Embed Size (px)
Citation preview

Archives of Disease in Childhood 1994; 71: Fll-F15
Effect of fetal brainsparing on the early neonatalcerebral circulation
Sicco A Scherjon, Hans Oosting, Joke H Kok, Hans A Zondervan
AbstractThe effect of antenatal brainsparing onsubsequent neonatal cerebral blood flowvelocity (CBFV) was studied in verypreterm infants. CBFV was determined,using a pulsed Doppler technique, both inthe fetal and neonatal period. Neonatally,blood pressure and transcutaneouscarbon dioxide tension (TcPco2) wasmonitored simultaneously; daily cranialultrasound examinations were performed.
In infants with evidence ofbrainsparinga higher mean value ofCBFV and a differ-ent pattern ofchanges ofCBFV during thefirst week of life was demonstratedcompared with infants with normal fetalcerebral haemodynamics. No differenceswere found in blood pressure and TcPco2.The incidence of intracranial haemor-rhages and ofischaemic echodense lesionswas also the same for both groups.
In a multivariate statistical model ges-tational age, antepartum brainsparing,and TcPco2 all contributed significantlyin explanation of variation in CBFV. It isspeculated that a different setting of cere-bral autoregulation related to differencesin gestational age or to brainsparingmight explain the difference in changesfound in neonatal CBFV.(Arch Dis Child 1994; 71: F1l-Fl 5)
University ofAmsterdam, AcademicMedical Centre,Amsterdam, TheNetherlands,Department ofObstetricsSicco A Scherjon*Hans A Zondervan
Department ofNeonatologySicco A Scherjon*Joke H Kok
Department of ClinicalEpidemiology andBiostatisticsHans Oosting
Correspondence and reprintrequests to: Dr S A Scherjon,Department of ObstetricsH4-205, Academic MedicalCentre, University ofAmsterdam, Meibergdreef 9,1105 AZ Amsterdam, TheNetherlands.
Accepted 7 December 1993
Following the report of Bada et al in 1979'considerable interest in the study of neonatalcerebral haemodynamics using Doppler ultra-sound has arisen. The use of this technique inneonatology has been reported in a widevariety of pathological conditions includingductal patency, pneumothorax, and hydro-cephalus. The association between intracranialhaemorrhage (ICH)2 or neonatal asphyxia3and blood flow velocity waveforms has alsobeen widely investigated. More recently,Wladimiroff et al 4 and Arduini et al 5 showedthe feasibility of the pulsed Doppler technique,in combination with real time ultrasound inexamining the fetal cerebral circulation. Thephenomenon of fetal blood flow redistributionoccurring in severe intrauterine growthretardation, well known from animal studies,6could also be demonstrated in human preg-nancy.7 During normal pregnancy the lowestvascular resistance is at the level of theplacenta. However, during severe fetal growthretardation the region with the lowest vascularresistance is no longer the placental vascularbed, but will be at the level of cerebral vessels.In severe fetal growth retardation this will
result in a decrease ofend diastolic velocities inthe umbilical artery, while an increase in enddiastolic velocities in cerebral vessels can befound. This centralisation of the fetal circula-tion is known as the 'brainsparing' effect. Theratio ofumbilical pulsatility index (PI)/cerebralPI (U/C ratio) has been used as an index of thebrainsparing effect.4 In fetal growth retarda-tion a significant increase in U/C ratio wasfound.7 Consequences of antenatal brain-sparing on cerebral haemodynamics in thepreterm infant after birth are unknown.Therefore we studied the relation betweenantenatal haemodynamic adaptation asdefined by a raised U/C ratio and cerebralhaemodynamics in the neonatal period.
Patients and methodsA cohort of 117 pregnant women consecu-tively admitted to our department betweenFebruary 1989 and December 1989 wasstudied. One pregnancy resulting in the birthof an infant with Down's syndrome wasexcluded. Two patients refused to take part inthe study. In 11 cases intrauterine fetal deathoccurred. The data of 103 pregnancies result-ing in the birth of 128 liveborn infants, with agestational age at delivery between 25 and 33weeks are reported. Reasons for hospitaladmission were imminent preterm labour(n=83), severe growth retardation (n=4),second/third trimester haemorrhage (n=2),abruptio placentae (n= 2), and pregnancyinduced hypertension (n= 12). There were 81singletons, 19 twin pregnancies resulting in thebirth of 38 infants, and nine infants fromtriplet pregnancies.
FETAL BLOOD FLOW VELOCITY STUDIESAntenatally, flow velocity waveforms wererecorded from the umbilical artery and themiddle cerebral artery. Recordings of signalsfrom the middle cerebral artery were made atthe level of the bifurcation of the internalcarotid artery into the anterior and middlecerebral artery. Vessels were identified by realtime ultrasound with a 3-5 MHz sector scanner(DRF400, Diasonics). Flow velocity wave-forms were obtained with a 2 MHz pulsedDoppler probe (SD50 VingMed) attached tothe imaging probe at a fixed angle of insonationof 30 degrees.8 Sample volume was 3 mm andthe high pass filter was set at the lowest possiblelevel of 100 Hz. Back scattered Doppler signalswere displayed visually as a sonogram and theaudiosignals were stored on audiotape.Recordings were made directly after maternal
Fll
on May 15, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.71.1.F11 on 1 July 1994. D
ownloaded from

Scheron, Oosting, Kok, Zondervan
admission and thereafter at weekly intervals.The last measurement before birth was usedfor analysis. By replaying the stored audiosig-nal, spectral analysis was performed off-lineusing fast Fourier transformation. Calculationswere performed on the maximum frequencyenvelope of the Doppler shift, which was auto-matically recognised by the Vingmed SD50.PI: (Vsys Vdias)/Vmean9 was calculated over atleast five sequential cardiac cycles. Then theratio of umbilical PI/cerebral PI (U/C ratio)was calculated.We found in an earlier study that the one
sided tolerance limit of the U/C ratio, calcu-lated for normal pregnancies with a gestationalage ranging from 25 to 33 weeks was 0.72.10This limit delineates the lowest 950 0 confi-dence interval of a 50 0 chance for normal preg-nancies to have a U/C ratio above this limit.A U/C ratio above the tolerance limit wasconsidered to be indicative of the brainsparingeffect. Infants were grouped according to thepresence of signs of brainsparing.
NEONATAL CEREBRAL BLOOD FLOW VELOCITY(CBFV) STUDIESIn the immediate neonatal period, flow velocitywaveforms from the middle cerebral artery wererecorded in the transcranial plane. The sameDoppler equipment was used. The Dopplertransducer was placed on the temporal bone at0 5-1 cm in front of the ear.11 The anglebetween the Doppler beam and the axis of thevessel is near zero and permits determination ofabsolute flow velocities in this artery. The initialdepth setting was 2-0 cm and by ranging thedepth, the localisation of the sample volumewas adjusted to obtain the maximal signal. Themaximum frequency shift and thus the highestpossible velocities were obtained by listening tothe audio signal and observing the sonogram inreal time. The complete audio spectrum wasused to calculate the time averaged meanvelocity (Vmean).12 By replaying the audiotapesVmean was calculated off-line automatically bythe integrated computer system (SD50VingMed) over at least five sequential cardiaccycles. Doppler studies in the neonate were per-formed at 1, 2, 4, 8, 12, 24, 48, 72, 120, and168 hours after birth. Doppler studies were per-formed by one investigator (SAS). The resultsof the Doppler studies were not available to theattending clinicians.
OTHER MEASUREMENTSSimultaneously with the neonatal Dopplerrecordings mean arterial blood pressure (MAP)(Dinamap 1846 SX) and transcutaneouscarbon dioxide tension (TcPcO2) (HewlettPackard, type 78834A) were measured.Neurosonography was performed at fixed
intervals during the first week of life and storedon videotape. Neurosonographic findings werecategorised by one observer (SAS) who wasunaware of patient characteristics. The mostsevere ultrasound diagnosis at the end of thefirst week of life was used for classification.ICH was classified as proposed by Volpe.13 For
Table I Combined neurosonographic classification
Ultrasouwdclassificationi Critena
Normal No intracranial haemorrhage or a subependymalhacmorrhage. Echodensities less bnrght thanthe choroid plexus
Suspect Intraventricular haemorrhage (< 50°/0 of lumenfilled). Any echodensity brighter than thechoroid plexus, lasting less than three days
Abnormal Intra-ventricular haemorrhage (>500 o of lumenfilled) and any intraparenchvmalhaemorrhage. Any echodensity brighter thanthe choroid plexus and lasting for more thanthree davs.
the classification of ischaemic lesions known asechodensities the description of Pidcock et alwas used.14 Any intraventricular haemorrhageor intraparenchymal haemorrhage was classi-fied as a severe haemorrhage. Echodensitiesbrighter than the choroid plexus and lasting formore than three days were considered severeforms of echodensities. The infants were sub-divided according to evidence of severe ICHand/or severe echodensities on cranial ultra-sound. For further analysis a classificationbased on the combination of haemorrhages aswell as ischaemic lesions was used (table 1).
Infants were regarded as small for dates iftheir birth weight was below the 10th centilefor gestational age, taking maternal parity andsex into account.15 All clinical decisions weremade according to department standards. Thestudy was approved by the ethics committee ofthe hospital.
STATISTICSMann-Whitney U test, Fisher's exact probabil-ity test, and analysis of variance for repeatedmeasurements were used when appropriate,using the BMDP statistical program package.CBFV as the dependent variable was analysedusing repeated measurements analysis. U/Cratio and gestational age were used as explain-ing variables; the time changing variables MAPand TcPco9 were used as covariables. Thewithin subject covariance matrix was specifiedas having the compound symmetry structure.The coefficient of determination (R2) was usedto estimate the proportion of explained vari-ance in neonatal CBFV.'6 To select variablescontributing significantly to the model a step-wise backward selection procedure based onthe likelihood ratio test was done. This proce-dure means that first all variables are includedin the model. Each variable not contributingsignificantly to the model were then succes-sively excluded. Because data of the infantswho died in the very early neonatal periodcould influence the result of the total group thedata were analysed with and without theseinfants. A p value of less than 0 05 wasassumed to denote a significant difference.
ResultsIn 117 of the 128 infants enrolled in the study,signals from the middle cerebral artery wererecorded antenatally (91 %). In the other 11cases (singletons) we were unable to record thesignals because of a short time lag between
F12
on May 15, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.71.1.F11 on 1 July 1994. D
ownloaded from
Effect offetal brainsparing on the early neonatal cerebral circulation
Table 2 U/C ratio and obstetrical outcome
U/C rano
Nonnal Raised(n=74) (n=43)
Range (median) gestational age (days) 179-230 (207) 188-230 (220)*Range (median) birth weight (g) 705-2295 (1330) 605-1940 (1 125)**Appropriate weight for dates (2 1Oth centile) 1 22Small for dates (<1Oth centile) 73 21
*p<0-01; **p<0-001.
-0 22m
20E
- 180 16
' 14E
> 12
12 4 8 12 24 48 72 120 168
admission and delivery (n= 9) or because oftheoccipitoanterior position of the fetal head(n=2). Gestational age at birth of the infantsranged between 25 and 33 weeks (median 30weeks). Birth weight ranged between 605 and2295 g (median 1245 g).The 117 infants were divided into two
groups according to their antenatally deter-mined U/C ratio. The group with a raised U/Cratio consisted of 43 (37%) infants. Theremaining 74 (63%) infants had a normal U/Cratio (that is below the tolerance limit).Obstetrical outcome was different for the twogroups (table 2). Five infants died within thefirst four days of birth because of immaturity(n=3) or respiratory insufficiency (n=2).Another five infants died later in the neonatalperiod. Causes of death were sepsis (n=3) andmultiorgan failure (n=2).The incidence of ICH and of ischaemic
lesions was not different between the two U/Cratio groups (table 3). Using the combinedclassification of neurosonographic findings asgiven in table 1 the relations between the U/Cratio, being small for dates, and brain damagewere further explored. These results are givenin table 4.
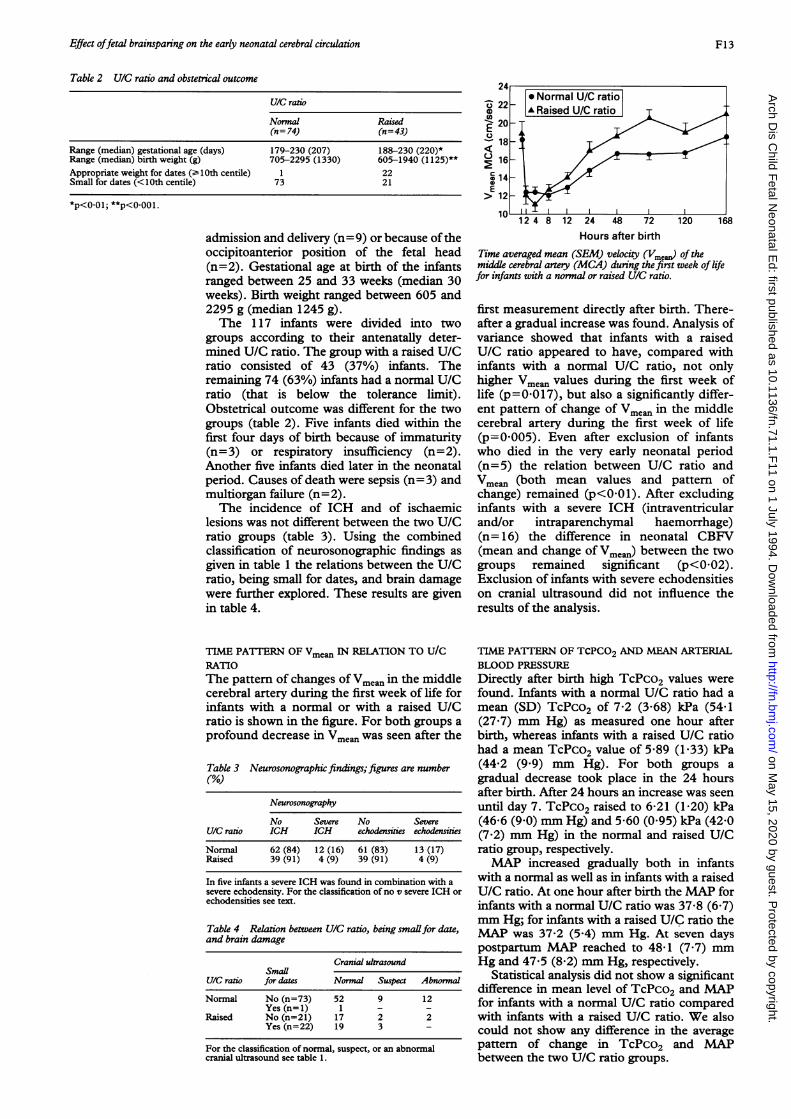
TIME PAITrERN OF Vmean IN RELATION TO U/CRATIOThe pattern of changes of Vmean in the middlecerebral artery during the first week of life forinfants with a normal or with a raised U/Cratio is shown in the figure. For both groups aprofound decrease in Vmean was seen after the
Table 3 Neurosonographic findings; figures are number(%O)
Neurosonography
No Severe No SevereU/C ratio ICH ICH echodensities echodnsities
Normal 62 (84) 12 (16) 61(83) 13 (17)Raised 39 (91) 4 (9) 39 (91) 4 (9)
In five infants a severe ICH was found in combination with asevere echodensity. For the classification of no v severe ICH orechodensities see text.
Table 4 Relation between U/C ratio, being smallfor date,and brain damage
Cranial ultrasoundSmaUl
U/C ratio for dates Normal Suspect Abnormal
Normal No (n=73) 52 9 12Yes (n=1) 1 - -
Raised No (n=21) 17 2 2Yes (n=22) 19 3 -
For the classification of normal, suspect, or an abnormalcranial ultrasound see table 1.
Hours after birthTime averaged mean (SEM) velocity (Vme)a(of themiddle cerebral artery (MCA) during the first week of lifefor infants with a normal or raised U/C ratio.
first measurement directly after birth. There-after a gradual increase was found. Analysis ofvariance showed that infants with a raisedU/C ratio appeared to have, compared withinfants with a normal U/C ratio, not onlyhigher Vmean values during the first week oflife (p=0-017), but also a significantly differ-ent pattern of change of Vmean in the middlecerebral artery during the first week of life(p=0 005). Even after exclusion of infantswho died in the very early neonatal period(n=5) the relation between U/C ratio andVmean (both mean values and pattern ofchange) remained (p<0-01). After excludinginfants with a severe ICH (intraventricularand/or intraparenchymal haemorrhage)(n= 16) the difference in neonatal CBFV(mean and change of Vmean) between the twogroups remained significant (p<002).Exclusion of infants with severe echodensitieson cranial ultrasound did not influence theresults of the analysis.
TIME PATTERN OF TCPCO2 AND MEAN ARTERIALBLOOD PRESSUREDirectly after birth high TcPco2 values werefound. Infants with a normal U/C ratio had amean (SD) TcPco2 of 7-2 (3-68) kPa (54-1(27.7) mm Hg) as measured one hour afterbirth, whereas infants with a raised U/C ratiohad a mean TcPco2 value of 5-89 (1-33) kPa(44'2 (9 9) mm Hg). For both groups agradual decrease took place in the 24 hoursafter birth. After 24 hours an increase was seenuntil day 7. TcPco2 raised to 6-21 (1-20) kPa(46-6 (9 0) mm Hg) and 5-60 (0 95) kPa (42-0(7-2) mm Hg) in the normal and raised U/Cratio group, respectively.MAP increased gradually both in infants
with a normal as well as in infants with a raisedU/C ratio. At one hour after birth the MAP forinfants with a normal U/C ratio was 37-8 (6 7)mm Hg; for infants with a raised U/C ratio theMAP was 37-2 (5-4) mm Hg. At seven dayspostpartum MAP reached to 48-1 (7.7) mmHg and 47-5 (8 2) mm Hg, respectively.
Statistical analysis did not show a significantdifference in mean level of TcPco2 and MAPfor infants with a normal U/C ratio comparedwith infants with a raised U/C ratio. We alsocould not show any difference in the averagepattern of change in TcPco2 and MAPbetween the two U/C ratio groups.
* Normal U/C ratioA Raised U/C ratio
11
?A.
in,1 -
F13
on May 15, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.71.1.F11 on 1 July 1994. D
ownloaded from
Scherion, Oosting, Kok, Zondervan
Table S Relation between neonatal CBFVand somevaniables
Variable (X) R p Value Regression line
TcPco2 0-19 0-047 y=11 9+0O07XXGestational age 0 40 <0-001 y=14-8+0-1OXXU/C ratio 0-28 0-002 y=10-6+1-1OXX
ANALYSIS OF VARIANCE WITH REPEATEDMEASUREMENTSAfter the backward selection procedure thevariables TcPco2 and either gestational age or
U/C ratio were significantly associated with thelevel and time pattern of neonatal CBFV.Because gestational age and U/C ratio are
highly correlated it is not possible to assess
their independent effects on CBFV properly.The multivariate model which included thesignificantly correlating variables TcPco2 andeither gestational age or U/C ratio couldexplain 30% of the variation of CBFV in theneonatal period. When TcPco2 was includedin the model, analysis of variance for repeatedmeasurements did not reveal any independenteffect of MAP on neonatal CBFV changes.The effect of TcPco2, gestational age, or
U/C ratio on the level of CBFV is shown intable 5. The correlation coefficient (R)between the individual mean of these variablesand the individual mean CBFV quantifiesthese effects; p values and the regression linesare shown.
DiscussionBrainsparing is defined as a circulatory adapta-tion of the fetus resulting in a preferentialperfusion of the central nervous system. Araised U/C ratio is a sensitive indicator of thebrainsparing effect and it is indicative of fetalgrowth retardation.'7 In our population onlyone infant with a normal U/C ratio appeared tobe small for dates (table 2). In the group with a
high U/C ratio 50% of the infants were abovethe 10th centile of the growth curve. As a
flattening of intrauterine growth might still becompatible with a birth weight above the 1 0thcentile, infants in the high U/C ratio groupclassified as normally grown, according to theclassical definition, might still have beengrowth retarded.
Using the combined classification theincidence of abnormal ultrasound findings washigher in the infants without fetal brainsparingcompared with infants with a normal U/C ratio(table 4). This finding was contrary to our
expectation as we hypothesised that antenatalbrainsparing might be associated with an
increase in fetal and neonatal brain damage.Also the incidence of suspect ultrasound find-ings was not higher for infants with signs ofbrainsparing, compared with infants without.Interestingly, the incidence of suspect findingson cranial ultrasound were equally distributedamong small for date infants and normallygrown infants, although both groups exhibitedantenatal signs of brainsparing.Flow velocity data of the middle cerebral
artery are important, as this vessel contributesto about 80% of fetal and neonatal
hemispheric blood flow.'8 Severe fetal growthretardation is clinically suspected especially ata more advanced gestational age. At earlygestational age (for example, 25-26 weeks)pregnant women are seldom referred becauseof growth retardation. This makes it under-standable that high U/C ratios were foundespecially at 30-33 weeks of pregnancy. It alsoexplains the finding that high U/C ratios wereso closely correlated with gestational age,making the assessment of the individual contri-bution of these variables on CBFV changesimpossible.Trend analysis of absolute changes OfVmean of
the middle cerebral artery contains informationon actual changes of cerebral blood flow.'9 20The profound decrease in Vmean immediatelyafter birth is in agreement with otherreports.21 22 Animal studies showed the fetalcerebral blood flow rate to be twice as highcompared with adult animals. The rapiddecrease in Vmean is most probably a reflectionof the transition from fetal to neonatal cerebralblood flow. This occurs within the first hoursafter birth.23 Absent end diastolic velocities,which are in our experience common on thefirst day, result in low Vmean values on the firstday. After the initial decrease in CBFV there isa gradual increase. Gray et al have argued thatthe initial decrease cannot be explained byductal patency alone.24 On the second dayafter birth 50% of preterm infants still have apatent ductus arteriosus.25 The fact that minorchanges were seen in CBFV after day 2,suggests that the impressive changes on day 1are not related to closure of the ductusarteriosus. The gradual increase in CBFVfound after the first eight hours of life is shownin many other studies.2' 22 26
Carbon dioxide tension27 and also bloodpressure'2 were found to be importantregulators of cerebral blood flow especially inthe distressed newborn. Therefore, changes inCBFV might be related to changes in bloodgases and/or changes in blood pressure. HighCBFV immediately postpartum reflects therelatively hypercarbic state during fetal life anddelivery. The decrease in CBFV in the firsthours after birth may be explained by thesudden fall in carbon dioxide tension due tothe initiation of respiration. TcPco2 values inour study are high immediately after birth anddecrease significantly in the first 24 hours afterbirth. Although statistically the effect ofTcPco2 may be small, changes of TcPco2 areprofound especially on day 1, and this willeffect especially the early changes in CBFV.Because of the profound changes in TcPco2,the effects of gestational age or of U/C ratio onCBFV were less during the early period ofhaemodynamic transition. They were shown tohave their effect especially at the end of theinvestigative period. Vasoactivity of majorcranial vessels causing vasoconstriction ofvessels that were dilated at birth was shown byDrayton and Skidmore.28 Carbon dioxide isthe most important regulator of CBFV29 and itexplained in animal experiments 550/o-90% ofthe reduction of CBFV at birth.23 Therelatively high CBFV in utero and directly after
F14
on May 15, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.71.1.F11 on 1 July 1994. D
ownloaded from

Effect offetal brainsparing on the early neonatal cerebral circulation
birth might also be a reflection of a low fetaloxygen tension; the decrease in CBFV beingthe result of the increase in neonatal arterialoxygen tension. We did not show a significantinfluence of changes in TcPo2 on changes inneonatal CBFV. From our data it seemsunlikely that changes in CBFV occurred due toan increase of MAP. This does not exclude,however, that changes in MAP may haveaffected CBFV in some infants. This mayparticularly be the case at high TcPco2values resulting in a disturbed cerebral flowautoregulation.As infants with a raised or normal U/C ratio
did not differ significantly in their patterns ofchange in TcPco2 and MAP, we could notattribute the difference found between the twogroups in neonatal pattern of CBFV to thesevariables. As the two groups had the sameprevalence of both severe intracranial haemor-rhages and of severe echodensities, a vasocon-strictive effect due to ICH or because ofischaemic lesions on CBFV is also unlikely.Because the analysis yielded the same resultsafter exclusion of the infants with an abnormalcranial ultrasound, the observed differences inCBFV cannot be attributed to intracranialpathology.The actual mechanism by which the
brainsparing effect during fetal life exerts itsinfluence on neonatal CBFV cannot be deter-mined from our data. In the model either ges-tational age or the U/C ratio were significantlyassociated with changes in CBFV. The highCBFV for infants with a raised U/C ratio couldbe a continuation of the fetal situation where agrowth retarded infant (as a result of chronichypercarbia or chronic hypoxia) has a vaso-dilated cerebral circulation, resulting in a
higher CBFV.30 Our findings are compatiblewith the findings of Yoshida et al that infantssmall for gestational age have a higher CBFVduring systole. Intrauterine stress might, inanalogy with the acceleration of lung matura-tion, induce a physiological alteration, leadingto a different setting of the autoregulation ofthe cerebral circulation. A higher gestationalage could have a maturational effect oncerebral autoregulation. This could alsoexplain the association between gestational ageand CBFV.
In conclusion: the level and time changes inCBFV were significantly related to TcPco2,whereas gestational age or U/C ratio both hada significant influence. No independent effectof changes ofMAP on neonatal CBFV changescould be demonstrated when TcPco2, gesta-tional age, and U/C ratio were included in themodel.
1 Bada HS, Hajjar W, Chua C, Sumner DS. Non-invasivediagnosis of neonatal asphyxia and intraventricularhemorrhage by Doppler ultrasound. J Pediatr 1979; 95:775-9.
2 Perlman JM, Volpe n1. Cerebral blood flow velocity inrelation to intraventricular hemorrhage in the pretermnewborn infant. I Pediatr 1982; 100: 956-9.
3 Archer LNJ, Levene MI, Evans DH. Cerebral arteryDoppler ultrasonography for prediction of outcome afterperinatal asphyxia. Lancet 1986; ii: 1116-7.
4 Wladimiroff JW, Tonge HM, Stewart PA. Doppler ultra-sound assessment of cerebral blood flow in the humanfetus. BrJ7 Obstet Gynaecol 1986; 93: 471-5.
5 Arduini D, Rizzo G, Romanini C, Mancuso S. Fetal bloodflow velocity waveforms as prediction of growth retarda-tion. Obstet Gynecol 1987; 70: 7-10.
6 Cohn EH, Sacks EJ, Heymann MA, Rudolph AM.Cardiovascular responses to hypoxemia and acidemia infetal lambs. Am 7 Obstet Gynecol 1974; 120: 817-24.
7 Scherjon SA, Smolders-DeHaas H, Kok JH, ZondervanHA. The 'brain-sparing effect'. Antenatal cerebralDoppler findings in relation to neurological outcome invery preterm infants. Am Jf Obstet Gynecol 1993; 169:169-75.
8 Eik-Nes A, Marsal K, Brubakk AO, Kristoffersson K,Ulstein M. Ultrasonic measurement of human fetal bloodflow. JfBiomed Eng 1984; 4: 28-36.
9 Gosling RG, King DH. Continuous wave ultrasound as analternative and complement to X-rays in vascular exami-nation. In: Reneman RS, ed. Cardiovascular application ofultrasound. Amsterdam: North Holland, 1974: 266-85.
10 Scherjon SA, Kok JH, Oosting H, Wolf H, Zondervan HA.Fetal and neonatal cerebral circulation: a pulsed Dopplerstudy. _J Perinat Med 1992; 20: 79-82.
11 Raju TNK, Zikos E. Regional cerebral blood velocity ininfants. A real-time transcranial and fontanellar pulsedDoppler study. J7 Ultrasound Med 1987; 6: 497-507.
12 Evans DH, Schlindwein FS, Levene MI. The relationshipbetween time averaged intensity weighted mean velocityand time averaged maximum velocity in neonatal cerebralarteries. Ultrasound Med Biol 1989; 15: 429-35.
13 Volpe nJ. Intraventricular hemorrhage and brain injury inthe premature infant. Clin Perinatol 1989; 16: 361-411.
14 Pidcock FS, Graziani U, Stanley C, Mitchell DG, MertonD. Neurosonographic features of periventricular echo-densities associated with cerebral palsy in preterm infants.J Pediatr 1990; 116: 417-22.
15 Kloosterman GJ. On intrauterine growth. The significanceof prenatal care. Int J7 Gynaecol Obstet 1970; 8: 895-912.
16 Nagelkerke NJD. A note on a general definition of the coef-ficient of determination. Biometrika 1991; 78: 691-2.
17 Wladimiroff JW, VanDenWijngaard JAGW, Degani S.Cerebral and umbilical arterial blood flow velocity wave-forms in normal and growth retarded pregnancies. ObstetGynecol 1987; 69: 705-9.
18 Kurmanavichius J, Karrer G, Hebisch G, Huch R, Huch A.Fetal and preterm newborn cerebral blood flow velocity.Early Hum Dev 1991; 26: 113-20.
19 Hansen NB, Stonestreet BS, Rosenkrantz TS, Oh W.Validity of Doppler measurements of anterior cerebralartery blood flow velocity: correlation with brain bloodflow in piglets. Pediatrics 1983; 72: 526-31.
20 Lundell BPW, Kennedy KA, Lindstrom DP, Sundell H.Stahlman MT. Intracranial Doppler flow velocimetrycompared with extracranial carotid blood flow measure-ments. Acta Paediatr Scand 1986; 329 (suppl): 127-33.
21 Archer LNJ, Evans DH, Levene MI. Doppler ultrasoundexamination of the anterior cerebral arteries of normalnewborn infants: the effects of postnatal age. Early HumDev 1985; 10: 225-60.
22 Winberg P, Sonesson SE, Lundell BPW. Postnatal changesin intracranial arterial blood flow velocities in preterminfants. Acta Paediatr Scand 1990; 79: 1150-5.
23 Barker JH. Fetal and neonatal cerebral blood flow. Am JPhysiol 1966; 210: 897-903.
24 Gray PH, Griffin EA, Drumm JE, Fitzgerald DE, DuingamNM. Continous wave Doppler ultrasound in evaluation ofcerebral blood flow in neonates. Arch Dis Child 1983; 58:677-81.
25 Gentile R, Stevenson G, Dooley T, Franklin D, Kawabori I,Pearlman A. Pulsed Doppler echocardiographic determi-nation of time of ductal closure in nornal newborninfants. J Pediatr 198 1; 98: 443-8.
26 Calvert SA, Ohlsson A, Hosking MC, Erskine L, Fong K,Shennan AT. Serial measurement of cerebral blood flowvelocity in preterm infants during the first 72 hours of life.Acta Paediatr Scand 1988; 77: 625-31.
27 Leahy FAN, Cates D, MacCallum M, Rigatto H. Effect ofCO2 and 100% 02 on cerebral blood flow in preterminfants. Journal of Applied Physiology: Respiratory,Environmental and Exercise Physiology 1980; 48: 468-74.
28 Drayton MR, Skidmore R. Vasoactivity of the majorintracranial arteries in newborn infants. Arch Dis Child1987; 62: 236-40.
29 Rosenkrantz TS, Diana D, Munson J. Regulation ofcerebral blood flow velocity in nonasphyxiated, very lowbirthweight infants with hyaline membrane disease.J Perinatol 1988; 8: 303-8.
30 VanBel F, VanDeBor M, Stijnen T, Ruys JH. Decreasedcerebrovascular resistance in small for gestational ageinfants. Eur3r Obstet Gynecol Reprod Biol 1986; 23: 137-44.
31 Yoshida H, Yasuhara A, Kobayashi Y. TranscranialDoppler sonographic studies of cerebral blood flowvelocities in neonates. Pediatr Neurol 1991; 7: 105-10.
F15
on May 15, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.71.1.F11 on 1 July 1994. D
ownloaded from



![Role of the Atg9a gene in intrauterine growth and survival of ......34 malnutrition, leading to fetal growth restriction (FGR) and intrauterine fetal death (IUFD) 35 [11-13]. Therefore,](https://img.pdfslide.net/doc/110x75/5fe3615f5637b735267b0386/role-of-the-atg9a-gene-in-intrauterine-growth-and-survival-of-34-malnutrition.jpg)



![Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://img.pdfslide.net/doc/110x75/5b63022f7f8b9ade588b8aac/early-intrauterine-development-of-mixed-giant-early-intrauterine-development.jpg)