Embed Size (px)
Citation preview

Ectopic PregnancyEctopic Pregnancy
Dr. Yasir KatibDr. Yasir KatibMBBS, FRCSC, MBBS, FRCSC, PerinatologistPerinatologist

Introduction Introduction
Ectopic pregnancy occurs when Ectopic pregnancy occurs when the developing blastocyst becomes the developing blastocyst becomes implanted at a site other than the implanted at a site other than the endometrium of the uterine cavityendometrium of the uterine cavity
The most common extra-uterine The most common extra-uterine location is the fallopian tube, which location is the fallopian tube, which accounts for 98%accounts for 98%

Types of EPTypes of EP

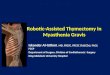
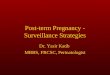
Sites of EPSites of EP
Fallopian tubeFallopian tube
AmpullaAmpulla 80%80%
IsthmusIsthmus 12%12%
Fimbrial endFimbrial end 5%5%
Cornual & interstitialCornual & interstitial 2%2%
AbdominalAbdominal 1.4%1.4%
OvarianOvarian 0.2%0.2%
CervicalCervical 0.2%0.2%
Heterotopic Pregnancies: 1 in 30 000

EpidemiologyEpidemiology 22ndnd leading cause of overall maternal mortality leading cause of overall maternal mortality
in USin US
Leading cause of pregnancy-related deaths Leading cause of pregnancy-related deaths during T-1during T-1
1-2% of all diagnosed pregnancies1-2% of all diagnosed pregnancies

EpidemiologyEpidemiology
Incidence is Incidence is incidence of salpingitis d/t chlamydia or incidence of salpingitis d/t chlamydia or
other STIother STI Improved diagnostic techniquesImproved diagnostic techniques ageage Blacks >non-whites>whitesBlacks >non-whites>whites
Most occur in multigravid women Most occur in multigravid women > 50% in women with > 50% in women with 3 pregnancies 3 pregnancies
10-15% in nulligravid women10-15% in nulligravid women

MortalityMortality
Causes 15% of maternal deathsCauses 15% of maternal deaths Overall risk of death 10X > the risk of Overall risk of death 10X > the risk of
childbirth; 50X > risk of legal abortionchildbirth; 50X > risk of legal abortion Cause of death dueCause of death due
blood loss (80%)Iblood loss (80%)I infection (3%)infection (3%) anesthesia (2%)anesthesia (2%)
Interstitial & abdominalInterstitial & abdominal 5X > risk of 5X > risk of death than other sitesdeath than other sites

Of Historical Note…….Of Historical Note…….
16931693 11stst documentation of unruptured ectopic documentation of unruptured ectopic
17521752 Infertility linked to EPInfertility linked to EP
mid 19mid 19thth century century Path reports stressed pelvic inflammation Path reports stressed pelvic inflammation
as cause of EPas cause of EP 1800s1800s
30 abd operations in (5 women survived)30 abd operations in (5 women survived) If not treated, 1 out of 3 survived (better!)If not treated, 1 out of 3 survived (better!)

Risk Factors for EPRisk Factors for EP
Definite (high risk)Definite (high risk) Previous EPPrevious EP Any tubal surgery or sterilization Any tubal surgery or sterilization
procedureprocedure In-utero DES exposure In-utero DES exposure

Risk Factors for EPRisk Factors for EP
Probable (modrate risk)Probable (modrate risk) PIDPID InfertilityInfertility ““Superovulating agents” Superovulating agents”
Pergonal, Clomiphene citratePergonal, Clomiphene citrate Multiple sexual partners Multiple sexual partners Smoking Smoking

Risk Factors for EPRisk Factors for EP
Uncertain Association (low risk)Uncertain Association (low risk) IUCDIUCD Vaginal douching Vaginal douching Maternal age (extremes)Maternal age (extremes) Use of reproductive techniquesUse of reproductive techniques
In vitro fertilizationIn vitro fertilization Gamete intrafallopian transferGamete intrafallopian transfer Embryo transferEmbryo transfer

Classic TRIAD of EPClassic TRIAD of EP
1.1. Delayed mensesDelayed menses
2.2. Irregular vaginal bleedingIrregular vaginal bleeding
3.3. Abdominal painAbdominal pain
Most commonly Most commonly NOT NOT encountered encountered

Symptoms of Ectopic Symptoms of Ectopic PregnancyPregnancy
SYMPTOMSYMPTOM PTS WITH PTS WITH SYMPTOMSYMPTOM
Abdominal painAbdominal pain 90-100%90-100%
AmenorrheaAmenorrhea 75-95%75-95%
Vaginal bleedingVaginal bleeding 50-80%50-80%
Dizzininess, faintingDizzininess, fainting 20-35%20-35%
Pregnancy symptomsPregnancy symptoms 10-25%10-25%
Urge to defecateUrge to defecate 5-15%5-15%
Passage of tissuePassage of tissue 5-10%5-10%

Signs of EPSigns of EPSIGNSIGN PTS WITH SIGNPTS WITH SIGN
Adnexal tendernessAdnexal tenderness 75-90%75-90%
Abdominal tendernessAbdominal tenderness 80-95%80-95%
Adnexal mass*Adnexal mass* 50%50%
Uterine enlargementUterine enlargement 20-30%20-30%
Orthostatic changesOrthostatic changes 10-15%10-15%
FeverFever 5-10%5-10%
* 20% of masses occur on the side opposite the EP.

Differential DiagnosisDifferential Diagnosis Complication of IUPComplication of IUP
AbortionAbortion Early pregnancy plus uterine fibroid or Early pregnancy plus uterine fibroid or
ovarian tumourovarian tumour Conditions causing acute abd painConditions causing acute abd pain
Torsion of ovarian tumour, FT, or subserous Torsion of ovarian tumour, FT, or subserous pedunculated fibroidpedunculated fibroid
Salpino-oophoritisSalpino-oophoritis Pelvic pain with an IUCD Pelvic pain with an IUCD in situin situ Appendicitis Appendicitis

Differential Dx – cont’dDifferential Dx – cont’d
Conditions causing Conditions causing hemoperitoneumhemoperitoneum Ruptured corpus luteumRuptured corpus luteum Ruptured follicular cystRuptured follicular cyst Ruptured endometriotic cystRuptured endometriotic cyst
Conditions simulating a pelvic Conditions simulating a pelvic hematocelehematocele Retroverted gravid uterusRetroverted gravid uterus Pelvic or tubo-ovarian abcessPelvic or tubo-ovarian abcess

Management of EPManagement of EP
Pre-operative diagnostic accuracy Pre-operative diagnostic accuracy of EP based on clinical features of EP based on clinical features alone is notoriously poor: ~50%alone is notoriously poor: ~50%
20% of EP occur as surgical 20% of EP occur as surgical emergenciesemergencies
Delay is justified only to correct Delay is justified only to correct shockshock

Acute Management of EPAcute Management of EP
Remember your ABCsRemember your ABCs OxygenOxygen Large bore IV(s) Large bore IV(s) crystalloids crystalloids Blood Blood
LabsLabs CBC, coagulation studies, T & CCBC, coagulation studies, T & C -hCG-hCG

Usefulness of Quantitaive Usefulness of Quantitaive -hCG-hCG
Assessment of pregnancy viabilityAssessment of pregnancy viability Serial rise usually indicates a normal Serial rise usually indicates a normal
pregnancypregnancy Correlation with ultrasonographyCorrelation with ultrasonography
With titers > 1500 IU/L, TVUS should ID an IUPWith titers > 1500 IU/L, TVUS should ID an IUP With multiple gestation, a gestational sac will With multiple gestation, a gestational sac will
not be apparent until titer rises a little highernot be apparent until titer rises a little higher Assessment of treatment resultsAssessment of treatment results
Declining levels are c/w effective medical or Declining levels are c/w effective medical or surgical Tx; if levels persistsurgical Tx; if levels persist think GTD think GTD

The Importance of TVUSThe Importance of TVUS
Documentation of an intrauterine Documentation of an intrauterine sacsac A viable IUP should be identified when A viable IUP should be identified when
-hCG > 1500 IU/ml-hCG > 1500 IU/ml Adnexal massAdnexal mass
An EP > 2 cm should be identified An EP > 2 cm should be identified Adnexal cardiac activityAdnexal cardiac activity
Detectable when Detectable when -hCG is -hCG is ~ 15 000 – 20 000 ~ 15 000 – 20 000

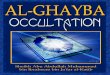
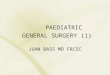
U/S – Is it EP or U/S – Is it EP or miscarriage?miscarriage?

Surgical Management of Surgical Management of EPEP
RadicalRadical Salpingectomy with/out oophorectomySalpingectomy with/out oophorectomy
ConservativeConservative Salpingotomy Salpingotomy Salpingostomy or segmental resection Salpingostomy or segmental resection
does not does not repeat EP rate repeat EP rate fimbrial evacuation (traumatizes the fimbrial evacuation (traumatizes the
endosalphinx & is assoc with endosalphinx & is assoc with rate of rate of recurrent EP (24%) compared with recurrent EP (24%) compared with salpingectomysalpingectomy

Medical Management of Medical Management of EPEP
Methotrexate (MTX)Methotrexate (MTX) 11stst used in Japan in 1982 used in Japan in 1982 Antimetabolite that interferes with Antimetabolite that interferes with
dihydrofolate reductasedihydrofolate reductase Considered for low Considered for low -hCG-hCG Success rate 67%-94%Success rate 67%-94% IndicationsIndications
Hemodynamically stable pt Hemodynamically stable pt good F/Ugood F/U Recurrent EP following Sx Recurrent EP following Sx
interventionintervention

Methotrexate – cont’dMethotrexate – cont’d ContraindicationsContraindications
Evidence of ruptureEvidence of rupture Serum Serum -hCG > 5 000 IU/L (varies)-hCG > 5 000 IU/L (varies) FH detected on U/SFH detected on U/S Adnexal mass> 3.5 cm on U/SAdnexal mass> 3.5 cm on U/S Unreliable ptUnreliable pt F/U unavailableF/U unavailable Laparoscopy required to make dxLaparoscopy required to make dx Solid adnexal masses (germ cell Solid adnexal masses (germ cell
tumour)tumour) Free fluid > 30mlFree fluid > 30ml

Methotrexate ProtocolMethotrexate Protocol
Exclude contraindications as well asExclude contraindications as well as No evidence of renal, liver, or hematopoietic No evidence of renal, liver, or hematopoietic
disease (Bilirubin, AST,ALT, urea, Cr, CBC)disease (Bilirubin, AST,ALT, urea, Cr, CBC) Informed consentInformed consent
5% risk of hematoperitoneum 25% risk of hematoperitoneum 2° to rupture of ° to rupture of EP following MTXEP following MTX
MTX 50mg/mMTX 50mg/m² body surface area ² body surface area (~1mg/kg) given IV or IM(~1mg/kg) given IV or IM

Methotrexate Protocol – Methotrexate Protocol – cont’dcont’d
Pt F/U Pt F/U repeat serum quantitative repeat serum quantitative -hCG in 3-4 -hCG in 3-4
days, 7days, then weekly until < 10 IU/Ldays, 7days, then weekly until < 10 IU/L If > day-4 level at day-7 If > day-4 level at day-7 repeat MTX repeat MTX If If -hCG fails to fall by at least 25%/week -hCG fails to fall by at least 25%/week
at any timeat any time repeat dose repeat dose U/S not required routinelyU/S not required routinely
Pt should avoidPt should avoid Alcohol use, sexual I/C, oral folic acid (until Alcohol use, sexual I/C, oral folic acid (until
HCG levels are neg)HCG levels are neg)

Methotrexate Protocol – Methotrexate Protocol – cont’dcont’d
What to expectWhat to expect Majority experience some degree of abd Majority experience some degree of abd
pain (occurs in ~ 50% at day-6)pain (occurs in ~ 50% at day-6) Shedding of a decidual castShedding of a decidual cast Moderate vaginal bleedingModerate vaginal bleeding
Side effects (usually at higher doses)Side effects (usually at higher doses) Impaired liver function, bone marrow Impaired liver function, bone marrow
suppression, neutropenia, stomatitis, suppression, neutropenia, stomatitis, hematosalpinxhematosalpinx

Expectant Mx of EPExpectant Mx of EP
Anticipates spontaneous regression of EPAnticipates spontaneous regression of EP Occurs in ~ 57%Occurs in ~ 57% Symptoms, HCG titers, & U/S findings Symptoms, HCG titers, & U/S findings
followedfollowed Risk of tubal rupture is 10% if HCG levels < Risk of tubal rupture is 10% if HCG levels <
10001000 Criteria includeCriteria include
Sonographic diameter < 3cmSonographic diameter < 3cm Initial Initial -hCG < 1 000 IU/ml, no -hCG < 1 000 IU/ml, no in 2-day in 2-day
period, subsequent levels period, subsequent levels asymptomaticasymptomatic

Future Fertility following Future Fertility following EPEP
Subsequent conception rate is ~ 60%Subsequent conception rate is ~ 60% Incidence of recurrent EP is 15%Incidence of recurrent EP is 15% Other factors influencing include:Other factors influencing include:
Age, parity, history of infertility, Age, parity, history of infertility, evidence of contralateral tubal disease, evidence of contralateral tubal disease, ruptured EP, IUCD use, salpingitisruptured EP, IUCD use, salpingitis
No difference b/t laparoscopy vs No difference b/t laparoscopy vs laparotomylaparotomy

Prevention of EPPrevention of EP
Treat salpingitis early & correctlyTreat salpingitis early & correctly MTX management lowers rate of MTX management lowers rate of
subsequent EPsubsequent EP Risk of EP is Risk of EP is with all methods of with all methods of
contraception, except progesterone contraception, except progesterone containing IUCDscontaining IUCDs
Remember Rh SensitizationRemember Rh Sensitization Rhogam for the Rh-neg womanRhogam for the Rh-neg woman