Embed Size (px)
Citation preview

Echotech Reporting GuidelinesVersion 12Authors: Dr R Sharma and K EltonNext Review: January 2013 Echotech © 2012
Principal brand markTo be used in the majority of situations.
2.1 BASIC ELEMENTS
1 Echotech Reporting Guidelines
Rationale
These guidelines have been devised to:
• promote both the quality and consistency of all Echotech reports• encourage a systematic approach to reporting and• facilitate the accurate comparison of echocardiograms performed by different Echotech Cardiac Physiologists at different sites
In terms of the echocardiographic views (see section 1) and measurements, the BSE guidelines for ‘AMinimum Dataset for a Standard Adult Transthoracic Echocardiogram’1 are followed.
In terms of reference values, this document reflects the BSE Guidelines for Chamber and ValveQuantification2.
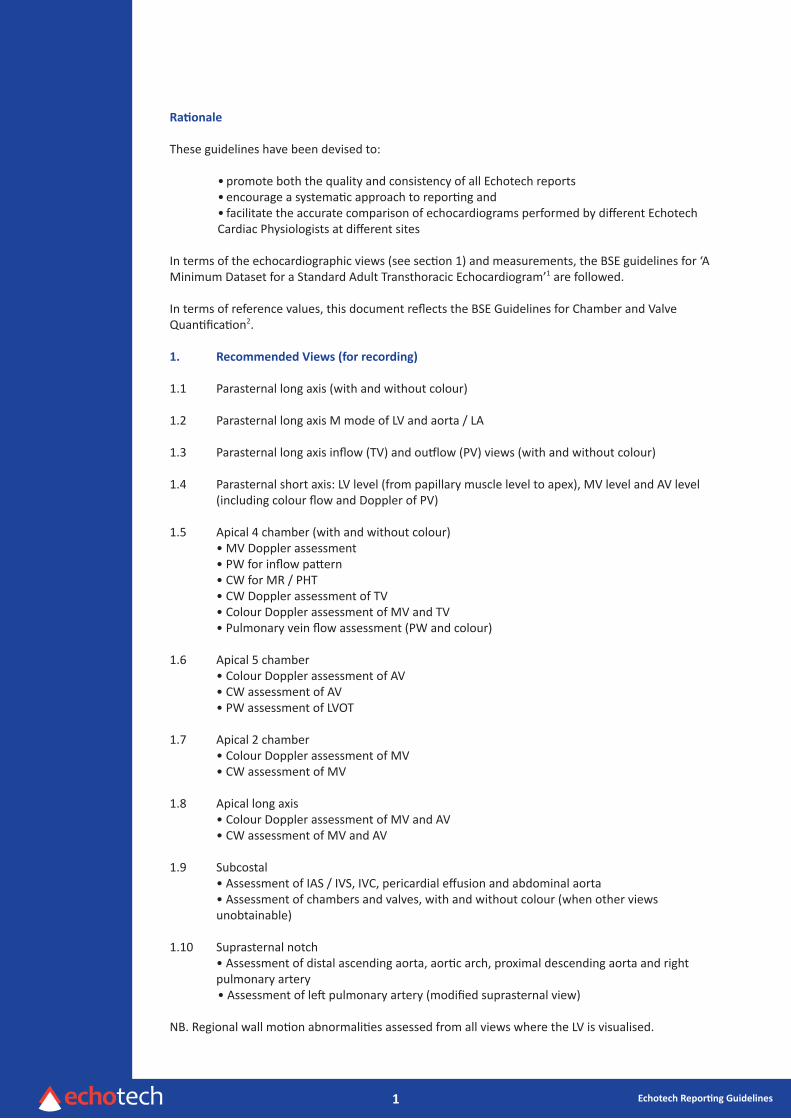
1. Recommended Views (for recording)
1.1 Parasternal long axis (with and without colour)
1.2 Parasternal long axis M mode of LV and aorta / LA
1.3 Parasternal long axis inflow (TV) and outflow (PV) views (with and without colour)
1.4 Parasternal short axis: LV level (from papillary muscle level to apex), MV level and AV level (including colour flow and Doppler of PV)
1.5 Apical 4 chamber (with and without colour) • MV Doppler assessment • PW for inflow pattern • CW for MR / PHT • CW Doppler assessment of TV • Colour Doppler assessment of MV and TV • Pulmonary vein flow assessment (PW and colour)
1.6 Apical 5 chamber • Colour Doppler assessment of AV • CW assessment of AV • PW assessment of LVOT
1.7 Apical 2 chamber • Colour Doppler assessment of MV • CW assessment of MV
1.8 Apical long axis • Colour Doppler assessment of MV and AV • CW assessment of MV and AV
1.9 Subcostal • Assessment of IAS / IVS, IVC, pericardial effusion and abdominal aorta • Assessment of chambers and valves, with and without colour (when other views unobtainable)
1.10 Suprasternal notch • Assessment of distal ascending aorta, aortic arch, proximal descending aorta and right pulmonary artery • Assessment of left pulmonary artery (modified suprasternal view)
NB. Regional wall motion abnormalities assessed from all views where the LV is visualised.
2 Echotech Reporting Guidelines
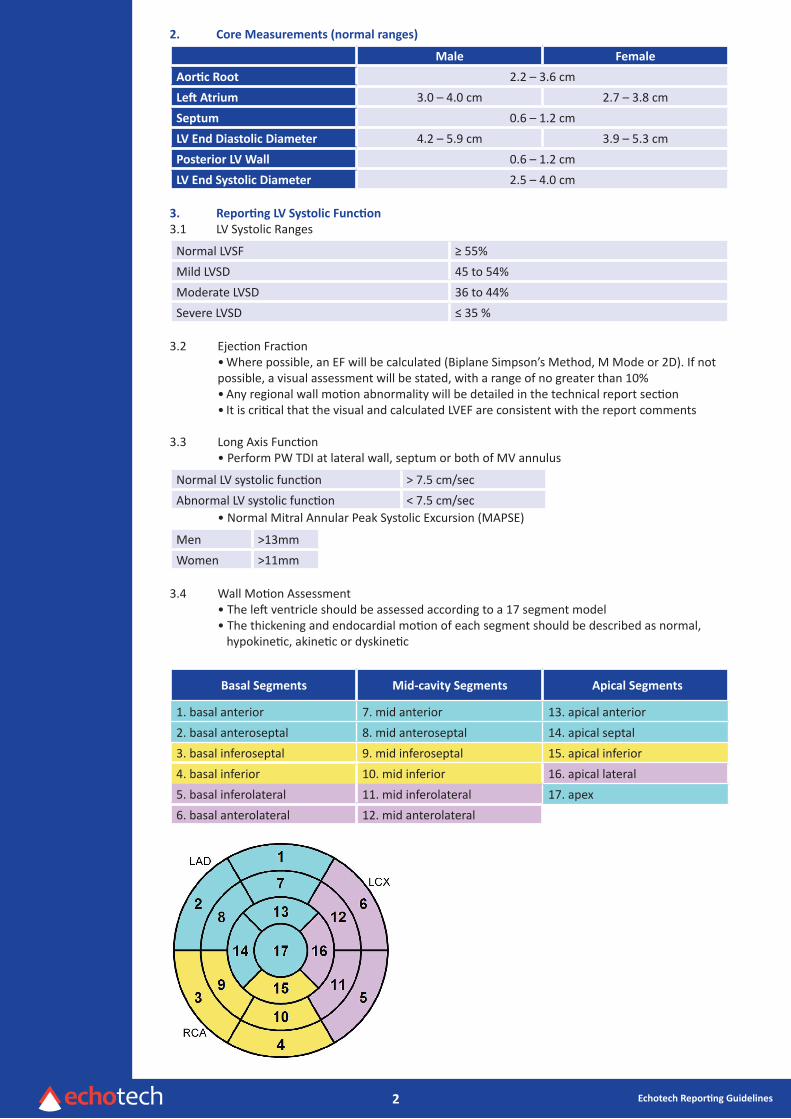
2. Core Measurements (normal ranges)
Male Female
Aortic Root 2.2 – 3.6 cmLeft Atrium 3.0 – 4.0 cm 2.7 – 3.8 cmSeptum 0.6 – 1.2 cmLV End Diastolic Diameter 4.2 – 5.9 cm 3.9 – 5.3 cmPosterior LV Wall 0.6 – 1.2 cmLV End Systolic Diameter 2.5 – 4.0 cm
3. Reporting LV Systolic Function3.1 LV Systolic Ranges
Normal LVSF ≥ 55%Mild LVSD 45 to 54%Moderate LVSD 36 to 44%Severe LVSD ≤ 35 %
3.2 Ejection Fraction• Where possible, an EF will be calculated (Biplane Simpson’s Method, M Mode or 2D). If not possible, a visual assessment will be stated, with a range of no greater than 10%• Any regional wall motion abnormality will be detailed in the technical report section• It is critical that the visual and calculated LVEF are consistent with the report comments
3.3 Long Axis Function • Perform PW TDI at lateral wall, septum or both of MV annulus
Normal LV systolic function > 7.5 cm/secAbnormal LV systolic function < 7.5 cm/sec
• Normal Mitral Annular Peak Systolic Excursion (MAPSE)
Men >13mmWomen >11mm
3.4 Wall Motion Assessment • The left ventricle should be assessed according to a 17 segment model • The thickening and endocardial motion of each segment should be described as normal, hypokinetic, akinetic or dyskinetic
Basal Segments Mid-cavity Segments Apical Segments
1. basal anterior 7. mid anterior 13. apical anterior2. basal anteroseptal 8. mid anteroseptal 14. apical septal3. basal inferoseptal 9. mid inferoseptal 15. apical inferior4. basal inferior 10. mid inferior 16. apical lateral5. basal inferolateral 11. mid inferolateral 17. apex6. basal anterolateral 12. mid anterolateral

3 Echotech Reporting Guidelines
17
apex
14 16
9 12
3 6
Recommended 17 LV Segment Model recognises LV apical segment
Basal
Mid-cavity
Apical
Short Axis (SA)
anterior
1
2
3
4
5
6
anteroseptal
anterolateral
inferolateral
inferior
inferoseptal
anterior
7
8
9 10
11
12
anteroseptal
anterolateral
inferolateral
inferior
inferoseptal
anterior
13
15
inferior
14 16
septal
lateral
Horizontal Long Axis (HLA)(4 chamber)
Vertical Long Axis (VLA)(2 chamber)
17
apex
4
10
15 13
7
1
4 Echotech Reporting Guidelines
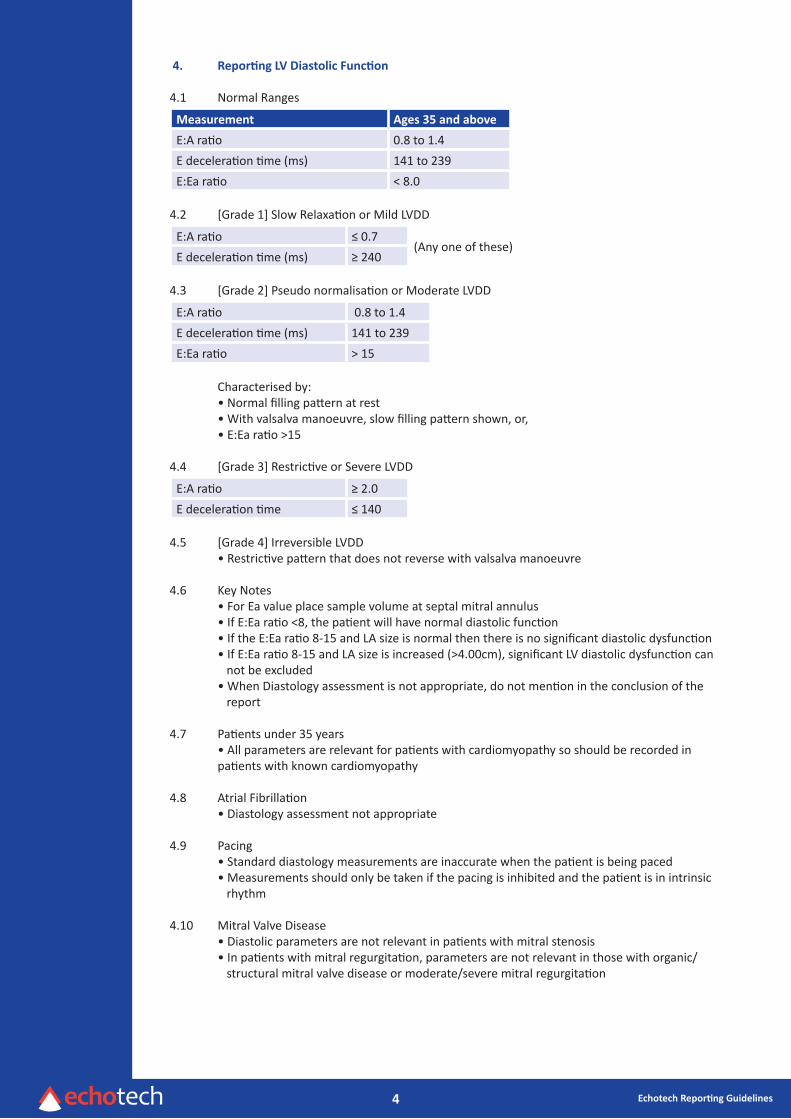
4. Reporting LV Diastolic Function
4.1 Normal Ranges
Measurement Ages 35 and above
E:A ratio 0.8 to 1.4E deceleration time (ms) 141 to 239E:Ea ratio < 8.0
4.2 [Grade 1] Slow Relaxation or Mild LVDD
E:A ratio ≤ 0.7(Any one of these)
E deceleration time (ms) ≥ 240
4.3 [Grade 2] Pseudo normalisation or Moderate LVDD
E:A ratio 0.8 to 1.4E deceleration time (ms) 141 to 239E:Ea ratio > 15
Characterised by: • Normal filling pattern at rest • With valsalva manoeuvre, slow filling pattern shown, or, • E:Ea ratio >15
4.4 [Grade 3] Restrictive or Severe LVDD
E:A ratio ≥ 2.0E deceleration time ≤ 140
4.5 [Grade 4] Irreversible LVDD • Restrictive pattern that does not reverse with valsalva manoeuvre
4.6 Key Notes • For Ea value place sample volume at septal mitral annulus • If E:Ea ratio <8, the patient will have normal diastolic function • If the E:Ea ratio 8-15 and LA size is normal then there is no significant diastolic dysfunction • If E:Ea ratio 8-15 and LA size is increased (>4.00cm), significant LV diastolic dysfunction can not be excluded • When Diastology assessment is not appropriate, do not mention in the conclusion of the report
4.7 Patients under 35 years • All parameters are relevant for patients with cardiomyopathy so should be recorded in patients with known cardiomyopathy
4.8 Atrial Fibrillation • Diastology assessment not appropriate
4.9 Pacing • Standard diastology measurements are inaccurate when the patient is being paced • Measurements should only be taken if the pacing is inhibited and the patient is in intrinsic rhythm
4.10 Mitral Valve Disease • Diastolic parameters are not relevant in patients with mitral stenosis • In patients with mitral regurgitation, parameters are not relevant in those with organic/ structural mitral valve disease or moderate/severe mitral regurgitation
5 Echotech Reporting Guidelines
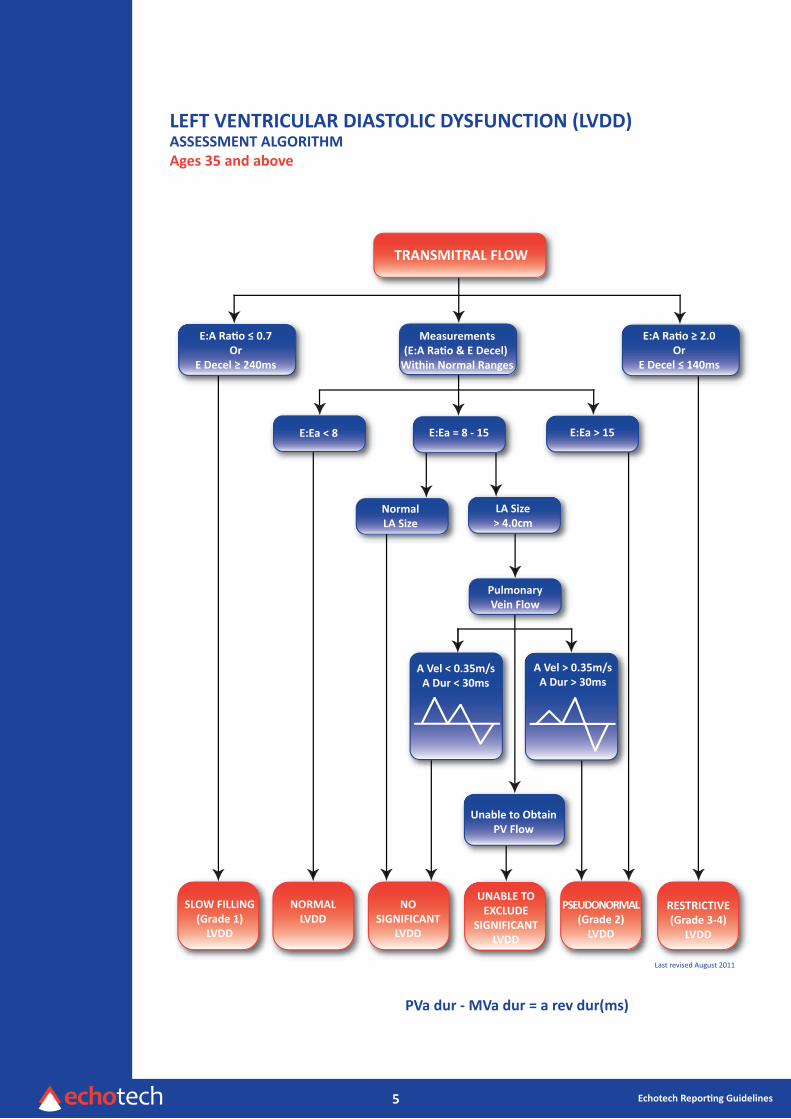
LEFT VENTRICULAR DIASTOLIC DYSFUNCTION (LVDD)ASSESSMENT ALGORITHMAges 35 and above
TRANSMITRAL FLOW
SLOW FILLING(Grade 1)
LVDD
NORMALLVDD
NOSIGNIFICANT
LVDD
UNABLE TOEXCLUDE
SIGNIFICANTLVDD
PSEUDONORMAL(Grade 2)
LVDD
RESTRICTIVE(Grade 3-4)
LVDD
E:A Ra o 0.7Or
E Decel 240ms
Measurements(E:A Ra o & E Decel)
Within Normal Ranges
E:A Ra o 2.0Or
E Decel 140ms
E:Ea < 8 E:Ea > 15E:Ea = 8 - 15
PulmonaryVein Flow
NormalLA Size
LA Size> 4.0cm
Unable to ObtainPV Flow
A Vel < 0.35m/sA Dur < 30ms
A Vel > 0.35m/sA Dur > 30ms
PVa dur - MVa dur = a rev dur(ms)
Last revised August 2011
6 Echotech Reporting Guidelines
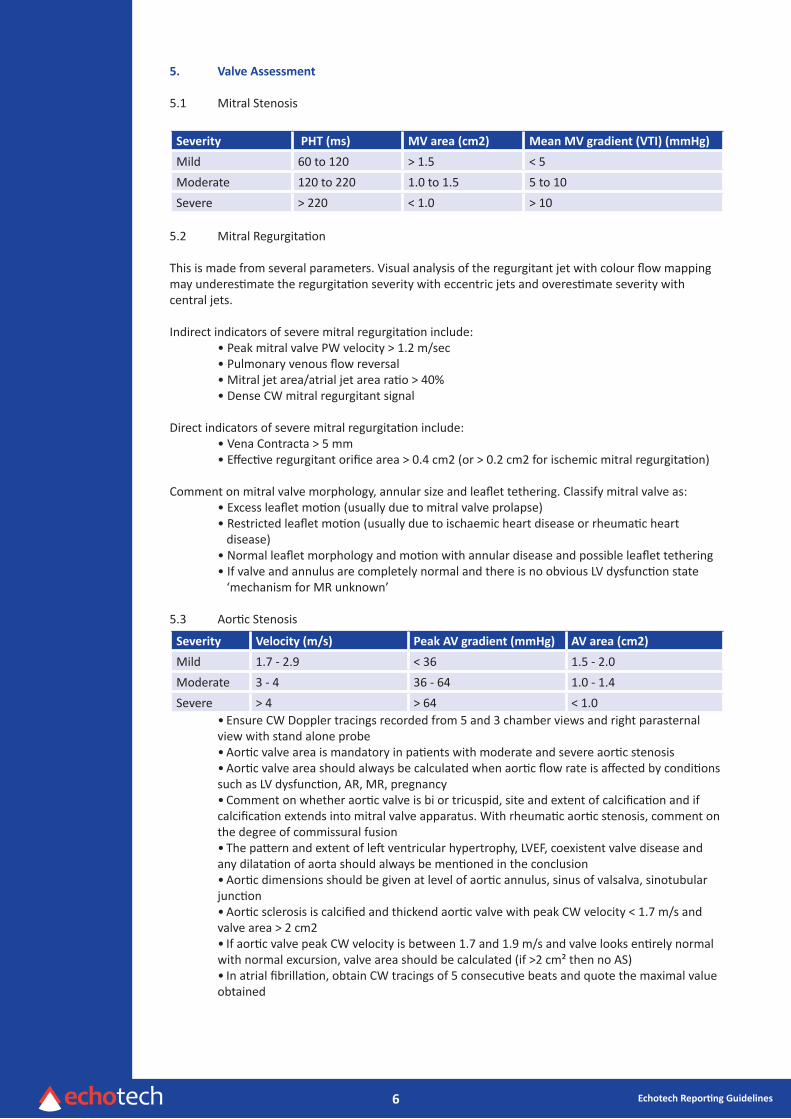
5. Valve Assessment
5.1 Mitral Stenosis
Severity PHT (ms) MV area (cm2) Mean MV gradient (VTI) (mmHg)
Mild 60 to 120 > 1.5 < 5Moderate 120 to 220 1.0 to 1.5 5 to 10Severe > 220 < 1.0 > 10
5.2 Mitral Regurgitation
This is made from several parameters. Visual analysis of the regurgitant jet with colour flow mappingmay underestimate the regurgitation severity with eccentric jets and overestimate severity withcentral jets.
Indirect indicators of severe mitral regurgitation include: • Peak mitral valve PW velocity > 1.2 m/sec • Pulmonary venous flow reversal • Mitral jet area/atrial jet area ratio > 40% • Dense CW mitral regurgitant signal
Direct indicators of severe mitral regurgitation include: • Vena Contracta > 5 mm • Effective regurgitant orifice area > 0.4 cm2 (or > 0.2 cm2 for ischemic mitral regurgitation)
Comment on mitral valve morphology, annular size and leaflet tethering. Classify mitral valve as: • Excess leaflet motion (usually due to mitral valve prolapse) • Restricted leaflet motion (usually due to ischaemic heart disease or rheumatic heart disease) • Normal leaflet morphology and motion with annular disease and possible leaflet tethering • If valve and annulus are completely normal and there is no obvious LV dysfunction state ‘mechanism for MR unknown’
5.3 Aortic Stenosis
Severity Velocity (m/s) Peak AV gradient (mmHg) AV area (cm2)
Mild 1.7 - 2.9 < 36 1.5 - 2.0Moderate 3 - 4 36 - 64 1.0 - 1.4Severe > 4 > 64 < 1.0
• Ensure CW Doppler tracings recorded from 5 and 3 chamber views and right parasternal view with stand alone probe• Aortic valve area is mandatory in patients with moderate and severe aortic stenosis• Aortic valve area should always be calculated when aortic flow rate is affected by conditions such as LV dysfunction, AR, MR, pregnancy• Comment on whether aortic valve is bi or tricuspid, site and extent of calcification and if calcification extends into mitral valve apparatus. With rheumatic aortic stenosis, comment on the degree of commissural fusion• The pattern and extent of left ventricular hypertrophy, LVEF, coexistent valve disease and any dilatation of aorta should always be mentioned in the conclusion• Aortic dimensions should be given at level of aortic annulus, sinus of valsalva, sinotubular junction• Aortic sclerosis is calcified and thickend aortic valve with peak CW velocity < 1.7 m/s and valve area > 2 cm2• If aortic valve peak CW velocity is between 1.7 and 1.9 m/s and valve looks entirely normal with normal excursion, valve area should be calculated (if >2 cm² then no AS)• In atrial fibrillation, obtain CW tracings of 5 consecutive beats and quote the maximal value obtained
7 Echotech Reporting Guidelines
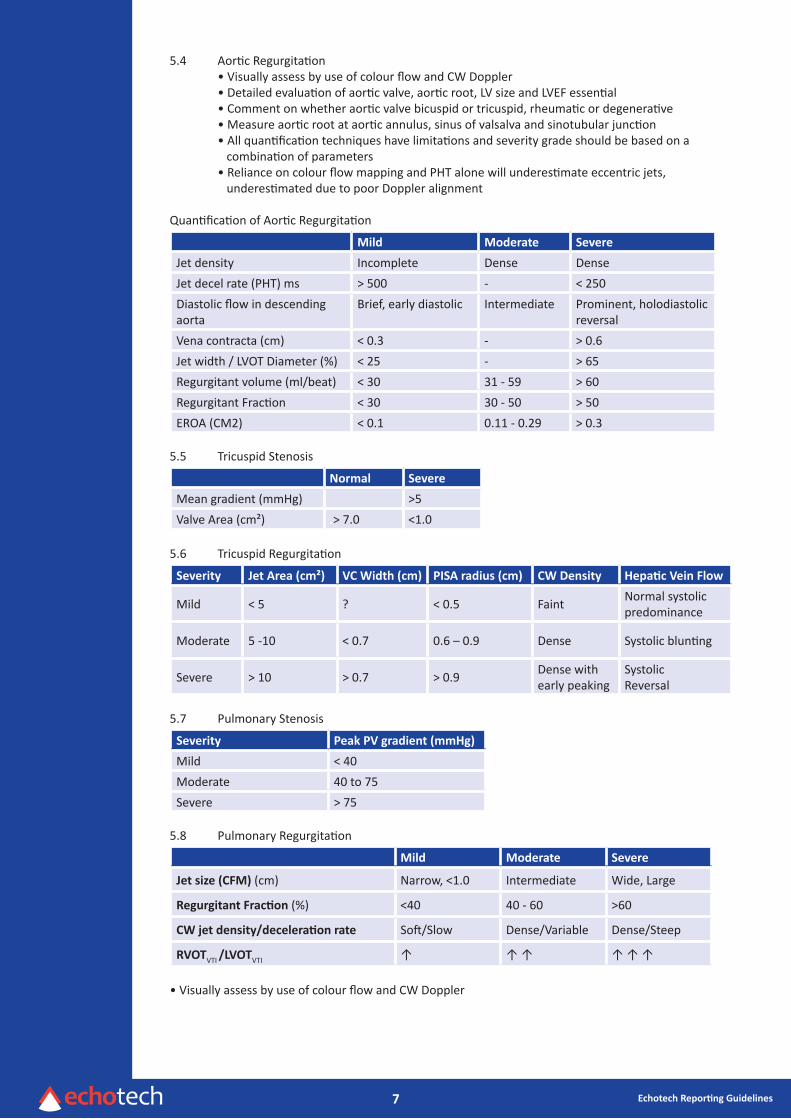
5.4 Aortic Regurgitation • Visually assess by use of colour flow and CW Doppler • Detailed evaluation of aortic valve, aortic root, LV size and LVEF essential • Comment on whether aortic valve bicuspid or tricuspid, rheumatic or degenerative • Measure aortic root at aortic annulus, sinus of valsalva and sinotubular junction • All quantification techniques have limitations and severity grade should be based on a combination of parameters • Reliance on colour flow mapping and PHT alone will underestimate eccentric jets, underestimated due to poor Doppler alignment
Quantification of Aortic Regurgitation
Mild Moderate Severe
Jet density Incomplete Dense DenseJet decel rate (PHT) ms > 500 - < 250Diastolic flow in descending aorta
Brief, early diastolic Intermediate Prominent, holodiastolic reversal
Vena contracta (cm) < 0.3 - > 0.6Jet width / LVOT Diameter (%) < 25 - > 65Regurgitant volume (ml/beat) < 30 31 - 59 > 60Regurgitant Fraction < 30 30 - 50 > 50EROA (CM2) < 0.1 0.11 - 0.29 > 0.3
5.5 Tricuspid Stenosis
Normal Severe
Mean gradient (mmHg) >5Valve Area (cm²) .> 7.0 <1.0
5.6 Tricuspid Regurgitation
Severity Jet Area (cm²) VC Width (cm) PISA radius (cm) CW Density Hepatic Vein Flow
Mild < 5 ? < 0.5 Faint Normal systolic predominance
Moderate 5 -10 < 0.7 0.6 – 0.9 Dense Systolic blunting
Severe > 10 > 0.7 > 0.9 Dense with early peaking
Systolic Reversal
5.7 Pulmonary Stenosis
Severity Peak PV gradient (mmHg)
Mild < 40Moderate 40 to 75Severe > 75
5.8 Pulmonary Regurgitation
Mild Moderate Severe
Jet size (CFM) (cm) Narrow, <1.0 Intermediate Wide, Large
Regurgitant Fraction (%) <40 40 - 60 >60
CW jet density/deceleration rate Soft/Slow Dense/Variable Dense/Steep
RVOTVTI /LVOTVTI ↑ ↑ ↑ ↑ ↑ ↑
• Visually assess by use of colour flow and CW Doppler
8 Echotech Reporting Guidelines
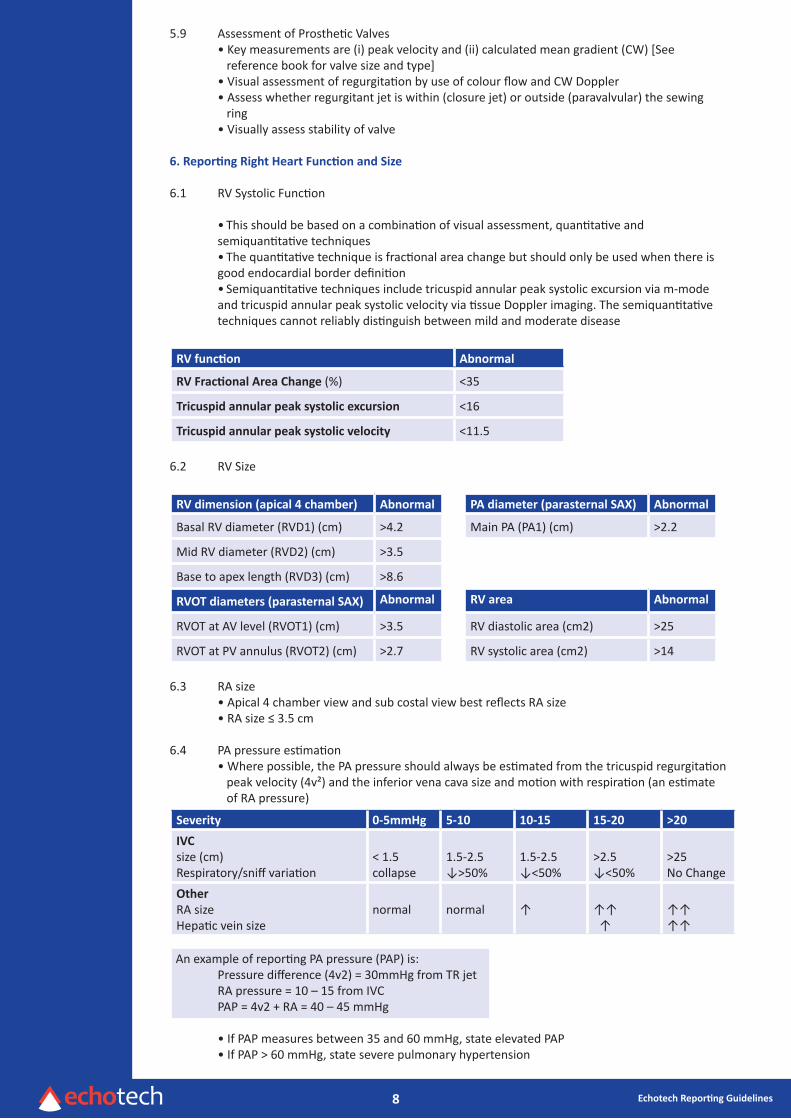
5.9 Assessment of Prosthetic Valves • Key measurements are (i) peak velocity and (ii) calculated mean gradient (CW) [See reference book for valve size and type] • Visual assessment of regurgitation by use of colour flow and CW Doppler • Assess whether regurgitant jet is within (closure jet) or outside (paravalvular) the sewing ring • Visually assess stability of valve
6. Reporting Right Heart Function and Size
6.1 RV Systolic Function
• This should be based on a combination of visual assessment, quantitative and semiquantitative techniques• The quantitative technique is fractional area change but should only be used when there is good endocardial border definition• Semiquantitative techniques include tricuspid annular peak systolic excursion via m-mode and tricuspid annular peak systolic velocity via tissue Doppler imaging. The semiquantitative techniques cannot reliably distinguish between mild and moderate disease
RV function Abnormal
RV Fractional Area Change (%) <35
Tricuspid annular peak systolic excursion <16
Tricuspid annular peak systolic velocity <11.5
6.2 RV Size
RV dimension (apical 4 chamber) Abnormal PA diameter (parasternal SAX) Abnormal
Basal RV diameter (RVD1) (cm) >4.2 Main PA (PA1) (cm) >2.2
Mid RV diameter (RVD2) (cm) >3.5
Base to apex length (RVD3) (cm) >8.6
RVOT diameters (parasternal SAX) Abnormal RV area Abnormal
RVOT at AV level (RVOT1) (cm) >3.5 RV diastolic area (cm2) >25
RVOT at PV annulus (RVOT2) (cm) >2.7 RV systolic area (cm2) >14
6.3 RA size • Apical 4 chamber view and sub costal view best reflects RA size • RA size ≤ 3.5 cm
6.4 PA pressure estimation • Where possible, the PA pressure should always be estimated from the tricuspid regurgitation peak velocity (4v²) and the inferior vena cava size and motion with respiration (an estimate of RA pressure)
Severity 0-5mmHg 5-10 10-15 15-20 >20
IVC size (cm)Respiratory/sniff variation
< 1.5collapse
1.5-2.5↓>50%
1.5-2.5↓<50%
>2.5↓<50%
>25No Change
OtherRA sizeHepatic vein size
normal normal ↑ ↑↑ ↑
↑↑↑↑
An example of reporting PA pressure (PAP) is: Pressure difference (4v2) = 30mmHg from TR jet RA pressure = 10 – 15 from IVC PAP = 4v2 + RA = 40 – 45 mmHg
• If PAP measures between 35 and 60 mmHg, state elevated PAP • If PAP > 60 mmHg, state severe pulmonary hypertension
9 Echotech Reporting Guidelines
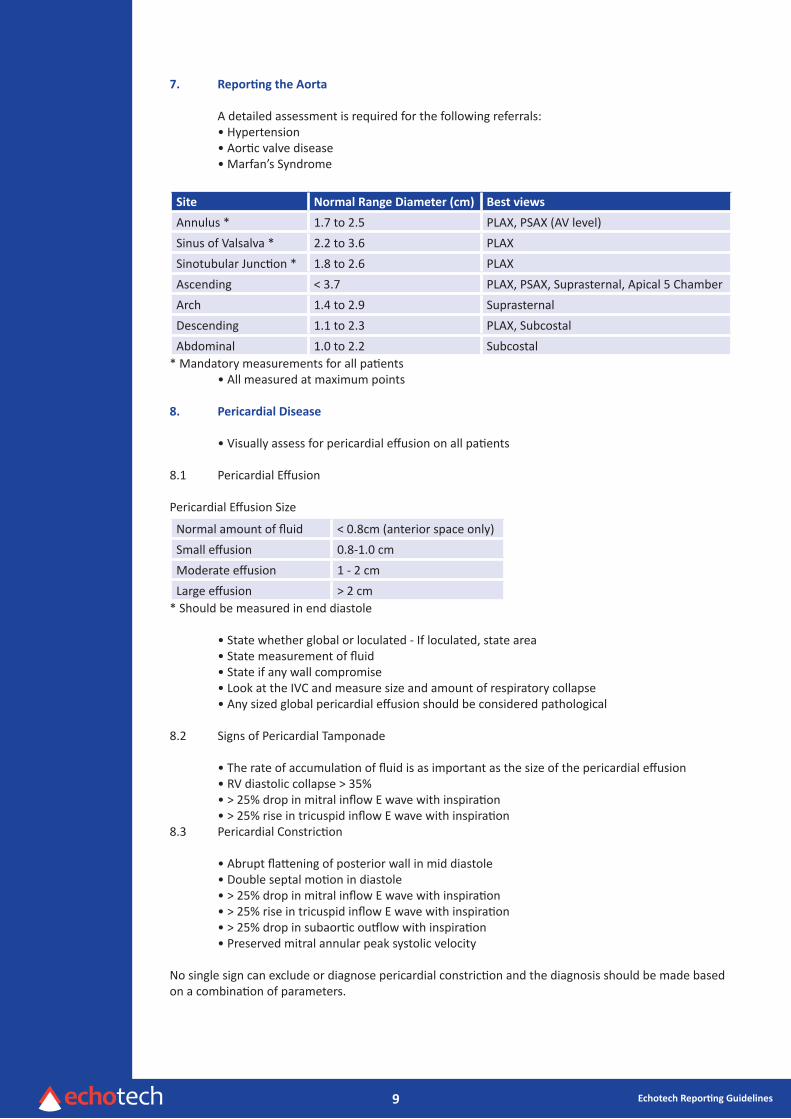
7. Reporting the Aorta
A detailed assessment is required for the following referrals: • Hypertension • Aortic valve disease • Marfan’s Syndrome
Site Normal Range Diameter (cm) Best views
Annulus * 1.7 to 2.5 PLAX, PSAX (AV level)Sinus of Valsalva * 2.2 to 3.6 PLAXSinotubular Junction * 1.8 to 2.6 PLAXAscending < 3.7 PLAX, PSAX, Suprasternal, Apical 5 ChamberArch 1.4 to 2.9 SuprasternalDescending 1.1 to 2.3 PLAX, SubcostalAbdominal 1.0 to 2.2 Subcostal
* Mandatory measurements for all patients • All measured at maximum points
8. Pericardial Disease
• Visually assess for pericardial effusion on all patients
8.1 Pericardial Effusion
Pericardial Effusion Size
Normal amount of fluid < 0.8cm (anterior space only)Small effusion 0.8-1.0 cmModerate effusion 1 - 2 cmLarge effusion > 2 cm
* Should be measured in end diastole
• State whether global or loculated - If loculated, state area • State measurement of fluid • State if any wall compromise • Look at the IVC and measure size and amount of respiratory collapse • Any sized global pericardial effusion should be considered pathological
8.2 Signs of Pericardial Tamponade • The rate of accumulation of fluid is as important as the size of the pericardial effusion • RV diastolic collapse > 35% • > 25% drop in mitral inflow E wave with inspiration • > 25% rise in tricuspid inflow E wave with inspiration8.3 Pericardial Constriction
• Abrupt flattening of posterior wall in mid diastole • Double septal motion in diastole • > 25% drop in mitral inflow E wave with inspiration • > 25% rise in tricuspid inflow E wave with inspiration • > 25% drop in subaortic outflow with inspiration • Preserved mitral annular peak systolic velocity
No single sign can exclude or diagnose pericardial constriction and the diagnosis should be made basedon a combination of parameters.
10 Echotech Reporting Guidelines
9. Technical Report Comments
• The technical report section is divided into 5 areas: LV assessment, Right Heart Assessment, Valves, Other and Conclusion
For each cardiac structure both morphology and function is described
• The Echotech report is primary care focussed and is therefore written in clear, descriptive terms, stating all key findings, whether normal or abnormal• Abbreviations are not used in the conclusion• All measurements that are not detailed elsewhere on the report but are relevant to the findings (e.g. aortic valve gradient) are stated within the technical report section (LV Assessment, Right Heart Assessment, Valves and Other)
• Measurements are not detailed in the Conclusion • When a finding requires clarification / peer review then the term ‘suspicion of /query of…’ is used within the technical report and the ‘peer review required’ box is ticked • The report states a conclusion / summary which 1) Details the LV systolic function and the LV diastolic function (where appropriate) 2) Emphasises the abnormal findings and 3) Answers the question(s) posed by the referring clinician
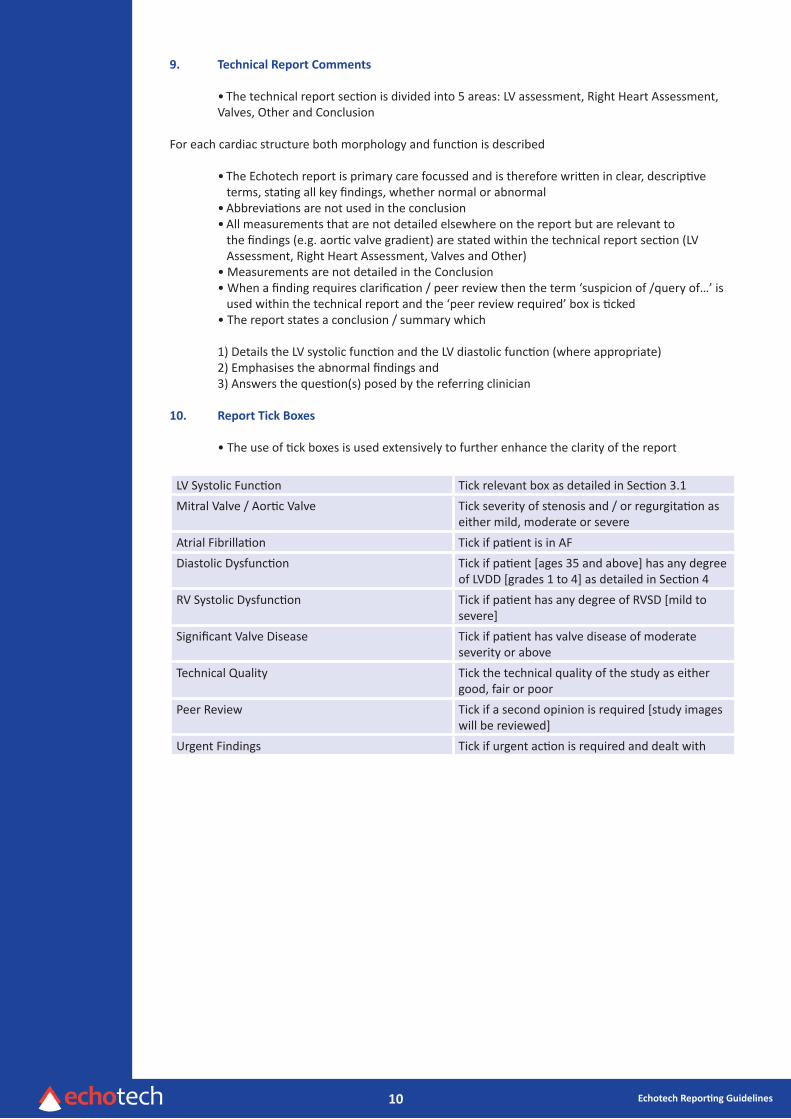
10. Report Tick Boxes
• The use of tick boxes is used extensively to further enhance the clarity of the report
LV Systolic Function Tick relevant box as detailed in Section 3.1Mitral Valve / Aortic Valve Tick severity of stenosis and / or regurgitation as
either mild, moderate or severeAtrial Fibrillation Tick if patient is in AFDiastolic Dysfunction Tick if patient [ages 35 and above] has any degree
of LVDD [grades 1 to 4] as detailed in Section 4RV Systolic Dysfunction Tick if patient has any degree of RVSD [mild to
severe]Significant Valve Disease Tick if patient has valve disease of moderate
severity or aboveTechnical Quality Tick the technical quality of the study as either
good, fair or poorPeer Review Tick if a second opinion is required [study images
will be reviewed]Urgent Findings Tick if urgent action is required and dealt with
11 Echotech Reporting Guidelines
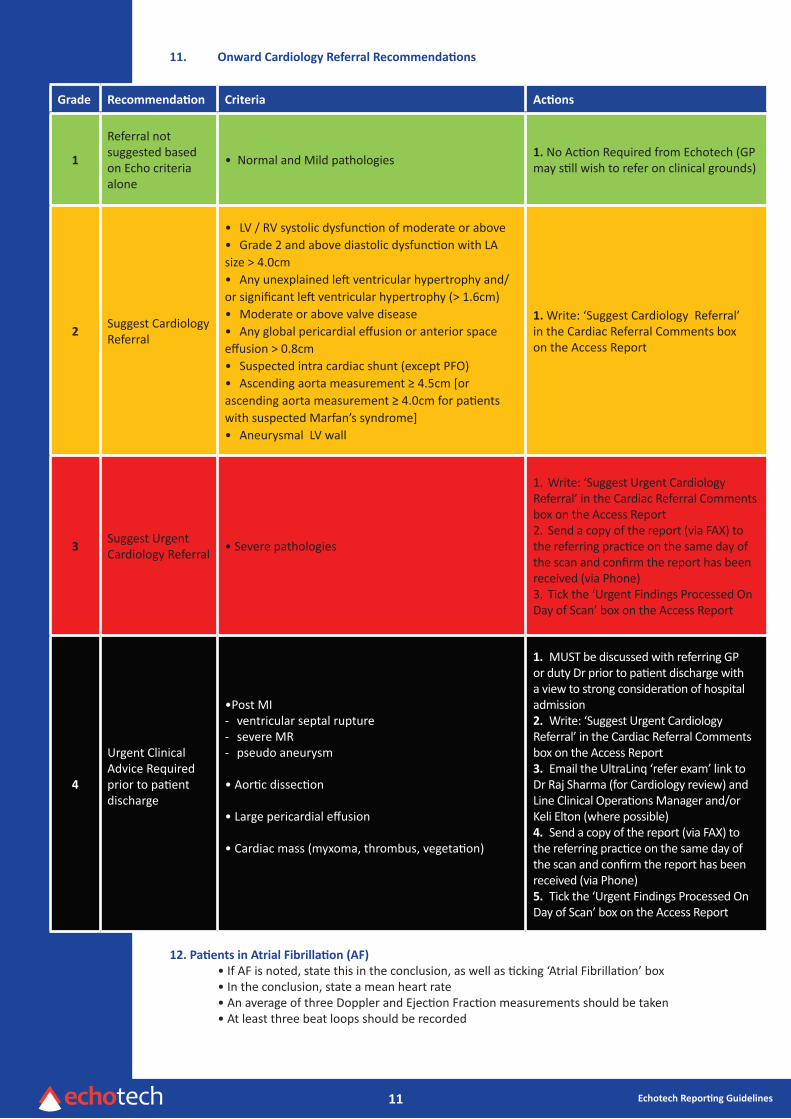
11. Onward Cardiology Referral Recommendations
Grade Recommendation Criteria Actions
1
Referral not suggested based on Echo criteria alone
• Normal and Mild pathologies 1. No Action Required from Echotech (GP may still wish to refer on clinical grounds)
2Suggest CardiologyReferral
• LV / RV systolic dysfunction of moderate or above• Grade 2 and above diastolic dysfunction with LA size > 4.0cm• Any unexplained left ventricular hypertrophy and/or significant left ventricular hypertrophy (> 1.6cm)• Moderate or above valve disease• Any global pericardial effusion or anterior space effusion > 0.8cm• Suspected intra cardiac shunt (except PFO)• Ascending aorta measurement ≥ 4.5cm [or ascending aorta measurement ≥ 4.0cm for patients with suspected Marfan’s syndrome]• Aneurysmal LV wall
1. Write: ‘Suggest Cardiology Referral’ in the Cardiac Referral Comments box on the Access Report
3Suggest Urgent Cardiology Referral • Severe pathologies
1. Write: ‘Suggest Urgent Cardiology Referral’ in the Cardiac Referral Comments box on the Access Report2. Send a copy of the report (via FAX) to the referring practice on the same day of the scan and confirm the report has been received (via Phone)3. Tick the ‘Urgent Findings Processed On Day of Scan’ box on the Access Report
4
Urgent Clinical Advice Required prior to patient discharge
•Post MI- ventricular septal rupture- severe MR- pseudo aneurysm
• Aortic dissection
• Large pericardial effusion
• Cardiac mass (myxoma, thrombus, vegetation)
1. MUST be discussed with referring GP or duty Dr prior to patient discharge with a view to strong consideration of hospital admission2. Write: ‘Suggest Urgent Cardiology Referral’ in the Cardiac Referral Comments box on the Access Report3. Email the UltraLinq ‘refer exam’ link to Dr Raj Sharma (for Cardiology review) and Line Clinical Operations Manager and/or Keli Elton (where possible)4. Send a copy of the report (via FAX) to the referring practice on the same day of the scan and confirm the report has been received (via Phone)5. Tick the ‘Urgent Findings Processed On Day of Scan’ box on the Access Report
12. Patients in Atrial Fibrillation (AF) • If AF is noted, state this in the conclusion, as well as ticking ‘Atrial Fibrillation’ box • In the conclusion, state a mean heart rate • An average of three Doppler and Ejection Fraction measurements should be taken • At least three beat loops should be recorded

12 Echotech Reporting Guidelines
Appendices
Appendix 1
Herceptin• BSE Guidelines state that patients should not be commenced on Herceptin (Trastuzumab)³ if their baseline EF is ≤ 55%• If the EF falls by more than 10% or to < 50%, referral to a Cardiologist should be suggested on the echo report• Accurate measurement of EF is required as a 10% change in EF should reflect a ‘true’ change• To assist the accurate measurement of EF, the use of (biplane) Simpson’s Rule Method is required [if this is not possible, then referral to the Secondary Care Cardiology Dept is appropriate]• To track the EF for serial echocardiograms, a folder for the Herceptin patients will be kept within the echo file
Appendix 2
Left ventricular hypertrophy due to hypertensive heart disease • Wall thickness rarely exceeds 2cm • Pattern LVH usually concentric but may be ASH • SAM and LVOTO less common but may occur • LVEF rarely > 65% • Often distinguishing HCM from Hypertensive heart disease very difficult and requires clinical features, ECG, ETT, 24 hour ECG, CMR
Features of physiological left ventricular hypertrophy (athletes heart) • LV wall thickness rarely exceeds 1.6cm • LVH pattern concentric with < 2mm difference between LV segments • LVEDD often 5.5 – 6.5cm (HCM LVEDD rarely > 4.5cm) • LVOTO and SAM rare • Ea usually > 9 cm/sec
Appendix 3
Echo Exclusion Criteria
• Age less than 16 • Known congenital heart disease • A congenital disorder in which cardiac disease may be suspected E.g. Down’s syndrome, Noonan’s syndrome, William’s disease
Appendix 4
Congenital Assessment
ASD Check atrial septum visually & with colour from all possible views i.e. SAX (AV level), 4 chamber & subcostal (4ch & SAX)Turn colour scale down (i.e. 54) to stop low velocity signals being missedRecord subcostal views on inspiration & expiration, as PFO’s are sometimes missed on inspiration aloneMeasure right heart size, ideally from 4 chamber view, but visually assess from all viewsIf possible measure the shunt velocity (in m/s) & size (in mm) of the defect
VSD Check ventricular septum visually & with colour from all possible views i.e. PLAX, SAX (all levels), 4 chamber & subcostalTurn colour scale down (i.e. 54) to stop low velocity signals being missedImportant to measure LV dimensions (Normally right heart is normal size)Measure the shunt velocity (in m/s)
13 Echotech Reporting Guidelines
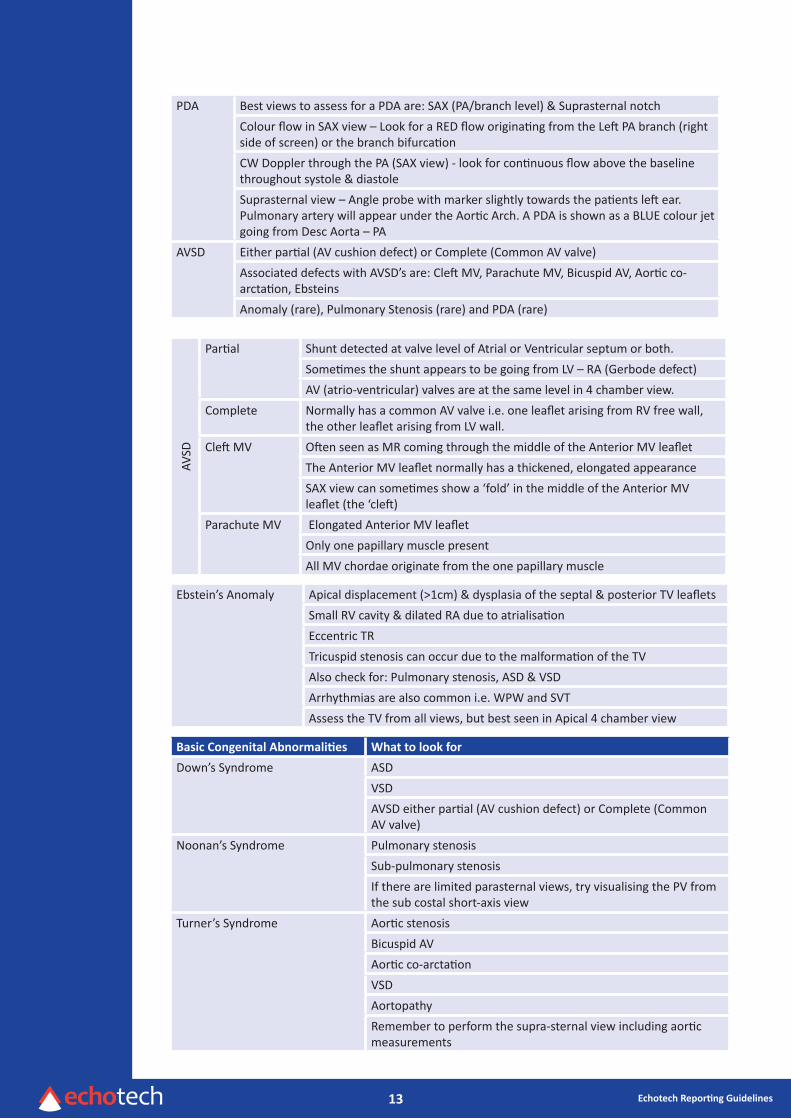
PDA Best views to assess for a PDA are: SAX (PA/branch level) & Suprasternal notchColour flow in SAX view – Look for a RED flow originating from the Left PA branch (right side of screen) or the branch bifurcationCW Doppler through the PA (SAX view) - look for continuous flow above the baseline throughout systole & diastoleSuprasternal view – Angle probe with marker slightly towards the patients left ear. Pulmonary artery will appear under the Aortic Arch. A PDA is shown as a BLUE colour jet going from Desc Aorta – PA
AVSD Either partial (AV cushion defect) or Complete (Common AV valve)Associated defects with AVSD’s are: Cleft MV, Parachute MV, Bicuspid AV, Aortic co-arctation, EbsteinsAnomaly (rare), Pulmonary Stenosis (rare) and PDA (rare)
AVSD
Partial Shunt detected at valve level of Atrial or Ventricular septum or both.Sometimes the shunt appears to be going from LV – RA (Gerbode defect)AV (atrio-ventricular) valves are at the same level in 4 chamber view.
Complete Normally has a common AV valve i.e. one leaflet arising from RV free wall, the other leaflet arising from LV wall.
Cleft MV Often seen as MR coming through the middle of the Anterior MV leafletThe Anterior MV leaflet normally has a thickened, elongated appearanceSAX view can sometimes show a ‘fold’ in the middle of the Anterior MV leaflet (the ‘cleft)
Parachute MV Elongated Anterior MV leafletOnly one papillary muscle presentAll MV chordae originate from the one papillary muscle
Ebstein’s Anomaly Apical displacement (>1cm) & dysplasia of the septal & posterior TV leafletsSmall RV cavity & dilated RA due to atrialisationEccentric TRTricuspid stenosis can occur due to the malformation of the TVAlso check for: Pulmonary stenosis, ASD & VSDArrhythmias are also common i.e. WPW and SVTAssess the TV from all views, but best seen in Apical 4 chamber view
Basic Congenital Abnormalities What to look for
Down’s Syndrome ASDVSDAVSD either partial (AV cushion defect) or Complete (Common AV valve)
Noonan’s Syndrome Pulmonary stenosisSub-pulmonary stenosisIf there are limited parasternal views, try visualising the PV from the sub costal short-axis view
Turner’s Syndrome Aortic stenosisBicuspid AVAortic co-arctationVSDAortopathyRemember to perform the supra-sternal view including aortic measurements
14 Echotech Reporting Guidelines
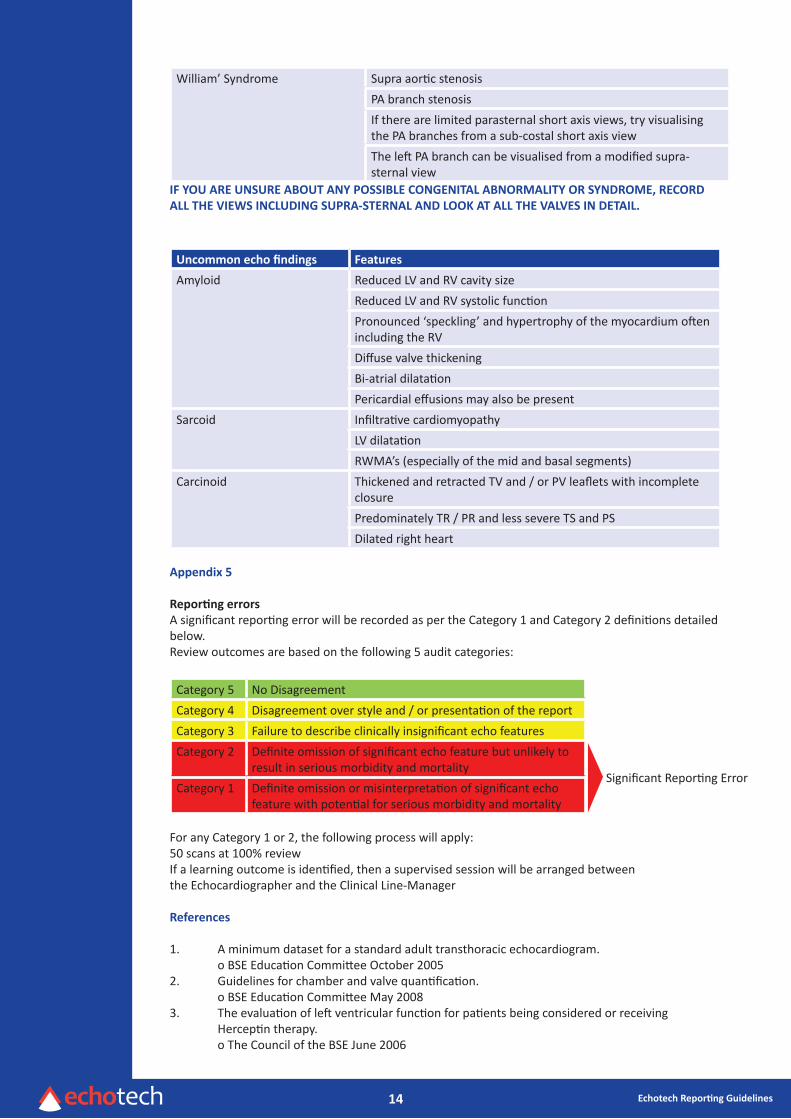
William’ Syndrome Supra aortic stenosisPA branch stenosisIf there are limited parasternal short axis views, try visualising the PA branches from a sub-costal short axis viewThe left PA branch can be visualised from a modified supra-sternal view
IF YOU ARE UNSURE ABOUT ANY POSSIBLE CONGENITAL ABNORMALITY OR SYNDROME, RECORDALL THE VIEWS INCLUDING SUPRA-STERNAL AND LOOK AT ALL THE VALVES IN DETAIL.
Uncommon echo findings Features
Amyloid Reduced LV and RV cavity sizeReduced LV and RV systolic functionPronounced ‘speckling’ and hypertrophy of the myocardium often including the RVDiffuse valve thickeningBi-atrial dilatationPericardial effusions may also be present
Sarcoid Infiltrative cardiomyopathyLV dilatationRWMA’s (especially of the mid and basal segments)
Carcinoid Thickened and retracted TV and / or PV leaflets with incomplete closurePredominately TR / PR and less severe TS and PSDilated right heart
Appendix 5
Reporting errorsA significant reporting error will be recorded as per the Category 1 and Category 2 definitions detailed below. Review outcomes are based on the following 5 audit categories:
Category 5 No DisagreementCategory 4 Disagreement over style and / or presentation of the reportCategory 3 Failure to describe clinically insignificant echo featuresCategory 2 Definite omission of significant echo feature but unlikely to
result in serious morbidity and mortalityCategory 1 Definite omission or misinterpretation of significant echo
feature with potential for serious morbidity and mortality
For any Category 1 or 2, the following process will apply:50 scans at 100% reviewIf a learning outcome is identified, then a supervised session will be arranged between the Echocardiographer and the Clinical Line-Manager
References
1. A minimum dataset for a standard adult transthoracic echocardiogram. o BSE Education Committee October 20052. Guidelines for chamber and valve quantification. o BSE Education Committee May 20083. The evaluation of left ventricular function for patients being considered or receiving Herceptin therapy. o The Council of the BSE June 2006
Significant Reporting Error





























