Embed Size (px)
Citation preview

Eating the QI Elephant….An example from New Hampshire…
Lea R. Ayers LaFave, PhD, RNCommunity Health Institute/JSI
Washington, DC September 16, 2010

The Charge: Provide insight into AIM statement development
Broad Concept for QI
Develop an AIM Statement
The Project – What we did…
What happened….

AIM Statement Development: Dimensions• Influence
– Is the problem workable?– Do we have control over the element?– Can a solution by implemented by the team?
• Focus– Internal or external?
• Issue– Target operational or strategic issues
• Measurement– Process measures more operational– Collected as work is performed or actions taken
Benefits: early success/skill development

AIM Statement Development: Challenges• Clear understanding of a problem
– May be evolving– May be complex
• Fine focus on an issue that can be– influenced– measured– affected within a finite time period
• Clear linkage to more global aims

Caring Community Network of the Twin Rivers, NH
Old Mill Town
Central NH

Background• Purpose of CCNTR
– To promote individual and environmental health as a fundamental requirement for healthy communities
– Includes FQHC
• Population: – High poverty level rural community with all associated morbidities
• Patterns: – Reaction rather than prevention culture (chronic disease, substance abuse,
emergencies)– Many providers don’t live in the community– Angry parents notified of student w/High BMI
• why didn’t MD say anything?– Lack of coordination/communication between PCPs and School Nurse about
childrens’ healthy weights– Providers uncomfortable raising the issue
• Healthy eating/active living not routinely discussed

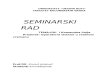
2007-2008 Age/ Gender Specific Body-Mass-I ndex (BMI ) Percentile for Franklin School District K-4th
Grade (n=496)
0%
10%
20%
30%
40%
50%
60%
BMI Percentile Risk Rating
% o
f S
tud
en
ts i
n R
isk
Rati
ng
Students (n=496) 0.48 0.22 0.29
HEAL Goal* 0.05
Healthy Weight Overweight Obese


The Problem
• Annual well-child visits to health care professionals should include measurement of BMI to determine weight status (American Pediatrics Committee on Nutrition, 2003)
• CCNTR PCPs rely on external websites to calculate BMI, then adjust the assessment tool to identify BMI risk rating.
• If exam rooms lack internet access, BMI calculation will not be computed and interpreted to the patient with a discussion of behavioral strategies for patients or families of overweight children.

PLANGetting Started
– Focus on Primary Care Setting and how weight related risk and behavioral assessment is being delivered to youth
– Run report at 4 local primary care practices of children ages 2-19 with a well-child visit in 2007 fiscal year with a documented BMI or BMI percentile
• BMI documentation rates – wide variation - 7/1/07-6/30/08 (12.6-90%)
Team• Community Health Center, Educators, Hospital-based
QI/IT
• Getting Started• Assemble the Team• Examine the Current
Approach• Identify Potential Solutions

PLAN
Current Approach • Local providers lack EMR capability to efficiently
screen/document BMI risk during well child visits
• Healthy eating/active living not routinely discussed during visits
• Lack of uniform office flow, self-management of health behavior goal setting
• Getting Started• Assemble the Team• Examine the Current
Approach• Identify Potential Solutions

PLAN
Potential Solutions• Install new technology
– calculates and documents BMI risk-rating and weight-related health behaviors into EMR at well-child visits.
• Clinical staff education – evidence on obesity as indicator for chronic disease risk
• Strengthen motivational interviewing techniques• Establish referral protocols
– to community-based education, treatment and consultation resources regarding health eating/active living
• Emphasize fit with Chronic Care Model
• Getting Started• Assemble the Team• Examine the Current Approach• Identify Potential Solutions

Develop an Improvement Theory
• If providers have access to BMI data, information about best practices and support in approaching families about health-related issues, they will address them.
• The team will improve health care provider access to timely BMI risk rating analysis through – redesign of clinical flow to assess behavior, – provide effective communication strategies and referrals, – interpret weight related health into diagnosis and treatment
• Goal: All 4 Primary Care Practices documenting at least 65% of children’s BMI seen in the following year

AIM Statement:
To increase the percentage of youth (>2 <19 years old) receiving primary care preventive services who had an age and gender appropriate Body Mass Index (BMI) percentile documented in their medical record at least once in the past year to 65% by June 30th, 2009
Discrete – Measurable – Timebound

Do
• Educated providers – BMI measures– community profile– available referral resources– research identifying weight-related health as an
indicator for chronic disease risk
• Identified EMR BMI risk rating tool and uploaded for prompt evaluation at time of visit
• Promoted routine calculation of BMI risk rating at each clinical encounter as a VITAL SIGN
Test the Theory for Improvement


Do • Designated a “Wellness Champion” in clinic
• Reviewed evidence and recommendations for increasing assessment, prevention, treatment and clinical guidelines
• Created diagram and educate medical staff on clinical office flow for weight-related health risk factor assessment
Test the Theory for Improvement



Do
Documented Self-Management goal in EMR as a measurable health indicator
Test the Theory for Improvement

Do
Identified locations suitable for outreach activities to distribute printed materials to community members
Test the Theory for Improvement

STUDYUse Data to StudyResults of the Test

ACTStandardize:
Continue to…
– educate and promote the importance of daily behaviors related to 5210 Healthy NH
– foster collaboration between CCNTR and local PCPs about referral for local nutritional and physical activity resources
– utilize QI tools in day-to-day activities
– engage in broad community outreach
– familiarize CCNTR staff with QI concepts, tools and methods with particular evidence on evidence-based interventions
• Standardize the Improvement• Establish Future Plans

ACTFuture Plans:
– Disseminate obesity statistics, trends and health indicators to health care partners to further develop QI echoing community efforts
– Expand QI efforts to other Healthy Eating Active Living (HEAL) sectors in the region
• worksites & workplaces • schools • food & recreation industries• communities & municipalities
• Standardize the Improvement• Establish Future Plans

Facilitating Factors
• Clear organizational mission • Root cause analysis
– Shared view of the problem
• Access to data• Wellness Champions • Regular meetings• Development of data-rich environment
– Clear linkage of outcome to intervening processes
• Clear, focused, discrete, time-bound, measurable AIM statement based on assessment

Building an Information-Rich
Environment

Thank you!
Questions?
Lea Ayers LaFave, PhD, RN
MLC-3 Project Director
Community Health Institute/JSI
501 South Street, 2nd Floor
Bow, NH 03304
603.573.3335

The Kansas Road: From The Kansas Road: From Concept to Action Concept to Action
The Kansas Road: From The Kansas Road: From Concept to Action Concept to Action
Tatiana Lin, Senior AnalystTatiana Lin, Senior Analyst
Kansas Health InstituteKansas Health Institute
MLC-3 Open ForumMLC-3 Open ForumWashington D.C. Washington D.C.
September 2010September 2010

ObjectivesObjectivesObjectivesObjectives
Demonstrate the process of developing an aim statement
Demonstrate the process of moving from concept to planning to implementation to outcomes

OverviewOverviewOverviewOverview Snapshot of the Kansas First (MCH) Collaborative Develop an aim statement
I. Plan
II. Do
III. Study
IV. Act
Lessons learned

Snapshot of the Snapshot of the Kansas First (MCH) Kansas First (MCH)
CollaborativeCollaborative

Map of the MLC-3 MCH Map of the MLC-3 MCH Collaborative TeamsCollaborative Teams
Map of the MLC-3 MCH Map of the MLC-3 MCH Collaborative TeamsCollaborative Teams
Source: U.S. Census Bureau, Census 2000


Introducing the Team - Northeast Corner Subregion Northeast Corner Subregion
Introducing the Team - Northeast Corner Subregion Northeast Corner Subregion
The Northeast Corner Subregion Shawnee County Health Agency Jefferson County Health Department
MLC-3 Team Composition: 9 members (e.g. pregnancy-testing clinics, STD
clinics, WIC clinics)
Targeted Programs: Title X Maternal Child Health Block Grant; Title X Family Planning/Pregnancy Testing; Women’s Infant and Children (WIC); SCHA Sexually Transmitted Disease; and SCHA-CHC M&I Prenatal Care

Develop
an Aim
Statement

Progression of the Aim Progression of the Aim StatementStatement
Progression of the Aim Progression of the Aim StatementStatement
Step 1: Learning about the issue Focusing Statement
Step 2: Looking ahead Issue Statement
Step 3: Narrowing focus Aim Statement

Step 1. Learning about the Issue - Step 1. Learning about the Issue - Focusing Statement Focusing Statement
Step 1. Learning about the Issue - Step 1. Learning about the Issue - Focusing Statement Focusing Statement
a. What is the issue? Late entry into prenatal care
b. What is the magnitude of the problem?Know your data: Prenatal care by trimester:
1st trimester: 51% 2nd trimester: 47% 3rd trimester: 2%
Population of concern: 24-44 yrs (White, Non-Hispanic & Hispanic/Spanish
speaking, not married, income <100%)

a. What is the main focus? Create your own question(s)
Does the group have complete control over the element?• Yes. The Northeast Subregion provides direct
services to a significant number of women of childbearing age.
What can we do for the patient(s)? Improve access? Improve outcomes? Provide better services? • All three components
What are the potential causes? • Existing referral system
Step 2: Looking Ahead -Step 2: Looking Ahead -
Issue Statement Issue Statement
Step 2: Looking Ahead -Step 2: Looking Ahead -
Issue Statement Issue Statement

What are the benefits of addressing the issue?• Improved timeliness of prenatal care • Improved birth outcomes
Step 2. Looking Ahead -Step 2. Looking Ahead -Issue Statement Cont. Issue Statement Cont. Step 2. Looking Ahead -Step 2. Looking Ahead -Issue Statement Cont. Issue Statement Cont.

Step 3. Narrowing Focus – Step 3. Narrowing Focus – Aim StatementAim Statement
Step 3. Narrowing Focus – Step 3. Narrowing Focus – Aim StatementAim Statement
a. How do we focus our region’s resources to address this issue? Connect to services Improve
access
Improve birth outcomes

Initial Aim Statement Initial Aim Statement
Achieve an annual average increase of pregnant women
accessing services at the SCHA-CHC M&I program in the first
trimester by 2% per year by 2013 (61%).

Final Aim StatementFinal Aim StatementFinal Aim StatementFinal Aim Statement: Final Aim Statement
By Oct. 1, 2009, in four clinic programs at two local health departments, pregnant women not enrolled in prenatal care will consistently be given a current listing of community obstetricians, 90% of those with limited resources will receive staff assistance in making a prenatal intake appointment, and 95% of those intakes will be scheduled within 10 working days from the date of request.
PMT Suggestions
1. Include a “target improvement date”
2. Include short-term measurable goals
4. Include the baseline rate, the target rate, and the percentage change
3. Include a “time component” such as “…to make a prenatal care appointment within the 14th week of pregnancy”

Final Aim Statement Cont. Final Aim Statement Cont. Final Aim Statement Cont. Final Aim Statement Cont. How will we know that a change is an
improvement? Increased number of scheduled prenatal
intake appointments Increased number of scheduled prenatal
intake appointments within two-weeks of the initial request
Increased number of women who entered prenatal care in the first trimester

PLAN PLAN

Current Approach Current Approach Current Approach Current Approach

Current Approach Cont. Current Approach Cont. Current Approach Cont. Current Approach Cont. Not all clinics provide a listing of area obstetricians
Providing a listing of obstetricians does not guarantee the client will make a prenatal appointment
Not all clinics consistently refer pregnant women to prenatal services
Limited number of prenatal intake appointments available each week
Outdated information in regard to clinic hours and choices available for delivery sites
Staff is challenged to complete referral paperwork Staff had an uncertain understanding of clients’
knowledge of the importance of early prenatal care

Do Do

Three PDSA CyclesThree PDSA Cycles
Three PDSA CyclesThree PDSA CyclesPDSA #1: Eliminate “cold handoff” referral Activities: Make intake appointment while the client is still on site – “Warm
handoff”.
PDSA #2: Increase the number of available intakeappointments Activities: Open/flex the M&I clinic intake appointment book to accommodate 2
– 5 more intakes per week.
PDSA #3: Identify common barriers to accessing prenatal care Activities: Conduct survey to identify common barriers to accessing prenatal
care, methods and resources used by women to obtain prenatal care information.
.

StudyStudy

PDSA #1: Eliminate “cold handoff” referralResults:
Intake appointments were scheduled less than 2 weeks out.
Linking clients can be accomplished while clients are on site as long as appointment call is made during the clinics working hours.
PDSA #2: Increase the number of available intake appointments Results:
Increased the percentage of intake appointments kept within 2 weeks from date of request from 83% to 97%.
Need to consistently expand the number of intake appointments on a weekly basis; up to 2 – 5 appointments per week to accommodate demand.
Three PDSA Cycles Three PDSA Cycles Three PDSA Cycles Three PDSA Cycles

Three PDSA Cycles Cont. Three PDSA Cycles Cont.
PDSA #3: Identify common barriers to accessing prenatal care
Results: Two-thirds of the pregnant women at both clinics did not
plan their pregnancies, making it harder for them to access prenatal care in a timely fashion after conception.
Need to continue analyzing the survey results

ResultsResults ResultsResults

ACT ACT ACT ACT
Continue to expand the number of prenatal intake appointments.
Standardize the process to schedule prenatal intake appointments within ten working days.
Adopt reformatted intake registration form in both English and Spanish.

Closing ThoughtsClosing Thoughts
Aim Statement Do’s
1. Base the aim statement on both data and organizational/regional needs Do your homework
Learn about the issue Understand the level of your control Use aim statement to guide your work
2. State the aim statement clearly and use numerical, measurable goals
Don’t1. Wordsmith 2. Spend too much time on the aim statement

Questions?

Contact Information Contact Information Contact Information Contact Information
Tatiana LinKansas Health Institute
212 8th Avenue, Suite 300Topeka, KS 66614
PHONE: 785/233- 5443
EMAIL: [email protected]
Web site: www.khi.org

Information for policymakers. Health for Kansans.Information for policymakers. Health for Kansans.
Kansas Health InstituteKansas Health Institute