Embed Size (px)
Citation preview

EditorialCerebral Vasospasm after Aneurysmal SubarachnoidHemorrhage: Mechanism and Therapies
Chih-Lung Lin,1,2 Aaron S. Dumont,3 John H. Zhang,4 Mario Zuccarello,5 and Carl Muroi6,7
1 Department of Neurosurgery, Kaohsiung Medical University Hospital, Kaohsiung 807, Taiwan2 Faculty of Medicine, Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung 807, Taiwan3Department of Neurosurgery, Tulane University, New Orleans, LA 70112, USA4Departments of Neurosurgery, Physiology, and Anesthesiology, Loma Linda University School of Medicine, Loma Linda, CA 92354,USA
5Department of Neurosurgery, University of Cincinnati, Cincinnati, OH 45219, USA6Neurocritical Care Unit, Department of Neurosurgery, University Hospital Zurich, Frauenklinikstrasse 10, 8091 Zurich, Switzerland7Department of Neurosurgery, Kantonsspital Aarau, Tellstrasse, 5001 Aarau, Switzerland
Correspondence should be addressed to Chih-Lung Lin; [email protected]
Received 13 August 2014; Accepted 13 August 2014; Published 8 September 2014
Copyright © 2014 Chih-Lung Lin et al.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Although cerebral vasospasm (CV) after aneurysmal sub-arachnoid hemorrhage (SAH) has been recognized for morethan half a century, its pathophysiologic mechanism remainselusive [1]. Delayed CV has classically been considered asthe leading and treatable cause of mortality and morbidityin patients following aneurysmal SAH. Despite intensiveresearch efforts, SAH-induced CV remains incompletelyunderstood from both the pathogenic and the therapeu-tic perspectives. Many pathological processes have beenproposed to explain the pathogenesis of delayed CV afterSAH, including endothelial damage, smoothmuscle contrac-tion, changing in vascular responsiveness, and inflammatoryand/or immunological response of the vascular wall [2]. Atpresent, the most important and critical aspects of SAH-induced CV are its failure to consistently respond to treat-ment and only partial success could be achieved in bothexperimental models and clinical trials.
For patients with SAH surviving the early phase, sec-ondary ischemia (or delayed cerebral ischemia, DCI) is pop-ularly considered as the leading determinant of poor clinicaloutcome. Amongst the complications after SAH,CVhas beenregarded as the major cause of DCI. However, there havebeen an increasing number of evidences supporting multipleetiologies of DCI other than CV. Although radiographic CV
is presented in up to 70% of SAH patients, only 20–30% ofall SAH patients suffer from clinically symptomatic CV [3].Nonetheless, it is now evident that CV alone is inadequateto completely explain DCI following aneurismal rupture [2,4]. Recent studies on the treatment of CV have failed tosolidly support the correlation between angiogram-shownimprovement in CV and prognosis. Besides, various drugsproven effective for better functional outcomes have demon-strated their independency of CV reduction. Currently, amultifactorial etiology for DCI has emerged, whereas therole of CV has shifted from the major and most significantdeterminant to one contributing factor, just like any otherfactors, to the process. The study of the pathophysiologyof DCI has become more broad-minded with several otherdifferent mechanisms being actively investigated.
The term “early brain injury” (EBI) was first postulatedin 2004, more than 40 years after delayed CV was firstdescribed, to explain the acute pathophysiological eventsoccurring within 72 hours of SAH [5, 6].These events includecerebral autoregulation and blood-brain barrier disruption,activation of inflammatory pathways, excitotoxicity, oxidativestress, and activation of apoptosis [7]. These are direct effectsof blood clot in the subarachnoid space and also of transientcerebral ischemia, leading to brain injury not confined to
Hindawi Publishing CorporationBioMed Research InternationalVolume 2014, Article ID 679014, 3 pageshttp://dx.doi.org/10.1155/2014/679014

2 BioMed Research International
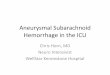
72 hours
Subarachnoid hemorrhage
Blood-brain barrierdisruption
Activation ofinflammatory pathways Activation of apoptosis
Oxidative stress activationof apoptosis
Excitotoxicity
Early brain injury
Cerebral autoregulationdisruption
0 hours
Delayed cerebral ischemiaDisruption of the
Cerebral vasospasm
Arteriolar constriction
Thrombosis and dysfunction in microcirculation
Cortical spreading ischemia
Endothelial damageSmooth muscle contractionChange in vascular responsivenessInflammatory and/or immunological
Activation of proapoptoticpathways
blood-brain barrier
Figure 1: The mechanisms of early brain injury and delayed cerebral ischemia following subarachnoid hemorrhage.
the site of hemorrhage. Many mechanisms of EBI contributeto the pathogenesis of DCI and are hence accountable for thepoor outcomes. Causes of DCI have been attributed to thecombined effects of delayed CV, activation of proapoptoticpathways, disruption of the blood-brain barrier, arteriolarconstriction, thrombosis and dysfunction in microcircula-tion, and cortical spreading ischemia, all brought about byEBI [2].
Accumulating data have suggested that apoptosis is akey mediator of secondary brain injury after SAH [8].Approximately, 50% of SAH survivors remain permanentlydisabled because of cognitive dysfunction and do not returnto their previous functions [9]. CV alone could not explainthe whole subtle changes in behavior and memory. In thisaspect, apoptosis induced by global ischemia should be takeninto consideration.
In this special issue, an update review of the mechanismand treatment of CV and DCI after aneurysmal SAH ispresented. The roles of mechanisms including microclot for-mation, downregulation of endothelial nitric oxide synthase,and upregulation of relaxin are discussed. Treatment withprogesterone, which attenuates experimental SAH-inducedCV by upregulation of endothelial nitric oxide synthase viaAkt signaling pathway, is investigated. Besides, a study onMagnesium Lithospermate B, an active extract of salvia mil-tiorrhizamediating sGC/cGMP/PKG translocation to reduceCV, is reported. Furthermore, new strategies using 17𝛽-estradiol, targeting at several CV-preventing mechanisms,have brought light to the reduction of CV and secondarybrain injury after SAH.The treatment and outcome including
extracerebral organs damage and long-term complicationsafter aneurysmal and nonaneurysmal SAH are also pre-sented. Medical resources utilization in patients followingSAH between the medical center and regional hospital isreported on a nationwide population-based study.
DCI, a result of different pathological pathways, is acomplex process and has shown its importance as the leadingdeterminant of poor functional outcome in patients survivingthe initial hemorrhagic insult of SAH. The possible mecha-nisms of EBI and DCI after SAH, as well as their relationshipwith CV, are illustrated in Figure 1. The importance of CV inDCI has long been overemphasized. CV is not the sole or nec-essary process leading to DCI. Treatment strategies targetingat CV prevention alone are not adequate. Considering CVas the only monitor of therapeutic effectiveness or the loneprognostic marker can be misleading. Strategies focusing onthe detection and treatment of EBI as an alleviation of theoccurrence of DCI to subsequently improve overall outcomecould make promising future study blueprints.
Chih-Lung LinAaron S. Dumont
John H. ZhangMario Zuccarello
Carl Muroi
References
[1] D. A. Cook, “Mechanisms of cerebral vasospasm in subarach-noid haemorrhage,” Pharmacology andTherapeutics, vol. 66, no.2, pp. 259–284, 1995.

BioMed Research International 3
[2] R. L. Macdonald, “Pathophysiology and molecular genetics ofvasospasm,”Acta Neurochirurgica, vol. 77, supplement, pp. 7–11,2001.
[3] N. W. C. Dorsch, “Cerebral arterial spasm: a clinical review,”British Journal of Neurosurgery, vol. 9, no. 3, pp. 403–412, 1995.
[4] E. Tani, “Molecular mechanisms involved in development ofcerebral vasospasm.,”Neurosurgical Focus, vol. 12, no. 3, pp. 1–4,2002.
[5] J. B. Bederson, A. L. Levy,W.H.Ding et al., “Acute vasoconstric-tion after subarachnoid hemorrhage,”Neurosurgery, vol. 42, no.2, pp. 352–362, 1998.
[6] G. Kusaka, M. Ishikawa, A. Nanda, D. N. Granger, and J.H. Zhang, “Signaling pathways for early brain injury aftersubarachnoid hemorrhage,” Journal of Cerebral Blood Flow andMetabolism, vol. 24, no. 8, pp. 916–925, 2004.
[7] F. A. Sehba, R. M. Pluta, and J. H. Zhang, “Metamorphosis ofsubarachnoid hemorrhage research: fromdelayed vasospasm toearly brain injury,”Molecular Neurobiology, vol. 43, no. 1, pp. 27–40, 2011.
[8] W. J. Cahill, J. H. Calvert, and J. H. Zhang, “Mechanisms ofearly brain injury after subarachnoid hemorrhage,” Journal ofCerebral Blood Flow and Metabolism, vol. 26, no. 11, pp. 1341–1353, 2006.
[9] K. M. Buchanan, L. J. Elias, and G. B. Goplen, “Differingperspectives on outcome after subarachnoid hemorrhage: thepatient, the relative, the neurosurgeon,” Neurosurgery, vol. 46,no. 4, pp. 831–840, 2000.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com





![Inflammation in human cerebral aneurysms: pathogenesis ... · aneurysmal subarachnoid hemorrhage (SAH) is higher in hypertensive patients, smokers, heavy drinkers, and females. [2,4]](https://img.pdfslide.net/doc/110x75/5ed55ef36933f508e973f11f/inflammation-in-human-cerebral-aneurysms-pathogenesis-aneurysmal-subarachnoid.jpg)






















