Embed Size (px)
Citation preview

Echocardiographic assessment of Aortic Stenosis
Dr. Md. Mashiul AlamPhase B residentCardiology
Chairpersion: Assoc. Prof. Naveen Sheikh

“A 30 year-old-man presented with shortness of breath for 1 month on mild to moderate exertion. He also complaints of recurrent loss of consciousness for last 6 months which last for less then 5 minutes and exertional chest discomfort for over one year. On examination he has low volume pulse, BP- 120/100. A systolic murmur best hear over aortic area with radiation to both carotid arteries”
What is the lesion?

Causes of Aortic Stenosis
1. Calcific degenerative stenosis of trileaflet or bicuspid valve
2. Congenital valve disease (Bicuspid or unicuspid valve)
3. Rheumatic Valve disease

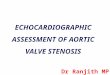
Aortic valve anatomy
• 3 cusp, 3 commisure• 3-4 cm sq

RCC
NCC

NoRmaL – clock wise



Options
• TTE
• TEE
• 3D echocardiography

Echocardiographic Views
• PLAX• PSAX at the level of great vessels• Apical views – A4CV, Apical long axis views• Right parasternal view• Suprasternal view

Aim of echocardiographic evaluation
• Define the cause of stenosis• Quantification of severity• Evaluation of co existing valvular lesions• Assessment of LV systolic function• Detection of response of chronic pressure load
over cardiac chambers and pulmonary vascular bed

Calcific degenerative AS
• Aortic sclerosis- early degenerative change• Areas of increased echogenicity- typically at
the base• Reduced systolic opening of aortic cusps• Calcification of aortic root• MAC






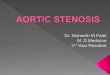
Bicuspid aortic valve

Diastolic sagging

Systolic doming

Eccentric closure line

PSAX view

Ellipsoid opening


3 D

Bicuspid Aortic Stenosis
Associated with:Dilatation of aortic rootCoarctation of aorta

Rheumatic AS
• Present in 30% patients with MS• Rarely isolatedFeatures:Increased echogenicity along the leaflet edgeCommissural fusionSystolic domingSuperimposed calcificationAssociated MV disease


Congenital Aortic Stenosis
• Unicuspid AS most common

• Eccentric single orifice• Prominent systolic doming• Only one point of attachment at 6 O’clock
position with funnel shaped opening



Other different LVOT obstruction
• Fixed subvalvular obstructionSubaortic membrane or muscular stenosis• Dynamic subaortic obstruciton (HOCM)• Supravalvular stenosis

Subaortic membrane
• A subaortic membrane should be suspected in young adults when the valve anatomy is not clearly stenotic, yet Doppler examination reveals a high transaortic pressure gradient.
• Best seen in TEE• Localization of the level of obstruction by
detection of post stenotic flow disturbance and site of increased flow velocity


Coarse apperance of velocity curve due to rough fluttering
Of valve


Supravalvular stenosis
• Williams syndrome


Quantification of AS severity
1. Maximum aortic jet velocity2. Mean transaortic pressure gradient3. Measurement of valve area – ideally by
Continuity equation
Planimetry more accurate in TEE and 3D echo


Aortic Jet Velocity
• Most reliable and reproducible measure for serial follow up
• Key element in decision making about timing of valve replacement
Views: Apical approach- 5 chamber or long axis viewHigh right parasternal positionSuprasternal approach




Simple Bernoulli Eqation P = 4 V 2

AVA by Continuity Equation
AV area = LVOT area X LVOT VTI / AV VTI
CSA = 0.785 x D2VTI = stroke distance ( how far single RBC travel
per single systole)
CSA X VTI = amount of blood travel (cm3) per stroke


LVOT area = 0.785 X Diameter of LVOT sq

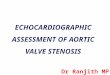
• LVOT diameter Zoomed PLAX view during mid systoleJust proximal to AV and parallel to AV plane≈ 2 cm


LVOT VTI
Sample volume just proximal to the AVOnly the closing click is seen


To close to AV

Aortic Valve VTI

Dimensionless index or velocity ratio
• When inaccurate measurement of LVOT diameter suspected
Ration of LVOT or AoV peak velocities or VTIs
Severe AS: <0.25Mild AS: >0.5

Indexed AVA
AVA by continuity equation or planimetry / BSA (cm sq./ m sq.)
Severe AS: <0.6Mild AS: >0.85


Coexisting valvular disease
• 80% AS patient has AR• MR due to MAC in calcific degenerative AS• MS or MR if rheumatic origin

Response to chronic pressure
• Left ventricleConc. LVHDiastolic dysfunctionSystolic dysfunction


Clinical application
• Mild stenosis is characterized by an aortic jet velocity between 2.6 and 3 m/s – additional measures of stenosis severity are rarely needed
• Valve area calculation is unnecessary in jet velocity is > 5 m/s
• When jet velocity between 3 to 4 m/s mean gradient and valve area calculation is essential as there may be low flow low gradient severe AS

Follow up echo in clinically stable patient
123 of AS
• 1 year or less in severe AS• 1-2 years with moderate AS• 3 years or longer in mild AS

Thank you