Embed Size (px)
Citation preview

DVD01 (09:10 – 09:18 / 30.11.12)
ROBOTIC VENTRAL MESH RECTOPEXY- JUDGEMENT DAY
Author(s): D Francis, C Elton, F E Rizal, B Stubbs Presenter: D Francis Institution: Barnet and Chase Farm Hospitals, UK
Aims: Laparoscopic ventral mesh rectopexy (VMR) is routinely performed for the management of rectal prolapse, rectocoele and intussusception, however it can be technically challenging due to the difficulty of suturing deep within the pelvis. Robotic surgery offers potential advantages due to articulated instruments and 3D vision, providing technical advantages. We demonstrate the robotic technique.
Methods: A robotic ventral mesh rectopexy was recorded in real time. Video footage was then edited down to 5 minutes duration, demonstrating the major steps of the procedure.
Results: The video demonstrates the robotic ventral mesh rectopexy with voiceover added to explain the relevant parts of the procedure.
Conclusion: The precision gained with the robotic assisted procedure is demonstrated and the advantages when working within the confined space of the pelvis are seen.
Key statement: Robotic VMR is technically advantageous in the pelvis, allowing for accurate dissection and suturing techniques within a small space, as shown in the video presentation.

DVD02 (09:18 – 09:26 / 30.11.12)
DVD PRESENTATION: LAPAROSCOPIC INTRAGASTRIC CYSTGASTROSTOMY
Author(s): J Bhoday, B Levy, C Pring Presenter: J Bhoday Institution: St Richard's Hospital, Chichester, West Sussex, UK
Aims: To demonstrate a novel technique for the surgical drainage of a pancreatic pseudocyst using a video demonstration of a laparoscopic intragastric cystgastrostomy in a 44 year old female patient with a 10cm x 7cm pseudocyst.
Methods: The pneumoperitoneum was created. An intragastric 12mm balloon-tip port and 5mm-port were inserted and the stomach insufflated with CO2. The pseudocyst was identified and the cyst entered with harmonic scalpel. An EGIA60 (white) stapler was used to create a cystgastrostomy. Gastrostomies were closed with 2’0 PDS.
Results: The operation took 47 minutes and the patient was discharged home within 23 hours. Unfortunately she was readmitted on day 3 post-operation with haematemesis. An upper GI endoscopy demonstrated a bleeding vessel at the port site, this was clipped and the patient subsequently discharged home without further complication.
Conclusion: This technique allows superior views and unlike traditional open drainage, the gastrostomy can be sited anywhere in the stomach without concern regarding access to the cyst. It is safe and precise and could easily be modified to remove eroded gastric bands and for the excision of gastrointestinal-stromal tumours.
Key Statement: We present an innovative technique for the safe and precise drainage of pancreatic pseudocysts that allows early discharge from hospital. The method described is also easily transferrable to other surgical procedures and provides surgeons new techniques to treat old problems.

DVD03 (09:26 – 09:34 / 30.11.12)
A LAPAROSCOPIC SURPRISE
Author(s): L Johnson, M Akhtar, S Doughan, A Hamade Presenter: L Johnson Institution: Queen Elizabeth the Queen Mother Hospital, Margate, UK
Aims: The availability of laparoscopic surgery has changed the way that idiopathic acute abdominal pain is managed in secondary care. We present an intraoperative recording of a rare case of omental infarction secondary to torsion in a virgin abdomen diagnosed and managed at laparoscopy.
Methods: A 67-year-old woman presented acutely with two days history of worsening right iliac fossa pain on the background of intermittent self-limiting abdominal pain for six months. Past medical and surgical history was unremarkable. Clinical examination revealed peritonism in the right iliac fossa with no palpable masses and normal biochemical investigations.
Results: At diagnostic laparoscopy a large haemorrhagic mass with free fluid was identified in the right side of the abdomen, adherent to omentum and small bowel. Gentle dissection revealed pedicled mass arising from the omentum. The pedicle was divided endoscopically and the mass removed.
Conclusion:The patient made an uneventful recovery and was discharged home the following day and her symptoms of intermittent abdominal pain have completely settled. Histological examination showed the mass to be omental infarction secondary to omental torsion.
Key statement: Omental torsion is a rare cause of abdominal pain and may mimic appendicitis. It typically presents with worsening right iliac fossa pain, a low-grade pyrexia and a mild leucocytosis making this almost indistinguishable from that of appendicitis based on clinical and laboratory findings.

DVD04 (09:34 – 09:42 / 30.11.12)
LAPAROSCOPIC LOW ANTERIOR RESECTION WITH INTERSPHINCTERIC DISSECTION AND COLO-ANAL ANASTOMOSIS
Author(s): N Siddiqi, M Odermatt, J Khan, A Parvaiz Presenter: N Siddiqi Institution: Portsmouth Hospitals NHS Trust, UK
Aims: To present the technique for laparoscopic ultra low anterior resection with intersphincteric dissection for rectal tumors extending up to top of anal canal without involvement of the intersphincteric plane.
Methods: The video demonstrates steps for laparoscopic ultra low anterior resection with intersphincteric dissection and colo-anal anastomosis.
Perineal dissection is performed in the beginning to assess the suitability for intersphincteric dissection. Prone position provides improved access and better views. Prospectively collected data (2006 – 2011) presented at the end of the video.
Results:
n (%)
Total Patients 62
Mean Age 66
BMI 26
Tumor Height From Anal Verge
0-2 cm
3-4 cm
5-6cm
1 (2%)
14 (22%)
47 (76%)
Length Of Stay (Median) 6 Days
R0 Resection (Curative Intent 60) 55 (91%)
Anastomotic Leak 2 (3.2%)
Mortality 0
Conclusion: Sphincter preservation is possible in larger number of patients with low rectal cancer. A highly standardized technique is required to achieve reproducible and beneficial results.
Key statement: A standardized technique of laparoscopic TME is presented with the aim to reproduce these steps independent of patient factors, such as gender, BMI or radiotherapy and to protect nerves and follow oncological principles of the TME plane.

DVD05 (09:42 – 09:50 / 30.11.12)
LAPAROSCOPIC ENTERRA PLACEMENT FOR GASTROPARESIS FOLLOWING SUBTOTAL GASTRECTOMY
Author(s): K J Dickinson, S P L Dexter Presenter: K J Dickinson Institution: St James University Hospital, Leeds, UK
Aims: The aim of this DVD presentation is to demonstrate the technique of Enterra placement following previous subtotal gastrectomy for gastroparesis, to allow neuromodulation of the remnant stomach.
Methods: We show the technique for laparoscopic Enterra placement in a patient who had previously undergone pyloromyotomy, antrectomy and subsequent subtotal gastrectomy for symptomatic gastroparesis.
Results: We demonstrate the technique of laparoscopic Enterra placement following subtotal gastrectomy.
Conclusion: Neuromodulation of the remnant stomach following multiple surgical interventions for gastroparesis can produce an excellent clinical outcome.
Key statement: Laparoscopic placement of the Enterra neuromodulation device can allow excellent symptomatic results following multiple previous surgical interventions for gastroparesis.

FP01 (11:00 – 11:10 / 30.11.12)
IS STROKE VOLUME OPTIMIZATION REALLY NECESSARY IN LAPAROSCOPIC COLORECTAL SURGERY?
Author(s): A Day, R Smith, B Fawcett, M Scott, T Rockall Presenter: A Day Institution: MATTU, Guildford, UK
Aims: There is growing evidence that goal directed fluid therapy (GDFT) improves outcome in laparoscopic colorectal surgery. NICE recommends the use of the oesophageal Doppler monitor (ODM) in major surgery. Perhaps an alternative formulaic approach to fluid administration could provide a cheap safe alternative to stroke volume optimisation.
Methods: A randomized clinical trial (NCT01128088) was conducted between 2010-2011. Patients were randomized to receive either Hartmann’s solution or 6% Volulyte as the fluid administered by GDFT with an ODM. Volumes of fluid administered to achieve stroke volume (SV) optimization prior to pneumoperitoneum were recorded.
Results: 120 patients completed the study (60 in each group). The mean amount (mls/kg) to achieve SV optimization in the 6%Volulyte group was 7.33 significantly less than the Hartmann’s group at 9.96 (<0.0005). Range of fluids (mls/kg) required to achieve SV optimization was 3.28-17.92 in the 6%Volulyte group and 3.39-20.08 in the Hartmann’s group. There was no difference in the length of stay or number of complications between the groups.
Conclusion: There is a large range of fluid required to achieve SV optimization across the cohort of patients undergoing laparoscopic colorectal surgery. It would seem that this can only be achieved adequately with the aid of GDFT.
Key statement: Optimal fluid administration in laparoscopic colorectal surgery requires an individualized goal directed approach.

FP02 (11:10 – 11:20 / 30.11.12)
THE OUTCOME OF GASTRO-OESOPHAGEAL REFLUX- RELATED RESPIRATORY MANIFESTATIONS AFTER LAPAROSCOPIC FUNDOPLICATION
Author(s): F Adaba, C Ang, A Perry, M Wadley, C Robertson Presenter: F Adaba Institution: Worcester Royal Infirmary, UK
Aims: Patients with refractory respiratory symptoms related to gastro-oesophageal reflux disease (GORD), such as asthma, hoarseness and cough are being referred for laparoscopic fundoplication (LFP), as recommended by the Society of American Gastrointestinal and Endoscopic Surgeons. However, there are limited data regarding symptomatic response to fundoplication in this group of patients.
Methods: A retrospective review was performed to study the efficacy of LFP in the treatment of all patients with chronic respiratory manifestations of GORD in a 7 year period at a single hospital. Patients were followed up in clinic at 4-6 weeks (short-term) and 6-12 months (long-term) post-operatively.
Results: Of 208 patients who underwent LFP, 73(35%) were eligible for inclusion in the study. 55(75%) had improved respiratory symptoms in the short-term. In the long-term, 7 patients had symptom recurrence, whilst 4 patients had symptomatic improvement not initially apparent. 190(91%) of 208 patients had GOR symptoms improvement at short-term follow-up.
Conclusion: LFP is effective in the control of respiratory manifestations of GORD with symptom response of 75%, compared to 91% response rate in the control GOR symptoms alone. More research is needed to identify pre-operative factors to aid patient selection to further improve symptom response rates.
Key statement: Laparoscopic fundoplication is effective in treating patients with intractable chronic respiratory manifestations as a primary symptom of gastro-oesophageal reflux disease. Currently, the response rate of this intervention is not as successful for the relief of symptoms of gastro-oesophageal reflux alone.

FP03 (11:20 – 11:30 / 30.11.12)
SINGLE STAGE MANAGEMENT OF GALLSTONE PANCREATITIS IN THE LAPAROSCOPIC ERA. DO WE NEED MRCP OR ERCP?
Author(s): A Mirza, S Zino, K Nassar, V Geoff, A Nassar Presenter: A Mirza Institution: Monklands Hospital, Airdrie, UK
Aims: The surgical management of uncomplicated acute gall stone pancreatitis is controversial. Most centres prefer a pre-operative MRCP and ERCP to diagnose and treat gallstone pancreatitis. Our aim was to evaluate the outcome of patients undergoing laparoscopic biliary surgery at a specialist biliary unit.
Methods: Prospectively collected data for patients undergoing laparoscopic biliary surgery over 20 years (N=3361) was analysed. We reviewed the data for patients who had surgery for gallstone pancreatitis.
Results: Total of 218 patients were identified. Mean age was 51 years (range, 14 to 82 years). 74% (n=160) were female patients. Major symptoms were chronic biliary pain (N=33, 15%) and jaundice (N= 92, 42%). Ultrasound identified common bile duct stones (CBD) in 33% (N= 72) of patients. IOC demonstrates biliary tree stones in the cystic duct 22% (N=47) and common bile duct 36% (N=78) and were removed laparoscopically. The average surgical time was 85 mins (range 22 to 570 mins). The average in hospital stay was 5 days (range 1-28 days). The major post-operative complications were aspiration pneumonia (N=1) and acute renal failure (N=1). Nine (4%) patients were readmitted with abdominal pain (N=7), cholangitis (N=1) and gastroenteritis (N=1).
Conclusion: One–session management of pancreatitis is preferable cost effective and safer than staged management. Routine IOC can identify CBD stones. In laparoscopic era preoperative MRCP and ERCP are not routinely indicated.
Key statement: The patients diagnosed with uncomplicated gall stone pancreatitis should be managed with routine intraoperative cholangiography and laparoscopic common bile duct exploration if indicated.
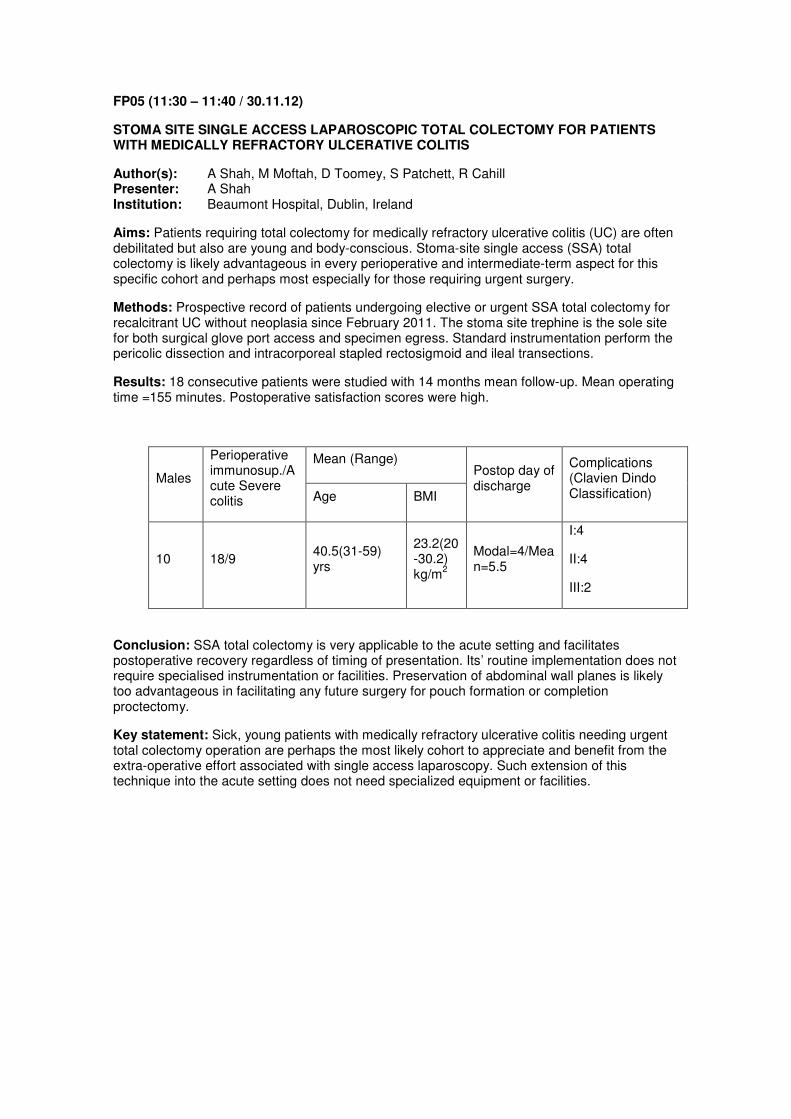
FP05 (11:30 – 11:40 / 30.11.12)
STOMA SITE SINGLE ACCESS LAPAROSCOPIC TOTAL COLECTOMY FOR PATIENTS WITH MEDICALLY REFRACTORY ULCERATIVE COLITIS
Author(s): A Shah, M Moftah, D Toomey, S Patchett, R Cahill Presenter: A Shah Institution: Beaumont Hospital, Dublin, Ireland
Aims: Patients requiring total colectomy for medically refractory ulcerative colitis (UC) are often debilitated but also are young and body-conscious. Stoma-site single access (SSA) total colectomy is likely advantageous in every perioperative and intermediate-term aspect for this specific cohort and perhaps most especially for those requiring urgent surgery.
Methods: Prospective record of patients undergoing elective or urgent SSA total colectomy for recalcitrant UC without neoplasia since February 2011. The stoma site trephine is the sole site for both surgical glove port access and specimen egress. Standard instrumentation perform the pericolic dissection and intracorporeal stapled rectosigmoid and ileal transections.
Results: 18 consecutive patients were studied with 14 months mean follow-up. Mean operating time =155 minutes. Postoperative satisfaction scores were high.
Males
Perioperative immunosup./Acute Severe colitis
Mean (Range) Postop day of discharge
Complications (Clavien Dindo Classification) Age BMI
10 18/9 40.5(31-59) yrs
23.2(20-30.2) kg/m
2
Modal=4/Mean=5.5
I:4
II:4
III:2
Conclusion: SSA total colectomy is very applicable to the acute setting and facilitates postoperative recovery regardless of timing of presentation. Its’ routine implementation does not require specialised instrumentation or facilities. Preservation of abdominal wall planes is likely too advantageous in facilitating any future surgery for pouch formation or completion proctectomy.
Key statement: Sick, young patients with medically refractory ulcerative colitis needing urgent total colectomy operation are perhaps the most likely cohort to appreciate and benefit from the extra-operative effort associated with single access laparoscopy. Such extension of this technique into the acute setting does not need specialized equipment or facilities.

FP05 (11:40 – 11:50 / 30.11.12)
LAPAROSCOPIC OESOPHAGEAL RESECTION AND ENHANCED RECOVERY AFTER SURGERY (ERAS)
Author(s): P Daliya1, David Humes
2, Simon Parsons
1, Neil Welch
1, James Catton
1
Presenter: P Daliya Institution:
1Department of Surgery, Nottingham City Hospital, UK,
2Nottingham Digestive
Disease Centre and Biomedical Research Unit, Queen's Medical Centre, Nottingham, UK
Aims: Surgical resection for oesophageal malignancy is associated with high mortality and morbidity. Laparoscopic resection and ERAS pathways have reduced length of stay in other surgical specialties. We implemented laparoscopic resection and an ERAS pathway in 2009 following oesophageal resection and aimed to assess the impact of this on standard outcomes.
Methods: An electronic review of a prospectively collected database was performed. Data was collected on mortality, morbidity and length of stay before (01/07/2007-31/07/2009) and after (01/08/2009-31/08/2011) the implementation of the ERAS pathway. The pathway included increased use of laparoscopic surgery and a standard pre and post operative care package.
Results: 57 and 101 oesophagectomies were undertaken (5 and 50 laparoscopically). There was no increase in hospital mortality or overall morbidity despite a significant reduction in length of stay (16 to 11 days, <0.0001). Those patients having neo-adjuvant therapy who had a major complication were less likely to receive adjuvant chemotherapy (<0.02).
Conclusion: Our study demonstrates that laparoscopic and open oesophageal resection can be undertaken in an ERAS pathway and results in a significant reduction in length of stay. If the post-operative course is complicated by a major complication (Clavien-Dindo, >grade II) patients are less likely to receive adjuvant chemotherapy.
Key statement: The implementation of a laparoscopic resection with an ERAS pathway for patients undergoing major oesophageal resections can have a significant reduction in the length of post-operative stay without any associated increase in hospital mortality.

FP06 (14:20 – 14:30 / 30.11.12)
A NATIONAL AUDIT OF ANTIBIOTIC PROPHYLAXIS IN ELECTIVE LAPAROSCOPIC CHOLECYSTECTOMY
Author(s): H Graham1,4
, A Vasireddy2,4
, A Rhodes1,4
, D Nehra3
Presenter: H Graham Institution:
1Kings College Hospital NHSFT, London, UK,
2Guy's & St. Thomas' NHSFT,
London, UK, 3Epsom & St. Helier NHS Trust, London, UK,
4London Deanery,
UK
Aims: To assess current practice across laparoscopic surgeons in Great Britain & Ireland for antibiotic prophylaxis in elective laparoscopic cholecystectomy.
Methods: Data was collected on routine use of antibiotics in elective laparoscopic cholecystectomy; and how that was influenced by factors such as bile spillage, patient co-morbidities and surgeons’ experience. An online questionnaire was sent to 493 laparoscopic surgeons in December 2011.
Results: Data was received from 111 surgeons (87 Consultants) representing over 7000 cases/yr. In routine cases without bile spillage 64% gave no antibiotics and 36% a single dose. In cases with bile spillage 11% of clinicians gave no antibiotics, however 80% gave one dose & 7% three doses.
Conclusion: The only national antibiotic guidelines in the UK are from the Scottish Intercollegiate Guideline Network; these state that antibiotics should only be considered in high risk patients. There is overuse of antibiotics in uncomplicated elective laparoscopic cholecystectomy.
Antibiotic overuse increases the risk of adverse reactions and development of resistance. Over 20,000 doses of antibiotics, amounting to £100,000 could be saved annually if surgeons modified their practice to follow evidence based guidelines.
Key statement: Online survey responses, representing 7,500 of 60,000 procedures/yr performed nationwide, showed >20,000 doses of antibiotics could be saved annually, if surgeons follow evidence based guidelines. In routine cases and cases with bile spillage 64% and 80% of clinicians respectively follow guidelines. This is independent of seniority and annual caseload.
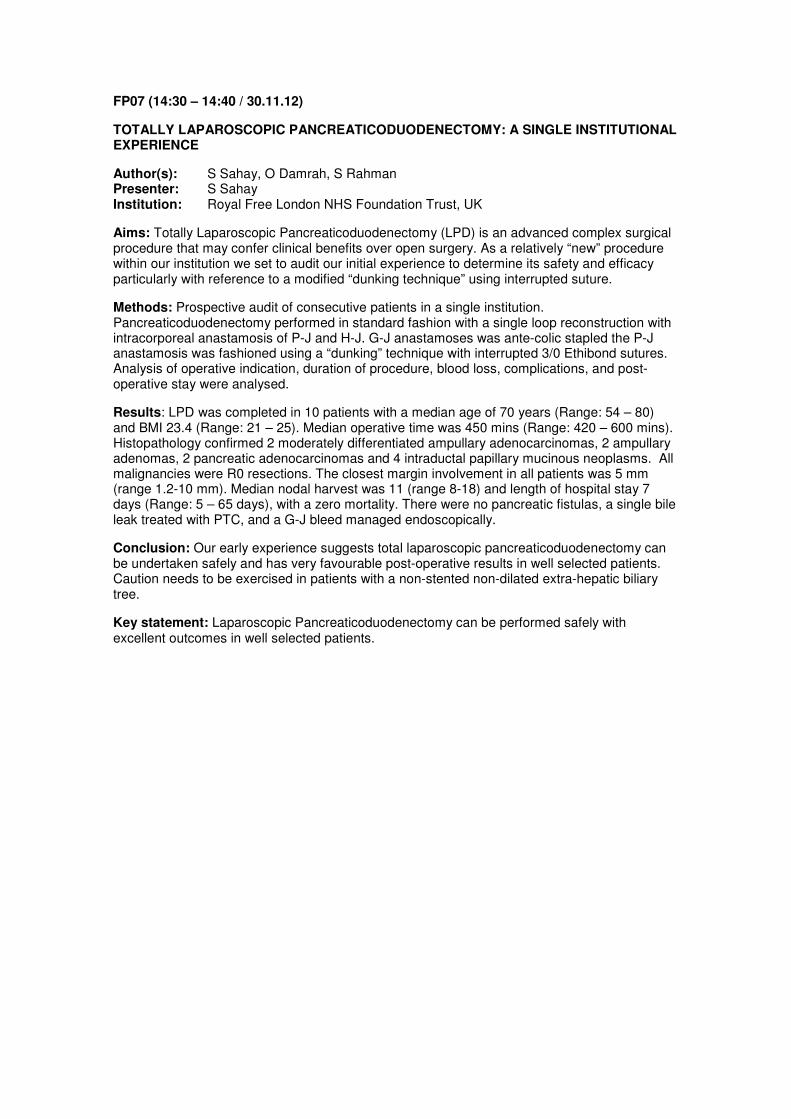
FP07 (14:30 – 14:40 / 30.11.12)
TOTALLY LAPAROSCOPIC PANCREATICODUODENECTOMY: A SINGLE INSTITUTIONAL EXPERIENCE
Author(s): S Sahay, O Damrah, S Rahman Presenter: S Sahay Institution: Royal Free London NHS Foundation Trust, UK
Aims: Totally Laparoscopic Pancreaticoduodenectomy (LPD) is an advanced complex surgical procedure that may confer clinical benefits over open surgery. As a relatively “new” procedure within our institution we set to audit our initial experience to determine its safety and efficacy particularly with reference to a modified “dunking technique” using interrupted suture.
Methods: Prospective audit of consecutive patients in a single institution. Pancreaticoduodenectomy performed in standard fashion with a single loop reconstruction with intracorporeal anastamosis of P-J and H-J. G-J anastamoses was ante-colic stapled the P-J anastamosis was fashioned using a “dunking” technique with interrupted 3/0 Ethibond sutures. Analysis of operative indication, duration of procedure, blood loss, complications, and post-operative stay were analysed.
Results: LPD was completed in 10 patients with a median age of 70 years (Range: 54 – 80) and BMI 23.4 (Range: 21 – 25). Median operative time was 450 mins (Range: 420 – 600 mins). Histopathology confirmed 2 moderately differentiated ampullary adenocarcinomas, 2 ampullary adenomas, 2 pancreatic adenocarcinomas and 4 intraductal papillary mucinous neoplasms. All malignancies were R0 resections. The closest margin involvement in all patients was 5 mm (range 1.2-10 mm). Median nodal harvest was 11 (range 8-18) and length of hospital stay 7 days (Range: 5 – 65 days), with a zero mortality. There were no pancreatic fistulas, a single bile leak treated with PTC, and a G-J bleed managed endoscopically.
Conclusion: Our early experience suggests total laparoscopic pancreaticoduodenectomy can be undertaken safely and has very favourable post-operative results in well selected patients. Caution needs to be exercised in patients with a non-stented non-dilated extra-hepatic biliary tree.
Key statement: Laparoscopic Pancreaticoduodenectomy can be performed safely with excellent outcomes in well selected patients.

FP08 (14:40 – 14:50 / 30.11.12)
LAPAROSCOPIC VERSUS OPEN SUBTOTAL COLECTOMY FOR INFLAMMATORY COLITIS: A CASE MATCHED STUDY COMPARING EARLY POST OPERATIVE OUTCOMES
Author(s): C Parnaby, G Ramsay, N Hope, C Macleod, T McAdam Presenter: C Parnaby Institution: Aberdeen Royal Infirmary, UK
Aims: To compare early post operative outcomes for patients with inflammatory colitis (IC) refractory to medical treatment undergoing laparoscopic (lap) versus open subtotal colectomy (STC).
Methods: 39 consecutive patients with IC undergoing lap STC (2006 – 2012) were identified. 31 patients were matched for age (within 10years), gender, ASA grade, operative classification and preoperative medical treatment with patients undergoing open STC (2005 – 2012). 30 day post operative complications were reported using the Clavien-Dindo (CD) classification (I – V)[minor:CDI-II, major CDIII-V]. Post operative stay and 30 day readmission rates were also reported.
Results: The median total anaesthetic time was longer for lap STC compared to open STC (225mins[IQR210-270]vs150mins[120-180],<0.005). Lap STC resulted in lower intraoperative blood loss compared to open STC (100mls[IQR5-150] vs400mls[100-675]). 2 patients required conversion in the laparoscopic group due to bleeding. Early post operative outcomes are summarised below:
Laparoscopic (n=31) Open (n=31) value
Overall CD complications
CD Minor
CD Major
30
26
4
35
26
8
0.830
1.000
0.335
Post op stay
(days, median [IQR])
7 (6-12) 11 (7-18) 0.145
Readmission 6 8 0.762
Conclusion: In this case matched study, overall complications were high and comparable between operative groups. Laparoscopic STC was associated with longer operating times but less blood loss. There was also a non significant trend towards a shorter hospital stay and reduced major complications.
Key statement: Patients undergoing subtotal colectomy for inflammatory colitis are associated with high morbidity. In this case matched study overall complication rates were comparable between operative groups. Laparoscopic subtotal colectomy was associated with longer operating times but reduced blood loss. There was also a non-significant trend towards shorter hospital stay and reduced major complications.
FP09 (14:50 – 15:00 / 30.11.12)
DOES LAPAROSCOPIC VS. OPEN COLORECTAL SURGERY HAVE AN IMPACT ON THE SUBSEQUENT LAPAROSCOPIC TREATMENT OF LIVER METASTASIS?
Author(s): F Di Fabio2, E Dimovska
1, H Alsaati
1, N Pearce
1, M Abu Hilal
1
Presenter: F Di Fabio Institution:
1Colorectal Surgery, University Hospital Southampton, UK,
2Hepatobiliary and
Pancreatic Surgery, University Hospital Southampton, UK
Aims: Laparoscopic liver surgery (LLS) for colorectal liver metastases (CRLM) is rapidly expanding. It is still unexplored whether the surgical trauma induced by open colorectal surgery may influence the subsequent laparoscopic management of CRLM.
Methods: This is a retrospective study from a tertiary referral university hospital. Consecutive patients undergoing LLS for CRLM where analyzed with respect to the previous approach adopted for the resection of the primary colorectal tumour (laparoscopic vs. open).
Results: One-hundred and five patients were included. Seventy-nine (75%) had previous open and 26 (25%) had laparoscopic colorectal resection. Postoperative length of stay (LoS) after LLS was a median of 4 days for patients who had laparoscopic colectomy and 5 days for those who had open colectomy (=0.053). Complication rates after LLS were 14/79 (18%) and 3/26 (12%) for patients who had open and laparoscopic colectomy, respectively (=0.554). Laparoscopic major hepatectomy was performed in 40 (38%) patients. In this group, intraoperative blood loss was significantly higher in patients who had previous open vs. laparoscopic colectomy (median 750ml vs. 400 ml; =0.005). Multivariate logistic regression analysis showed that blood loss >300ml was 4 times less likely to happen in patients who had previous laparoscopic colectomy vs. open colectomy (=0.015).
Conclusion: Adhesions induced by open colorectal surgery may cause substantial difficulties for the laparoscopic management of subsequent liver metastases. Laparoscopic colorectal surgery may maximize the advantages of minimally-invasive liver surgery, particularly for major hepatectomy.
Key statement: The laparoscopic approach for colorectal surgery may have a long-term impact on the laparoscopic treatment of liver metastases. A completely minimally-invasive management of the colorectal cancer primary and liver metastases should be implemented.

FP10 (15:00 – 15:10 / 30.11.12)
CROSS-OVER TRIAL OF THREE-DIMENSION VS. TWO-DIMENSION VISION SYSTEMS FOR ADVANCED LAPAROSCOPIC SKILLS IN SURGICAL TRAINEES
Author(s): W Elbakbak1,2
, B S Alaraimi2,3
, S J Sarker1,2
, R G Goriparthi2, B Patel
1,2
Presenter: W Elbakbak Institution:
1Barts Cancer Institute, London, UK,
2Queen Mary University of London, UK,
3Royal London Hospital, UK
Aims: To objectively evaluate and compare surgical trainee’s performances in laparoscopic intracorporeal suturing using 2D and 3D vision systems in terms of performance times, number of repetitions and errors on a box trainer.
Methods: 24 core surgical trainees randomised to 3D and 2D imaging systems performed laparoscopic intracorporeal suturing according to the validated fundamentals of laparoscopic surgery (FLS) curriculum until task proficiency is achieved. The trainees were swapped to the other vision system one week later in a cross-over design and repeated the same task.
Results: The task was completed in 39% less time under the 3D group than the 2D group.
Vision System 3D 2D
Median (range) Median (range) P value
Time to reach proficiency (min) 36 (14-132) 59 (12-239) 0.37
Number of repetitions 16 (6-16) 22 (7-62) 0.042
Accuracy errors 4 (0-8) 5.5 (0-25) 0.05
Error score 9 (0-82) 49 (2-122) 0.05
Conclusion: Three-dimensional vision allows for significant improvement in performance times and error rates compared to the two-dimensional vision while performing complex laparoscopic skills such as intracorporeal suturing.
Key statement: Three-dimensional vision allows for significant improvement in performance times and error rates compared to the two-dimensional vision while performing complex laparoscopic skills such as intracorporeal suturing.

P01
POST–OPERATIVE OUTCOMES FOLLOWING COLORECTAL CANCER SURGERY IN THE ELDERLY: A COMPARISON OF LAPAROSCOPIC AND OPEN SURGERY
Author(s): M Wyn-Williams, M Monteiro, K Bowling, R Harries, A Lala Presenter: M Wyn-Williams Institution: Ysbyty Gwynedd, Bangor, UK
Background: Elderly patients have a high incidence of colorectal cancer, and with our ageing population the number of elderly patients undergoing colorectal cancer (CRC) procedures will significantly increase. Although laparoscopic surgery has international acceptance for CRC, there has been little evidence focusing on its use in patients aged over 75 years.
Aims: The aim of this study was to assess the post-operative outcomes comparing laparoscopic with open surgery in elderly patients undergoing CRC surgery.
Methods: We performed a retrospective review of our prospectively maintained database, from 2008-2011, of all patients aged over 75 who had under went either laparoscopic or open CRC surgery. Anal cancers and emergency surgery were excluded from our analysis. Demographic data, post-operative length of stay, complications and 30 day mortality were recorded.
Results: 62 cases were laparoscopic and 102 open.
Median length of stay was 8 days for laparoscopic vs. 13 days for open (=0.0013). Anastomotic leak rate was 1.6% and 4.9% in the laparoscopic and open groups respectively (=0.4102); wound infection was 6.4% in the laparoscopic group and 0.9% in the open group (=0.0682).
Conclusion: Our study showed that laparoscopic surgery has a statistically significantly shorter post-operative length of stay compared to open surgery, with no difference in 30 day mortality and complication rate. Laparoscopic CRC surgery has been shown to be safe and have significant benefits within the elderly population.
Key statement: Although laparoscopic surgery has international acceptance for Colorectal Cancers, there has been little evidence focusing on its use in patients aged over 75 years. A prospectively maintained database was analysed retrospectively for patients in 2008-2011 undergoing open and laparoscopic surgery analysing their outcomes.
P02
LAPAROSCOPIC PORT SITE HERNIA: ARE WE CONSENTING ADEQUATELY?
Author(s): M I Aslam, A Penshon, C Tully, I Ahmad, R Farrell Presenter: M I Aslam Institution: Queen Elizabeth Hospital, Gateshead, UK
Aims: To assess adequacy of consenting for occurrence of port site hernia following laparoscopic surgical procedures.
Methods: An audit was designed to assess for port site hernia in consents. As proof of principle, a pilot project has been completed that included random assessment of 43 consents by various grades and for various Laparoscopic procedures.
Results: Of the 43 consents examined, 24 were for patients undergoing laparoscopic cholecystectomy, 12 for laparoscopic bowel resection and 7 for laparoscopic appendicectomy. Port site hernia was consented for in only 12 out of 43 patients (27%).
Conclusion: The incidence of port site hernia varies though has been reported to be around 1.7% after laparoscopic cholecystectomy. Patients undergoing laparoscopic surgical procedures should be routinely informed of the risks of port site hernia when being consented for such procedures. Our pilot data demonstrates that only 27% of patients were consented for this.
Key statement: Port-site hernia is a rare though important and potentially serious complication of laparoscopic surgery. Patients undergoing laparoscopic surgery should be routinely informed of the risks of port site hernia when being consented for these procedures.
P03
SURGEON ADMINISTERED, LAPAROSCOPICALLY GUIDED TAP BLOCK: A NEW TOOL FOR THE LAPAROSCOPIC SURGEON?
Author(s): C Magee1,2
, S Graham1,3
Presenter: C Magee Institution:
1Antrim Area Hospital, UK,
2Royal Victoria Hospital, Belfast, UK,
3Mater
Infirmorum, Belfast, UK
Aims: Sensory nerves to the abdominal wall traverse the neurovascular plane between internal oblique and transversus abdominis. Placement of local anaesthetic in this plane (TAP block) is an established technique for abdominal surgery. This study aims to investigate the feasibility of using a laparoscopically guided TAP block for laparoscopic cholecystectomy (LC).
Methods: Right subcostal TAP block was administered under laparoscopic vision at the beginning of surgery (30ml chirocaine 2.5%) by a single surgeon. Pain VNRS and length of stay were recorded. Results were compared to patients who had usual care - wound infiltration (WI) at the end of surgery (20ml chirocaine 2.5%).
Results: Ten patients had successful TAP blocks, with one exclusion (converted to open). No complications or technical difficulties were encountered. Mean pain score at 4 hours was 2.06 (range 0-5) compared to 5.38 (range 5-7) after WI. Length of stay was 29.1 hours (TAP) versus 36 hours (WI).
Conclusion: This observational study shows that surgeon administered, laparoscopically guided TAP block, as part of a multi-modal regimen for laparoscopic cholecystectomy, is feasible and provides reliable post-operative analgesia. The low pain scores achieved could facilitate earlier discharge, improving daycase LC rates. Further study is required to establish efficacy.
Key statement: Adequate pain control is an essential component of safe discharge criteria for daycase surgery. The observed pain scores after laparoscopic TAP block could facilitate earlier fulfilment of discharge criteria, improving rates of same day discharge after LC.

P04
PAIN AND COSMESIS FOLLOWING FOUR-PORT LAPAROSCOPIC CHOLECYSTECTOMY; THE PATIENT VIEW
Author(s): M Patel, A Dennison, A Buchanan, C Neal, M Metcalfe, G Garcea Presenter: M Patel Institution: University Hospitals of Leicester, Department of Hepatobiliary & Pancreatic Surgery, UK
Aims: Standard 4-port laparoscopic cholecystectomy (SLC) is presently the gold standard in gallbladder surgery. The introduction of single incision laparoscopic cholecystectomy (SILC) is said to offer potential improvements in pain and cosmesis post-operatively. This study surveyed patient satisfaction at each of their port-sties following uncomplicated 4-port cholecystectomy.
Methods: Retrospective postal questionnaire poll of 100 patients aged between 18 and 82. A ten point visual analogue score was used to asses post-operative pain at each respective port-site. A similar scale was used to assess cosmetic satisfaction relating to scar colour, stiffness, thickness and irregularity. Patients were asked to report port site infection and also whether or not they would prefer a single incision operation based on their experience of the standard 4-port technique.
Results: Fifty nine patients returned their questionnaires (59% response rate). The median pain scores were highest at the umbilical port-site and the epigastric port site collectively had the worst cosmetic outcome in terms of satisfaction with scar colour, stiffness, thickness and irregularity. Port site infections were only reported at the site of gallbladder retrieval (epigastric port). 79.7% of patients were satisfied with the four-port procedure and only 20.3% would have preferred a single-port operation if given the option.
Conclusion: Patient satisfaction with standard 4-port cholecystectomy is high. The umbilical port was consistently the most painful post-operatively, with cosmesis scores being worst for the epigastric port site. However, there is no firm data that would support SILC over SLC based on this evidence.
Key statement: The single incision laparoscopic cholecystectomy (SILC) is said to offer potential improvements in pain and cosmesis post-operatively<b>. </b> This study surveyed patient satisfaction at each of their port-sties following standard 4-port cholecystectomy (SLC). Our results show high patient satisfaction with the SLC with little evidence to support the SILC over the SLC.

P05
IMPROVING OUTCOMES IN LAPAROSCOPIC APPENDICECTOMY
Author(s): E Dinneen, T Tillmann, J Preston, R Navaratnam, M Nair Presenter: E Dinneen Institution: North Middlesex University Hospital, London, UK
Aims: To identify modifiable pre-operative and operative variables in patients undergoing emergency Laparoscopic Appendicectomy (LA) with a view to improving future outcomes. Our study spans a period during which the laparoscopic approach appendicectomy became increasingly popular in our hospital.
Methods: Two independent assessors identified all emergency LAs between March 2007 and January 2012 using hospital coding data and theatre records. Comprehensive admission and operative variables were captured from medical records and operation notes including laparoscopic technique (endoloop vs. endoGIA). Outcome data analyzed included post-operative complications, readmissions and length of post-operative stay.
Results: One hundred and seven LAs were identified. For patients whose intra-operative findings denoted acute, uncomplicated appendicitis, the use of endoGIA to transect the appendix base was associated with shorter post-operative inpatient stay, 35 hours (95% CI 15 to 55) vs. 59.7 hours (95% CI 20.2 to 99.2; <0.05) using endoloop.
Conclusion: In acute uncomplicated appendicitis, use of endoGIA significantly reduced length of post-operative inpatient stay in comparison to endoloop. There was no statistical difference in post-operative inpatient stay between endoGIA and endoloop techniques when LA was performed on complicated appendicitis, or when there was no evidence of appendicitis.
Key statement: EndoGIA is more expensive than endoloop, £200 vs. £2. However, this study finds these costs can be offset by shortening the inpatient post-operative stay by 24 hours, valued a £240 in our hospital. Therefore, when acute, uncomplicated appendicitis is identified during LA, endoGIA should be considered to optimise pot-operative outcome.

P06
TAP BLOCKS IN LAPAROSCOPIC SURGERY: A REVIEW OF THE EVIDENCE
Author(s): C Magee Presenter: C Magee Institution: Royal Victoria Hospital, Belfast, UK
Aims: To establish and appraise the evidence base for the use of TAP blocks in the management of postoperative pain after laparoscopic surgery.
Methods: Electronic database searches were performed to identify studies of the use of TAP blocks in adults undergoing laparoscopic abdominal surgery. Opinion pieces and studies available only in abstract form were excluded. Outcomes considered were opioid consumption, postoperative pain scores, length of stay and adverse events.
Results: Eight relevant studies were identified, 3 systematic reviews (laparoscopic and open procedures), 3 RCTs (2 laparoscopic cholecystectomy, 1 daycase gynae laparoscopy) and 2 retrospective studies (laparoscopic hysterectomy and colorectal surgery). Significant reduction in opioid consumption was shown in 7, other outcomes favoured TAP blocks over usual care.
Conclusion: The review found statistically significant opioid sparing, with a tendency to lower pain scores after TAP block. Results for length of stay are suggestive of a positive effect. Heterogeneity of primary studies limits generalisability, procedure specific trials and cost-analysis studies are required.
Key statement: Laparoscopic surgery is expanding and appropriate management of postoperative pain is an essential component in facilitating recovery and safe discharge. A regional blockade, such as TAP block, may bridge the gap between wound infiltration with LA and neuraxial techniques reducing opioid consumption and associated adverse effects.

P07
LAPAROSCOPIC OR OPEN LIVER RESECTION? LET SYSTEMATIC REVIEW DECIDE IT
Author(s): A Rao, I Ahmed, G Rao Presenter: A Rao Institution: University of Aberdeen, UK
Aims: Laparoscopic liver resection is increasingly being used for the excision of benign and malignant hepatic lesions. The aim of this study was to perform meta-analysis on the compiled data from available observational studies. Methods: All the studies comparing laparoscopic versus open liver resections were searched on the available databases. Data were analyzed using Review Manager software version 5.0 (The Cochrane Collaboration, Software Update, Oxford, UK). Results: There was a total of 2,466 patients: 1,161 (47.1%) in the laparoscopic group and 1,305 (52.9%) in the open group. The laparoscopic group was associated with a reduced overall complication rate (odds ratio = .35; 95% confidence interval [CI], .28-.45; P < .001; heterogeneity (HG): P = .51), fewer positive resection margins for malignant tumour resections (odds ratio = .38; CI, .20-.76; P = .006; HG: P = .52) and a decrease in the number of patients requiring blood transfusion (odds ratio = .36; CI, .23-.74; P = .001; HG: P = .30). Conclusion: Laparoscopic liver resection showed a reduced overall morbidity rate and favourable and comparable outcomes when compared with the open group. However, there is still a need for randomized controlled trials to compare laparoscopic versus open hepatic resection in benign and malignant lesions.
Key statement: Laparoscopic liver resection showed a reduced overall morbidity rate and favorable and comparable outcomes when compared with the open group.

P08
THE OPTIMAL POSTOPERATIVE ANALGESIA TO REDUCE LENGTH OF STAY IN LAPAROSCOPIC COLORECTAL SURGERY
Author(s): A Day, B Levy, R Smith, B Fawcett, M Scott, T Rockall Presenter: A Day Institution: MATTU, Guildford, UK
Aims: Laparoscopic colorectal surgery in combination with an enhanced recovery programme can achieve reduced length of stays. The optimal postoperative analgesia is not yet clear. We aim to identify whether patients receiving spinal or patient controlled analgesia (PCA) have a shorter length of stay.
Methods: Two RCT’s (NCT 18926278 and 01128088) were conducted between 2007-2011 at one institution. Patients underwent laparoscopic colorectal surgery within an enhanced recovery programme with goal directed fluid therapy. Patients that were randomly assigned to either spinal or PCA analgesia had patient characteristics and lengths of stay analysed.
Results: 181 patients were analysed (spinal n=91, PCA n=90). There was no significant difference for age, ASA classification, BMI, POSSUM, operative time, diagnosis or type of operation. There was no difference in median length of stay measured from the end of operation, however significantly more patients were discharged on an earlier postoperative day in the spinal group (=0.019). The spinal group had significantly earlier return of bowel function (=0.016) and reduced complications (=0.008).
Conclusion: Spinal postoperative analgesia in patients undergoing laparoscopic colorectal surgery within an enhanced recovery programme have an earlier return of bowel function, reduced complications and are likely to be discharged on an earlier postoperative day.
Key statement: Spinal analgesia appears to provide greater benefits in terms of reduced length of stay, complications and earlier bowel function compared to PCA analgesia.<b></b>

P09
SCOTTISH POPULATION PREFERENCES FOR ADVANCED UROLOGICAL TECHNIQUES: A GUIDE TO FUTURE SURGICAL DEVELOPMENTS?
Author(s): A Rao1, M Anwar
1, M Rashid
1, B Somani
2, I Ahmed
2, N Cohen
1, S McClinton
1
Presenter: A Rao Institution:
1University of Aberdeen, UK,
2Aberdeen Royal Infirmary, UK
Aims: Two novel minimally invasive surgical techniques, Natural Orifice Transluminal Endoscopic Surgery (NOTES) and Laparo-Endoscopic Single Site Surgery (LESS) are undergoing rapid development to reduce complications historically associated with open surgery. Our study aimed to analyse Scottish public preferences regarding these new surgical techniques in the hope that this would help inform future development and resource allocation in urological surgery.
Methods: A questionnaire based survey was carried out with members of the general public in North East Scotland. The survey consisted of four questions about surgery in two hypothetical scenarios of kidney disease, and was designed to identify whether the concepts of innovative techniques were acceptable to the general population.
Results: A total of 500 participants took part in the study from a wide variety of social backgrounds. 59% and 47.4% of participants would accept LESS or NOTES for kidney cancer and non-functioning kidney hypothetical scenarios respectively. LESS was highest ranked option (rank mean value 2.0 [kidney tumour] and 1.89 [non-functioning kidney]).
Conclusion: Of the newer surgical techniques LESS was more preferred than NOTES. The general public more readily accepted the concept of LESS as it was seen as a further development of previously established laparoscopic surgical techniques.
Key statement: A questionnaire based survey was designed to identify whether the concepts of innovative techniques were acceptable to the general population in North East Scotland. The concept of Laparo-Endoscopic Single Site (LESS) Surgery was more readily accepted. It was seen as a further development of previously established laparoscopic surgical techniques.

P10
DO WE REALLY NEED ROUTINE GROUP AND SAVE ON THE MORNING OF SURGERY FOR PATIENTS UNDERGOING LAPAROSCOPIC CHOLECYSTECTOMY?
Authors: N Hamza, M Pereira, A Gilliam Presenter: N Hamza Institution: Darlington Memorial Hospital, UK
Aims: Group and save (G&S) obtained during pre-assessment clinic prior to laparoscopic cholecystectomy (LC) is valid for 5 days hence is repeated on the day of LC. The aim of this study was to establish whether there is a requirement for this sample to be taken on the day of LC. Methods: All LC cases carried out at our Trust were sought from the clinical coding department. The electronic records of 1000 patients (November 2009 to March 2011) were reviewed to identify the patients who were issued with and received blood products. Results: 11/1000 (1%) patients received transfusion; mean (range) interval between the postoperative bleeding and transfusion was 35 (3-240) hours. In nearly 50% of the cases another sample was sent despite the routine G&S still being valid. 89/1000 (9%) patients had one or more sample rejected, while 4% had no valid G&S.
Conclusion: The G&S sent on the day of LC is unnecessary. Significant cost savings (£ 13,280 per annum) can be achieved. An increase in the O-ve reserve stock may be required as a “safety net”. G&S samples should still be checked at pre-assessment to exclude atypical antibodies.
Key statement: Only 1% of this patients' group required blood transfusion post LC. The routine preoperative ‘group and save' sample on the day of LC didn't alter the management of postoperative bleeding hence is not required. Alternative approaches to achieve financial savings without compromising patients' safety should be implemented.

P11
TAP BLOCK VS LOCAL WOUND INFILTRATION FOLLOWING LAPAROSCOPIC COLORECTAL RESECTION: A SINGLE CENTRE EXPERIENCE
Author(s): A Oomman1, S Gurung
2, S Gunasekaran
2, A Anter
2, J Mathias
2
Presenter: A Oomman Institution:
1University Hospital Wales, Cardiff, UK,
2Withybush General Hospital,
Haverfordwest, UK
Aims: To assess the efficacy of TAP block Vs Local wound infiltration following Laparoscopic Colorectal Surgery.
Breakthrough pain treated with Opiods can have a detrimental effect on bowel function, cause nausea and vomiting which ultimately results in delayed recovery. The optimal postoperative analgesia following Laparoscopic Colorectal Surgery is yet undetermined.
Methods: 75 Laparoscopic resections performed by a single surgeon between June2010 and March2012 was analysed retrospectively. Notes were divided into TAP block and local infiltration based on post-operative analgesia used. Primary outcome of interest was total morphine usage over 48hrs. Secondary outcome of interest was pain score and length of stay.
Results: TAP block was used in 33/75 (44%) cases, LA was used in 42/75 (56%). Total morphine usage was 20.5 mg/48hrs for the TAP group and 33.5mg/48hrs in LA. Length of stay in hospital was 2.9 days following TAP and 3.8 days following LA. 78% following TAP block reported minimal pain.
Conclusion: Overall 48hr morphine consumption, pain score and hospital stay was significantly reduced in the patients who had the TAP block when compared to LA infiltration. We are currently in the process of beginning a Randomised controlled trial at our centre to compare the efficacy TAP block Vs local infiltration.
Key statement: TAP block provides better post-operative pain relief which means there is a reduced intake of morphine. This negates the side-effects of opiods resulting in quicker recovery of patients and overall length of stay.

P12
ROBOTIC VENTRAL MESH RECTOPEXY: RISE OF THE PELVIC FLOOR
Author(s): F E Rizal, B Stubbs, C Elton, D Francis Presenter: F E Rizal Institution: Barnet and Chase Farm Hospital, UK
Aims: Laparoscopic ventral mesh rectopexy (VMR) is becoming the operation of choice for the management of rectal prolapse, rectocoele and intussusception, but may be technically challenging. Robotic surgery has advantages as the articulated instruments allow accurate dissection and suturing in a confined space. We describe our experience of the robotic technique.
Methods: Prospective data for all robotic VMRs performed from November 2011 to date were included. The operation was performed using a Da Vinci surgical robot (Intuitive Surgical) by 2 experienced colorectal surgeons using a standard technique. Data included; Indication, age, operative time, length of stay, complications (including conversion) and recurrence.
Results: All 10 patients were female, median age 65. Indications included rectal prolapse(6), rectocoele(3) and rectocoele/intussusception(1). Median operative time was 262 minutes. One conversion(pfannnenstiel) for bleeding occurred. Median stay was 2 days. Median follow up was 9.5 weeks. All patients reported symptomatic improvement. 1 patient had a small asymptomatic clinical recurrence.
Conclusion: Robotic VMR is safe, however operative time was prolonged. All patients had good functional outcomes and short inpatient stays. Robotic surgery is associated with longer operative times and increased equipment costs which need to be balanced against potentially better technical and functional success.
Key statement: Use of VMR is likely to increase as more pelvic floor dysfunction is recognised. Robotic VMR is likely to become more popular as it is less technically challenging. Operative times are likely to improve with experience, and as robotic surgery expands in other disciplines, associated costs are likely to decrease.

P13
URINARY RETENTION POST COLORECTAL RESECTION: LAPAROSCOPIC VS OPEN
Author(s): B Stubbs, F E Rizal, H Lee, S Warren, D Francis Presenter: B Stubbs Institution: Barnet and Chase Farm Hospitals, UK
Aims: Enhanced Recovery after colorectal surgery aims to remove urinary catheters (TWOC) early. Laparoscopic surgery has advantages over open surgery including earlier mobilisation and less post operative pain, which may impact on postoperative urinary retention rates. We investigate the timing of TWOC and urinary retention rates in open vs laparoscopic surgery.
Methods: All patients undergoing colonic resection within an enhanced recovery programme at our hospital over the last 5 years were included. Data was collected prospectively by a dedicated enhanced recovery nurse. Patient gender, method of surgery (laparoscopic or converted/open) was documented. Timing of TWOC and urinary retention rates were investigated.
Results: 139 laparoscopic and 90 open/converted cases were identified. Laparoscopic cases were significantly more likely to have an earlier TWOC ( <0.00001) Retention rates did not differ between groups (=0.42). Pelvic dissection did not influence retention rates (laparoscopic = 0.90, open =0.56) Men were more likely to develop urinary retention (=0.05)
Conclusion: Laparoscopic cases were more likely to have an earlier TWOC. Retention rates were similar between open and laparoscopic groups (5.56% vs 8.63%). Pelvic surgery did not influence urinary retention rates in either group. In keeping with previous studies men were more likely to develop post operative retention (10.8% vs 3.67%).
Key statement: Laparoscopic colorectal surgery has become accepted as having many advantages in terms of patient recovery from surgery. The Enhanced recovery programme has improved the pathway of post-operative care and has reduced length of stay. Laparoscopic surgery allows earlier TWOC and has no significant adverse impact on urinary retention rates.

P14
SUBCLINICAL EMPHYSEMATOUS CHOLECYSTITS, EMPYEMA AND PORCELAIN GALL BLADDER, A CASE REPORT
Author(s): A Zaidi, A R Morgan Presenter: A Zaidi Institution: Morriston Hospital, Swansea, UK
Aims: Emphysematous cholecystitis (EC) is a rare and life threatening form of acute cholecystitis which should be diagnosed and treated early to avoid complications. Asymptomatic cases are rare.
Methods: A 73 years old female presented to a general practitioner with 2 weeks history of RUQ pain. USS showed emphysematous cholecystitis. She was treated with antibiotics as outpatient and referred to the surgeons. Surgery was delayed due to new onset AF. Per operatively she had a porcelain gall bladder and the laproscopic procedure was converted to open and a partial cholecystectomy was done. Recovery was uneventful. Histology showed changes of chronic calcific cholecystitis.
Results: EC is a clinical variant of acute cholecystitis with a mortality rate of approximately 15%. Clinical presentation may mimic acute cholecystitis from a spectrum of minimal pain to septic shock. Gram negative organisms are common. USS shows gaseous halos in the gall bladder wall and has less sensitivity and specificity in the diagnosis of EC. CT should be the next investigation of choice if EC is suspected on USS. Antibiotics should be started early to prevent complications. Treatment consensus by majority of the authors is cholecystectomy.
Conclusion: EC is a clinical form of cholecystitis which carries a high mortality. There should be high index of suspicion. Cholecystectomy is the treatment of choice unless contraindicated.
Key statement: Emphysematous cholecystitis is a life threatening condition which should be diagnosed with low index of suspicion and treated promptly to prevent morbidity and mortality.

P15
A PROSPECTIVE, RANDOMISED, SINGLE BLIND TRIAL OF 5MM VS. 3MM PORTS FOR LAPAROSCOPIC CHOLECYSTECTOMY
Author(s): M Bignell, M Lewis, E Cheong, M Rhodes Presenter: M Bignell Institution: Norfolk and Norwich University Hospital, UK
Aims: Single incision laparoscopic cholecystectomy (SILC) is said to provide improved cosmesis with a reduction in postoperative pain, but involves a change in operative technique. We have conducted a single-blind, randomised controlled trial study of cosmetic outcome and post-operative pain comparing laparoscopic cholecystectomy (LC) using either 3mm or 5 mm ports.
Methods: 80 patients were recruited and randomised to a LC using either 5mm ports (control) or 3mm ports. Operative details, time and pain scores at 1h, 6h, and 1 week and analgesia required in the 1
st week were collected. Cosmetic outcome was assessed at 6 months using a
validated questionnaire.
Results: Operative time was similar between the two groups. Pain scores in the 3mm group were significantly lower at 1h and 1 week compared to the control group ( Value = 0.003 and 0.002 respectively). The 3mm group had significantly better cosmetic outcome scores at 6 months.
Conclusion: The use of 3mm ports is technically feasible in patients undergoing LC for gallstones with comparable operating times to conventional LC with reduced pain scores and a better cosmetic outcome.
Key statement: This trial shows that 3mm instruments have an advantage over CLC in both post-operative analgesia scores and more importantly cosmetic outcome at 6 months. It offers a realistic alternative to Single Port Laparoscopic Cholecystectomy (SPLC) without a significant learning curve or increase in operative time

P16
COMPARISON OF SILS - CHOLECYSTECTOMY WITH STANDARD FOUR PORT LAPAROSCOPIC CHOLECYSTECTOMY WITH LONG-TERM FOLLOW-UP
Author(s): H Shabana1, J O' Keefe
2, C J O' Boyle
1
Presenter: H Shabana Institution:
1Surgical Department, Bon Secours Hospital, Cork, Ireland,
2Best Practice
Department, Bon Secours Hospital, Cork, Ireland
Aims: We evaluated our initial experience with single-incision laparoscopic surgery (SILS) cholecystectomy in comparison to standard laparoscopic cholecystectomy (LC) over 2 year period.
Methods: Between June 2008 and June 2010, 48 consecutive patients undergoing SILS were evaluated and compared retrospectively to a cohort of 24 consecutive patients undergoing LC. Patient records were retrieved and patients completed a telephone survey. Particular attention was paid to post-operative morbidity, post-operative pain scores, analgesia requirements, return to normal activity and cosmetic satisfaction. Patients were subsequently surveyed at a median of ? 40(26-50) months following surgery
Results: During the study period 10 patients were considered inappropriate candidates for SILS due to multiple previous laparotomies and/or medical co-morbidity. There were no significant differences between the groups for age, sex, body mass index or indications for surgery. There was no conversion to laparotomy or early surgery-related morbidity in either group. Thirteen patients presented with acute cholecystitis (7LC v 6SILS, = ns). Median operative time was greater for SILC (50, 55 v 25 min, <0.001). A further access (5mm) port was required in 2 (10%) SILS. There was no difference in post-operative length of stay (2 v 2 days), average pain scores, daily narcotic analgesic requirement and time to return to normal activity (14 vs14 days). SILS patients had a higher cosmetic satisfaction score (10 v 10 <0.05). At 40 months post-op 2 patients (6%) in the SILS group developed Incisional hernia compared with none in the LC group
Conclusion: Single –incision laparoscopic cholecystectomy can be performed safely and with high patient satisfaction. However is technically demanding and more time-consuming. Furthermore the incidence of incisional hernia is higher with longer follow-up. The authors have abandoned routine SILS cholecystectomy.
Key statement: Single -incision laparoscopic cholecystectomy can be performed safely and with high patient satisfaction. However is technically demanding and more time-consuming. Furthermore the incidence of incisional hernia is higher with longer follow-up. The authors have abandoned routine SILS cholecystectomy.

P17
LAPAROSCOPIC MESH INCISIONAL HERNIORRAPHY: A SINGLE CENTRE EXPERIENCE
Author(s): H Shabana, C J O' Boyle Presenter: H Shabana Institution: Department of Surgery, Bon Secours Hospital, Cork, Ireland
Introduction: Incisional herniae occur in 4-20% of patients after laparotomy. Surgical repair with onlay mesh is technically demanding and associated with significant morbidity.
Aims: The aim of this study was to review the outcomes of laparoscopic mesh herniorraphy performed by a single consultant surgeon.
Methods: Eighty-two patients who underwent laparoscopic mesh herniorraphy between July 2008 and March 2012 at our institution were reviewed.
Results: Median age was 60 (36-81) years. Fifty two percent (n=43) were female. The size of the defect was <5cm in 44% (n=36), 5-8cm in 44% (n=36) and 9-25cm in 12% (n=10) patients.
The defects were located in the midline in 51% (n=42), suprapubically in 20% (n=16), in the right upper quadrant in 9% (n=7), in the right or left flank in 10% (n=8) and in the right or left ilica fossa in 10% (n=8). Eighty percent (n=66) had primary defects. Of the 16 patients with recurrent herniae, four had recurred on more then one occasion. Intra-abdominal adhesions were extensive in 32% (n=26), moderate in 22% (n=18), minimal in 38% (n=31) and not present in 9% (n=7).
Median duration of surgery was 50 (15-125) minutes. Immediate postoperative complications occurred in 11% (n=9) patients: Seroma (n=2), Ileus (n=4), Haemorrhage (n=1), Cellulitis (n=2). Median post-operative stay was 2 (1-23) days.
Four patients (5%) developed recurrence at median follow-up of 15 (1-44) months. One patient underwent successful laparoscopic re-intervention. Three required open mesh herniorraphy.
Conclusion: Laparoscopic incisional herniorraphy is more technically demanding and somewhat controversial for larger defects compared with open repair. Our experience compares favourably with the open approach.
Key statement: Laparoscopic incisional herniorraphy is more technically demanding and somewhat controversial for larger defects compared with open repair. Our experience compares favourably with the open approach.

P18
STRATIFIED RANDOMISED TRIAL OF 2D VS 3D VISION SYSTEMS FOR LAPAROSCOPIC INTRACORPOREAL SUTURING IN SURGICAL SHO`S
Author(s): W Elbakbak1,3
, S Sarker3, A Almarzouq
1,2 , R B Manohar
1, B Patel
1,2,
Presenter: W Elbakbak
Institution: 1Barts Cancer Institute, London, UK,
2Barts and the Royal London Hospital, UK,
3Queen Mary University of London, UK
Aims: To objectively evaluate and compare surgical trainee’s performances in laparoscopic intracorporeal suturing using 2D and 3D vision systems in terms of performance times, number of repetitions and errors on a box trainer.
Methods: 24 core surgical trainees were randomised between two vision systems (3D or 2D) stratified by gender. The trainees were asked to perform laparoscopic intracorporeal suturing according to the validated fundamentals of laparoscopic surgery (FLS) curriculum until task proficiency is achieved.
Results: The 3D group showed 33% fewer accuracy errors and better precision although it was statistically insignificant.
Vision System 3D 2D
Median (range) Median (range) P value
Time to reach proficiency (min) 73 (39-137) 78 (31-228) 0.8
Number of repetitions 25 (16-32) 28 (15-62) 0.71
Accuracy errors 4 (1-8) 6 (0-25) 0.5
Gap error 1.5 (0-4) 2 (0-7) 0.63
Error score 51 (6-82) 50 (4-104) 0.82
Conclusion: We concluded that the performance and error rates while performing laparoscopic suturing under 3D and 2D vision systems were similar but a trend towards fewer errors and better precision score was observed in 3D group. Training in the 3D group was influenced by tiredness, headache and stereoscopic adaptation.
Key statement: Acquiring laparoscopic suturing skills using 3D vision system is as effective as conventional 2D laparoscopy with no statistical difference in time, number of repetitions and measured error rates in reaching proficiency using FLS curriculum. However, there is a trend towards fewer errors and better precision score in 3D group.

P19
PATIENTS’ PERCEPTION OF SURGICAL SAFETY: A CROSS-SECTIONAL STUDY
Author(s): R Goriparthi, S Makkiyah, S Sarker, S Nikpour-Valiseh, B Patel Presenter: R Goriparthi Institution: Barts Cancer Institute, London, UK
Aims: A survey of patients’ perception of surgical safety, and its association with socio-demographic factors.
Methods: 612 adult English-speaking patients were interviewed using 35 element questionnaire to explore perceptions of admission-related safety measures, hygiene, discharge instructions, doctor’s competency and equipment safety. Responses were scored (+10), (-10) and (zero) for a positive, negative and equivocal answers respectively. The mean score was tested against socio-demographics using linear regression.
Results: Mean age was 54 years with 54% males. 98%, 94%, 96% and 81% patients gave positive perception regarding whether patients’ identity was checked, treatment explained, allergies inquired, and operation site marked respectively. 48% had good perception of thrombo-prophylactic measures. 22% were unaware of staff hand washing. Perception of discharge instructions regarding follow up, wound dressing and pain control was positive in 89%, 84% and 93% of patients respectively. 90% of patients perceived their doctors as competent. The overall score of safety perception ranged from -1 to +12 (mean=7.9). Linear regression showed that perception was negatively significantly influenced by female gender (P= 0.04), young age (P=0.016), and being single (P=0.031).
Conclusion: Patients in surgical outpatient clinics had good perceptions of safety. Perception levels were not influenced by education, employment, ethnicity or income. Young patients, singles and females showed lower perception.
Key statement: Patients’ pereption of safety was negatively significantly influenced by young age, female gender and being single. Efforts should be directed towards raising awareness of these groups of patients.

P20
INTRAGASTRIC BALLOON IN THE MANAGEMENT OF MORBID OBESITY
Author(s): M Nnaji, J Tham, R Welbourn, D Mahon Presenter: M Nnaji Institution: Musgrove Park Hospital, Taunton and Somerset NHS Foundation Trust, UK
Aims: BioEnterics Intragastric Balloon (BIB) together with a diet restriction program has gained wide popularity in the initial management of morbid obesity. The aim of this study was to evaluate the effectiveness of intragastric balloon in the management of morbid obesity.
Methods: A retrospective study was conducted on 34 patients who underwent BIB insertion for morbid obesity (BMI > 50 kg/m²) prior to gastric bypass between February 2007 and November 2011.
Results: The mean age, weight and BMI of patients were 44.29±11.49years, 183.76±30.39kg, and 63.7±7.3kg/m² respectively. Six months after BIB application, mean weight and BMI had reduced to 163.36±25.96kg and 56.98±5.87kg/m² respectively (<0.001). Excess weight loss at six months ranged between 0-56.2kg (0–41.3%), mean value 20.51±16.17kg (17.11±12.66%). No complications were recorded.
Conclusion: BioEnterics Intragastric Balloon application is a safe procedure and results in significant weight loss in morbidly obese patients.
Key statement: BioEnterics Intragastric Balloon is effective in the management of morbid obesity.

P21
AN ALTERNATIVE METHOD FOR CLOSURE OF UMBILICAL PORT-SITES FOLLOWING LAPAROSCOPY
Author(s): T Wiggins, S Lisa, A Khan, A Rohatgi Presenter: T Wiggins Institution: Whipps Cross University Hospital, London, UK
Aims: Following laparoscopic surgery secure closure of the fascial layer reduces the incidence of port-site herniation. We present a simple and effective method of closing the fascial layer by using placed sutures to provide upwards traction and allow sequential closure of the fascial defect.
Methods: A Littlewood’s forceps is applied to the cicatrix and upwards traction applied. A suture is used to close the superior part of the fascial defect. A mosquito clip is then placed on the suture to provide upward traction. The defect can then be closed sequentially.
Results: This technique has been used effectively in our practice in 140 cases over two years with no reported cases of incisional hernia following this method of fascial closure.
Conclusion: This method provides a simple and effective method of closing the fascial defect produced by laparoscopic port sites. It is easily reproducible and can be particularly useful for obese patients.
Key statement: This is a safe and effective technique for closing the fascial defect in laparoscopic surgery, and there are no reported incidences of port-site herniation following this method.

P22
PATIENTS UNDERGOING ELECTIVE LAPAROSCOPIC CHOLECYSTECTOMY DO NOT NEED A GROUP AND SAVE SAMPLE
Author(s): S Whelan-Johnson, J Taylor, B Ridler, J Thompson Author: S Whelan-Johnson Institution: Royal Devon and Exeter NHS Foundation Trust, UK
Aims: To audit the need for and timing of perioperative blood transfusion in patients undergoing elective laparoscopic cholecystectomy, to establish if a routine Group and Save sample is needed.
Methods: A retrospective analysis of all elective laparoscopic cholecystectomy patients over a six month period was performed. The patients were identified from Theatre database and data was collected from clinic letters, discharge summaries, laboratory records and case notes.
Results: 273 patients were identified. 100 patients (37%) had a Group and Save sample sent. No patients needed a transfusion intra-operatively. Two patients (0.7%) required a transfusion post-operatively. One of these patients was on bridging therapy with Low Molecular Weight Heparin and their operation was converted to an open procedure. Conclusion: A routine Group and Save sample (£15) before elective laparoscopic cholecystectomy is not required and does not compromise patient safety. Patients at high risk of bleeding should be identified on clinical grounds and a sample sent if needed. This could have saved over £8000 per annum in our hospital.
Key statement: Pre-operative guidelines suggest a “Group and Save” prior to laparoscopic cholecystectomy. This audit found that the very small number of patients requiring transfusion needed it post-operatively. Group and Save samples should be reserved for those at high risk of bleeding, thus reducing hospital costs and laboratory time.

P23
LAPAROSCOPIC CARDIOMYOTOMY FOR ACHALASIA: IS POST OPERATIVE CONTRAST SWALLOW NECESSARY?
Author(s): W Carr, A Madhavan, YKS Viswanath Presenter: W Carr Institution: James Cook University Hospital, Teeside, UK
Aims: Laparoscopic cardiomyotomy for achalasia is an effective treatment for achalasia. Whilst laparoscopic approaches minimize the surgical insult to the patient care needs to be taken to minimize the risk of mucosal perforation. This study aims to identify if intra-operative endoscopy and air leak test followed by post-operative contrast swallows was indicated.
Methods: A retrospective audit of Laparoscopic cardiomyotomy performed in a single centre over a 7-year period. A case note review was performed after production of a proforma. 24 cases were identified between 2004-2011.
Results: M:F 5:3, mean age 50(18-79), mean BMI 28(17-37). 9 patients had previously undergone 1 pneumatic dilatation and 4 more than 1 dilatation. Intra-operative endoscopy and air leak test was performed in all cases followed by a post-operative swallow. 1 intra operative mucosal perforation was identified and repaired. No leaks were seen on the post-operative swallow. 1 patient was readmitted with a contained leak 1-week post op.
Conclusion: The addition of a routine post-operative contrast swallow to the intra-operative endoscopy and air-leak test did not change management and failed to predict the only readmission occurring at 1 week post op. The mean length of stay was 2 nights(1-4) and this was determined by the time taken to obtain the contrast swallow.
Key statement: When performing laparoscopic cardiomyotomy for achalasia routine intra-operative and post-operative tests can identify mucosal perforations. Whilst intra-operative leak tests are useful by allowing immediate surgical intervention in our series of cases a routine post opertive swallow does not change management and fails to predict the possibility of delayed leak.

P24
LAPAROSCOPIC VERSUS OPEN REPAIR OF STRANGULATED ABDOMINAL WALL HERNIAE – A 5 YEAR EXPERIENCE
Author(s): A Simpson, S Isreb, S Woodcock Presenter: A Simpson Institution: North Tyneside General Hospital, North Shields, UK
Aims: Elective laparoscopic hernia repair is a well-recognised, safe procedure. There is less published data on the role of laparoscopy in the context of emergency repair. We analysed the outcomes of patients undergoing emergency laparoscopic repair of abdominal wall herniae to assess its efficacy and safety compared to open repair.
Methods: Following Caldicott approval, retrospective interrogation of the emergency theatres database for all abdominal wall hernia repairs between August 2006 to August 2011 was performed, identifying the patient cohort. Individual case notes were reviewed to calculate parameters including length of stay, procedure time, 30 day mortality and morbidity.
Results: 169 patients in total, 71 undergoing laparoscopic repair, 93 open and 4 were converted. The majority were femoral herniae (27.8%). Average procedure length and length of stay was shortest for the laparoscopic group (43 minutes and 6 days respectively). Mortality was 8.6% for open repair, 1.4% for laparoscopic.
Conclusion: Laparoscopic repair can be considered for the majority of strangulated abdominal wall herniae. The surgeon’s experience with laparoscopy is a key factor in whether it is used. Some patients experience significant delay in receiving treatment, particularly when they have an occult hernia and are admitted under a non-surgical specialty.
Key statement: Further training and education in the use of laparoscopy for emergent repair of strangulated herniae could encourage more surgeons to adopt this technique. Our study shows that laparoscopic repair gives shorter operating times and lengths of stay, but more randomised-controlled trials are needed to help influence the debate.

P25
A RETROSPECTIVE ONE YEAR AUDIT OF LAPAROSCOPIC CHOLECYSTECTOMY IN A DISTRICT GENERAL HOSPITAL
Author(s): S Wardle, J Breslin Presenter: S Wardle Institution: Royal Cornwall NHS Trust, UK
Aims: The aim of the audit was to determine the 30 day readmission, day case and conversion to open rate for all Laparoscopic Cholecystectomies performed within our trust, which supplies a population of 420,000. Comparison was made to data published by the NHS Institute for Innovation and Improvement. Focus on: Cholecystectomy.
Methods: Data was collected retrospectively over a one year period, using information from the coding database, and obtaining relevant information from out patient information database, and reviewing case notes where required. Reason for readmission was identified, and included those related to and unrelated to initial surgery.
Results: 669 Laparoscopic Cholecystectomies were performed in 2011 by 12 consultants. 81% of the operations performed were as elective operations, with a day case rate of 43%. 20 cases (3%) required conversion to open cholecystectomy. There were 63 (9%) readmissions within 30 days which were related to the initial surgery.
Conclusion: Conversion to open rate fell within those suggested. Our readmission rate leaves room for improvement. We have addressed with the implementation of an information booklet given to all patients before surgery, and a nurse led follow-up telephone conversation within one week of surgery.
Key statement: Rates for 30 day readmission, day case and conversion to open for all laparoscopic cholecystectomies, was collected retrospectively for a 1 year period. We performed well compared to suggested data, however there is room for improvement, which we have addressed with the implementation of an information booklet.

P26
VENETIAN BLINDS TECHNIQUE TO FIX ULTRA PRO MESH IN LAPAROSCOPIC TEP HERNIA REPAIR
Author(s): R Kochupapy1, G Ranganathan
2, T Cummins
1
Presenter: R Kochupapy Institution:
1Plymouth NHS Trust, UK,
2Bournemouth NHS Trust, UK
Aims: 17 % general surgical procedures are performed for inguinal hernias. Laparoscopic TEP hernia repairs have become the standard practice for this condition. Non-absorbable mesh is placed in the pre peritoneal space. Various types of meshes are used, and they are usually not fixed. One of the the meshes used for this type of hernia is a lightweight ultrapro mesh. Placing this mesh in right place takes about 15 minutes average on either side.
Here we present our Venetian blinds technique to fix the mesh at a right place quickly and elegantly.
Methods: Ultra pro mesh comes in the size of 15 by 15 cms. Make a superior flap (3 by 1 cm) on the medial superior aspect of the mesh and round the lateral edges. Roll the mesh inferior to superior fashion and fix the mesh in rolled-up position with 2 vicryl ties 5 cms apart. Leave the flap area free for grasping.
Introduce the mesh through the 10 mm port into the lateral space. Bring the rolled-up mesh 5 cms above the deep ring. Now holding the flap cut the vicryl strings and unroll the mesh as you unroll the venetian blinds. Mesh is placed in a well-secured position after making sure the peritoneal edge is medially placed and a 5 cm radial cover over the internal ring achieved. If necessary either use 1 tack to the medial flap on to the rectus muscle or fix with a loose vicryl stitch.
Results: We have used this technique in our department and reduced around 15 minutes of our operation time to place a ultrapro mesh. Moreover, it reduced the frustrating moments of placing this ultra-thin mesh in place.
Key statement: Common Laparoscopic surgical procedure performed is TEP repairs. One of the mesh used is light weight Ultrapro mesh. Frustrating moments of the surgery is the placement of the ultra thin mesh in the extra peritoneal space. This venetian blind technique is an easy technique to place the mesh and also easy to teach.
P27
SYMPTOM RESOLUTION POST CHOLECYSTECTOMY
Author(s): G van Boxel, A Kiszely, E Trafford, G Howat, S Appleton Presenter: G van Boxel Institution: Buckinghamshire NHS Healthcare Trust, High Wycombe, UK
Aims: The aim of the study was to investigate symptom resolution following laparoscopic cholecystectomy (LC).
Methods: The study was performed using a standardized telephone questionnaire. Patients that underwent planned day-case LC in the period of February 2011 – February 2012 were asked in June 2012 whether they had complete resolution of symptoms. In addition we asked about new symptoms since the operation.
Results: Of 152 patients that underwent LC, over 95% had biliary-type symptoms and ultrasound proven gallstones pre-operatively. Following surgery 66% had complete resolution of their symptoms. 34% had continuing abdominal symptoms. Of these, 44% suffered with “indigestion” commonly aggravated by fatty foods, 38% had RUQ pain and18% had diarrhoea.
Conclusion: LC results in complete symptom resolutions in two thirds of patients. Surprisingly, one third of patients continue to have symptoms. The commonest residual symptom is indigestion. This study could indicate that LC is performed in a significant group of patients whose symptoms may not be related to their proven gallstones.
Key statement: Elective LC is routine day-case surgery performed in our hospital without formal follow up. A retrospective telephone study of 152 patients revealed that complete symptom resolution occurred in 66%. One third of patients have residual or new symptoms, such as diarrhoea, at greater than 3 months post LC.

P28
ACQUIRING LAPAROSCOPIC SKILLS IN NOVICES USING TWO DIMENSION AND THREE DIMENSION VISUAL SYSTEMS: A RANDOMISED CONTROL STUDY
Author(s): B S Alaraimi1,2
, S J Sarker1, W S Elbakbak
1, A Al-Marzouq
1, B Patel
1
Presenter: B S Alaraimi Institution:
1Barts Cancer Institute, London, UK,
2Barts and Royal London Hospital, UK
Aims: To compare performance of novices on three dimension (3D) and two dimension (2D) vision systems using fundamentals of laparoscopic surgery (FLS) tasks.
Methods: Thirty medical students were randomised to 3D and 2D for acquiring laparoscopy skills using four FLS tasks. Performance measured included completion time, number of repetitions and errors.
Results:
FLS Task
Total Time(minutes)
Median(IQR)
Total Repetitions
Mean(±SD)
Total Errors
Median(IQR)
2D 3D 2D 3D 2D 3D
Peg transfer 108(37) 149(29)* 75(±7) 80(±0)* 11(10) 4(4)*
Endoloop 6(8) 5(5) 7(±5) 6(±4) 2(8) 2(4)
Extracorporeal suturing
48(27) 36(18) 14(±6) 11(±5) 44(44) 4(28)*
Intracorporeal suturing
73(46) 42(39) 19(±8) 19(±8) 28(32) 12(14)*
*Sig at 5% level,SD=Standard deviation,IQR=Interquartile range
Mean of the total number of repetitions and total time to complete curriculum was lower in 3D vs 2D; 113 vs 115(P=.81) and 60.4 vs 59.3 hrs (P=.62) respectively. Median errors in 3D group (37) was less compared to 2D group (85) (P=.00).
Conclusion: 3D group performed better in more advanced tasks of the FLS with significant reduction in error scores. Performance time and repetitions were less in the 3D group although it’s not statistically significant and this was observed to be related to visual adaption time needed for the 3D group for each exercise and relatively flat field in box trainer with fewer points of reference for variable depth perception for 3D effect.
Key statement: Three dimension enhanced visual field has the potential to reducing errors and enhancing the performance in laparoscopic surgery enabling more complex operations to be performed with fewer complications.

P29
COMPLICATIONS FOLLOWING ELECTIVE DAY-CASE LAPAROSCOPIC CHOLECYSTECTOMY
Author(s): G van Boxel, A Kiszely, E Trafford, G Howat, S Appleton Presenter: G van Boxel Institution: Buckinghamshire NHS Healthcare Trust, High Wycombe, UK
Aims: The aims of the study were to identify the incidence of post-operative complications in patients undergoing elective daycase laparoscopic cholecystectomy (LC).
Methods: The study was performed using a standardized telephone questionnaire. Patients that underwent planned day-case LC in the period of February 2011 – February 2012 were retrospectively asked whether they had attended hospital or their GP practice in the 30 days post surgery for any complications related to the surgery.
Results: 356 laparoscopic cholecystectomies were performed and we obtained 217 responses (61%). The incidence of wound infection was 7.5%, bile leak (from cystic duct or accessory ducts) 1.8%, pancreatitis 0.9%, retained stones 0.9%, pulmonary embolism 0.4%, pneumonia 0.4%, myocardial infarction 0.4% and deep vein thrombosis 0.4%.
Conclusion: Wound infection is the most common post-operative complication in day-case LC. Of these, the umbilical port was involved in 80%, even though gallbladder extraction was routinely through the epigastric port. Female patients are at increased risk of wound infection. Serious complications are rare and no case required conversion to open.
Key statement: Elective LC is routine day-case surgery in our hospital performed without formal follow up. A retrospective telephone study revealed the incidence and nature of post-operative complications to be minimal. Wound infection occurred in 7.5% of patients but resolved in all cases with a single course of antibiotics.

P30
AN EVALUATION OF STEREOACUITY IN PRACTISING SURGEONS ACROSS A RANGE OF SURGICAL SPECIALITIES
Author(s): S Hamid1, M Biddle
1, N Ali
2
Presenter: S Hamid Institution:
1St George's University of London, UK,
2Moorfields Eye Hospital, London, UK
Aims: Judging depth is important in surgery. Stereoacuity has been singled out as a possible predictor of surgical ability. However, it is not clear whether high-grade stereoacuity is necessary for a career in surgery. We therefore aimed to evaluate stereoacuities in practising surgeons across different surgical specialties using three standard stereotests.
Methods: We recorded stereoacuity values on surgeons at a London teaching hospital using the Titmus, TNO and Frisby stereotests. We defined a high-grade stereocauity value as <60 sec arc. We defined a reduced stereoacuity value as >120 sec arc for Titmus and TNO and >250 sec arc for Frisby.
Results: 66 surgeons (36 trainees and 30 consultants) were tested from 12 surgical specialties. Median stereoacuities were: 40 sec arc on Titmus (40-800), 30 sec arc on TNO (15-480) and 20 sec arc on Frisby (20-600). 4 surgeons had no recordable stereoacuity on TNO, and 1 was also unrecordable on Titmus.
Conclusion: Depending on the test used, high-grade stereopsis was found in 74%-83% of surgeons and reduced stereopsis in 2%-14% of surgeons. Most surgeons have high-grade stereoacuity but around 20% do not, and a few have no recordable stereoacuity. It is therefore not necessary to have high-grade stereoacuity for a surgical career.
Key statement: Stereoacuity has been singled out as a possible predictor of surgical ability. This is increasing relevant with advancing three-dimensional surgical techniques. Our study shows that high-grade stereoacuity is not necessary for a surgical career.
P31
MEASUREMENT OF LIVER FUNCTION TESTS FOLLOWING LAPAROSCOPIC BILIARY SURGERY
Author(s): A Mirza, S Zino, A Nassar Presenter: A Mirza Institution: Monklands Hospital, Airdrie, UK
Aims: To assess the incidence and clinical management of elevated liver function tests (LFTs) following laparoscopic biliary surgery in a department where intraoperative cholangiography (IOC) is routinely performed with laparoscopic cholecystectomy (LC).
Methods: A prospective study of LC without IOC (Group A, n=25) and with IOC (Group B, n=25) with normal preoperative LFTs were included. Post operative AST, ALT, LDH, AP, GGT and bilirubin were recorded daily. Elevation in LFTs was defined as levels 1.5 times or more. The groups were compared for incidence of raised LFTs and duration of surgery.
Results: The male to female ratio was 1:4. 8 patients in Group A (32%) and 16 patients in Group B (64%) had at least one abnormal value ( = 0.01). 11 patients (44%) with IOC showed elevation of AST on post-op day one while it was elevated in 7 patients (28%), who underwent only LC. Raised GGT was noted in 6 patients (24%). Bilirubin and AP were elevated in 3 patients (12%, =0.81) after LC and IOC. There was no difference in the difficulty of surgery, gallbladder inflammation and duration of surgery. IOC was significantly related to the elevation of liver enzymes.
Conclusion: Self limiting disturbances in LFTs are more common following LC and IOC. This deterioration in liver function tests had no effect on patient management. It is not necessary to routinely evaluate LFTs following LC and IOC.
Key statement: Liver function tests should not be routinely measured following laparoscopic biliary surgery.
P32
LAP-TRAINER: A COST EFFECTIVE APPROACH IN IMPROVING LAPAROSCOPIC SKILLS FOR SURGICAL TRAINESS IN THE AGE OF AUSTERITY
Author(s): A Mirza, A Nassar Presenter: A Mirza Institution: Monklands Hospital, Airdrie, UK
Aims: The achievement of core skills in laparoscopic surgery are necessary for early specialist surgical training years. The laparoscopic training models and simulators available are expensive and can be only be bought by hospitals and trusts. Our aim was to develop user friendly and cost-effective laparoscopy trainer which can be easily developed and reproduced by other trainees.
Methods: We searched the available laparoscopy simulator and training models in the market and identified cost-effective approach. We bought 20 litres plastic container (£ 5.00), Sony HD webcam with USB cable and light source (£ 39.00), plastic tubing (£ 4.00) laparoscopic ports and instruments (£ 22.00, eBay). Three separate holes were made in the lid of the plastic container 3 cm in diameter. The central hole was used to place the camera which was attached to the laptop monitor via the USB cable. The two side holes were used for insertion of ports for laparoscopic instruments.
Results: The above laparoscopy trainer was used to perform manipulation, suturing and cutting of cloth, tissue paper, plastic glove and animal tissue. A standard triangulation, illumination, depth perception and 2-dimensional imaging was achieved.
Conclusion: This laparoscopy trainer can be adopted and made at home by other trainers and can help them to improve their laparoscopic skills.
Key statement: Lap-Trainer is a low budget and cost-effective approach in improving laparoscopic surgical skills.

P33
RECTAL OBLITERATION FOLLOWING STAPLED HAEMORRHOIDOPEXY: A NEW ENDOSCOPIC APPROACH TO RESTORE LUMINAL CONTINUITY
Author(s): A Mustafa, M Jabbar, M Rashid, M Downey, K Shalli Presenter: A Mustafa Institution: Wishaw General Hospital, Lanarkshire, UK
Aims: Life threatening complications following stapled haemarrhoidopexy are uncommon. We describe our experience in dealing with a major but rarely reported complication of this procedure in a 60 year old lady with a partial thickness rectal prolapse and circumferential haemarrhoids.
Methods: Stapled haemarrhoidopexy was performed using an Ethicon PPH to treat both circumferential haemorrhoid and partial thickness rectal prolapse. After firing the device, complete rectal obliteration was noticed. Therefore, laparoscopic loop colostomy was fashioned. Contrast study confirmed mucosal obliteration. A new endoscopic technique was used to restore continuity of the bowel.
Results: Reopening of rectal obliteration was achieved after passing an endoscope via colostomy to snare a guide wire that was inserted rectally via a cannula from PEG’s set. The wire was tied to the anvil of an EEA circular stapler and under endoscopic guidance it was passed through the obstructed site. Stapler was then locked to anvil per rectum and fired with resulted complete circular luminal continuity.
Conclusion: Rectal obliteration following stapled haemarrhoidopexy is a very rare complication but it could be under reported. Such complication was managed successfully using a new endoscopic technique and the stoma reversed weeks later. The patient had uneventful recovery with no reported problems on follow up.
Key statement: Rectal obliteration had occurred despite the standard precautions taken during stapled haemorrhoidopexy and a complete disc of mucosa on the stapler ring was obtained. Therefore, extreme caution should be taken when performing this procedure. We suggest avoiding PPH as a treatment for combined circumferential haemorrhoids and prolapsed rectal mucosal disorder.

P34
PRE OPERATIVE ASSESSMENT AND DOCUMENTATION OF PATIENT SYMPTOMS IS KEY TO THE SUCCESSFUL LAPAROSCOPIC CHOLECYSTECTOMY OUTCOME
Author(s): C Brown, R Singh, T Boyce Presenter: C Brown Institution: Royal Gwent Hospital, Newport, UK
Aims: Significant numbers of patients undergoing cholecystectomy for apparently symptomatic gallstones continue to experience abdominal symptoms post-operatively. Retrospective pre-operative assessments were analysed particularly looking at the documentation of overlapping biliary and gastro-oesophageal reflux symptoms and the subsequent cholecystectomy symptomatic outcome.
Methods: Pre and post operative clinic letters of 100 consecutive patients who underwent laparoscopic cholecystectomy were retrospectively reviewed. Preoperative symptoms as documented by the surgeon were assessed particularly for inclusion of the presence and/or absence of biliary and GORD symptoms as well as mention of potential persistent symptoms post operatively.
Results: 21 of 100 patients described potentially overlapping symptoms. A need for oesophagoduodenoscopy was documented in 9 cases (42.8%) and only 6 (28.6%) of these underwent OGD. Post operatively 6 patients (6%) re-attended with GORD symptoms. Only 1 patient went on to have OGD showing evidence of gastritis.
Conclusion: While an effective treatment for symptomatic gallstones, it’s the surgeon’s duty to accurately assess and document their patient’s symptoms and investigate appropriately where there’s uncertainty about the diagnosis. It’s important to ensure that patients are fully informed and have a realistic understanding that despite surgery, some symptoms may be persistent.
Key statement: Accurate assessment and documentation of pre operative symptoms and their likely cause is vital in patient counselling and informed consent. It’s important to ensure that patients are fully informed and have a realistic understanding that despite surgery, some symptoms may be persistent.

P35
LAPAROSCOPIC REVISIONAL ANTIREFLUX SURGERY IS SAFE AND FEASIBLE WHEN PERFORMED IN A HIGH-VOLUME CENTRE
Author(s): R Parameswaran, T Lo, A Hamouda, H Ali, A Nisar Presenter: R Parameswaran Institution: Maidstone & Tunbridge Wells Hospitals NHS Trust, UK
Aims: Around 4% of the patients undergoing laparoscopic antireflux surgery may require revision surgery. The aim of this study was to evaluate the short-term clinical outcomes after laparoscopic revisional antireflux surgery (LRAS) in a high volume, tertiary referral centre for complex oesophagogastric disorders.
Methods: The study was a retrospective review of all LRAS performed between January 2007 and February 2012.
Results: The unit performed 30 LRAS (median age 58 years). Recurrent reflux was the most common presenting symptom, wrap migration and extensive adhesions were the most common operative finding. There were no conversions, median operative time 135 mins and median stay was one day. Only one patient required further redo surgery.
Conclusion: Laparoscopic revisional antireflux surgery appears to be safe and feasible in a high-volume unit that performed 600 primary antireflux surgeries over five years.
Key statement: Laparoscopic revisional antireflux surgery appears to be safe and feasible when performed in a high-volume centre with extensive experience of primary laparoscopic antireflux operations.

P36
IS THERE A NEED TO STANDARDISE ENDOSCOPIC ASSESSMENT PRIOR TO UNDERTAKING LAPAROSCOPIC REVISIONAL ANTIREFLUX SURGERY?
Author(s): R Parameswaran, T Lo, A Hamouda, H Ali, A Nisar Presenter: R Parameswaran Institution: Maidstone & Tunbridge Wells Hospitals NHS Trust, UK
Aims: In addition to other investigations, preoperative endoscopic assessment by an experienced endoscopist prior to laparoscopic revisional antireflux surgery (LRAS) is the single most important test. The aim of this study was to compare endoscopic assessment between operating surgeons (OS) and other endoscopists (OE) prior to undertaking LRAS.
Methods: The study was a retrospective review of endoscopic assessments prior to LRAS performed between January 2007 and February 2012 in a high-volume centre.
Results: 30 LRAS were performed with OS and OE undertaking 16 and 14 endoscopies respectively. OS reported wrap status (69%), recurrent herniae (33%), and oesophagitis (17%) whilst OE identified recurrent herniae (33%) but only reported wrap status in 7% (=0.03). Correlation with operative findings for OS and OE groups were 75% and 36% respectively (=0.35).
Conclusion: Endoscopic assessment prior to LRAS seems to be more informative with a higher correlation with operative findings when performed by the operating surgeon compared to other endoscopists.
Key statement: Preoperative endoscopic assessment prior to laparoscopic revisional antireflux surgery needs to be undertaken by an operating surgeon with experience in performing antireflux surgery in a high-volume centre. There may be a need to standardise endoscopic assessments prior to revisonal antireflux surgery to help better plan these complex operations.

P37
COMPARING KIDNEY-PRESERVING SURGERY VS. RADICAL SURGERY IN THE TREATMENT OF UPPER URINARY TRACT TRANSITIONAL CELL CARCINOMA, A SYSTEMATIC REVIEW
Author(s): A Al-Marzouq, S Makkiyah, S J Sarker, B Patel, H R H Patel Presenter: A Al-Marzouq Institution: Barts Cancer Institute, London, UK
Aims: Compare outcomes following radical nephroureterectomy and kidney-preserving surgery for upper urinary tract transitional cell carcinoma.
Methods: Systematic review of the literature in MEDLINE, Web of Science and Cochrane data bases using key words and MESH terms nephroureterectomy, segmental, endourolog*, endoscopic resections, urothelial, transitional cell carcinoma and upper urinary tract. The extracted data were pooled together for each parameter and an overall percentage representative of the sample available for analysis was produced.
Results: Total search findings were 1718 articles of which 93 studies met the inclusion criteria.
Radical
N= 23855
Kidney-preserving
N=2121
Tumour location distribution Renal: 57.99%
Ureteric: 39.96%
Renal: 46%
Ureteric: 50.4%
Muscle invasive tumours 51.2% 29.7%
Overall rate of surgical complications 18.4% 13.8%
Tumor recurrence rate 22.7% 38.5%
2 years disease specific survival 86.77% 88.5%
5 years disease specific survival 78.5% 76%
10 years overall survival 48.1% 45.5%
5 years disease free survival 69% 52.5%
Conclusion: Kidney-preserving procedures offer favorable surgical outcomes in patients with non-muscle invading tumours. Radical nephroureterectomy remains the gold standard with significantly superior 5 years disease free survival and 10 years survival rates.
Key statement: Kidney-preserving surgery for upper urinary tract transitional cell carcinoma though a very attractive option in terms of preserving renal function is only suitable for non-muscle invading tumours and in patients with solitary kidney or other imperative indications. Radical nephroureterectomy remains the gold standard with significantly superior disease free survival rate.
P38
LAPAROSCOPIC ASSISTED COLONOSCOPY
Author(s): A Quyn, N Henderson, R Steele, K Campbell Presenter: A Quyn Institution: Ninewells Hospital and Medical School, Dundee, UK
Aims: Failed colonoscopy is frequently due to fixed angulation from previous surgery or inflammation. Patients with suspected polyps >1cm on subsequent imaging, present a management dilemna. Segmental resection may be excessive intervention but observation is unsatisfactory. This study describes our experience using laparoscopy to facilitate colonoscopy and polypectomy in such patients.
Methods: All patients from 2008 to 2012 with an incomplete colonoscopy and polyps detected underwent standard laparoscopy with colonic mobilisation and division of adhesions to facilitate direct vision, laparoscopic assisted colonoscopy. Primary end points were completion of colonoscopy and polypectomy. Secondary end points were intra-operative complications, post-operative morbidity and successful standard follow-up colonoscopy.
Results: Twelve patients underwent the procedure. Complete colonoscopy to caecum was successful in all, mean of 2.1 polyps per patient (range 1-5). One iatrogenic enterotomy during adhesiolysis was repaired immediately, with no sequelae. Three patients have since undergone successful colonoscopy under sedation.
Conclusion: Laparoscopic assisted colonoscopy allows safe polypectomy in patients with failed colonoscopy without the need for segmental resection. This less invasive procedure yields recovery times similar to colonoscopy alone, avoiding the morbidity of a segmental resection with the added benefit of successful routine colonoscopy in the future.
Key statement: Laparoscopic assisted colonoscopy permits safe endoscopic polypectomy in patients with known polyps who have had failed attempts at routine colonoscopy due to intra-abdominal adhesions thus avoiding the need for segmental colonic resections.

P39
WHERE DO SURGEONS LOOK DURING 3D MINIMALLY INVASIVE SURGERY? THE INFLUENCE OF DISPARITY ON VISUAL ATTENTION WHILE VIEWING PASSIVE-POLARISING DISPLAYS
Author(s): R Smith1, A Day
1, D Windridge
2, S Taya
2, T Rockall
1, I Jourdan
1
Presenter: R Smith Institution:
1MATTU, Guildford, UK,
2University of Surrey, Guildford, UK
Aims: 3D pop out influences viewer’s eye movements during 3D cinematic productions. This study investigates the impact of 3D motion cues on experienced and novice surgeon’s visual attention patterns while viewing minimally invasive surgery.
Methods: 20 surgeons (10 expert and 10 novices) were randomized to view 10 high definition video sequences of minimally invasive surgical procedures in 2D followed by 3D mode, or in the reverse order. The Eyelink 1000 recorded eye movement characteristics throughout the viewings.
Results: Mean fixation count, fixation duration (ms), saccadic count and saccade duration (ms) for novices using 2D and 3D respectively were 19.8(SEM 0.5) vs. 21.3(SEM 0.46) P=0.002, 561.1(SEM 49.4) vs. 468.9(SEM 13.6) P=0.38, 19(SEM 0.5) vs. 20.4(SEM 0.5) P=0.002 and 2.2(SEM 0.09) vs. 2.1(SEM 0.1) P=0.18. Experienced surgeons fixation duration was also significantly increased in 3D.
Conclusion: Visual attention patterns for participants were significantly influenced by disparity cues from the 3D display. Eye movements may be directed toward salient task-irrelevant regions or guided by unique exploratory search strategies during 3D viewing. A period of adaptation is suggested prior to participating in surgical procedures using passive polarizing 3D displays.
Key statement: 3D minimally invasive surgery using passive polarising displays generates unique perceptual cues for the operating surgeon. A period of viewing adaptation may be required to ensure filtering of irrelevant 3D cues and promote task relevant hierarchical attention.

P40
THE ON-GOING DEBATE; TO OTC OR NOT TO OTC?
Author(s): J Simmonds, S Davies, A Peckham-Cooper, H Gompertz Presenter: J Simmonds Institution: Queens Hospital Burton FT, Burton-on-Trent, UK
Aims: A retrospective review of all laparoscopic cholecystectomies (LC) performed at a District General Hospital over a six-month period. The study aims to explore our local data with a view to identifying potential benefits and drawbacks of performing OTC in all patients regardless of any previous abnormal pre-operative investigations or not.
Methods: All patients undergoing laparoscopic cholecystectomy (with or without OTC) between April and November 2011 at our institution were included. Data was collected retrospectively
utilising the hospitals patient record system (HISS). Patients were excluded if undergoing laparoscopic cholecystectomy for alternative aetiologies than gallstones. Data for 176 cases were identified and analysed.
Results:
Total Mean Duration (mins (SD))
Mean LOS
(SD)
Post-op
complication
Rate
LC + OTC 134 98 (32) 2.5 16%
LC alone 42 94 (27) 2.4 12%
-value 0.17273 0.93 0.1170
(CI 95% = -1.9% - 19.5%)
Statistical significance <0.05
OTC failure rate = 4%. Other parameters were also measured.
Conclusion: Our results clearly demonstrate no significant difference in operating time, LOS or post-operative complications. Successful intubation was over 96% in line with current evidence. There was no detrimental effect demonstrated in our patient cohort and performing an OTC in all patients undergoing LC continues to be our departmental policy.
Key statement: The benefits of performing on-table cholangiography have been well documented with clarity of anatomy, the potential for picking up missed stones and avoiding risks of ERCP. With no significant impact on procedural duration or complications, can we really justify and afford the potential risks and cost of not performing OTC?

P41
SUBJECTIVE REPORTS OF VISUAL FATIGUE WHILE PERFORMING MINIMALLY INVASIVE SURGICAL SKILLS USING PASSIVE POLARISING 3D DISPLAYS
Author(s): R Smith, A Day, T Rockall, M Bailey, I Jourdan Presenter: R Smith Institution: MATTU, Guildford, UK
Aims: 3D passive polarising displays have been shown to significantly improve performance of minimally invasive surgical skills in simulated settings. This study investigates the subjective viewing experience for surgeons performing minimally invasive surgical skills using passive polarising 3D displays.
Methods: 20 novice and 20 expert surgeons were randomised to perform a series of sequential repetitions of standardised surgical skills tasks using 2D followed by 3D, or in the reverse order. Participants completed a visual symptom severity questionnaire comprising 27 items (ranked 1-7) following the 2D and 3D sessions.
Results: Median total visual fatigue severity scores for novice surgeons following the 2D vs. 3D skills sessions were 35.5 (IQR 33-48.25) vs. 36.0 (IQR 31.25-42.75), P= 0.305. Interestingly, there was a significant reduction in visual fatigue severity scores for experienced surgeons following the 3D compared to the 2D session.
Conclusion: Viewing the passive polarising 3D display did not induce additional adverse visual symptoms in this study. The subjective viewing experience is equivocal to a high definition 2D display while performing minimally invasive surgical skills. We anticipate that 3D passive polarising displays will have acceptable image quality for minimally invasive surgical procedures.
Key statement: Passive polarising 3D displays have significantly improved viewer tolerance levels compared to previous 3D projection systems and are equivocal to a high definition 2D display in simulated settings.

P42
NEEDLESCOPIC LAPAROSCOPIC TECHNIQUE IN APPENDICECTOMY: IS IT WORTH IT?
Author(s): H Lee, K Ramdoo, A Bassi, O Warren, S Warren Presenter: H Lee Institution: Barnet & Chase Farm Hospitals NHS Trust, UK
Aims: This study investigates using a needlescopic laparoscopic technique in place of a 5mm supraumbilical port during laparoscopic surgery for acute appendicitis. Needlescopic appendicectomy (NA) may have potential benefits of minimal scarring, reduced port size and thus potentially less postoperative pain.
Methods: The study analysed prospectively collected data on sequential patients undergoing NA and LA performed by a single laparoscopic surgeon from 2008 to 2012. Information was collected on duration of procedure, number of days requiring analgesia post operatively and time to return to normal activities.
Results: 17 patients underwent NA and15 LA. Mean age was 34 and 36 respectively. Comparative mean operative time was not statistically significant (= 0.48), 43mins for NA and 32mins for SA. Analgesia requirements post operatively were similar in both groups (=0.25) as was time to return to normal activities (=0.45).
Conclusion: NA took no longer than LA and is equally feasible. Although cosmesis is marginally improved, there was no advantage in terms of post-operative analgesia requirements and time to return to normal activity, probably because this young group of patients are likely to do well whatever the surgical approach.
Key statement: Needlescopic appendicectomy is comparable to laparoscopic appendicectomy in terms of safety and efficacy but confers little advantage for appendicectomy. The use of needlescopic instruments allows laparoscopic surgeons to refine their increasingly minimally invasive techniques.

P43
ACCEPTABILITY AND FEASIBILITY OF VIDEO HOSTING WEBSITE (YOUTUBE®) FOR FEEDBACK PROVISION IN LAPAROSCOPIC SURGICAL TRAINEE: RESULTS OF A PILOT STUDY
Author(s): M Riaz1, M Tang
1, R Welbourn
1,2, I Tait
1, A Alijani
1
Presenter: M Riaz Institution:
1Cuschieri Skill Centre, Ninewells Hospital and Medical School, Dundee, UK,
2Musgrove Park Hospital, Somerset, UK
Aims: To analyse the acceptability and feasibility of Video feedback provision through video hosting website YouTube
®, in order to improve learning outcomes in laparoscopic training
centres.
Methods: Twenty international surgeons performed a laparoscopic enterotomy closure task with video recording during intermediate laparoscopic skills course. Video and paper feedbacks were created. An email was sent to each trainee with a file attached as PF and an online reference of VF, uploaded on YouTube
®. Candidates completed Likert scale survey.
Results: 80% candidates strongly agreed to the training approach and assessment process. 90% strongly agreed to VF as a method of choice for error identification and correction through better understanding as compared to 10% agreeing to PF (<0.001). 20/20 (100%) candidates strongly agreed to YouTube® as a method of feedback provision.
Conclusion: Video feedback method is strongly favoured among international surgical trainees when provided through YouTube
® for laparoscopic task performance during a training course.
Key statement: The demand of laparoscopic surgical training is growing internationally. Video feedback of any laparoscopic task learnt during a course can be provided through YouTube
®. It
provides a source for continuous learning and facilities like geographical analysis could be a valuable resource for estimating the international influence of a training centre.

P44
A SYSTEMATIC REVIEW AND META-ANALYSIS OF LAPAROSCOPIC COMPARED WITH OPEN RESTORATIVE PROCTOCOLECTOMY
Author(s): P Singh1, A Bhangu
2, R J Nicholls
3,4, P Tekkis
2
Presenter: P Singh Institution:
1Faculty of Medicine, Imperial College, London, UK,
2Department of Colorectal
Surgery, The Royal Marsden Hospital, London, UK, 3Department of Surgery, St.
Mark’s Hospital, Harrow, UK, 4Department of Biosurgery and Surgical
Technology, Imperial College, London, UK
Aims: The benefits of a laparoscopic approach to restorative proctocolectomy (RPC) are controversial. The aim of this meta-analysis was to compare the outcome following laparoscopic and open RPC, with particular attention to adverse events and long-term function.
Methods: A systematic search of the MEDLINE, EMBASE and Ovid databases was performed for studies published until March 2012. The primary endpoint was long-term function. Secondary endpoints were intra-operative details and short-term post-operative outcome and post-operative adverse events. Weighted mean difference (WMD) and odds ratio (OR) were calculated using meta-analysis.
Results: 27 studies of 2428 patients, of whom 1097 (45.1%) underwent laparoscopic surgery were included. Laparoscopic RPC was associated with fewer nocturnal bowel movements (<0.05), reduced pad usage (<0.001), longer operation (<0.001), shorter hospital stay (<0.001), and lower incidence of wound infection (<0.005). There was no difference in pouch failure rate.
Conclusion: A laparoscopic approach led to only a slight improvement in long-term function amongst these non-randomised studies. Both approaches led to a similar incidence of adverse events.
Key statement: Laparoscopic RPC resulted in similar daily bowel function but slightly reduced nocturnal bowel frequency and pad usage compared with open surgery. Although the long-term adverse events (e.g. pouch failure) were similar, the pooled results from included studies may be underpowered to detect significant differences.

P45
RANDOM COLONIC BIOPSIES AT ENDOSCOPY: ARE THEY WORTHWHILE?
Author(s): Eleanor Katherine Harrison, Krishan Ramdoo, Henry Lee, Stephen Warren Presenter: E K Harrison Institution: Chase Farm Hospital, London, UK
Aims: Random colonic biopsies are often taken at endoscopy in patients with chronic diarrhoea to rule out a diagnosis of microscopic colitis. This study aimed to examine the diagnostic yield of such biopsies and the subsequent clinical value of the information gained when considered in the light of their economic cost.
Methods: A prospective record of endoscopic random biopsies at Chase Farm Hospital over a 12 month period (01/09/11 to 31/08/12) was correlated with pathology reports. These biopsies were analysed with respect to both their indication and result. The economic cost was estimated using figures from the Histopathology and Endoscopy departments.
Results: 210 endoscopic random colonic biopsies were performed: 71.9% for chronic diarrhoea and 28.1% for rather ‘nebulous’ variable indications. Only 1.9% of biopsies showed microscopic colitis, of which none were from the group with nebulous indications. The estimated additional cost of performing and analysing these biopsies was £25,200 (€31,248/$40,824) per annum.
Conclusion: This study demonstrates that the diagnostic yield of random colonic biopsies performed at endoscopy is very low and that their additional economic cost is high. Furthermore, this study shows that a large proportion of these biopsies were performed for indications that are incongruous with the diagnostic criteria for microscopic colitis.
Key statement: We question the economic and clinical diagnostic value of random colonic biopsies at endoscopy where no macroscopic disease is seen.

P46
COMPARISON OF ANASTOMOTIC COMPLICATIONS BETWEEN TOTALLY-ROBOTIC AND ROBOTIC-ASSISTED WITH CONVENTIONAL LAPAROSCOPY IN GASTRIC BYPASS SURGERY: A SYSTEMATIC REVIEW
Author(s): R Goriparthi1,3
, S Makkiyah1,3
, SJ Sarker1,3
, H Patel1,3
, B Patel1,2
Presenter: R Goriparthi Institution:
1Barts Cancer Institute, London, UK,
2Barts and the Royal London, UK,
3Queen
Mary University of London, UK
Aims: To compare totally-robotic and robotic-assisted surgery with conventional laparoscopy (CL) in terms of complications, conversions and equipment setup time in gastric-bypass surgery.
Methods: Following PRISMA 2009 guidelines, literature search was performed in PubMed and Cochrane databases. General inclusion criteria were English articles, from year 2000, humans, adults (>18yrs), Roux-en-y gastric bypass and sample size >5. Specific inclusion criteria were da Vinci systems for robotic surgery (RS) and randomized clinical trials (RCT’s) for CL.
Results:
• 21 RS studies (n=2529) and 26 RCT’s in CL (n=2143) were reviewed.
• Complication rate in RS vs. CL for anastomotic stricture was 1.22% vs. 5.97%, anastomotic leak was 0.28% vs. 1.08%, where the difference was statistically significant (<0.01). Gastro-gastric fistula rate in RS vs. CL was 0.12% vs. 0.23% and marginal ulcer rate was 0.94% vs. 1.3%, difference for both was statistically insignificant.
• Conversion rate in RS vs. CL was 0.74% vs. 0.93%. Mean equipment setup time in RS was 15.64mins and no studies from CL contributed to this parameter.
Conclusion: Strictures and anastomotic leaks were significantly low in RS, which were mostly hand sutured anastomosis compared to stapled anastomosis of CL. Other outcome measures were similar for both groups with RS showing a trend towards lower complication rates.
Key statement: Conventional laparoscopy is gold standard operation for bariatric patients. Our study has shown a trend towards fewer anastomotic related complications following robotic-sutured compared to laparoscopic-stapled anastomosis. A well conducted randomized-control study should explore this benefit of robotic surgery including cost analyses.
P47
COMPARISON OF SURGICAL OUTCOMES BETWEEN TOTALLY-ROBOTIC AND CONVENTIONAL LAPAROSCOPY IN GASTRIC BYPASS SURGERY: A SYSTEMATIC REVIEW
Author(s): R Goriparthi1,3
, SJ Sarker1,3
, S Makkiyah1,3
, W Elbakbak1,3
, B Patel1,2
Presenter: R Goriparthi
Institution: 1Barts Cancer Institute, London, UK,
2Barts and the Royal London, London, UK,
3Queen Mary, University of London, London, UK
Aims: To compare complications, conversions, operative time, duration of hospital stay and mortality rate between totally-robotic technique (TRT) and conventional laparoscopy (CL) in gastric-bypass surgery.
Methods: Following PRISMA 2009 guidelines, literature search was performed in PubMed and Cochrane databases. General inclusion criteria were English articles, from year 2000, humans, adults (>18yrs), Roux-en-y gastric bypass and sample size >5. Specific inclusion criteria were da Vinci systems for TRT and randomized clinical trials (RCT’s) for CL.
Results:
• 4 TRT studies (n=158) and 26 RCT’s in CL (n=2143) were reviewed.
• Complication rate in TRT vs. CL for anastomotic leak was 0% vs. 1.07%,
anastomotic stricture was 3.16% vs. 5.97%, bowel obstruction was 0.63% vs.
1.95%, internal hernia was 0.63 vs. 0.74% and bleeding requiring intervention was
0% vs. 1.63%. None of the above outcome measures were statistically significant.
• TRT had significantly high (<0.01) operative times (184.61 vs. 145.94mins) and
conversion rates (9.49% vs. 0.93%).
Conclusion: Patient outcomes were similar in both groups with TRT showing a trend towards fewer complications compared to CL even though not statistically significant. However, TRT had longer operative times and high conversion rate to both open and conventional laparoscopy.
Key statement: Robotic gastric bypass is as effective as conventional laparoscopy. Our study demonstrated a trend towards fewer complications following totally-robotic surgery, even though statistically insignificant. However, robotic surgery had longer operative time and higher conversion rate. A well conducted randomized-control study should explore this benefit of robotic surgery including cost analyses.

P48
SHOULD WE BE MOVING TOWARDS NEEDLESCOPIC LAPAROSCOPIC SURGERY?
Author(s): M Stubbs, E Rizal, B Stubbs, H Lee, O Warren Presenter: M Stubbs Institution: Chase Farm Hospital, London, UK
Aims: This feasibility study aimed to investigate whether needlescopic laparoscopic cholecystectomy (NLC) with routine intra-operative cholangiogram had advantages over the standard three-port laparoscopic technique (3LC) used in our practice.
Methods: We compared consecutive needlescopic cholecystectomies with conventional laparoscopic cholecystectomies performed by a single surgeon and anaesthetist. Data included operative duration, analgesic requirements, patient scar satisfaction, time to return to normal daily activities (TRNDA) and complication rates.
Results: 51 patients underwent NLC and 43 3LC with no differences in age, BMI, operative time and TRNDA. NLC patients required significantly less analgesia (=0.04). All patients found the needlescopic scar cosmetically appealing. Overall there were no conversions and all NLCs were completed without additional ports. There was one needleport infection.
Conclusion: NLC with intraoperative cholangiogram is feasible in an unselected consecutive series of patients without prolonging operative time. It has the advantages of improved cosmesis and reduced requirements for post-operative analgesia, with similar time taken to return to normal daily activities.
Key statement: Needlescopic laparoscopic cholecystectomy with cholangiogram is no more difficult than three port laparoscopic cholecystectomy and may help laparoscopic surgeons move stepwise towards less invasive minimal access techniques such as single-port laparoscopic surgery.

P49
IMPROVING THE GOLD STANDARD: ETHICON ATS STAPLED PANCREATIC STUMP CLOSURE MAY REDUCE PANCREATIC FISTULA RATES AFTER LAPAROSCOPIC DISTAL PANCREATECTOMY
Author(s): S Sahay, P Lykoudis, S Rahman Presenter: S Sahay Institution: Royal Free London NHS Foundation Trust, UK
Aims: To compare clinical outcomes of laparoscopic versus open distal pancreatectomy for presumed benign lesions of the pancreas in a single institution.
Methods: Prospective audit of consecutive patients undergoing distal pancreatectomy for presumed non-malignant lesions of the pancreas either laparoscopically (LDP) or open technique (ODP). Clinico-pathological outcomes were analysed: Operative time, blood loss, pancreatic fistula rates (ISGF classification), hospital stay and method of stump closure. Histopathological parameters included size and pathology of lesion, resection margin clearance, and lymph node harvest.
Results: There were 17 patients in the LDP and 22 in the ODP group. LDP was associated with significantly higher spleen preservation rates (54 v 5%, =0.002), shorter operative times (180 v 240 mins, =0.013), and a shorter hospital stay (6 vs 11 days, =0.002). Pancreatic fistula rates were 5.6 % and 33.3% in the LDP and ODP group respectively (=0.05, Fishers Exact Test).
Tumour clearance rates, nodal harvest, and pathology types were comparable.
Stapled stump closures were used in all patients undergoing LDP (Ethicon ATS EndoFlex 2.5mm compression) and 32 % of ODP (Echelon EndoFlex 2.5mm). Among the vascular stapled stump closure group, the Ethicon ATS method was associated with shorter hospital stay (<0.001) and a tendency for reduced pancreatic fistulas (=0.059).
Conclusion: Laparoscopic distal pancreatectomy should be accepted as the gold standard for left sided pancreatic resections. Pancreatic stump closure using the Ethicon ATS may be associated with significantly reduced pancreatic fistula rates by providing a mechanical difference in the degree of compression.
Key statement: We report significantly reduced pancreatic fistula rates and outcomes following laparoscopic distal pancreatectomy.

P50 A RANDOMISED CONTROLLED TRIAL TO ESTABLISH THE EFFECT OF ARTICULATING INSTRUMENTS UPON PERFORMANCE IN SINGLE INCISION LAPAROSCOPIC SURGERY Author(s): H Corker
1,2, P Singh
1, M Sodergren
1, S Balaji
1, P Paraskeva
1
Presenter: H Corker Institution:
1Imperial College London, UK,
2Newcastle University, UK
Aims: Single Incision Laparoscopic Surgery (SILS) is a novel approach presenting unique technical challenges. Articulating instruments may counter these but heterogeneity exists within the literature as to their benefit. This randomised controlled trial aimed to evaluate the effect of articulating instruments upon performance in SILS. Methods: Surgeons used two straight (STR), one articulating and one straight (STR-ART) or two articulating instruments (ART). After baseline testing, they completed the Fundamentals of Laparoscopic Surgery (FLS) peg transfer task (PEG) 25 times. Maximum FLS scores and hand motion analysis assessed performance. NASA Raw Task Load Index (RTLX) assessed workload. Results: Twenty-one surgeons participated; STR (n=7), STR-ART (n=7) or ART (n=7). Baseline FLS scores were similar (=0.63). STR-ART achieved higher maximum FLS scores than STR or ART (239 vs. 228 vs. 210, respectively, =0.002). Path length, number of hand movements and NASA RTLX scores were similar (=0.55, =0.08, =0.708, respectively). Conclusion: The use of STR-ART conferred improved SILS performance when surgeons undertook a SILS-validated FLS task. This is in spite of not requiring any significant alteration in hand movements or proving any more taxing in terms of workload. STR-ART may, therefore, be the optimum instrument configuration for clinical SILS. Key statement: SILS is a novel technique for which no consensus exists over optimal instrumentation. A randomised controlled trial was conducted. Surgeons using one straight and one articulating instrument demonstrated improved SILS performance over those using either two straight or two articulating instruments. This configuration may, therefore, be promising in clinical SILS.

P51
A RANDOMISED CONTROLLED TRIAL TO EVALUATE THE IMPACT OF INSTRUMENT AND LAPAROSCOPE LENGTH ON PERFORMANCE IN SINGLE INCISION LAPAROSCOPIC SURGERY
Author(s): S Balaji, P Singh, M Sodergren, H Corker, P Paraskeva Presenter: S Balaji Institution: Imperial College London, UK
Aims: Single Incision Laparoscopic Surgery (SILS) is a technique to further reduce the invasiveness of laparoscopic surgery. While it offers cosmetic benefits, ergonomic difficulties are created by instrumentation entering adjacent to each other. This randomised controlled trial evaluated whether varying instrument and laparoscope length could overcome some of these technical challenges.
Methods: Surgeons were randomised; Group 1 (1 long/1 standard grasper), Group 2 (long laparoscope/standard graspers) and Control (2 standard graspers/ standard laparoscope). They performed 25 repetitions of the validated peg-transfer task from the Fundamentals of Laparoscopic Surgery (FLS) program. Performance was analysed using FLS parameters, hand motion-tracking and the NASA-TLX workload questionnaire.
Results: Twenty four surgeons were recruited. No significant differences were found between groups for baseline performance and operative experience. Peak performance was higher in Group 1 compared to control (P<0.05). Workload assessment demonstrated that group 2 perceived higher performance than control (<0.05). Hand motion-tracking parameters demonstrated no significant differences across groups.
Conclusion: This study demonstrates that by varying instrument length, SILS performance can be improved. The combination of 1 long and 1 short instrument conferred the highest performance.
Key statement: Varying instrument and laparoscope length are simple, low cost techniques to overcome the technical challenges of SILS procedures. This study objectively demonstrates an improvement in SILS performance through use of these methods.

P52
THE ROLE OF LAPAROSCOPY IN THE MANAGEMENT OF ACUTE ABDOMEN
Author(s): S Smith, M Al-sheikh, H Toghyan, H Khout Presenter: S Smith Institution: Queen Elizabeth Hospital, Gateshead, Tyne and Wear, UK
Aims: Laparoscopic operations have become more popular in approaching general surgical emergencies. This has led to increased demand on training surgeons and nursing staff to utilize laparoscopic instruments. The aim the study is to audit the prevalence and indication of laparoscopic intervention as an abdominal emergency operation in our hospital.
Methods: 456 patients underwent abdominal emergency operation for the period between August 2011 and August 2012. Data collected using computer software and patients case notes.
Results: 239 (52.41%) patients underwent laparoscopic operation. This represents more than half of the total number of abdominal emergency operations. In 121 (12.6%) patients, the indication for the surgery was diagnostic laparoscopy for right side pain.30 patients had laparoscopic cholecystectomy. Out of 239 laparoscopic operations, 6 (0.625%) converted to open.
Conclusion: Laparoscopy has become an established method for approaching acute abdomen. Most of the cases in this study were for diagnostic laparoscopy, appendicectomy and cholecystectomy. This has an implication on surgical as well as nursing training.
Key statement: Laparoscopic intervention is getting more popular recently in treating acute abdominal emergencies. Early training of the junior surgeons and nursing staff is recommended to achieve the required laparoscopic skills.

P53
DIAGNOSTIC LAPAROSCOPY VS ULTRASOUND SCAN: WHICH IS BETTER IN THE MANAGEMENT OF RIGHT ILIAC FOSSA PAIN?
Author(s): S Smith, M Al-sheikh, H Khout, H Toghyan, T Fasih Presenter: S Smith Institution: Queen Elizabeth Hospital, Gateshead, Tyne and Wear, UK
Aims: The aim of this study is to assess whether ultrasound scan or diagnostic laparoscopy represent a more accurate procedure to diagnose acute appendicitis in female patients presenting with right iliac fossa pain.
Methods: We reviewed the medical notes for all female patients presented to the surgical unit with right iliac fossa pain for the period from August 2011 to August 2012. Data was collected retrospectively
Results: 61 patients underwent diagnostic laparoscopy and laparoscopic appendicectomy. 45 out of 61 (73.7%) had final pathological report confirming acute appendicitis. While the sensitivity and specificity of the abdominal ultrasound scan in our study was 47.05% and 92.3% respectively.
Conclusion: Although ultrasound scan can represent a cheep non invasive diagnostic tool, the accuracy of this scan is still not as good as diagnostic laparoscopy. In addition, laparoscopy can provide both a valuable diagnostic tool and therapeutic intervention at the same time
Key statement: Diagnostic laparoscopy is more invasive procedure than Ultrasound scans. However it is, more accurate in the diagnosis of acute appendicitis in female patients presenting with right iliac fossa pain.

P54
SUCCESSFUL LAPAROSCOPIC SIMULATOR TRAINING: LOCALLY ACCESSIBLE AND TARGET-BASED Author(s): M Pellen, B Dobbins Presenter: M Pellen Institution: Huddersfield Royal Infirmary, UK
Aims: Laparoscopic surgery requires psychomotor skills with definite learning curves. Repetitive practise can achieve expert-defined targets which lead to improved intra-operative performance. Simulator training is inconsistent across the UK and uptake poor when resources available. We sought to evaluate participation in a simulator curriculum applying best-evidenced principles in a District Hospital. Methods: Over 12 months, pre-HST trainees were enrolled in a structured, open access programme on the iSurgicals laparoscopic simulator. All received induction, explicit target criteria, open access to the simulator and feedback. Primary outcome was achievement of median expert performance on three tasks. Learning curve and participant questionnaire data was analysed. Results: 11/12(91.7%) trainees used the single simulator subsequent to induction. 9/12 trainees found all tasks of training benefit. Most trainees used the simulator between theatre cases (67%), lunchtime (50%) or after work (33%). Expert criterion levels were achieved in two tasks by 42% trainees and one task by 17%. Conclusion: Provision of an inexpensive laparoscopic simulator with defined targets results in engaged trainees who can feasibly achieve expert-defined targets through drills practise on site and within their post. Induction, feedback and availability of a simulator within an accessible environment promotes successful uptake of a valuable training tool with measurable outcomes. Key statement: Laparoscopic training can be achieved through continuous simulator programmes delivered locally and affordably so long as key principles are applied.

P55
SUCCESSFUL IMPLEMENTATION OF A “PROACTIVE IMPROVEMENT STRATEGY” CHECKLIST TO INCREASE RATES OF DAYCASE LAPAROSCOPIC CHOLECYSTECTOMY IN A DISTRICT GENERAL HOSPITAL
Author(s): K Mann, M Graham, S Purlackee, A Ray, A Kaul, P Kuduvalli Presenter: K Mann Institution: St. Helens & Knowsley Teaching Hospitals NHS Trust, Merseyside, UK
Aims: Laparoscopic cholecystectomy has been widely accepted as a day case procedure but many trusts struggle to attain this. Techniques have been described to reduce pain and immediate/early complications from surgical and anaesthetic perspectives. We evaluated our theatre practices, targeting areas of improvement, to create and implement a “Proactive Improvement Strategies” (PIS) checklist.
Methods: A cohort of patients who had LC in 2009 were retrospectively reviewed. Various anaesthetic/surgical techniques were highlighted that delayed discharge. These PIS were preoperative motivation, intraoperative antiemetics, multimodal analgesia, regional blockade, specific postoperative instructions and staff education. We re-evaluated outcomes over a nine month period in 2011 to assess the impact of PIS.
Results: 329 vs 36 cases were reviewed (Pre-PIS vs PIS). Causes for delayed discharge were inadequate analgesia, post operative nausea/vomiting, and drain removal. 3 patients (1%) were discharged within 24hrs pre-PIS vs 23 (64%) post PIS (<0.05). Readmission rates were 18 (5.5%) vs 0 (=0.236, Pre-PIS vs PIS). Median length of stay was 2 days (pre.PIS) and 1 days (post PIS) <0.05. There were no significant differences in conversion to open rates (2 vs 10, =0.134) and there were no bile duct injuries in either group.
Conclusion: We have achieved significant improvements in day-case discharge for LC with our systematic, structured, team-based implementation of PIS. We plan to build on this and evaluate the known risk factors for complex LC and pre-empt possible complications.
Key statement: Day case laparoscopic cholecystectomy has now developed into a well estblished day case procedure. There are many smaller institutions that have not been able to achieve this and we provide a checklist of improvements that make this more feasible from surgical and anaesthetic perspective.
P56
CLINICAL EVALUATION OF SAFETY AND EFFICACY OF A NEW LAPAROSCOPIC ENERGY DEVICE (THUNDERBEAT)
Author(s): J Tuynman, M Buckingham, S Folkard, R Guy, N Mortensen Presenter: J Tuynman Institution: Oxford University Hospitals, UK
Aims: The introduction of the laparoscopic energy device Thunderbeat combines ultrasonic and electrical bipolar energy and has potential advantages in laparoscopic surgery. The aim of the clinical trial of was to clinically evaluate efficacy and safety of the Thunderbeat in patients undergoing laparoscopic colonic resections
Methods: From October 2011 until January 2012 a consecutive cohort of 180 patients undergoing laparoscopic colonic resections was evaluated. In 58 cases Thunderbeat was employed. In 122 patients other energy devices according surgeons preference were used. Emergency cases were excluded. Data were prospectively collected; intention to treat analysis was performed.
Results; No significant differences in sex, age, ASA grading, or BMI in both groups. Median operation time (03:27 versus 03:21, =0.640,) blood loss (60 versus 90ml,=0.096), and intraoperative complications (3% versus 9%, =0.187) were comparable (Thunderbeat versus control). In procedure matched analysis Thunderbeat was associated with trend for shorter operation times (=0.069) and less bloodloss (=0.066).
Conclusion: We have shown in a clinical trial that the Thunderbeat instrument is safe and effective in laparoscopic colonic resection. There were no significant peroperative parameters in the total group whereas trends for faster procedure time and less bloodloss were observed in matched case analysis
Key statement: This is the first clinical trial evaluating the new laparoscopic energy device, Thunderbeat. We compared the use of thunderbeat in 58 colonic resections versus 122 control patients. The Thunderbeat has shown to be safe and effective.

P57
NURSE PRACTITIONER LED DISCHARGE IMPROVES DAY CASE RATE FOR ELECTIVE LAPAROSOPIC CHOLECYSTECTOMY
Author(s): N C Law Presenter: N C Law Institution: Wrightington Wigan and Leigh NHS Trust, Greater Manchester, UK
Aims: Day case laparoscopic cholecystectomy carries huge financial incentive to acute trusts as patients are discharged on the same day. The study aims to compare the day case and readmission rate when nurse practitioner led discharge is being implemented in a district general hospital.
Methods: A pilot study for nurse led discharge was conducted during July and August 2012, involving 16 patients in total. Patients with ASA I and II were included. A proforma is filled in by a nurse for every patient prior discharge and any readmission within 30 days will be highlighted.
Results: 15 out of 16 patients involved in the study were discharged on the same day, achieving day case rate of 93%. 1 patient was readmitted for uncontrolled pain and nausea. This is a significant improvement from previous audit result (day case rate 21.5%, readmission rate 3.7%; n=273).
Conclusion: This study demonstrates that nurse led discharge is safe and cost effective. Future re-auditing is needed as pilot study involved limited amount of patients.
Key statement: Nurse practitioner led discharge is proven to be safe and helps to improve day case rate of elective laparoscopic cholecystectomy in a district general hospital.

P58
STRIVING TO IMPROVE OUTCOMES FOR ACUTE PANCREATITIS: THE FIRST STEP
Author(s): R Cave, W Cook, P Chana, J Warbrick-Smith, J Hewes Presenter: R Cave Institution: North Bristol Trust, UK
Aims: The aim of this audit is to assess compliance with the British Society of Gastroenterologists (BSG) guidelines in the management of acute pancreatitis at our trust. This will quantify a baseline performance level which we will then attempt to improve.
Methods: The first 50 patients admitted in 2011 with acute pancreatitis were selected. Audit standards were taken directly from the guidelines and electronic and paper notes were retrospectively reviewed.
Results: 70% of patients were severity scored during the first 48 hours of their admission (BSG standard: 100%). 8/50 patients were diagnosed with severe pancreatitis, yet only two of those patients were discussed with intensive care.
3/20 patients with gallstone pancreatitis underwent an inpatient laparoscopic cholecystectomy. Seven patients underwent outpatient cholecystectomy.
Conclusion: This audit demonstrates variability in the adherence to the BSG recommendations in our trust. The proportion of patients with gallstone pancreatitis undergoing laparoscopic cholecystectomy either as an inpatient or within two weeks of discharge is suboptimal.
Key statement: The aim of this audit is to assess compliance with the British Society of Gastroenterologists (BSG) guidelines in the management of acute pancreatitis at our trust.This audit demonstrates variability in the adherence to the BSG recommendations. In order to improve clinical practice and outcomes we have designed a pancreatitis pathway.

P59
FEMALE GENDER AND DIABETES INCREASE THE RISK OF RECURRENCE FOLLOWING LAPAROSCOPIC INCISIONAL HERNIA REPAIR
Author(s): Steve Hornby, Frank McDermott, Mark Coleman Presenter: S Hornby Institution: Plymouth Hospital NHS Trust, UK
Aims: To determine, with data gathered from the Severn and Peninsula Audit and Research Collaborative (SPARCS), the risk factors for recurrence in laparoscopic incisional hernia repair. To test the hypothesis that laterality or proximity to the xiphoid process and pubis leads to increased recurrence.
Methods: A co-ordinated multi-centre review of laparoscopic incisional hernias at six sites in the Southwest was performed, encompassing January 2004 to December 2009. A retrospective review of case notes and a structured telephone follow-up was completed. A logistic regression was fitted with recurrence as the primary outcome.
Results: 186 cases (91 female) were identified. Telephone interview was achieved in 115/186 (62%). Logistic regression suggested that only female sex (odds ratio (OR) 3.32 (95%CI;1.15-9.62) and diabetes
OR=6.95 (95%CI;1.61-29.99) increase the risk of recurrence. Position of the defect has no effect.
Conclusion: This analysis suggests an increased risk of recurrence following laparoscopic incisional hernia repair in females and diabetics. This will help to inform surgeons and patients when considering laparoscopic management of incisional hernias. SPARCS recommends the use of centrally hosted prospectively kept national/international databases to robustly study such findings.
Key statement: Females and diabetics have an increased risk of recurrence following laparoscopic incisional hernia repair.

P60
THE IMPORTANCE OF ENHANCED RECOVERY WHEN CONDUCTING COMPARISONS BETWEEN LAPAROSCOPIC AND OPEN PROCEDURES USING OESOPHAGECTOMY AS AN EXAMPLE
Author(s): M Ghisel, R Brickwood, N Patel, S Andrews, R Berrisford, J Rahamim, T Wheatley, G Sanders Presenter: M Ghisel Institution: Derriford Hospital, Plymouth, UK
Aims: It is unknown if performing the abdominal component of a two stage oesophagectomy laparoscopically provides advantage in terms of reduced length of hospital stay. This study compares patients with open and laparoscopic abdominal components (hybrid) before and after introduction of enhanced recovery programme.
Methods: A retrospective analysis of patients undergoing 2 stage Ivor Lewis oesophagectomy was performed during two time periods, pre enhanced recovery (January 2010 and September 2011) and within enhanced recovery (October 2011 and June 2012).
Results: The results are illustrated in the table below.
Conclusion: There was no significant difference in length of stay between the laparoscopic and open groups. However, enhanced recovery significantly reduced the length of stay within the open (14 to 11 days =0.002) and laparoscopic (12 to10 days =0.009) groups.
Key statement: All studies comparing laparoscopic with open procedures, with length of stay as an outcome measure, should be performed within and enhanced recovery program as this significantly reduces length of stay independently.
Enhanced Recovery
n Abdominal Phase Length of Stay Days
Median (Range)
Pre ERAS 143 Open 98
14 days (8-47)
Laparoscopic 45
12 days (8-57)
Within ERAS 28 Open 9
11 days (6-34)
Laparoscopic 19
10 days (7-51)
P61
WHY USE 4 WHEN YOU CAN USE 3? MINIMISING INVASION
Author(s): H Lee, K Ramdoo, M Stubbs, K Harrison, S Warren Presenter: H Lee Institution: Chase Farm Hospital, London, UK
Aims: Traditional training advocates using four large sized ports for laparoscopic anterior resection, but gradually laparoscopic colorectal surgeons are aware of the benefits of becoming less invasive. We have always used a 3-port technique (two 5mm and one 12mm ports) and describe our experiences of this approach.
Methods: Prospectively collected data on a consecutive case series of a single surgeon’s laparoscopic anterior resections for cancer with and without chemoradiotherapy, were analysed from November 2002 to the present, including age, sex, surgery length, BMI, hospital stay, complications and whether a 4th-port was required. Open conversions were excluded.
Results: 48 patients completed laparoscopic surgery; 86% with three ports (46% males),14% requiring an additional 5mm port (71% male pelvis). 3-port surgery took 193 minutes with no significant differences with a fourth port (196), nor mean age, BMI and recovery time. The 4-port group had 2 anastomotic leaks with one death.
Conclusion: Small-sized 3-port laparoscopic anterior resection is usually achievable and rarely requires a 4
th port. Addition of this port, if required (more frequently with a male pelvis, though
not BMI dependant), does not result in increased operative time or recovery time, though complication rates in this small group are higher.
Key statement: Although the use of a 4th port may be useful during initial training, surgeons
with advanced laparoscopic skills should consider ‘downsizing' to a small-sized 3-port technique to minimize invasion.

P62
LAPAROSCOPIC MANAGEMENT OF GALL STONE PANCREATITIS IN THE ELDERLY WITHOUT MRCP OR ERCP IS SAFE AND FEASIBLE
Author(s): S Zino, A Mirza, K Nassar, J Geoff, A Nassar Presenter: S Zino Institution: Monkland Hospital, Glasgow, UK
Aims: Surgical management of gall-stone pancreatitis (AGSP) in the elderly is a challenge. We aimed to assess single-session laparoscopic management of pancreatitis in patients ≥ 70 years.
Methods: Prospectively collected data for patients undergoing laparoscopic biliary surgery over 20 years (N=3361) was analysed. We reviewed the data for patients aged ≥ 70 years with AGSP.
Results: A total of 36 patients were identified. The mean age was 75 years. 75% were females. 97% were emergency admissions, and 53% were jaundiced. ASA score was 2 in 36% and 3 in 33%. Initial conservative management was followed by surgery in the majority according to the protocol. MRCP was requested in two cases and only one patient underwent ERCP prior to referral to the biliary firm. We perform Intra-operative cholangiography routinely. CBD stones were identified in 7 cases (19%); all extracted laparoscopically.. The mean surgical time was 60 mins (16 to 185 mins). The average inpatient hospital stay was 7 days (3 to 40 days). All but one patient were treated during the index admission. There were no post-operative complications, readmissions or deaths.
Conclusion: One–session management of pancreatitis in elderly patients is preferable to and safer than staged management. Laparoscopic bile duct exploration can be performed when necessary, allowing optimal utilisation of resources such as MRCP and ERCP. It reduces hospital stay, number of admissions and presentation to resolution intervals.
Key statement: Acute Gallstone pancreatitis in the elderly can be safely managed surgically according to the guidelines, without preoperative endoscopic intervention.

P63
LAPAROSCOPIC LIGATION OF TYPE II ENDOLEAKS POST ENDOVASCULAR ANEURSYM REPAIR (EVAR): CURRENT EVIDENCE FOR PRACTICE – A SYSTEMATIC REVIEW
Author(s): T Marjot1, A Choong
1, K Patel
1,2, V Bhrugubanda
1,2, S Renton
1
Presenter: T Marjot Institution:
1Northwick Park Hospital, Middlesex, UK,
2Imperial College School of Medicine,
London, UK
Aims: Type II endoleak complicates 10-25% of EVAR. Although the clinical significance of type II endoleak remains contentious, the strategies used for its management have continued to expand. We systematically review the literature and comprehensively appraise the effectiveness of laparoscopic intervention in the management of this common complication.
Methods: Review methods were according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Published literature from five electronic databases was searched. Studied outcomes included patient demographic, aneurysm type, graft type, endoleak type, previous endovascular embolization attempted, vessel ligated laparoscopically, length of stay and follow up duration.
Results: 9 studies representing 19 patients were investigated. Mean age was 57.7. All patients were ASA II and above. All underwent standard infrarenal EVAR. 14 patients suffered a type II endoleak from the inferior mesenteric artery. 36.8% (7/19) patients had unsuccessful or were unsuitable for embolization. 30-day mortality was 5.3%
Conclusion: Direct laparoscopic ligation of feeding vessels causing type II endoleak is particularly useful in cases where standard endovascular embolization has failed. It is associated with low 30-day mortality and should be considered an essential tool in the armamentarium of the vascular and laparoscopic surgeon.
Key statement: Type II endoleak is a common complication post EVAR and cannot always be treated by endovascular means such as embolization. Failure to treat can lead to continued sac pressurisation and aneurysm rupture. Direct laparoscopic ligation is a useful adjunct to the armamentarium of the treatment of this condition.

P64
LAPAROSCOPIC LIVER SURGERY: A MAJOR SINGLE-CENTRE UK EXPERIENCE
Author(s): M A Hilal, F Di Fabio, E Dimovska, T Armstrong, N Pearce Presenter: M A Hilal Institution: Hepatobiliary and Pancreatic Surgery, University Hospital Southampton, UK
Aims: Laparoscopic liver surgery is progressively expanding mainly for minor hepatectomy. However, safe expansion of the laparoscopic approach must be supported by critical analysis of data from high-volume laparoscopic liver centers including major hepatectomies and complex cases.
Methods: We reviewed a prospectively collected single-centre database of 320 patients undergoing laparoscopic liver resections between 2003 and 2012. These included patients undergoing laparoscopic multiple redo hepatectomy and 2-stage resections for bilobar colorectal liver metastases.
Results: Of the 320 patients, 161 were female, with a median age of 64 years. The indication for surgery was benign disease in 32% (including: adenoma, cystadenoma, focal nodular hyperplasia, simple and complex cyst, hydatid cyst, and haemangioma) and malignant disease in 68% (including: unilobar and bilobar colorectal carcinoma liver metastases, hepatocellular carcinoma, neuro-endocrine tumour metastases, non-colorectal liver metastases, lymphoma, and intrahepatic cholangiocarcinoma). There were 96 (30%) major resections. The conversion rate was 6%. Median operation time was 190min (range 30-480min). Median intraoperative blood loss was 200ml (range 0-5000ml). Fifty-three patients (16.5%) developed postoperative complications. Postoperative mortality was 1.25% (4/320). The median postoperative hospital stay was 4 days (range 1-21 days). In patients with colorectal liver metastases the proportion of microscopic positive resection margins was 4%.
Conclusion: The laparoscopic approach for liver surgery may be adopted for a large variety of benign and malignant conditions without compromising patient safety and oncological principles. Extensive experience in laparoscopic liver surgery is required in order to preserve the benefits related to the minimally-invasive approach also when major hepatectomies are required.
Key statement: The laparoscopic approach for liver surgery may be adopted for a large variety of benign and malignant conditions without compromising patient safety and oncological principles.

P65
ROBOTIC VERSUS SINGLE INCISION LAPAROSCOPIC COLECTOMY: A SYSTEMATIC REVIEW
Author(s): R B Manohar1,3
, S J Sarker1,3
, W Elbakbak1,3
, B Patel1,2
Presenter: R B Manohar Institution:
1Bart's Cancer Institute, London, UK,
2Bart's and the Royal London Hospital,
UK, 3Queen Mary University of London, UK
Aims: This study is comparing the short-term outcomes (operation time, length of hospital stay, estimated blood loss, conversion rates and complications) of Robotic and Single incision laparoscopic colectomy (SILC). Methods: A systematic search of the literature following PRISMA 2009 guidelines was undertaken to identify relevant articles from 2002 to 2012. English language articles (>10 adult patients) involving both benign and malignant conditions were included. Results: This study included 87 articles with 3879 patients.
N=3879 SILC(n=1597) Robotic(n=2282)
Operative time (minutes) 141.1(75-300) 257(134-385)
Length of hospital stay (days) 6.9 (2.7-9.2) 7.8 (2-17.6)
Blood loss (ml) 75.6(9-140) 82.9 (21-167.3)
Anastomotic leak 2.6% 5.5%
Anastomotic stricture 1.1% 2.9%.
Incisional hernia 2.1% 0.8%.
Conversion rates 5.2% 2.1%
Conclusion: The operation time and anastomotic complications (leak and stricture) were higher in robotic surgery, whereas incisional hernia and conversion rate were higher in SILC. These findings may be a reflection of case selection bias in either group, which is difficult to prove in this review. We can however conclude SILC is a safe technique with a trend towards fewer anastomotic related complications compared to robotic colectomy.
Key statement: Short-term surgical outcomes are more favourable in patients undergoing single incision laparoscopic colectomy compared to robotic colectomy in terms of operating time and anastomotic complications.

P66
CUTTING THE COST: SINGLE PORT LAPAROSCOPIC SURGERY WITH AN IMPROVISED PORT SYSTEM, OUR INITIAL EXPERIENCE
Author(s): A Brookes, T Pinkney, N Suggett, C Keh Presenter: A Brookes Institution: University Hospitals Birmingham NHS Trust, UK
Aims and Methods: Laparo-endoscopic single site surgery (LESS) is an evolving field however a barrier to uptake is the unit of cost of the port systems. We report our initial experience with a previously described port system using an Alexis Wound Protector (Applied Medical, UK) and a small surgeon’s glove in conjunction with traditional laparoscopic ports and instruments.
Results: 31 operations were performed including 2 subtotal colectomies, 7 right hemicolectomies (1 with sigmoid resection), 6 colostomies and 8 ventral hernia repairs.
5 operations were emergencies. Modal ASA 2. Mean BMI 25.7.
There was 1 port site infection. 3 cases required additional ports. 2 cases were converted to open procedures.
Conclusion: We believe, with a total cost of under £25, the technique offers a cost effective, efficient alternative to the commercially available port systems. It does not require a significant learning curve and may be used in both the elective and emergency setting for a range of procedures including colonic resections.
Key statement: Single port surgery is an evolving field however a barrier to uptake is the cost of the port systems. We report our experience with an improvised port system that offers a cost effective, efficient alternative to the commercially available systems for a range of procedures including colonic resections for IBD.

P67
SINGLE PORT LAPAROSCOPIC SURGERY FOR PATIENTS NEEDING SURGERY FOR CROHN’S DISEASE
Author(s): A Shah, M Moftah, J Burke, S Patchett, R Cahill Presenter: A Shah Institution: Beaumont Hospital, Dublin, Ireland
Aims: Single port laparoscopic surgery is a modified access technique that allows grouping of instruments at a single, confined site on the abdominal wall. While intuitively appealing for patients with Crohn’s disease (CD) needing surgery, there is sparse literature yet available for this cohort.
Methods: All patients presenting either electively or urgently for resectional surgery for CD over an 18 month period were considered for SPLS using a surgical glove port sited transumbilically and followed prospectively (including satisfaction scores). Standard, straight rigid laparoscopic instrumentation were used and no additional resources were allocated.
Results: Of 25 consecutive patients presenting for elective or urgent resectional surgery for ileal or segmental colonic CD, 23 (92%) had their procedure by SPLS. 22 patients had an extracorporeal ileocolic anastomosis. Mean incision size was 3.5cm. Patient satisfaction scores were high.
Planned /Urgent
CD Phenotype
Mean (Range) Conversion Postop day of discharge
Complication(Clavien Dindo)
Age BMI
11/12
Stricture:16 (3 redos)
Fistula: 7(3 psoas abscess)
36.3 (17-69) yrs
21.9 (15.4-30.2) kg/m
2
1 (extra port); 2 wound extension >5cm
Modal=4/Mean=4.8
I:5
II:1
III:1
Conclusion: SPLS allows intestinal resectional surgery for CD without additional parietal injury above that needed for specimen extraction in the majority of patients presenting electively or urgently. The surgical glove port performs capably and, by minimizing cost, can facilitate broad embrace of this approach.
Key statement: Single port laparoscopic surgery can safely and effectively provide ileocolic resectional surgery in the majority of patients with Crohn’s Disease in both elective and urgent settings. It need not be associated with increased costs either in terms of access devices or theatre efficiency and is viewed very favorably by patients.

P68
LAPAROSCOPIC CHOLESCYSTECTOMY – DOES INTRA-OPERATIVE GALLBLADDER PERFORATION IMPACT ON LENGTH OF HOSPITAL STAY?
Author(s): H Tafazal, P Spreadborough, H McMahon, M Hanif Presenter: H Tafazal Institution: Sandwell and West Birmingham Hospitals NHS Trust, Birmingham, UK
Aims: In recent years there has been a trend towards performing laparoscopic cholecystectomy as a day case procedure on selected patients. We evaluated whether intra-operative perforation of the gallbladder resulting in bile spillage impacted on the length of inpatient stay (LOS) and re-admission rates.
Methods: We performed a retrospective analysis of 200 patients who underwent laparoscopic cholecystectomy. We looked at the number of cases where the gallbladder (GB) had been perforated intra-operatively and assessed LOS, 30 day re-attendance and readmission rates, and complications.
Results: In 46 (23%) cases, the GB was perforated intra-operatively. LOS of ≥2 days was 14 (30%) and 22 (14%) in the perforated and intact GB groups respectively. Re-attendance rates were 7 (15.2%) and 19 (12.3%) and re-admission rates were 5 (10.9%) and 12 (7.8%) respectively.
Conclusion: Intra-operative perforation of the gallbladder during laparoscopic cholecystectomy results in a longer initial hospital stay and increased re-attendance and re-admission when compared to the intact group. Higher post operative complications in the perforated group may represent increased costs with respect to further investigations and prolonged hospital stays.
Key statement: The utmost care should be taken during surgery to avoid gallbladder perforation as it may delay discharge and result in a higher percentage of re-attendees. As laparoscopic cholecystectomy increasingly becomes a day case procedure, removal without perforation may be necessary to reduce the burden on inpatient bed capacity.

P69
LAPAROSCOPIC APPENDICECTOMY: A RETROSPECTIVE ANALYSIS OF 440 CASES
Author(s): H Nair, C Skouras, M Leeman, S Patterson-Brown Presenter: H Nair Institution: Department of General Surgery, Royal Infirmary of Edinburgh, UK
Aims: The aim of this study was to audit the peri-operative and post-operative results of laparoscopic appendicectomies conducted for clinically suspected acute appendicitis during a 12 month period.
Methods: Patients undergoing laparoscopic appendicectomy between 1st January 2010 and 31st December 2010 were identified from a prospectively maintained operative database. Data from electronic and paper records were reviewed retrospectively. Primary outcome measures were morbidity, including need for re-intervention, mortality, length of stay and re-admission rate.
Results: 440 patients (46.6% male) were identified; median age 28.4 years. There was no mortality, 17.5% morbidity, 10.0% conversion and 14.1% negative appendicectomy rate. Median length of stay was 2 days. 12.5% required readmission and 2.5% required re-intervention (1.4% percutaneous drainage and 1.1% operative drainage).
Conclusion: Laparoscopic appendicectomy can safely be performed for clinically suspected acute appendicitis with a short length of stay, acceptable conversion rate and low complication rate.
Key statement: This large contemporary case series demonstrates that laparoscopic appendicectomy is acceptable as the standard of care for clinically suspected acute appendicitis. There was a low rate of intra-abdominal collection requiring re-intervention in comparison with early series.

P70 THE DIAGNOSTIC ACCURACY OF ULTRASOUND, WHITE CELL COUNT, C-REACTIVE PROTEIN, AND LAPAROSCOPY IN ACUTE APPENDICITIS Author(s): H Nair, Christos Skouras, Matthew Leeman, Simon Patterson-Brown Presenter: H Nair Institution: Department of General Surgery, Royal Infirmary of Edinburgh, UK
Aims: The aim of this study was to audit the diagnostic accuracy of commonly used investigations in the assessment of clinically suspected acute appendicitis. Methods: Patients undergoing laparoscopic appendicectomy between 1st January 2010 and 31st December 2010 were identified from a prospectively maintained operative database. Data from electronic records were reviewed retrospectively. Ultrasound, white cell count (WCC), C-reactive protein (CRP), WCC and CRP combined and laparoscopic findings were compared with histopathology results. Results: 440 patients (46.6% male) were identified; median age 28.4 years. The sensitivity and specificity of investigations were: Ultrasound 0.49 sensitive, 0.91 specific; WCC 0.70 and 0.24; CRP 0.81 and 0.57; WCC and CRP combined 0.91 and 0.16; laparoscopy 0.96 and 0.73. 3.6% of macroscopically normal appendices had appendicitis on histopathology. Conclusion: The combination of WCC and CRP has the highest sensitivity of the commonly used pre-operative investigations, while ultrasound has the highest specificity. Key statement: This large contemporary case series demonstrates that the commonly used pre-operative tests (WCC, CRP and ultrasound) together produce a high level of diagnostic accuracy. The finding of microscopic appendicitis supports a policy of routine removal of the appendix at an otherwise normal laparoscopy for clinically suspected appendicitis

P71
LAPAROSCOPIC HARTMAN’S RESECTION – A SAFE AND FEASIBLE OPTION
Author(s): N Siddiqi, S Zeidan, K Flashman, J Khan, A Parvaiz Presenter: N Siddiqi Institution: Portsmouth Hospitals NHS Trust, UK
Aims: Hartman’s resection remains an important surgical option in patients with cancer and diverticulitis. We aim to analyze our experience of laparoscopic Hartman’s resection for patients presenting in emergency and elective setting.
Methods: All patients operated for a Laparoscopic Hartman’s resection over the last five year (2007-2012) were included in this study. Patient demographics and clinical outcomes were recorded on a prospective database.
Results: 24 patients underwent Laparoscopic Hartman’s resection during the study period with a median age of 74 years. Median BMI was 27. Eight cases were performed for diverticular disease and 16 were cancer resections.
Median operating time was 180 minutes. Three patients were converted to open (12%). Median length of stay was 8 days. One third of these patients presented as an emergency with perforation or obstruction. There was no mortality. Two patients were readmitted and one required a reoperation for drainage of pelvic abscess.
Conclusion: Laparoscopic Hartman’s resection in both emergency and elective setting is feasible and safer option in patients with colorectal cancer or diverticular disease.
Key statement: Hartmans procedure is an important treatment option for a variety of colorectal conditions. Open procedures are associated with a significant morbidity. We analysed our database for laparoscopic Hartmans resection. Clinical outcomes support the safety and feasibility of this approach.
P72
HIDA SCAN - USE IT OR LOSE IT?
Author(s): T Chituku, B Dobbins, A Hetmanski, S Aman Presenter: T Chituku Institution: Huddersfield Royal Infirmary, UK
Aims: Patients who are referred with acalculous biliary-type symptoms present a difficult diagnostic scenario. HIDA scan has been suggested as a useful tool in diagnosing biliary dyskinesia and planning further management. We retrospectively assessed the clinical response of patients who underwent cholecystectomy following HIDA scan.
Methods: We performed a retrospective review of pts who had a HIDA scan and laparoscopic cholecystectomy from January 2006-present. Presenting symptoms, HIDA scan, Ultrasound, OGD, histology results and out- patient follow up records were reviewed. Patients were also followed-up with a phone call asking about symptom resolution.
Results: 60% of patients had symptomatic relief following cholecystectomy. A positive HIDA scan didn’t predict those that do well (67% improved vs 79% not improved). Patients with negative OGD seemed to have greater symptom resolution following cholecystectomy (62.5% vs 36%). Gallbladder Histology didn’t correlate with an abnormal HIDA scan results.
Conclusion: Persistently symptomatic patients with negative USS for gallstones should be offered a laparoscopic cholecystectomy, especially if their OGD is normal. HIDA scan result, severity of symptoms and gallbladder histology result are not predictive of which patients improve following a cholecystectomy.
Key statement: HIDA scan delays surgery and offers no added clinical benefit in the management of biliary dyskinesia.

P73
ROBOTIC SPLENECTOMIES – A SYSTEMATIC REVIEW
Author(s): K Au-Yeung, T Satyadas, J Kan Presenter: K Au-Yeung Institution: Manchester Royal Infirmary, UK
As we step into the twenty-first century, the introduction of robotic splenectomy has caused considerable excitement in the surgical community.
Aims: to assess the feasibility of robotic splenectomies
Methods: A systematic literature search of current literature using the Cochrane, Embase, Medline and PubMed database using MESH terms “robotic splenectomy”, “robotics” OR “robotic” AND “splenectomy”, “da Vinci” AND “splenectomy” yielded 22 English-medium articles which reported a total of 179 robotic splenectomies conducted.
Indications, size and weight of spleen, operative time, total blood loss, complications and length of stay were analyzed.
Results: Complication rates were minimal and operative time has become noticeably shorter in the later studies compared to those prior to 2003.
Conclusion: Robotic splenectomies may indeed be feasible in the near future but equipment limitations will need to be addressed prior to robotic splenectomies becoming available worldwide.
Key statement: As we step into the twenty-first century, the introduction of robotic splenectomy has caused considerable excitement in the surgical community. A systematic review was conducted to assess the feasibility of this novel technique.

P74
A PROSPECTIVE 6-YEAR AUDIT REPORTING THE INTRODUCTION OF LAPAROSCOPIC SURGERY TO A TERTIARY CENTRE IN NORTHERN TANZANIA Author(s): L Horgan
1,2, Alastair Hayes
1
Presenter: L Horgan Institution:
1Victoria Hospital, Fife, UK,
2Hexham General Hospital, Northumberland, UK
Aims: We present a 6-year activity report following the introduction of laparoscopy in 2004 by a laparoscopic team from Northumbria NHS Trust to a tertiary referral hospital in northern Tanzania. Differences in clinical outcomes before and after the introduction in 2008 of a trans-continental audio-visual mentoring laparoscopic link were assessed.
Methods: A 6-year (Aug 2005 - Aug 2011) prospective laparoscopy database at the tertiary hospital in northern Tanzania was interrogated. The following outcomes were audited: complications, conversion rate and length of surgery. Statistical differences were analysed by Chi square and Mann-Whitney U test (<0.05 considered significant).
Results: 233 laparoscopic procedures were performed: 192 cholecystectomies, 34 appendicectomies and 7 diagnostic laparoscopies. For cholecystectomy, there were 2 duct injuries, 2 deaths, 17 conversions and 6 re-operated. Reduced conversion (14% to 7%) did not reach significance. Median operating time (90mins) was significantly (<0.001) reduced (66mins) in the latter 3 years.
Conclusion: An improvement in cholecystectomy outcomes was observed during the latter three years in which an audio-visual mentoring link was in operation. This project supports the feasibility of establishing a laparoscopic service in an under-resourced healthcare setting including the use of a trans-continental audio-visual mentoring link.
Key statement: A laparoscopic service can be provided by local surgeons in an under-resourced healthcare setting with training from visiting surgeons and use of an audio-visual mentoring link. Successful and significant outcomes are achievable.
P75
ROBOTICALLY ASSISTED RECTAL CANCER RESECTION – PRELIMINARY RESULTS
Author(s): R Madani, R Alexander, H Tilney, M Gudgeon Presenter: R Madani Institution: Frimley Park Hospital NHS Foundation Trust, Surrey, UK
Aims: To audit the introduction and early results of Robotic assisted minimal access rectal cancer resection.
Methods: Data are prospectively collected on a PMAS database for all patients undergoing colorectal cancer resection. Robotic rectal cancer resection was introduced to our unit in July 2009 as a hybrid procedure with the robot (4-arm Da Vinci S) being docked for the rectal dissection.
Results: Of 60 patients treated 77% were male. Median stay 6 days (IQR 5-12). There were 3/53(5.7%) anastomotic leaks and 7/60(10.7%) abdominoperineal resections. 4 were converted to an enlarged pfannenstiel incision to complete the TME or facilitate stapling. There have been no involved circumferential margins and no local recurrences to date.
Conclusion: Robotic rectal cancer surgery can be safely introduced in experienced laparoscopic centres with good short term surgical and oncological outcomes. A randomised trial is required to show whether there is any benefit over standard laparoscopic surgery.
Key statement: Initial results show that robotic rectal cancer surgery is safe and oncologically effective with a subjective view that there are advantages from the high definition 3 dimensional imaging and the use of intuitive wristed instrumentation.

P76
TIME FOR A CONSENSUS ON LAPAROSCOPIC APPENDICECTOMY?: A SURVEY OF TRAINING, TECHNIQUE AND EXPERIENCE ACROSS ENGLAND
Author(s): W Carr5, F McNicol
2, B Thava
3, S Pilgrim
4, D McGrath
1
Presenter: W Carr Institution:
1Royal Berkshire Hospital, Reading, UK,
2Royal Liverpool Hospital, UK,
3John
Radcliffe Hospital, Oxford, UK, 4Norfolk & Norwich University Hospital, UK,
5Sunderland Royal Hospital, UK
Aims: Laparoscopic Appendicectomy (LA) has become common practice in the UK. The operative techniques, and intra-operative decision making varies between surgeons. This survey aims to assess current training in LA and tries to identify a consensus for the optimal technique.
Methods: Surgical registrars across 5 different deaneries were invited to complete a questionnaire designed to determine their experience of LA. Operative numbers, level of training, preferred port setup / camera placement, dissection technique and other variables were collated and analysed.
Results: 95 questionnaires were returned from 5 deaneries with a mean of 48 LA per trainee. LA was used by 90% routinely, in all patients, with 10% preferring open Appendicectomy in children. A three-port technique was used by 90% and all used an umbilical port. More than two-thirds skeletalised the appendix, the remainder removing the whole mesoappendix. A macroscopically normal appendix would be removed by 59%.
Conclusion: There is great variation in the set-up and technique employed by trainees across England. Training courses, which cover LA, are widely available, but the majority of trainees have not attended such a course. This may explain the observed variation in port placement, operative technique and intra-operative decision-making. Whilst there is no high quality evidence to recommend any single approach, the commonest approach should constitute a consensus.
Key statement: On questioning 95 trainees with a combined experience of 4560 LA:
1. LA is the preferred approach to appendicectomy
2. There is great variation in the approach and technique of LA
3. A consensus of approach to LA is required
P77
CURRENT GUIDELINES ON LYMPH NODE HARVEST ARE EASILY ACHIEVABLE IN LAPAROSCOPIC COLORECTAL SURGERY
Author(s): R Makar, V Ng, K Akbari, D Coull, P Conaghan, D McGrath, S Middleton Presenter: R Makar Institution: Royal Berkshire Hospital, Reading, UK
Aims: Inadequate lymph node excision during bowel resection is associated with poor long-term outcomes. Current guidelines suggest a minimum of 12 lymph node should be excised / examined. We wished to audit the total number of lymph node excised during laparoscopic colorectal resections, offered as first line treatment in our institution.
Methods: Retrospective data was collected on a series of consecutive patients, with colorectal cancer/dysplastic polyps, who underwent laparoscopic resection over a 6-month period. Data pertaining to tumour site, stage and grade; resection type, conversion to open procedure; number of lymph node excised, specimen length and diameter of tumour; and neo-adjuvant therapy were collated and analysed.
Results: 81 patients were evaluated, 69 underwent cancer resection, having excluded 12 non-cancer resections. The mean number of nodes harvested was 18.5. Lymph node numbers were correlated with diameter of tumour. Fewer lymph nodes were retrieved from patients undergoing pre-operative neoadjuvant therapy.
< 12 nodes retrieved >12 nodes retrieved
Total 4 (5.8%) 65 (94.2%)
+ve Nodes 3 25
Highest node +ve 0 5
Conclusion: With more than 94% of cases have 12 or more lymph nodes harvested our institution is compliant with the current guidelines. Concordance with the Royal College of Pathologists and NICE guidelines is achievable in the era of laparoscopic colorectal surgery.
Key statement: Concordance with the current guidelines on lymph nide harvest in colorectal suregy is achievale in the era of Laparoscopic surgery

P78
ARE THEY WAITING TOO LONG? A REVIEW OF THE INCIDENCE OF RECURRENT ACUTE CHOLECYSTITIS WHILE AWAITING LAPAROSCOPIC CHOLECYSTECTOMY
Author(s): G Sadadcharam, M Varzgalis, E Andrews Presenter: G Sadadcharam Institution: Cork University Hospital, Ireland
Aims: With longer waiting lists the risk of recurrent attacks of acute cholecystitis is a major concern for patients awaiting an interval laparoscopic cholecystectomy. Here we review the incidence of acute symptoms or complications during the waiting period for a laparoscopic cholecystectomy.
Methods: A prospective database from a single colorectal surgeon in a tertiary referral unit was analysed to determine the number of patients who presented with acute cholecystitis whilst awaiting an elective cholecystectomy. Patient demographics, operative variables and the numbers presenting with acute symptoms during the waiting period were analysed.
Results: A total of 95 patients underwent laparoscopic cholecystectomy in a 14 month period. The mean age was 50.5 years (male to female ratio = 27:68). Forty-one percent presented acutely during their index visit. The average waiting time was 14 weeks for an interval cholecystectomy. Ten patients (10.5%) presented with recurrent cholecystitis.
Conclusion: Although the waiting time to elective surgery was 14 weeks only 10.5 percent of patients had a recurrent attack of acute cholecystitis. Half were managed surgically in the acute setting with one patient requiring conversion to an open procedure. There was a low morbidity rate and no mortalities seen.
Key statement: Current surgical management of acute cholecystectomy not only involves an elective interval cholecystectomy but often involves an emergency cholecystectomy during the index presentation. Despite longer waiting times to elective cholecystectomy, there is a low rate of recurrent cholecystitis in those patients waiting surgery.

P79
LYMPH NODE CLEARANCE FOR COLONIC CANCER RESECTION: LAPAROSCOPIC VERSUS OPEN APPROACH
Author(s): N Foley, G Sadadcharam, A Shafiq, M Mushtaque, E Andrews Presenter: N Foley Institution: Cork University Hospital, Ireland
Aims: The National Comprehensive Cancer Network (NCCN) guidelines suggest a minimum of 12 lymph nodes after colonic or rectal cancer surgery for oncological assurance. The oncological adequacy of the laparoscopic colorectal resection is still being reported. We compared the lymph node yield between the laparoscopic and open approach.
Methods: A prospectively maintained database from a single colorectal surgeon in a tertiary referral unit was interrogated. All cancer resections from July 2010 – September 2012 were assessed. Analysis of the lymph node clearance between laparoscopic and open procedures was carried out.
Results: Fifty laparoscopic and 23 open procedures were performed. Both groups were similar in mean age and the elective/emergency procedure ratio. Sigmoid or rectal tumours accounted for 31.5% (n=23) of all cancers. The average node count from laparoscopic and open resections was 16.9 and 17.2 respectively (=0.33).
Conclusion: This study has shown that a similar lymph node clearance can be achieved using either the laparoscopic or open approach. This also applies to left sided tumors requiring a total mesorectal excision where the nodal count has been linked to outcomes.
Key statement: Laparoscopic and open resections were similar with regards to the nodal yield for oncological resections of the colon and rectum. The benefits of laparoscopic surgery can be applied to cancer patients without compromising oncological quality.
P80
INCISIONAL HERNIA RATE AFTER LAPAROSCOPIC COLORECTAL RESECTION REDUCED WITH STANDARDISATION OF EXTRACTION
Author(s): A Navaratnam, N Smart, R Motson, T Arulampalam Presenter: A Navaratnam Institution: ICENI Centre, Colchester, UK
Aims: Incisional hernia (IH) is a common complication of laparoscopic colorectal surgery (LCS) with the majority occurring within the first two postoperative years. Risk factors for the development of incisional hernias include age, diabetes, obesity and smoking status. This study investigated the effect of specimen extraction site on IH rate.
Methods: In this retrospective single-centre study, two cohorts of patients that underwent LCS with two year follow up were indentified in year groups 2005 (n=110) and 2009 (n=151). In 2005, specimens were extracted through transverse muscle cutting incisions. In 2009 all specimens were extracted through midline incisions.
Results: The total IH rate for the series was 8.4% at two years follow up (2005:13.6% (n=15) and 2009: 4.6% (n=7). There was no statistically significant difference between the two year groups or between IH and non-IH patients in regards to age, sex, diabetes, BMI, smoking status or ASA.
Conclusion: The 2005 year group had a statistically significantly higher IH rate compared to the 2009 year group. This is due to the differences in the incision technique and extraction site in the two year groups.
Key statement: Incisional hernia rate may be reduced by standardisation of extraction site after laparoscopic colorectal surgery.

P81
DO INTRAOPERATIVE FACTORS INFLUENCE THE LENGTH OF STAY OF PATIENTS UNDERGOING LAPAROSCOPIC COLORECTAL RESECTIONS WITHIN A WELL ESTABLISHED ERAS PROGRAMME?
Author(s): K Marwan, N Noor, N Smart, T Arulampalam, R W Motson Presenter: K Marwan Institution: ICENI Centre, Colchester, UK
Aims: Enhanced recovery after surgery (ERAS) in combination with laparoscopic colorectal surgery (LCS) results in shorter lengths of stay (LOS) and better outcomes for patients. The aim of this study was to determine whether intraoperative factors influenced length of stay after LCS.
Methods: 1001 consecutive patients undergoing LCS had data prospectively collected between April 2005 and September 2011. Data was extracted for LOS, demographic variables, cancer status, seniority of surgeon, rectal resection, blood loss, operative duration. A logarithmic transformation was used (LogLOS).
Results: 868 (425 male) patients were included. Mean age was 65.4 years. Median LOS was 7 days (range 1-168). Thirty-day mortality was 4.2%. All prediction models seeking to explain the variation in LOS produced poor fits. Operative duration and blood loss were the two predictors to stand out in these models.
Conclusion: Intraoperative factors are poor predictors of postoperative length of stay in patients undergoing laparoscopic colorectal surgery within an established ERAS programme.
Key statement: Intraoperative factors are poor predictors of postoperative length of stay in patients undergoing laparoscopic colorectal surgery within an established ERAS programme

P82
'TRAINEE' EVALUATION OF THE STEPS LAPAROSCOPIC COLO-RECTAL SURGERY FOUNDATION COURSE
Author(s): N Srinivasaiah1, T Arulampalam
2
Presenter: N Srinivasaiah Institution:
1Specialty Trainee, London Postgraduate School of Surgery, London Deanery,
London, UK, 2Iceni Centre, Colchester General Hospital, UK
Aims: The STEPS Laparoscopic Colorectal Foundation Course, established by Ethicon Endo-Surgery in partnership with The ICENI Centre in Colchester, offers advanced training in laparoscopic colorectal surgery over six days, split between Colchester and ESI, Hamburg. We aim to review trainees' opinions of the training they had received through the STEPS course.
Methods: A 22-item electronic-survey questionnaire (www.surveymonkey.com) was given to STEPS-course participants. Opinions gathered using four-point Likert scale along with satisfaction and intentions for participation in future courses. Percentages, mean values and SD were presented. Mann-Whitney U-tests were used to examine the impact of different factors on the overall rating of satisfaction.
Results: A total of 13 (54%) responded out of twenty four. Examination of course outcomes showed participants agreed strongly that they were glad to attend course (mean=3.7 ±0.48), their self confidence had improved (mean=2.9 ±0.67), felt more knowledgeable (mean=3.2 ±0.56), skills improved (mean=3.0 ±0.70), and felt were better surgeons (mean=3.1 ±0.50).
Conclusion: The large majority of trainees were highly satisfied with the training received in this innovative multimodal foundation programme for Laparoscopic colo-rectal surgery. Majority 85% would recommend the course in its current format. 100% would like continuing support and be interested in being part of STEPS alumni.
Key statement: A multimodal training approach involving clinical knowledge, technical skills and decision making can be delivered in a structured programme of this nature to augment laparoscopic training needs of Colo-rectal trainees. The STEPS foundation programme seems to be effective for laparoscopic Colo-rectal surgical training, with current content and structure.

P83
LAPAROSCOPIC LATERAL PANCREATICOJEJUNOSTOMY, BEGER’S AND FREY’S PROCEDURES FOR THE TREATMENT OF CHRONIC PANCREATITIS: THE FIRST UK EXPERIENCE
Author(s): A S Khaled1, Y S Khaled
1,2, B J Ammori
1,2
Presenter: A S Khaled1
Institution: 1North Manchester General Hospital, UK,
2University of Manchester, UK
Aims: Pancreatic resection and/or ductal drainage are common surgical options in the management of unremitting abdominal pain of chronic pancreatitis (CP). We describe the results of the laparoscopic approach to pancreatic duct drainage and head resection for CP.
Methods: Patients with CP and intractable abdominal pain requiring Beger’s, Frey’s or Puestow procedure were offered laparoscopic surgery by a single surgeon. The results shown represent median (range).
Results: Seven patients (3 males) with CP (alcohol induced, n=5; idiopathic, n=2) underwent surgery between 2009 and 2012. The pancreatic duct diameter was 8.7 (6-11) mm. Surgery included lateral pancreaticojejunostomy (LPJ; n=5), Beger’s procedure (n=1) and Frey’s procedure (n=1), and all were completed laparoscopically. The operating time was 265.5 (250-360) minutes. There were no deaths, while one patient was readmitted 10 days postoperatively and had laparotomy for pancreatic bleeding following LPJ (morbidity, 14%). The hospital stay was 5 (5-8) days. At a follow-up of 10 months (4-25) five of the patients were pain-free whereas two patients required one-third and half of the preoperative oral opioid dose for pain control.
Conclusion: The laparoscopic approach to pancreatic duct drainage and limited head resection in carefully selected patients and in experienced hands is feasible and safe with good short-term results and potential advantages. Further expansion of experience and longer follow up is required.
Key statement: This is the first case series of laparoscopic Puestow and Frey's procedures for the treatment of chronic pancreatitis in the UK and the first case report on laparoscopic Beger's procedure in literature. We present the operative techniques, safety and effectiveness for the interest of the highly skilled laparoscopic surgeons.

P84
PRIMARY DUCT CLOSURE FOLLOWING LAPAROSCOPIC BILE DUCT EXPLORATION FOR CHOLEDOCHOLITHIASIS IS SAFE AND EFFECTIVE
Author(s): A S Khaled1, Y S Khaled
1,2, D J Malde
2, C De Suza
2, A Kalia
2, B J
Ammori1
Presenter: A S Khaled1
Institution: 1North Manchester General Hospital, UK,
2University of Manchester, UK
Aims: The common bile duct is traditionally managed with T-tube drainage after holedochotomy and removal of common bile duct (CBD) stones, but this approach carries an associated tube-related morbidity rate, including bile leak, of 10.5-20% .This study examines the safety and effectiveness of laparoscopic CBD exploration (LCBDE) followed by primary duct closure.
Methods: This is a retrospective analysis of 120 consecutive patients (37 male) who underwent LCBDE between October 2002 and August 2012. The duct was primarily closed in all patients. The results shown represent the median (range).
Results: All procedures were completed laparoscopically. The maximum diameter of the CBD was 9.4 (3-30) mm and the number of CBD stones was 3 (0-20). The exploration was transcystic in 6 patients and trans-CBD in 114 patients. The biliary tree was clear at the end of exploration with no subsequent evidence of retained stones in 118 patients (98.3%). The operating time was 132 (70-650) minutes. Postoperative bile leakage was encountered in four patients (3.3%) who were managed successfully with re-laparoscopy and re-suturing of the choledochotomy (n=2) and conservatively (n=2). The morbidity rate was 5.8% and included pulmonary complications (n=3), myocardial infarction (n=2), urinary tract infection (n=1) and wound infection (n=1). There were no operative deaths, and the postoperative hospital stay was 2.1 (1-29) day. At a follow up of 39.2 (3-82) months, 115 (97.5%) had no biliary symptoms, while one patient required endoscopic extraction of a retained stone, one developed bile duct stricture that was managed successfully by endoscopic balloon dilatation, and two patients (1.6%) failed to attend.
Conclusion: Primary duct closure following LCBDE is safe, and can be employed as an alternative to T-tube insertion with short hospital stay and lower morbidity rate
Key statement: This is the largest UK series of laparoscopic common bile duct exploration, predominantly via choledochotomy, with primary closure. We present the safety and effectiveness of this approach with median follow up of 39.2 months.