Embed Size (px)
Citation preview
Echocardiographic Evaluation of Mitral Stenosis
Enrique TueroOctubre 7, 2016 Albert Starr
Sociedad de Cardiologia Rosarioviernes 7 de octubre 2016
Ausencia de interes financieroni asociacion o afiliacion conorganización/es que se puedapercibir como conflicto de interes

Redefinicion de historia natural / riesgo quirurgico
Avances en el diagnostico no invasivo
Avances en las tecnicas percutaneas
Realizacion de trabajos multicentricos
Logros valvulopatias
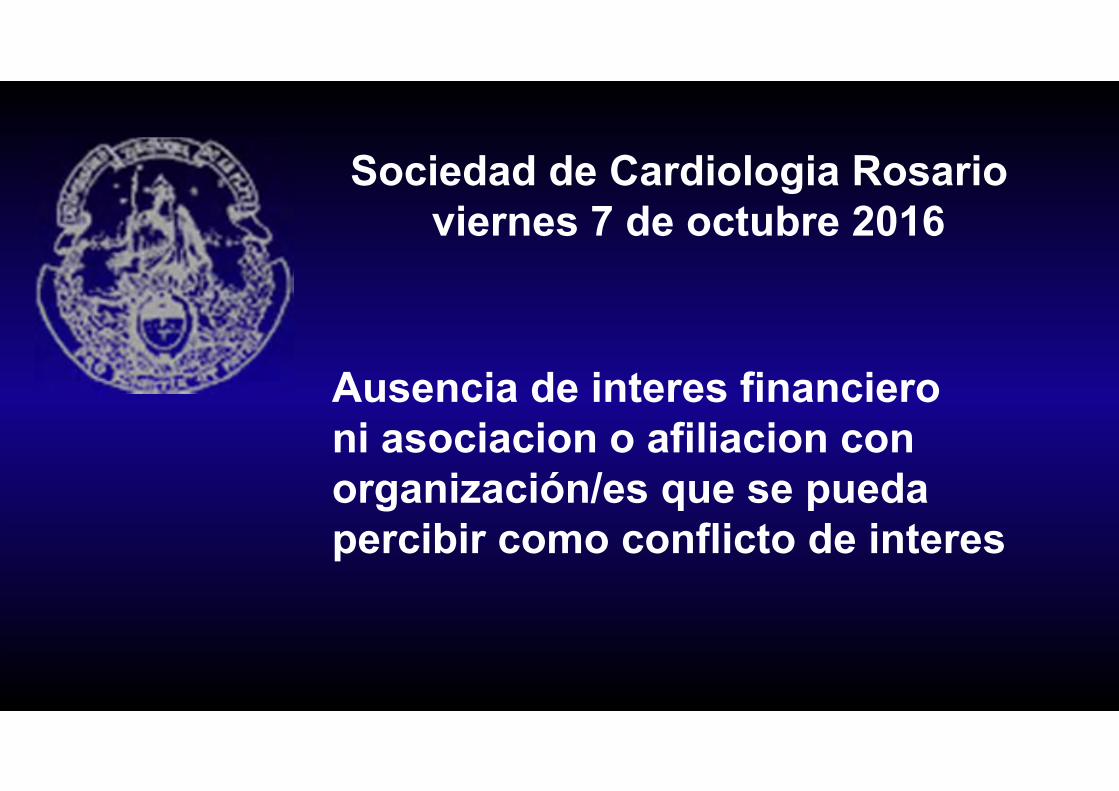
Mitral Stenosis
Etiologies• Rheumatic - almost all adults cases (RHD> 15million worldwide)
-60% of pts don’t have a history of ARF-50% of pts who have ARF don’t develop VHD
Very Severe Mitral Annular Ca++- (uncommon- CRF- hyperparathyroid,elderly)Congenital – rare parachute , Shone complexCor triatiatum sinister, mixoma,vegetation,thrombusProsthetic valve disfunction – 2 to Mitra Clip / surgery
Valvulopatias alta prevalenciaFR etio principal
Ecocardiografia
3 %
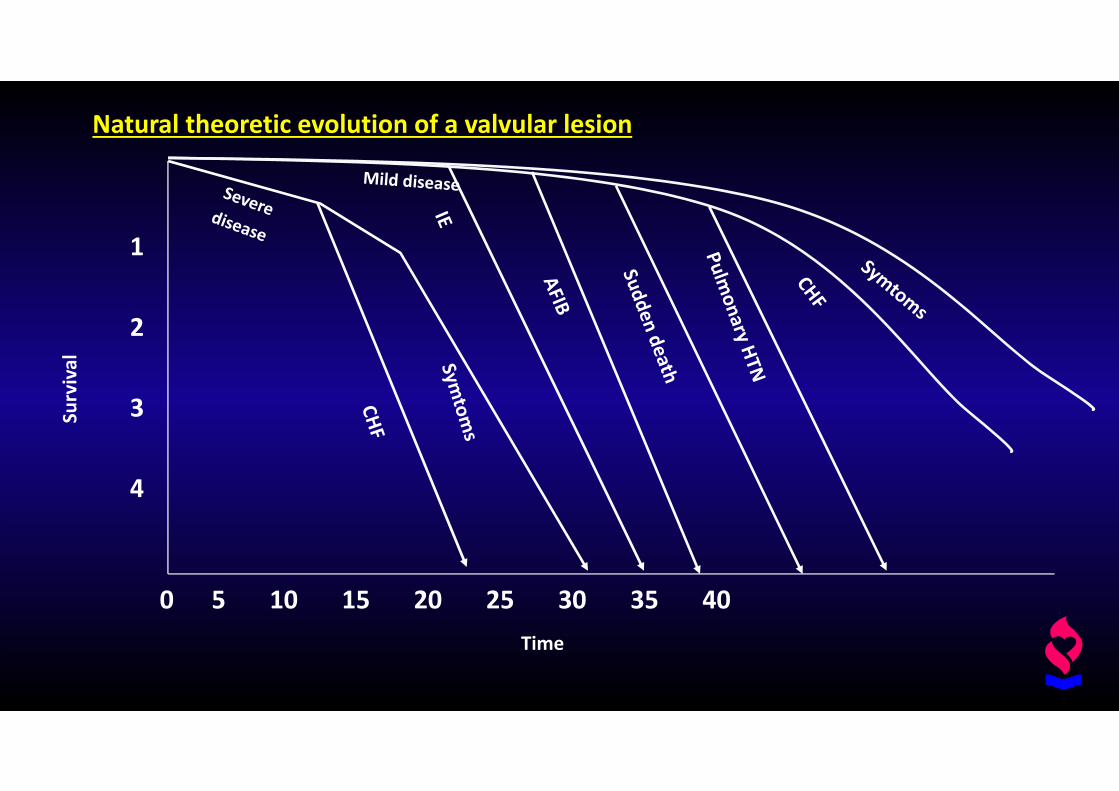
0 5 10 15 20 25 30 35 40
1
2
3
4
Time
Survival
Natural theoretic evolution of a valvular lesion

Mitral stenosisNatural history
100
80
60
40
20
05 10 15 20
Years
Survival %
1
2
34
Carabello1990
Natural historyLonger evolution
Mitral stenosisGeneral considerations & treatment
Diagnostic & severityEcodopplerScorePulmonary hypertension
ExerciseNon invasive
Percutaneous valvuloplastyEarlier indicationETE
ATG - EI
SurgicalReparativeProsthesisMaze surgeryLAA exclusion
Percutaneous MV replacementExperimental valveNon aproved FDA valve
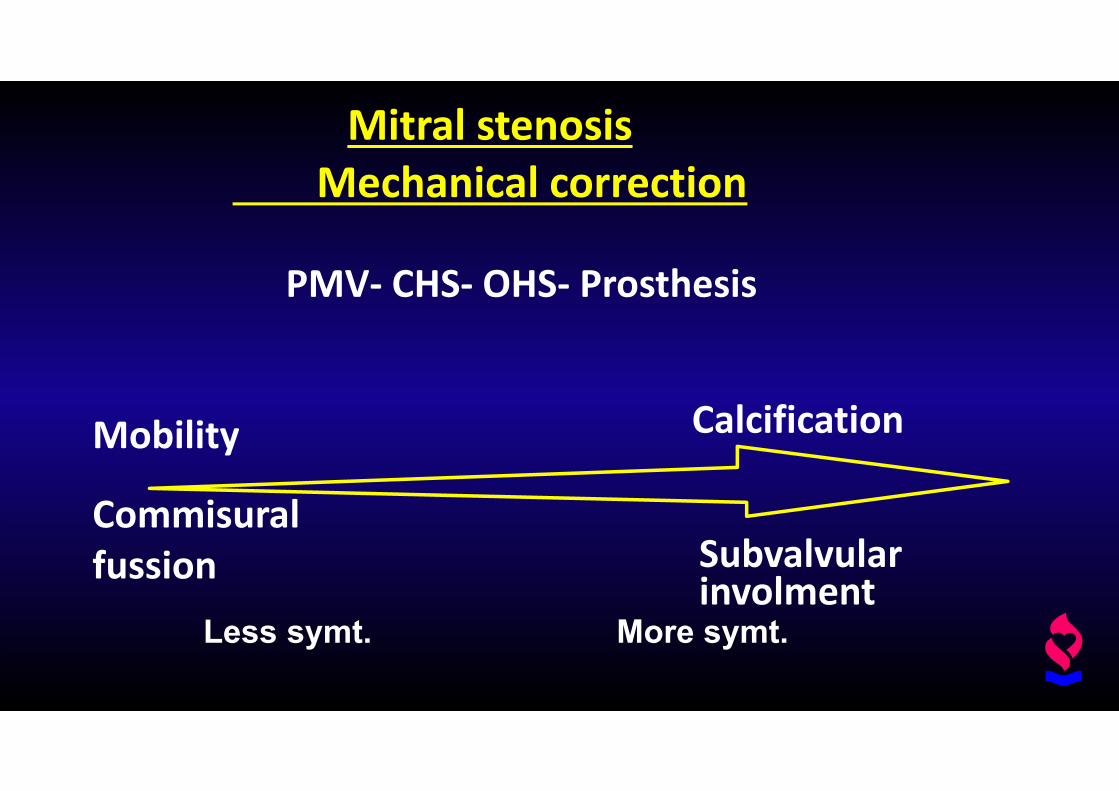
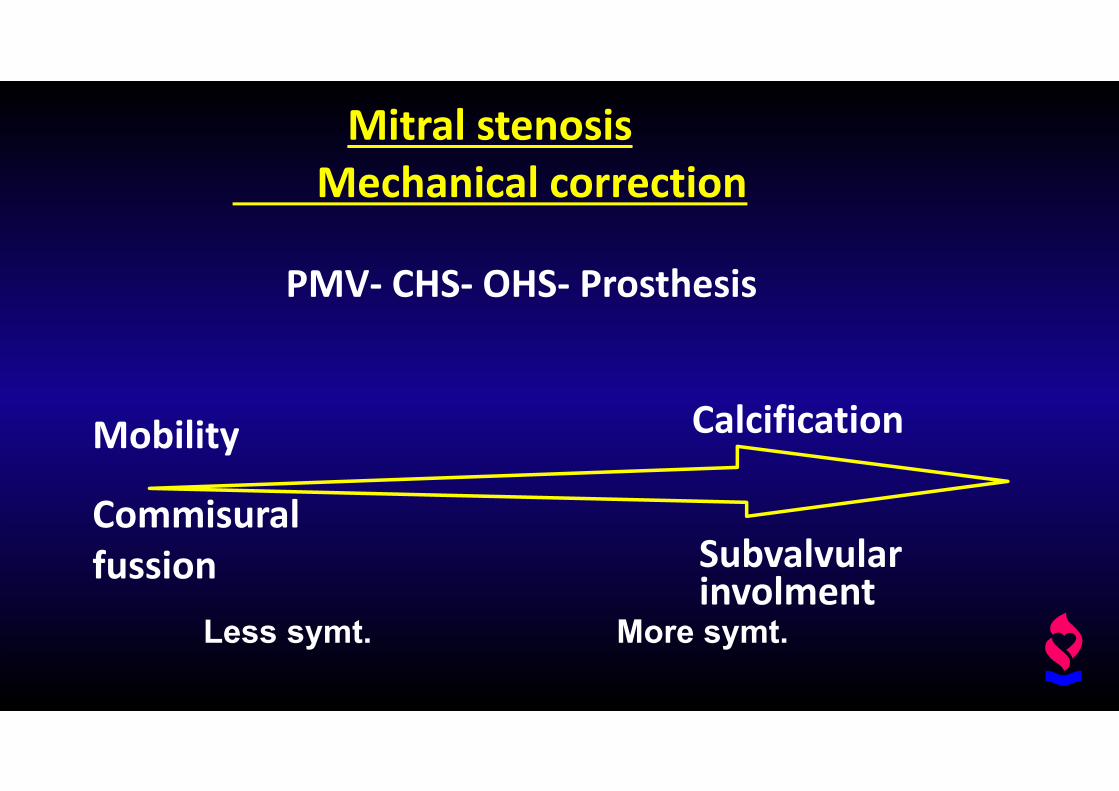
Mitral stenosisMechanical correction
PMV‐ CHS‐ OHS‐ Prosthesis
Mobility
Commisuralfussion
Calcification
Subvalvularinvolment
Less symt. More symt.
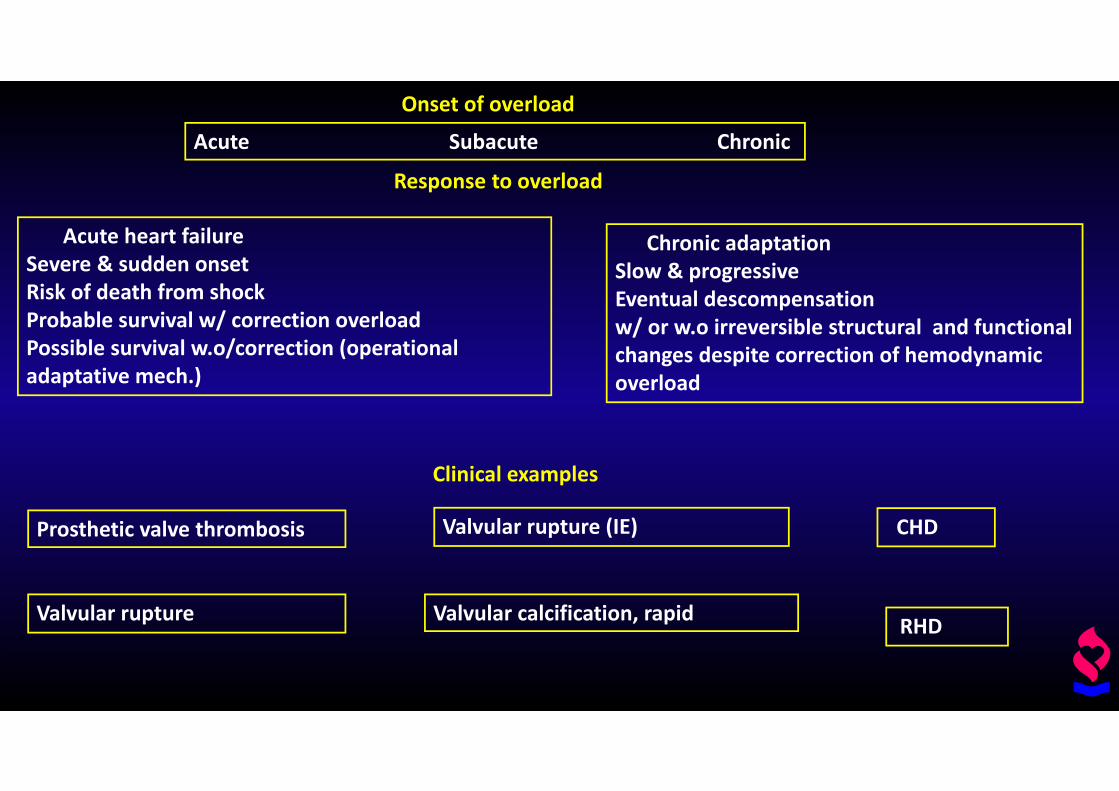
Acute Subacute Chronic
Onset of overload
Acute heart failureSevere & sudden onsetRisk of death from shockProbable survival w/ correction overloadPossible survival w.o/correction (operational adaptative mech.)
Response to overload
Chronic adaptationSlow & progressiveEventual descompensation w/ or w.o irreversible structural and functional changes despite correction of hemodynamic overload
Prosthetic valve thrombosis
Clinical examples
Valvular rupture
Valvular rupture (IE)
Valvular calcification, rapid
CHD
RHD
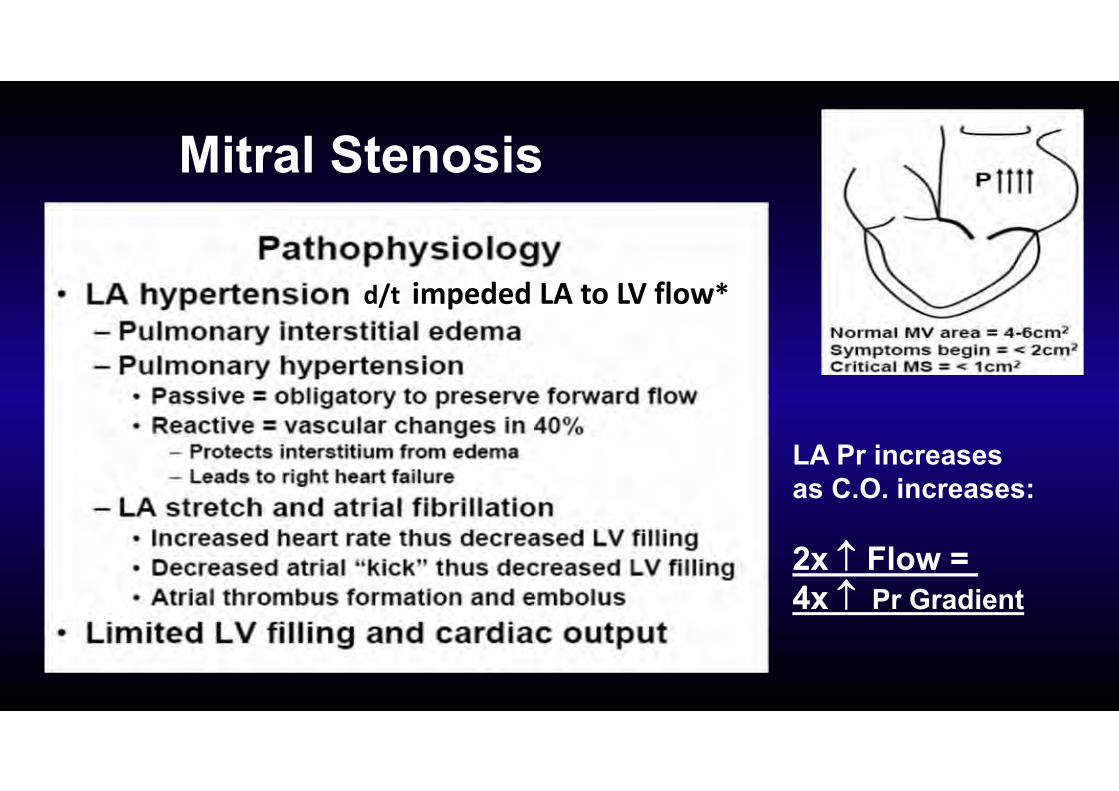
Mitral Stenosis
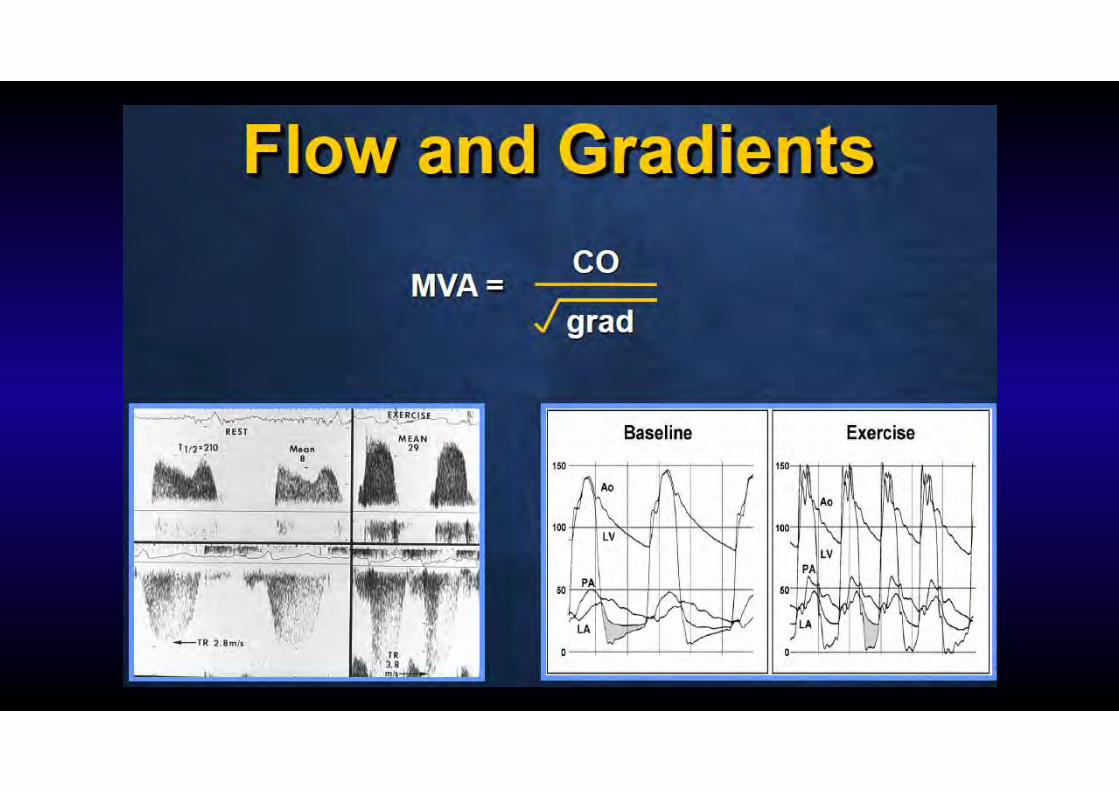
LA Pr increases as C.O. increases:
2x Flow = 4x Pr Gradient
d/t impeded LA to LV flow*
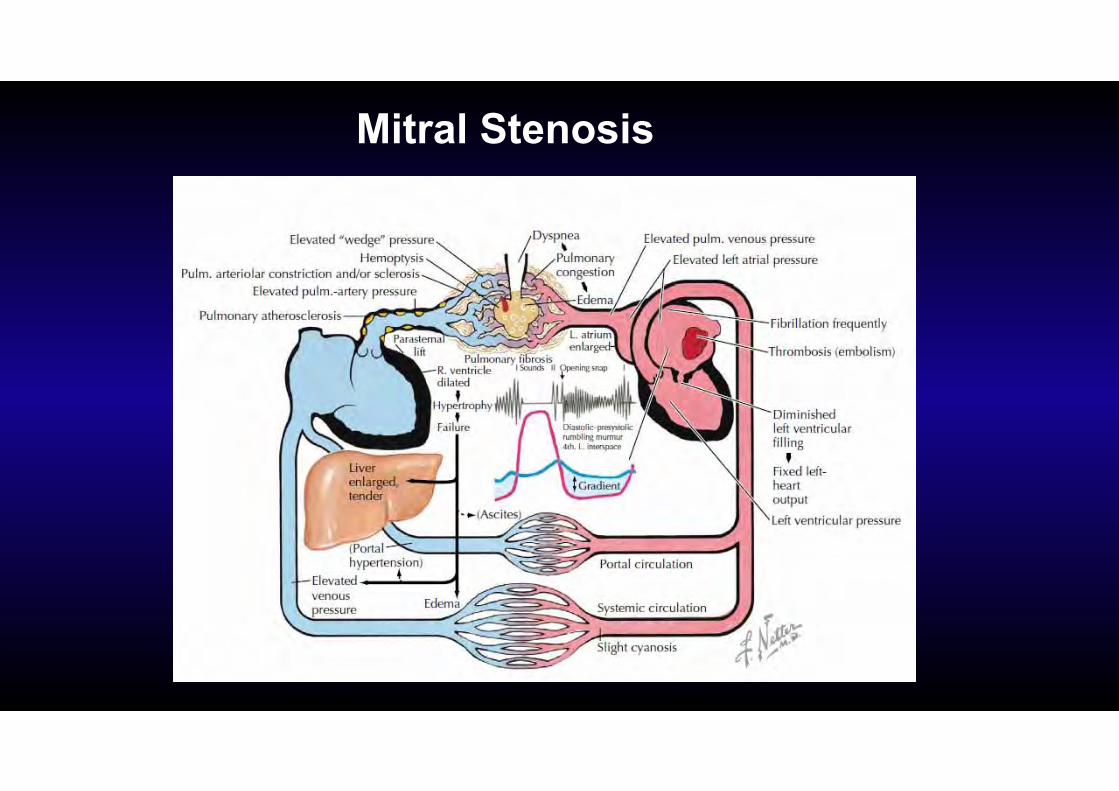
Mitral Stenosis
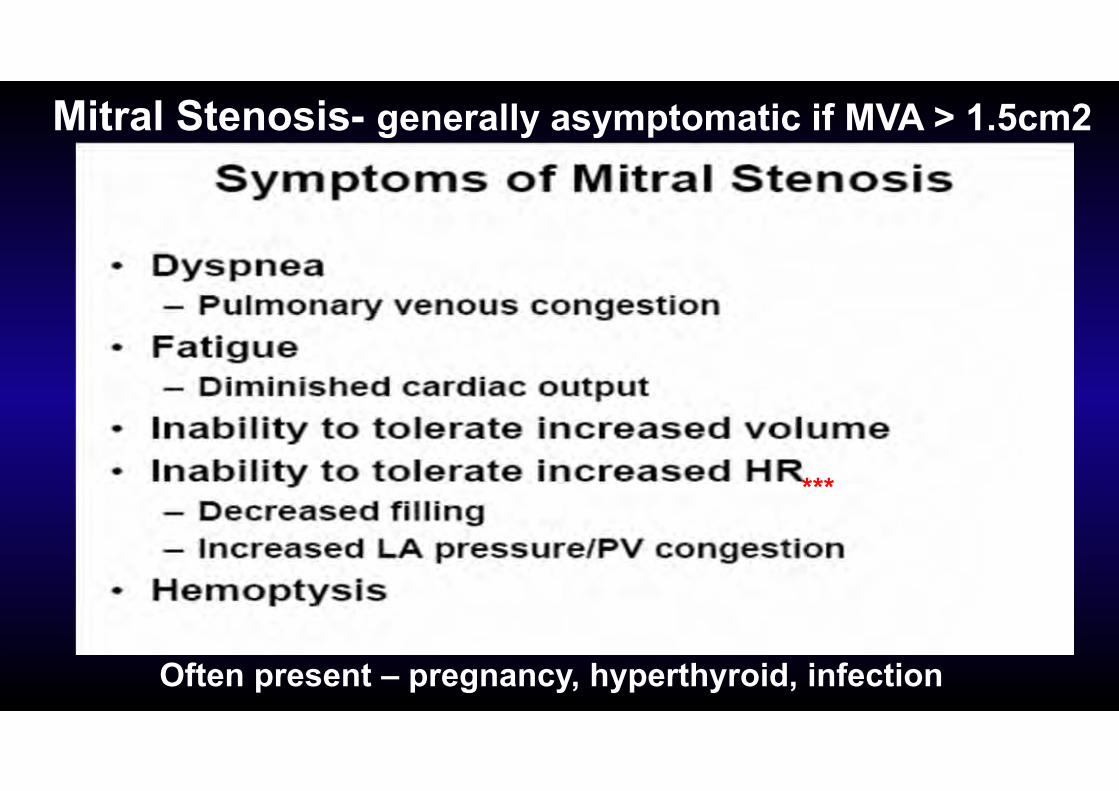
Mitral Stenosis- generally asymptomatic if MVA > 1.5cm2
Often present – pregnancy, hyperthyroid, infection
***

Physical Exam of Mitral Stenosis• Loud S1• Opening Snap• Diastolic Apical Rumble (murmur)• May be associated with:
• MR or AS• Right Sided Murmurs- PI – Graham Steel Murmur , or TR
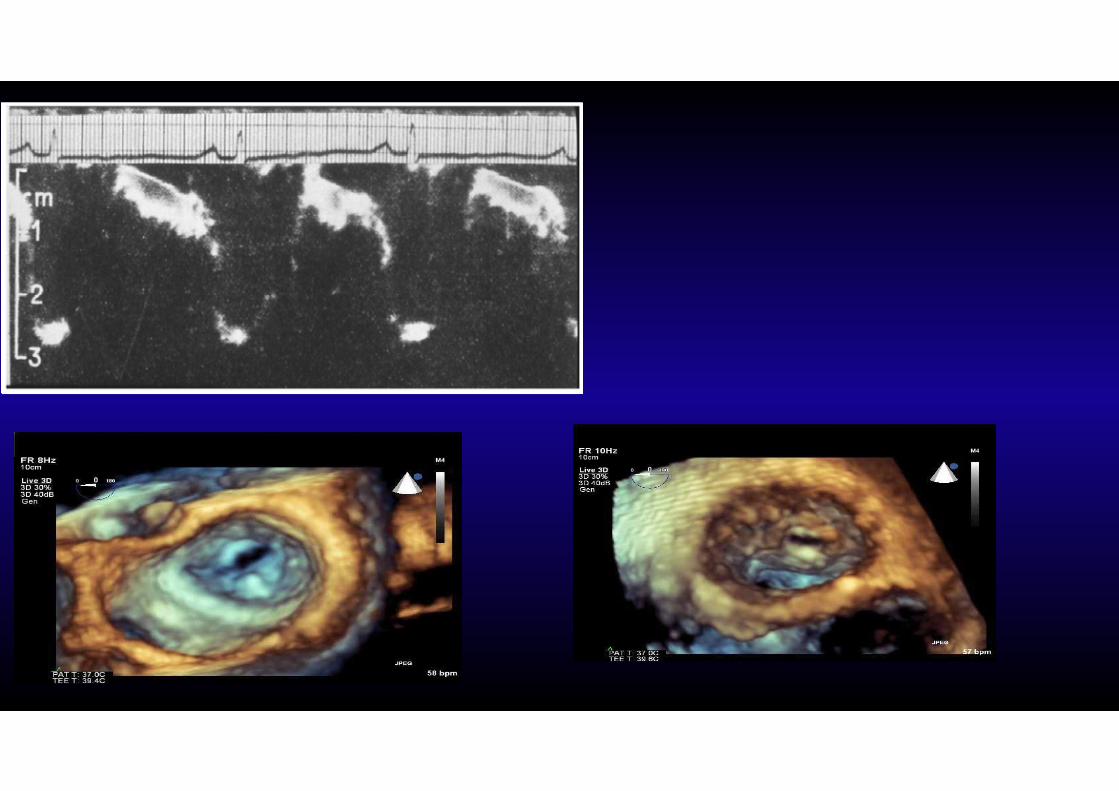
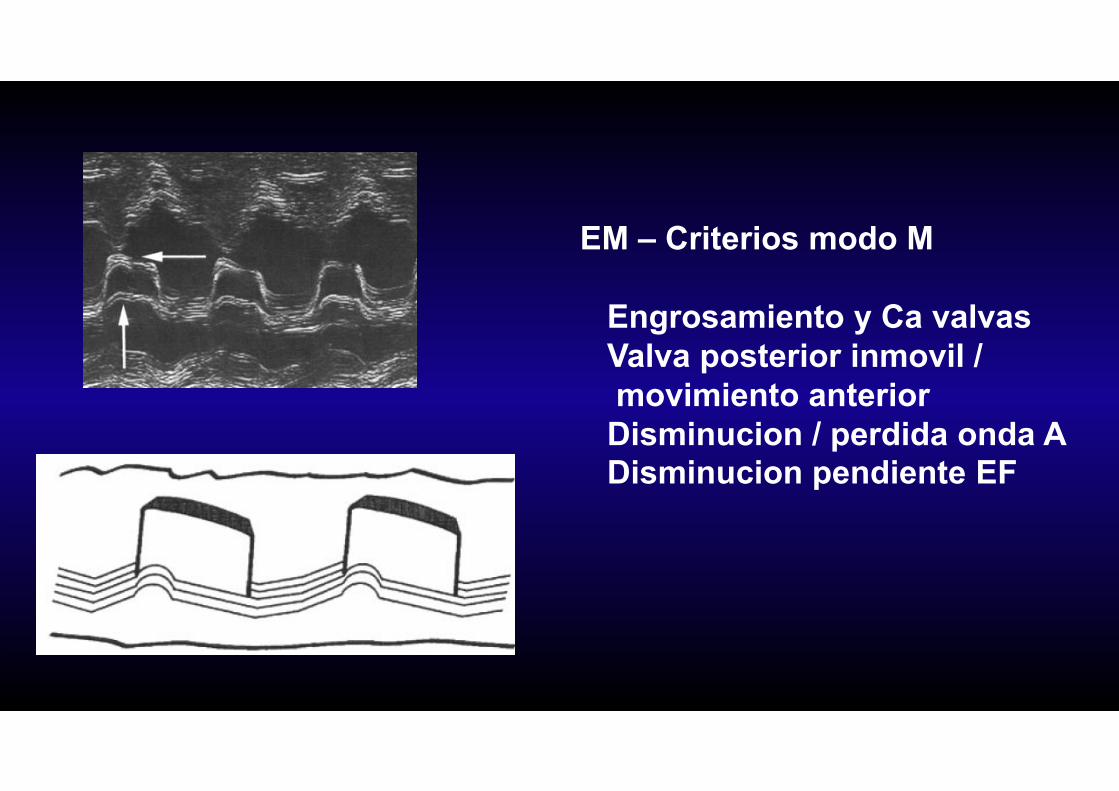
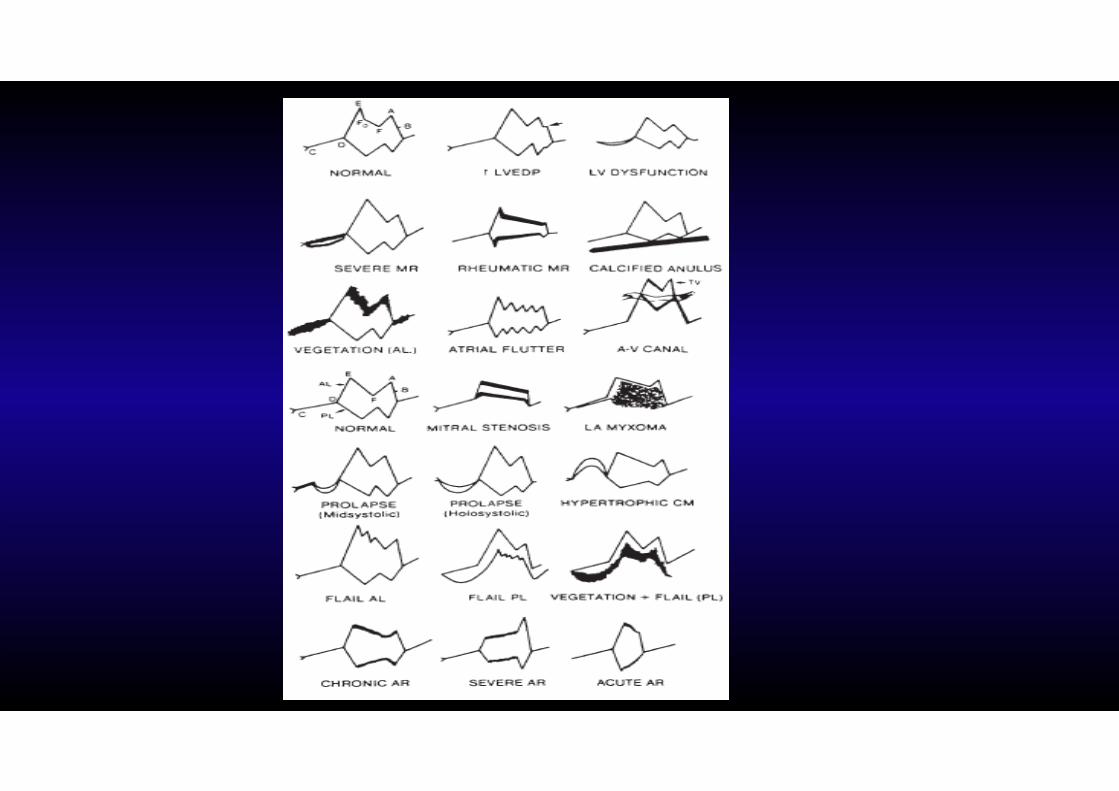
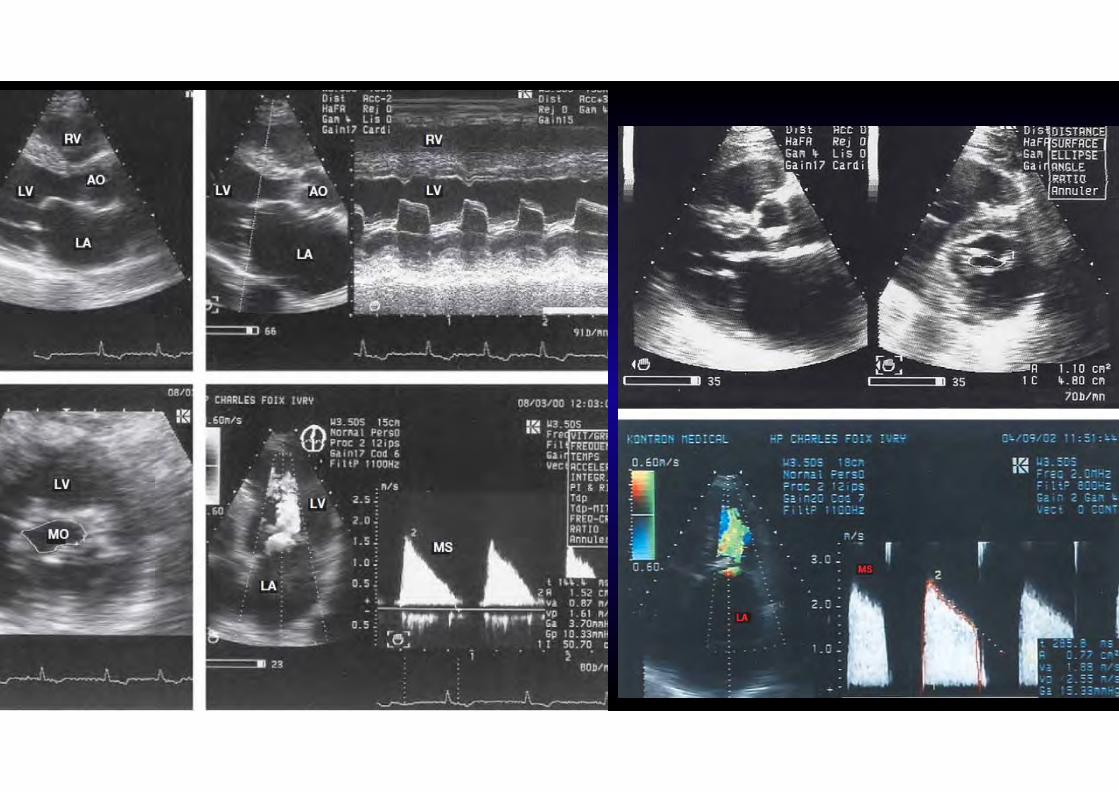
EM – Criterios modo M
Engrosamiento y Ca valvasValva posterior inmovil /movimiento anterior
Disminucion / perdida onda ADisminucion pendiente EF
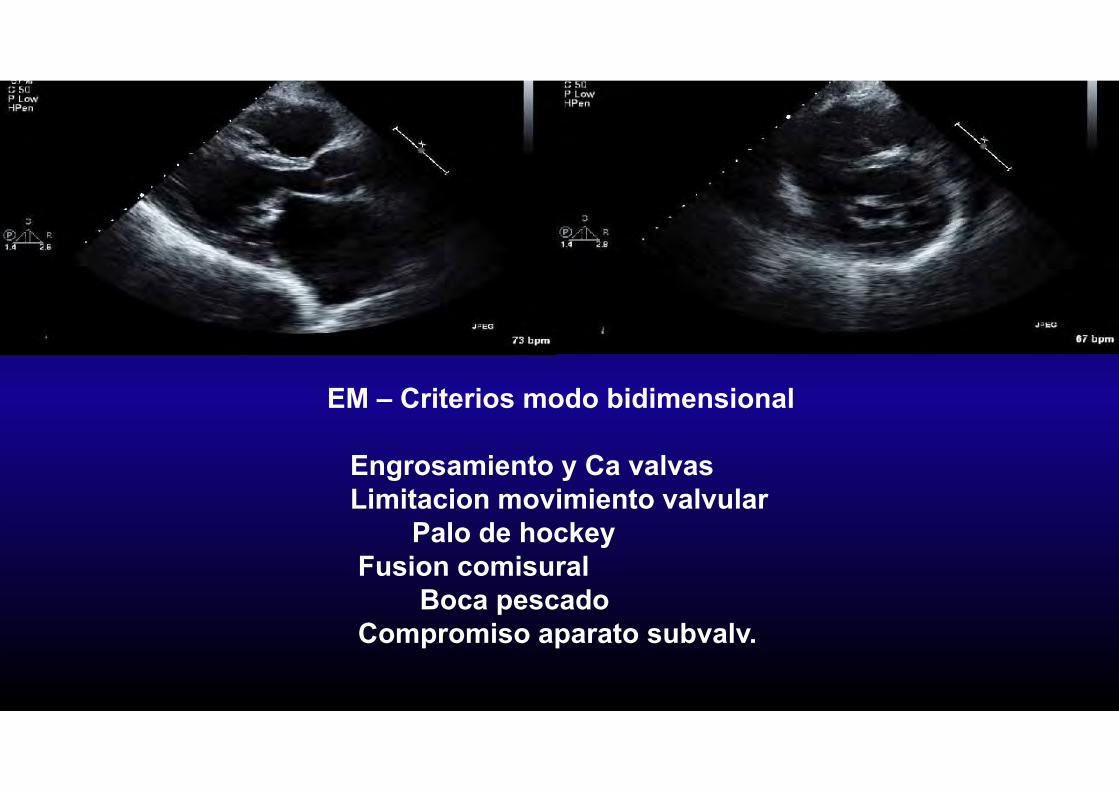
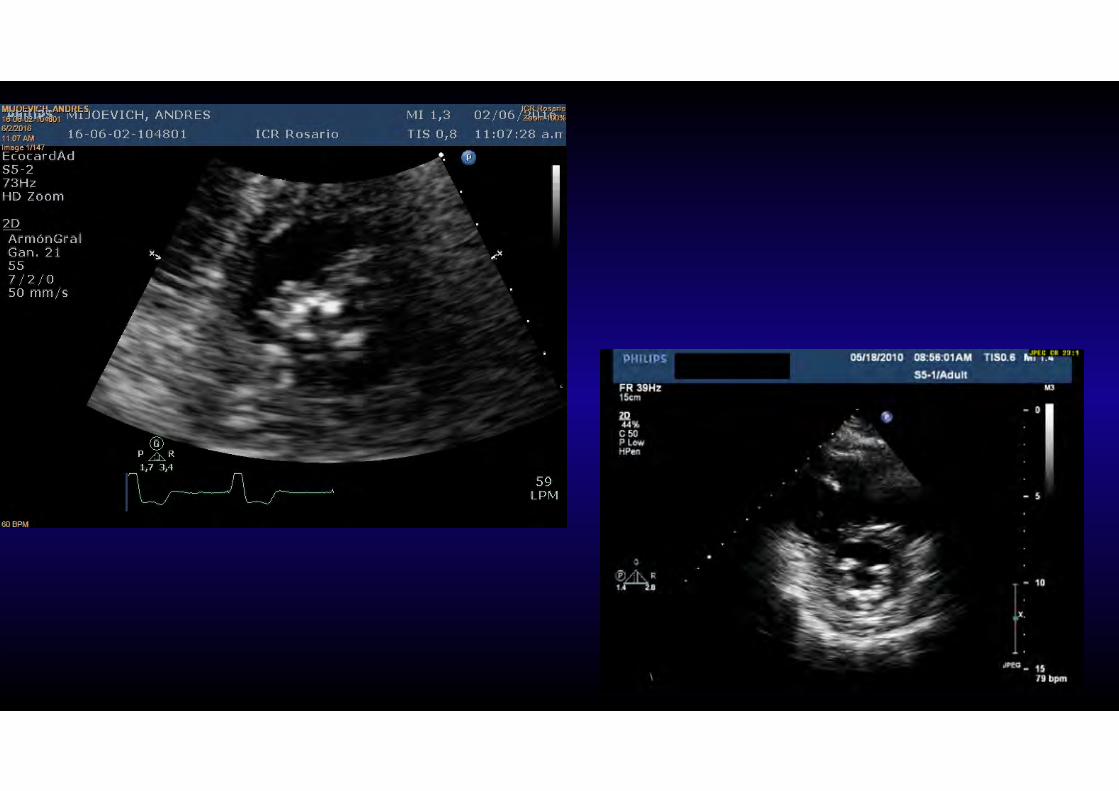
EM – Criterios modo bidimensional
Engrosamiento y Ca valvasLimitacion movimiento valvular
Palo de hockeyFusion comisural
Boca pescadoCompromiso aparato subvalv.

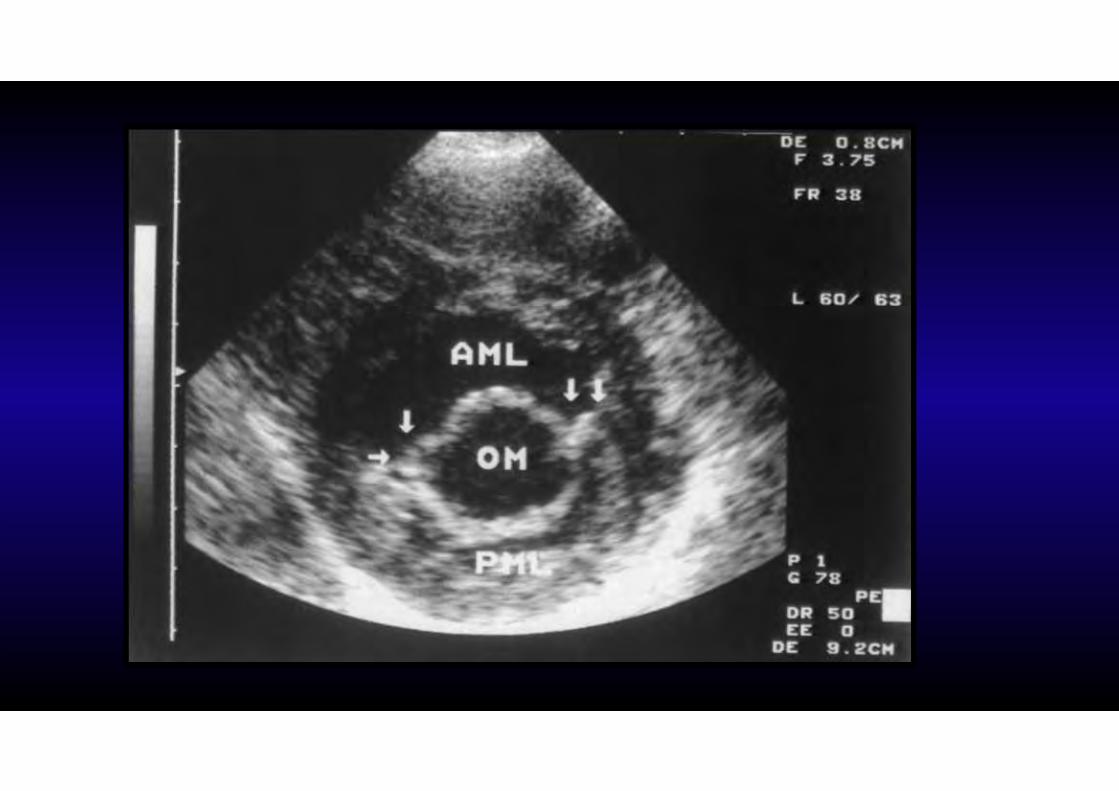
EM – Criterios modo bidimensional
Engrosamiento y Ca valvasLimitacion movimiento valvular
Palo de hockeyFusion comisural
Boca pescadoCompromiso aparato subvalv.

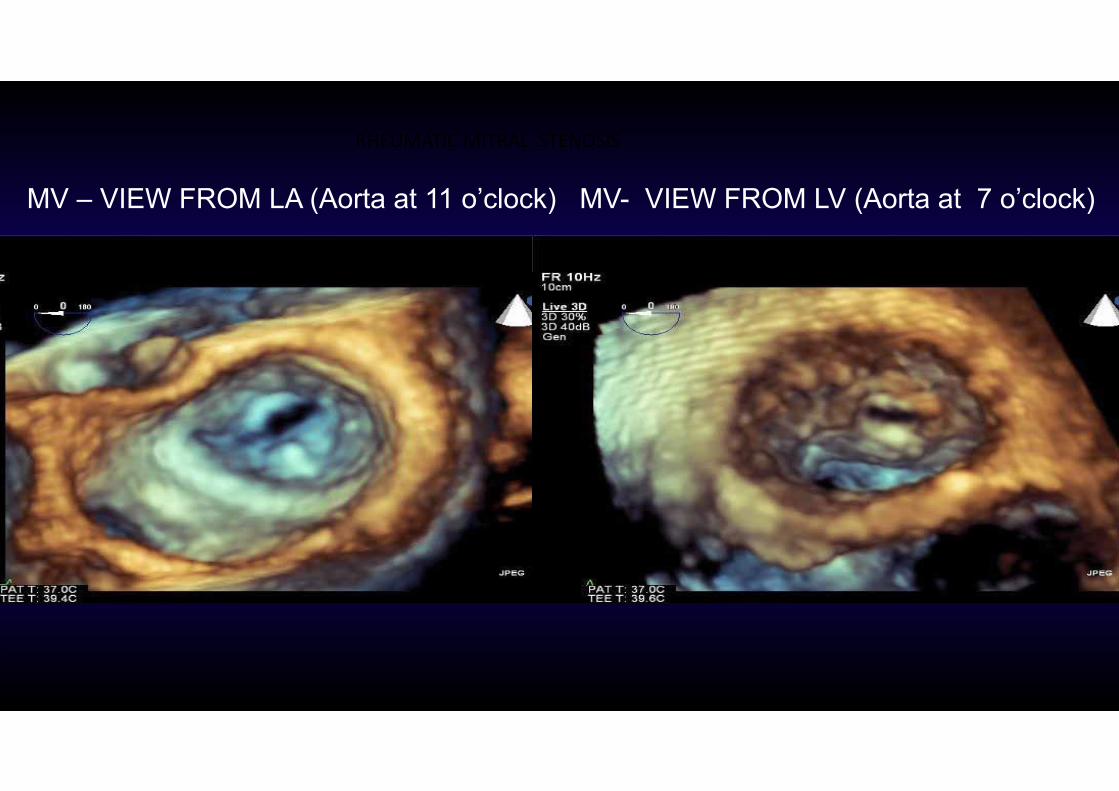
MV – VIEW FROM LA (Aorta at 11 o’clock) MV- VIEW FROM LV (Aorta at 7 o’clock)
RHEUMATIC MITRAL STENOSIS
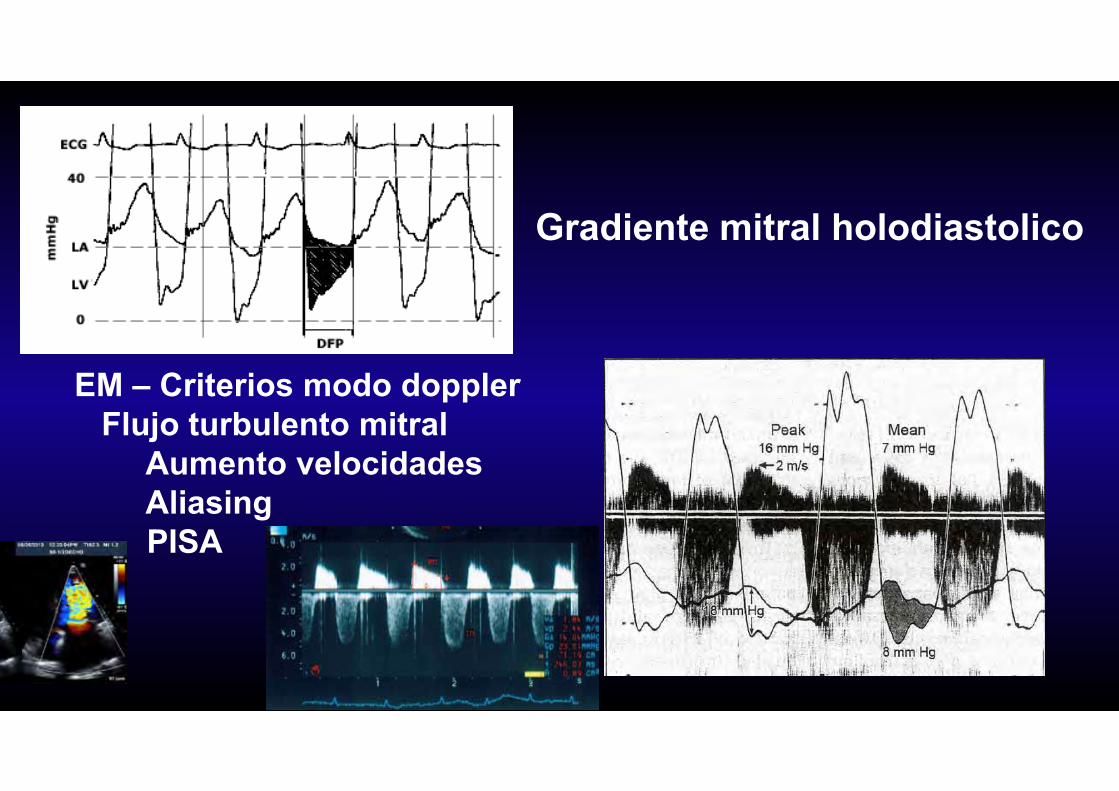
EM – Criterios modo dopplerFlujo turbulento mitral
Aumento velocidadesAliasingPISA
Gradiente mitral holodiastolico
Echo-Doppler Assessment of MS Severity
• MV area by planimetry*- 2D or 3D• Diastolic MV Pressure ½ time*• Continuity equation• PISA• Mean Gradient*• PA pressure
*Most common
Most accurate method is Direct LA & LV pressure measurement but
Echo- Doppler BETTER than PCWP- LV pressure gradient d/t delay in PCWP
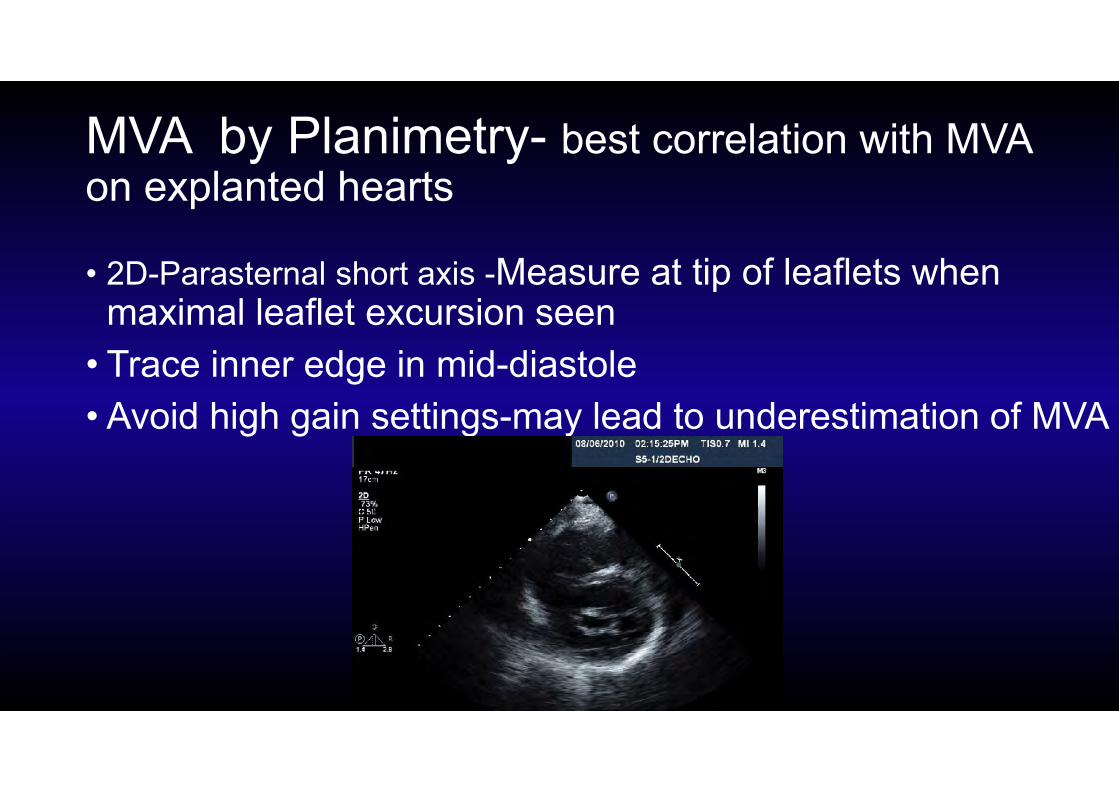
MVA by Planimetry- best correlation with MVA on explanted hearts
• 2D-Parasternal short axis -Measure at tip of leaflets when maximal leaflet excursion seen
• Trace inner edge in mid-diastole• Avoid high gain settings-may lead to underestimation of MVA
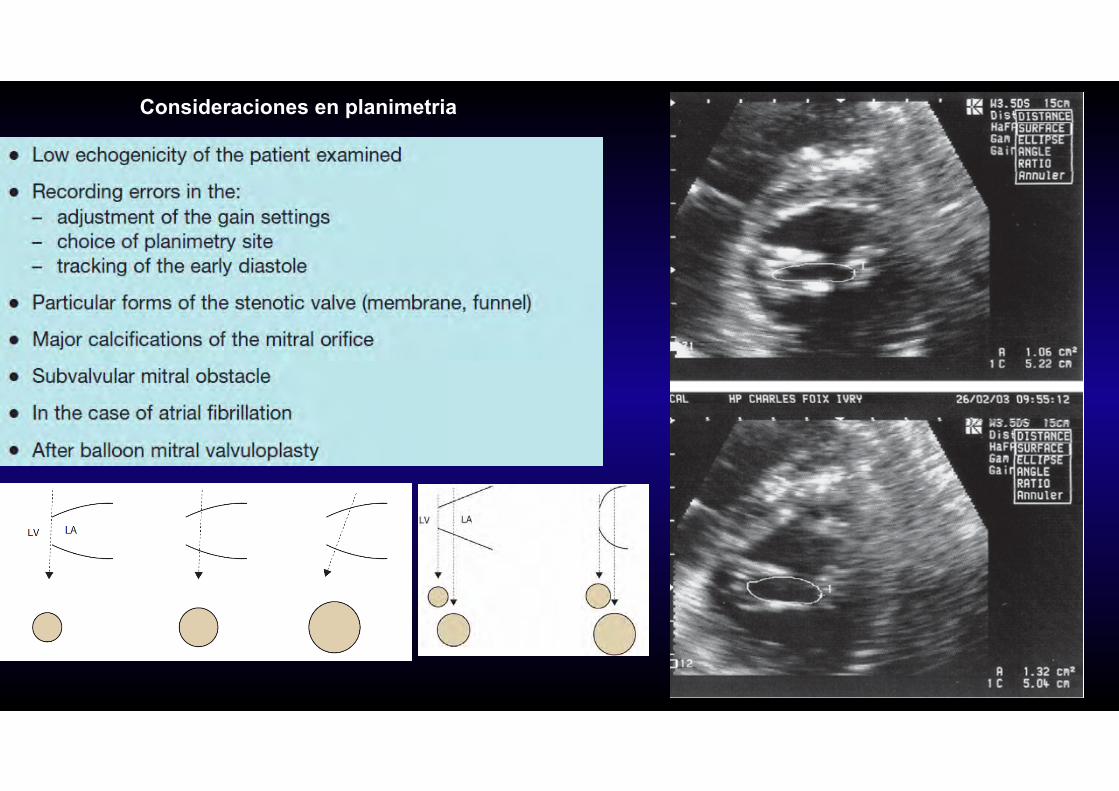
Consideraciones en planimetria
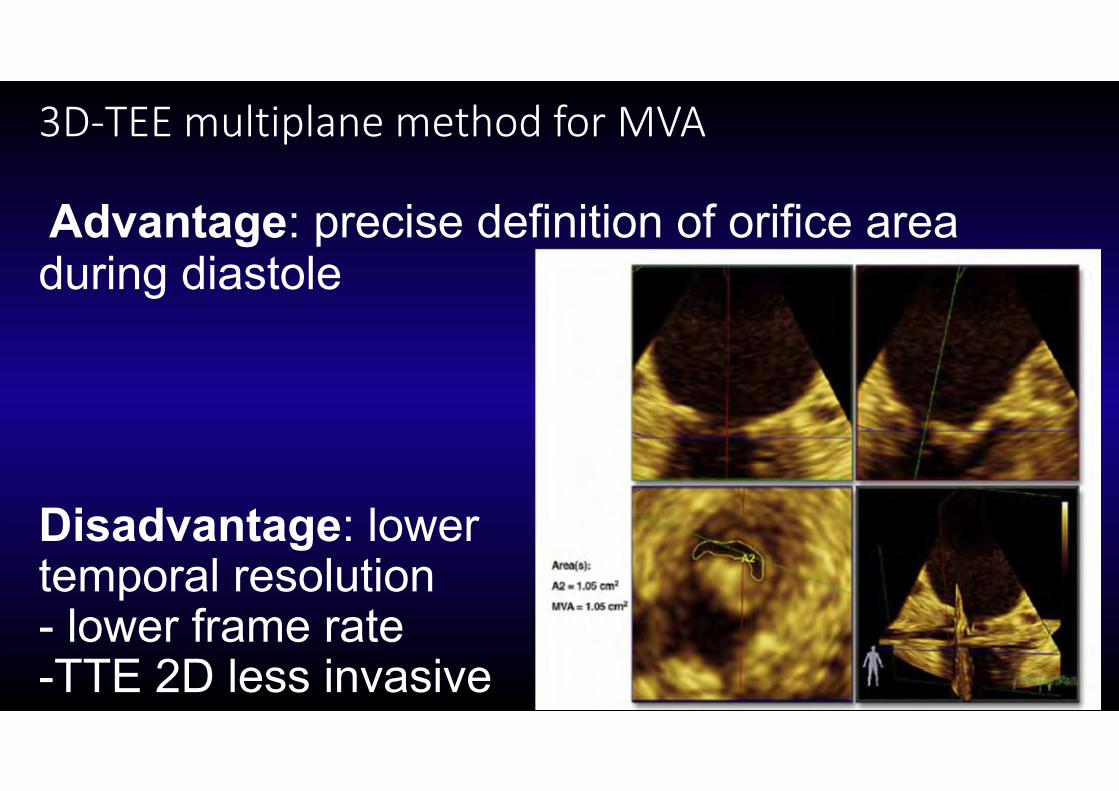
3D‐TEE multiplane method for MVA
Advantage: precise definition of orifice area during diastole
Disadvantage: lowertemporal resolution- lower frame rate-TTE 2D less invasive
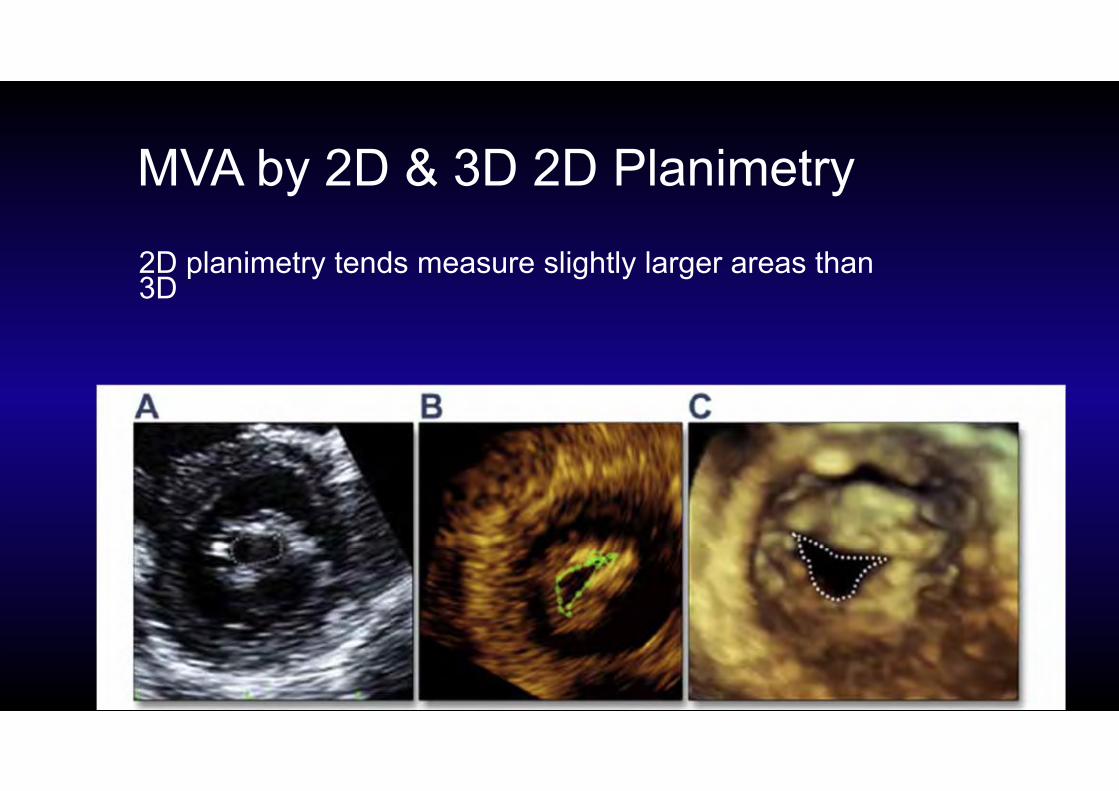
MVA by 2D & 3D 2D Planimetry2D planimetry tends measure slightly larger areas than 3D
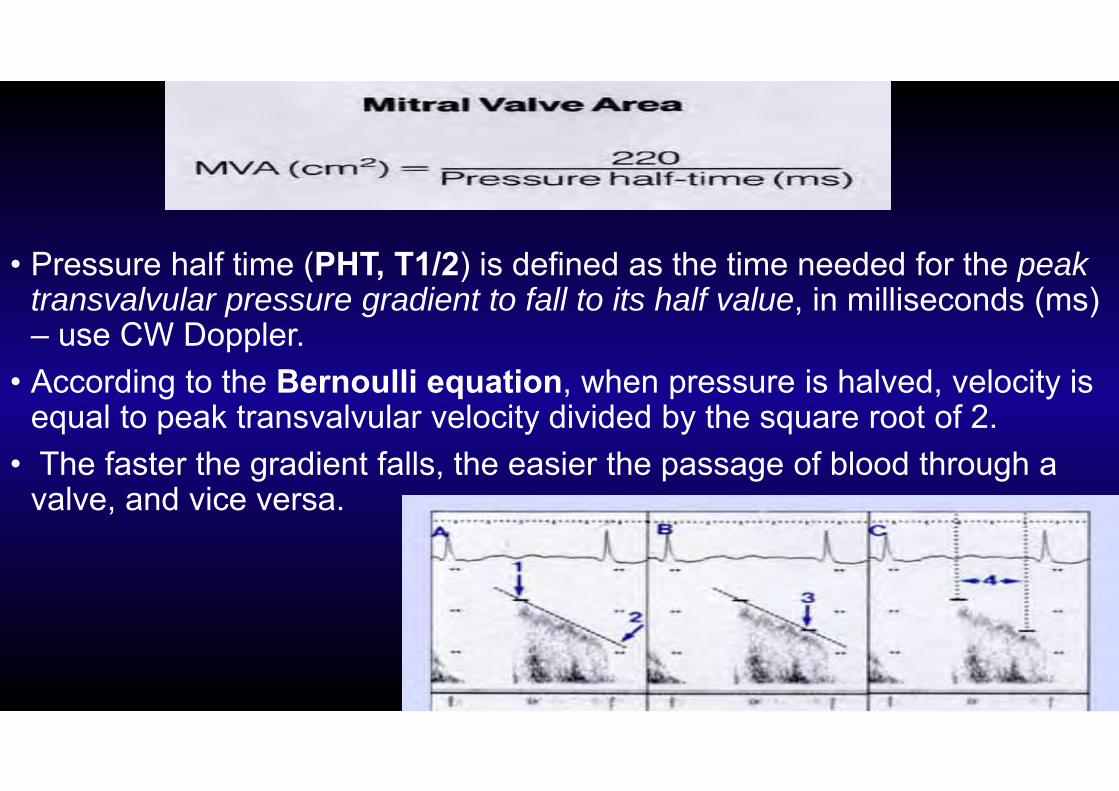
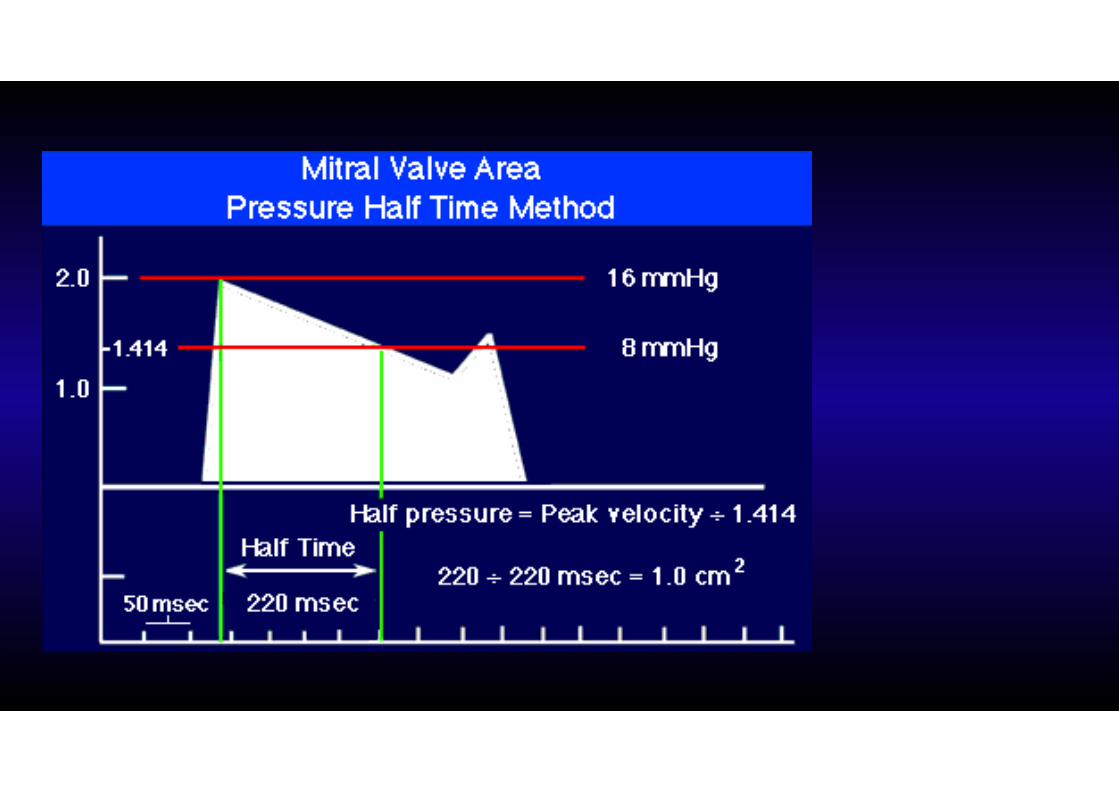
• Pressure half time (PHT, T1/2) is defined as the time needed for the peak transvalvular pressure gradient to fall to its half value, in milliseconds (ms) – use CW Doppler.
• According to the Bernoulli equation, when pressure is halved, velocity is equal to peak transvalvular velocity divided by the square root of 2.
• The faster the gradient falls, the easier the passage of blood through a valve, and vice versa.
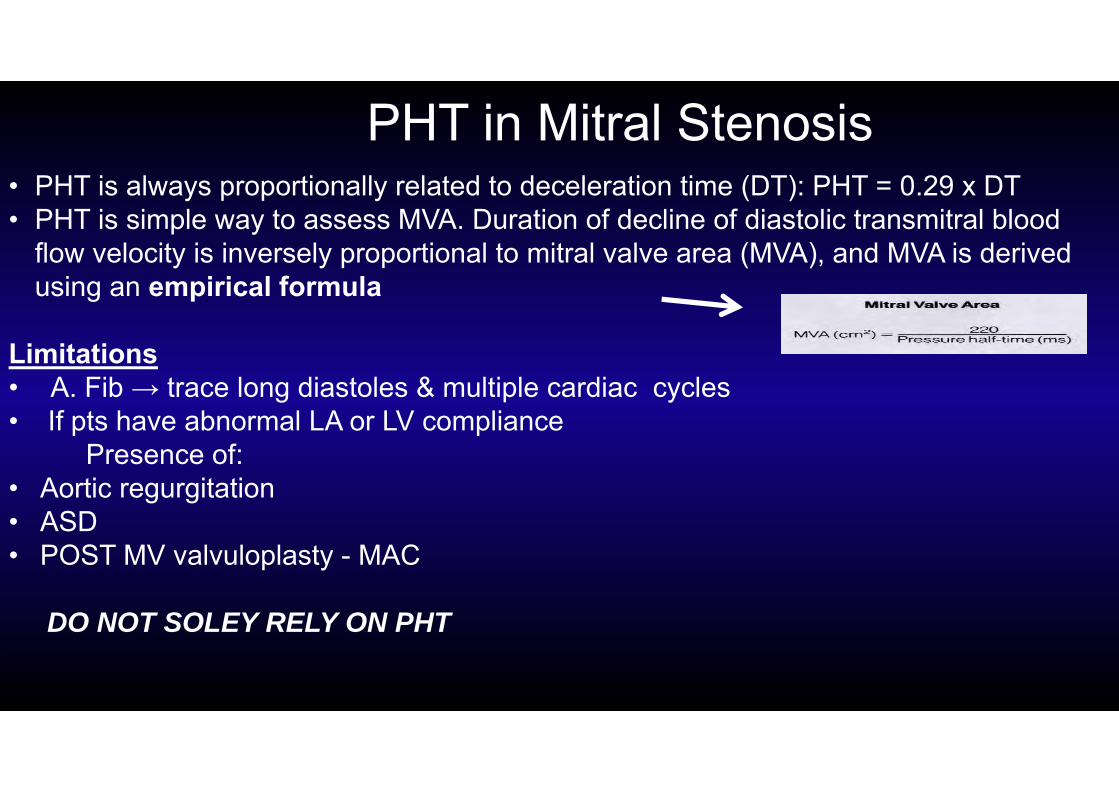
• PHT is always proportionally related to deceleration time (DT): PHT = 0.29 x DT• PHT is simple way to assess MVA. Duration of decline of diastolic transmitral blood
flow velocity is inversely proportional to mitral valve area (MVA), and MVA is derived using an empirical formula
Limitations• A. Fib → trace long diastoles & multiple cardiac cycles • If pts have abnormal LA or LV compliance
Presence of: • Aortic regurgitation • ASD• POST MV valvuloplasty - MAC
DO NOT SOLEY RELY ON PHT
PHT in Mitral Stenosis
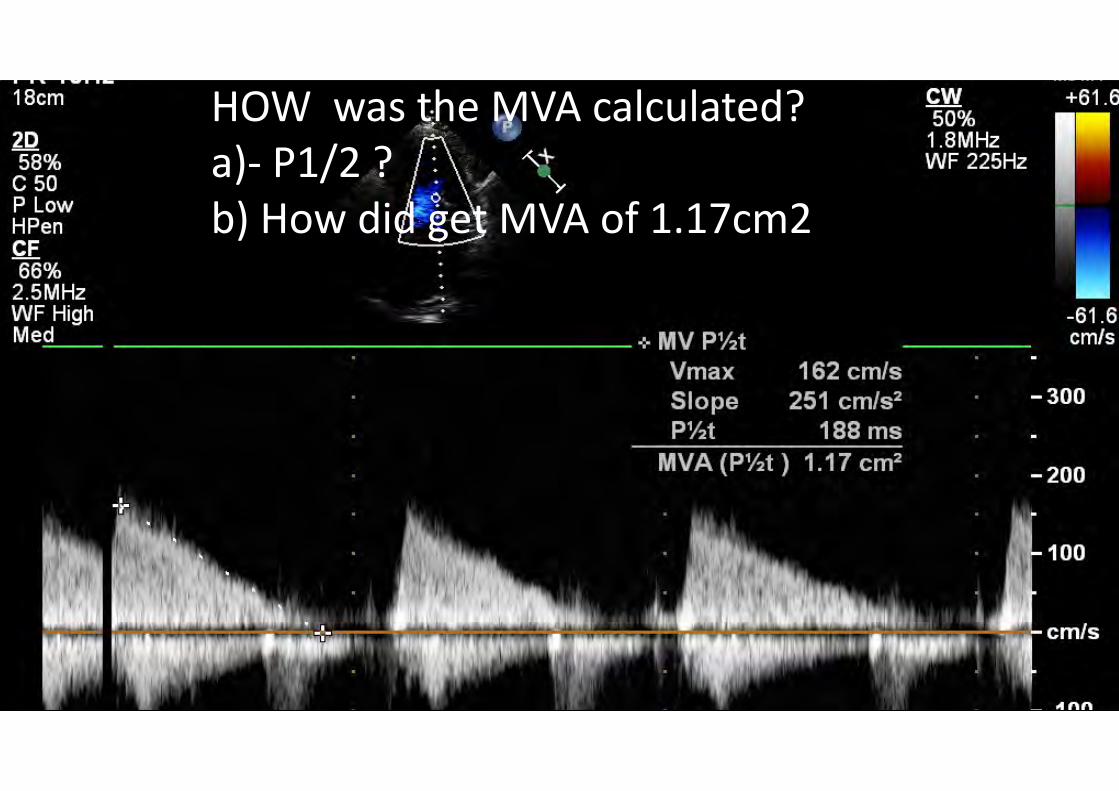
HOW was the MVA calculated?a)‐ P1/2 ?b) How did get MVA of 1.17cm2
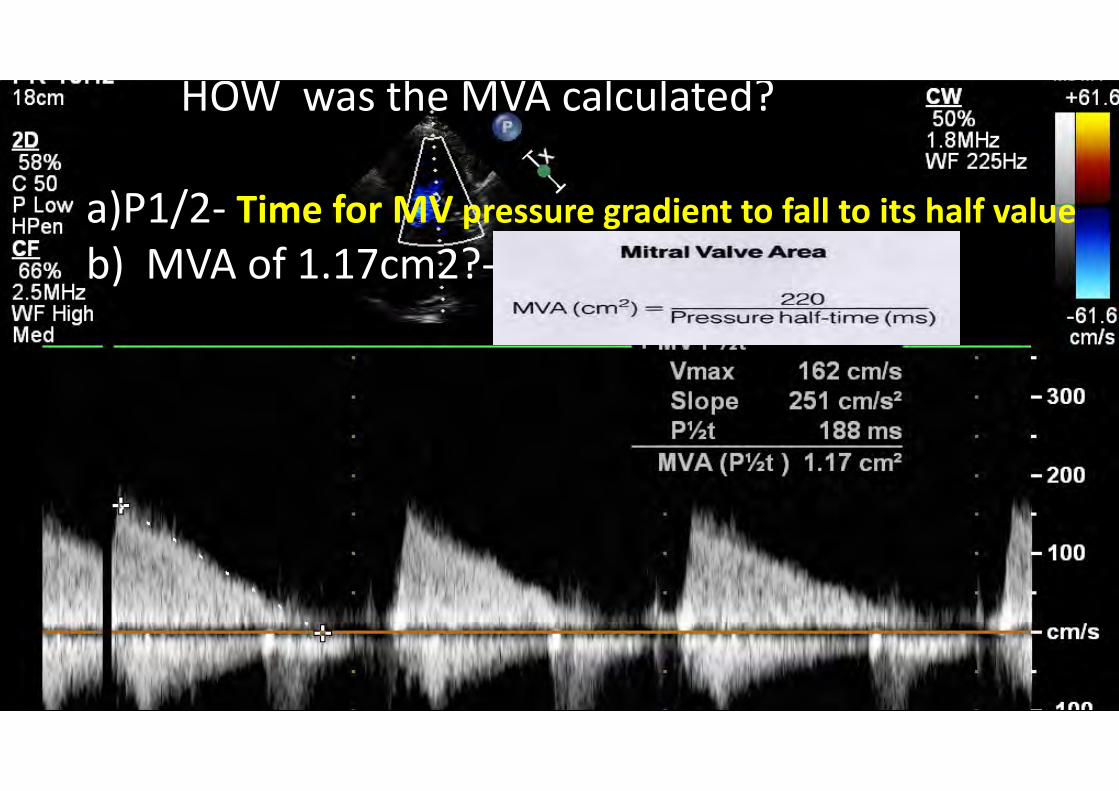
HOW was the MVA calculated?
a)P1/2‐ Time for MV pressure gradient to fall to its half valueb) MVA of 1.17cm2?‐
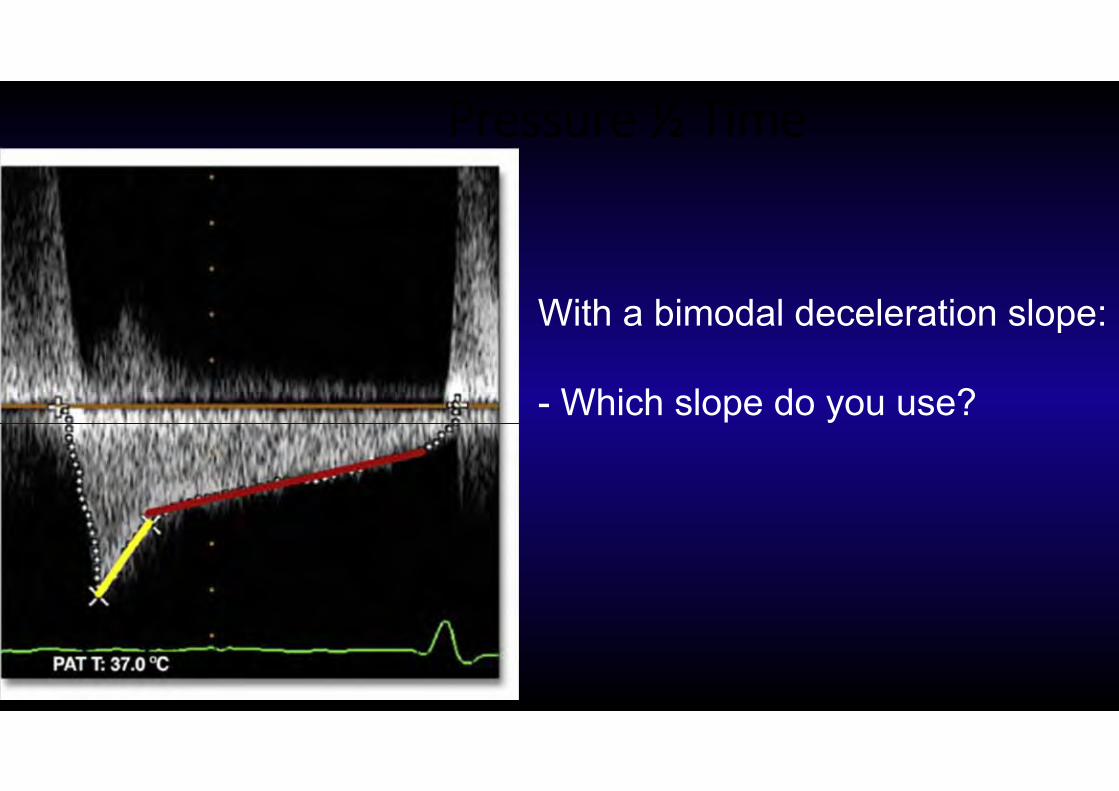
Pressure ½ Time
With a bimodal deceleration slope:
- Which slope do you use?
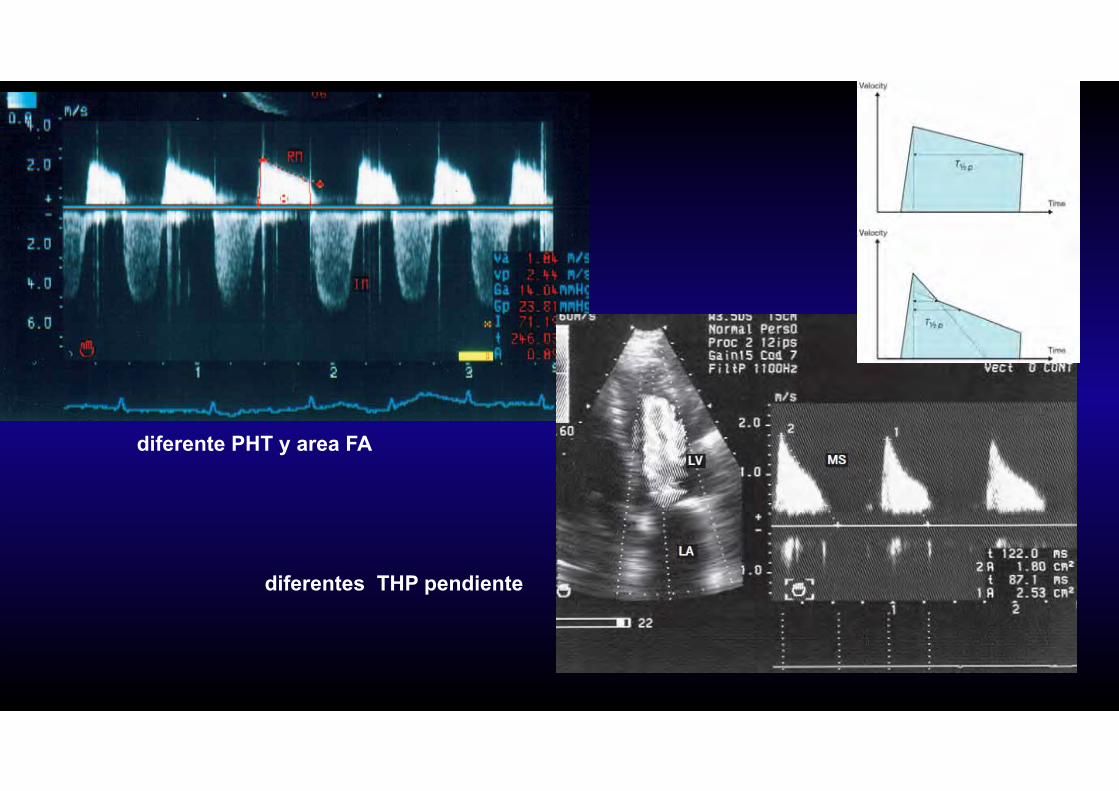
diferente PHT y area FA
diferentes THP pendiente
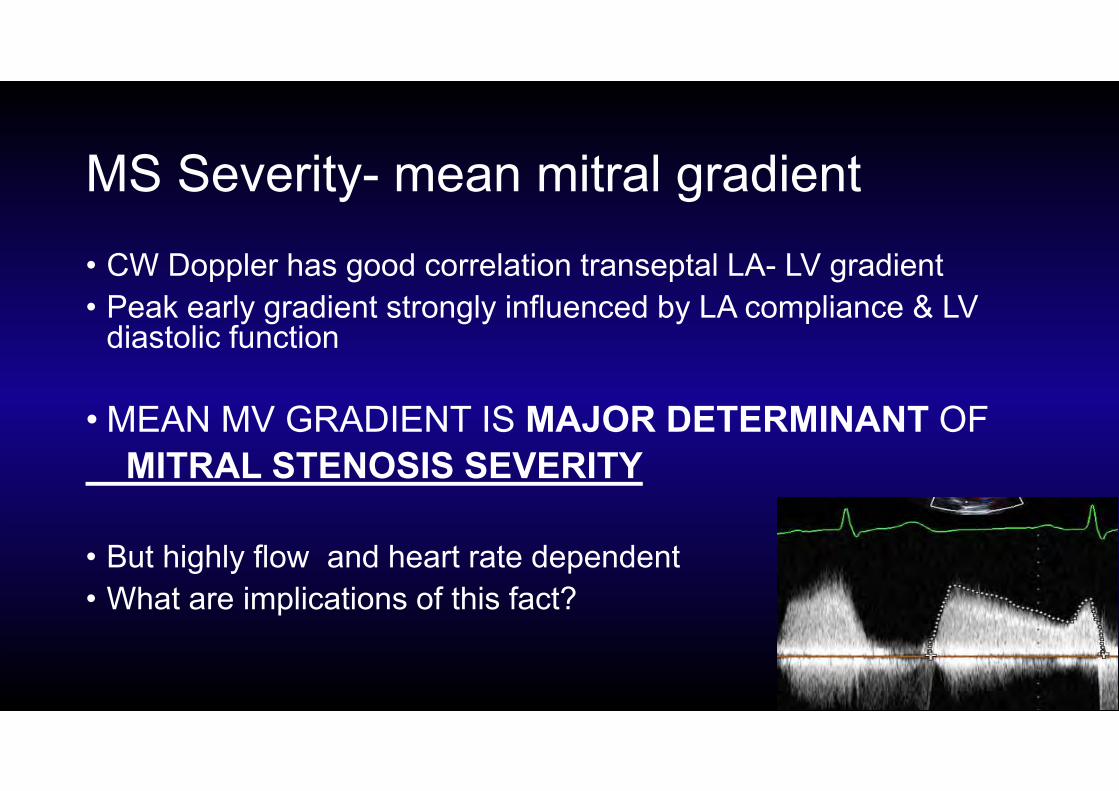
MS Severity- mean mitral gradient• CW Doppler has good correlation transeptal LA- LV gradient• Peak early gradient strongly influenced by LA compliance & LV
diastolic function
• MEAN MV GRADIENT IS MAJOR DETERMINANT OF MITRAL STENOSIS SEVERITY
• But highly flow and heart rate dependent• What are implications of this fact?
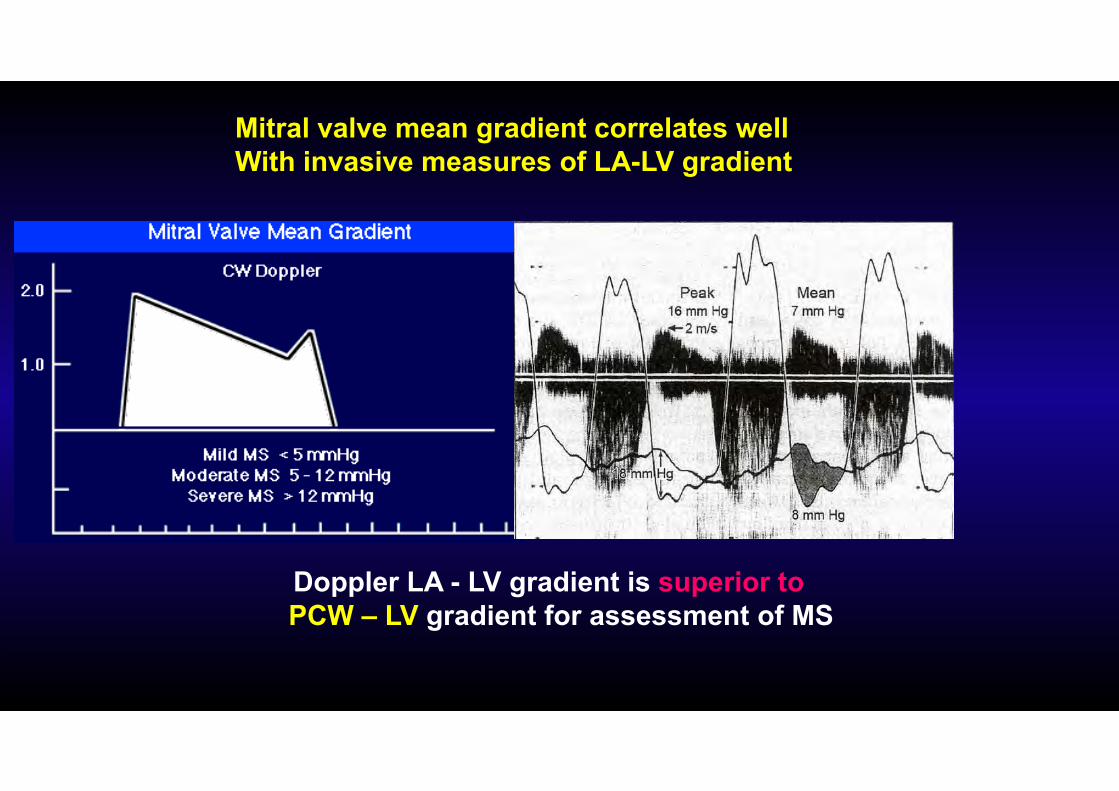
Doppler LA - LV gradient is superior to PCW – LV gradient for assessment of MS
Mitral valve mean gradient correlates wellWith invasive measures of LA-LV gradient
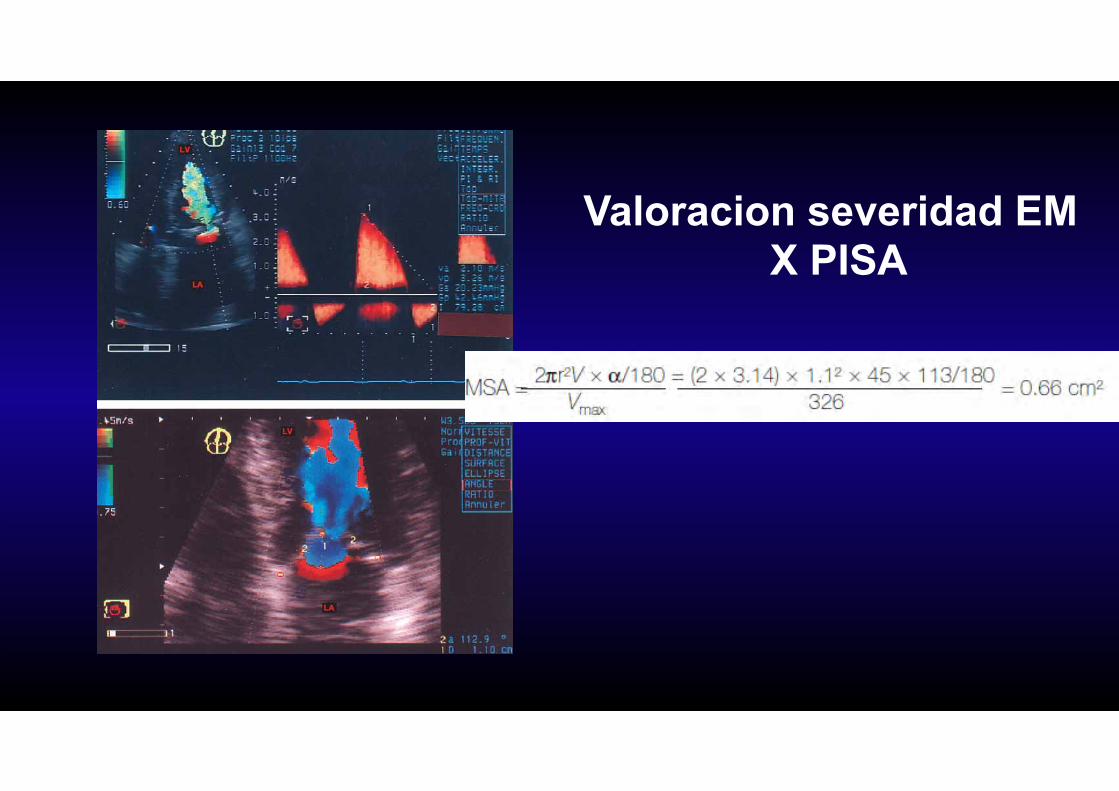
Valoracion severidad EM X PISA
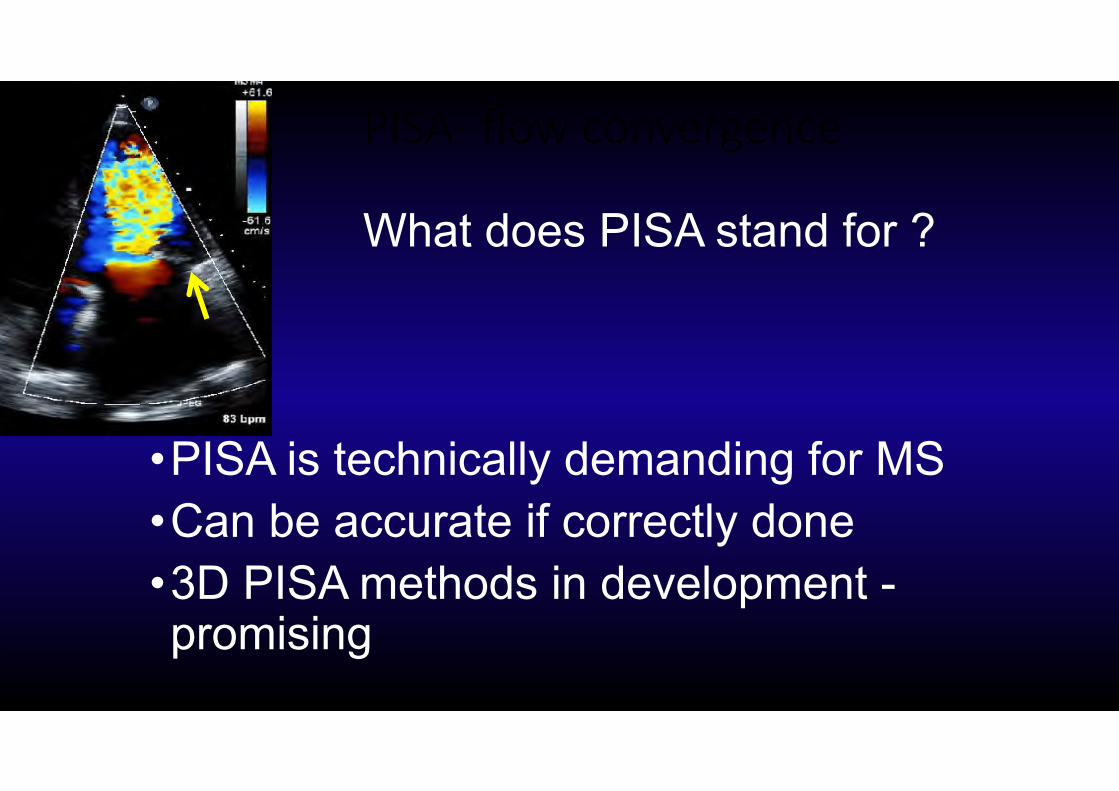
PISA‐ flow convergence
What does PISA stand for ?
•PISA is technically demanding for MS•Can be accurate if correctly done•3D PISA methods in development -promising
MVA by continuity ecuation
Assume diastolic MV flow = aortic stroke volume = Pulm.SV
MVA = pi ( D2/4 ) ( VTI aorta cm ) / ( VTI mitral cm )D= LVOT diameter
Limited accuracy and reproducibility due to # of measurements
If > mild MR or AR not valid
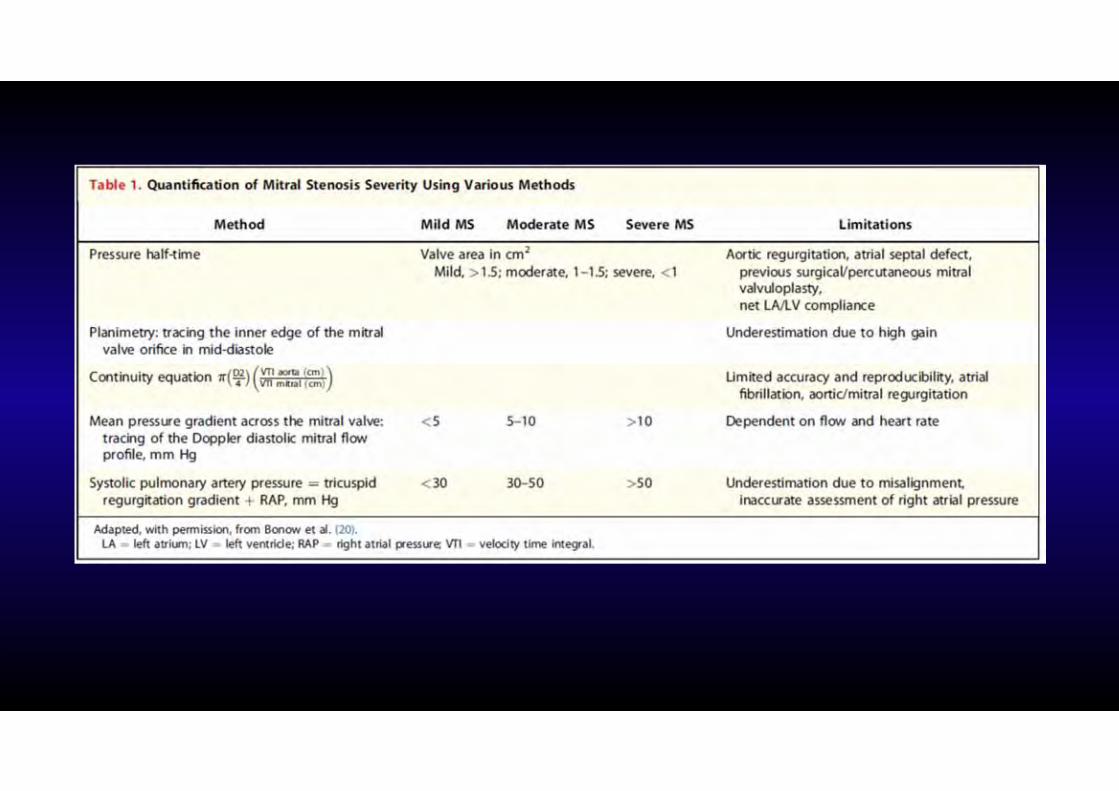
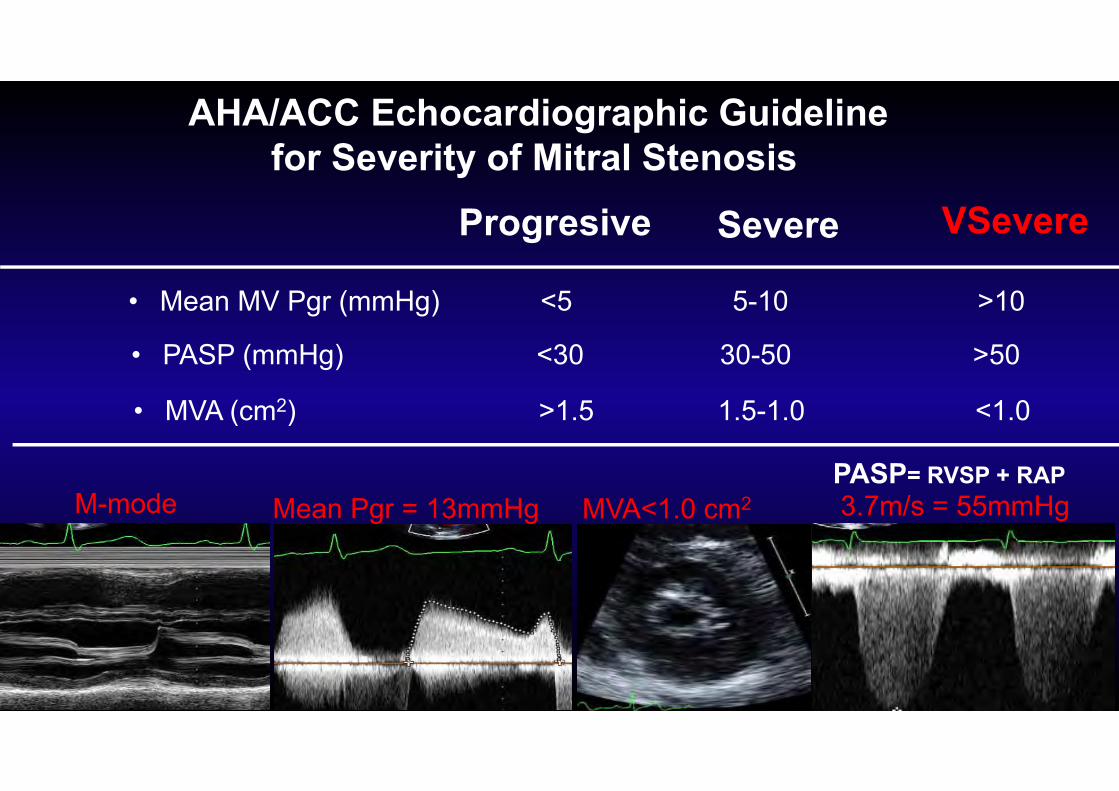
AHA/ACC Echocardiographic Guideline for Severity of Mitral Stenosis
• Mean MV Pgr (mmHg) <5 5-10 >10
• PASP (mmHg) <30 30-50 >50
• MVA (cm2) >1.5 1.5-1.0 <1.0
Progresive Severe VSevere
3.7m/s = 55mmHgMVA<1.0 cm2Mean Pgr = 13mmHgM-modePASP= RVSP + RAP
Mitral stenosisMechanical correction
PMV‐ CHS‐ OHS‐ Prosthesis
Mobility
Commisuralfussion
Calcification
Subvalvularinvolment
Less symt. More symt.
ValvulopatiaEtiologiareumatica2 valvulas
lesion predominanteEMSeveridad
RepercusionDilatacion AI y ADDilatacion VDMov. Anormal septum IA/IVHTP
ComplicacionEI2 valvulasperforacion y fistula
Pronostico
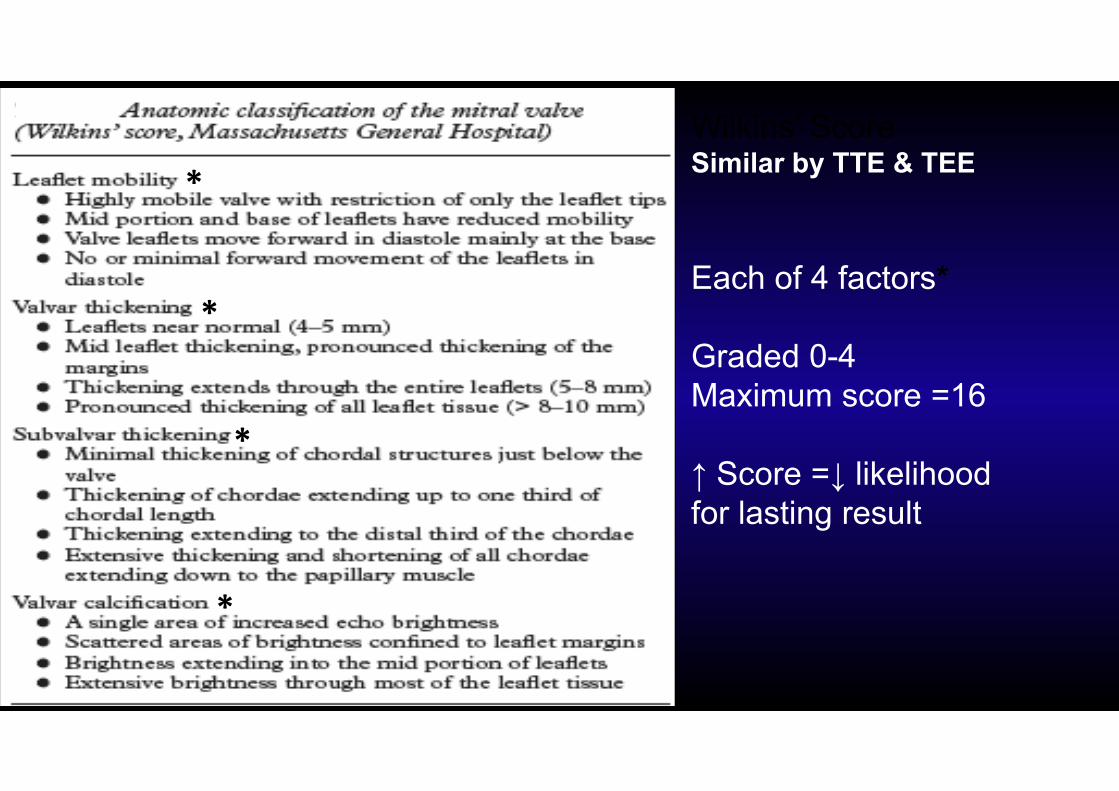
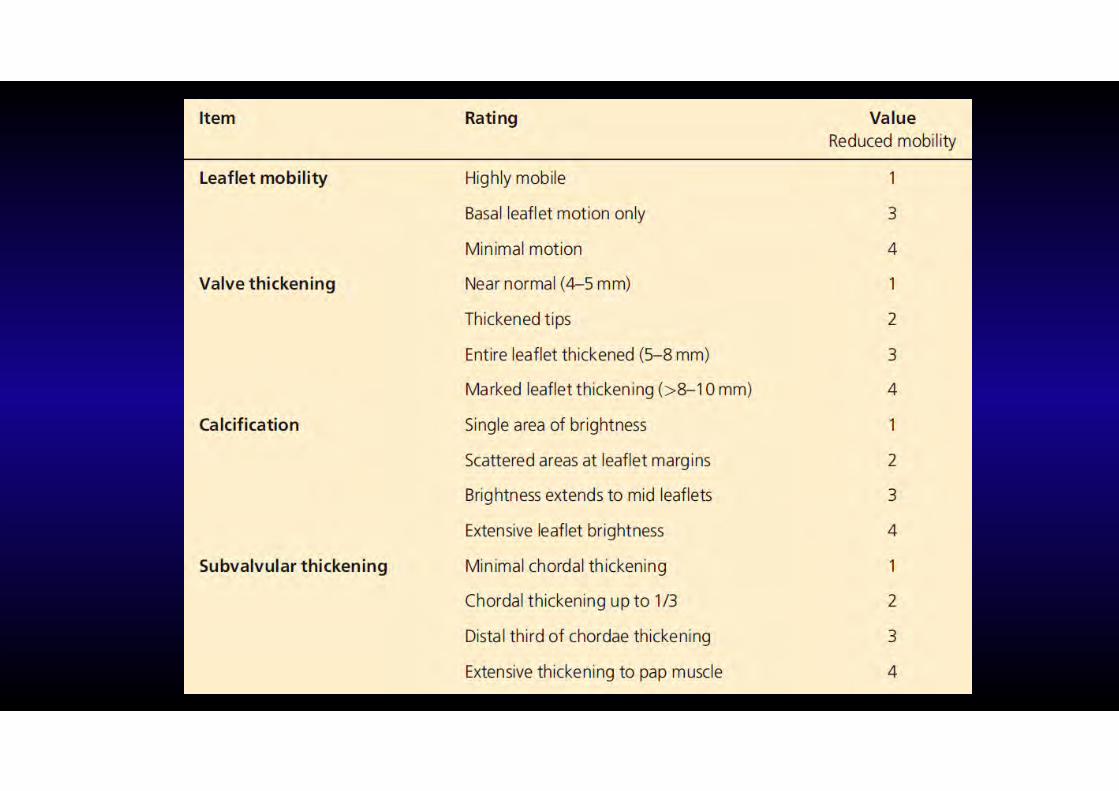
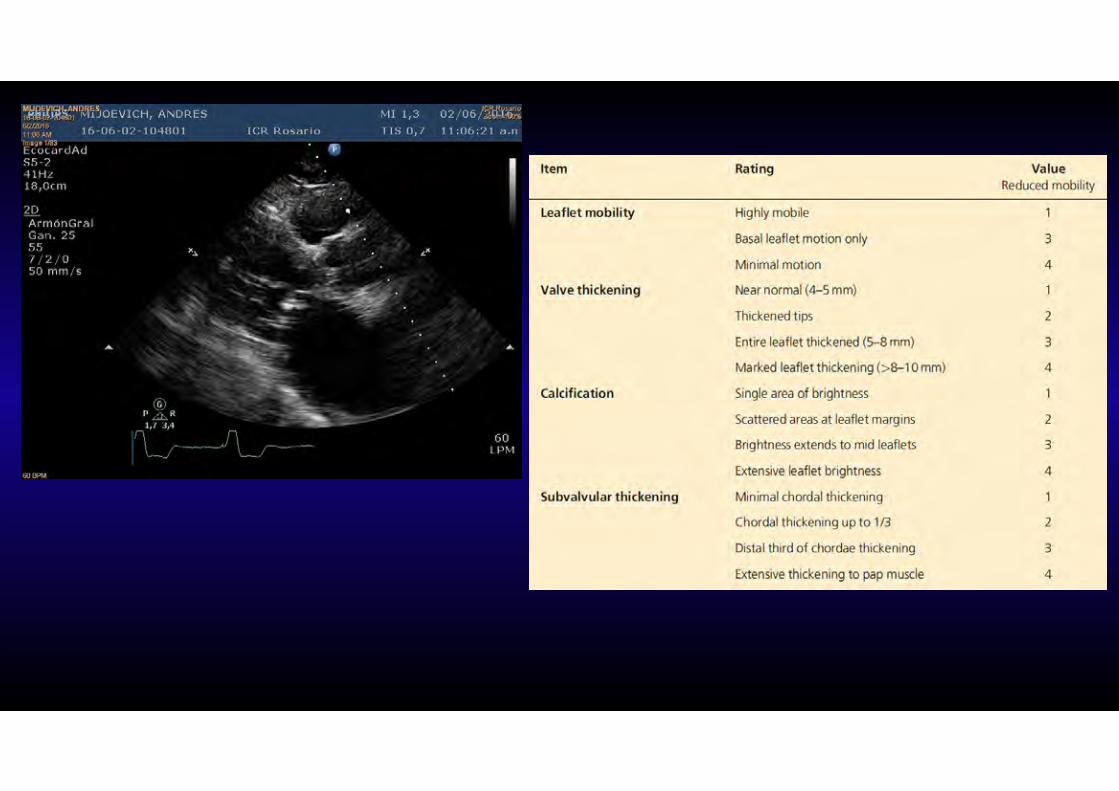
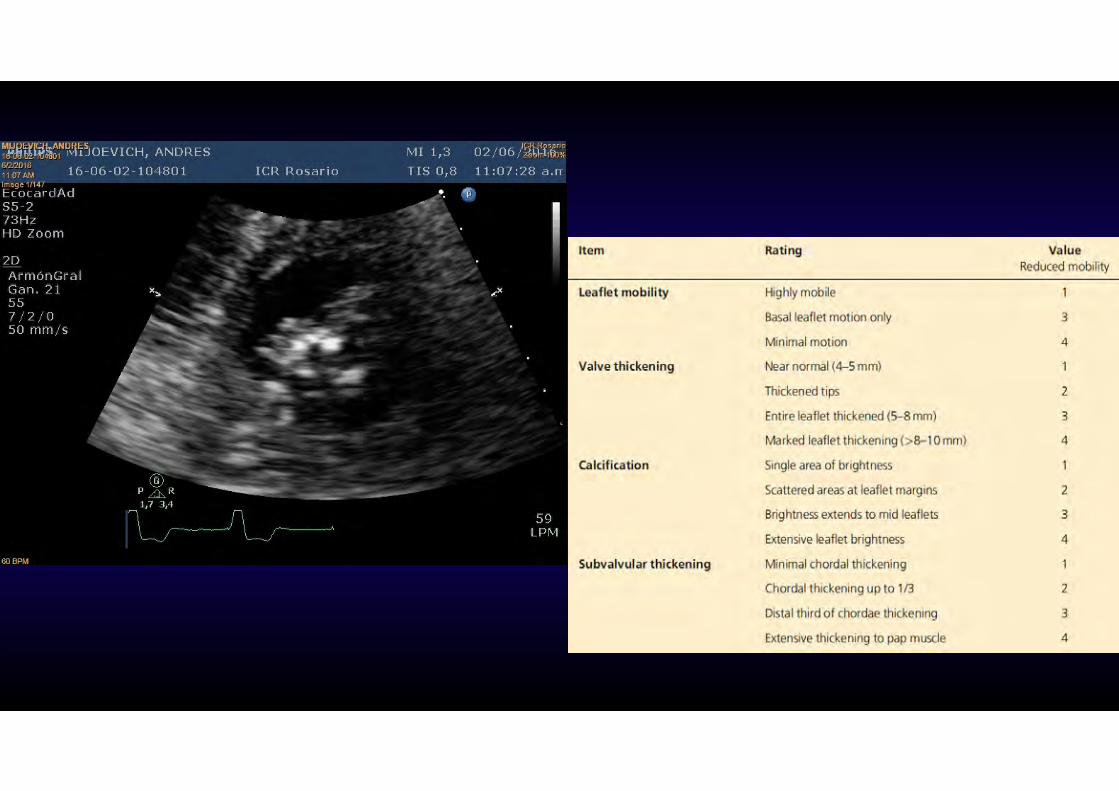
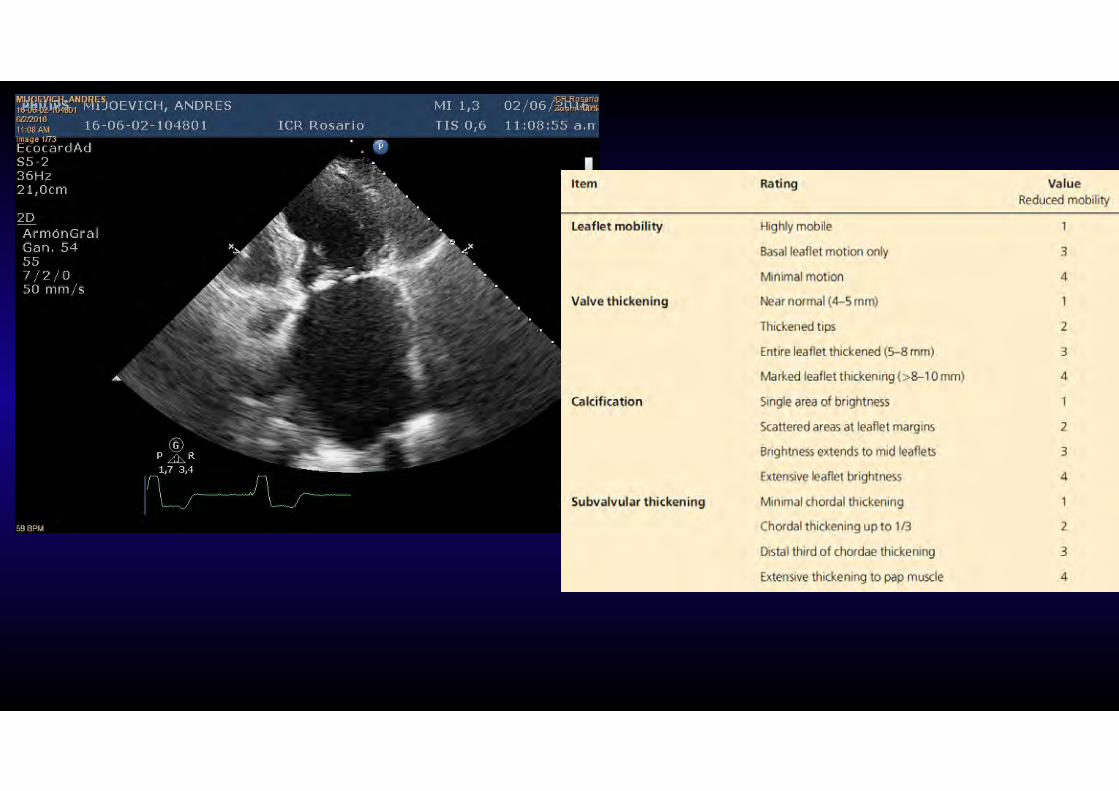
Wilkins’ ScoreSimilar by TTE & TEE
Each of 4 factors*
Graded 0-4Maximum score =16
↑ Score =↓ likelihoodfor lasting result
*
*
*
*
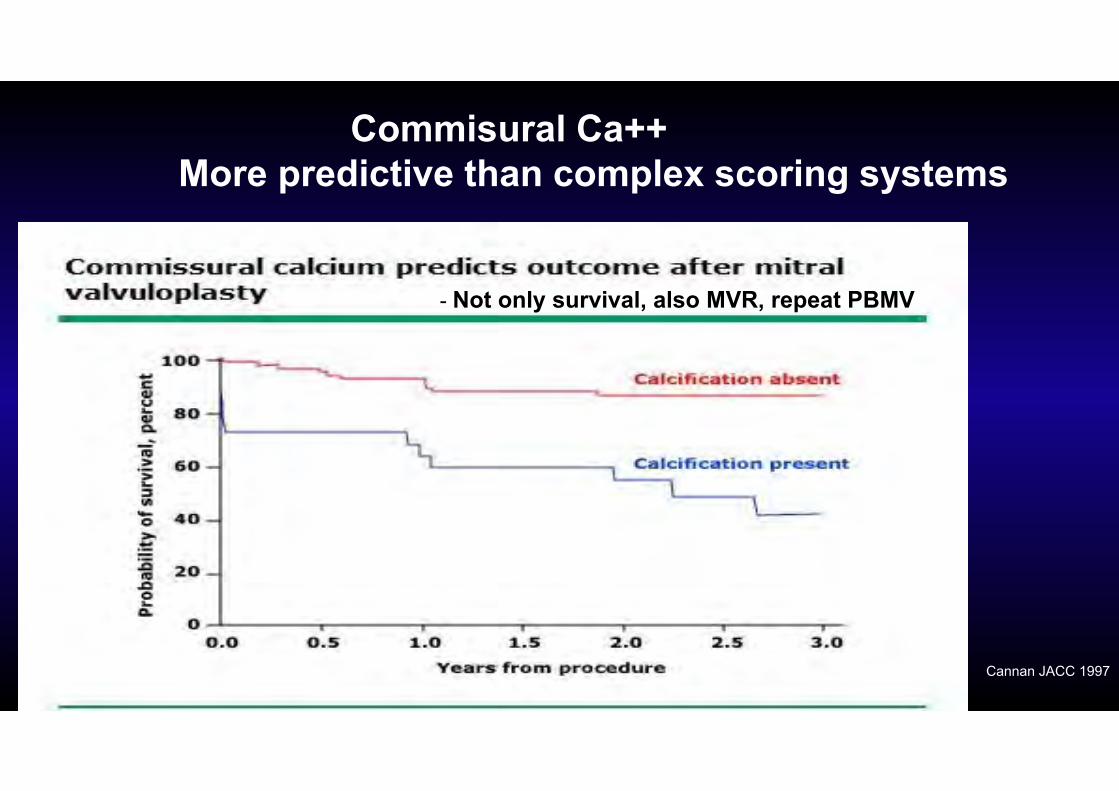
Commisural Ca++ More predictive than complex scoring systems
Cannan JACC 1997
- Not only survival, also MVR, repeat PBMV
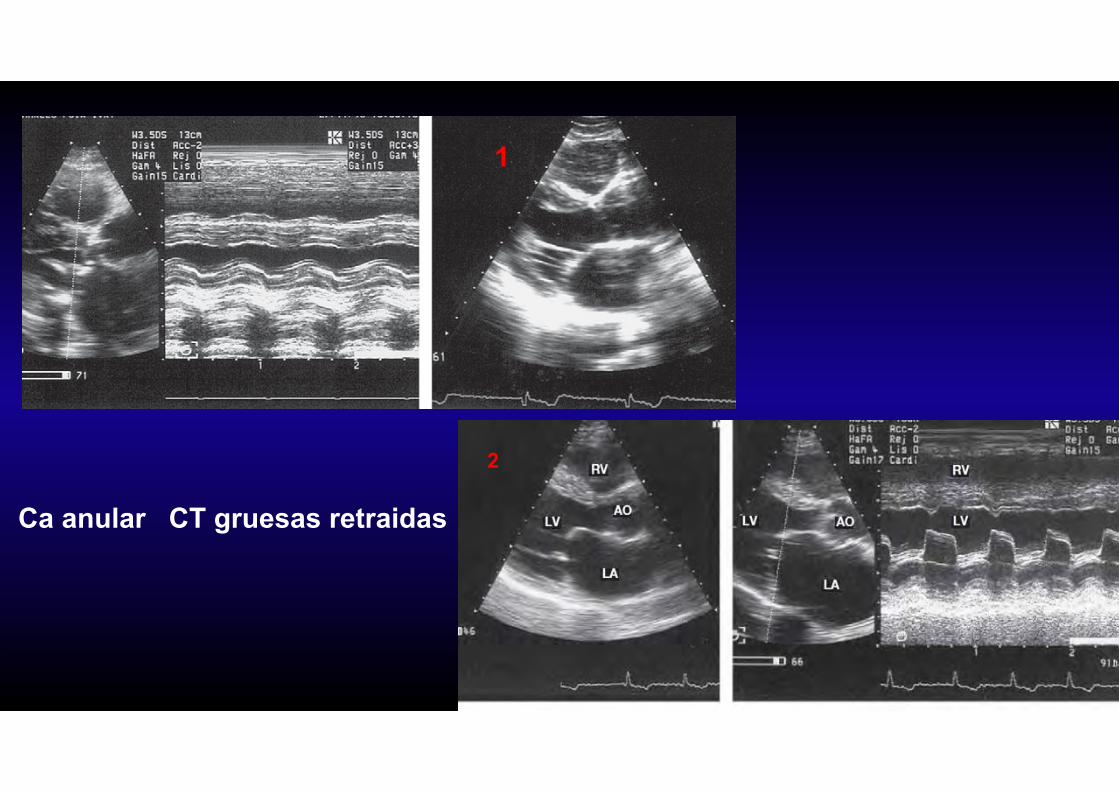
Ca anular CT gruesas retraidas
1
2


Cateterismo en estenosis mitral
Patron oro
Se utiliza
para realizar VMP
discordancia clinico ecocardiografica
Mujer 35 aAntc FRDisnea IIEM severa ecoScore valvular 8
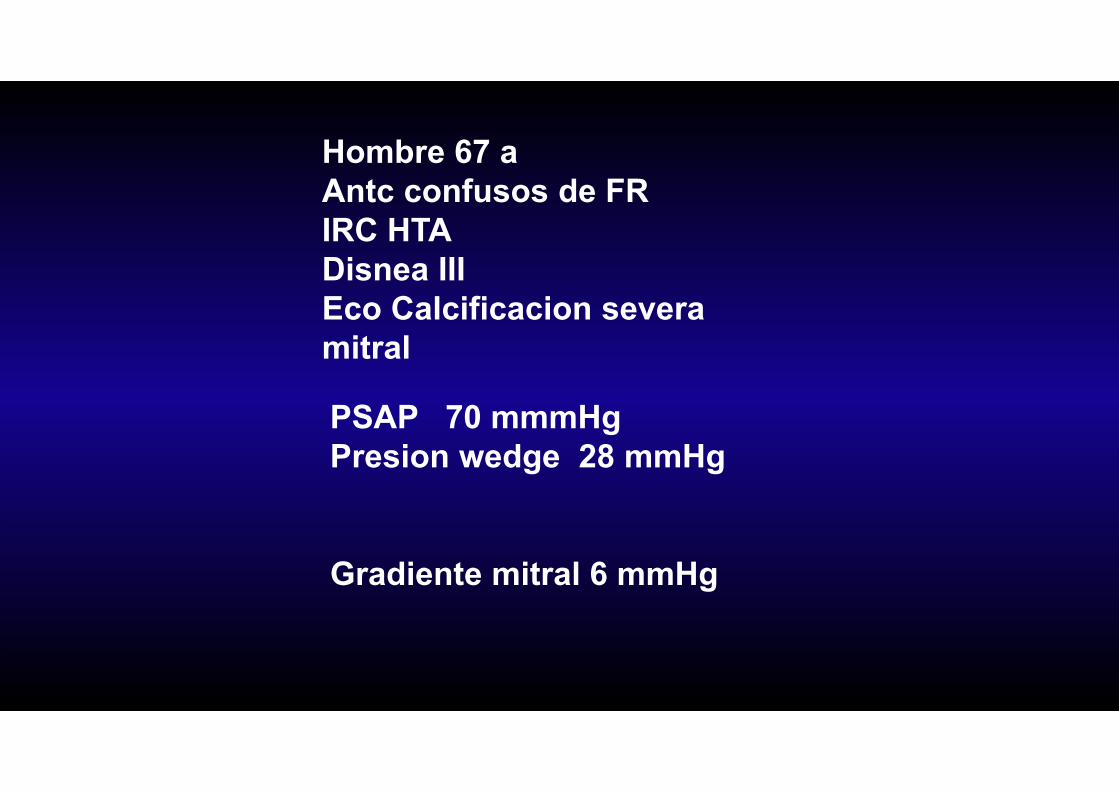
Hombre 67 aAntc confusos de FRIRC HTADisnea IIIEco Calcificacion severamitral
PSAP 70 mmmHgPresion wedge 28 mmHg
Gradiente mitral 6 mmHg
Conducta
1- Administrar liquidos2- Ejercicio3- Modificar FC4- Repetir mediciones SG5- Cateterismo
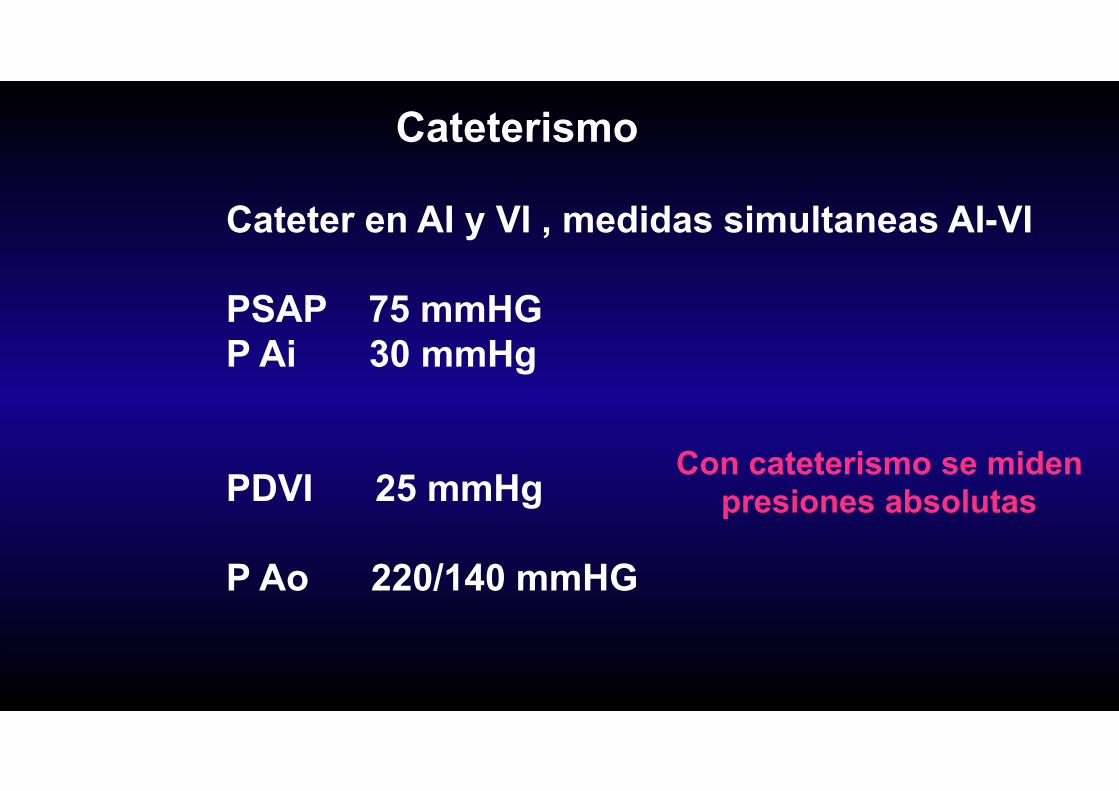
Cateterismo
Cateter en AI y VI , medidas simultaneas AI-VI
PSAP 75 mmHGP Ai 30 mmHg
PDVI 25 mmHg
P Ao 220/140 mmHG
Con cateterismo se midenpresiones absolutas
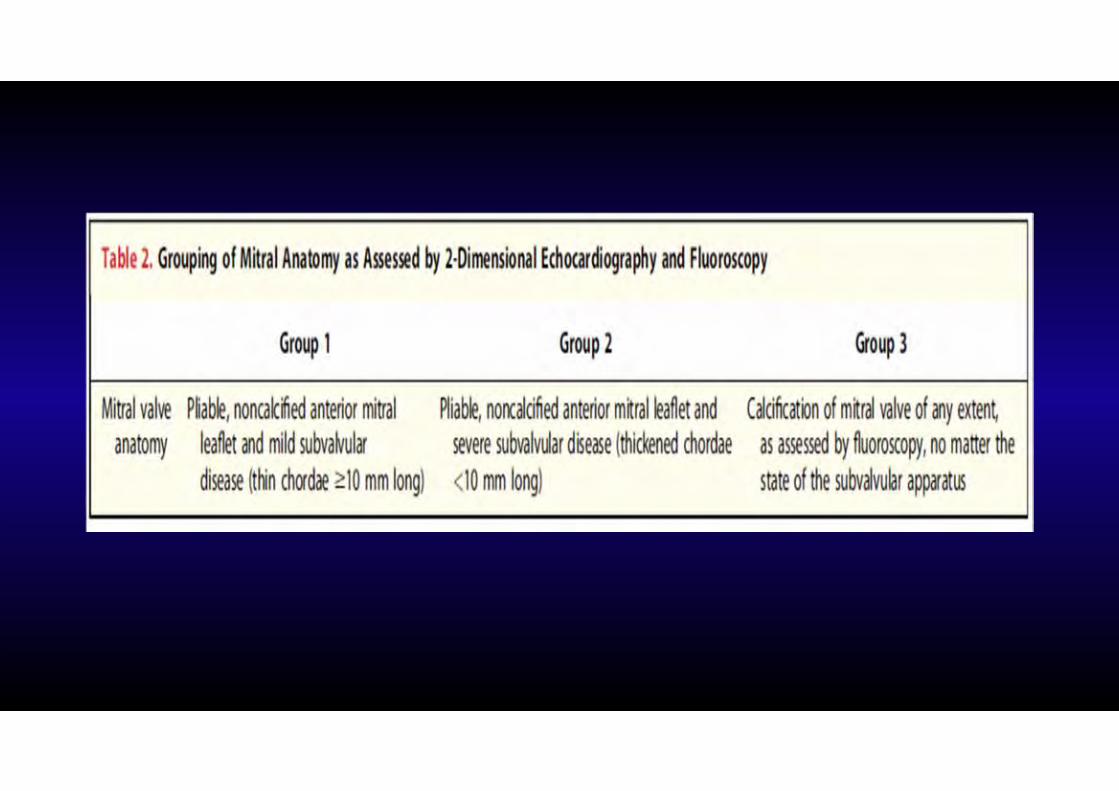
≥3 scoring systems - Wilkins most commonFor PMBV – need commissural fusion
Other important factors:Leaflet mobility & thickeningInvolvement of sub-mitral apparatusSeverity of calcificationPre-procedure MRLA or LAA thrombus
MS- suitability for PMBV
TEE for PBMV- LA Thrombus
• LAA thrombus “contraindication” for PBMV (AHA/ACC) If + postpone procedure - Rx Warfarin→ INR 3.0 until resolved on TEEIf not resolved many recommend surgery
• Several cases of uneventful PBMV reported in patients with LAA thrombus
Park - JASE 2000, Nobuyoshi - Circ 1989, Thomas Br Heart J 1992, Ritoo – Am Heart J 1993
LA thrombus – Sens / Spec 81 / 99 %
LAA thrombus – Sens / Spec 98 / 98 % (surgery – gold STD)