Embed Size (px)
Citation preview

stromal invasion. Patients with relapse in the upper tract orprostate had frequent recurrent papillary or in situ tumors ofthe bladder. Of the patients with high grade Ta tumors 45(36%) underwent radical cystectomy for lamina propria (12),muscle (16) or prostate (17) invasion. Median time to cystec-tomy was 58 months (range 6 to 216). The survival rate ofpatients after cystectomy was 71% (32 survived and 13 diedof cancer). Of the 148 patients with Ta tumors 5 died of uppertract tumor and 27 of metastasis from bladder cancer orstromal invasion of the prostate. Another 31 patients died ofcauses unrelated to bladder cancer.
DISCUSSION
There is a paucity of data on long-term outcome of patientswith high grade Ta tumors evaluated independently ofthose with TaG1 or T1 tumors. Holmang et al followed 55patients with TaG2,3 bladder tumors for 20 years and re-ported that 8 (15%) had progression in stage and 6 (11%) diedof disease compared to 99 with T1 tumors, of whom 39% hadprogression and 30% died.8 These patients presented withprimary papillary tumors without associated carcinoma insitu and were treated primarily with transurethral resectionalone. Haukaas et al reported 10-year disease specific sur-vival rates of 94% for low grade Ta, 68% for high grade Taand 66% for T1 tumors in 231 patients with superficial blad-der cancer.9
The current report documents 15-year outcome of a popu-
lation of patients with papillary bladder tumors who were athigh risk of stage progression due to frequent recurrence ofpredominately high grade tumors associated with carcinomain situ, and who were selected for referral to a cancer center.The results affirm excellent progression-free and disease spe-cific survival of patients with low grade Ta tumors. On theother hand, high grade Ta tumors represent a significant riskof tumor progression and death from urothelial cancer. Thisrisk is manifested in 15-year progression-free and diseasespecific survival rates of 61% and 74%, respectively, in pa-tients with high grade Ta tumors compared to 44% and 62%,respectively, in those with T1 tumors. Multiple, recurrenthigh grade noninvasive papillary bladder tumors, despiteaggressive local therapy, appear to have a lifelong risk oftumor progression similar to that of T1 tumors.
CONCLUSIONS
High grade Ta tumors have a higher risk of associationwith carcinoma in situ and invasive disease than low gradeTa tumors. High grade Ta tumors should be considered aspotentially lethal as T1 tumors, and treated aggressivelywith repeat transurethral resection and intravesical therapyas well as cystectomy if they cannot be eradicated or at thefirst evidence of stage progression. Patients with high gradeTa tumors require lifelong surveillance for relapse in thebladder and extravesical urothelium.
REFERENCES
1. Jordan, A. M., Weingarten, J. and Murphy, W. M.: Transitionalcell neoplasms of the urinary bladder. Can biologic potentialbe predicted from histologic grading? Cancer, 60: 2766, 1987.
2. Heney, N. M., Ahmed, S., Flanagan, M. J. et al: Superficialbladder cancer: progression and recurrence. J Urol, 130: 1083,1983.
3. Leblanc, B., Duclos, A. J., Benard, R. et al: Long-term followup ofinitial Ta grade 1 transitional cell carcinoma of the bladder.J Urol, 162: 1946, 1999.
4. Jakse, G., Loidl, W., Seeber, G. et al: Stage T1, grade 3 transi-tional cell carcinoma of the bladder: an unfavorable tumor?J Urol, 137: 39, 1987.
5. Herr, H. W.: Tumor progression and survival in patients withT1G3 bladder tumors: 15-year outcome. Br J Urol, 80: 762,1997.
6. Althausen, A. F., Prout, G. R., Jr. and Daly, J. J.: Non-invasivepapillary carcinoma of the bladder associated with carcinomain situ. J Urol, 116: 575, 1976.
7. Epstein, J. I., Amin, M. B., Reuter, V. R. et al: The World HealthOrganization/International Society of Urological Pathologyconsensus classification of urothelial (transitional cell) neo-plasms of the urinary bladder. Bladder Consensus ConferenceCommittee. Am J Surg Pathol, 22: 1435, 1998.
8. Holmang, S., Hedelin, H., Anderstrom, C. et al: The relationshipamong multiple recurrences, progression and prognosis of pa-tients with stages Ta and T1 transitional cell cancer of thebladder followed for at least 20 years. J Urol, 153: 1823, 1995.
9. Haukaas, S. A., Daehlin, L., Maartmann-Moe, H. et al: Long-term outcome in patients with superficial transitional cellcarcinoma of the bladder. Unpublished data.
EDITORIAL COMMENT
The author presents an important review of a highly unusualgroup of patients. The subset of 125 high grade Ta tumors is likely tobe seen only at a referral center for bladder cancer. High grade Tatumors are more common in a minority of cases, such as the 1% to 3%reported by Prout et al.1 The cases are also highly associated withconcomitant carcinoma in situ, which suggests that the underlyingurothelial dysfunction may be different than a typical Ta tumoralone. Nearly all Ta tumors recurred, and progression (39%) andmortality (26%) rates were even higher than those reported byHeney et al for G2G3 Ta tumors (11% to 14% mortality at 10 years)(reference 2 in article). More than a third of the patients withprogression had muscle invasive disease and 29% of those treatedwith cystectomy died of disease. The aggressive behavior of these
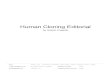
FIG. 1. Fifteen-year progression-free survival of patients withhigh grade Ta versus T1 bladder tumors. Of 125 patients with Tatumors 76 (61%) had no and 49 (39%) had progression compared to32 (44%) and 41 (56%), respectively, of 73 with T1 tumors. Medianprogression-free survival time for T1 tumors was 96 months (95%confidence intervals [CI] 89 to 141) and to date has not been reachedfor Ta tumors (152, 95% CI 121 to 182).
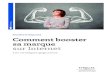
FIG. 2. Fifteen-year disease specific survival of patients with highgrade Ta versus T1 bladder tumors. Of 125 patients with Ta tumors93 (74%) were alive and 32 (26%) were dead of disease compared to45 (62%) and 28 (38%), respectively, of 73 with T1 tumors. Meandisease specific survival time for T1 tumors was 173 months (95% CI150 to 195) compared to 174 (95% CI 147 to 201) for Ta tumors.
HIGH GRADE, NONINVASIVE PAPILLARY BLADDER TUMORS 61

high grade Ta tumors closely mimics high grade T1 disease. Perhapsthese are really “incipient G3T1” tumors that have yet to invadethrough the basement membrane. A percentage may also be T1tumors whose microinvasive component was not removed by theresectionist and/or not identified on histological examination,thereby creating stage migration down to Ta disease. Hopefully themany markers for progression, that is tumor associated antigens,proliferation antigens, oncogenes, growth factors and their receptors,cellular adhesion molecules, angiogenesis factors and cell cycle reg-ulatory proteins, that are being investigated for T1 disease caneventually be applied to high grade Ta tumors to identify particu-
larly aggressive tumors. Earlier cystectomy may decrease the 26%disease specific mortality noted in this high risk noninvasive tumor.
Samuel J. PeretsmanUrologic OncologyUrology Specialists of the CarolinasCharlotte, North Carolina
1. Prout, G. R., Jr, Barton, B. A., Griffin, P. P., et al. Treatedhistory of nonivasive grade 1 transitional cell carcinoma: TheNational Bladder Cancer Group. J Urol, 148: 1143, 1992.
HIGH GRADE, NONINVASIVE PAPILLARY BLADDER TUMORS62