-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
1/19
Feature Article
Early Life Events and Their Consequences for LaterDisease: A
Life History and Evolutionary Perspective
PETER D. GLUCKMAN,1,2* MARK A. HANSON,2 AND ALAN S.
BEEDLE11Liggins Institute, University of Auckland, and National
Research Centre for Growth and Development,
Private Bag 92019, Auckland, New Zealand2Centre for
Developmental Origins of Health and Disease, University of
Southampton, Southampton SO16 5YA,United Kingdom
ABSTRACT Biomedical science has little considered the relevance
of life history theory and
evolutionary and ecological developmental biology to clinical
medicine. However, the observa-
tions that early life influences can alter later disease riskthe
developmental origins of health
and disease (DOHaD) paradigmhave led to a recognition that these
perspectives can inform
our understanding of human biology. We propose that the DOHaD
phenomenon can be consid-ered as a subset of the broader processes
of developmental plasticity by which organisms adapt
to their environment during their life course. Such adaptive
processes allow genotypic variation
to be preserved through transient environmental changes. Cues
for plasticity operate particu-
larly during early development; they may affect a single organ
or system, but generally they
induce integrated adjustments in the mature phenotype, a process
underpinned by epigenetic
mechanisms and influenced by prediction of the mature
environment. In mammals, an adverse
intrauterine environment results in an integrated suite of
responses, suggesting the involve-
ment of a few key regulatory genes, that resets the
developmental trajectory in expectation of
poor postnatal conditions. Mismatch between the anticipated and
the actual mature environ-
ment exposes the organism to risk of adverse consequencesthe
greater the mismatch, the
greater the risk. For humans, prediction is inaccurate for many
individuals because of changes
in the postnatal environment toward energy-dense nutrition and
low energy expenditure, con-tributing to the epidemic of chronic
noncommunicable disease. This view of human disease from
the perspectives of life history biology and evolutionary theory
offers new approaches to preven-
tion, diagnosis and intervention. Am. J. Hum. Biol. 19: 119,
2007. ' 2006 Wiley-Liss, Inc.
There has been an increased focus on thepossible role that early
life events might playin the generation of later disease risk
inhumans. There is a considerable literaturerelating the nature of
infant feeding to laterhealth consequences (e.g., Lucas, 1991)
and
also relating birth size to later risk of disease(e.g., Syddall
et al., 2005). These observationsin turn arose from earlier studies
linking theconditions of life in infancy to later disease riskand
mortality (Barker and Osmond, 1986;Forsdahl, 1977), a link more
recently con-firmed by extensive epidemiological studies(reviewed
by Godfrey, 2006).
Although the epidemiological associationsare strong, a
mechanistic understanding isessential in order to demonstrate that
theseassociations are causal and in what way, andto identify the
potential for intervention.
Mechanistically and experimentally, there isan increasing body
of knowledge showing that
manipulation of the environment in the periodextending from
conception to infancy can beassociated with permanent changes in
physiol-ogy and/or structure. In turn, many of thesechanges are
associated with permanent altera-tions in gene expression regulated
by epige-
netic factors such as DNA methylation and his-tone
methylation/acetylation (Gluckman andHanson, 2006a).
In this article, we place these clinical and ex-perimental
observations connecting early life
Contract grant sponsor: M.A.H. is supported by theBritish Heart
Foundation.
*Correspondence to: Peter D. Gluckman, Liggins Insti-tute,
University of Auckland, Private Bag 92019, Auckland,New Zealand.
E-mail: [email protected]
Received 1 June 2006; Revision received 17 August 2006;Accepted
29 August 2006
Published online in Wiley InterScience
(www.interscience.wiley.com). DOI 10.1002/ajhb.20590
AMERICAN JOURNAL OF HUMAN BIOLOGY 19:119 (2 007)
VVC 2006 Wiley-Liss, Inc.
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
2/19
events with later disease consequences, gener-ally known as the
developmental origins ofhealth and disease (DOHaD)
phenomenon,within a wider framework encompassing life
history and evolutionary concepts. We suggestthat the DOHaD
phenomenon represents themost visible manifestation of the
fundamentalprocesses of developmental plasticity by whichmammals
adjust their life history strategy inresponse to environmental cues
during earlydevelopment.
DEVELOPMENTAL ORIGINS OF HEALTHAND DISEASE
The origin of the DOHaD concept arosefrom epidemiological
observations relatingbirth size to an altered risk of
cardiovasculardisease (Barker and Osmond, 1986) and type2 diabetes
(Hales et al., 1991). The earliest con-cepts directly linked
failure of fetal growth topermanent changes in structure and
functionthat predisposed to disease. Subsequently, itwas suggested
that these changes might alsohave adaptive value in a deprived (in
nutri-tional terms) postnatal environment by makingthe individual
permanently thrifty, e.g. bybeing small and insulin resistant. This
thriftyphenotype hypothesis (Hales and Barker,
2001) was placed in contradistinction to Neelsthrifty genotype
hypothesis (Neel, 1962) inwhich he had proposed that the thrifty
aspectsof the contemporary individual arose from genesselected over
a long time period during ourancestors huntergatherer existence.
The con-sequences were however similarthe adult or-ganism would be
well suited to an environmentin which nutrient supplies were
limited butwould be more likely to be become unhealthy ina
nutritionally rich environment.
It is now clear that small birth size is not anobligatory part
of the pathway leading to in-
creased disease riskduring development,many environmental
factors (cues) can inducechanges in physiology and anatomy with
long-term consequences, and in humans, these maybe manifested as
altered disease risk, withoutnecessarily inducing a major, or
indeed any,change in birth size. This is partly evident fromthe
graded relation between disease risk andbirth size that occurs
across the normal birth-weight range (e.g., Barker, 1998).
Moreover, itis now known that prematurity independent ofgrowth
retardation is also associated with long-term metabolic
consequences (Hofman et al.,
2004), and the offspring of women subjected tosevere
undernutrition in early pregnancy dur-
ing the famine in the winter of 1944/1945 inthe Netherlands did
not have reduced birthweight but do have an increased risk of
obesity(Painter et al., 2005).
A range of epidemiological studies in manypopulations now
extends the disease risk pro-file to include coronary heart disease
andstroke; insulin resistance and thus type 2 dia-betes; altered
endothelial function and in-creased risk of hypertension; central
and pe-ripheral propensity to obesity; altered bodycomposition,
including reduced bone mineraldensity which may lead to
osteoporosis; andpossible effects on cognitive and
emotionalfunction. There are several recent biomedicallyfocused
reviews of the DOHaD concept and theobservations that support it
(Gluckman andHanson, 2006a), including those published re-cently in
this journal (Kuzawa and Pike, 2005),so this review will focus on
the broader inter-pretation and significance of this
association.
There are limitations to both the classicalthrifty genotypic and
phenotypic models, al-though both have been important in the
evolu-tion of understanding in the field. We havebuilt off these to
consider further the potentialadaptive basis of the DOHAD
phenomenon andits relationship to the processes of develop-mental
plasticity. The original thrifty geno-
type hypothesis posited that the high incidenceof obesity and
insulin resistance in westernpopulations was a result of ancestral
selectionfor marginal nutritional environments andthat the
expression of these thrifty genes re-sulted in a greater risk of
obesity and insulinresistance in the presence of high energy
in-take and low energy expenditure. But faminein our huntergatherer
ancestors may havebeen less common than supposed (Benyshekand
Watson, 2006), the search for thrifty geneshas been unproductive,
and the ability to repro-duce these phenomena by manipulation of
ex-
perimental animals of uniform genetic back-ground (reviewed in
Gluckman et al., 2005b;McMillen and Robinson, 2005) and by
short-term natural experiments such as the DutchHunger Winter
(Painter et al., 2005) arguesagainst a purely genetic explanation.
Nonethe-less, genetic variation will play a role in deter-mining
sensitivity to environmental stimuli,and the presence of such
effects as reflected inthe influence of specific polymorphisms
withinthe epidemiological observations is well docu-mented
(Eriksson et al., 2002; Jordan et al.,2005; Kajantie et al., 2004;
Kubaszek et al.,
2004; Weedon et al., 2005). How genetic varia-tion and
environmental cues may interact to
2 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
3/19
match the phenotype predictively to the envi-ronment has
recently been modeled (Leimaret al., 2006).
The thrifty phenotype model developed by
Hales and Barker attempted to explain the epi-demiological
relationship between birth sizeand disease risk by proposing that
the fetusadapts to maternal undernutrition by growthretardation,
which leaves the adult better eq-uipped to cope in a deprived
rather than an en-riched postnatal environment. This adaptivemodel
suggests that the organism responds toimmediate challenges by
reducing growth, per-haps by mechanisms involving reduced
insulinsensitivity, but must then cope postnatally withthe
consequences for the rest of its life. Al-though this model can
explain a relationship
between low birthweight and disease risk, ithas limitations. As
noted above, it cannot easilyexplain the continuous relationship
betweenbirth size and disease risk that occurs even inthe upper
part of the birthweight range. Norcan it explain how early life
events can inducelong-term physiological changes withoutchanges in
birth size. It cannot explain develop-mental induction in systems
not involvingnutritionfor example induction in the sys-tems
regulating behavior, body temperature, orfluid balance for which
there is good experi-mental evidence (Gate et al., 1999; Ross et
al.,2005; Vickers et al., 2003). Finally, it is incon-sistent with
recent clinical data suggesting thatsmall-for-gestational-age
individuals are bornwith enhanced insulin sensitivity and that
in-sulin resistance appears later in life (Ibanezet al., 2006;
Mericq et al., 2005)these observa-tions imply that any adaptive
advantage ofreduced insulin sensitivity only becomes mani-fest
after the neonatal period.
The word thrifty implies directionality in-herent in the
underlying mechanisms and thisis not the case. Recent studies in
infants born
after in vitro fertilization show that they growup thinner,
taller, and with enhanced insulinsensitivity, demonstrating that
early life eventscan adjust subsequent metabolic physiology
ineither direction (Cutfield, 2005). Moreover,large infants are
also at risk of other later-lifedisease consequences, such as an
increasedrisk of breast cancer (Dos Santos et al., 2004)probably
mediated by higher estradiol levels(Jasienska et al., 2006). We
have thereforesuggested that the original observations re-lating
birth size to cardiovascular and meta-bolic disease risk represent
a special case of a
much broader and generalizable phenomenonthat allows the pattern
of development to be
modified in either direction as a result of de-velopmental cues
(Gluckman and Hanson,2004b; Gluckman et al., 2005c,d).
CLASSES OF DEVELOPMENTAL RESPONSEAND THEIR ADAPTIVE VALUE
Environmental factors acting during thephase of developmental
plasticity can either actto disrupt the normal program of
developmentor to modulate it (Gluckman et al., 2005d).Developmental
disruption may be overtly ter-atogenic, leading to gross structural
malfor-mation, or may be much more subtle. Clearly,such disruptive
responses cannot be consid-ered adaptive.
The processes of phenotypic plasticity per-
mit a range of phenotypes to be expressedfrom one
genotypeindeed, the concept of thereaction norm was developed to
demonstrateand illustrate this potential range of pheno-types
(Schlichting and Pigliucci, 1998). Thepresumption is that there is
potential adapt-ive advantage for a particular phenotype in
aspecific environmental situation (Eshel andMatessi, 1998),
although empirical proof ofsuch enhanced fitness is a formidable
chal-lenge. However, as we have detailed elsewhere(Gluckman and
Hanson, 2005), it is useful todistinguish adaptive responses to
environmen-tal cues that have their potential advantage inclose
temporal proximity to the cue from thosewhere the cue operates in
one phase but thepotential advantage is manifested in a laterphase
of the life course.
Immediately adaptive responses
Traditionally, developmental plasticity haslargely been viewed
in terms of the immedi-ately adaptive class of response. For
example,the altered morphology of the tadpole in re-
sponse to intraspecific competition can be seenas immediately
advantageous although it mayincur a cost later in life (Relyea and
Hoverman,2003). Premature metamorphosis in the spa-defoot toad is
another example of a responsewhere the advantage is essentially
immedi-atelinked to survival if the pond is evapo-ratingbut which
may have a fitness cost inreduced adult size later in life (Newman,
1992).Both these examples illustrate that the ad-vantages of an
immediate alteration in devel-opmental pattern that ensures
short-termsurvival must be traded off against potential
disadvantages in a later environment, andsuch adaptive arguments
are generally used
3DEVELOPMENTAL CHOICE OF LIFE HISTORY STRATEGY
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
4/19
to explain the evolution of developmentalplasticity.
Intrauterine growth retardation and mildprematurity in the human
can both be seen as
analogous immediately advantageous adapta-tions. The major
nongenetic cause of intrau-terine growth impairment is a reduced
nutri-tional supply across the placenta to the fetus.This may arise
because of maternal or placen-tal disease or from excessive
maternal con-straint. The fetus responds to reduced nutri-ent
supply by reducing its anabolic demand,in part by reducing plasma
concentrations ofinsulin and of plasma and tissue concentra-tions
of insulin-like growth factor (IGF)-1,which are the two
best-documented fetal growth-promoting hormones (Gluckman, 1995).
There
is also a major redistribution of fetal blood flowto protect
development of the critical organs, inparticular the fetal brain,
which can lead to adegree of asymmetrical growth retardation.This
reduction in fetal growth is clearly neces-sary to allow fetal
survival to birth. But beingborn small has consequences. The risk
of neo-natal death and morbidity is significantlyhigher (Spencer,
2003; Wilcox, 2001) and so arethe risks of subsequent cognitive
impairmentand persistent growth failure (Gluckman andHarding, 1997;
McCarton et al., 1996). Clearly,immediate survival has been
achieved at thecost of the individual being at greater subse-quent
risk.
Prematurity provides a similar example. Pre-mature birth can
result from an infectiousintrauterine environment in which the
fetus isat greater risk. Some prematurity also appearsto be induced
by maternal behavior that mightcompromise the fetus, such as poor
nutrition orsmoking, or by maternal psychosocial stress.Premature
induction of labor clearly involves atradeoff between the risk of
continued exposureto an abnormal intrauterine environment and
that of being born at full-term but with the in-creased risk of
postnatal morbidity and mortal-ity (Pike, 2006). Preterm delivery
as an imme-diately adaptive response may also benefit themothers
future reproductive fitness by limitinginvestment in a particular
pregnancy (Pike,2006).
Predictive adaptive responses
Conversely, there are a number of clear ex-amples where the
developing organism makesphenotypic responses during development
to
obtain an adaptive advantage, but where thatadaptive advantage
is delayed. We have termed
these predictive adaptive responses (Gluckmanet al., 2005c).
Adult desert locusts show polyphenism, ex-isting as migratory or
solitary forms in which
metabolism, wing shape, behavior, and colora-tion differ. The
choice of adult phenotype isdetermined in the larval stage in
response tochemical cues from the mother, but the advan-tages and
appropriateness of the choice are ex-hibited only after final
metamorphosis (Apple-baum and Heifetz, 1999). Clearly in this
casethe constraints of developmental pathwaysrequire the choice to
be made at an early stagein development, and in polyphenic species
suchas the locust there are two distinct morphs,although
intermediates may form. In themountain vole, the decision about the
tempo of
growth and acquisition of sexual maturity ismade in relation to
the season of yearanimalsborn early in the summer undergo
rapidgrowth and breed early, whereas animals bornlate in the season
grow slowly and overwinteras prepubertal animals of subadult size
(Neguset al., 1992). In the meadow vole, coat thicknessfor life is
determined before birth by maternalsignals involving melatonin,
related to whetherday length is shortening or lengthening.
Thethermal environment before birth and in thenest is similar, so
the advantage of the choice ofcoat thickness does not appear until
somemonths later when summer or winter tempera-tures are
encountered (Lee and Zucker, 1988;Lee et al., 1989). In each of
these examples, adevelopmental pathway is chosen in expecta-tion of
a future environment and fitness is en-hanced if the predicted
environment is matchedto the phenotype that has developed. It is
easy toenvisage the evolutionarypathwayto the appear-ance of these
predictive adaptive responses, sincethey involve some
relativelypredictable feature oftheenvironment.Although these
examples illus-trate a dichotomy in the mature phenotype, we
would anticipate that predictive adaptive res-ponses can also be
reflected over a continuousrange of phenotypes.
Predictive adaptive responses can only beadaptive if the
forecast is correct and will bemaladaptive if it is not. The
retention of mecha-nisms underpinning such phenotypic memorywill be
advantageous provided that the predic-tion is generally more often
correct than incor-rect, although this in turn depends on the
rela-tive fitness of each phenotype in the predictedand
nonpredicted environments and on therate of environmental change
relative to gener-
ation time (Jablonka et al., 1995; Moran, 1992;Sultan and
Spencer, 2002). Modeling shows
4 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
5/19
that these processes would be particularlyvaluable in allowing
an organism to survive dur-ing a transient environmental shift
(Gluckmanet al., 2005c; Jablonka et al., 1995; Moran,
1992).These different types of responseimmedi-
ate or predictive, disruptive, or adaptiveto anenvironmental cue
have been presented as dis-continuous, but there will be overlap.
Indeed,the same environmental cue may induce pre-sumptively
adaptive or disruptive responsesdepending on its magnitude. For
example,maternal hyperglycemia may induce congeni-tal heart
defects, a disruptive response, oralterations in fetal growth with
long-term con-sequences that may be adaptive. A develop-mental
response to an endocrine disruptor may
involve interactions between the hormone-liketoxin and the
normal processes of developmen-tal plasticity (Heindel and Lawler,
2006), butalthough such interactions use physiologicalmechanisms
they disrupt development andcannotbeconsideredadaptive.
Evaluating whether a response is adaptiveor disruptive may be
difficult in a given experi-mental situation. For example, is the
reductionin nephron number in sheep after maternal ex-posure to
very high doses of glucocorticoids inearly gestation (Wintour et
al., 2003) a process
where the steroid has disrupted the normalpattern of nephron
differentiation, or is it partof some adaptive process mimicking a
normalsituation where the fetus responds to mater-nal
glucocorticoids crossing the placenta undersituations of maternal
stress? Similarly, is thecontinuous relationship between
maternalvitamin A intake and nephron number in therat
(Lelievre-Pegorier et al., 1998) a dose-de-pendent disruptive
effect or doesit have adaptivevalue? Equally, a fetal adaptive
response mayhave both an immediate and a predictive compo-nent. The
accelerated maturation of the fetus of a
malnourished mother may induce prematuredelivery, which we can
consider as providingadvantage potentially benefiting both
motherand fetus (Pike, 2006), but it may also be partof a
predictive response allowing the organismto cope better in a later
environment perceivedto be threatening.
There are now several lines of evidence thatsupport the
predictive adaptive hypothesis. Inrats subjected to maternal
undernutrition dur-ing pregnancy, the offspring develop a
per-turbed metabolic phenotype showing
obesity,hyperphagia,hyperinsulinemia, andreducedac-
tivity in open field testing, particularly if theyare fed a
high-fat diet after weaning (Vickers
et al., 2000, 2003). In this case, the poor prena-tal nutrition
led to prediction of a poor post-natal environment, but in reality
the postnatalenvironment was nutritionally rich. Recent
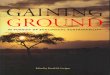
data (Fig. 1) show how the prediction can be re-versed provided
that the modifying cue occursduring the phase of developmental
plasticity. Ifprenatally undernourished rat pups are givenleptin
subcutaneously in the neonatal periodthey grow up, even on a
high-fat diet, with ametabolic phenotype identical to that of
ratsborn to a normally nourished mother (Vickerset al., 2005). It
appears that the neonatal ratpup has been tricked into perceiving
that it isfatter than it is, leptin being a hormone madeby fat.
Because this neonatal stimulus occurswithin the window of
developmental plasticity,
at least for metabolic physiology, it is possiblefor the
prenatal prediction to be changed fromone of an adverse environment
to one of anenergy-rich environment, with the consequentalterations
in physiology (Gluckman et al.,2006). At a mechanistic level this
may involvethe synaptogenic actions of leptin (Bouretet al., 2004)
or its peripheral actions, for exam-ple on pancreatic cell
apoptosis and prolifera-tion (Islam et al., 2000; Shimabukuro et
al.,1998).
Another consideration recently recognized isthe importance of
the interaction between theeffect of the prenatal cues on the
phenotypeand its consequent effect on the response to thepostnatal
environment. For example, in ratsthe prenatal environment
determines both pe-ripheral and central sensitivity to
high-energynutritional intake imposed after weaning(Vickers et al.,
2000). The effects of the inducedphenotype can be exacerbated
(Hales andOzanne, 2003; Vickers et al., 2000) or amelio-rated
(Jimenez-Chillaron et al., 2006; Stofferset al., 2003; Vickers et
al., 2005; Wyrwoll et al.,2006) by postnatal interventions,
indicating a
window of physiological plasticity that extendsbeyond the
intrauterine period. In this discus-sion, we have simplistically
described only onedevelopmental environment and only one ma-ture
environment, but it would be more realis-tic to envisage a cascade
whereby a series of ge-notype-environment interactions during
onestage in development determines the settingfor interactions with
the environment at thenext stage, and so on.
There is increasing evidence that predictiveadaptive responses
are underpinned by epige-netic changes. These may be manifest as
al-
tered gene expression and consequent alteredregulatory control
or, given the importance of
5DEVELOPMENTAL CHOICE OF LIFE HISTORY STRATEGY
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
6/19
epigenetic mechanisms to developmental biol-ogy, as
organizational change and altered tis-sue development. There is a
growing body of lit-
erature relating prenatal manipulation by hor-monal or
nutritional stimuli to methylation ofDNA andchanges in chromatin
structure affect-ing the expression of genes underlying thealtered
phenotype. For example, maternalbehavior in rats can be manipulated
to leave theoffspring as adults with altered stress responsesand
behavior. This is associated with alterationsin the expression of
the glucocorticoid receptorin the hippocampus, which in turn are
causedby alterations in DNA methylation in a pro-moter sequence for
the gene. The altered pheno-type can be reversed by chemical
manipulation
of histone acetylation, one of the consequencesof DNA
methylation (Weaver et al., 2004). In
another experimental model, the offspring offemale rats exposed
to a low-protein diet showchanges in expression of several genes,
includ-
ing that for the glucocorticoid receptor, in theliver, heart,
muscle, and fat (Bertram et al.,2001); such changes are associated
with alteredDNA methylation and can be reversed by folicacid
supplementation during the period ofmaternal malnutrition
(Lillycrop et al., 2005).We have preliminary evidence that the
reversalof the effects of prenatal undernutrition by post-natal
leptin treatment (Vickers et al., 2005) isaccompanied by
coordinated changes in expres-sion and promoter methylation of key
genes.
There is increasing interest in epigenetictransmission across
generations (Chong and
Whitelaw, 2004; Drake and Walker, 2004),although the mechanisms
and their relevance
Fig. 1. Reversal of developmental induction by neonatal leptin
treatment. Rat dams were fed ad libitumthroughout pregnancy (AD) or
undernourished throughout pregnancy (UN). Pups from UN mothers were
cross-fos-tered to AD mothers after birth to standardize postnatal
feeding, and all offspring were fed a high-fat diet afterweaning.
The neonates were treated with either saline (S) or recombinant rat
leptin (L) on postnatal days 313.Total body fat and metabolic
profile as reflected by fasting plasma leptin, insulin and
C-peptide (a marker of pan-creatic insulin secretion)
concentrations were measured in adult females (postnatal day 170).
Untreated prenatallyundernourished animals (UN S) were obese,
hyperinsulinemic and hyperleptinemic as adults compared with
con-trol animals (AD S); development of this metabolic phenotype
was prevented by neonatal leptin treatment (UN L).
Values are means6SEMfor eight animals pergroup(redrawnfrom data
in Vickers et al., 2005).
6 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
7/19
to reported transgenerational inheritance inhumans (Kaati et
al., 2002; Pembrey et al.,2006) are poorly understood. There is
experi-mental evidence that developmental induction
can be transmitted from the F0 generation tothe F1 generation
and beyond through the maleand/or female lines after hormonal
(Drakeet al., 2005) or nutritional (Benyshek et al.,2006; Zambrano
et al., 2005) cues. Alterna-tively, there are indirect means by
which envi-ronmental influences can be reflected acrosstwo or more
generationsfor example, theuterine size of a female may be
influenced byher experience as a fetus (Ibanez et al., 2003)and
this in turn may influence the size of herown progeny.
THE DOHaD PARADIGMAN ADAPTIVEPERSPECTIVE
We have used the concept of predictive ad-aptive responses to
explain the observationsthat led to the development of the DOHaD
par-adigm (Gluckman et al., 2005b). We have sug-gested that the
developing organism senses itsmetabolic milieu and adjusts its
physiologicalhomeostatic setpoints according to the environ-ment it
forecasts will exist after birth. If thesignals in the
developmental phase suggest
limited nutrient availability, then the organismwill adjust its
developmental trajectory suchthat the mature individual has a
metabolic ho-meostasis better adapted for survival in asparse
environment. Any association betweenthe outcome and birth size is
thus an epipheno-menon of the relationship between
nutrientavailability and the induction of predictive ad-aptive
responses. Such a model can explain theobserved continuous
associations between birthsize and disease risk, how disease risk
may beindependent of changes in birth size, and howdevelopmental
induction can occur in other
physiological systems.An important feature of such a model is
thatthe alterations in regulatory systems inducedby the
developmental cues may be subtle andnot observable under basal
conditionstheymay affect the sensitivity of a physiologicalresponse
underpinning a specific trait in theadult and thus make the
organism more or lesssusceptible to disease in an extreme
postnatalenvironment. Lifestyle disease in the humanthen occurs
when the individual lives in anenvironment beyond their forecasted
andinduced physiological homeostatic rangewe
term this the match-mismatch model. Wherethe organisms
physiology is matched by devel-
opmental processes to the environment inwhich it lives in later
life, its risk of disease islower; when it is mismatched, its risk
is higher(Fig. 2). Clearly, both immediate and predictive
components may play a role in the final pheno-type and there
will be a degree of interactionbetween the two, particularly if the
environ-mental cues are more extreme. For example,we have elsewhere
suggested that predictiveresponses play a role in determining the
role ofprenatal nutrition in the timing of menarche,although this
effect is modified by nutritionalstatus in the peripubertal period
(Gluckmanand Hanson, 2006b).
Implicit in this discussion is the view thatthe DOHaD phenomenon
is underpinned byphysiological mechanisms that have evolved in
mammals to provide adaptive advantage. Thereare several reasons,
based on a large body of ex-perimental evidence reviewed in detail
else-where (Gluckman et al., 2005b), why we believethis to be so.
First, it is very easy to demon-strate this phenomenon in a wide
variety ofmammalian species with diverse life historystrategies,
there being data from experimentalmanipulation in mice, rats,
sheep, pigs, guineapigs, and non-human primates and from
epide-miological studies in humans. Second, relation-ships similar
to the human epidemiologicalfindings can be seen in animals even in
the ab-sence of maternal manipulation, suggesting aphenomenon that
represents physiological plas-ticity rather than pathology. Third,
a relativelysimilar phenotype can be induced by a varietyof
nutritional or hormonal manipulations act-ing either early or late
in developmentfor ex-ample, a trend to obesity, insulin
resistance,and endothelial dysfunction can be inducedby high-fat
diets, low-protein diets, maternalglobal undernutrition, and
maternal glucocorti-coid exposure at differing times in gestation
insheep, rats, mice, and guinea pigs. That these
different cues converge on a common outcomereflecting an
integrated response of the fetus toa perceived threatening
postnatal environmentsuggests that the induced phenotype has
valuefor the fitness of the offspring. Finally, our dem-onstration
that the integrated phenotypeinduced by prenatal nutritional insult
can becompletely reversed by a simple postnatal endo-crine
manipulation (Fig. 1; Vickers et al., 2005)argues for a single
mechanism underpinning abroad range of developmental effects.
Stearns and Ebert (2001) have usefully sum-marized criteria for
distinguishing adaptive
from nonadaptive processes. One such criteriondefines an
adaptation as a change in a phe-
7DEVELOPMENTAL CHOICE OF LIFE HISTORY STRATEGY
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
8/19
notype that occurs in response to a specificenvironmental signal
. . . resulting in improvedgrowth, survival, or reproduction. We
havelinked prenatal nutritional insult to a definedchange in
phenotype; later in this review, weexplain why we believe that this
phenotypeimproves survival in a sparse postnatal envi-ronment.
To summarize, our model invokes establishedconcepts from
comparative biology to extend
the thrifty hypotheses by proposing that thedeveloping organism
senses its environmentthroughout development and adjusts its
physi-ology to be appropriate for the environment inwhich it
predicts that it will live until andthrough reproductive age. These
mechanismsconstitute predictive adaptive responses thatare
influenced by the normal range of environ-ments experienced by the
organisms mother.The fetus may also make some immediately ad-aptive
responses if they assist in surviving untilbirth, and these
responses may be reflected inbirth size. In this way, developmental
plasticity
tunes physiological homeostatic settings in waysthat are much
faster and potentially more sen-
sitive to changing conditions than those achievedby classical
genetic mechanisms alone. For anypostnatal environment there will
be a set ofphysiological settings associated with optimalfitness
for that environment, and in the case ofhumans a risk of disease
will exist when welive beyond the range of the expected
environ-ment.
THE FETAL ENVIRONMENT AND MATERNAL
CONSTRAINT
The consequences of alterations in the de-velopmental
environment will depend on howthe fetus perceives that environment
and theaccuracy of the forecasts it makes. The mam-malian embryo
and fetus has the particularchallenge of interpreting the
maternalpla-cental transduction of environmental informa-tion, a
process that may not operate with com-plete fidelity.
Fetal nutrition is not the same as maternaldietary intake. The
provision of fetal nutrients
depends on the maternal nutritional environ-ment, her energy
expenditure, her behavior
Fig. 2. The matchmismatch paradigm of metabolic disease. The
developing organism senses maternally trans-mitted environmental
cues, such as undernutrition, during prenatal and early postnatal
life. Developmental plas-ticity in response to these cues modifies
the default trajectory defined by the inherited fetal genome and
epigenomeaccording to whether the environment is perceived as
adequate (dark background) or deprived (light background),resulting
in adjustment of metabolic setpoints. If the eventual mature
environment, whether adequate or deprived,matches the prediction
then the risk of metabolic disease in later life is low. If there
is a mismatch between the pre-dicted and actual mature
environments, particularly if the mature environment is richer than
anticipated, thenthe risk of metabolic disease is enhanced.
8 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
9/19
and health, her metabolic and cardiovascularfunction, placental
health and function, andfetal endocrine status. A further feature
ofmammalian development is that fetal growth
is constrained by a number of factors. Theterm maternal
constraint was introduced byOunsted (1965) to describe nongenetic
mater-nally determined environmental and physio-logical influences
that limit fetal growth. Theconcept derived from the classical work
of Wal-ton and Hammond (1938) which showed thatthe size of the
fetus was significantly affectedby the size of the mother, as
opposed to the fetalgenotype. Later work has confirmed this to
bethe case in several monotocous mammalianspecies. Indeed, in human
pregnancies origi-nating from egg donation and surrogate moth-
erhood, birth size is more tightly correlatedwith recipient
stature than with donor stature(Brooks et al., 1995).
The mechanisms underlying maternal con-straint are poorly
understood. In some way, ma-ternal size determines nutrient
availability tothe fetus. Whether the constraint mechanismlies in
the uterine vasculature or in placentalstructure and function is
not yet clear, but ingeneral shorter mothers who have smaller
pel-vises have smaller babies. An alternative expla-nation might
lie in parentoffspring conflict, aconcept originated by Trivers
(1974) and ex-tended by Haig to include the observations thatthe
genes for IGF-2 and the IGF-2 clearancereceptor are imprinted in
the mouseIGF-2being expressed in the fetus from the paternalallele
and the receptor being expressed fromthe maternal allele in the
placenta (Haig andGraham, 1991). The conflict argument suggeststhat
the fetus drives fetal growth under pater-nal influences, while the
mother attempts tolimit fetal growth by clearing IGF-2 from the
fe-tal circulation via the placenta. However, inhumans the IGF-2
receptor is not imprinted,
and in species that have a long gestation with along fetal as
opposed to embryonic phase IGF-1and insulin are the primary
determinants offetal growth in late gestation and thus of birthsize
(Gluckman and Pinal, 2003). However, thereare some limited data
suggesting that the pla-centa might also clear IGF-1 (Gluckman
andPinal, 2003). Whatever the mechanism, non-genetic factors
including maternal constrainthave been estimated to contribute over
50% ofthe variance in birth size in humans (Morton,1955; Ounsted
and Ounsted, 1973).
Maternal constraint is of particular impor-
tance in human evolution. Maternal heightand pelvic proportions
are tightly correlated.
As a result of the adoption of an upright pos-ture, pelvic
proportions were altered. Further,the large brain of our species
meant that wehad to adopt a secondarily altricial life course
to ensure the head could exit the pelvic canal.Even so, whereas
the chimpanzee head can re-adily exit the pelvis, the human head
can only
just exit the maternal pelvic canal and onlythen by some complex
rotations (Trevathan,1988). Thus, maternal constraint has been
thekey to limit fetal growth and allow our speciesto reproduce
successfully.
The concept of maternal constraint has beenextended to include
other nongenomic and in-trinsic physiological mechanisms that
impacton birth size and developmental trajectory, al-though whether
all rely on the same underly-
ing mechanisms is not clear (Gluckman andHanson, 2004a). Such
effects are seen in primi-parous women, who generally have
smallerbabies, in women of young maternal age, andin multiple
pregnancies. There is no a priorireason why the mechanisms by which
thesedifferent situations constrain fetal growth needbe identical.
Indeed, the reduced growth oftwins is obviously a reflection of
limits on thenutrient supply that can cross from mother tofetus.
The constraint on fetal size in the firstpregnancy is likely to be
due to poorer perfu-sion of the uterine bed but can also be
inter-preted in life history terms as a mechanism bywhich a mother
limits her investment in herfirst offspring, which generally would
havehappened at a young age, in expectation of sub-sequent
pregnancies. Recent studies indeedshow that the effect of parity on
maternal con-straint is an important influence on relation-ships
between birth size and later outcomes:truncal obesity is greater in
first-born children(Stettler et al., 2000) and the inverse
relation-ship between blood pressure and birth size isstronger in
first-borns (Hardy et al., 2004).
The reduced size of infants born to adolescentmothers appears to
be due to continued diver-sion of nutrients to support maternal
develop-ment (Wallace et al., 2004) and again can beargued in life
history terms as a strategy to en-hance maternal survival, both by
protecting hernutritional status and because her pelvis doesnot
reach maximal dimensions until some yearsafter menarche. As women
now delay their firstpregnancy, at least in western societies, we
areseeing a greater number of pregnancies at ad-vanced maternal
agethese babies are also ofreduced birthweight (Gilbert et al.,
1999).
Parenthetically, variation in birthweightmight also be affected
by subtle changes in
9DEVELOPMENTAL CHOICE OF LIFE HISTORY STRATEGY
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
10/19
gestational length. There is experimental, andincreasing
clinical, evidence that mothers un-dernourished or stressed early
in pregnancymay give birth after shorter gestational
lengths (reviewed in Gluckman et al., 2005a).This is an
alternative strategy that the fetusmay use to respond to a
threatening situation,and in experimental studies it is
associatedwith accelerated activation of the
hypothala-micpituitaryadrenal (HPA) axis (Bloomfieldet al.,
2003).
The net effect of maternal constraint is gen-erally to limit
nutrient availability to the fetus.Thus one does not anticipate a
linear relation-ship between birth size and maternal nutri-tional
status. As fetal conditions improve, fetalgrowth increases
asymptotically (at least in terms
of lean body mass). There are exceptionsforexample, the fetal
overgrowth syndromes suchas the BeckwithWeidemann syndrome
whereboth alleles of IGF-2 are expressed by the fetusinstead of one
being silenced by parental im-printing. In infants of diabetic
mothers, the fe-tus is heavier due to increased fat mass second-ary
to the adipogenic effects of increased fetalinsulin that is
released in response to the in-creased transplacental glucose
transfer (Schwartzand Teramo, 2000). There is a much smallereffect
on lean body mass. Such infants arelarge, but have an abnormal body
compositionwith increased adiposity and suffer pathologi-cal
consequences. Historically, their poor sur-vival might have
excluded them from the nor-mal pattern of human development. Thus,
withthe exception of gestational diabetes, fetalgrowth in virtually
all human pregnancies islimited by maternal constraint, even
whenbirth weight is within the normal range. Thislimits the
environmental range that the fetuscan detect and therefore predict.
This in turnhas the effect of limiting the range of nutri-tional
environments to which the physiology
of the organism can respond in postnatal life(Gluckman and
Hanson, 2004b; Gluckmanand Hanson, 2004c).
Analyses of fitness in wild populations(Charmantier and Garant,
2005) confirm thatenvironmental factors play a greater role
inphenotypic variation in populations under poorconditions than
under good conditions. Such anobservation is compatible with the
relation-ships we have described. The asymptotic rela-tionship seen
under conditions when the fetusis exposed to a good environment
will meanthat trait variation in such fetuses is primarily
a reflection of genetic variation. Conversely,when the fetus is
making predictions based on
a poor environment, the individual lies on asteeper part of the
predicted/actual relation-ship curve (Fig. 3) and one would
anticipategreater variation in the trait as an adult. The
variation is enhanced further because of thevarious ways in
which maternal nutritional in-formation may be misinterpreted by
the fetus,for example after maternal or placental dis-ease, thus
giving rise to a greater risk of inac-curacy in the prediction.
DEVELOPMENTAL MISMATCH ANDPATTERNS OF DISEASE
In a population living in a stable environ-ment, evolution will
have matched physiologyto that environment. But the
developmentalenvironment may vary and thus shift the posi-tioning
of the range of environments an indi-vidual can live in as an adult
(discussed inDeWitt and Scheiner, 2004). One way in whichthis can
occur is through predictive adaptation.If the prediction is correct
then there will be agood match between the phenotype adoptedand the
environment in which the organismwill later live, and resulting
fitness will behigh. If the prediction is poor, there will be
amismatch between the environment experi-
enced and the phenotype induced. We havesuggested that concepts
of developmental mis-match can provide a useful perspective on
theDOHaD phenomenon (Gluckman et al., 2005a).
Impaired fetal growth is an indirect reflectionof an impaired
fetal environment arising fromexcessive maternal constraint, the
presence ofa severe maternal environment, or maternal orplacental
disease. The fetus sees all these sit-uations as reflecting
impaired nutrition, pre-dicts a deprived postnatal environment and
ad-
justs its metabolic phenotype accordingly.But most of these
situations lead to faulty
predictions, because the postnatal environ-ment is adequate.
Thus, the individual willhave some mismatch between its
maturephysiology and the environment it inhabits.The greater the
mismatch, the greater is therisk of adult disease.
Such a paradigm can explain why popula-tions undergoing rapid
nutritional transitionsuch as in India and China are witnessing
amassive increase in the prevalence of metabolicand cardiovascular
disease. Although the intra-uterine environment can only change
slowlyacross generations (Gluckman and Hanson,
2005), the postnatal environment can changevery rapidly. Thus, a
stunted mother will se-
10 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
11/19
verely constrain the growth of her fetus andinduce a metabolic
phenotype appropriate for a
nutritionally deprived environment, but thepostnatal environment
will not match thosesettings. Indeed, Figure 3 would suggest
thatdevelopment in a severely constrained settingreduces the upper
limit of the range of post-natal environments that can be tolerated
with-out risk of disease. Such a paradigm explainsthe increase in
lifestyle disease that occurswhen a population migrates rapidly
from theless developed to the developed world, for ex-ample from
Ethiopia to Israel (Cohen et al.,1988). One implication of such a
model is that,even if there is optimal fetal growth, maternal
constraint always limits the postnatal environ-ment that the
fetus can predict and prepare for.
Thus, the issue is the relative change (mismatch)from
developmental to adult environment, not
whether the fetal environment is deprived oradequate, and the
model is therefore relevantto the current obesity epidemic in the
devel-oped world.
PRENATAL AND POSTNATAL EFFECTS
Most of the discussion above has focused onthe nutritional and
energetic environment.This is inevitable, given that in life
historyterms energetics are a very important compo-nent of the
environment and nutritional manip-ulation has been the major
experimental sys-
tem studied. However, the same model canapply to other
dimensions of the environment,
Fig. 3. Consequences of a mature environment outside the
predicted range. The zone of maximal fitness result-ing from the
different developmental trajectories determined by environmental
cues in early life is shaded. Note
the nonlinearity of the relationship, arising from maternal
constraint acting to limit the size of the fetus at deliveryand
setting the upper limit of the postnatal environment which the
species can tolerate without the risk of meta-bolic disease even
when maternal constraint is minimal (horizontal heavy broken line).
Fetuses A and B are shownat the upper limits of their range of
fitness. Fetus A has set its developmental trajectory in
expectation of a rela-tively deprived environment. If the mature
environment is richer than predicted, the risk of metabolic disease
isincreased. In contrast, fetus B has developed in expectation of
an adequate environment, the extent of unpredictedexcess is
smaller, and a higher level of postnatal nutrition is needed for
the risk of metabolic disease to beincreased. As increasing
affluence raises the richness of the mature environment and because
of the limiting effectof maternal constraint, a greater proportion
of even optimally nourished fetuses in utero are mismatched to
theirpostnatal environment (modified from Gluckman and Hanson,
2005).
11DEVELOPMENTAL CHOICE OF LIFE HISTORY STRATEGY
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
12/19
in particular stress which in comparative termsmay reflect both
intraspecific competition andpredator risk. There is ample data
suggestingthat glucocorticoid exposure in utero as a result
of elevated maternal glucocorticoid levels caninduce long-term
changes in the glucocorticoidaxis (ORegan et al., 2001) that may
have short-term adaptive valuefor example, by tuningstress
responses during the population cycle ofthe snowshoe hare (Boonstra
et al., 1998).There is also increasing evidence that nutri-tional
and hormonal cues intersect. In experi-mental animals, the
phenotypes arising frommaternal glucocorticoid exposure and from
ma-ternal nutritional manipulation are very simi-lar (Bertram and
Hanson, 2001). The enzyme11b-hydroxysteroid dehydrogenase type 2
in
the placenta normally inactivates maternalglucocorticoids to
limit fetal exposure. Under-nutrition reduces 11b-hydroxysteroid
dehy-drogenase type 2 activity in the rat (Bertramet al., 2001) and
low birthweight is associatedwith reduced enzymatic activity in the
humanplacenta (reviewed in Seckl and Meaney, 2004),suggesting a
possible common mechanism. Theglucocorticoid receptor in the brain
and liverappears to be a target of epigenetic regulationby maternal
factors (Lillycrop et al., 2005;Weaver et al., 2004). The same
paradigm canalso explain the induction of long-term changein other
physiological systems, such as thoseregulating temperature
(Diamond, 1991), thirst(El-Haddad et al., 2004) and
reproduction(Cooper et al., 1996; Gluckman and Hanson,2006b).
The initial cues may act at differing points inthe window of
plasticity. For each organ, therewill be a time in development
after which plas-ticity is clearly no longer possible. Equally,some
cues may act very early in developmentthere is, for example,
experimental evidencethat changing the maternal environment in
the
pre-implantation period can have long-termeffects on metabolic
and cardiovascular func-tion (Kwong et al., 2000). Similarly, in
experi-mental in vitro fertilization, changing the cul-ture
conditions can induce long-term develop-mental changes (Walker et
al., 1996; Younget al., 2001). Some may be disruptive in naturebut
others may be a reflection of evolved adapt-ive processes. In the
agouti mouse, changingnutrient balance in the periconceptional
periodalters for life the methylation status of the mu-tant gene
underlying the agouti phenotype(Cooney et al., 2002; Wolff et al.,
1998), again
suggesting that the periconceptional period is astage in which
epigenetic change can be in-
duced. The limited human data suggests thatnutritional status at
conception also has im-portant influences on both gestational
length(Susser and Stein, 1994) and birth size (Neggers
and Goldenberg, 2003; Villar and Rivera, 1998).Conversely, there
is both experimental (re-
viewed above) and clinical evidence to suggestthat the postnatal
period is also one in whichlonger-term effects can be induced or
the effectsof earlier cues can be modulated. In humans,there is
much data suggesting that the natureof infant feeding has long-term
metabolic, car-diovascular and cognitive effects (Lucas et
al.,1998; Singhal et al., 2003; Singhal et al., 2004;Stettler et
al., 2005). Parenthetically, the termprogramming was first adopted
to describesuch linkages and the same term has been used
extensively in discussions of the fetal originsparadigm. We have
avoided using it, as we andothers see conceptual limitations in its
use. Itimplies a hardwired process, whereas theeffects observed are
clearly much more flexible.In general, bottle-feeding appears to
have rela-tively deleterious effects. Such studies have ledsome to
conclude that enhanced infant growthitself induces long-term
consequences (Singhaland Lucas, 2004). This may indeed be so, but
itis difficult to separate out this effect from theearlier and
inevitable constraint in utero whichthen sets the scene for such
accelerated infantgrowth to occur. Other studies have
suggestedthat, rather that rapid infant growth being themost
significant factor, it is prolonged impairedinfant growth followed
by rapid growth inchildhood (Bhargava et al., 2004; Erikssonet al.,
2003). Although these different conclu-sions have led to some
considerable debate as tothe importance of different patterns of
growth,one consistent theme emergesthat constrainedfetal or infant
growth followed by nutrition-enhanced infant or later childhood
growth hasmetabolic consequences. Both patterns are
compatible with the predictive model and thedeleterious effect
of nutritional mismatch sug-gested earlier. The issue of whether
these twophases of perinatal development are independ-ent or
interdependent is more complex and re-quires further research.
DOHaD, EVOLUTION, AND LIFE HISTORYSTRATEGY
There has been much recent progress in thefield of ecological
developmental biology as wellas a greater integration of
developmental biol-
ogy into the evolutionary synthesis (Gilbert,2001;
West-Eberhard, 2003). Much of this
12 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
13/19
paper has suggested that the phenomena re-flected in the
experimental and clinical obser-vations associated with the DOHaD
paradigmare generalizable and related to basic processes
of development.We would suggest that the processes of devel-
opmental plasticity, in particular those havinglonger-term
potential adaptive significance,have been central to the survival
of mamma-lian species through variable environments.They would have
been particularly importantin a generalist species such as the
human. De-velopmental plasticity acts to increase thepotential for
phenotypic variation, allowing ashift in the positioning of the
individuals phys-iology within the reaction norm to optimize
itsphenotype for a particular environment and
increase its fitness (survival and reproductivesuccess). In this
way, a greater proportion ofindividuals will survive a transient
environ-mental shift and greater genotypic variationcan be
maintained (Gluckman and Hanson,2005). The concept that an
environmental stim-ulus can shift the organism into a
differentdevelopmental pathway (in the case of theDOHaD paradigm, a
pathway anticipating asparse or threatening postnatal
environment)was classically visualized by Waddington (1942,1957) as
canalization towards alternativeend-states, with constraint on
variation of aparticular end-state pictured as the steepnessof the
local gradients of the epigenetic land-scape. More recent usage of
the term canaliza-tion, also termed auto-regulation by
Schmal-hausen (1949), has focused on the impliedaspect of
constraint of phenotypic variationagainst the effects of genetic or
environmen-tal perturbations (Debat and David, 2001).
Although developmental plasticity and envi-ronmental
canalization act in opposite direc-tions on phenotypic variation,
they both act topreserve genetic variationthe former by pro-
moting variation of the phenotype in a chang-ing environment,
the latter by constrainingvariation of an evolved optimal phenotype
in astable environment. The classic experiments ofBelyaev and his
coworkers, who demonstratedthat phenotypic variation could be
exposedwhen an apparently homogeneous populationof foxes was
selected for one behavioral charac-teristic, tameness, are
particularly relevantto our model of integrated responses in
thatsuch selection appeared to act on componentsof the HPA axis but
resulted in the appearanceof variation in a wide range of
morphological,
physiological, and behavioral traits (Trut,1999).
Human development does not involve thegeneration of the distinct
morphs describedabove for the desert locust, but it can
nonethe-less be envisaged in an analogous way. The
human embryo, fetus and neonate senses itsfuture nutritional
status via signals from itsmother and makes an integrated response
tothose signals. This response is manifest as arange of phenotypes
later in life, with conse-quences dependent on the energy density
of theenvironment in which the individual lives asan adult.
We propose that such plasticity is a result ofwell-integrated
responses regulated by a lim-ited number of key genes whose
expression isaffected by the developmental cue and whichthen
regulate subsequent patterns of gene
expression and tissue organization. Whethersuch regulation is
positive (conceptually, acti-vation of plasticity) or negative
(conceptually,deactivation of canalization) remains to
bedetermined. The existence of genes for plastic-ity is a subject
of debate (DeWitt and Scheiner,2004), whereas candidate
canalization genesacting at the whole-organism level have
beenidentified, for example HSP90 in Drosophila(Queitsch et al.,
2002). However they are re-gulated, these integrated responses
determinethe subsequent phenotype and life course.
Life-history theory is based on considerationof the allocation
of resources to somatic effort(growth and survival) and
reproductive effort,with the assumption that selection operates
tomaximize reproductive fitness by determiningthe optimal
allocation between somatic andreproductive investment. A corollary
is that in-vestment in post-reproductive longevity doesnot affect
reproductive fitness and is not fa-vored by selection. Our model
suggests that ifthe fetus predicts an uncertain future, whichmay be
reflected in being born smaller or pre-maturely, it will invest
less in somatic effort,
possibly by lower investment in maintenanceand repair (Kirkwood,
2002), and hence thoseborn smaller tend to die earlier (Kajantie et
al.,2005). Associated with this there may be lessinvestment in
systems in which there is someredundancy, for example fewer
nephrons (Hin-chliffe et al., 1992; Langley-Evans et al., 2003)and
fewer neurons in some regions of the brain(Mallard et al., 2000;
Tolsa et al., 2004)obser-vations confirmed both experimentally and
clin-ically. Because the fetus predicts a shorter life itwill
invest less in musculoskeletal growth, pre-disposing to sarcopenia
and osteopenia, both
features of the human born smaller (Sayer andCooper, 2005).
There is advantage when living
13DEVELOPMENTAL CHOICE OF LIFE HISTORY STRATEGY
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
14/19
in a poor nutritional environment to layingdown fat when
possible and to having periph-eral insulin resistance, both
features well dem-onstrated in humans. In experimental animals,
this potential advantage can be seen in hyper-phagia (Vickers et
al., 2000), altered appetiteregulation (Plagemann et al., 2000) and
apreference for a high-fat diet (Bellinger et al.,2004). Given the
relationship between thenutritional and HPA axes, it would not
besurprising that the HPA axis is altered undersuch conditions, as
is reported in both humans(Phillips et al., 1998) and animals
(Seckl andMeaney, 2004), and this change may also con-tribute to
the obese phenotype.
Resource allocation to reproductive effort, re-flected in age of
maturity and fecundity, will
also be affected by developmental cues. Inhumans, good nutrition
in childhood leads toearlier puberty (Karlberg, 2002).
Conversely,low birthweight leads to accelerated sexualmaturation if
postnatal energetics allow (Cooperet al., 1996; Gluckman and
Hanson, 2006b;Ibanez et al., 2000; Karlberg, 2002),
althoughfecundity is lower in both females (Ibanezet al., 2003) and
males (Cicognani et al.,2002; Francois et al., 1997) of low
birth-weight; both these observations are in accord-ance with
predictions of life history theory(Stearns and Koella, 1986). Lower
testoster-one levels in males may also represent a trade-off
between reproductive and immune func-tions (Muehlenbein and
Bribiescas, 2005). Fur-thermore, early maturation may itself
involvea trade-off between offspring quantity andquality in the
subsequent generation (Coalland Chisholm, 2003; Wallace et al.,
2004), per-petuating a cycle of low birthweight.
Two extreme examples are illustrated inFigure 4a fetus exposed
to an optimal nutri-tional environment in utero and a fetus
ex-posed to a less than optimal environment. Al-
though the definitive life courses will inevitablybe modified by
subsequent environmental expo-sure, consideration of the
developmental compo-nent alone in the context of the
immediatelyadaptive and predictive responses made in thealternative
environments allows us to under-stand the biology of those born
smaller.
While we have focused on the extremes tomake this point, we
propose that there is a con-tinuous range of human metabolic
morphsrepresenting a suite of integrated responses tothe
environmental cues received in utero or bythe neonate which
establish the setpoints of
the metabolic and related systems. We suggestthat these
different developmental trajectories
are set by altered expression, presumably regu-lated by
epigenetic processes, of key regulatorygenes. Although the specific
nature of theseprocesses remains to be determined, compo-
nents of the HPA axis seem to be key candi-dates. Depending on
the postnatal environment,such responses may manifest in an altered
riskof disease.
Such an integrated suite of somatic and re-productive responses
to early cues forecastinga sparse or threatening postnatal
environmentwill have evolved to promote individual sur-vival to
reproductive age and avoid extinctionof the lineage, and at a
population level willpreserve genetic variation. But in an
enrichedpostnatal environment this mismatched devel-opmental
trajectory results in metabolic dis-
easemechanisms to ameliorate such diseasewould not have evolved
since the adverse con-sequences occur predominantly in the
post-reproductive period. In this way the predictionsof the
match-mismatch model are not dissimi-lar from those of antagonistic
pleiotropy (Wil-liams, 1957), which model suggests that
allelesconferring fitness advantage early in life willbe selected
for even if they are deleterious laterin life. The fundamental
difference between thetwo models is that an adaptive
mechanisminvolving phenotypic plasticity will allow re-versibility
at the individual (Vickers et al.,2005) level should environmental
conditionsimprove (or be perceived to have improved).
It has been argued that although induction ofthriftiness in the
offspring has adaptiveadvantage, such advantage is predominantly
forthe mother, reducing the demand of the currentpregnancy and
lactation cycle and enhancingher future reproductive fitness
(Wells, 2003).There are several reasons why we believe this tobe a
flawed argument. First, predictive res-ponses cause an integrated
change in the off-springs phenotype and subsequent life history
across several dimensions rather than a reduc-tion in birth size
alone, an observation not read-ily explained by the maternal
fitness hypothesis.Second, such reduction in birth size is not
anobligatory partof the suite of alterations inducedby an adverse
prenatal environment. Third, weagain point to data showing that one
of the hall-marks of thriftinessinsulin resistancedoesnot appear
until well after birth in small-for-gestational-age individuals
(Ibanez et al., 2006;Mericq et al., 2005), implying little
immediateadvantage for the mother.
Humans evolved in environments very dif-
ferent from those in which we now live. Analy-sis of
paleoclimatic data (Potts, 1998) offers
14 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
15/19
support for the view that hominin evolutionoccurred in response
to change over long (sev-eral generations) rather than short
(seasonalor single-generation) time frames. In such asituation,
forecasting (Bateson et al., 2004)of the environment would have
been valuable,and the accuracy of the cue reaching the fetusmay
have been enhanced by phenotypic iner-tia integrating the signal
across multiple gen-erations to reduce the effects of short-term
fluc-tuations (Kuzawa, 2005). It is probable that
enriched environments were experienced onlyrarely and that
selection favored the operationof maternal constraint and the
continued oper-ation of ancestral mechanisms of adaptive
de-velopmental plasticity because they matchedthe individual to the
postnatal environmentmost of the time. Together with the
relativelyshort life expectancy of Paleolithic and Neo-lithic
humans (Austad, 1994), this meant thatthese processes were usually
adaptive. How-ever, in the enriched and rapidly changingnutritional
environments of post-industrial so-ciety the risk of postnatal
mismatch between
the developmentally induced phenotype andthe actual conditions
experienced has increased
dramatically. Lifestyle diseases reflect that welive in a manner
and in an environment beyondthe range we evolved to live within, a
rangethat remains limited by maternal constraint.What clinicians
observe as the DOHaD phe-nomenon is actually part of a fundamental
pro-cess by which the organism adjusts its lifecourse strategy in
response to environmentalinfluences acting early in
development.
CONCLUSIONS
Attempts to explain the original observationsof a relationship
between birth size and laterrisk of heart disease and of the
long-term im-pact of various infant feeding regimens havemoved from
consideration of specific situationsto a much broader emphasis on
how life historyand evolutionary biology intersect with studiesof
human disease. Major research questions re-main to be resolved: the
genotypic determinantsof environmental sensitivity during
develop-ment, the identification of the key regulatorygenes, the
fundamental epigenetic processes
involved in phenotypic plasticity, the basis ofthe adjustment
and integration of the various
Fig. 4. Integrated life history responses to developmental cues.
Two extreme examples of developmental trajec-tories are shown, one
in response to a perceived adequate nutritional environment and the
other in response to aperceived deprived environment.
15DEVELOPMENTAL CHOICE OF LIFE HISTORY STRATEGY
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
16/19
components of the life course strategy, and thecomplexities
surrounding the role of the infantperiod in modifying earlier
phenotypic choices.It is clear that life history biology offers
much
to inform our understanding of human chronicnoncommunicable
disease. It shifts the diseaseparadigm from one of external
causation to oneof the match or mismatch between the
evolutio-narily and developmentally defined constitu-tion of the
organism and the environment inwhich it finds itself. This bridges
the gapbetween the traditional medical and anthropo-logical models.
The developmental componentoffers approaches to prevention and the
expand-ing knowledge of epigenetics offers approachesto
intervention.
At a pragmatic level, this perspective means
that different strategies may be more appropri-ate for disease
reduction in different popula-tions (Gluckman et al., 2005b). Thus,
in devel-oped countries the focus must remain on post-natal
interventions to limit energy intake andincrease energy
expenditure. In populations indeveloping countries a greater focus
on the wellbeing of the mother may be important to allowsubsequent
generations to maintain metabolichealth during a socioeconomic
transition to anenvironment of higher energy density. Impor-tant
approaches in this setting include delayingfirst pregnancy until
the mother is fully grown,say at least 45 yr after menarche,
ensuringadequate nutritional status at conception, andfocusing on
maternal health and nutrition dur-ing pregnancy.
ACKNOWLEDGMENTS
We thank Patrick Bateson, Hamish Spencer,David Raubenheimer, and
Chris Kuzawa forthoughtful discussions.
LITERATURE CITED
Applebaum SW, Heifetz Y. 1999. Density-dependent physio-logical
phase in insects. Annu Rev Entomol 44:317341.
Austad SN. 1994. Menopause: An evolutionary perspective.Exp
Gerontol 29:255263.
Barker DJ, Osmond C. 1986. Infant mortality, childhoodnutrition,
and ischaemic heart disease in England andWales. Lancet
1:10771081.
Barker DJP. 1998. In utero programming of chronic disease.Clin
Sci 95:115128.
Bateson P, Barker D, Clutton-Brock T, Deb D, DUdine B,Foley RA,
Gluckman P, Godfrey K, Kirkwood T, MirazonLahr M, McNamara J,
Metcalfe NB, Monaghan P,Spencer HG, Sultan SE. 2004. Developmental
plasticityand human health. Nature 430:419421.
Bellinger L, Lilley C, Langley-Evans SC. 2004. Prenatal
ex-posure to a maternal low-protein diet programmes a pref-
erence for high-fat foods in the young adult rat. Br J
Nutr92:513520.
Benyshek DC, Johnston CS, Martin JF. 2006. Glucose me-tabolism
is altered in the adequately-nourished grand-offspring (F3
generation) of rats malnourished duringgestation and perinatal
life. Diabetologia 49:11171119.
Benyshek DC, Watson JT. 2006. Exploring the thrifty geno-types
food-shortage assumptions: A cross-cultural com-parison of
ethnographic accounts of food security amongforaging and
agricultural societies. Am J Phys Anthropol131:120126.
Bertram C, Trowern AR, Copin N, Jackson AA, WhorwoodCB. 2001.
The maternal diet during pregnancy programsaltered expression of
the glucocorticoid receptor and type2 11b-hydroxysteroid
dehydrogenase: Potential molecu-lar mechanisms underlying the
programming of hyper-tension in utero. Endocrinology
142:28412853.
Bertram CE, Hanson MA. 2001. Animal models and pro-gramming of
the metabolic syndrome. Br Med Bull 60:103121.
Bhargava SK, Sachdev HS, Fall CHD, Osmond C, Lakshmy R,Barker
DJP, Biswas SK, Ramji S, Prabhakaran D,
Reddy KS. 2004. Relation of serial changes in childhoodbody-mass
index to impaired glucose tolerance in youngadulthood. N Engl J Med
350:865875.
Bloomfield FH, Oliver MH, Giannoulias D, Gluckman PD,Harding JE,
Challis JRG. 2003. Brief undernutrition inlate-gestation sheep
programmes the hypothalamic-pitu-itary adrenal axis in adult
offspring. Endocrinology 144:29332940.
Boonstra R, Hik D, Singleton GR, Tinnikov A. 1998. Theimpact of
predator-induced stress on the snowshoe harecycle. Ecol Monogr
68:371394.
Bouret SG, Draper SJ, Simerly RB. 2004. Trophic action ofleptin
on hypothalamic neurons that regulate feeding.Science
304:108110.
Brooks AA, Johnson MR, Steer PJ, Pawson ME, Abdalla HI.1995.
Birth weight: Nature or nuture? Early Hum Dev 42:
2935.Charmantier A, Garant D. 2005. Environmental quality
andevolutionary potential: Lessons from wild populations.Proc R Soc
B 272:14151425.
Chong S, Whitelaw E. 2004. Epigenetic germline inheri-tance.
Curr Opin Genet Dev 14:692696.
Cicognani A, Alessandroni R, Pasini A, Pirazzoli P, Cassio
A,Barbieri E, Cacciari E. 2002. Low birth weight for gesta-tional
age and subsequent male gonadal function. J Pediatr141:376379.
Coall DA, Chisholm JS. 2003. Evolutionary perspectives
onpregnancy: Maternal age at menarche and infant birthweight. Soc
Sci Med 57:17711781.
Cohen MP, Stern E, Rusecki MJ, Zeidler A. 1988. Highprevalence
of diabetes in young adult Ethiopian immi-grants to Israel.
Diabetes 37:824828.
Cooney CA, Dave AA, Wolff GL. 2002. Maternal methylsupplements
in mice affect epigenetic variation and DNAmethylation of
offspring. J Nutr 132:2393S2400S.
Cooper C, Kuh D, Egger P, Wadsworth M, Barker D. 1996.Childhood
growth and age at menarche. Br J ObstetGynaecol 103:814817.
Cutfield W. 2005. IVF children are taller with increasedIGF-I,
IGF-II and IGFBP-3 levels suggesting altered geneticimprinting. In
Proceedings of the 3rd International Con-gress on Developmental
Origins of Health and Disease,Toronto, Canada, November 1619,
2005.
Debat V, David P. 2001. Mapping phenotypes:
Canalization,plasticity and developmental stability. Trends Ecol
Evol16:555561.
DeWitt TJ, Scheiner SM. 2004. Phenotypic plasticity: Func-tional
and Conceptual Approaches. Oxford: Oxford Uni-versity Press.
Diamond J. 1991. Pearl Harbor and the emperors physiolo-gists.
Nat Hist 100:27.
16 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
17/19
Dos Santos SI, de Stavola BL, Hardy RJ, Kuh DJ,McCormack VA,
Wadsworth ME. 2004. Is the associationof birth weight with
premenopausal breast cancer riskmediated through childhood growth?
Br J Cancer 91:519524.
Drake AJ, Walker BR. 2004. The intergenerational effectsof fetal
programming: Non-genomic mechanisms for theinheritance of low birth
weight and cardiovascular risk.J Endocrinol 180:116.
Drake AJ, Walker BR, Seckl JR. 2005.
Intergenerationalconsequences of fetal programming by in utero
exposureto glucocorticoids in rats. Am J Physiol 288:R34R38.
El-Haddad MA, Desai M, Gayle D, Ross MG. 2004. In
uterodevelopment of fetal thirst and appetite: Potential
forprogramming. J Soc Gynecol Investig 1:123130.
Eriksson JG, Forsen T, Tuomilehto J, Osmond C, Barker DJ.Early
adiposity rebound in childhood and risk of Type 2 di-abetes in
adult life. Diabetologia 2003; 46:190194.
Eriksson JG, Lindi V, Uusitupa M, Forsen TJ, Laakso M,Osmond C,
Barker DJ. 2002. The effects of thePro12Ala polymorphism of the
peroxisome proliferator-
activated receptor-g2 gene on insulin sensitivity andinsulin
metabolism interact with size at birth. Diabetes51:23212324.
Eshel I, Matessi C. 1998. Canalization, genetic assimilationand
preadaptation: A quantitative genetic model. Genet-ics
149:21192133.
Forsdahl A. 1977. Are poor living conditions in childhoodand
adolescence an important risk factor for arterioscle-rotic heart
disease? Br J Prev Soc Med 31:9195.
Francois I, de Zegher F, Spiessens C, DHooghe TM,
Van-derschueren D. 1997. Low birth weight and subsequentmale
subfertility. Pediatr Res 42:899901.
Gate JJ, Clarke L, Lomax MA, Symonds ME. 1999. Chroniccold
exposure has no effect on brown adipose tissue innewborn lambs born
to well-fed ewes. Reprod Fertil Dev11:415418.
Gilbert SF. 2001. Ecological developmental biology:
Devel-opmental biology meets the real world. Dev Biol 233:112.
Gilbert WM, Nesbitt TS, Danielsen B. 1999. Childbearingbeyond
age 40: Pregnancy outcome in 24,032 cases. ObstetGynecol
93:914.
Gluckman PD. 1995. The endocrine regulation of fetalgrowth in
late gestation: The role of insulin-like growthfactors. J Clin
Endocrinol Metab 80:10471050.
Gluckman PD, Beedle AS, Hanson MA, Vickers MH. Leptinreversal of
the metabolic phenotypeevidence for the roleof developmental
plasticity in the development of the met-abolic syndrome. Horm Res
(in press).
Gluckman PD, Cutfield W, Hofman P, Hanson MA. 2005a.The fetal,
neonatal and infant environmentsThe long-term consequences for
disease risk. Early Hum Dev 81:.
5159.Gluckman PD, Hanson MA. 2004a. Maternal constraint offetal
growth and its consequences. Semin Fetal NeonatalMed 9:419425.
Gluckman PD, Hanson MA. 2004b. The developmental ori-gins of the
metabolic syndrome. Trends Endocrinol Metab15:183187.
Gluckman PD, Hanson MA. 2004c. Living with the past:Evolution,
development, and patterns of disease. Science305:17331736.
Gluckman PD, Hanson MA. 2005. The Fetal Matrix: Evolu-tion,
Development, and Disease. Cambridge: CambridgeUniversity Press.
Gluckman PD, Hanson MA, editors. 2006a. DevelopmentalOrigins of
Health and Disease. Cambridge: CambridgeUniversity Press.
Gluckman PD, Hanson MA. 2006b. Evolution, developmentand timing
of puberty. Trends Endocrinol Metab 17:712.
Gluckman PD, Hanson MA, Morton SMB, Pinal CS. 2005b.Life-long
echoesA critical analysis of the developmentalorigins of adult
disease model. Biol Neonate 87:127139.
Gluckman PD, Hanson MA, Spencer HG. 2005c. Predictiveadaptive
responses and human evolution. Trends Ecol
Evol 20:527533.Gluckman PD, Hanson MA, Spencer HG, Bateson P.
2005d.
Environmental influences during development and theirlater
consequences for health and disease: Implicationsfor the
interpretation of empirical studies. Proc R Soc B272:671677.
Gluckman PD, Harding JE. 1997. Fetal growth
retarda-tionUnderlying endocrine mechanisms and
postnatalconsequences. Acta Paediatr Scand 86:6972.
Gluckman PD, Pinal CS. 2003. Regulation of fetal growthby the
somatotrophic axis. J Nutr 133:1741S1746S.
Godfrey K. 2006. The developmental origins
hypothesis:Epidemiology. In: Gluckman PD, Hanson MA, editors.
De-velopmental Origins of Health and Disease. Cambridge:Cambridge
University Press. pp 632.
Haig D, Graham C. 1991. Genomic imprinting and the
strange case of the insulin-like growth factor II receptor.Cell
64:10451046.
Hales CN, Barker DJ. 2001. The thrifty phenotype hypoth-esis. Br
Med Bull 60:520.
Hales CN, Barker DJ, Clark PM, Cox LJ, Fall C, Osmond C,Winter
PD. 1991. Fetal and infant growth and impairedglucose tolerance at
age 64. BMJ 303:10191022.
Hales CN, Ozanne SE. 2003. The dangerous road of catch-up
growth. J Physiol 547:510.
Hardy R, Wadsworth MEJ, Langenberg C, Kuh D. 2004.Birthweight,
childhood growth, and blood pressure at 43years in a British
cohort. Int J Epidemiol 33:121129.
Heindel JJ, Lawler C. 2006. Role of exposure to
environmentalchemicals in developmental origins of health and
disease.In: Gluckman PD, Hanson MA, editors. DevelopmentalOrigins
of Health and Disease. Cambridge: Cambridge
University Press. pp 8297.Hinchliffe SA, Lynch MRJ, Sargent PH,
Howard CV, Van-Velzen D. 1992. The effect of intrauterine growth
retar-dation on the development of renal nephrons. Br J
ObstetGynaecol 99:296301.
Hofman PL, Regan F, Jackson WE, Jefferies C, Knight DB,Robinson
EM, Cutfield WS. 2004. Premature birth andlater insulin resistance.
N Engl J Med 351:21792186.
Ibanez L, Ferrer A, Marcos MV, Hierro FR, de Zegher F.2000.
Early puberty: Rapid progression and reduced finalheight in girls
with low birth weight. Pediatrics 106:7274.
Ibanez L, Ong K, Dunger DB, de Zegher F. 2006. Early
de-velopment of adiposity and insulin resistance followingcatch-up
weight gain in small-for-gestational-age chil-dren. J Clin
Endocrinol Metab 91:21532158.
Ibanez L, Potau N, Enriquez G, Marcos MV, DeZegher F.2003.
Hypergonadotrophinaemia with reduced uterineand ovarian size in
women born small-for-gestational-age. Hum Reprod 18:15651569.
Islam MS, Sjoholm A , Emilsson V. 2000. Fetal pancreaticislets
express functional leptin receptors and leptin stim-ulates
proliferation of fetal islet cells. Int J Obes RelatMetab Disord
24:12461253.
Jablonka E, Oborny B, Molnar I, Kisdi E, Hofbauer J,Czaran T.
1995. The adaptive advantage of phenotypicmemory in changing
environments. Philos Trans R SocLond B 350:133141.
Jasienska G, Ziomkiewicz A, Lipson SF, Thune I, Ellison PT.2006.
High ponderal index at birth predicts high estradiollevels in adult
women. Am J Hum Biol 18:133140.
Jimenez-Chillaron JC, Hernandez-Valencia M, Lightner A,
Faucette RR, Reamer C, Przybyla R, Ruest S, Barry K,Otis JP,
Patti ME. 2006. Reductions in caloric intake and
17DEVELOPMENTAL CHOICE OF LIFE HISTORY STRATEGY
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
18/19
early postnatal growth prevent glucose intolerance andobesity
associated with low birthweight. Diabetologia 49:19741984.
Jordan KM, Syddall H, Dennison EM, Cooper C, Arden NK.2005.
Birthweight, vitamin D receptor gene polymorphism,
and risk of lumbar spine osteoarthritis. J Rheumatol
32:678683.
Kaati G, Bygren LO, Edvinsson S. 2002. Cardiovascular
anddiabetes mortality determined by nutrition during parentsand
grandparents slow growth period. Eur J Hum Genet10:682688.
Kajantie E, Rautanen A, Kere J, Andersson S, Yliharsila H,Osmond
C, Barker DJP, Forsen T, Eriksson J. 2004. Theeffects of the ACE
gene insertion/deletion polymorphismon glucose tolerance and
insulin secretion in elderly peo-ple are modified by birth weight.
J Clin Endocrinol Metab89:57385741.
Kajantie E, Osmond C, Barker DJP, Forsen T, PhillipsDIW,
Eriksson JG. 2005. Size at birth as a predictor ofmortality in
adulthood: A follow-up of 350 000 person-years. Int J Epidemiol
34:655663.
Karlberg J. 2002. Secular trends in pubertal development.Horm
Res 57 (Suppl 2):1930.
Kirkwood TBL. 2002. Evolution of ageing. Mech AgeingDev
123:737745.
Kubaszek A, Markkanen A, Eriksson JG, Forsen T,Osmond C, Barker
DJP, Laakso M. 2004. The associationof the K121Q polymorphism of
the plasma cell glycopro-tein-1 gene with type 2 diabetes and
hypertension de-pends on size at birth. J Clin Endocrinol Metab
89:20442047.
Kuzawa CW. 2005. Fetal origins of developmental plastic-ity: Are
fetal cues reliable predictors of future nutritionalenvironments?
Am J Hum Biol 17:521.
Kuzawa CW, Pike IL, editors. 2005. Fetal origins of
devel-opmental plasticity (Wiley-Liss Plenary Symposium). AmJ Hum
Biol 17:1118.
Kwong WY, Wild AE, Roberts P, Willis AC, Fleming TP.2000.
Maternal undernutrition during the preimplanta-tion period of rat
development causes blastocyst abnor-malities and programming of
postnatal hypertension.Development 127:41954202.
Langley-Evans SC, Langley-Evans AJ, Marchand MC.2003.
Nutritional programming of blood pressure and re-nal morphology.
Arch Physiol Biochem 111:816.
Lee TM, Spears N, Tuthill CR, Zucker I. 1989. Maternalmelatonin
treatment influences rates of neonatal devel-opment of meadow vole
pups. Biol Reprod 40:495502.
Lee TM, Zucker I. 1988. Vole infant development is influ-enced
perinatally by maternal photoperiodic history. AmJ Physiol
255:R831R838.
Leimar O, Hammerstein P, van Dooren TJM. 2006. A newperspective
on developmental plasticity and the princi-
ples of adaptive morph determination. Am Nat
167:367376.Lelievre-Pegorier M, Vilar J, Ferrier ML, Moreau E,
Freund N, Gilbert T, Merlet-Benichou C. 1998. Mild vita-min A
deficiency leads to inborn nephron deficit in therat. Kidney Int
54:14551462.
Lillycrop KA, Phillips ES, Jackson AA, Hanson MA, BurdgeGC.
2005. Dietary protein restriction of pregnant ratsinduces and folic
acid supplementation prevents epige-netic modification of hepatic
gene expression in the off-spring. J Nutr 135:13821386.
Lucas A. 1991. Programming by early nutrition in man.Ciba Found
Symp 156:3850.
Lucas A, Morley R, Cole TJ. 1998. Randomised trial of earlydiet
in preterm babies and later intelligence quotient.BMJ
317:14811487.
Mallard C, Loeliger M, Copolov D, Rees S. 2000. Reducednumber of
neurons in the hippocampus and the cerebel-
lum in the postnatal guinea-pig following
intrauterinegrowth-restriction. Neuroscience 100:327333.
McCarton CM, Wallace IF, Divon M, Vaughan HG Jr. 1996.Cognitive
and neurologic development of the premature,small for gestational
age infant through age 6: Compari-
son by birth weight and gestational age. Pediatrics
98:11671178.
McMillen IC, Robinson JS. 2005. Developmental origins ofthe
metabolic syndrome: Prediction, plasticity, and pro-gramming.
Physiol Rev 85:571633.
Mericq V, Ong KK, Bazaes RA, Pena V, Avila A, Salazar T,Soto N,
Iniguez G, Dunger DB. 2005. Longitudinalchanges in insulin
sensitivity and secretion from birth toage three years in small-
and appropriate-for-gesta-tional-age children. Diabetologia
48:26092614.
Moran NA. 1992. The evolutionary maintenance of alterna-tive
phenotypes. Am Nat 139:971989.
Morton NE. 1955. The inheritance of human birth weight.Ann Hum
Genet 20:125 134.
Muehlenbein MP, Bribiescas RG. 2005. Testosterone-medi-ated
immune functions and male life histories. Am J Hum
Biol 17:527558.Neel JV. 1962. Diabetes mellitus: A thrifty
genotype rendered
detrimental by progress? Am J Hum Genet 14:353362.Neggers Y,
Goldenberg RL. 2003. Some thoughts on body
mass index, micronutrient intakes, and pregnancy out-come. J
Nutr 133:1737S1740S.
Negus NC, Berger PJ, Pinter AJ. 1992. Phenotypic plastic-ity of
the montane vole (Microtus montanus) in unpre-dictable
environments. Can J Zool 70:21212124.
Newman RA. 1992. Adaptive plasticity in amphibian
meta-morphosis. BioScience 42:671678.
ORegan D, Welberg LL, Holmes MC, Seckl JR. 2001. Glu-cocorticoid
programming of pituitary-adrenal function:Mechanisms and
physiological consequences. Semin Neo-natol 6:319329.
Ounsted M. 1965. Maternal constraint of foetal growth in
man. Dev Med Child Neurol 7:479491.Ounsted M, Ounsted C. 1973.
On Fetal Growth Rate: ItsVariations and Their Consequences. London:
HeinemannMedical Books.
Painter RC, Roseboom TJ, Bleker OP. 2005. Prenatal expo-sure to
the Dutch famine and disease in later life: Anoverview. Reprod
Toxicol 20:345352.
Pembrey ME, Bygren LO, Kaati G, Edvinsson S, North-stone K,
Sjostrom M, Golding J, the ALSPAC study team.2006. Sex-specific,
male-line transgenerational responsesin humans. Eur J Hum Genet
14:159166.
Phillips DI, Barker DJ, Fall CH, Seckl JR, Whorwood CB,Wood PJ,
Walker BR. 1998. Elevated plasma cortisol con-centrations: A link
between low birth weight and the in-sulin resistance syndrome? J
Clin Endocrinol Metab 83:757760.
Pike IL. 2006. Maternal stress and fetal responses:
Evolu-tionary perspectives on preterm delivery. Am J Hum
Biol17:5565.
Plagemann A, Waas T, Harder T, Rittel F, Ziska T, Rohde W.2000.
Hypothalamic neuropeptide Y levels in weaning off-spring of
low-protein malnourished mother rats. Neuro-peptides 34:16.
Potts R. Environmental hypotheses of hominin evolution.1998.
Yearbk Phys Anthropol 41:93136.
Queitsch C, Sangster TA, Lindquist S. 2002. Hsp90 as a
ca-pacitor of phenotypic variation. Nature 417:618624.
Relyea R, Hoverman JT. 2003. The impact of larval preda-tors and
competitors on the morphology and fitness of ju-venile treefrogs.
Oecologia 134:596604.
Ross M, Desai M, Guerra C, Wang S. 2005. Prenatal pro-gramming
of hypernatremia and hypertension in neonatal
lambs. Am J Physiol Regul Integr Comp Physiol 288:R97R103.
18 GLUCKMAN ET AL.
American Journal of Human Biology DOI 10.1002/ajhb
-
7/28/2019 Early Life Events and Their Consequences for Later
Disease a Life History and Evolutionary Perspective
19/19
Sayer A, Cooper C. 2005. Fetal programming of body com-position
and musculoskeletal development. Early HumDev 81:735744.
Schlichting CD, Pigliucci M. 1998. Phenotypic Evolution:
AReaction Norm Perspective. Sunderland, MA: Sinauer
Associates.Schmalhausen IL. 1949. Factors of Evolution. New
York: