Embed Size (px)
Citation preview
Pediatric Pulmonology 42:204–209 (2007)
Effect of a Sustained Inflation on RegionalDistribution of Gas and Perfluorocarbon
During Partial Liquid Ventilation
Kevin Morris, MD, FRCPCH,1 Peter Cox, FRCA, FRCP(C),1* Helena Frndova, MEng,1
Stephanie Holowka, MRT(R),2 and Paul Babyn, MDCM2
Summary. Objective: To study the effect of a sustained inflation (SI) maneuver on the regional
distribution of gas and perfluorocarbon (PFC) during partial liquid ventilation (PLV) in normal pigs
using computerized densitometry.
Study Design: Observational study.
Setting: Animal research laboratory.
Participants: Three healthy anaesthetized pigs.
Interventions: Partial liquid ventilation, lung recruitment, CT densitometry.
Methodology: LungswerefilledwithPFC to ‘‘liquid functional residual capacity (FRC)’’ (35–41ml/kg)
andCT imageswere recordedat a series of predeterminedairwaypressure levels (0, 20, 30, 40 cm
H2O) both before and after SI to an airway pressure of 40 cmH2O for 30 sec. Anterior, middle, and
posterior regions from upper (apical lung) to lower (basal lung) CT slices were analyzed at each
pressure level for Hounsfield units to describe the relative distribution of gas and PFC before and
after SI. Using anocclusion technique true gas volumeaboveFRCwas determinedat each pressure
level, before and after SI, and a pressure-volume (gas) envelope determined for each animal.
Results: At low airway pressures (<20 cm H2O) gas was distributed predominantly to the anterior
(non-dependent) part of the lung and PFC predominantly to the posterior (dependent) lung. Gas
and liquid were more uniformly distributed throughout the lung at airway pressures >20 cm H2O.
Generation of a pressure-volume (gas) envelope for eachanimal demonstrated an increase in total
gas volume above FRC at each pressure level following recruitment of the lung with SI. However,
marked regional differences were evident with the greatest effects of SI seen at higher airway
pressures in posterior and basal regions.
Conclusion: The healthy PFC filled lung demonstrates an increase in total gas volume following
SI. CT densitometry suggests marked heterogeneity of gas/PFC distribution between different
regions of lung and heterogeneity of response to SI. Pediatr Pulmonol. 2007; 42:204–209.
� 2007 Wiley-Liss, Inc.
Key words: perfluorocarbon; partial liquid ventilation; CT scan; lung recruitment;
sustained inflation.
INTRODUCTION
In 1991, Fuhrman and colleagues1 described a newconcept in ventilation using perfluorocarbons (PFC)—partial liquid ventilation (PLV). Here, the lung is filledwith PFC and mechanical gas ventilation is resumed, sothat the lung becomes partially filled with liquid andpartially filled with gas. Numerous studies have demon-strated that this technique leads to improved gas exchangeand improved pulmonary mechanics.2–5
In studies of PLV in healthy and oleic acid lung-injuredsheep Quintel et al.6 and Luecke et al.7 used CTdensitometry to examine the end-expiratory regionaldistribution of PFC along the ventral-dorsal axis of thelung. They found that healthy lungs were filled in a dose-dependent, gravity-governed fashion with PFC predomi-nantly distributed to the dependent (dorsal) regions of thelung. Total end-expiratory lung volumewas also estimated
1Department of Critical Care Medicine, The Hospital for Sick Children,
Toronto, Ontario, Canada.
2Department of Radiology, The Hospital for Sick Children, Toronto,
Ontario, Canada.
Grant sponsor: Department of Critical Care Medicine Research Fund, The
Hospital for Sick Children, Toronto, Ontario, Canada.
Kevin Morris’s present address is Department of Paediatric Intensive Care,
Birmingham Children’s Hospital, Birmingham, UK
*Correspondence to: Dr. Peter Cox, Department of Critical Care Medicine,
The Hospital for Sick Children, 555 University Avenue, Toronto, Ont.,
Canada M5G 1X8. E-mail: [email protected]
Received 20 February 2006; Revised 29 July 2006; Accepted 7 August
2006.
DOI 10.1002/ppul.20522
Published online 19 January 2007 in Wiley InterScience
(www.interscience.wiley.com).
� 2007 Wiley-Liss, Inc.
and found to be significantly increased in a dose-dependent manner.
Animal and human data support the use of a recruitmentstrategy in ventilated patients with acute lung injury, withan increase in lung volume and improved oxygenation.8,9
A sustained inflation (SI) maneuver is a technique that isemployed to recruit the lung, in which airway pressure isincreased to between 30 and 40 cm H2O and held for30 sec. We are not aware of any published data relating tothe effect of SI in the setting of PLV.
In this study we set out to characterize the relativedistribution of gas andPFC, usingCTdensitometry, acrossa range of airway pressures both before and afterrecruiting the lung to an airway pressure of 40 cm H2O.We chose to study a healthy lung model to facilitateinterpretation, in the knowledge that lung injury per seresults in marked regional changes on CT densitometry.7
Using an occlusion technique at end-expiration we werealso able to measure total gas volume above FRC at eachairway pressure, thus creating a pressure-volume (P-V)envelope for each animal.
MATERIALS AND METHODS
Following approval from the Animal Care Committeeat The Hospital for Sick Children and in accordance withNIH guidelines, three healthy male pigs (16–22.6 kg)were studied. The pigs were premedicated with intra-muscular Akmezine 0.25 ml/kg (containing ketamine58.8 mg/ml, acepromazine 1.18 mg/ml, and atropine90 mg/ml). Anesthesia was maintained with a continuoussolution of pentobarbital (975 mg in 500 ml 0.9% NaCland infused at a rate of 50–100 ml/h). Once muscleparalysis was attained with pancuronium bromide(0.1 mg/kg), the animal was intubated with a 7.0-mmcuffed endotracheal tube. Paralysis was maintained withan infusion of Pancuronium at a rate of 0.2 mg/kg/h.Peripheral venous access was established for fluidadministration (7 ml/kg/h Ringers lactate solution) andan arterial line was inserted for monitoring of arterialblood pressure (Hewlett–Packard model 1280) andintermittent arterial blood gas sampling. Arterial bloodgases were measured on an ABL 330 Radiometer,Copenhagen, Denmark. Throughout the experiment thepigs were nursed in the supine position. The animals wereventilated with tidal volumes of 12 ml/kg with a PEEP of3 cm/H2O. Respiratory rate was 20 breaths/min and FiO2
was maintained at 1.0. The animals were then transportedto the Radiological suite for further imaging. Oncestabilized, and after an initial CT scan, the animals’ lungswere filled with PFC (RM101, Mercantile Development,Inc., Bridgeport, CT). Filling was continued until ameniscus of liquid PFC was visible in the endotrachealtube at the height of the anterior chest wall at zero endexpiratory pressure, this generally being regarded as
‘‘liquid functional residual capacity.’’ Partial liquidventilation was continued with similar settings to thosedescribed above (Vt 12 ml/kg, frequency of 20, and anFiO2 of 1.0).
CT Densitometry
Sequential spiral computerized tomographic (CT)scans of the thorax before and after filling with PFC wereobtained utilizing a General Electric HiSpeed Advantagespiral CT scanner (GE, Milwaukee, WI). Scans wereobtained with slice thickness of 5 mm, pitch 1.5:1, and5mm collimation. KVwas 120 with mAs 140. The thoraxwas scanned from the level of the thoracic inlet to the levelof the diaphragm at a series of predetermined ventilatorpressures (0, 10, 20, 30, and 40 cm H2O). Animals weredisconnected from ventilation to atmospheric pressureprior to each measurement. Scans were performed after2 min at each static pressure setting before and after arecruitment maneuver (a sustained inflation pressure of40 cm H2O for 30 s). Ventilation was recommencedbetween these measurements. Throughout the experimentadditional PFC was instilled to maintain a visiblemeniscus of liquid PFC in the endotracheal tube at zeroend expiratory pressure.Upper (apical), mid-upper, mid-lower, and lower
(basal) slice levels of the thorax were selected for furtheranalysis. At each of these levels, three regions of the lung(anterior (non-dependent), middle and posterior (depen-dent)) were evaluated at each of the above pressuresettings (Fig. 1). Using a standardized electron sensor setto at least 14 mm2, these regions (anterior, middle, andlower) were analyzed for mean Hounsfield units (HU).Vessels and lung fissures were not included. A bottle of
Fig. 1. Diagrammatic representation of the four CT slices of the
thorax that were used for the analysis (U, upper; M-U, mid-upper;
M-L, mid lower; L, lower) (A) and of the three regions of interest
within each slice that were analyzed (A, anterior; M, middle; P,
posterior) (B).
Sustained Inflation and Perfluorocarbon Distribution During PLV 205
PFC was scanned to determine the density (HU) of PFC.When analyzing the density profile from anterior (non-dependent) to posterior (dependent) lung, density datafrom all four slices (upper, mid-upper, mid-lower, lower)were included. Similarly, when analyzing the profile fromlung apex (upper slice) to lung base (lower slice) densitydata from all three regions (anterior, middle, posterior)were included.
Occlusion Technique to MeasureLung Volume (Gas)
Using a rapid onset Hans Rudolph shutter valve, anocclusion technique with passive expiration to atmo-spheric pressure was used to measure flow through aFleisch pneumotachometer. Simultaneous measurementof airway pressure was recorded (Validyne MP 45transducer, Validyne Engineering Corp., Northridge,CA). Anadat software (McGill University, Montreal,Canada) was used to calculate volume from the integratedflow signal and to store all the data. Animals weredisconnected from ventilation to atmospheric pressureprior to each measurement. With the lung filled with PFCmeasurements were made at a series of pre-determinedairway pressures (0, 5, 10, 15, 20, 25, 30, 35, 40 cm H2O)both before and after a recruitment maneuver (a sustainedinflation to 40 cm H2O for 30 s). In this way a pressure-volume envelope was created for each animal.
RESULTS
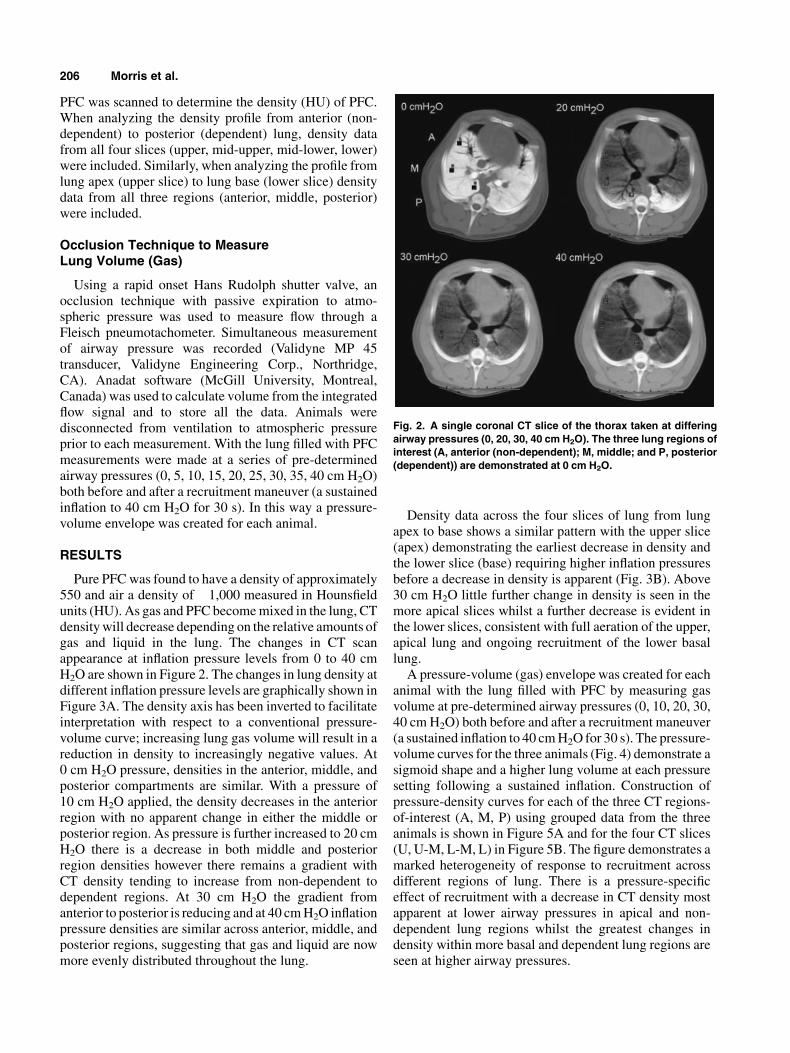
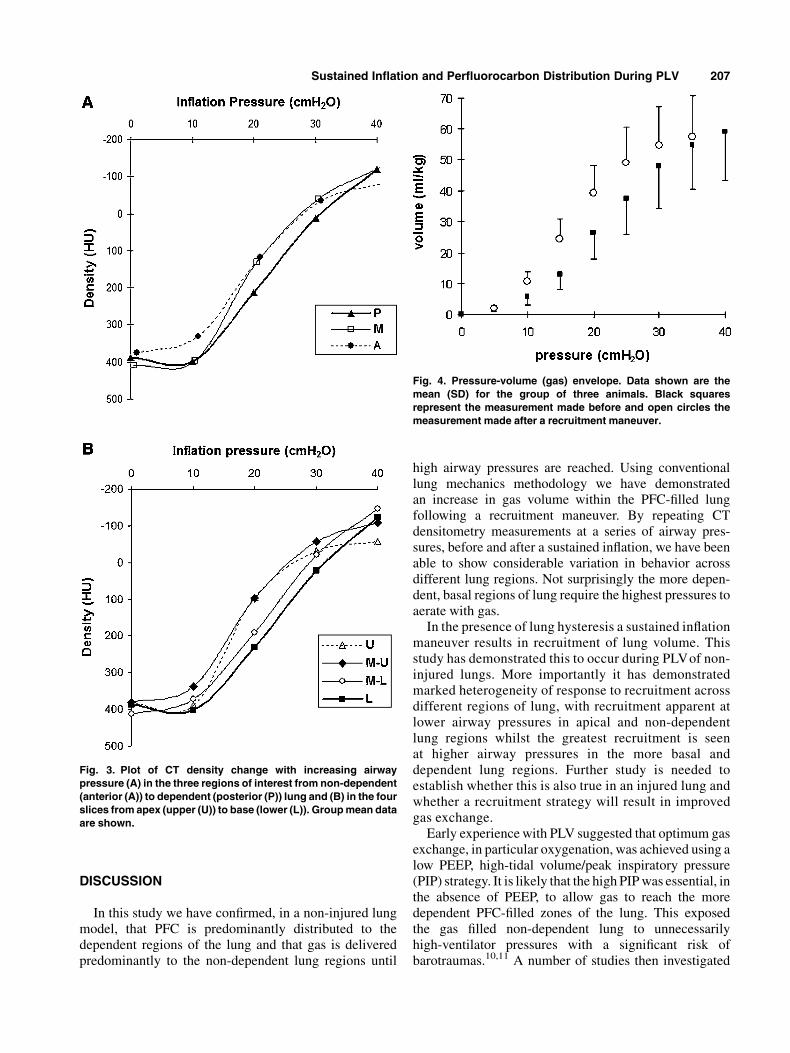
Pure PFCwas found to have a density of approximately550 and air a density of �1,000 measured in Hounsfieldunits (HU). As gas and PFC becomemixed in the lung, CTdensitywill decrease depending on the relative amounts ofgas and liquid in the lung. The changes in CT scanappearance at inflation pressure levels from 0 to 40 cmH2O are shown in Figure 2. The changes in lung density atdifferent inflation pressure levels are graphically shown inFigure 3A. The density axis has been inverted to facilitateinterpretation with respect to a conventional pressure-volume curve; increasing lung gas volume will result in areduction in density to increasingly negative values. At0 cm H2O pressure, densities in the anterior, middle, andposterior compartments are similar. With a pressure of10 cm H2O applied, the density decreases in the anteriorregion with no apparent change in either the middle orposterior region. As pressure is further increased to 20 cmH2O there is a decrease in both middle and posteriorregion densities however there remains a gradient withCT density tending to increase from non-dependent todependent regions. At 30 cm H2O the gradient fromanterior to posterior is reducing and at 40 cmH2O inflationpressure densities are similar across anterior, middle, andposterior regions, suggesting that gas and liquid are nowmore evenly distributed throughout the lung.
Density data across the four slices of lung from lungapex to base shows a similar pattern with the upper slice(apex) demonstrating the earliest decrease in density andthe lower slice (base) requiring higher inflation pressuresbefore a decrease in density is apparent (Fig. 3B). Above30 cm H2O little further change in density is seen in themore apical slices whilst a further decrease is evident inthe lower slices, consistent with full aeration of the upper,apical lung and ongoing recruitment of the lower basallung.A pressure-volume (gas) envelope was created for each
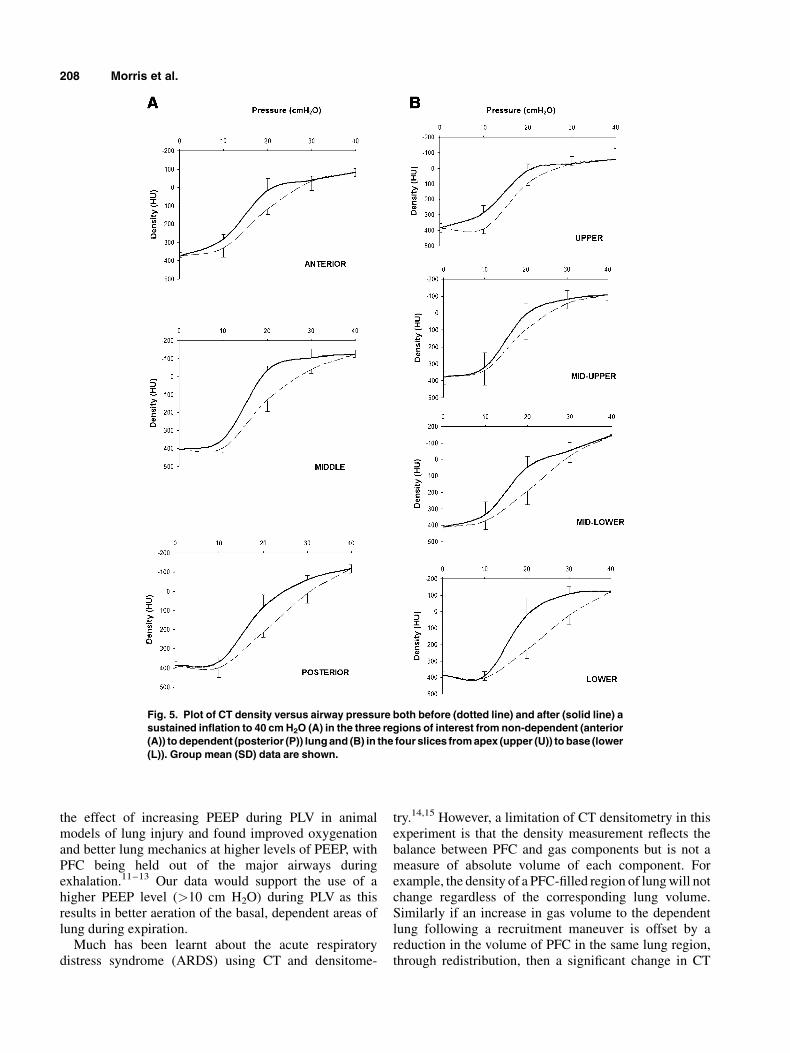
animal with the lung filled with PFC by measuring gasvolume at pre-determined airway pressures (0, 10, 20, 30,40 cmH2O) both before and after a recruitment maneuver(a sustained inflation to 40 cmH2O for 30 s). The pressure-volume curves for the three animals (Fig. 4) demonstrate asigmoid shape and a higher lung volume at each pressuresetting following a sustained inflation. Construction ofpressure-density curves for each of the three CT regions-of-interest (A, M, P) using grouped data from the threeanimals is shown in Figure 5A and for the four CT slices(U, U-M, L-M, L) in Figure 5B. The figure demonstrates amarked heterogeneity of response to recruitment acrossdifferent regions of lung. There is a pressure-specificeffect of recruitment with a decrease in CT density mostapparent at lower airway pressures in apical and non-dependent lung regions whilst the greatest changes indensity within more basal and dependent lung regions areseen at higher airway pressures.
Fig. 2. A single coronal CT slice of the thorax taken at differing
airway pressures (0, 20, 30, 40 cm H2O). The three lung regions of
interest (A, anterior (non-dependent); M, middle; and P, posterior
(dependent)) are demonstrated at 0 cm H2O.
206 Morris et al.
DISCUSSION
In this study we have confirmed, in a non-injured lungmodel, that PFC is predominantly distributed to thedependent regions of the lung and that gas is deliveredpredominantly to the non-dependent lung regions until
high airway pressures are reached. Using conventionallung mechanics methodology we have demonstratedan increase in gas volume within the PFC-filled lungfollowing a recruitment maneuver. By repeating CTdensitometry measurements at a series of airway pres-sures, before and after a sustained inflation, we have beenable to show considerable variation in behavior acrossdifferent lung regions. Not surprisingly the more depen-dent, basal regions of lung require the highest pressures toaerate with gas.In the presence of lung hysteresis a sustained inflation
maneuver results in recruitment of lung volume. Thisstudy has demonstrated this to occur during PLVof non-injured lungs. More importantly it has demonstratedmarked heterogeneity of response to recruitment acrossdifferent regions of lung, with recruitment apparent atlower airway pressures in apical and non-dependentlung regions whilst the greatest recruitment is seenat higher airway pressures in the more basal anddependent lung regions. Further study is needed toestablish whether this is also true in an injured lung andwhether a recruitment strategy will result in improvedgas exchange.Early experiencewith PLV suggested that optimum gas
exchange, in particular oxygenation, was achieved using alow PEEP, high-tidal volume/peak inspiratory pressure(PIP) strategy. It is likely that the high PIPwas essential, inthe absence of PEEP, to allow gas to reach the moredependent PFC-filled zones of the lung. This exposedthe gas filled non-dependent lung to unnecessarilyhigh-ventilator pressures with a significant risk ofbarotraumas.10,11 A number of studies then investigated
Fig. 3. Plot of CT density change with increasing airway
pressure (A) in the three regions of interest from non-dependent
(anterior (A)) to dependent (posterior (P)) lung and (B) in the four
slices from apex (upper (U)) to base (lower (L)). Group mean data
are shown.
Fig. 4. Pressure-volume (gas) envelope. Data shown are the
mean (SD) for the group of three animals. Black squares
represent the measurement made before and open circles the
measurement made after a recruitment maneuver.
Sustained Inflation and Perfluorocarbon Distribution During PLV 207
the effect of increasing PEEP during PLV in animalmodels of lung injury and found improved oxygenationand better lung mechanics at higher levels of PEEP, withPFC being held out of the major airways duringexhalation.11–13 Our data would support the use of ahigher PEEP level (>10 cm H2O) during PLV as thisresults in better aeration of the basal, dependent areas oflung during expiration.Much has been learnt about the acute respiratory
distress syndrome (ARDS) using CT and densitome-
try.14,15 However, a limitation of CT densitometry in thisexperiment is that the density measurement reflects thebalance between PFC and gas components but is not ameasure of absolute volume of each component. Forexample, the density of a PFC-filled region of lungwill notchange regardless of the corresponding lung volume.Similarly if an increase in gas volume to the dependentlung following a recruitment maneuver is offset by areduction in the volume of PFC in the same lung region,through redistribution, then a significant change in CT
Fig. 5. Plot of CT density versus airway pressure both before (dotted line) and after (solid line) a
sustained inflation to 40 cm H2O (A) in the three regions of interest from non-dependent (anterior
(A)) to dependent (posterior (P)) lung and (B) in the four slices from apex (upper (U)) to base (lower
(L)). Group mean (SD) data are shown.
208 Morris et al.

density will result without a great change in absolute lungvolume in that region.
The physical properties of individual PFCs, such asviscosity and vapor pressure, vary considerably.16 It isconceivable that our findings would have been different ifwe had used an alternative PFC. In additionwe are not ableto say anything about the influence and distribution of PFCvapor within the lung. A further limitation of this study isthe small number of animals that were investigated,preventing any meaningful statistical interpretation of thedata.
There has been considerable debate about the optimumdose of PFC, PEEP, and tidal volume in PLV.10,13,17 Todate little consideration has been given to the role of arecruitment maneuver. In this small study of non-injuredlungs we have demonstrated a beneficial effect on gasvolume within the PFC-filled lung and highlightedregional heterogeneity in response to recruitment. Athigher airway pressures the greatest changes following asustained inflation maneuver are seen in the moredependent, basal regions of the lung, regions thatdemonstrate the greatest atelectasis in ARDS. Furtherstudy is needed to see if these effects can be reproduced inan injured lung model.
ACKNOWLEDGMENTS
The authors thankMs.VickyHannon and the staff of theAnimal Laboratory at the Research Institute for help withthis study.
REFERENCES
1. Fuhrman BP, Paczan PR, DeFrancisis M. Perfluorocarbon-
associated gas exchange. Crit Care Med 1991;19:712–722.
2. Curtis SE, Peek JT, Kelly DR. Partial Liquid Breathing with
Perflubron Improves Arterial Oxygenation in Acute Canine Lung
Injury. J Appl Physiol 1993;75:2696–2702.
3. Hernan LJ, Fuhrman BP, Kaiser RE, Penfil S, Foley C, Papo MC,
Leach CL. Perfluorocarbon-associated gas exchange in normal
and acid-injured large sheep. Crit Care Med 1996;24:475–481.
4. Hirschl RB, Tooley R, Parent A, Johnson K, Bartlett RH.
Improvement of gas exchange, pulmonary function, and lung
injury with partial liquid ventilation: a study model in a setting of
severe respiratory failure. Chest 1995;108:500–508.
5. Tutuncu AS, Faithfull NS, Lachmann B. Comparison of
ventilatory support with intratracheal perfluorocarbon adminis-
tration and conventional mechanical ventilation in animals with
acute respiratory failure. Am Rev Respir Dis 1993;148:785–
792.
6. Quintel M, Hirschl RB, Roth H, Loose R, van Ackern K.
Computer tomographic assessment of perfluorocarbon and gas
distribution during partial liquid ventilation for acute respiratory
failure. Am J Respir Crit Care Med 1998;158:249–255.
7. Luecke T, Meinhardt JP, Herrmann P, Klemm S, Weiss A, Weisser
G, Hirschl RB, Quintel M. End-expiratory lung volumes and
density distribution patterns during partial liquid ventilation in
healthy and oleic acid-injured sheep: a computed tomography
study. Crit Care Med 2003;31:2190–2197.
8. Rimensberger PC, Cox PN, Frndova H, Bryan AC. The open lung
during small tidal volume ventilation: concepts of recruitment and
‘‘optimal’’ positive end-expiratory pressure. Crit Care Med 1999;
27:1946–1952.
9. Lapinsky SE, Aubin M, Mehta S, Boiteau P, Slutsky AS. Safety
and efficacy of a sustained inflation for alveolar recruitment in
adults with respiratory failure. Intensive Care Med 1999;25:
1297–1301.
10. Cox PN, Frndova H, Tan P, Nakamura T, Middleton W, Maser D,
Bryan AC. Concealed air leak associated with large tidal volumes
in partial liquid ventilation. Am J Respir Crit Care Med 1997;156:
992–997.
11. Reickert CA, Rich PB, Crotti S, Mahler SA, Awad SS, Lynch
WR, Johnson KJ, Hirschl RB. Partial liquid ventilation and
positive end-expiratory pressure reduce ventilator-induced lung
injury in an ovine model of acute respiratory failure. Crit Care
Med 2002;30:182–189.
12. Kaisers U, Kuhlen R, Keske U, Sommerer A, Mohnhaupt A,
Falke KJ, Rossaint R. Superimposing positive end-expiratory
pressure during partial liquid ventilation in experimental lung
injury. Eur Respir J 1998;11:1035–1042.
13. Kirmse M, Fujino Y, Hess D, Kacmarek RM. Positive end-
expiratory pressure improves gas exchange and pulmonary
mechanics during partial liquid ventilation. Am J Respir Crit
Care Med 1998;158:1550–1556.
14. Gattinoni L, Pelosi P, Crotti S, Valenza F. Effects of positive end-
expiratory pressure on regional distribution of tidal volume and
recruitment in adult respiratory distress syndrome. Am J Resp
Crit Care Med 1995;151:1807–1814.
15. Gattinoni L, Caironi P, Pelosi P, Goodman LR. What has
computed tomography taught us about the acute respiratory
distress syndrome? Am J Respir Crit Care Med 2001;164:1701–
1711.
16. Bull JL, Reickert CA, Tredici S, Komori E, Frank EL, Brant DO,
Grotberg JB, Hirschl RB. Flow limitation in liquid-filled lungs:
effects of liquid properties. J Biomech Eng 2005;127:630–636.
17. Nakamura T, Tamura M. Partial liquid ventilation with low dose
of perflubron and a low stretch ventilation strategy improves
oxygenation in a rabbit model of surfactant depletion. Biol
Neonate 2002;82:66–69.
Sustained Inflation and Perfluorocarbon Distribution During PLV 209