Embed Size (px)
Citation preview
Easing the Transition: Private Practice to Employment
Leslie Garson, MD Executive Director, Physician Practices
St. Vincent Regional Medical Center
Howard Gershon Principal,
New Heights Group
4/30/13 Slide 2
Agenda • Introductions • Why employment? • Who is being employed? • What are the key challenges? • How are these being addressed?
4/30/13 Slide 3
St. Vincent Regional Medical Center
• Est. 1865 • New Mexico's oldest hospital • Non-profit, non-affiliated • Local board of directors • Major medical center for
19,000 square-mile area
4/30/13 Slide 4
• 268 licensed beds • 250 physicians • 22 medical specialties • 45 employed physicians • Level III Trauma Center
(Only in northern New Mexico) • More than 56,000 Emergency
patients treated annually
St. Vincent Regional Medical Center
4/30/13 Slide 5
Threats to Private Practices • Increasing Government regulation • Growing capital requirements • Declining reimbursement • Shifting power toward payers • Skyrocketing malpractice rates • Growing consumer demands • Move towards transparency • Lifestyle concerns
4/30/13 Slide 6
Why do Hospitals Employ Physicians? • To fully integrate care across the continuum
– Improve outcomes and patient safety – Reduce resource utilization and duplication – Align incentives
• To place committed physicians in outlying markets • To create or strengthen ties with specialists who
support the Hospital • To address specific community/employer needs
• To maximize use of Information Technology
4/30/13 Slide 7
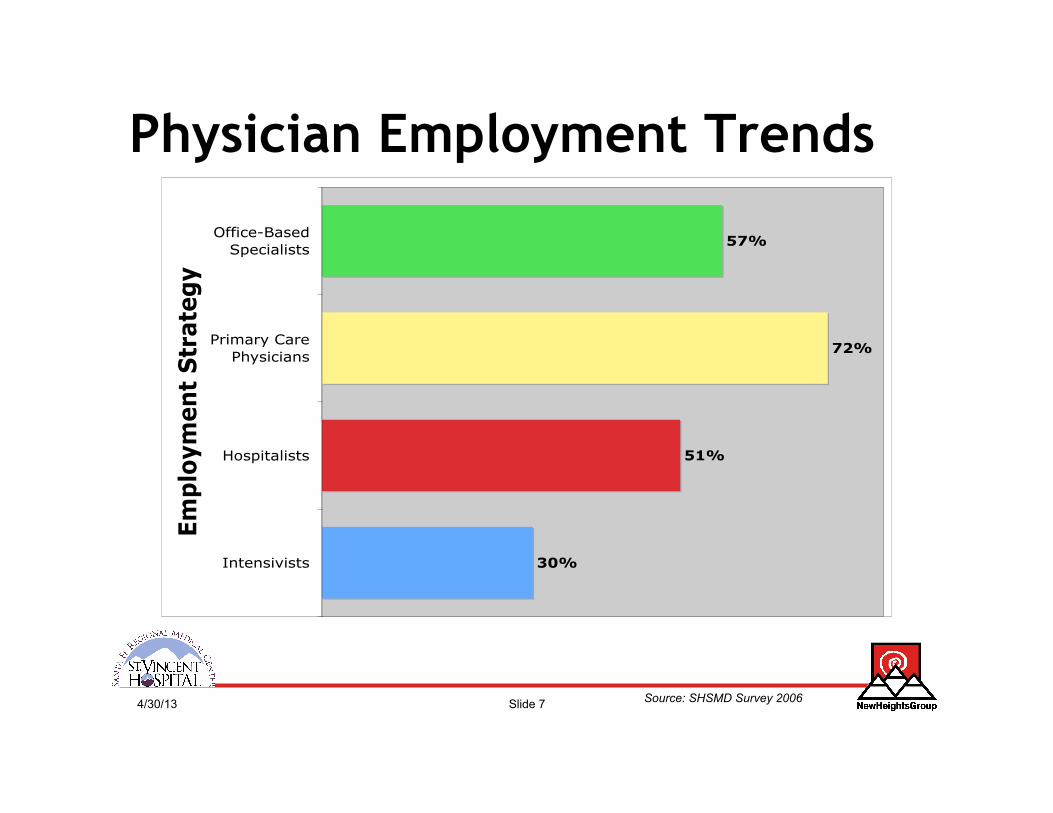
Physician Employment Trends
Source: SHSMD Survey 2006
30%
51%
72%
57%
Intensivists
Hospitalists
Primary Care
Physicians
Office-Based
Specialists
Em
plo
ym
en
t S
trate
gy
4/30/13 Slide 8
Source of Employed MDs
• Established Private Practices • Other employment situations • Newly graduated residents
4/30/13 Slide 9
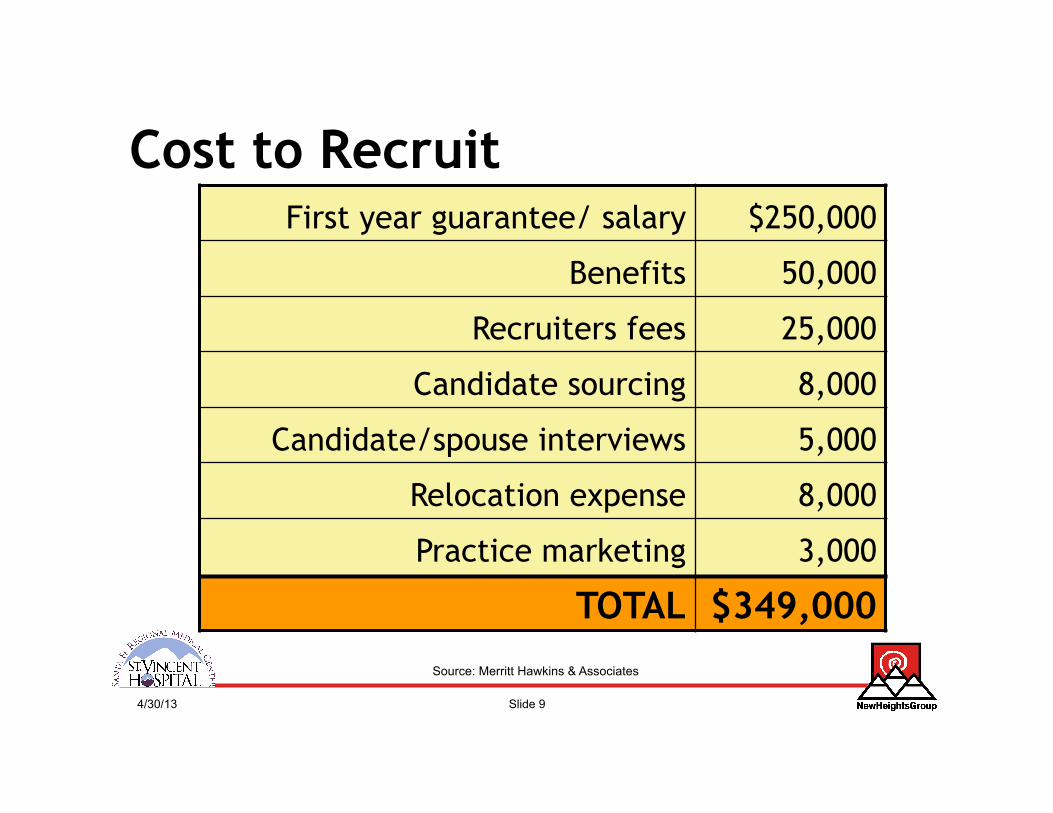
Cost to Recruit
Source: Merritt Hawkins & Associates
First year guarantee/ salary $250,000
Benefits 50,000
Recruiters fees 25,000
Candidate sourcing 8,000
Candidate/spouse interviews 5,000
Relocation expense 8,000
Practice marketing 3,000
TOTAL $349,000
4/30/13 Slide 10
Cost to Replace • Financial consequences
– Recruitment expenses – Lost revenue
• Effects on patient satisfaction • Effects on the organization • Effects on public relations
Source: American Journal of Medical Quality, Vol. 19, No. 2, 56-66 (2004); A Review of Physician Turnover: Rates, Causes, and Consequences Anita D. Misra-Hebert, MD, et al.
4/30/13 Slide 11
Why Physicians Move? • More money • Hours/ call schedule • Focus on patients • Lack of autonomy/appreciation • Poor relationships with Hospital
Administration • Poor relationships with Colleagues
Source: Pinnacle Health Group
4/30/13 Slide 12
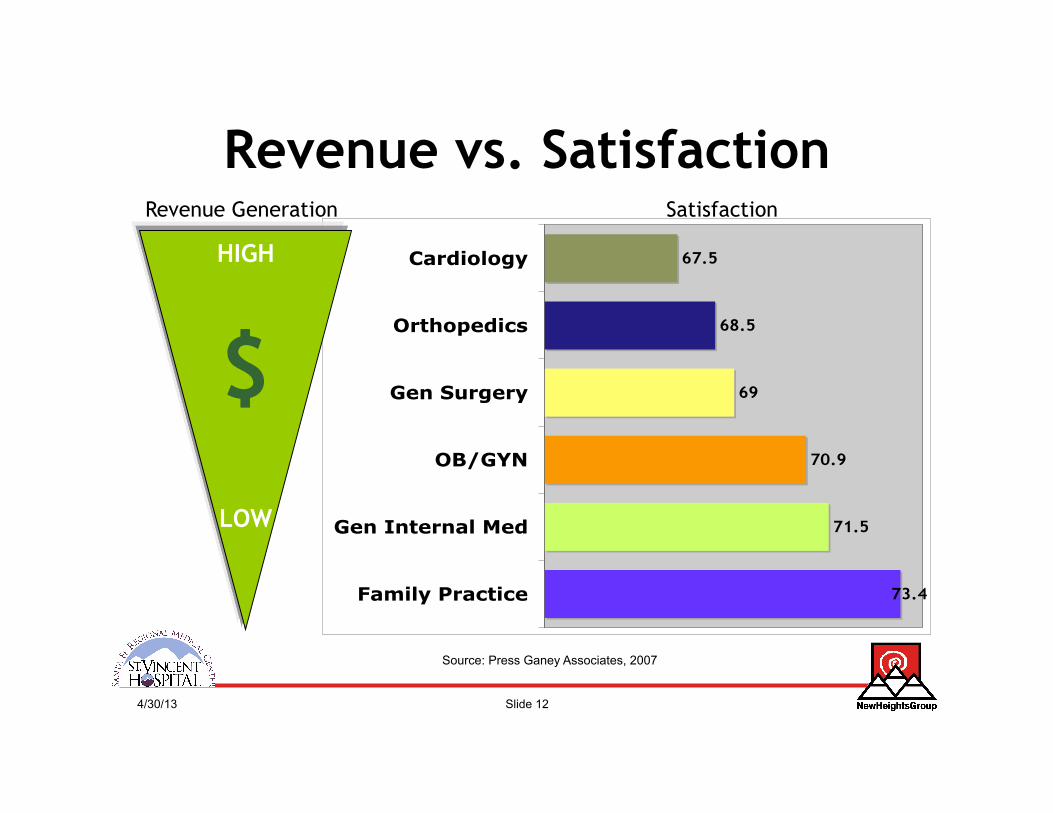
Revenue vs. Satisfaction
73.4
71.5
70.9
69
68.5
67.5
Family Practice
Gen Internal Med
OB/GYN
Gen Surgery
Orthopedics
Cardiology
Satisfaction
HIGH
$
LOW
Revenue Generation
Source: Press Ganey Associates, 2007
4/30/13 Slide 13
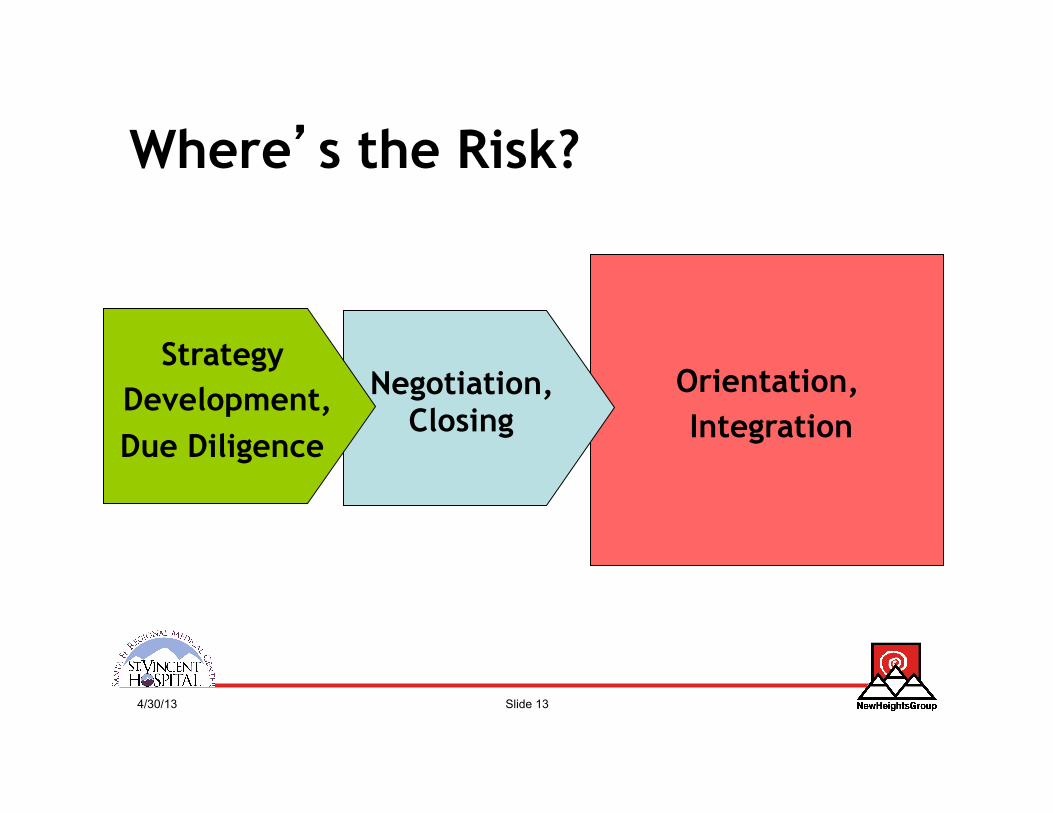
Where’s the Risk?
Orientation, Integration
Negotiation, Closing
Strategy Development, Due Diligence
4/30/13 Slide 14
You have to have a strategy, not something you hope for, but something you work for.
Floyd Loop, MD
4/30/13 Slide 15
Key Components of a Strategy • Expectations • Governance/Leadership • Compensation • Practice Management
4/30/13 Slide 16
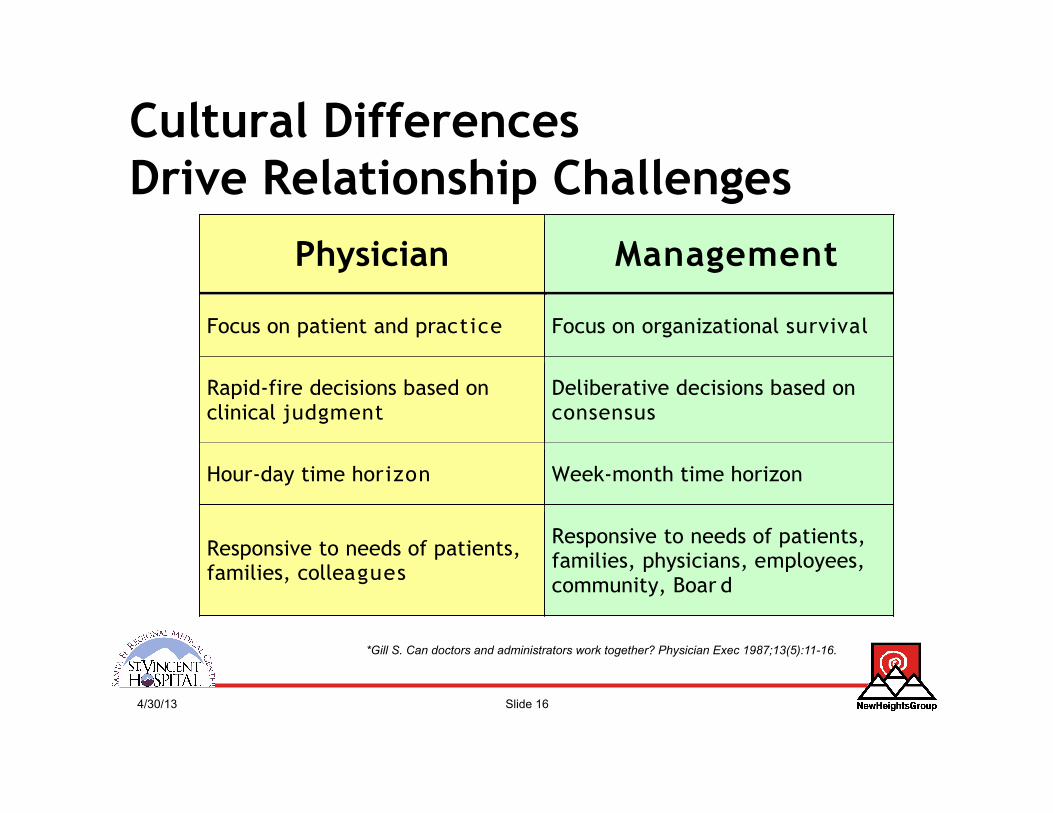
Cultural Differences Drive Relationship Challenges
*Gill S. Can doctors and administrators work together? Physician Exec 1987;13(5):11-16.
Physician Management
Focus on patient and practice Focus on organizational survival
Rapid-fire decisions based on clinical judgment
Deliberative decisions based on consensus
Hour-day time horizon Week-month time horizon
Responsive to needs of patients, families, colleagues
Responsive to needs of patients, families, physicians, employees, community, Boar d
4/30/13 Slide 17
4/30/13 Slide 18
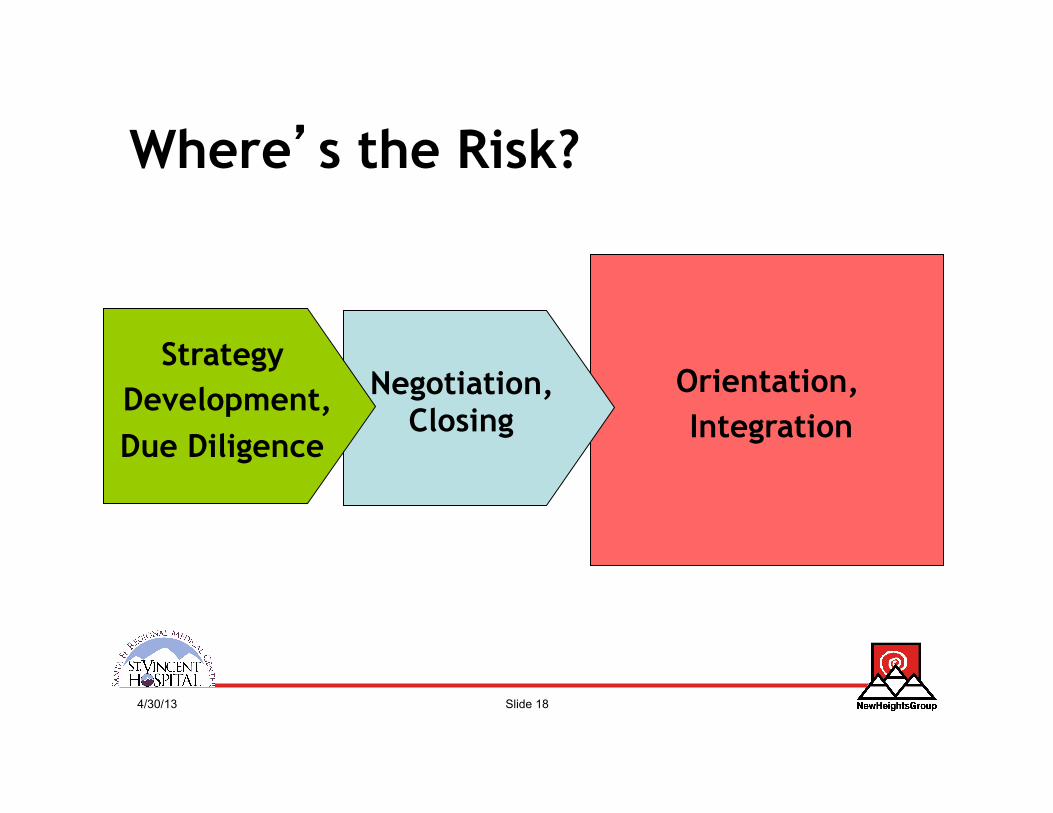
Where’s the Risk?
Orientation, Integration
Negotiation, Closing
Strategy Development, Due Diligence
4/30/13 Slide 19
The Devil is in the Details • Term • Duties &
Performance • Licenses • Salary • Benefits • Vacation & PTO • Expense
Reimbursement
• Malpractice Insurance
• Acceptance of Patients
• Ownership of Records
• Non-compete • Non-solicit • Termination
4/30/13 Slide 20
Where’s the Risk?
Orientation, Integration
Negotiation, Closing
Strategy Development, Due Diligence
4/30/13 Slide 21
• Orienting • Mentoring • Monitoring
Physician Transition Guide
4/30/13 Slide 22
First Impressions Count: Physician Priorities
1. Response of hospital administration 2. Administration deals with changes 3. Confidence in hospital
administration 4. Communication with hospital
administration
Source: Press Ganey Associates, 2007
4/30/13 Slide 23
Orienting: Employee Checklist
• ID Badge • Parking Sticker • TB Fit Testing • TB Screening • Mailbox location • Medical Staff Library location • Hospital policies & procedures
4/30/13 Slide 24
Orienting: Hospital Leaders
• Senior Management Team • Executive Committee • Section Chiefs • Medical Directors
4/30/13 Slide 25
Orienting: Departmental Meetings
• Emergency Department • Information Systems • Health Information Management • Pharmacy • Operating Room • ICU • Obstetrics • Outpatient Clinic • Radiology • Hospitalist Program
4/30/13 Slide 26
Orienting: Key Committees
• Credentials Committee • Quality Mgmt. Committee • Pharmacy, Nutrition and Therapeutics (PNT)
Committee • Infection Control Committee • Transfusion Committee • Radiation Safety Sub-Committee • Medical Education Committee • Critical Care Committee • Bylaws Committee • ER Trauma Committee • Cancer Care Committee • Physician Assistance Committee
4/30/13 Slide 27
Orienting: Information Systems
• Available Clinical & Specialty Applications
• Access Codes and Passwords
• Requesting Support & Services
4/30/13 Slide 28
• Orienting • Mentoring • Monitoring
Physician Transition Guide
4/30/13 Slide 29
Mentoring • The Merriam-Webster Dictionary
defines a mentor as "a trusted counselor or guide."
• The Anesthesiology Department of Cleveland’s MetroHealth System defines mentor as "a wise, loyal advisor or coach."
4/30/13 Slide 30
Mentoring @John Muir
• “Local” mentor • “Leadership” mentor • Social activities
4/30/13 Slide 31
• Orienting • Mentoring • Monitoring
Physician Transition Guide
4/30/13 Slide 32
Monitoring • Productivity
– WRVUS – Clinic Revenue Growth
• Quality – Clinical Indicators (HEDIS, PQRI)
• Patient satisfaction – Satisfaction Surveys
• Professional growth. – CMEs
4/30/13 Slide 33
Putting it all Together
4/30/13 Slide 34
Focus on Patients “ After becoming an employed physician, I found the
key benefits tend to be fewer management
concerns and general peace of mind. As a result,
I’m able to concentrate on taking care of
patients.”
~ Dr. Gupta, Norton Healthcare
4/30/13 Slide 35
”My excitement is to have found a place that works for me….It is absolutely acceptable to make choices between money and time, between work
and family. And the career growth I am experiencing is really interwoven with the
personal growth I'm feeling.”
~ Tanya Threewitt, MD, Family Practice
John Muir Medical Group
Quality of Life
4/30/13 Slide 36
Questions & Comments




















![[BLT] 2015년 정부지원사업 - 06월 ver3.1](https://img.pdfslide.net/doc/110x75/55d5ae1fbb61eb6e068b45e4/blt-2015-06.jpg)