Embed Size (px)
Citation preview
ED Management of Falls in the Geriatric PopulationJennifer Oman, MD, MBAClinical Professor of Emergency MedicineUC Irvine School of Medicine
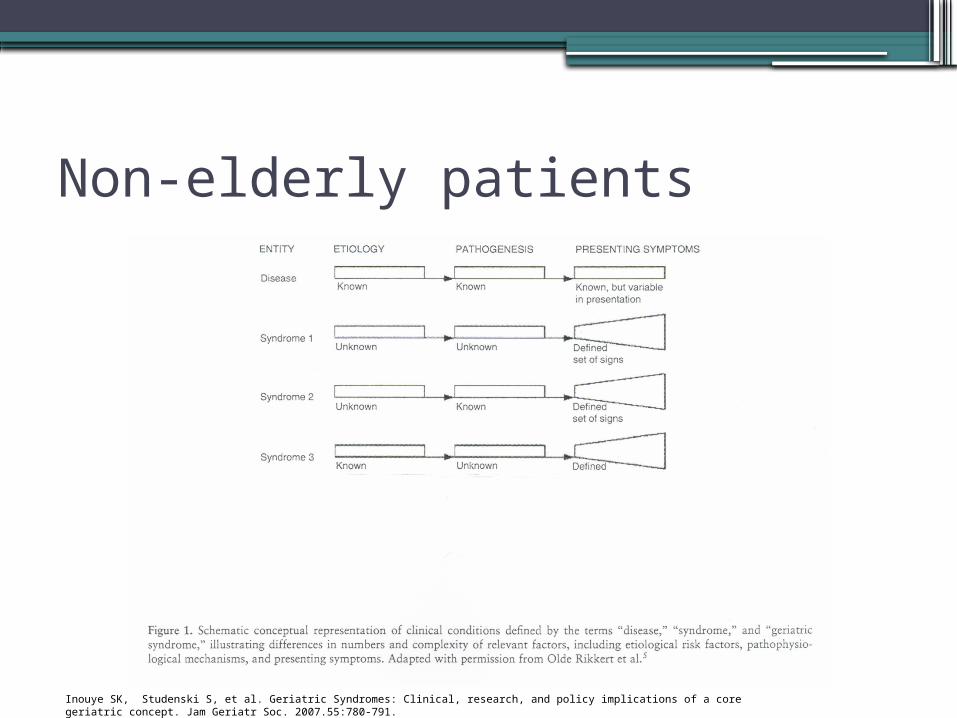
Non-elderly patients
Inouye SK, Studenski S, et al. Geriatric Syndromes: Clinical, research, and policy implications of a core geriatric concept. Jam Geriatr Soc. 2007.55:780-791.
Geriatric Syndromes
•Elderly do not have single disease category•Significant impact on quality of life•Multiple underlying factors and multiple
organ systems
Inouye SK, Studenski S, et al. Geriatric Syndromes: Clinical, research, and policy implications of a core geriatric concept. Jam Geriatr Soc. 2007.55:780-791.

Geriatric Disease
Geriatric Syndromes
•Delirium•Falls•Frailty•Syncope•Dizziness•Urinary incontinence

Did you know?
•Roughly one third of older individuals over the age of 65 fall every year
•More than half of older adults living in institutions fall every year
•Half of the older individuals who fall have repeated falls
Kannus P, Parkkari J et al. Fall induced injuries and deaths among older adults. JAMA. 1999; 281: 1895-1899.
Did you also know?
•The fall may represent the initial event in an elder adults life▫Beginning of serious decline▫New or worsening medical illness
•More than 2/3 of those that fall will fall again in 6 months
•If hospitalization, risk of death in the year following the fall is 15%-50%
Baraff LJ, Della Penna R et al. Practice guideline for the ED management of falls in community dwelling elderly persons. Ann emerg Med. Oct 1997; 30:480-489.

What we will discuss
•Evaluation after the fall•Prevention of future falls
Evaluation
•Some falls result in serious injury•First things first•Stabilize and treat emergent conditions
Evaluation•And sometimes the patient’s condition
gives you more time to take the history •Cause of the fall•Location of the fall•Long lie•Medications•Functional status•Medical problems
And they wouldn’t call us ED Docs if we didn’t consider
Was this syncope?
Evaluation
•Physical Exam specifics▫Vital signs▫Get-up-and-go-test
History in the Elderly
•Present with more than one problem•They overestimate their own healthiness:
they explain away or minimize symptoms or problems – explain away as normal aging
•Under-reporting of symptoms is common•Use ancillary sources of history--- family,
caregiver•Develop problem list rather than chief
complaint
Evaluation• Cause of the fall
▫50% will tell you they tripped• Location of the fall
▫Only the precipitant of the fall▫Have they fallen in the previous 3 months?▫Don’t overlook underlying etiology
• Long lie (>5 minutes)▫Ask if they were able to get up unassisted▫ If needed assistance more likely to sustain
decline in ADLs, be hospitalized or die earlyKannus P, Parkkari J. fall induced injuries and deaths among older adults. JAMA1999;281:1895-1899

Medications
•Medications•Use of 4 or more prescription medications •Which drugs?
▫The usual suspects- neuroleptic agents, benzodiazapines, anticonvulsants, cardiovascular drugs (antihypertensives)
▫SSRIs▫Tricyclics
Tinetti, ME. Preventing falls in elderly persons. N Engl J Med. 2003; 348:1. 42-49.
Functional Status
•Verify functional status•Do they live alone?•Are they able to carry out activities of
daily living for themselves?•If in a care facility, what is their baseline
transfer and mobility?
Medical Problems
•Urinary frequency or incontinence•Alcohol use•Special considerations:
▫Blood thinners
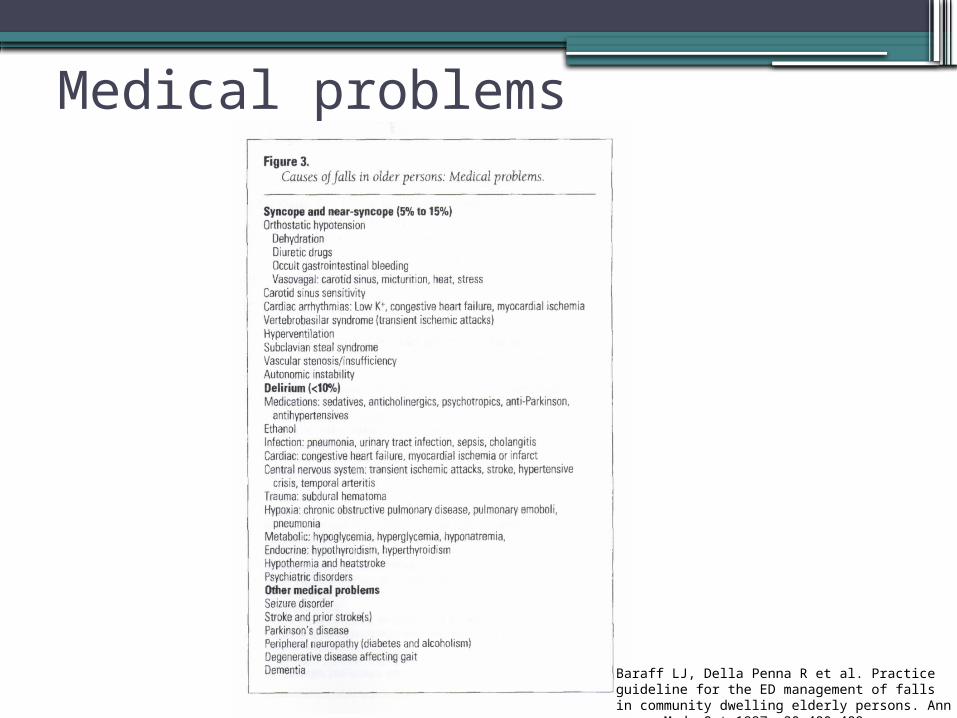
Medical problems
Baraff LJ, Della Penna R et al. Practice guideline for the ED management of falls in community dwelling elderly persons. Ann emerg Med. Oct 1997; 30:480-489.
Syncope?
•Tips for eliciting the history of syncope•Ask multiple ways
▫Is there a period of time you don’t remember
▫Go through the events for me•Ask multiple times
Syncope?
•Bystanders….•Just like on the board exam- don’t let the
medics or witnesses leave until you have gotten the information they know!
•Make sure you talk to everyone possible even if that means calling the SNF or patient’s home or relative/friend
•Only sometimes helpful

Caveats to believing the bystander• All shaking is not a seizure
▫Mild brief tonic-clonic activity can occur with any etiology of syncope
▫Cerebral hypoperfusion• Orthostatic vital signs in the elderly population are
helpful▫Found in up to 40% or asymptomatic patients over
70 and 23% of those younger than 60• Patients will adopt the bystanders interpretation of
the event
Huff JS, Decker WW et al. Clinical policy; critical issues in the evaluation and management of adult patients presenting to the emergency department with syncope. Ann Emerg Med. 2007;49:431-444.

Physical Exam
•Vital signs are vital but ….•Remember the elderly may not mount a
fever even in the face of significant infection
•Heart rate may be artificially low for their status if on beta blockers
•Systolic hypertension is common- may not demonstrate hypotension
Physical Exam
•Orthostatics: maybe yes maybe no•Largely abandoned in the ED•May have asymptomatic orthostasis
▫Found in up to 40% or asymptomatic patients over 70 and 23% of those younger than 60
•Will still see it recommended but its usefulness in the ED is debatable
Physical Exam
•Nutritional status:▫Subcutaneous fat and temporal wasting▫May suggest underlying physical or mental
illness•Mental Status:
▫Determine if change from baseline▫May have delirium, dementia or psychiatric
illness▫Delirium could be a cause of a fall or a
result of the fall
Dementia vs Delirium
•Dementia- a fall in the intellectual ability from a person’s previous level of performance causing an altered pattern of activity in the setting of normal consciousness
•Delirium- a disorder of attention▫Cognitive impairment with an acute onset
or fluctuating course▫Inattention or difficulty maintaining focus▫Disorganized thinking
Rule out Dementia
•Mini cog•Three item recall and draw a clock• If the patient is able to recall all 3 items-
you are done – likelihood ratio of dementia <0.1
• If the Patient is unable to recall a single item- the likelihood ratio for dementia is 14- also done
• If able to recall 1 or 2 items have them draw a clock. If clock normal likelihood ratio for dementia is 0.14. If abnormal the likelihood ration for dementia is 10-14
Delirium
•VAMPIRE▫ Vitals▫ Acute events ( MI, PE, CVA)▫ Medications (sedative hypnotics, pain
medication, drug-drug interactions)▫ Pain control▫ Infections (UTI)▫ Restricted mobility▫ Environment (sleep deprivation, vision
impairment, hearing impairment)

Rule in delirium
• Confusion assessment method (CAM)• Need
▫1. Acute onset symptoms or mental status changes of fluctuating course and
▫2. inattention • Also need either
▫3. disorganized thinking or▫4. altered consciousness (other than alert)
Inouye SK, van Dyck CH, Alessi CA, et al.Clarifying confusion: The confusion assessment method. Ann Intern Med 1990; 113:941–948
Rule in delirium
• CAM positive- meaning your patient has delirium- if 1 and 2 present and either 3 or 4
•>94% sensitive and 90-95% specific for diagnosing delirium
Physical Exam
•Specific cardiopulmonary exam•And finally- look for injuries•Multiple old and new injuries should
make you think of abuse
Get-up-and-go-test
•Tests gait, strength and balance•Evaluates for symptomatic orthostasis •Rules out lower extremity, pelvic and
spine injury•Lowers suspicion of intracranial
pathology
Get-up-and-go-test
•Have patient get up from gurney•Once sitting must get up without using
arms •Walks a few feet and returns•High risk for subsequent falls if unable to
perform
Prevention of future falls
•Some interventions may be done in the ED
•Guidance to patients and families as to what to expect/ measures to take to help prevent future falls
•Make appropriate referrals
ED interventions
•Medication assessment▫Benzos or sedatives, antihypertensives
•Alcohol screening•Discussion about potential risks at home-
at least given in discharge instructions•Referral for assessment
▫More than 4 prescription medications▫One previous fall in the preceding 3 months▫A long lie or assistance to get up from a fall▫Multiple medical problems
ED Management of falls in the Elderly- Pearls•The elderly do not have discrete cause
and effect illness– multi-factorial•Half of the older individuals who fall have
repeated falls- opportunity to affect quality of life as and ED MD
•Don’t forget to address not only immediate injuries but the causes of the fall
•Remember to evaluate functional status

ED Management of falls in the Elderly- Pearls•Beware the bystander/eye witness•Convince yourself the fall wasn’t syncope•Rule out dementia and rule in delirium
▫CAM, clock assessment•Perform the get-up-and-go-test•Referral for assessment
▫More than 4 prescription medications▫One previous fall in the preceding 3 months▫A long lie or assistance to get up from a fall▫Multiple medical problems





























