Embed Size (px)
Citation preview

Edema & Proteinuria
Complications of overtreatment
• A 47-Yr-old woman with a history of intermittent and reversible swelling in her feet and ankle since 10 years ago ,underwent medical examination at primary care physician office when this Edema did not reverse and weight gain from 74 to 82.
• PMH: DM(-) HTN(-) HLP(-) Pulmonary D(-) IHD(-) Thyroeid D(-)
• DH:NO any special drugs such as Non steroidal anti-inflamatory agent & diuretics
• HH:NO Addiction• V.S: Bp:120/85mmhg PR:82 RR:14
• P/E: HEENT No palor ,No Icter No Thyromegaly ,No LAP , NL JVP• Heart:NL sounds-
NLrate&rhythm,no murmur• Lung: Bilateral clear• Abdomen:Soft,No mass or
organomegaly,No ascitis• EXT: 2+ Pitting Edema to knee
Increased capillary hydraulic pressure
A. Increased plasma volume due to renal Na+ retention 1. Heart failure, including cor pulmonale 2. Primary renal sodium retention a. Renal disease, including the nephrotic syndrome b. Drugs: minoxidil, diazoxide, thiazolidinediones, calcium channel blockers (particularly nifedipine), nonsteroidal anti-inflammatory drugs, fludrocortisone, estrogens c. Refeeding edema d. Early hepatic cirrhosis 3. Pregnancy and premenstrual edema 4. Idiopathic edema, when diuretic induced
Increased capillary hydraulic pressure
B. Venous obstruction 1. Cirrhosis or hepatic venous obstruction 2. Acute pulmonary edema 3. Local venous obstruction C. Decreased arteriolar resistance 1. Calcium channel blockers (?) 2. Idiopathic edema (?)
Hypoalbuminemia
A. Protein loss1. Nephrotic syndrome2. Protein-losing enteropathyB. Reduced albumin synthesis1. Liver disease2. Malnutrition
Increased capillary permeability
A. Idiopathic edema (?)B. BurnsC. TraumaD. Inflammation or sepsisE. Allergic reactions, including certain forms of angioedemaF. Adult respiratory distress syndromeG. Diabetes mellitusH. Interleukin-2 therapyI. Malignant ascites
Lymphatic obstruction or increased interstitial oncotic pressure
A. Lymph node dissection
B. Nodal enlargement due to malignancy
C. Hypothyroidism D. Malignant ascites
Uncertain mechanism
A. Docetaxel B. Pramipexole
The history is clearly important, and several general questions
should be addressed
CLINICAL MANIFESTATIONS AND DIAGNOSIS
Is there a history of any disorder(eg):• coronary disease• hypertension• alcohol abuse or drug that can cause cardiac, hepatic, or renal disease?
Where is the edema located?• Patients with a primary complaint of
shortness of breath may have left heart failure and pulmonary edema
• those with ascites may have cirrhosis• those with only peripheral edema may
have right-sided heart failure, pericardial disease, renal disease, or local venous or lymphatic disease
Is the edema intermittent or persistent?
Intermittent edema is a common premenstrual symptom. Some women are given chronic diuretic therapy for this disorder; such treatment is not necessary and can produce a form of diuretic-dependenc that accounts for some cases of idiopathic edema.
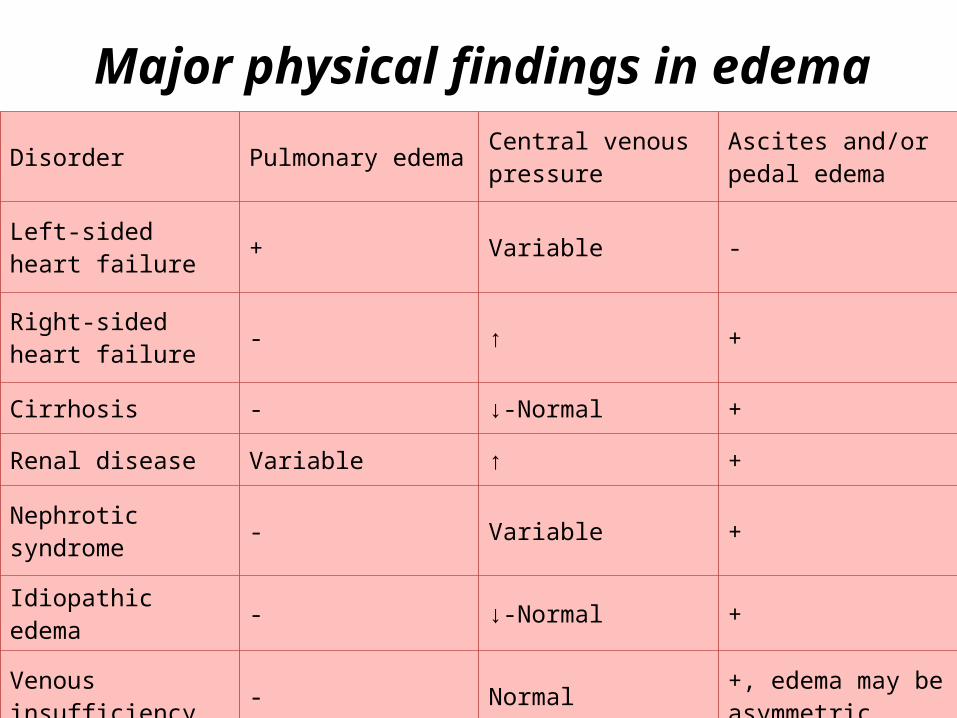
Major physical findings in edemaDisorder Pulmonary edema Central venous
pressure Ascites and/or pedal edema
Left-sided heart failure + Variable -
Right-sided heart failure - ↑ +
Cirrhosis - ↓-Normal +
Renal disease Variable ↑ +
Nephrotic syndrome - Variable +
Idiopathic edema - ↓-Normal +
Venous insufficiency - Normal +, edema may be asymmetric
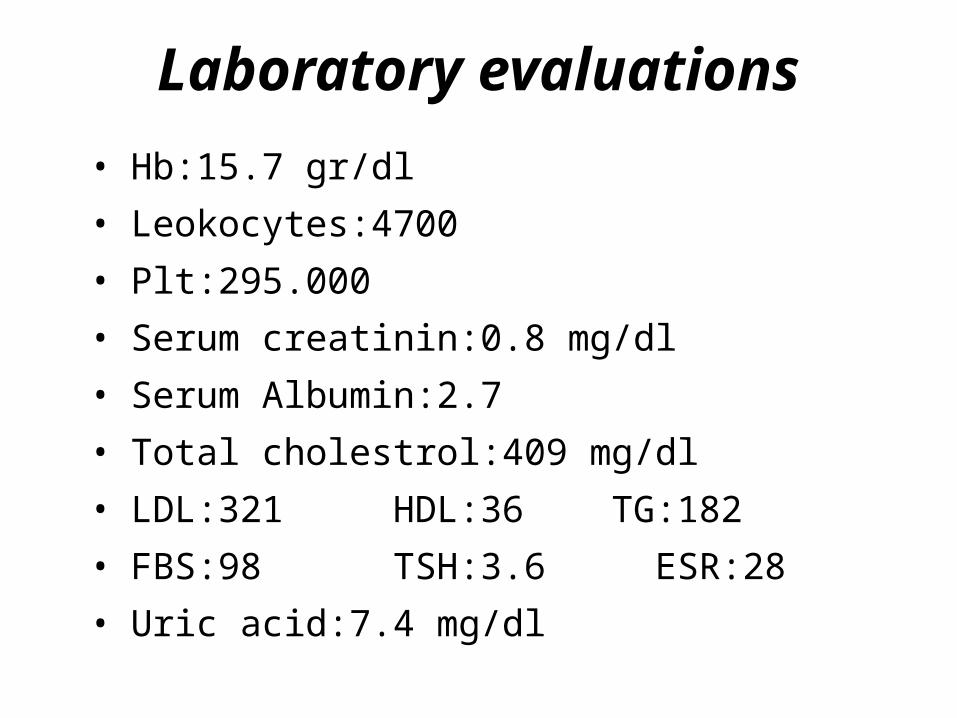
Laboratory evaluations
• Hb:15.7 gr/dl• Leokocytes:4700• Plt:295.000• Serum creatinin:0.8 mg/dl• Serum Albumin:2.7• Total cholestrol:409 mg/dl• LDL:321 HDL:36 TG:182• FBS:98 TSH:3.6 ESR:28• Uric acid:7.4 mg/dl
• Urine Analysis showed 3+ proteinuria,without any RBC or RBC cast.• 24 hr urine collection showed
3600 mg protein exertion.
• Renal ultrasound showed both kidney normal in size and echotexture and negative for hydronephrosis or mass.
• Alsow ultrasound showed :liver and spleen had normal size and echo.
• Renal vein were patent bilateraly.• CXR was normal.• Echocardiography showed normal systolic and diastolic
function without any valvular disease.
Nephrotic syndrom presentation
• nephrotic-range proteinuria (≥3.5 g/day)• hyperlipidemia• edema• hypoalbuminemia • and/or an active urine sediment
containing red cells (which are often dysmorphic) and red cell casts.
• GFR may be decreased
• Patients with the nephrotic syndrome with a nephrotic pattern in the urinalysis may have :
• primary renal disease: • minimal change disease• focal segmental glomerulosclerosis• membranous nephropathy• systemic disorder that affects the kidneys • Lupus• amyloidosis• hepatitis B or C virus infection, or HIV infection
Mild glomerulonephritisActive urine sediment without renal insufficiency or nephrotic syndrome
•Less than 15 years of age - Mild postinfectious glomerulonephritis, IgA nephropathy, thin basement membrane disease, hereditary nephritis, Henoch-Schönlein purpura, mesangial proliferative glomerulonephritis
•15 to 40 years of age - IgA nephropathy, thin basement membrane disease, lupus, hereditary nephritis, mesangial proliferative glomerulonephritis
•Greater than 40 years of age - IgA nephropathy
Moderate to severe glomerulonephritis
Active urine sediment with renal insufficiency and variable proteinuria, which can include nephrotic syndrome
•Less than 15 years of age - Postinfectious glomerulonephritis, membranoproliferative glomerulonephritis
•1years of age 5 to 40 - Postinfectious glomerulonephritis, lupus, rapidly progressive glomerulonephritis, fibrillary glomerulonephritis, membranoproliferative glomerulonephritis
•Greater than 40 years of age - Rapidly progressive glomerulonephritis, vasculitis (including mixed cryoglobulinemia), fibrillary glomerulonephritis, postinfectious glomerulonephritis
Nephrotic syndrome
Heavy proteinuria, bland sediment although some hematuria allowed
•Less than 15 years of age - Minimal change disease, focal glomerulosclerosis, mesangial proliferative glomerulonephritis
•15 to 40 years of age - Focal glomerulosclerosis, minimal change disease, membranous nephropathy (including lupus), diabetic nephropathy, preeclampsia, postinfectious glomerulonephritis (later stage)
•Greater than 40 years of age - Focal glomerulosclerosis, membranous nephropathy, diabetic nephropathy, minimal change disease, IgA nephropathy, primary amyloidosis or the related disorder light chain deposition disease (which can account for 15 to 20 percent of cases in patients over the age of 60), benign nephrosclerosis, postinfectious glomerulonephritis (later stage)
• After a patient has been identified as having proteinuria, a careful medical history and physical exam may reveal secondary cause such as:• diabetes mellitus• malignancy• systemic autoimmune disease• prior history of kidney disease
• The subsequent evaluation of patients with persistent isolated proteinuria usually involves referral to a nephrologist and, depending upon the degree of proteinuria and the results of other tests, a kidney biopsy .
Role of kidney biopsy
• In all patients with proteinuria of more than 3 g/day (ie, nephrotic range)
• non-nephrotic proteinuria is associated with an active urine sediment (ie, hematuria or cellular casts) or decreased GFR.
Role of kidney biopsy
In isolated non-nephrotic proteinuria, a kidney biopsy is indicated when the degree of proteinuria increases and persists above 1 g/day or new glomerular hematuria, hypertension, or a reduction in estimated GFR.
Role of kidney biopsy
kidney biopsy may be helpful in patients with isolated non-nephrotic proteinuria to diagnose a suspected systemic process if the diagnosis cannot be made reliably any other way.
…Our paitent underwent serologic workup including:
Monoclonal proteins studies Serum complement level Anti nuclear antibody Hepatitis B &C &HIV serology.
AND all of which were negative or in the normal range.
The patient was treated with• low sodium diet(<2g/d).• low protein diet(0.8 g/kg /day).• atorvastatin 20mg/d• losartan 25mg/d• Furosemide 20mg/BidShe was alsow recommended that she undergo a kideny biopsy to delineate further the diagnosis.
• She went undergun kidney biopsy when her proteinuria was 2.5g/day,but creatinin clearance was normal .
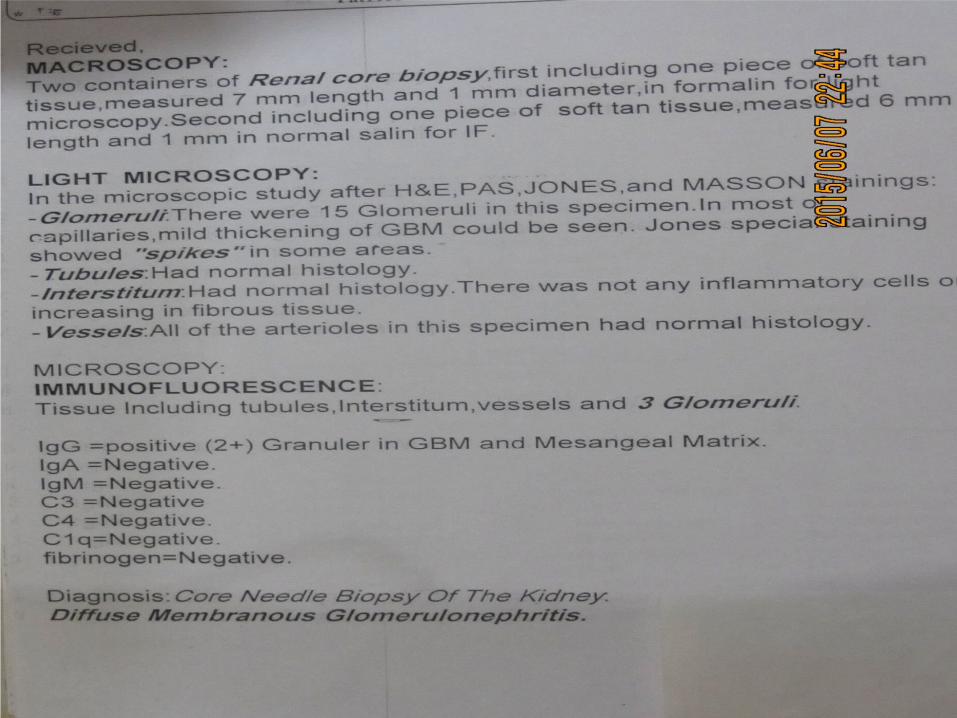
Diagnosis
Diffuse Membranous Glomerolonephritis
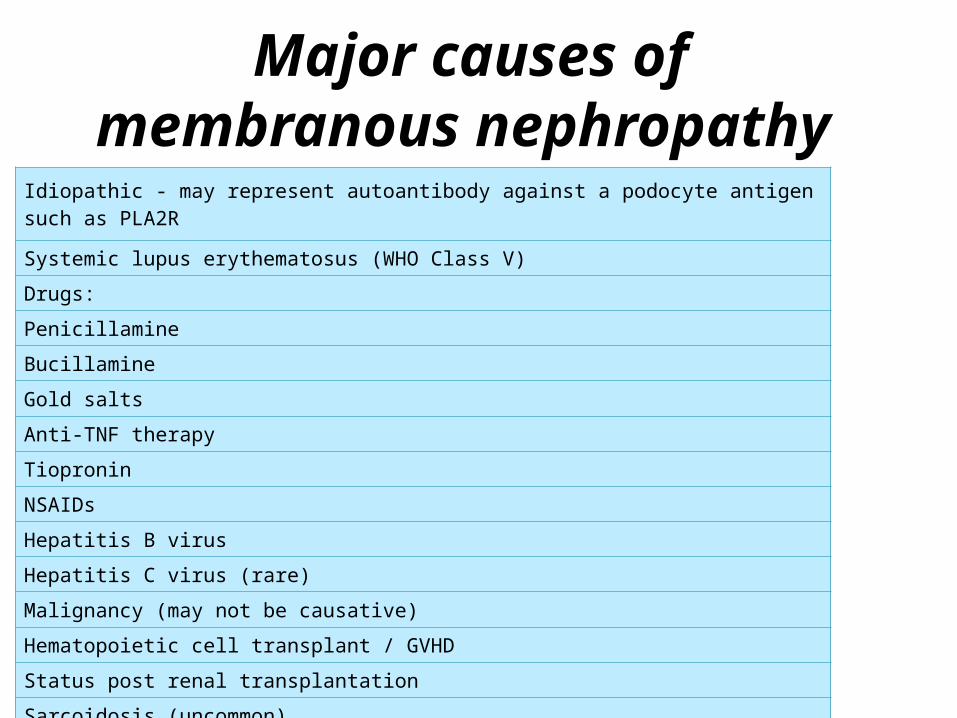
Major causes of membranous nephropathy
Idiopathic - may represent autoantibody against a podocyte antigen such as PLA2R
Systemic lupus erythematosus (WHO Class V)
Drugs:
Penicillamine
Bucillamine
Gold salts
Anti-TNF therapy
Tiopronin
NSAIDs
Hepatitis B virus
Hepatitis C virus (rare)
Malignancy (may not be causative)
Hematopoietic cell transplant / GVHD
Status post renal transplantation
Sarcoidosis (uncommon)
Secondary workups done• Anti nuclear antibody• Anti double stranded –DNA• HBV,HCV serology• All were negative.
•Mammography showed:No • evidence of suspicious mass or• pathologic microcalcifications.
• PAPANICOLAOU smear was normal.
• At last with no evidens for any underleing disease• Our diagnosis for this patient
was: IMN
• In this stage we recommended her to continue :• ARB agent (losartan 25mg/d)• Diuretic agents (furosemid 20mg tds
& spironolacton 25mg/d)• Statin (atorvastatin 20mg/d)• And follow up…
•….BUT
• She went to another medical center near our province and received another treatment include:
• Prednisolon 25mg/d &• Cyclosporin 100mg/d for one
month….
• After that her laboratory tests :• WBC COUNT:9600• Hb:13.6 g/dl• PLT:270.000• CR:0.6 mg/dl TG:376 mg/dl• Chol:329 mg/dl Ca:8.5 mg/dl• FBS:181 mg/dl HbA1C:7.1%• 24 h urine protein collection:• 2400 mg/d
• Her physicion change her drug to:• Prednisolon 12.5mg/d• Cyclophosphamide(ENDOXAN)/d
• ONE month after beigining this cytotoxic drug…
• She catched fever,shake,myalgia and sweating.• She took several outpatient
antibiotic therapy and at last with • development of Dyspnea,Productive
cough,Fever,shake,sweating ,mild Hemoptesis and reduction in urine output …
•She admited in the NEPHROLOGY department.
• On admision time her vital sign:
• Blood pressure:90/60 mmhg• Puls rate:110/min• Respiratory rate:28/min• Tempreture:40 dcg• O2saturation:87%
• Physical examinations:• Head & Neck:• Conjunctive:pale • Sclera was not icteric• No lymphadenopathy• Throat had purulent postnasal
discharge• JVP was not up
• CHEST• Heart:normal S1&S2,NO murmur• Lung:Bilateral inspiratory coarse
crackle specially on the base of the right lung.• Abdomen: soft. No organomegaly&
No tenderness• Extrimity:Bilateral 3+ pitting edema• Nervous sys & cranial n.:nl
• Paraclinic & Lab data on admition• WBC:800 Hb:8.4 Plt:197.000• Urea:125 Cr:4.96 Na:128• K:5.4 Ca:9.2 P:5.4• ESR:98 Serum Alb:3.2• LDH:752 LFT:NL• HbA1C:9.1 U/A:3+ PROTEINURIA• 24 h urine protein:2300 mg
• THEN by diagnosis of:• sever pneumosepsis & septic
shock• Broad Spectrum Antibiotics• Started for her and
cyclophosphamide Discontinued.• She resusitated with adequate IV
fluid .
• She alsow received • GCSF(granulocyt stimulating
factor)• Hydrocortison• EPO(erythropoetin stimulating
hurmon) &• Ca-co3 for phosphate binding.
• Kidney ultrasound was normal.• Venous Doppler sonography did
not show any thrombosis.• Echocardiography Ruled out
endocarditis & cardiac systolic & diastolic function was normal• Spiral chest CTscan:Consolidation
with airbronchogram in LLL & RLL.
• Her symptoms dyspnea,cough,fever improved better and lab data changed.• Cr reduced from 4.96 to 1 mg/dl• WBC:4.500• Hb:10• Plt:356.000
• She Discharged from hospital in stable condition and recommended to follow up 2 weeks later
• NOW after 8 weekes from discharge she is in a good healthy state and lab data are:• U/A: protein Trace • Cr:0.8 FBS:83 Serum Alb:3.6• WBC:5200 Hb:12.9 Plt:265000• 24 h urine protein:1050 mg/d
Side effects of cyclophosphamide• Dermatologic: Alopecia• Endocrine & metabolic:
Amenorrhea, azoospermia, gonadal suppression, oligospermia, oogenesisimpaired, sterility
• Gastrointestinal: Abdominal pain, anorexia, diarrhea, mucositis, nausea/vomiting (dose-related), stomatitis
• Genitourinary: Hemorrhagic cystitis
• Hematologic: Anemia, leukopenia (dose-related; recovery: 7-10 days after cessation), myelosuppression, neutropenia, neutropenic fever, thrombocytopenia