Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 9 , N O . 1 4 , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 7 . 0 1 . 0 5 4
Early Feasibility Study of aTranscatheter TricuspidValveAnnuloplastySCOUT Trial 30-Day Results
Rebecca T. Hahn, MD,a,b Christopher U. Meduri, MD,c Charles J. Davidson, MD,d Scott Lim, MD,e
Tamim M. Nazif, MD,a Mark J. Ricciardi, MD,d Vivek Rajagopal, MD,d Gorav Ailawadi, MD,e Mani A. Vannan, MBBS,c
James D. Thomas, MD,d Dale Fowler, MD,e Stuart Rich, MD,d Randy Martin, MD,c Geraldine Ong, MD,b
Adam Groothuis, PHD,f Susheel Kodali, MDa
ABSTRACT
Fro
Un
Ce
Un
Ha
inv
is a
pro
Lif
is a
an
con
Ab
Dr
BACKGROUND The SCOUT (Percutaneous Tricuspid Valve Annuloplasty System for Symptomatic Chronic Functional
Tricuspid Regurgitation) trial is a prospective, single-arm, multicenter, early feasibility study of a novel transcatheter
device to plicate the tricuspid annulus (TA) and reduce tricuspid regurgitation (TR).
OBJECTIVES This study tested the feasibility and safety of a novel transcatheter device and assessed its early
performance and functional outcomes.
METHODS Between November 2015 and June 2016, 15 patients with New York Heart Association (NYHA) functional
class $II and moderate or greater functional TR were enrolled. Primary performance and safety endpoint outcomes were
technically successful at 30 days with no reintervention. Echocardiographic measurements (TA diameter, effective
regurgitant orifice area [EROA], left ventricular stroke volume [LVSV]) and quality-of-life (QoL) measurements (NYHA
functional class, Minnesota Living with Heart Failure Questionnaire [MLHFQ], and 6-min walk test [6MWT]) were
performed at baseline and 30 days.
RESULTS All patients (mean 73.2 � 6.9 years of age, 87% female) underwent successful device implantation with no
deaths, strokes, bleeding, tamponade, or valve reintervention. Technical success rate at 30 days was 80%, with 3
single-pledget annular detachments without reintervention. In the remaining 12 patients, there were significant reductions
in TA (12.3 � 3.1 cm2 to 11.3 � 2.7 cm2, respectively; p ¼ 0.019) and EROA (0.51 � 0.18 cm2 vs. 0.32 � 0.18 cm2,
respectively; p ¼ 0.020), with significant increase in LVSV (63.6 � 17.9 ml vs. 71.5 � 25.7 ml, respectively; p ¼ 0.021). In
the intention-to-treat cohort, there were significant improvements in NYHA functional class ($1 class, p ¼ 0.001), MLHFQ
(47.4 � 17.6 to 20.9 � 14.8; p < 0.001), and 6MWT (245.2 � 110.1 to 298.0 m � 107.6 m; p ¼ 0.008).
CONCLUSIONS The 30-day results of the SCOUT trial confirmed the safety of the novel transcatheter
device, which reduced TA and EROA, increased LVSV, and improved QoL. (Early Feasibility of the
Mitralign Percutaneous Tricuspid Valve Annuloplasty System (PTVAS) Also Known as TriAlign [SCOUT];
NCT02574650.) (J Am Coll Cardiol 2017;69:1795–806) © 2017 by the American College of Cardiology Foundation.
m the aDepartment of Medicine, Division of Cardiology/New York Presbyterian Hospital, New York-Presbyterian/Columbia
iversity Medical Center, New York, New York; bCardiovascular Research Foundation, New York, New York; cMarcus Heart Valve
nter, Piedmont Heart Institute, Atlanta, Georgia; dBluhm Cardiovascular Institute, Feinberg School of Medicine, Northwestern
iversity, Chicago, Illinois; eUniversity of Virginia, Charlottesville, Virginia; and fMitralign, Inc., Tewksbury, Massachusetts. Dr.
hn is a speaker for Edwards Lifesciences, Abbott Vascular, Boston Scientific, and GE Medical; is an unpaid national principal
estigator for the SCOUT Trial; and is an uncompensated director of Echo Core for multiple industry-sponsored trials. Dr. Meduri
consultant and proctor for and has received a research grant from Medtronic; is an advisory board member, consultant, and
ctor for Boston Scientific; and has received research grants from Edwards Lifesciences. Dr. Nazif is a consultant for Edwards
esciences. Dr. Rajagopal is a consultant for Boston Scientific, Abbott Vascular, Medtronic, and Edwards Lifesciences. Dr. Alawadi
consultant for Abbott Vascular, Edwards Lifesciences, Medtronic, St. Jude Medical, and Atricure. Dr. Vannan is a speaker for
d has research support from Abbott Vascular and Siemens Healthcare. Dr. Thomas has received honoraria from and is a
sultant for Siemens, GE Medical, and Edwards Lifesciences. Dr. Martin is a speaker for Medtronic, Edwards Lifesciences, and
bott Vascular; and holds stock/ownership in BayLabs. Dr. Groothuis is an employee of and holds ownership stock in Mitralign.
. Kodali is a consultant for Dura Biotech; consults for and has received research support from Edwards Lifesciences, Medtronic,

ABBR EV I A T I ON S
AND ACRONYMS
6MWT = 6-min walk test
EROA = effective regurgitant
orifice area
MLHFQ = Minnesota Living
with Heart Failure
Questionnaire
NYHA = New York Heart
Association
PISA = proximal isovelocity
surface area
QoL = quality of life
TAPSE = tricuspid annular
plane systolic excursion
TEE = transesophageal
echocardiography
TR = tricuspid regurgitation
TTE = transthoracic
echocardiography
and Abbott
relationship
Manuscript
Hahn et al. J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7
Transcatheter Annuloplasty for Functional TR A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6
1796
I nterest in functional or secondarytricuspid valve regurgitation (TR) hasincreased in recent years (1) due to its
high prevalence (2), progressive nature (3),and impact on outcomes (4–6). According tothe American Heart Association/AmericanCollege of Cardiology guidelines, the onlyclass 1 indication for TR repair is duringconcomitant left heart surgery (Level of Evi-dence: C) (7). Despite the benefits of tricuspidrepair (8,9), a large number of patients under-going left-sided valve surgery do not undergotreatment of concomitant significant TR. Inpatients who develop severe TR late afterleft-sided heart valve surgery, operative mor-talitymay be as high as 10% to 20% (2,10,11). Inaddition, an increasing number of patients arecurrently being treated with transcathetertherapies, and severe TR has been shown toaffect outcomes in these patients (12,13).
Thus, there is significant interest in development of atranscatheter therapy for TR.
SEE PAGE 1807
Although the original Kay bicuspidization proced-ure is infrequently used (14), the Trialign system(Mitralign Inc., Tewksbury, Massachusetts) attemptsto replicate the results of the current modified Kayprocedure, which has shown efficacy and long-termoutcomes similar to those of other surgical repairmethods (15,16). Since its first-in-human implantation(17), numerous other investigators have reported us-ing this device successfully for TR (18,19). The SCOUT(Percutaneous Tricuspid Valve Annuloplasty System[PTVAS] for Symptomatic Chronic FunctionalTricuspid Regurgitation) trial (NCT02574650) is aprospective, single-arm, multicenter, early feasibilitystudy of this novel device. The following 30-dayresults of the SCOUT trial constitute the first reportof an early feasibility trial for a transcatheter tricuspidvalve device.
METHODS
PATIENT SELECTION, STUDY DESIGN, AND
MANAGEMENT. Between November 2015 and June2016, 15 patients with New York Heart Association(NYHA) functional class $II and greater than or equalto moderate functional TR, with no indication of
Vascular; and holds equity in Thubrikar Aortic Valve and BioTrac
s relevant to the contents of this paper to disclose.
received December 5, 2016; revised manuscript received Januar
left-sided valve surgery, were enrolled at 4 sites inthe United States. Exclusion criteria were >85 yearsof age, pacemaker implantation, systolic pulmonaryartery pressure >60 mm Hg, left ventricle ejectionfraction <35%; tricuspid annular plane systolicexcursion (TAPSE) <13 mm; or tricuspid effectiveregurgitant orifice area (EROA) >1.2 cm2. OnlineTable 1 lists the complete inclusion/exclusion criteria.
ECHOCARDIOGRAPHY CORE LABORATORY
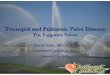
ANALYSIS. All echocardiograms were analyzed at anindependent core laboratory that followed theAmerican Society of Echocardiography standards forechocardiography core laboratories (20). Pre- and post-procedural transthoracic echocardiograms (TTE) wereperformed according to specific core laboratory pro-tocols for assessment of tricuspid valve and ventricularand atrial functions, and core laboratory measure-ments were performed according to previously pub-lished guidelines (21,22). Right ventricular functionwas assessed by using TAPSE, fractional area change,and tricuspid annulus tissue Doppler systolic velocity(S0) (23,24). TR was assessed using standard colorDoppler methods, as described in American Society ofEchocardiography guidelines (25), with minimum andmaximum vena contracta diameters also recorded(Figure 1). The ellipticity of the vena contracta wascalculated as minimum/maximum diameters.
The following echocardiographic measurementsand calculations were performed (see Figure 2 forcalculations):
1. Proximal isovelocity surface area (PISA) (26–28): APISA EROA was calculated using color DopplerNyquist baseline shift, recording aliasing velocityand maximum PISA radius view, where TR jet wasparallel to the insonation beam, peak TR velocity,and TR velocity time integral.
2. Quantitation of TR by relative stroke volumes(26,29,30):a. The forward stroke volume was calculated using
left ventricular outflow tract radius and velocitytime integral. In the setting of greater mildaortic regurgitation, the forward stroke volumewas calculated using the right ventricularoutflow tract radius and velocity time integral.
b. Quantitative Doppler method for calculatingtricuspid stroke volume as the product of thetricuspid annular area (TAA) and pulsed-waveDoppler annular velocity time integral.
e. All other authors have reported that they have no
y 23, 2017, accepted January 24, 2017.

FIGURE 1 Vena Contracta Measurements
Representative maximum (A) and minimum (B) VC measurements are shown. The noncircular nature of the tricuspid orifice is clear from the
differences in these measurements. VC ¼ vena contracta.
J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7 Hahn et al.A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6 Transcatheter Annuloplasty for Functional TR
1797
i. TAA: orthogonal plane annular diameters(inflow and 4-chamber views) in early dias-tole (1 frame after initial valve opening) wereused in an ellipse formula to calculate TAA. Ifa simultaneous biplane image of the annuluswas obtained, the orthogonal diameters wereobtained from that image.
ii. The tricuspid annular velocity time integralwas obtained by averaging 5 to 10 sequentialpulsed-wave diastolic spectral waveformsfrom the view with flow most parallel to theinsonation beam (typically the apical view).
c. Regurgitant volume was calculated as [tricuspidvalve diastolic stroke volume minus forwardstroke volume].
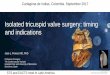
TA PLICATION PROCEDURE. Implantation of thedevice was previously described (Figure 3) (17).Before device implantation, a guidewire is placed inthe right coronary artery to help identify its locationrelative to the tricuspid annulus (TA). Two 14-Fgauge sheaths are introduced into the right jugular
vein for delivery of the device. A deflectable guidecatheter is introduced to position a wire deliverycatheter beneath the annulus, between the posteriorand septal tricuspid leaflet commissures (poster-oseptal position). Before crossing the annulus,transesophageal echocardiographic (TEE) imaging isused to visualize the wire delivery catheter andconfirm that: 1) adequate annular depth (2 to 4 mmfrom the base of the leaflet); 2) distance from theright coronary artery; and 3) direction (into the rightatrium). An insulated radiofrequency (20 to 30 W forw3 s) wire is passed through the tissue of theannulus, and the wire’s position is confirmed byTEE. The wire is snared in the right atrium, exteri-orized, and a pledget delivery catheter is introducedover the wire and across the annulus. Fluoroscopyand TEE guide withdrawal of the pledget deliverycatheter and seating of the ventricular side of thepledget. The proximal (atrial) side of the pledgetedsuture is deployed and cinched onto the annulus.After placement of the first pledget, a second wire ispositioned between 2.4 and 2.8 cm from the first

FIGURE 2 Methods for Quantifying Regurgitant Orifice Area
QuantitationMethod
MeasurementsRequired
Example Calculation
PISA
QuantitativeDoppler
1. PISA radius [r]2. PISA aliasing velocity [v] (approximately 28 cm/s)3. TR peak velocity [v0]4. TR velocity time integral [TRVTI]
1. LVOT Stroke Volume• LVOT diameter• LVOT PW
2. Diastolic TVannulus Area• Inflow and 4Ch TV annular diameters (simultaneous multiplane imaging can also be used)
3. TV velocity time integral[TVVTI]• PW Doppler sample volume at the annulus
Note: Forward strokevolume may be either theleft ventricular or rightventricular stroke volume
ROA = RegVol ÷ TRVTI
RegVol =Diastolic Stroke Volume –Forward Stroke Volume
Diastolic Stroke Volume =TVannulus Area × TVVTI
Forward Stroke Volume:-LVOTannulus Area × LVOTVTI
ROA = Q/v0
RegVol = ROA × TRVTI
Q = 2πr2v
The 2 methods used for calculating the tricuspid ROA and regurgitant volume (RegVol): PISA method, and quantitative Doppler with relative
stroke volume comparison. 4Ch ¼ 4-chamber; LVOT ¼ left ventricular outflow tract; PISA ¼ proximal isovelocity surface area; PW ¼ pulsed
wave; Q ¼ flow; ROA ¼ regurgitant orifice area; TR ¼ tricuspid regurgitation; TV ¼ tricuspid valve; VTI ¼ velocity time integral.
Hahn et al. J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7
Transcatheter Annuloplasty for Functional TR A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6
1798
site, near the commissure, between the posteriorand anterior tricuspid valve leaflets (anteroposteriorposition), and a second pledgeted suture is placedusing the same technique. A dedicated plication lockdevice is used to bring the 2 sutures together,drawing the anteroposterior pledget toward theposteroseptal pledget (Central Illustration). Usingfluoroscopic and TEE imaging, maximal plicationof the TA is performed. Completion of a right coro-nary artery angiogram is performed followingimplantation.
ENDPOINTS. The primary safety and performanceendpoint of the early feasibility trial was a technicalsuccess at 30 days. Secondary endpoints are listed inOnline Table 1. Patient quality of life (QoL) wasassessed by using NYHA functional class assessment,6-min walk test (6MWT) results, and MinnesotaLiving with Heart Failure Questionnaire (MLHFQ)responses.
STATISTICAL METHODS. Data are summarized andreported for the intention-to-treat population and theas-treated population of subjects, as appropriate,with technical success at 30 days. Categorical vari-ables are summarized using frequency tables, andcontinuous variables are presented as mean � SD.Statistical comparisons of characteristics collected atbaseline and at 30 days were performed using paireddata, using the Student t test or the Wilcoxon signedrank test when the assumption of normality wasviolated (as assessed by the Shapiro-Wilk test of thedistribution of change scores).
RESULTS
Baseline demographics are listed in Table 1. The meanage was 73.6 � 6.6 years, and 87% were women. Allpatients were symptomatic and in NYHA functionalclass II (33%) or III (67%). The majority of patientshad a history of hypertension (80%) or pulmonary

FIGURE 3 Summary of Procedural Steps
The systemuses a deflectable guide catheter introduced through the transjugular approach to position awire delivery catheter ([A] artist rendering)
and the 3-dimensional transesophageal image ([B] asterisk) on the ventricular side of the annulus and then introduce an insulated radiofrequency
wire across the annulus. After a pledgeted suture is delivered across the annulus, the process is repeated at a predetermined distance from the first
pledget (C, D). The 2 sutures are then plicated (E, F) and locked to reduce the annular dimensions and regurgitant orifice. The sutures are then cut,
and the delivery system is removed to leave a bicuspidized valve (G, H). Ant¼ anterior; Post¼ posterior; RA¼ right atrium; RV¼ right ventricle;
Sept ¼ septum.
J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7 Hahn et al.A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6 Transcatheter Annuloplasty for Functional TR
1799

CENTRAL ILLUSTRATION Transcatheter Repair System for Severe Tricuspid Regurgitation andQuality-of-Life Outcomes
Hahn, R.T. et al. J Am Coll Cardiol. 2017;69(14):1795–806.
The SCOUT trial is the first multicenter early feasibility study of a novel transcatheter device for functional tricuspid regurgitation that showed a significant reduction in
tricuspid annular area and regurgitant orifice, with functional status and quality of life measures. (Top) Basic steps for implantation of the device. (Bottom) Changes in
NYHA functional class (A), MLHFQ, (B), and 6MWT (C) are shown for the 12 patients with the device in the intended position. 6MWT¼ 6-min walk test; AT ¼ as-treated
population; MLHFQ ¼ Minnesota Living with Heart Failure Questionnaire; NYHA ¼ New York Heart Association.
Hahn et al. J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7
Transcatheter Annuloplasty for Functional TR A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6
1800
hypertension (60%) or had undergone prior mitralvalve intervention (67%) and were in atrial fibrillation(67%). All patients were treated with diuretic agents,and the majority (93%) were also receiving a beta-blocker agent. Additional medications are shown inOnline Table 2.PROCEDURAL RESULTS. All 15 patients underwentsuccessful implantation of the device, in the intendedposition, with successful plication. Procedural dataare listed in Table 2. There were no instances of death,stroke, bleeding or access site complications, cardiactamponade, or valve reintervention. In 1 subject, thecompletion angiogram obtained post-implantation
showed tenting of the distal right coronary artery inthe region of the plication with significant narrowingconfirmed by fractional flow reserve of 0.57, whichwas associated with ST-segment elevations on elec-trocardiogram. These changes resolved with rightcoronary stent placement with post-procedure peaktroponin concentration of 1.79 mg/l, which decreasedto 0.7 mg/l.
At 30 days (Table 3), 3 patients had echocardio-graphic evidence of a single pledget detachmentfrom the annulus. The detached pledget was post-eroseptal in 1 patient and anteroposterior in 2 pa-tients. All detached pledgets remained securely

TABLE 2 Procedural Data of the 15 Patients Enrolled in the
SCOUT Trial
Total procedure time, min 124 � 62
Total contrast volume, ml 51.4 � 58.0
Total fluoroscopy time, min 96.2 � 30.8
Total general anesthesia time, min 352.9 � 69.0
Vascular access site closure
Manual compression 11 (73.3)
Vascular closure device 2 (13.3)
Permanent implantation of device inthe correct position
15 (100.0)
Plication performed 15 (100.0)
Pledget detachment 1 (6.7)
Bleeding/access site complications 0 (0.0)
MACE 1 (6.7)
Tamponade 0 (0.0)
Values are mean � SD or n (%). MACE ¼ major adverse cardiac events: death,nonfatal myocardial infarction, or revascularization.
TABLE 1 Baseline Demographics of the 15 Patients Enrolled in
the SCOUT Trial
Age, yrs 73.6 � 6.6
Female 13/15 (86.7)
NYHA functional class
I 0/15 (0.0)
II 5/15 (33.3)
III 10/15 (66.7)
IV 0/15 (0.0)
Prior myocardial infarction 1/15 (6.7)
Prior CABG 4/15 (26.7)
Prior PCI 1/15 (6.7)
Hypertension 12/15 (80.0)
Hyperlipidemia 10/15 (66.7)
History of pulmonary hypertension 9/15 (60.0)
Diabetes 10/15 (66.7)
Chronic renal disease 5/15 (33.3)
Vascular disease in lower extremities 2/15 (13.3)
Cerebrovascular disease
Stroke 3/15 (20.0)
TIA 0/15 (0.0)
Prior valve replacement/repair
Mitral intervention 10/15 (66.7)
Surgical replacement 6/15 (40.0)
Surgical repair 3/15 (20.0)
Percutaneous repair 1/15 (6.7)
Aortic intervention 0/15 (0.0)
Pulmonic intervention 0/15 (0.0)
In primary rhythm
Sinus rhythm 5/15 (33.3)
Atrial fibrillation 10/15 (66.7)
Other conduction abnormality 5/15 (33.3)
Taking cardiac medications
Digoxin 5/15 (33.33)
ACE inhibitor or angiotensin II blocker 7/15 (43.3)
Beta-blocker 14/15 (93.3)
Calcium antagonist 4/15 (26.7)
Nitrates 4/15 (26.7)
Diuretic agents 15/15 (100.0)
Inotropic agent 0/15 (0.0)
Other 11/15 (73.3)
Values are mean � SD or n/N (%). ACE ¼ angiotensin-converting enzyme; CABG ¼coronary artery bypass graft; NYHA ¼ New York Heart Association; PCI ¼percutaneous coronary intervention; TIA ¼ transient ischemic attack.
J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7 Hahn et al.A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6 Transcatheter Annuloplasty for Functional TR
1801
attached to the remaining pledgeted suture and didnot require reintervention or result in adverseevents.
ECHOCARDIOGRAPHIC RESULTS. Echocardiographicmeasurements for the intention-to-treat populationare listed in Table 4 (complete list of measurementsare in Online Table 3). Right ventricular function byTAPSE and tissue Doppler was unchanged (p ¼ 0.46and 0.48, respectively). In the intention-to-treatcohort, there was a significant reduction in TAdiameter (4.0 � 0.5 cm vs. 3.9 � 0.5 cm, respectively;p ¼ 0.017) and a trend to reduction in TAA (12.3 �
2.8 cm2 vs. 11.5 � 2.5 cm2, respectively; p ¼ 0.061).The mean vena contracta diameter (1.3 � 0.3 vs. 1.1 �0.4, respectively; p ¼ 0.13) and EROA by both PISA(0.51 � 0.16 vs. 0.41 � 0.27, respectively; p ¼ 0.19) andquantitative Doppler (0.93 � 0.27 vs. 0.93 � 0.74,respectively; p ¼ 0.53) were not significantly reduced.Left ventricular stroke volume was significantlyincreased (67.1 � 18.1 ml vs. 72.8 � 23.2 ml, respec-tively; p ¼ 0.04) in the setting of stable left ventric-ular ejection fraction (p ¼ 0.85) and right ventricularfunction by TAPSE (p ¼ 0.46).
The TTE findings from the 12 patients withoutpledget detachment or as-treated population are lis-ted in Table 5 (complete list of measurements is inOnline Table 4). Of note, there was a significantreduction in mean vena contracta diameter (1.3 �0.4 vs. 1.0 � 0.3, respectively; p ¼ 0.022), TAA (12.3 �3.1 cm2 vs. 11.3 � 2.7 cm2, respectively; p ¼ 0.019),EROA by PISA (0.51 � 0.18 cm2 vs. 0.32 � 0.18 cm2,respectively; p ¼ 0.020) and quantitative Doppler(0.85 � 0.22 cm2 vs. 0.63 � 0.29 cm2, respectively;p ¼ 0.045). There were no changes in left ventricularejection fraction (p ¼ 0.90) or right ventricular TAPSE(p ¼ 0.31). There was, again, a significant increase inleft ventricular stroke volume (63.6 � 17.9 ml to71.5 � 25.7 ml, respectively; p ¼ 0.021).
In the as-treated patients with pledgets in theintended positions, the ellipticity of the regurgitantorifice showed no significant change (0.6 � 0.2 vs.0.6 � 0.2, respectively; p ¼ 0.92). In the setting of anelliptical orifice, the EROA by PISA method wassignificantly less than the EROA by quantitativeDoppler, both at baseline (0.5 � 0.2 vs. 0.9 � 0.2,respectively; p < 0.001) and after device implantation(0.3 � 0.2 vs. 0.6 � 0.3, respectively; p < 0.001).

TABLE 3 Measures of Technical Success
30-Day Outcome
Overall technical success 12/15 (80.0)
Successful access, delivery, and retrieval of the system 15/15 (100.0)
Deployment and correct positioning of device 12/15 (80.0)
No unplanned or emergency surgery or reinterventionrelated to the device or access procedure within 30days
14/15 (93.3)
Freedom from mortality within 30 days 15/15 (100.0)
Values n/N (%).
Hahn et al. J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7
Transcatheter Annuloplasty for Functional TR A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6
1802
In the 3 patients with single-pledget detachment,there were no significant differences between base-line and 30 days for TAA (12.18 � 1.34 cm2 vs. 12.54 �1.27 cm2, respectively; p ¼ 1.00), EROA by PISA (0.51 �0.06 cm2 vs. 0.76 � 0.28 cm2, respectively; p ¼ 0.18),or quantitative Doppler (1.22 � 0.31 cm2 vs. 2.00 �0.98 cm2, respectively; p ¼ 0.18).
QoL MEASURES. In the as-treated population(Table 6, Central Illustration), there were significantimprovements in NYHA functional class (allpatients $1 class; p ¼ 0.001), MLHFQ (49.6 � 15.7 to18.8 � 12.0, respectively; p < 0.001) and 6MWT (236.5� 107.4 m to 305.1 � 106.5 m, respectively; p ¼ 0.003).Quality of life for the intention-to-treat group is listedin Online Table 5. Compared with their baseline
TABLE 4 Summary of TEE Findings in the Intention-to-Treat Study G
Echocardiographic Variable Baseline
LVEF, % 59.9 � 11.5 (15)64.0 (39.2, 73.8)
RV TAPSE, cm 1.6 � 0.4 (15)1.6 (1.1, 2.1)
LVOT Doppler stroke volume, ml 67.1 � 18.1 (14)70.2 (38.5, 96.1)
TR vena contracta, cm 1.3 � 0.3 (14)1.3 (0.8, 2.2)
PISA EROA, cm2 0.51 � 0.16 (15)0.49 (0.30, 0.88)
PASP estimated, mm Hg 43.6 � 9.3 (15)44.4 (25.6, 56.4)
TV annular diameter, cm 4.0 � 0.5 (15)4.1 (3.1, 5.0)
Tethering distance, cm 0.7 � 0.2 (15)0.7 (0.3, 1.0)
2D TV annulus area, cm2 12.3 � 2.8 (15)11.9 (8.5, 17.4)
TR regurgitant volume, ml 86.0 � 21.3 (14)92.7 (52.0, 130.7)
Quantitative Doppler TR EROA, cm2 0.93 � 0.27 (15)0.87 (0.42, 1.57)
Values are mean � SD (N) and median (minimum, maximum). *Change from baseline tosigned rank test when normality assumptions are violated.
2D ¼ 2-dimensional; EROA ¼ effective regurgitant orifice area; LVEF ¼ left ventmin ¼ minimum; PASP ¼ pulmonary artery systolic pressure; PISA ¼ proximal isovelocityRVOT ¼ right ventricular outflow tract; TEE ¼ transesophageal echocardiography; TR ¼
values, these patients experienced significantimprovement in NYHA functional class ($1 class,p ¼ 0.001), MLHFQ (47.4 � 17.6 to 20.9 � 14.8,respectively; p < 0.001), and 6MWT results (245.2 �110.1 m to 298.0 � 107.6 m, respectively; p ¼ 0.008).
In the 3 patients with single-pledget detachment,there were no significant differences between base-line and 30 day values for NYHA functional class ($1class; p ¼ 0.17), MLHFQ (38.7 � 25.5 to 29.7 � 24.3,respectively; p ¼ 0.75), and 6MWT (279.7 � 138.3 m to269.7 � 130.8 m, respectively; p ¼ 1.00).
DISCUSSION
This is the first early feasibility trial to completeenrollment for an investigational tricuspid repairdevice. In this study, we report that the transcatheterplication device achieved 93% procedural successwith no procedural mortality or stroke, successfuldelivery, and retrieval of the device delivery systemwith proper device placement in all patients;quantitative reduction of TA measurements andTR severity, with concomitant increase in LVforward stroke volume; and improvement in QoLmeasurements.
Although functional or secondary TR is the mostcommon cause of severe TR in the Western world(31), it remains undertreated. The presence of
roup
30-Day Change* p Value†
59.7 � 11.9 (13)60.7 (37.6, 81.3)
0.4 � 7.6 (13)�1.6 (�12.7, 12.4)
0.853
1.6 � 0.4 (12)1.6 (1.3, 2.7)
0.0 � 0.6 (12)0.0 (�0.6, 1.4)
0.456
72.8 � 23.2 (14)69.7 (40.9, 124.5)
8.5 � 13.4 (13)6.6 (�7.8, 32.1)
0.041
1.1 � 0.4 (15)1.1 (0.6, 1.9)
�0.2 � 0.4 (14)�0.2 (�0.9, 0.7)
0.133
0.41 � 0.27 (15)0.32 (0.13, 1.04)
�0.11 � 0.30 (15)�0.10 (�0.49, 0.47)
0.192
40.9 � 9.5 (15)38.2 (29.2, 57.5)
�2.7 � 7.0 (15)�0.6 (�20.2, 5.9)
0.222
3.9 � 0.5 (15)3.9 (2.9, 4.8)
�0.2 � 0.4 (15)�0.2 (�0.6, 1.1)
0.017
0.6 � 0.1 (15)0.6 (0.4, 0.8)
�0.1 � 0.2 (15)�0.1 (�0.4, 0.4)
0.037
11.5 � 2.5 (15)11.1 (8.1, 15.2)
�0.7 � 1.4 (15)�0.6 (�2.7, 2.2)
0.061
78.7 � 53.3 (14)55.9 (31.0, 213.5)
�2.7 � 39.5 (13)�14.7 (�49.0, 82.7)
0.811
0.93 � 0.74 (14)0.68 (0.32, 3.06)
0.00 � 0.56 (14)�0.19 (�0.59, 1.49)
0.530
30 days computed using paired data. †p value by paired Student t-test or Wilcoxon
ricular ejection fraction; LVOT ¼ left ventricular outflow tract; max ¼ maximum;surface area; RV TAPSE ¼ right ventricular tricuspid annular plane systolic excursion;tricuspid regurgitation; TV ¼ tricuspid valve.

TABLE 6 QoL Outcomes for Intention-to-Treat Patients (N ¼ 15)
Outcome Baseline 30-Day Change p Value
NYHA functional classification 0.001
I 0/15 (0.0) 7/15 (46.7) –
II 5/15 (33.3) 8/15 (53.3) –
III 10/15 (66.7) 0/15 (0.0) –
IV 0/15 (0.0) 0/15 (0.0) –
MLHFQ score 47.4 � 17.6 (15)44.0 (13.0, 86.0)
20.9 � 14.8 (15)18.0 (2.0, 56.0)
�26.5 � 20.4 (15)�30.0 (�68.0, 17.0)
<0.001
6MWT (m) 245.2 � 110.1 (15)229.0 (56.7, 463.0)
298.0 � 107.6 (15)327.0 (76.2, 486.0)
52.9 � 72.6 (15)23.0 (�30.0, 262.7)
0.008
Values are n/N (%) or mean � SD (N) and median (minimum, maximum). 6MWT ¼ 6-min walk test; MLHFQ ¼Minnesota Living with Heart Failure Questionnaire; NYHA ¼ New York Heart Association.
TABLE 5 Summary of TTE Findings in the As-Treated Study Group
Echo Variable Baseline 30-Day Change* p Value†
LVEF, % 59.8 � 12.7 (12)66.0 (39.2, 73.8)
59.1 � 12.9 (11)60.7 (37.6, 81.3)
�0.3 � 7.3 (11)�1.6 (�12.7, 12.4)
0.904
RV TAPSE, cm 1.7 � 0.4 (12)1.7 (1.1, 2.1)
1.6 � 0.2 (10)1.6 (1.3, 1.9)
�0.1 � 0.4 (10)0.0 (�0.6, 0.3)
0.308
LVOT Doppler stroke volume, ml 63.6 � 17.9 (11)59.6 (38.5, 92.4)
71.5 � 25.7 (11)66.6 (40.9, 124.5)
11.7 � 13.2 (10)8.7 (�6.0, 32.1)
0.021
TR vena contracta mean, cm 1.3 � 0.4 (11)1.2 (0.8, 2.2)
1.0 � 0.3 (12)1.0 (0.6, 1.4)
�0.3 � 0.3 (11)�0.3 (�0.9, 0.3)
0.022
PISA EROA, cm2 0.51 � 0.18 (12)0.50 (0.30, 0.88)
0.32 � 0.18 (12)0.28 (0.13, 0.78)
�0.20 � 0.25 (12)�0.24 (�0.49, 0.42)
0.020
PASP estimated, mm Hg 44.1 � 10.2 (12)46.0 (25.6, 56.4)
42.0 � 9.5 (12)39.9 (29.2, 57.5)
�2.1 � 6.6 (12)�0.5 (�20.2, 5.9)
0.327
TV annular diameter, cm 4.0 � 0.5 (12)4.0 (3.1, 5.0)
3.8 � 0.6 (12)3.9 (2.9, 4.8)
�0.2 � 0.4 (12)�0.3 (�0.6, 1.1)
0.038
Tethering distance, cm 0.7 � 0.1 (12)0.7 (0.3, 0.8)
0.6 � 0.1 (12)0.6 (0.4, 0.7)
�0.1 � 0.2 (12)�0.1 (�0.4, 0.4)
0.116
TV annulus area (2D), cm2 12.3 � 3.1 (12)11.6 (8.5, 17.4)
11.3 � 2.7 (12)10.0 (8.1, 15.2)
�1.0 � 1.3 (12)�0.9 (�2.7, 1.5)
0.019
TR regurgitant volume, ml 79.6 � 17.5 (11)88.0 (52.0, 97.9)
57.1 � 29.0 (11)51.1 (31.0, 136.3)
�18.1 � 27.2 (10)�27.6 (�49.0, 44.2)
0.065
Quantitative Doppler TR EROA, cm2 0.85 � 0.22 (12)0.87 (0.42, 1.14)
0.63 � 0.29 (11)0.62 (0.32, 1.37)
�0.22 � 0.29 (11)�0.28 (�0.59, 0.53)
0.045
Values are mean � SD (N) and median (minimum, maximum). *Change from baseline to 30 days computed on paired data. †p value by paired Student t-test or Wilcoxon signed-rank test when normality assumptions are violated.
TTE ¼ transthoracic echocardiography; other abbreviations as in Table 4.
J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7 Hahn et al.A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6 Transcatheter Annuloplasty for Functional TR
1803
functional TR, either isolated or in combination withleft heart disease, is associated with an unfavorableprognosis (4,32–34). Surgical mortality for isolatedtricuspid valve interventions remains higher than forany other single valve surgery (35,36). Combinedtricuspid repair at the time of the left-sided diseasetreatment is not associated with a significant increasein mortality (37) and is recommended in the setting ofsignificant annular dilation and TR (7,38). Nonethe-less, moderate-to-severe TR is present in 1.6 millionU.S. individuals, and only a small portion (<0.5%) ofthis population currently undergoes surgicaltricuspid valve repair or replacement (39). Similarly,despite the benefits of tricuspid repair (8,9), a largenumber of patients undergoing left valve surgery donot have concomitant treatment of significant TR.This could be explained by an underestimation of TRseverity under anesthesia (40); or the misconceptionthat TR resolves following mitral valve surgery(9,41,42); and the overestimation of surgical riskwhen concomitant tricuspid valve surgery is per-formed at the time of mitral valve surgery (43–45). Asmore left-sided valve disease is treated with trans-catheter therapies, the negative impact of TR onsurvival in these patients has underscored theimportance of developing transcatheter solutions tothis disease (12,13,46).
The transcatheter plication system attempts toreplicate the results of the modified Kay
bicuspidization procedure described by Ghanta et al.(16) in 2007. This suture bicuspidization technique isperformed by placing a double pledget-supportedmattress suture from the anteroposterior commis-sure to the posteroseptal commissure along theposterior annulus and tying the suture down on anobturator to reduce the stress on the annulus. In theirfollow-up in 237 patients, Ghanta et al. (16) demon-strated that bicuspidization annuloplasty and ringannuloplasty for functional TR were equally durableand efficacious for reducing TR up to 3 years post-operatively.
The high procedural success achieved in thisstudy by 4 different heart teams speaks to the

Hahn et al. J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7
Transcatheter Annuloplasty for Functional TR A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6
1804
generalizability of this procedure. All patients had thedevice placed in the intended position, and all ach-ieved annular plication with no mortality and only 1unplanned right coronary artery stent implantedwithout adverse consequences. At 30 days, in 3 pa-tients, 1 of the 2 pledgeted sutures was no longerattached to the annulus but remained attached to theremaining annular suture, and importantly, no pa-tient required reintervention. The first patientdetachment occurred in the first patient entered intothe trial and could be explained by excessive manip-ulation of the annulus during initial pledget deliveryand cinching. Refinement in operator techniqueresulted in 4 subsequently successful implantationprocedures at this site. The second and third devicedetachments occurred at a single site, and determi-nation of cause is being investigated. Modeling andimproved characterization of TA tissue and variablesthat affect the degree of stress on the tissue generatedby the plication process may improve technicalsuccess.
Echocardiography plays an integral role in thesuccessful pre-procedural, intraprocedural, and post-procedural analysis of tricuspid valve morphologyand function. This is the first study to use not onlymultiparametric methods for assessing tricuspidregurgitant severity but multiple quantitative mea-sures as well. We purposefully elected to avoid usingthe labels mild, moderate, or severe TR whenreporting the results of this trial. Unfortunately, thecurrent guideline-suggested grading scheme for TR(25) fails to take into account its “torrential” nature inpatients we are currently treating. A vena contractaqualifies as severe at $0.7 cm; however, our patients,on average, had a vena contracta width of 1.3 cm.Likewise, an EROA of $0.40 cm2 qualifies as severe;however, our patients had an average quantitativeEROA of 0.85 cm2, more than double what theguidelines consider severe. If just the reduction inEROA is evaluated, the transcatheter plication systemreduced the quantitative EROA, on average, by>0.20 cm2, which according to the current guidelines,would be the equivalent of 1 to 2 grades. The PISAmethod is simple and easy to perform (26); however,the complex relationship of the isovelocity shellto the often elliptical shape (47,48) and enlarged sizeof the TR EROA results in a significant underestima-tion of the true EROA (49). If one uses the PISA EROAonly, the patients in this trial had TR EROA reducedfrom severe (0.51 � 0.18 cm2) to moderate (0.32 �0.18 cm2). Although the accuracy of the quantitativemethod should be validated, both methods per-formed in a core laboratory before and after devicedeployment showed significant reductions in TR
EROA, are associated with an increase in forwardstroke volume, and resulted in significant improve-ments in QoL measures.
The main objectives of any treatment of heartvalve disease are to improve QoL and survival.Tricuspid regurgitation does not have the same im-mediate impact on short-term mortality as otherheart valve diseases, and thus, QoL measurements,such as the disease-specific MLHFQ (50), may play asignificant role in future trial designs. In the SCOUTtrial, the as-treated population experienced animprovement in average MLHFQ score from 50 (poorhealth) to 19 (good health), with this change of31 points substantially exceeding the 5-point changeconsidered to be a large effect (51). In addition topatient-reported symptoms, tests such as the 6MWT,according to American Thoracic Society guidelines(52), have been used to objectify QoL and can predictmorbidity and mortality in some patients. Improve-ment in 6MWT has been shown to be reflect clinicallyimportant changes in symptoms and health status incohorts of patients with cardiac disease (53,54). In asmall study of patients with chronic heart failure,changes in 6MWTD of 25 to 50 m were associated withclinically meaningful changes in health status (54). Inthis study, a significant improvement in patient-reported symptoms was associated with objectiveimprovement in 6MWT (increase of 52.9 � 72.6 m).The substantial improvements in both MLHFQ and6MWT results support the findings of significant im-provements in echocardiographic measurements ofdisease severity and show that a reduction of even1 grade of TR is enough to improve QoL.
The 1 patient with failure to remodel the annulusdid not improve in QoL measures. At the time of theprocedure, the EROA was significantly larger than onqualifying TTE (>2 cm2), with marked dilation of theright ventricle. In this patient, the lack of responsemight have been due to the persistent and/or ongoingventricular dilation that was greater than could beeffectively treated with a single-pledget annular de-vice. A current modification of the SCOUT I protocolnow includes the possibility of implanting 2 pairsof pledgets, potentially allowing greater annularreduction.
STUDY LIMITATIONS. The relatively small number ofpatients in this early feasibility trial make conclu-sions about efficacy less robust; however, theconsistent reduction in TR and annular dimensionsassociated with a consistent improvement in QoLmeasures is promising. The quantitation of TR hasnot been extensively validated, but the methods ofthis study show the feasibility of preforming repeat

PERSPECTIVES
COMPETENCY IN PATIENT CARE AND PROCEDURAL
SKILLS: In selected patients, functional TR can be reduced by
transcatheter plication of the valve annulus.
TRANSLATIONAL OUTLOOK: Larger trials of transcatheter
tricuspid repair are needed to confirm the efficacy and safety of
this technology, quantify its impact on echocardiographic and
hemodynamic measurements of TR severity, and assess the
outcome and durability of the intervention in terms of symptoms
and QoL.
J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7 Hahn et al.A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6 Transcatheter Annuloplasty for Functional TR
1805
quantitation by multiple techniques and show achange in these parameters that correlates withclinical outcomes. Further studies comparing theseechocardiographic methods with cardiac magneticresonance should be performed. Finally, optimalmedical therapy in this study was determined by thereferring physician, and medication changesthroughout the study could have influenced theresults.
CONCLUSIONS
The SCOUT trial is the first multicenter early feasi-bility study of a novel transcatheter device for func-tional TR to complete enrollment in the United States.The 30-day results of the SCOUT trial confirmed thatthe device was safe, successfully reduced annulararea and regurgitant orifice, and improved left ven-tricular forward stroke volume. These changes wereassociated with improvements in functional statusand QoL measures.
ADDRESS FOR CORRESPONDENCE: Dr. Rebecca T.Hahn, Columbia University Medical Center, NewYork-Presbyterian Hospital, 177 Fort WashingtonAvenue, New York, New York 10032. E-mail: [email protected].
RE F E RENCE S
1. Rogers JH, BollingSF. The tricuspid valve: currentperspective and evolving management of tricuspidregurgitation. Circulation 2009;119:2718–25.
2. AntunesMJ, Barlow JB.Management of tricuspidvalve regurgitation. Heart 2007;93:271–6.
3. Najib MQ, Vinales KL, Vittala SS, et al. Pre-dictors for the development of severe tricuspidregurgitation with anatomically normal valve inpatients with atrial fibrillation. Echocardiography2012;29:140–6.
4. Nath J, Foster E, Heidenreich PA. Impact oftricuspid regurgitation on long-term survival. J AmColl Cardiol 2004;43:405–9.
5. Topilsky Y, Nkomo VT, Vatury O, et al. Clinicaloutcome of isolated tricuspid regurgitation. J AmColl Cardiol Img 2014;7:1185–94.
6. Taramasso M, Vanermen H, Maisano F, et al.The growing clinical importance of secondarytricuspid regurgitation. J Am Coll Cardiol 2012;59:703–10.
7. Nishimura RA, Otto CM, Bonow RO, et al. 2014AHA/ACC guideline for the management of pa-tients with valvular heart disease: a report of theAmerican College of Cardiology/American HeartAssociation Task Force on Practice Guidelines.J Am Coll Cardiol 2014;63:e57–185.
8. Tang GH, David TE, Singh SK, et al. Tricuspidvalve repair with an annuloplasty ring results inimproved long-term outcomes. Circulation 2006;114:I577–81.
9. Dreyfus GD, Corbi PJ, Chan KM, et al. Secondarytricuspid regurgitation or dilatation: which shouldbe the criteria for surgical repair? Ann Thorac Surg2005;79:127–32.
10. Mangoni AA, DiSalvo TG, Vlahakes GJ, et al.Outcome following isolated tricuspid valve
replacement. Eur J Cardiothoracic Surg 2001;19:68–73.
11. Kwon DA, Park JS, Chang HJ, et al. Predictionof outcome in patients undergoing surgery forsevere tricuspid regurgitation following mitralvalve surgery and role of tricuspid annular systolicvelocity. Am J Cardiol 2006;98:659–61.
12. Lindman BR, Maniar HS, Jaber WA, et al. Theeffect of tricuspid regurgitation and the rightheart on survival after transcatheter aortic valvereplacement: insights from the Placement ofAortic Transcatheter Valves II inoperable cohort.Circ Cardiovasc Interv 2015;8:e002073.
13. Ohno Y, Attizzani GF, Capodanno D, et al. As-sociation of tricuspid regurgitation with clinicaland echocardiographic outcomes after percuta-neous mitral valve repair with the MitraClip sys-tem: 30-day and 12-month follow-up from theGRASP registry. Eur Heart J Cardiovasc Imaging2014;15:1246–55.
14. Kay JH, Maselli-Campagna G, Tsuji KK. Surgicaltreatment of tricuspid insufficiency. Ann Surg1965;162:53–8.
15. Navia JL, Nowicki ER, Blackstone EH, et al.Surgical management of secondary tricuspid valveregurgitation: annulus, commissure, or leafletprocedure? J Thorac Cardiovasc Surg 2010;139:1473–82.
16. Ghanta RK, Chen R, Narayanasamy N, et al.Suture bicuspidization of the tricuspid valve versusring annuloplasty for repair of functional tricuspidregurgitation: midterm results of 237 consecutivepatients. J Thorac Cardiovasc Surg 2007;133:117–26.
17. Schofer J, Bijuklic K, Tiburtius C, et al. First-in-human transcatheter tricuspid valve repair in apatient with severely regurgitant tricuspid valve.J Am Coll Cardiol 2015;65:1190–5.
18. Latib A, Ancona MB, Agricola E, et al. Percu-taneous bicuspidization of the tricuspid valve.J Am Coll Cardiol Img 2016;10:488–9.
19. Malasa M, Werner N, Nickenig G, et al. Trans-catheter tricuspid valve repair in a patient withisolated functional tricuspid valve regurgitation.Eur Heart J 2016;37:855.
20. Douglas PS, DeCara JM, Devereux RB, et al.Echocardiographic imaging in clinical trials:American Society of Echocardiography standardsfor echocardiography core laboratories:endorsed by the American College of CardiologyFoundation. J Am Soc Echocardiogr 2009;22:755–65.
21. Baumgartner H, Hung J, Bermejo J, et al.Echocardiographic assessment of valve steno-sis: EAE/ASE recommendations for clinicalpractice. J Am Soc Echocardiogr 2009;22:1–23;quiz 101–2.
22. Lang RM, Badano LP, Mor-Avi V, et al.Recommendations for cardiac chamber quantifi-cation by echocardiography in adults: an updatefrom the American Society of Echocardiographyand the European Association of CardiovascularImaging. J Am Soc Echocardiogr 2015;28:1–39.
23. Haddad F, Hunt SA, Rosenthal DN, et al. Rightventricular function in cardiovascular disease, partI: anatomy, physiology, aging, and functionalassessment of the right ventricle. Circulation2008;117:1436–48.
24. Hergan K, Schuster A, Fruhwald J, et al.Comparison of left and right ventricular volumemeasurement using the Simpson’s method and thearea length method. Eur J Radiol 2008;65:270–8.
25. Zoghbi WA, Enriquez-Sarano M, Foster E, et al.Recommendations for evaluation of the severity ofnative valvular regurgitation with two-

Hahn et al. J A C C V O L . 6 9 , N O . 1 4 , 2 0 1 7
Transcatheter Annuloplasty for Functional TR A P R I L 1 1 , 2 0 1 7 : 1 7 9 5 – 8 0 6
1806
dimensional and Doppler echocardiography. J AmSoc Echocardiogr 2003;16:777–802.
26. Rivera JM, Mele D, Vandervoort PM, et al.Effective regurgitant orifice area in tricuspidregurgitation: clinical implementation and follow-up study. Am Heart J 1994;128:927–33.
27. van der Hulst AE, Westenberg JJ, Kroft LJ,et al. Tetralogy of Fallot: 3D velocity-encoded MRimaging for evaluation of right ventricular valveflow and diastolic function in patients aftercorrection. Radiology 2010;256:724–34.
28. de Agustin JA, Viliani D, Vieira C, et al. Prox-imal isovelocity surface area by single-beat three-dimensional color Doppler echocardiographyapplied for tricuspid regurgitation quantification.J Am Soc Echocardiogr 2013;26:1063–72.
29. Loeber CP, Goldberg SJ, Allen HD. Dopplerechocardiographic comparison of flows distal tothe four cardiac valves. J Am Coll Cardiol 1984;4:268–72.
30. Meijboom EJ, Horowitz S, Valdes-Cruz LM,et al. A Doppler echocardiographic method forcalculating volume flow across the tricuspid valve:correlative laboratory and clinical studies. Circu-lation 1985;71:551–6.
31. Cohen SR, Sell JE, McIntosh CL, et al. Tricuspidregurgitation in patients with acquired, chronic,pure mitral regurgitation. II. Nonoperative man-agement, tricuspid valve annuloplasty, andtricuspid valve replacement. J Thorac CardiovascSurg 1987;94:488–97.
32. Voelkel NF, Quaife RA, Leinwand LA, et al.Right ventricular function and failure: report of aNational Heart, Lung, and Blood Institute work-ing group on cellular and molecular mechanismsof right heart failure. Circulation 2006;114:1883–91.
33. Bustamante-Labarta M, Perrone S, De LaFuente RL, et al. Right atrial size and tricuspidregurgitation severity predict mortality or trans-plantation in primary pulmonary hypertension.J Am Soc Echocardiogr 2002;15:1160–4.
34. Lee JW, Song JM, Park JP, et al. Long-termprognosis of isolated significant tricuspid regur-gitation. Circ J 2010;74:375–80.
35. Kilic A, Saha-Chaudhuri P, Rankin JS, et al.Trends and outcomes of tricuspid valve surgery inNorth America: an analysis of more than 50,000patients from the Society of Thoracic Surgeons
database. Ann Thorac Surg 2013;96:1546–52;discussion 1552.
36. Beckmann A, Funkat AK, Lewandowski J, et al.Cardiac surgery in Germany during 2012: a reporton behalf of the German Society for Thoracic andCardiovascular Surgery. Thorac Cardiovasc Surg2014;62:5–17.
37. Badhwar V, Rankin JS, He M, et al. Performingconcomitant tricuspid valve repair at the time ofmitral valve operations is not associated withincreased operative mortality. Ann Thorac Surg2017;103:587–93.
38. Gosev I, Yammine M, McGurk S, et al. Shouldmoderate-to-severe tricuspid regurgitation berepaired during reoperative left-sided valve pro-cedures? Semin Thorac Cardiovasc Surg 2016;28:38–45.
39. Stuge O, Liddicoat J. Emerging opportunitiesfor cardiac surgeons within structural heart dis-ease. J Thorac Cardiovasc Surg 2006;132:1258–61.
40. Frater R. Tricuspid insufficiency. J ThoracCardiovasc Surg 2001;122:427–9.
41. McCarthy PM, Bhudia SK, Rajeswaran J, et al.Tricuspid valve repair: durability and risk factors forfailure. J Thorac Cardiovasc Surg 2004;127:674–85.
42. Porter A, Shapira Y, Wurzel M, et al. Tricuspidregurgitation late after mitral valve replacement:clinical and echocardiographic evaluation. J HeartValve Dis 1999;8:57–62.
43. Di Mauro M, Bivona A, Iacò AL, et al. Mitralvalve surgery for functional mitral regurgitation:prognostic role of tricuspid regurgitation. Eur JCardiothoracic Surg 2009;35:635–9; discussion639–40.
44. Calafiore AM, Gallina S, Iacò AL, et al. Mitralvalve surgery for functional mitral regurgitation:should moderate-or-more tricuspid regurgitationbe treated? A propensity score analysis. AnnThorac Surg 2009;87:698–703.
45. Pfannmueller B, Verevkin A, Borger MA, et al.Role of tricuspid valve repair for moderatetricuspid regurgitation during minimally invasivemitral valve surgery. Thorac Cardiovasc Surg 2013;61:386–91.
46. Frangieh AH, Gruner C, Mikulicic F, et al.Impact of percutaneous mitral valve repair usingthe MitraClip system on tricuspid regurgitation.EuroIntervention 2016;11:e1680–6.
47. Sugeng L, Weinert L, Lang RM. Real-time 3-dimensional color Doppler flow of mitral andtricuspid regurgitation: feasibility and initialquantitative comparison with 2-dimensionalmethods. J Am Soc Echocardiogr 2007;20:1050–7.
48. Song JM, Jang MK, Choi YS, et al. The venacontracta in functional tricuspid regurgitation: areal-time three-dimensional color Doppler echo-cardiography study. J Am Soc Echocardiogr 2011;24:663–70.
49. Rodriguez L, Anconina J, Flachskampf FA,et al. Impact of finite orifice size on proximal flowconvergence. Implications for Doppler quantifica-tion of valvular regurgitation. Circ Res 1992;70:923–30.
50. Supino PG, Borer JS, Franciosa JA, et al.Acceptability and psychometric properties of theMinnesota Living With Heart Failure Questionnaireamong patients undergoing heart valve surgery:validation and comparison with SF-36. J CardiacFail 2009;15:267–77.
51. Holmes C, Briffa N. Patient-Reported OutcomeMeasures (PROMS) in patients undergoing heartvalve surgery: why should we measure them andwhich instruments should we use? Open Heart2016;3:e000315.
52. ATS Committee on Proficiency Standardsfor Clinical Pulmonary Function Laboratories.ATS statement: guidelines for the six-minutewalk test. Am J Respir Crit Care Med 2002;166:111–7.
53. Shoemaker MJ, Curtis AB, Vangsnes E, et al.Triangulating clinically meaningful change in thesix-minute walk test in individuals with chronicheart failure: a systematic review. CardiopulmPhys Ther J 2012;23:5–15.
54. O’Keeffe ST, Lye M, Donnellan C, et al.Reproducibility and responsiveness of quality oflife assessment and six minute walk test in elderlyheart failure patients. Heart 1998;80:377–82.
KEY WORDS echocardiography,transcatheter repair, tricuspid valveregurgitation
APPENDIX For supplemental tables, pleasesee the online version of this article.