, splash to eyes, etc.): Flush the wound with copious amounts of water and dress it. Contact Occupational Medicine for a consult. If the cut or needle-stick involved contact with human blood, immediately dial 115 to contact the "Blood-Borne Pathogens" hotline. This takes precedence over any radiation considerations. The risk associated with hepatitis (B or C) and HIV is far higher than that of radiation. For splashes to the eyes, flush with water using a chemical eye-wash station. For splashes to bare skin, flush with copious amounts of water, then wash with soap and water. Survey the skin using a pancake GM detector; repeat if radioactivity is still present. Do not use a scrub-brush or solvents to clean skin.
(2) For major contamination (explosions, accidental ingestions, etc): Dial 911 and arrange for immediate transport to the Duke Emergency Department.
How Radiation Safety Will Respond
Radiation Safety Staff are available for consultation regarding personnel surveys and dose reconstruction.
Radioactive Seed Localzation Procedure: Seed Loss or Transection
Radiation Safety Division -- OESO
Duke University and Duke University Medical Center
What You Should Do Immediately
FOR SEED LOSS:
(1) Prevent access to the area to prevent inadvertent transport of the seed into unrestricted areas on shoes or clothing.
(2) Notify the Radiation Safety Division, using any of the means on the "Contact Us" link on the Main Page.
(3) Attempt to locate the seed using the radiation detection equipment normally used for the excision procedure, or a GM detector if in Mammography or Surgical Pathology. In Mammography, check implantation needles, operator's shoes, clothing, pants cuff's, etc. and re-survey the patient. In Surgery and Surgical Pathology, check specimen containers, waste receptables, staff clothing, surgical instruments and re-survey the patient.
(4) If the seed is located, do not handle it with bare fingers, even if gloved. Use forceps (preferably "reverse-action" type) to grasp seed and place in the shielded wrapper or other shielded container.
FOR SEED TRANSECTION AND/OR LEAKAGE:
(1) If a seed has been transected in the Operative Suite or Surgical Pathology with a release of the encapsulated radioactive material, prevent access to the spill to prevent personnel exposure and the spread of radioactive contamination.
(2) Using an appropriate radiation detection instrument, determine the extent of the spill.
(3) Contain the spill. If the spilled material is on the patient, cover liberally with sterile gauze. If on another surface, use absorbent paper. Do not wipe up; let the absorbent material contain the material.

(4) DO NOT activate the HEICS 'Code Orange' process before consulting Radiation Safety.
(5) Notify the Radiation Safety Division, using any of the means on the "Contact Us" link on the Main Page.
(6) In consultation with the Radiation Safety Division and the Radiopharmacy Director, consider oral administration of SSKI to the patient if the tissue absorption of radioactive iodine is likely.
How Radiation Safety Will Respond
(1) Assist in locating the seed and performing any required decontamination procedures.
(2) Assist in surveying the area to ensure that residual contamination levels are acceptable.
(3) Notify State authorities if required.
Inadvertent Exposure to Radiation While Pregnant
Radiation Safety Division -- OESO
Duke University and Duke University Medical Center
What You Should Do Immediately
(1) Do not panic. Most radiation exposures encountered in a campus research environment will not result in significant exposure to the fetus.
(2) Contact Employee Health (684-3136) and ask for a formal "Declaration of Pregnancy", if you have not already done so. You will receive an Occupational Medicine Consult. Occupational Medicine physicians will work with Radiation Safety Staff to perform the appropriate radiation dose reconstruction.
(3) If the exposure was to a patient during the course of a diagnostic or therapeutic procedure, inform the physician responsible for conducting the procedure.
How Radiation Safety Will Respond
Radiation Safety Division Staff will work with employees, Occupational Medicine physicians and individual physicians in Radiology, Cardiology or Radiation Oncology in performing dose reconstructions and risk assessments. Radiation Safety will provide appropriate radiation dosimeters to pregnant employees on a case-by-case basis.
Preventative Measures
(1) If you learn that you are pregnant, Declare your pregnancy to Employee Health (684-3136) as soon as possible. This confidential process assures you of maximum protection if you work with radioactive materials, hazardous chemicals (including chemotherapy drugs) or biohazards.

(2) Always use proper laboratory techniques when working with radioactive materials, whether or not you know you are pregnant.
(3) When interviewing patients who are being considered for elective diagnostic studies, obtain an age-appropriate history of sexual activity, birth control measures, last menstrual period and so forth to assess the need for further testing to rule out pregnancy.
Radioactive Patients In the Hospital, or Coming to the HospitalRadiation Safety Division -- OESO
Duke University and Duke University Medical Center
As a physician, nurse or ancillary care-giver, you may hear or believe that an in-patient you are caring for is 'radioactive'. Or, you may hear from the news media that people who were exposed to radiation by a nuclear accident or terrorist attack are coming to Duke.
What You Should Do:
(1) In all cases, report to work and carry on as usual. If required, Duke Radiation Safety will issue special procedures for you to follow.
(2) Patients who have been involved in nuclear accidents or terrorist attacks may be sent to Duke for specialized treatment such as intensive care or bone marrow transplants. Most patients will have been decontaminated (cleansed of radioactive materials or chemicals) before they get to Duke. In no case will a person exposed to radiation be a significant risk to your health. Follow any instructions issued by Duke Radiation Safety.
(3) Inpatients and outpatients who have had diagnostic scans in PET or Nuclear Medicine do contain small amount of radioactive drugs but present negligible risk to you, even if you are pregnant. Consult Duke Radiation Safety if you have concerns.
(4) Patients who have been to Radiation Oncology for linear accelerator treatments or high-dose-rate (HDR) implant treatments are not radioactive at all when they return to your Division. They present no risk to you.
(5) Patients who have had radioactive implants for prostate cancer or certain types of eye cancer present negligible risk to you. Follow the special "Radiation Precautions" issued by Duke Radiation Safety.
How Radiation Safety Will Respond
If necessary, Duke Radiation Safety Staff will issue special instructions, and are always available for consultation.
Loss or Theft of Radioactive Materials or Therapy Sources
Radiation Safety Division -- OESO
Duke University and Duke University Medical Center
What You Should Do Immediately
(1) Use a survey meter (pancake GM or ionization chamber) to attempt to locate the radioactive material. Check lab coats, trash cans, waste barrels, bed linens, food trays, etc. Visually check what you think may be "empty" lead pigs or shipping cartons.
(2) If the material cannot be located, notify Radiation Safety by dialing 911 from the Duke campus and requesting assistance with a radiological emergency.
(3) If theft is suspected, notify the Duke Police.
How Radiation Safety Will Respond
(1) Assist in locating the material in your laboratory or patient room.
(2) Survey the Laundry Facilities, trash carts, dumpsters, etc. to locate material.
(3) Report incidents to appropriate State authorities if required.
Preventative Measures
(1) Secure your radioactive materials. Keep them in lock-boxes, locked refrigerators or locked cabinets. Lock your laboratory doors if you must leave during experiments. Do not leave radioactive materials unattended.
(2) Be vigilant. Do not throw away newly received shipments of radioactive laboratory reagents. Do not allow unauthorized persons access to your laboratory areas. Keep proper inventory of radioactive materials and brachytherapy sources.
Death of a Patient Containing Radioactive Materials
Radiation Safety Division -- OESO
Duke University and Duke University Medical Center
What You Should Do Immediately
(1) Notify the Radiation Safety technologist on call (beeper 970-9703), or by calling the Duke Police.
(2) Do not remove the patient from the room until cleared to do so by the Radiation Safety Staff.
(3) For brachytherapy (implant) patients, notify the Radiation Oncology resident on call.
(4) Secure the room and do not permit entry to persons other than Radiation Oncology or Radiation Safety staff.
How Radiation Safety Will Respond
(1) Survey the patient to determine the hazard level.
(2) Assist in the removal of radioactive implants.
(3) Supervise the removal of the patient from the room.
(4) Assist Pathology Department staff and/or Decedent Care staff in completing their tasks.