Embed Size (px)
Citation preview

Effectiveness of User Controlled Peroneal Stimulator
for foot drop in patients with hemiplegia following
Cerebrovascular Accident in an Indian Rehabilitation
set up: A Randomized Control Trial, Pilot Phase
Dissertation submitted to the Tamil Nadu Dr. MGR Medical University,
Chennai, in the partial fulfillment of requirements for the
MD Branch XIX (Physical Medicine and Rehabilitation) examination in
March 2014

Certificate
This is to certify that “Effectiveness of User Controlled Peroneal
Stimulator for foot drop in patients with hemiplegia following
Cerebrovascular Accident in an Indian Rehabilitation set up: A
Randomized Control Trial, Pilot Phase” is the bona fide work of Dr Kriti
Mishra, Candidate number 20116502, in partial fulfilment of the
requirement of the Tamil Nadu Dr MGR Medical University, Chennai,
for the MD Branch XIX (Physical Medicine and Rehabilitation)
examination in March 2014.
Dr. Alfred Job Daniel
Principal
Christian Medical College
Vellore

Certificate
This is to certify that “Effectiveness of User Controlled Peroneal
Stimulator for foot drop in patients with hemiplegia following
Cerebrovascular Accident in an Indian Rehabilitation set up: A
Randomized Control Trial, Pilot Phase” is the bona fide work of Dr Kriti
Mishra, Candidate number 20116502, in partial fulfilment of the
requirement of the Tamil Nadu Dr MGR Medical University, Chennai,
for the MD Branch XIX (Physical Medicine and Rehabilitation)
examination in March 2014, under my supervision and guidance.
Dr. Raji Thomas
Professor
Department of Physical Medicine and Rehabilitation
Christian Medical College
Vellore



Acknowledgement
This study has been one of the most interesting and learning experience
of my PG curriculum.
My sincere gratitude to Dr. George Tharion who made me believe in the
feasibility of the study and encouraged me to take this topic as my
dissertation. I express my deep gratitude to Dr. Jacob George for his
constant guidance throughout and to Dr. Raji Thomas for helping me to
pen down the entire study.
A special thanks to Dr. Suresh Devasayam and Mr. Akhil Mohan for the
fabrication of the device and for the consistent technical inputs and
feedback regarding the study.
I thank Dr. Judy Ann John for her continuous motivation, Dr. V. Anand
and Dr.Rajdeep Ojha for their inputs regarding the data analysis, the
statistics and the dissertation presentation.
A heartfelt gratitude to Mr. Ramesh who was the primary physiotherapist
for the intervention group and the rest of the Rehabilitation Institute and
OPD physiotherapists without whose co-operation the study would not
have completed.

I would also like to thank all my colleagues who shared my clinical work
while I finalised the study; Ms. Joyce for being the neutral assessor of the
study outcome measures; Ms Grace for helping in the randomisation and
final statistical analysis.
Most of all, I am grateful to the patients and their relatives who readily
agreed to participate in the study and gave honest feedbacks regarding the
intervention and the study.
Kriti Mishra

Index
Chapter Page
Title 1
Aim and Objectives 2
1. Introduction 3-5
2. Justification for the study 6-8
3. Review of Literature 9-49
3.1. Epidemiology
3.2. Risk factors for CVA
3.3. Etiopathogenesis
3.4. Presentations of Stroke
3.5. Stroke Syndromes
3.6. Evaluation of a stroke patient
3.7. Initial Treatment
3.8. Admission to Hospital and Acute Management
(After Hospitalization)
3.9. Neurological Recovery
3.10. Motor Impairment
3.10.1. Normal Gait
3.10.2. Role of Ankle Muscles in Normal Gait
And Biomechanics

3.10.3. Biomechanics of the Ankle
3.10.4. Gait Impairments Seen in Stroke
3.11. Rehabilitation in Stroke
3.11.1. Principles of Stroke Rehabilitation
3.11.2. Rehabilitation Related to Motor
Impairments
3.12. FES System
3.12.1. FES System Components
3.12.2. Drop Foot Stimulator or Peroneal
Stimulator (PS)
3.12.3. Studies Related to the PS
4. Methodology 50-61
4.1. Study Design
4.2. Settings and Locations Where the Study was
Conducted
4.3. Participants
4.4. Sample Size
4.5. Randomization
4.6. Interventions
4.7. Outcome Measures
4.7.1. Primary Outcome
4.7.2. Secondary Outcomes

4.8. Statistical Analysis
4.9. Statistical Methods
5. Results 62-79
5.1. Recruitment, Screening and Randomization
5.2. Baseline Demographic and Clinical
Characteristics of Participants
5.3. Primary Outcomes
5.3.1. 6 minute walk test (Walking Endurance)
5.3.2. 10 meters test (Walking Speed)
5.4. Secondary Outcomes
5.4.1. Spatial Asymmetry
5.4.2. Stride Length
5.4.3. Stance Percentage (% of the total stride time)
5.4.4. Dynamic Ankle Range of Movement
5.5. Additional Analysis
5.5.1. Duration of the Stroke
5.5.2. MMSE
5.6. User Feedback
6. Discussion 70-91
7. Limitations 92
8. Recommendations for further Study 93

9. Conclusion 94-95
Bibliography
Annexure
1. Institutional Review Board Acceptance Letter
2. Patient Information Sheet and Consent Form
3. Case Sheet
4. Database for all Patients

1
Title of the study
“Effectiveness of User Controlled Peroneal Stimulator for foot
drop in patients with hemiplegia following Cerebrovascular
Accident in an Indian Rehabilitation set up: A Randomized
Control Trial, Pilot Phase”
Place of study
Department of Physical Medicine and Rehabilitation
Christian Medical College
Vellore

2
Aim
To evaluate the orthotic effectiveness of a peroneal stimulator [Functional
Electrical Stimulation (FES) based neuroprosthesis] controlled by a
switch placed on the user's assistive walking aid (quadripod) and compare
it with conventional rehabilitation method of using an Ankle Foot
Orthosis (AFO) in the treatment of foot drop in hemiplegic patients
following Cerebrovascular Accident (CVA).
Objectives
The study proposes to:
• Compare the orthotic effect of a user based PS to AFO in
hemiplegic foot drop rehabilitation.
• Compare the effectiveness of the manually controlled peroneal
nerve stimulator for gait training during sub-acute and chronic phases of
stroke rehabilitation and in patients with two different levels of cognitive
ability as measured by MMSE.
• Evaluate the subjective perception of patients regarding the
effectiveness of the manually operated hand switch in the Indian
rehabilitation setting.

3
1. Introduction
Over the past few decades, cerebrovascular accident (CVA) has become a
predominant global health care problem(1)and is one of the leading
causes of mortality as well as acquired disability worldwide. There has
been a change in the prevalence rate of CVA with the trend shifting from
developed countries to developing countries including India, where it has
become a silent epidemic(2). Lack of health care facilities at the primary
level for risk factor screening, non-accessibility to appropriate treatment
and common drugs, inadequate follow-up and secondary prevention
programmes and rehabilitation facilities have been attributed to higher
rates of death and disability in these low income countries, adding to the
disease burden(3). With these changing trends, a further increase in
prevalence of stroke related disease burden is anticipated over the next
two decades and hence, continuum of care post stroke and rehabilitation
has an essential role(4).
Stroke related impairment is multi-fold and include those related to
cognition, behaviour, language and speech, vision, swallowing, motor
and sensory functions. The motor impairment is the most widely
recognized impairment since it affects the mobility of patients and limits
the day to day functions(4). The hemiplegia leads to increase in muscle

4
tone in the lower limb. The weakness is more in distal muscles rather than
proximal. The weakness of ankle dorsiflexors results in inability to clear
the foot during the swing phase and inability to control foot falling after
the heel strike of stance phase (slap foot). The condition is called foot
drop(5). Ankle plantar -flexor spasticity or plantar flexor contracture can
further contribute to this impairment. A number of compensatory
movement patterns and limited functional mobility accompany the
condition(5).
In the conventional rehabilitation method, patients are trained to walk
with an ankle foot orthosis (AFO) to provide ankle stability, with or
without an appropriate walking aid.
An alternative tried over the past 6 decades is a drop-foot stimulator or
peroneal stimulator. The stimulator involves application of electric
current to the intact common peroneal nerve to generate muscle
contraction and enhance gait by improving foot clearance during the
swing phase and stability during initial stance phase(6). There have been
a number of studies to report a positive orthotic effect of Functional
Electrical Stimulation (FES) including recent studies comparing it with
AFO use(7–9). These studies have been done using automatic as well as
foot switches which have had their own limitations. Moreover, most of

5
these studies have evaluated FES in patients with hemiplegia of more
than 6 months duration.
The current study involved FES with a quadripod based switch gait
sensor making it a technically simpler and more adaptable device for use
in the Indian rehabilitation setting, with the sensor being a user controlled
system. Moreover, the stimulator, being an in-house development at our
Bioengineering department, was a low cost device. The study was
designed to investigate its use during the subacute and chronic phases of
stroke rehabilitation comparing its use with AFO and in patients with two
different levels of cognitive ability.

6
2. Justification for the study
Gait training with AFO and a walking aid (quadripod/ cane) is an
important goal of stroke rehabilitation. The AFO holds the foot in the
neutral position and prevents foot drop during the swing phase, thereby
helping in ground clearance. It also provides stability to the ankle during
the initial phase of stance(5). However, the AFO has its own
disadvantages in the form of limited ankle mobility, discomfort and
cosmetic issues(7,8).
The alternative option of providing electric stimulation to the common
peroneal nerve activates the ankle dorsiflexors and helps in ground
clearance. It has a two–fold effect: orthotic and therapeutic(7,8).
Immediate orthotic effect is that active dorsiflexion is more close to
physiologically normal gait biomechanics. Therapeutic effects include
improvement in muscle strength and joint range of motion and increased
voluntary control due to regular activation of the muscles.
Over the last six decades the PS (peroneal nerve stimulator) has
undergone constant innovations making it more user friendly with better
orthotic effect(6). Initial trials till the early 1990s involved stimulators
with surface electrodes activated by foot switches. However, foot
switches (either open/ close mechanical switch or force sensitive

7
resistors) tended to wear and tear on prolonged use, had inappropriate
firing of the switch due to poor contact or insufficient force during
hemiplegic gait (mainly because of gait asymmetry). The poor reliability
and size of the foot-switch, and the requirement for fitting of electrodes
and the foot-switch each day made these early devices unattractive(6).
In order to overcome these limitations came the advent of implantable PS
and automatic contactless artificial gait sensors in the form of
accelerometers and gyroscopes. The accelerometer with gyroscopes
detects the joint segment orientation and determines the timing for the
stimulus for dorsiflexion. However, being automatic sensors, they require
a more precise synchronization with the swing phase of gait cycle to
prevent inappropriate dorsiflexion. The gait asymmetry seen in
hemiplegic gait further contributes to this limitation.
Hence, in the present study, we chose to use a user controlled device.
Since the foot switch had its limitations as mentioned previously, a
manually operated hand switch was used to control stimulation. In low
resource settings as prevalent in India, where patients may prefer walking
bare-foot and are often given a walking stick/quadripod or similar aid for
safety purposes, a hand switch placed over the walking aid (quadripod)
was considered a reasonable option. It provided the patients with

8
voluntary control over the stimulation timing which is particularly useful
in avoiding small obstacles on the ground.
The evidence related to the effectiveness of hand switch based PS in the
literature is insufficient to approve or disprove its use clinically. A similar
device was fabricated in 1990’s (10). However, to our knowledge, its
effectiveness in clinical settings is unknown.
With these considerations, the study was designed to address the needs of
hemiplegic patients with foot drop admitted to our rehabilitation set-up
within 1 year of stroke. The study was also an attempt to make the PS
better adapted to the Indian settings mainly in terms of its low cost, small
size, technical simplicity and allowing option of bare-foot walking. In
view of better technical feedback, a wired switch was used for the study
with a plan to make a wireless device subsequently.

9
3. Review of Literature
Stroke or cerebrovascular accident as defined by WHO is “the rapid
development of clinical signs and symptoms of a focal neurological
disturbance lasting more than 24 hours or leading to death with no
apparent cause other than vascular origin”(11). It is caused by occlusion
or rupture of cerebral blood vessels resulting in sudden onset of
neurologic deficit characterized by loss of motor control, altered
sensation, cognitive or language impairment, disequilibrium, or coma
depending on the area in the brain affected. It excludes nonvascular
conditions of focal brain damage presenting with stroke-like symptoms,
such as seizure, hypoxemia, traumatic brain injury, demyelinating lesions
and brain tumour (12).
3.1 Epidemiology:
Incidence of stroke is 15 million per year worldwide and a prevalence
rate of 27–34/1,00,000 in the 35–44 age group to 822– 1116/100,000
in the 75+ age group has been noted in Indian studies(13). There has
been a recent trend change with stroke being more prevalent in
developing countries than in the high income countries. In fact, stroke in
younger age is more prevalent in India as compared to the global
prevalence of young stroke and hence, it has a significant economic

10
impact in developing nations like ours. This further adds to the disease
burden, in turn affecting the quality of life for these patients(13).
3.2 Risk factors for CVA:
This can be classified as modifiable and non-modifiable as shown
in figure 1 (12,14).
Figure 1: Risk factors
Table 1: Risk factors and Their Role
Risk factor Role in etiopathogenesis of CVA
Hypertension Increases risk of thrombotic, lacunar, and haemorrhagic stroke.
Heart disease Coronary Artery Disease doubles stroke risk. Fivefold increase in stroke risk in chronic and stable atrial fibrillation and up to 17 times the normal in
Risk factors for CVA
Non‐modifiable: age,
race/ethnicity, sex and family
history
Modifiable: hypertension,
smoking, atrial fibrillation, diabetes, obesity, sedentary
lifestyle

11
atrial fibrillation related to rheumatic heart disease.
Diabetes mellitus Independent risk factor leading to two-fold increase in stroke risk
Smoking Directly proportional increase in stroke risk with greater amounts of smoking
Hyperlipidemia Indirect risk factor for stroke by its contribution to the development of coronary artery disease and atherosclerosis.
Metabolic Syndrome
Include high waist circumference, increased blood pressure, low HDL level, elevated serum triglyceride and elevated fasting glucose. A graded increase in stroke risk seen with an increased number of metabolic risk factors and hence, the presence of all five components led to a fivefold increase in stroke risk.
Homocysteine Elevated homocysteine levels have been associated with higher risk of ischemic stroke.
3.3 Etiopathogenesis:
Based on the etiopathogenesis, CVA can be broadly divided into
two categories(12,14)
A. Intracranial haemorrhage includes 15% of all strokes. It can
further be divided into:-
1. Intracerebral bleed (10%) caused by rupture within the brain
parenchyma of weakened vessels due to hypertension,

12
arteriovenous malformation (AVM), tumor or other risk factors
like trauma, vasculitis, and bleeding into a tumor, disorders of
bleeding diathesis (e.g.: thrombocytopenia or coagulation
disorders). Most common site for hypertensive bleed is putamen or
thalamus followed by cerebellum in 10 % of patients.
2. Subarachnoid haemorrhage (5%) resulting from aneurysmal
rupture of a cerebral artery into the subarachnoid space
surrounding the brain.
B. Ischemic injury is responsible for 85% of strokes resulting from:-
1. Thrombosis : large vessel (40%) or small vessel (20%) thrombosis
is commonly caused by atherosclerotic cerebrovascular disease.
Small vessel thrombosis is often associated with lipohyalinosis of
small, deep, perforating arteries found in chronic hypertension.
2. Cerebral embolism (20%): Emboli are often of cardiac origin,
formed due to valvular disease or atrial fibrillation or chronic
ischemic cardiovascular disease associated with secondary
ventricular wall hypokinesia and subsequent increased intra cardiac
thrombus formation. The deep vein thrombosis in pelvis or lower
limbs can embolize to the right side of the heart, through a patent

13
foramen ovale into the left atrium and then into the cerebral
circulation. This is known as paradoxical embolism
3. Other causes (5%) such as cerebral vasculitis or cerebral
hypoperfusion.
3.4 Presentations of stroke (12,14)
Transient Ischemic Attacks (TIA): American Stroke Association
defined TIA as “a brief episode of neurologic dysfunction caused
by focal brain or retinal ischemia, with clinical symptoms typically
lasting less than an hour, and without evidence of acute infarction”
as determined by cranial imaging. It is sudden in onset with
apparent full resolution of symptoms including no imaging
findings.
Cerebral thrombosis: Insidious onset, worsening of deficits over
hours or days followed by stabilisation and gradual improvement.
Cerebral Embolism: The presentation is sudden. The embolus may
break into smaller fragments and result in multiple small infarcts.
Hence the initial clinical deficits may change and eventually fade if
the embolus undergoes lysis and fragmentation.

14
Lacunar stroke: It arises due to small, circumscribed infarcts less
than 1.5 cm in diameter resulting from occlusions of the deep
penetrating branches of the large vessels perfusing the subcortical
structures. They are often associated with hypertension and can
cause major neurologic deficits if they occur in key regions, or
vice-versa.
Intracerebral Haemorrhage: Abrupt onset with severe headache,
rapidly progressive neurologic deficits and progressive impairment
of consciousness leading to coma. Brain displacement leading to
cerebral oedema and transtentorial herniation and death, is seen
within the first few days post-stroke.
Subarachnoid Haemorrhage: It presents as severe sudden
headache followed by vomiting and signs of meningeal irritation.
Focal signs may develop subsequently. Coma frequently occurs
and one third patients die acutely.
Higher mortality rate is seen in cerebral haemorrhage than
infarction. The neurological deficit from haemorrhage recovers
better than the initial deficit from an infarction. Urgent
decompression with hematoma evacuation can be lifesaving.
Nimodipine is routinely administered to reduce the severity of
arterial vasospasm seen with subarachnoid haemorrhage and early

15
surgical/ invasive radiological intervention in the form of clipping
the aneurysm neck or coiling to thrombose the aneurysm is done to
obliterate the aneurysm and prevent recurrent haemorrhage.
Hydrocephalus is common in SAH. It can develop immediately
due to obstruction of the ventricular system from intraventricular
haemorrhage or as a later complication due to arachnoiditis
(fibrosis of arachnoid granulations) from blood in the CSF causing
functional disruption of CSF resorption. It presents with the classic
symptoms of subcortical dementia, incontinence, and gait disorder
or decline in performance in a rehabilitation program.
3.5 Stroke Syndromes:
Based on the brain vascular anatomy, stroke involving certain
regional vascular supply leads to specific neurological deficits. This
produces ischemic stroke syndromes and thereby assist in localising the
stroke lesion and predicting functional outcome(12,14).
Internal Carotid Artery Syndrome: Depending on the collateral
circulation available, clinical consequences can vary from no
significant deficit to severe deficits. Massive infarction before the
ACA and MCA division can present with dense contralateral motor
and sensory deficits. Severe cerebral oedema can cause

16
transtentorial herniation and death. Decompression with
craniectomy can be lifesaving.
Middle Cerebral Artery Syndromes: It originates from internal
carotid artery. It passes through Sylvian fissure onto the lateral
surface and divides into upper and lower division. In the Sylvian
fissure, it gives rise to lenticulostriate arteries perfusing the basal
ganglia and internal capsule. Occlusion of MCA leads to different
symptoms as mentioned in Table 2
Table 2: MCA Occlusion Features
MCA1 occlusion site Features
Origin Depressed consciousness, deviation of eyes to
lesion side, contralateral hemiplegia, decreased
sensation, homonymous hemianopia
Dominant lobe: aphasia
Non-dominant lobe: dysphagia, contralateral
hemianopia, perceptual deficits and neglect
Superior Division Dense contralateral sensory-motor deficits,
initially global aphasia if dominant side

17
involved, later expressive aphasia
Inferior division Left side: aphasia, right side: severe left sided
neglect, attention deficits, constructional apraxia,
dressing apraxia, perceptual deficits, aprosodia,
Partial or complete contralateral homonymous
hemianopia
1MCA: Middle Cerebral Artery
Lacunar Stroke: The varied presentation of lacunar stroke
depends on the site of occlusion as specified in Table 3.
Table 3: Lacunar stroke
Site Features
Internal capsule Pure motor hemiplegia, associated dysarthria,
hand clumsiness in anterior lesion of the internal
capsule
Thalamus Contralateral sensory loss with or without
weakness
Anterior Cerebral Artery Syndromes: Anterior cerebral arteries
supply the median and paramedian regions of the frontal cortex

18
and the strip of the lateral surface of the hemisphere along its
superior border. The deep penetrating branches supply the head
of the caudate nucleus and the anterior limb of the internal
capsule. The deficits include contralateral hemiparesis (lower
limbs weaker than upper limbs), associated sensory loss of the
leg and foot, urinary incontinence , transcortical motor aphasia
with preserved repetition, behavioural issues like diminished
reasoning, lack of initiation, distractibility etc.
Vertebrobasilar Syndromes: The two vertebral arteries join to
form the basilar artery at the junction of the medulla and pons.
The basilar artery terminates into two posterior cerebral arteries
at the upper midbrain level. The posterior cerebral arteries are
connected to the middle cerebral arteries via the posterior
communicating arteries forming the circle of Willis. The
vertebral arteries and basilar artery supply the brainstem via
short circumferential and paramedian branches and through the
long circumferential branches supply the cerebellum. Lesions in
the vertebrobasilar system produces hemisensory deficits, visual
impairment, visual agnosia, prosopagnosia, dyschromatopsia,
alexia without agraphia, memory deficits, dysarthria, dysphagia,
disequilibrium and vertigo, and Horner’s syndrome.

19
3.6 Evaluation of a stroke patient
There are a number of guidelines for the management of patients
following stroke. In our hospital, the guidelines are broadly based on the
guidelines by the American Stroke Association(15). A few salient
features of the recent recommendations (March 2013) include the
following:
The goal of acute management is complete emergency evaluation
of patients with suspected stroke and initiate fibrinolytic treatment
within 60 minutes of arrival in emergency department. An
organized protocol is recommended for this evaluation (Class I;
Level of Evidence B).
Initial evaluation should include limited number of hematologic,
coagulation, and biochemistry tests with mandatory blood glucose
prior to the initiation of intravenous recombinant tissue
plasminogen activator (rtPA). Baseline electrocardiogram and
cardiac enzymes (troponin) assessment to assess for associated
Coronary Artery Disease (CAD).
Non–contrast-enhanced CT or MRI to determine ischemia by
presence of CT hypodensity or MRI hyperintensity to exclude

20
intracerebral haemorrhage since it is an absolute contraindication
to rtPA
CT perfusion and MRI perfusion and diffusion imaging including
measures of infarct core and penumbra especially for patients
beyond time windows for intravenous fibrinolysis who are being
considered for rtPA
Noninvasive imaging of the cervical vessels for patients with
resolved cerebral ischemic symptoms and for those with suspected
TIAs
CT angiography or magnetic resonance angiography of the
intracranial vasculature to exclude the presence of proximal
intracranial stenosis and/or occlusion.
The imaging study should be interpreted within 45 minutes of
patient arrival in the emergency department by an expert physician
or radiologistto prevent any delay in administration of rtPA.
3.7 Initial treatment (15)
1. Airway support, including ventilatory assistance to maintain
oxygen saturation >94%.

21
2. Cardiac monitoring at least for the first 24 hours for atrial
fibrillation and cardiac arrhythmias.
3. Lowering of the blood pressure keeping systolic blood pressure <
185 mmHg and diastolic blood pressure <110 mmHg is important.
Many patients have spontaneous decline in blood pressure during
the first 24 hours after onset of stroke. Medications should be
withheld unless the systolic blood pressure is >220 mm Hg or the
diastolic blood pressure is >120 mm Hg. No data are available to
guide selection of medications for the lowering of blood pressure
in the setting of an acute ischemic stroke.
4. Correction of hypovolemia and correction of hypoglycemia (blood
glucose <60 mg/dL) or hyperglycemia should be done.
5. Intravenous Fibrinolysis rtPA (0.9 mg/kg, maximum dose 90 mg)
for eligible patients within 3 hours of onset of ischemic stroke. For
patients with time period of 3 to 4.5 hours after stroke onset, rtPA
can be considered following exclusion criteria: patients >80 years
old, those taking oral anticoagulants, baseline NIHSS score >25,
imaging showing ischemic injury involving more than one third of
the middle cerebral artery territory, or patients with a history of
both stroke and diabetes mellitus.

22
6. Endovascular Intervention: Intra-arterial fibrinolysis is useful in
patients with major ischemic strokes of less than 6 hours duration
caused by occlusion of the middle cerebral artery who are not
otherwise candidates for intravenous rtPA (Class I; Level of
Evidence B). The optimal dose of intra-arterial rtPA is not well
established.
Mechanical thrombectomy (Class I; Level of Evidence A):
Emergent angioplasty and/or stenting of the extracranial carotid or
vertebral arteries using stent retrievers such as Solitaire FR and
Trevo are generally preferred to coil retrievers such as Merci. It is
used in patients with contraindication to intravenous therapy or
those with large artery occlusion not responding to intravenous
fibrinolysis. It can be used alone or in combination with
pharmacological fibrinolysis (Class IIa; Level of Evidence B).
Additional randomized trial data are needed to prove its
effectiveness. (New recommendation)
7. Anticoagulants: Urgent anticoagulation not recommended for
treatment of patients with acute ischemic stroke (Class III; Level of
Evidence A).
8. Antiplatelet Agents: Oral Aspirin (initial dose is 325 mg) within 24
to 48 hours after stroke onset is recommended.(Class I; Level of

23
Evidence A). Other intravenous antiplatelet agents inhibiting the
glycoprotein IIb/IIIa receptor is not recommended (Class III; Level
of Evidence B).
9. Neuroprotective Agents are not recommended since no
pharmacological agents have demonstrated efficacy (Class III;
Level of Evidence A).
10. Surgical interventions: Emergent or urgent endarterectomy is not
recommended for a small infarct core with large territory at risk
(eg, penumbra), for patients with compromised inadequate flow
from a critical carotid stenosis or occlusion, or in patients with
unstable neurological status (either stroke in-evolution or
crescendo TIA), (Class IIb; Level of Evidence B).
3.8 Admission to the Hospital and Acute
Management (After Hospitalization)
The use of comprehensive specialized stroke care (stroke units)
including rehabilitation, as shown in Table 4, is recommended
(Class I; Level of Evidence A).

24
Table 4: Intervention post-acute phase with level of evidence
Intervention Level of evidence
Antibiotics : Suspected pneumonia or Urinary
tract infection
(Class I; Level of
Evidence A)
Anti-coagulants: to prevent deep vein
thrombosis
(Class I; Level of
Evidence A)
Nasogastric/ nasoduodenal/ PEG1 feeds: for
nutrition and adequate hydration especially in
patients with inadequate swallowing
(Class I; Level of
Evidence B).
Early mobilisation (Class I; Level of
Evidence C)
Early Interventions to prevent recurrent stroke (Class I; Level of
Evidence C)
Anticoagulants or aspirin: for DVT2
prophylaxis
(Class IIa; Level of
Evidence A).
Treatment of acute neurological complications
Anti-oedema measures Class I; Level of
Evidence A

25
Close monitoring for signs of neurological
worsening
Class I; Level of Evidence
A
Decompressive surgical evacuation of a space-
occupying cerebellar infarction for treating
herniation and brain stem compression
(Class I; Level of
Evidence B).
Decompressive surgery for malignant oedema
of the cerebral hemisphere is effective and
potentially life saving
(Class I; Level of
Evidence B).
Ventricular drain for acute hydrocephalus ---
Anti-epileptics for recurrent seizures ---
1PEG: Percutaneous Entero Gastrostomy,
2DVT: Deep Vein Thrombosis
Rehabilitation is usually initiated during the acute phase. Subsequent to
the acute phase, rehabilitation depends on the deficits and disabilities in
an individual. The site and size of the initial stroke lesion and the extent
of subsequent recovery usually determines the long term effect of stroke.

26
3.9 Neurologic Recovery
Neurological recovery begins immediately after the stroke with initial
recovery in areas of the ischemic penumbra, mainly following resolution
of oedema and associated mass effect. Subsequently for several months,
cerebral plasticity and functional re-organization of the cerebral cortex
forms the basis for this recovery through spontaneous and learning-
dependent processes. This involves restitution (restoring the functionality
of damaged neural tissue), substitution (reorganisation of partly-spared
neural pathways to relearn lost functions), and compensation
(improvement of the disparity between the impaired skills of a patient and
the demands of their environment)(4). This learning dependent process is
observed with intensive training in stroke survivors and research is on-
going to determine the optimal training program to achieve maximal
motor recovery. Therefore approaches for rehabilitation have started
including interventions and therapy facilitating neuroplasticity, apart from
the compensatory techniques such as ambulating with a cane and AFO
for lower limb motor impairment.
Recovery from Impairments:
In the majority of hemiparetic patients, there is a classic pattern of
recovery. The functional motor recovery in the arm is less than in the leg,

27
reason being that ischemic strokes affecting the MCA territory are more
common than those affecting only the anterior cerebral artery territory.
This is due to higher flow through the MCA and the more direct path for
embolism. Other reason is the distinct functional demands placed on
the upper versus the lower limb. The lower limb can be functional with
some gross voluntary movements and its ability to maintain extended
position while the upper limb requires fine motor control for functional
tasks (12)
3.10 Motor Impairment
Motor impairment restricting mobility is the most easily
recognisable impairment. Motor impairment can include deficits in
muscle power (the speed with which force can be generated), motor
control and coordination, muscle tone, and balance(12).
Prior to specific motor problems related to CVA sequelae, a review
of the normal gait cycle and ankle biomechanics would enable better
understanding of the impairments following stroke.
3.10.1 Normal Gait:
Bipedal locomotion is unique to human beings with each person
having a characteristic gait pattern. It is a continuous movement with
repetition of the basic unit called the gait cycle. Each gait cycle starts

28
from the time a limb strikes the ground and continues till the whole
episode re-occurs on the same side. It has an alternate pattern of one
lower limb supporting the body weight and other limb advancing and
propelling the body further(14,16).
Hence, each gait cycle comprises of two phases: stance phase where
the foot is in contact with ground and swing phase when the foot is in the
air for limb advancement(14,16). Further functional subdivisions of the
swing and stance phase are as follows:
1. Stance phase:
Initial contact: Foot strikes the ground
Loading response: Foot in flat position on the ground till the
opposite foot is off the ground for swing at the end of double limb
support. It forms 11% of gait cycle
Midstance: body weight is directly over the supporting lower
extremity and involves lifting of the opposite foot until the
ipsilateral tibia is vertical. It starts at 11% of gait cycle and ends at
30 % of the gait cycle when the weight is directly over the
ipsilateral limb.
Terminal stance: It begins when weight is directly over the
supporting limb and continues until the opposite foot contacts the

29
ground (contralateral initial contact). It extends from 30 % of gait
cycle to 50% of the gait cycle.
Pre-swing: It begins with initial contact of the opposite foot and
ends with ipsilateral toe-off, i.e, toe of the ipsilateral foot leaves the
ground. It forms 10% of the stance phase.
2. Swing Phase:
Initial swing: involves the lift-off of the foot from the floor and
ends with alignment of the foot to the opposite foot until maximum
knee flexion occurs.
Midswing: begins with alignment of the ipsilateral foot to the
opposite foot and ends when the tibia is vertical.
Terminal swing: begins with vertical tibia and ends when the foot
contacts the ground (initial contact).
During the gait cycle, based on the foot-floor contact, the stance
phase can additionally be subdivided into two periods of double limb
support and one period of single limb support. Double limb support is the
period when both feet are on the ground for transferring the body weight
from one limb to the other. This period is seen during the beginning and
the end of the stance phase. When double support is absent completely,
the locomotion is running. Single limb support periods initiates when the

30
opposite foot is lifted off the ground for the swing phase. The gait cycle is
broadly divided into 60% of the stance phase and 40% of the swing phase
and approximately 10% overlap for each double support time. These
ratios changes with the variation in velocity of ambulation(14,16).
Gait cycle is further subdivided into different periods for better analysis.
The stride period is the time period involving an event of one foot till the
recurrence of the same event for the same foot, i.e., the initial contact to
the next initial contact of the same foot Stride length is the distance
covered between same events of the same foot in the direction of
progression during one stride. The step period is the time measured
from an event in one foot to the subsequent occurrence of the same event
in the other foot. Hence, each stride period of the gait cycle has two
step periods. Step length is the distance covered between the feet in the
direction of progression during one step. Cadence refers to the number
of steps in a period of time (commonly expressed as steps per minute).
The step length, step time and cadence are found to be symmetric for
both legs in normal individuals and is useful in identifying and
measuring asymmetry between the two sides of the body in pathologic
conditions and hence, are useful parameters when evaluating pathologic
gait(14,16).

31
3.10.2 Role of ankle muscles in normal gait and
biomechanics
Ankle dorsiflexors form the anterior compartment muscles of the
lower limb and include tibialis anterior, extensor hallucis longus,
extensor digitorum longus and peroneus tertius. They originate
from the tibia and fibula and adjoining interosseous membrane and
are inserted into the tarsal and meta-tarsal bones and phalanges of
the toes(16,17).
Ankle plantarflexors form the posterior compartment muscles of
leg and are classified as superficial and deep. The superficial
muscles include gastrocnemius, soleus and plantaris. Deep muscles
are popliteus, flexor digitorum longus, flexor hallucis longus and
tibialis posterior. Gastrocnemius originates from the femur and
capsule of knee joint and soleus from the tibia and fibular shaft.
Tendon of gastrocnemius and soleus fuses to form tendo-calcaneus
(achillis) and is inserted into the posterior surface of the
calcaneum. Rest of the muscles originate from tibia and fibular
shaft and adjoining interosseous membrane and are inserted into
tarsal bones and phalanges of the toes(16,17).

32
Nerve supply to these muscles is from the tibial and common
peroneal nerves, both of which are terminal divisions of the sciatic
nerve. The tibial part is formed by ventral divisions of anterior
primary rami of L4, L5, S1, S2, S3 and common peroneal nerve is
formed by dorsal divisions of anterior primary rami of L4, L5, S1,
S2. The common peroneal nerve is the smaller terminal branch and
extends from the superior angle of popliteal fossa to lateral angle,
along the medial border of biceps femoris. It continues and winds
around the posterolateral aspect of the neck of fibula, passes
through peroneus longus and divides into superficial and deep
peroneal nerves. The deep peroneal nerve supplies the anterior
compartment muscles. The tibial nerve is the larger terminal
branch of the sciatic nerve and extends from the superficial angle
to inferior angle of the popliteal fossa crossing popliteal vessels
from lateral to medial side. It gives muscular branches to posterior
compartment muscles(16,17).
3.10.3 Biomechanics of the ankle
Ankle joint is the articulation between the distal tibia and fibula
proximally and the body of the talus distally. It is a synovial hinge joint
and has single oblique axis with one degree of freedom around which the
motions of dorsiflexion/ plantarflexion occur. Muscles near ankle joint

33
produce movement across the sagittal, frontal, and transverse planes.
Dorsiflexion is the movement of the distal end of the foot towards the
tibia occurring in the saggital plane and in coronal axis and has a range of
10 – 20 degrees. Plantarflexion involves motion of the distal end of the
foot away from the tibia and has a range of 20 – 50 degrees(16).
The muscles function is dependent on where the muscle crosses in
relation to the joint axis. Hence, muscles passing anterior to ankle joint
act as dorsiflexors and posterior to the joint as plantarflexors. The
muscles on medial side of joint function as supinators and those on the
lateral side as pronators of the ankle. The muscles crossing the ankle joint
also cross the subtalar joint and hence, act at both joints resulting in a
combination of functions.
Any restriction or tension in the muscle property can affect the range of
joint. Gastrosoleus acts as plantarflexor when contracting concentrically
and on contracting eccentrically control dorsiflexion. Any limitation in its
length can result in limitation of dorsiflexion since it passes posterior to
ankle joint. This is especially evident when knees are extended as the
short gastrocnemius is lengthened over two joints (ankle and knee) in
knee extension. Since the Gastrosoleus tendon passes medial to the
subtalar joint and because of increased surface area, it becomes a
powerful supinator of the joint. Rest of the posterior compartment

34
muscles (tibialis posterior, flexor hallucis and flexor digitorum)
contribute to 5% of plantarflexion(16).
Anterior compartment muscles act as dorsiflexors as they pass anterior to
ankle joint and are activated in different phases of gait as discussed
subsequently. The extensor hallucis longus also extends MTP joint of
hallux and prevents dragging of the big toe. The extensor digitorum
longus and the peroneus tertius muscles insert anterior to ankle joint and
lateral to the subtalar joint axis and acts as dorsiflexors of the ankle and
pronators of the hindfoot. The extensor digitorum longus muscle also
keeps the lateral four toes up when foot is off the ground by extending the
metatarsophalangeal joints of toes. Tension in the anterior compartment
muscles can limit plantarflexion. Muscles are assisted in their function by
the ligaments which prevent excess dorsiflexion and plantarflexion,
minimize medio-lateral movement and/or rotation of ankle(16).
Ankle dorsiflexors during the stance phase of the gait cycle keeps foot in
neutral position at initial contact and contracts eccentrically in loading
response to make foot come in full contact with the ground. During the
swing phase, it contracts concentrically to keep the foot in neutral
position and clear the ground and help in limb advancement(16).

35
Ankle plantarflexors eccentrically contract during the midstance and
undergoes concentric contraction in the terminal stance and pre-swing, to
generate sufficient push-off for the limb advancement(16).
3.10.4 Gait impairments seen in stroke:
In stroke, there is residual weakness of the limbs with distal muscles
being weaker than the proximal. The weakness of the ankle dorsiflexors
leads to a condition called foot drop. The ankle plantarflexor spasticity or
contracture further contributes to the condition. Foot drop is seen in other
UMN conditions also like spinal cord injury, multiple sclerosis, cerebral
palsy, head injury and in LMN lesions as well. In the LMN lesions
(peripheral nerve injuries, neuropathies, drug toxities, diabetes), there is
direct damage to common peroneal nerve and cortical connections
(cortico-spinal tracts) are intact(12).
However, in UMN lesions, as in stroke, the foot drop is accompanied by a
number of other typical abnormal movement patterns like reduced knee
flexion during swing and stance phases (spastic paretic stiff-legged gait),
knee hyperextension (dynamic recurvatum) during stance, and excessive
ankle plantar flexion (equinus) during swing and/or stance(12).

36
Hence, in many stroke survivors, compensatory manoeuvres such as hip
circumduction, hip hiking, and contralateral vaulting with excessive
elevation of the pelvis to avoid toe drag is seen. In these patients, there is
asymmetry of stepping with reduced percentage of the gait cycle in
single-limb stance (SLS) on the affected side. There is a prolonged period
of weight release for the hemiparetic limb during double limb stance
(DLS) to correct foot drop. All these gait abnormalities lead to speed
reduction and associated increased energy cost and effort for
ambulation(12).
3.11 Rehabilitation in Stroke
Stroke rehabilitation broadly comprises of:
• Initial assessment to identify the patient's needs
• Goal setting to define realistic and attainable goals for
improvement
• Intervention to assist in the achievement of goals
• Reassessment to assess progress against agreed goals
Initial assessment done within few days post-stroke, should include a
complete neurological examination. This helps in prognostication,
entailing the rehabilitation plan, evaluation of long-term rehabilitation

37
needs and identifying the appropriate rehabilitation setting. Patients with
isolated disabilities such as a partial aphasia, visual loss, or monoparesis
can receive an out-patient rehabilitation(4)
3.11.1 Principles of Stroke rehabilitation include the following
as mentioned in table 5: - (4)
Table 5: Principles of stroke rehabilitation
Goal setting Specific, measurable and time-dependent to
guide management.
High-intensity practice Increased therapy or intervention.
Multidisciplinary team
care
Team of medical, nursing, therapy, and social-
work staff providing rehabilitation inputs and
coordinating their work
Task-specific training Rehabilitation approaches where specific
functional tasks are practised repeatedly.
3.11.2 Rehabilitation related to motor impairments
Motor impairments include weakness, incoordination and spasticity.
Spasticity can be managed conservatively with stretching, positioning,
oral antispasticity medications, use of injection therapy (principally
botulinum toxin, but previously more commonly phenol or alcohol

38
injection).Initial early poststroke phase should also include prevention of
contractures or nerve pressure palsies. Hence, proper positioning in bed
and wheelchair and range of motion exercises for all joints should be
done daily.
Numerous guidelines exist for stroke rehabilitation for motor impairment.
The latest guidelines by NICE released in June 2013 recommends initial
physiotherapy for at least 45 minutes of each relevant rehabilitation
therapy for a minimum of 5 days per week for people who have the
ability to participate, and where functional goals can be achieved. Later
the rehabilitation therapy is modified according to the person's needs at
that time. Treatment is recommended to be continued until the person is
able to maintain or progress function either independently or with
assistance from others(18).
Progressive strengthening exercises include increasing repetitions of body
weight activities (for example, sit-to-stand repetitions), weights (for
example, progressive resistance exercise), or resistance exercise on
machines such as stationary cycles. Approaches to facilitate and enhance
motor recovery, including traditional approaches by Rood, the
neurodevelopmental technique advocated by Bobath, Brunnstrom
technique, proprioceptive neuromuscular facilitation, rehabilitation
approaches where specific functional tasks are practised repeatedly,

39
functionally oriented exercise training (such as practising transfers and
early ambulation), and a recent focus on repetitive task-oriented practice
has been tried. Walking therapies like treadmill with or without body
weight support helps in mobility training for stroke patients.
Electromechanical gait training is still in the research/ experimental
stages(18).
The conventional ambulation training is mainly with use of Ankle–foot
orthoses (AFO). Ankle foot orthosis is a device applied externally over
the ankle and foot of the lower limb which can be fabricated from
metal/leather, thermoplastics, carbon, graphite, or a hybrid design
assembly incorporating some or all the mentioned materials . It can be a
solid ankle or articulated type or a leaf spring type. It helps in providing
foot clearance in the swing phase of the gait cycle thereby prevent
tripping and falling. It also provides stance-phase control by preventing
knee and ankle collapse or by preventing knee hyper-extension that in
turn, affects walking. Effectiveness of AFO is determined in terms of
speed, ease of walking and comfort (5,14).
The alternative is the Functional Electrical Stimulation (FES) system. As
per NICE guidelines, 2013, there is adequate evidence on the safety and
efficacy ( in terms of improving gait) of FES for drop foot of central
neurological origin to support its use (18).

40
3.12 FES system
Electrical stimulation can be used in a number ways in rehabilitation. It
can be used for therapeutic or functional purposes. Therapeutic
stimulation induces physiological changes that are persistent even after
stimulation and thereby improve the voluntary contraction. It therefore
decreases or prevents further impairment as a consequence of
immobilisation or disuse atrophy(19).
Functional Electrical Stimulation (FES) is the application of electric
current to stimulate nerve or muscle to generate muscle contraction and
incorporation of multiple co-ordinated muscle contractions to bring about
functional activity. The effect lasts till the time the FES application
system is giving the stimulation and hence, these systems have to be
donned by the user to bring about the functional activity and act as
replacement for the lost function. Hence, they are called neuroprosthesis.
They bring about specific, active repetitive movements to facilitate motor
relearning by reducing the intracortical inhibition as evidenced in
functional MRI (fMRI) studies. Hence, it facilitates probably motor
neuroplasticity via cortical mechanisms(19).
In the neuroprosthesis, electrical current is delivered via a pair of
electrodes which generates a localised electric field causing

41
depolarisation of motor axonal membranes. When the depolarisation
reaches the critical threshold, the sodium ions move from the
extracellular compartment to the intracellular space leading to an action
potential. This action potential propagates from the site of stimulation and
reaches the axon terminals, releasing the neurotransmitter and causing the
contraction of muscle fibres.
The advantage is easier stimulation of nerve than muscle. The lowest
level of current is able to stimulate neural tissue since the stimulation
threshold for neural tissue is lesser than that of the muscle fibre. Hence,
for the application of neuroprosthesis, the peripheral nerve should be
intact, i.e., lower motor neurons must be preserved from the anterior
horns of the spinal cord to the neuromuscular junctions of the target
muscles(19).
On application of neuroprosthesis to nerves, the large diameter axons get
excited as they have a lower stimulus threshold and preferably, recruit the
type 2 muscle fibres (fast fatiguing). With disuse that occurs in any
chronic disease, the type 1 muscle fibres (fatigue resistant) get converted
to the type 2 muscle fibres (fast fatiguing). However, fatigue resistant
fibres are required for the application of neuroprosthesis and hence, over
a period of time, use of neuroprosthesis converts these fast fatiguing
fibres to fatigue resistant fibres. Also, application of neuroprosthesis

42
should be accompanied by muscle conditioning regimen to maintain
fatigue resistant muscle. Electrodes for the neuroprosthesis delivering the
stimulation should be placed in close proximity to the target nerve as the
trans membrane potentials generated in axons near the electrode are
largest and the electric field generated is maximum(19).
The stimulation parameters determining the waves of current pulses and
therefore strength of a muscle contraction include the pulse frequency,
amplitude, and duration. The ideal stimulation frequency is the lowest
frequency producing a fused contraction. This in turn depends on the type
of muscle fibre and manner of stimulation delivery (surface vs. implanted
electrode). A too low pulse frequency produces a series of twitches and
increase in frequency causes overlapping of twitches to produce a fused
contraction (temporal summation). However, if the frequency is too high,
the muscle fatigues more rapidly. Hence, exact pulse frequency is needed.
Increase in the pulse amplitude and pulse duration also increases the
strength of muscle contraction since it increases the electric charge per
pulse, generates a larger electric field and activates a broader region and
thus recruits more axons and more motor units (spatial summation). In
most neuroprostheses, pulse frequency is kept constant and modulation of
the pulse amplitude and pulse duration controls the strength of the muscle

43
contraction. The pulse frequency is not only constant but also as low as
possible to prevent premature muscle fatigue(19).
3.12.1 FES system components:
Functional ES systems comprises of electrodes, a multichannel
stimulator, and a controller. The stimulator produces the current
waveforms for multiple cathodes and this current is delivered to the
excitable tissue via the electrodes. The controller regulates the
stimulation according to the user. The controller can be a simple switch
modulated by the patient on and off, or may include sensors recording
patient-elicited bio potentials (e.g., EMG or EEG) and using these signals
to regulate the stimulation(19).
Electrodes used include an active electrode or cathode placed near the
nerve or muscle motor point to be stimulated and the return electrode or
anode over less excitable tissue (tendon or fascia). In multichannel
NMES systems, additional electrodes are required to bring about
simultaneous activation of multiple muscles in a co-ordinated manner.
They use either a bipolar (1 anode for each cathode) or monopolar (1
anode for multiple cathode) arrangement of electrodes. Bipolar
multichannel systems allow greater selective activation but require more
electrodes and leads. Monopolar electrode systems addresses this issue by
reducing the number of electrodes(19).

44
Based on arrangement of the electrodes, multichannel stimulator and the
controller, the neuroprosthesis can be categorized as surface,
percutaneous, or implanted. In surface systems, all the three components
are external to the body. The advantages include the easier application of
the electrodes, reversible and non-invasive stimulation mode and being
relatively inexpensive. These systems also have disadvantages like
inability to produce isolated muscle contractions, change in electrode
position with movement of the target muscle causing inconsistent muscle
contraction and force production, varying position of electrodes due to
daily donning and doffing of the device and intolerance to increased
sensation of stimulation application site mainly due to stimulation of
cutaneous pain receptors. In order to overcome these disadvantages,
implanted electrodes were designed(19).
In percutaneous systems, stimulator is external and connected through
leads to the electrodes implanted near a muscle or nerve. This activates
deep muscles and hence provides isolated and repeatable muscle
contractions. Since it does not stimulate the sensory afferents in the skin,
the chances of pain during stimulation are minimal. The electrodes are
made of multifilament lead within a single insulator with a helical
configuration to produce maximum flexibility. The electrodes are inserted
using a hypodermic needle with withdrawing of the needle leaving the

45
electrode in place and lead exiting the skin. The exit sites on the skin are
cleaned and maintained to reduce the risk of complications. The return
electrode is a large surface electrode. Since they are minimally invasive,
they investigate the feasibility of functional muscle contractions prior to
implantable system surgery and hence, have served as precursors to fully
implanted systems. The longevity of percutaneous electrodes and failure
of the system depends on type of percutaneous lead, lead-routing
technique, and the muscles implanted. Potential complications include
infection due to electrodes and granuloma formation due to retained
electrode fragments(19).
In implanted systems, both electrodes and stimulator are implanted and
the controller components are either external or partly implanted and
partly external. It is mainly designed for long term use. The connection
between the controller and stimulator is through radio-frequency (RF)
transmission. The stimulator receives radio-frequency impulses, generates
stimuli and directly sends to the implanted electrodes connected directly
to the implanted stimulator with inline connectors. The RF link eliminates
the need for an active battery and the need for replacements. The
controller receives inputs from the user via switches, sensors, an
implanted joint angle sensor, or bio potential electrodes to determine
stimulation accordingly. Implanted systems have advantages mainly in

46
terms of improved convenience, cosmesis, reliability and repeatability.
Electrodes used for implanted NMES systems include epimysial
electrodes (sutured directly to the epimysium on the muscle surface),
intramuscular electrodes (inserted directly into a muscle belly), epineural
electrodes(sutured to the connective tissue surrounding a motor nerve and
nerve helix) or cuff electrodes (implanted around a nerve)(19).
Numerous neuroprosthesis have been tried to facilitate functional activity
in paralysed lower limbs affected by UMN lesions (like traumatic brain
injury, stroke) as the peripheral nervous system is still intact in these
patients. One of the commonest used and experimented is drop foot
stimulator. Drop foot stimulator or peroneal stimulator involves
application of electric current to stimulate intact peroneal nerve to
generate muscle contraction and enhance gait by improving foot
clearance during swing phase and stability during initial stance phase(19).
3.12.2 Drop foot stimulator or peroneal stimulator(PS)
The concept of foot drop stimulator was first proposed by Liberson in
1961 where he synchronized the electrical stimulation to swing phase of
gait cycle using a foot-switch and achieved the orthotic effect of
stimulation. Thereafter, a number of modifications have been made over
the past 6 decades ranging from hard wired single channel surface
stimulator to hard wired multichannel surface stimulator to single channel

47
implanted system followed by microprocessor based surface and
implantable single/ multichannel DFS systems(6).
There has been an evolution in the footswitches being replaced by sensors
initially artificial and currently natural sensors. The artificial sensors
include a tilt sensor (an accelerometer which detects the joint segment
orientation and determines the stimulus for dorsiflexion). Natural sensors
like the sural nerve, a purely sensory nerve, have also been tried where
inputs are the touch sensors on the lateral part of the foot and detects if
the affected foot was supporting weight. This information was used to
control the application of stimulus in the DFS. There are DFS systems
incorporating real-time control of FES. There also have been
development and trial of completely implanted DFS systems(6).
3.12.3 Studies related to the PS
There have been a number of studies to report positive orthotic effect of
FES. Evidence based review for stroke rehabilitation done in Canada in
2007 by commissioned group states that there is strong (Level 1a)
evidence that FES and gait retraining results in improvements in
hemiplegic gait(20). East midlands specialized commissioning group in
April 2011 evaluated orthotic effect of the drop foot FES system and
found that there are nearly 15 studies including 2 systematic reviews that
reported positive effect. It also mentions that 3 high quality and two low

48
quality systematic reviews show inconclusive evidence for effectiveness
of stimulator in treatment of drop foot(21).
NICE guidelines, 2013 have recommended the use of FES system based
on the current evidence on its safety and efficacy(18). Recent studies
have shown that the stimulator has significant orthotic effect in
comparison to no orthosis(13). There have been small scale and also
multicentre trial studies that have directly compared the system with
conventional AFO(7–9). These trials still have not proven which of the
two is better since patients in both the groups were found to improve
significantly. Studies have also shown that there is near normal gait
pattern with the stimulator group(22).
In most of the trials, the peroneal stimulator has been tried in the chronic
phase of the stroke. Few studies have investigated its use in the acute and
sub-acute phases (23,24).
Currently, FES systems are being tried outside the clinical settings, on a
daily use basis. However, the evidence that the drop foot system is more
beneficial than AFO is lacking.
This study is designed for trial of drop foot system in Indian rehabilitation
settings. It involved the use of a stimulator with a user controlled hand
switch making it technically simpler and more adaptable device for use,

49
the sensor being the user controlled switch. The stimulator was adapted to
Indian settings mainly in terms of its low cost, small size, no requirement
for foot switch, allowing bare-foot walking. The study proposed to
compare its use in the rehabilitation of patients in the sub-acute and
chronic phases of stroke (which largely is the stroke population admitted
in our rehabilitation set-up) and its comparison with AFO.

50
4. Methodology
4.1. Study Design: Randomized Control Trial, pilot phase, parallel
groups
4.2. Settings and locations where the study was conducted:
Department of Physical Medicine and Rehabilitation, Christian Medical
College, Vellore.
4.3. Participants: Persons with hemiplegia secondary to
cerebrovascular accident
I Inclusion Criteria:
Age 18 to 70 years
Adequate cognition and communication abilities (> 18/30 on
MMSE)
History of independent function prior to stroke, including walking
with assistive device
2 weeks to 1 year post stroke
Inability to dorsiflex ankle to clear foot during swing phase of gait

51
Ankle dorsiflexion range of motion coming to at least neutral in
affected lower limb with application of peroneal FES stimulation
Ability to walk 5 meters using AFO and quadripod inside parallel
bar.
II. Exclusion Criteria:
Excessive pain in affected leg (>5 on a 10 point visual analog
scale)
Participating in any other studies
Implants such as cardiac pacemaker or vagal nerve stimulator or
implants generating electrical signals or implants in lower limb
having metal parts
Lower motor neuron disease or injury resulting in inadequate
response to stimulation
Significant swelling in affected leg extending up to knee
Disease limiting wearing of orthosis such as venous stasis or
history of lower extremity ulcer, chronic skin condition or
peripheral neuropathy
Pregnancy

52
Pre-existing orthopedic condition or history of pain that could limit
ambulatory progress (eg: total hip or knee replacement, limited
ROM, arthritis)
Contracture of ankle
4.4. Sample size: 20 (10 in experimental group and 10 in control
group). Since the study was testing the feasibility of the user controlled
hand switch based peroneal stimulator in a clinical setting, it was done as
a pilot study and both intervention and control participants were kept at
equal numbers.
Approval was obtained from the Institutional Review Board and Ethics
committee.
4.5 Randomisation:
Method of allocation concealment: Serially labelled opaque envelopes
concealed random allocation
Method of randomization: Block randomisation (block size=5); (uniform
distribution random numbers generated by computer)
Blinding and masking was not possible as the stimulator and AFO are
externally applied. However, the outcome assessor was not directly
involved with the study.

53
Implementation: The random allocation sequence was computer
generated and was concealed in opaque envelopes. After the recruitment
of the participants by the principal investigator based on the inclusion/
exclusion criteria, an informed written consent was obtained and a pre-
analysis of the outcome measures was done. The group to which the
particular patient was assigned to was disclosed by the statistician to the
principal investigator. The participants were accordingly assigned to the
respective therapists for the intervention and control group for 3 weeks.
4.6. Interventions: Both the groups initially received physiotherapy
for 3-4 weeks as per the requirement to ambulate for 5 meters within
parallel bars. Following this, they were randomly allocated into PS group
and AFO group.
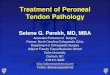
Peroneal Nerve Stimulator(PS): The device as shown in figure 2
included 3 components: (i) a pair of surface electrodes (square shaped
and re-usable), (ii) an electrical stimulator with in-built microprocessor
based controller and (iii) a hand switch mounted on the quadripod. The
stimulator is an in-house development of the Department of
Bioengineering of our institution. It has the following specifications:
frequency= 20 Hertz, pulse amplitude=70 milli Amperes, pulse width=
250 microseconds. It was operated using a small mobile phone battery.

54
The stimulator was controlled by a push-button switch, and was normally
off.
The cathode electrode was placed over the common peroneal nerve (as
identified 2 cm below the head of fibula where the nerve winds around
the fibular neck) and the anode electrode was placed over the anterior
compartment muscles. The electrode locations were adjusted so that
maximum ankle dorsiflexion was noticed. The inter-electrode distance
was usually around 4 cm.
The electrodes were connected through wires to the portable stimulator,
often kept in the trouser pocket of the participant. The stimulator was
further connected through wires to the switch placed on the quadripod,
which the participant held on the unaffected side.
Figure 2: In-built User Controlled Peroneal Stimulator

55
On pressing the switch by the subject during the pre-swing phase of gait
of the affected limb, the electric stimuli generated, are transmitted via the
electrodes to the common peroneal nerve. This activates the dorsiflexors
of the ankle and toes causing ankle lift resulting in ground clearance
during the swing phase for the affected limb. As the limb progressed
towards initial contact of the stance, the participant would release the
switch and stimulation would stop. Since the switch release was done at
the initial contact, the stimulation was continued till initial loading
response and helped in smooth foot contact thereby, preventing the foot
slap. Hence, the switch press was co-ordinated with different gait phases
and required the patient to voluntarily control the movement.
The patient received gait training with the peroneal stimulator and
quadripod for 1 hour during the therapy time. Initial 4 days were given as
the familiarisation time to get used to the stimulator and understanding
the mechanism of operating and co-ordination of the switch. Remaining
hours of the therapy training was continued with AFO and walking aid
since the patient had to be discharged from the hospital with an AFO.
Control group: The control group received gait training using AFO and
walking aid all throughout the therapy hours.

56
At the end of 3 weeks, post-intervention analysis was performed for both
groups and a feedback form was used for the intervention group to assess
the patients’ satisfaction with the device.
4.7. Outcome measures:
4.7.1. Primary Outcome:
The effectiveness of peroneal stimulator was measured in terms of
walking speed and endurance.
1. Walking speed was assessed by the 10 meters walk test in meters
per second(25). This test involves the individual to walk a distance
of 10 meters with or without assistive device at self-selected
“comfortable speed” and at “as-fast-as-possible” speed. The time
taken for initial and last 2 meters is not used for measurement to
accommodate for the acceleration and deceleration. The starting
time is when foot crosses 2 meters mark and stop time is when the
foot crosses 8 meters and this intermediate time duration for the
intermediate 6 meters is considered. A total of 3 trials is done and
an average of the three time durations is taken. The speed is
obtained by dividing the 6 meters with the calculated average time.
2. Walking endurance is measured by the 6 minute walk test(26). It
measures the distance walked in the time period of 6 minutes over

57
an even surface kept constant for all the participants. Each patient
is asked to perform at the preferred speed possible.
4.7.2. Secondary Outcomes:
Kinematic Gait parameters:
1. Step length ( distance covered during an event of one foot till the
recurrence of the same event for the other foot ,i.e., the initial
contact of the one foot to the initial contact of the alternate foot)
Spatial Asymmetry: derived from the step length of the each
patient using the formula:
Step length (unaffected limb) – Step length (affected limb)/ Step
length (unaffected limb)
2. Stride length (distance from heel strike of one leg to heel strike of
the same leg in meters)
3. Stance percentage: Duration of swing phase and stance phase is
measured. Stance percentage is computed as percentage of stance
duration for each stride.
All these parameters were assessed in the Gait lab of the Department of
PMR The patient had infra-red LEDs placed on specific points on their
limbs and ankles and their movements were recorded on infra-red

58
sensors. A computerized system computes the position of limbs and the
information hence obtained, gives the above data.
4. Dynamic range of motion of the ankle (during ambulation):
The ankle angle change in the PS group is calculated for the period
when the stimulator was switched on up to its switch off period.
This is done from the video analysis of the gait cycle of each
participant (as explained subsequently). The change in ankle is also
timed according to different phases of gait cycle. The difference
between the maximum plantarflexion during the pre-swing and
maximum dorsiflexion during the midswing is taken as the ankle
angle change and is attributed as the orthotic function of the PS.
The ankle angle in control group using AFO was taken as neutral
(0 degrees).
Statistical analysis:
Data collection and outcome assessment: The primary and secondary
outcomes for all the 20 patients were measured by a neutral assessor (gait
lab co-ordinator) both for pre and post-intervention analysis. The derived
calculations were done by the principal investigator.
It is should be noted that during the study period, there was technical
difficulty in the force plate system of the gait lab and hence, computer

59
generated values from patient no. 7 till patient no. 14 could not be
obtained. Hence, a manual calculation of each of the kinematic
parameters from the video was done as follows:
A gait cycle perpendicular to the camera is selected from the chosen
video. The frames sorting each phase of the gait cycle was obtained and
using the software GIMP and individual’s shank length, the step length
and stride length were calculated. The number of frames corresponding to
the stance phase was calculated as percentage of the total gait cycle.
The same frame is used to assess the ankle angle range. Each frame is
labelled according to the gait phase and ankle angle is calculated in each
frame and the difference of the maximum plantarflexion and maximum
dorsiflexion is calculated. This difference was accepted as the ankle angle
change.

60
Figure 3: Video frame with Maximum Plantarflexion
Figure 4: Video frame with Maximum Dorsiflexion
4.8. Statistical methods:
Continuous variables were assessed using t-test (paired t test) (to check
pre-post effect) for within the groups.

61
For inter group comparison, Student t-test (two sample, unequal
variance) was used. Fischer exact test was used for inter group
comparison regarding the improved and not-improved categories.
Methods for additional analyses for subgroup analysis:-
Spearman's rank correlation coefficient (Spearman's rho) was used for the
subgroup analyses, i.e., MMSE score and the duration from the stroke
and their correlation with the outcome measures.

62
5. RESULTS
5.1. Recruitment, screening and randomization
More than 200 patients post stroke admitted as in-patients as well as
attending the outpatient clinics including the Stroke clinic were screened
for eligibility to participate in the study based on the inclusion criteria. 45
patients were found to match the inclusion criteria. Among them, 13
patients were excluded based on the exclusion criteria and 9 patients
refused to give consent for the study. 3 other patients were noted to have
significant behavioural issues hindering their participation in the
rehabilitation programme. Hence, 20 patients were enrolled and
randomised into intervention and control groups.
Both PS and AFO groups had 10 participants each and all 20 participants
received the treatment for 3 weeks. They were analysed for primary and
secondary outcomes both pre training and 3 weeks post training. There
were no drop-outs after recruitment throughout the study. The study was
conducted from 1st July 2012 to 3rd August 2013.

63
CONSORT(27)
Excluded (n= 25 ) Not meeting inclusion criteria
(n=13 ) More than 1 year (n=3) Cardiac Implants (n=2) Arthritic pain/ OA (n=2) Multiple co-morbidities
(n=4) Improved (n =1) Too much assistance (
n=1) Declined to participate (n=9 ) Other reasons (n= 3 )
Analysed (n=10)
Excluded from analysis (n=0)
Lost to follow-up (n= 0)
Discontinued intervention (n=0)
Allocated to Intervention PS (n=10)
Received allocated intervention (n=10)
Did not receive allocated intervention
(n=0 )
Lost to follow-up (n=0)
Discontinued intervention (n= 0)
Allocated to Control AFO (n=10)
Received allocated intervention
(n=10 )
Did not receive allocated intervention
(n= 0 )
Analysed (n=10)
Excluded from analysis (n= 0)
Allocation
Analysis
Follow‐Up
Randomized (n= 20)
Enrolment

64
5.2. Baseline demographic and clinical characteristics of
the participants
Baseline parameters among the subjects differed mainly in terms of
treatment of acute event and duration following the acute event. About 60
% of the participants in the intervention group were within 3 months of
the acute episode, 10% had stroke for 3-6 months and 30% had onset of
stroke more than 6 months ago. On the other hand, the control group had
a more uniform distribution of patients with 40 % within 3 months, 30%
within 3- 6 months and 30% had the stroke more than 6 months ago.
Among the intervention group, 60 % were managed conservatively
(non-surgically and no thrombolysis) while 60% of the control group
patients were treated with decompressive surgeries. Rest of the
parameters were uniform between the two groups.

65
Table 6: Demographic details in the AFO and PS group
Characteristics PS AFO
Age (mean+/- S.D) 45.8 +/- 13.73 56.3 +/- 8.95
Gender (Male /
Female)
10 / 0 9 / 1
CVA TYPE
Haemorrhage (H) 2 2
Ischemic ( I ) 8 8
Affected side (right/ left)
Right / Left 5/5 5/5
MMSE score
18 - 23 5 5
24 - 30 5 5
Treatment group
T1 (rt-PA) 1 2
T2 (conservative) 6 2

66
T3 (surgical
decompression)
2 6
T4 (rt-PA &
decompression)
1 0
Duration
< 3 months 6 4
3 – 6 months 1 3
> 6 months 3 3
5.3. Primary outcomes:
5.3.1. 6 minute walk test (Walking endurance):
At the end of 3 weeks, there was improvement in the mean walking
endurance for both the groups, but this was not statistically significant (p
value of 0.95 in control and 0.78 in PS). The difference between the two
groups at the end of 3 weeks was not statistically significant. (t-test for
intergroup comparison: p value: 0.423 and Fischer exact test p value: 1)
as shown in table 7.

67
Table 7: Primary Outcome- 6 minute walk test for AFO and PS
(meters)
Statistical tests AFO STIMULATOR
Pre Mean ±
S.D1
54.39 ± 37.72 59.56 ± 16.19
Post Mean ± S.D 73.8 ± 41.71 77.89 ± 46.89
Post-pre Mean ± S.D 19.41 ± 29.14 18.32 ± 42.75
Within group p-value 0.95 0.78
Inter-group t-
test
p-value Pre: 0.503 Post: 0.423
Fischer exact
test
p-value 1
1S.D: Standard deviation

68
5.3.2. 10 meters test (Walking speed):
There was improvement in the mean speed for both the groups. However,
it was not statistically significant (p value for AFO: 0.97 and PS: 0.794).
For intergroup, post analysis values calculated did not show any
statistically significant difference. (t-test for intergroup comparison: p
value: 0.456 and Fischer exact test p value: 1) as shown in table 8.
Table 8: Primary Outcome- 10 meter walk test for AFO and PS,
(time in minutes)
Statistical tests AFO STIMULATOR
Pre Mean ± S.D 9.84 ± 7.77 10.3 ± 2.79
Post Mean ± S.D 14.43 ± 8.65 13.3 ± 9.06
Post-pre Mean ± S.D 4.58 ± 5.77 3 ± 7.18
Within group p-value 0.97 0.794
Inter-group t-
test
p-value Pre: 0.41 Post: 0.456
Fischer exact
test
p-value 1

69
5.4. Secondary outcomes:
All the kinematic gait outcome measures had similar pattern with no
significant difference between the groups as well as within the groups.
5.4.1. Spatial Asymmetry: There was no significant change in the spatial
asymmetry in the PS (p-value: 0.713) or the AFO group (p value: 0.62).
The difference between the two groups was not significant (Fischer exact
test: p value: 1 and t-test for intergroup: p value: 0.718) as mentioned in
table 9.
Table 9: Spatial Asymmetry for AFO and PS, pre and post
intervention
Statistical Analysis AFO STIMULATOR
Pre Mean ± S.D 0.023 ± 0.313 0.0802 ± 0.39
Post Mean ± S.D 0.0913 ± 0.336 0.226 ± 0.326
Post-pre Mean ± S.D 0.068 ± 0.310 0.146 ± 0.49
Within group p-value 0.626 0.713
Inter-group t-
test
p-value Pre: 0.487 Post: 0.718
Fischer exact
test
p-value 1

70
5.4.2. Stride length:
The post intervention stride length improved in the AFO group and
reduced in PS group; but this was not statistically significant with
AFO group p value 0.668 and PS group p-value 0.417. The difference
was not statistically significant between the two groups (Fischer exact
test: p value: 1 and T-test for intergroup: p value: 0.373) as mentioned
in table 10.
Table 10: Stride length for AFO and PS (meters)
Statistical Analysis AFO STIMULATOR
Pre Mean ± S.D 45.1 ± 11.81 54.8 ± 12.99
Post Mean ± S.D 51.3 ± 17.44 50.5 ± 26.65
Post-pre Mean ± S.D 6.2 ± 24.4 -4.3 ± 29.16
Within group p-value 0.668 0.417
Inter-group t-
test
p-value Pre: 0.924 Post: 0.373
Fischer exact
test
p-value 1

71
5.4.3. Stance percentage (% of the total stride time):
No significant changes seen in the pre and post stance percentages in both
the groups [AFO (p value: (0.917) and PS (p-value: 0.565)] The
difference between the two groups was not significant [Fischer exact test
: p value: 1 and T-test for intergroup: p value: 0.486] as specified in table
11.
Table 11: Stance % for AFO and PS, pre and post intervention
Statistical Analysis AFO STIMULATOR
Pre Mean ± S.D 82.6 ± 8.07 77.9 ± 3.48
Post Mean ± S.D 78.2 ± 11.25 76.5 ± 10.12
Post-pre Mean ± S.D -4.4 ± 7.75 -1.4 ± 11.69
Within group p-value 0.917 0.565
Inter-group t-
test
p-value Pre: 0.91 Post: 0.486
Fischer exact
test
p-value 1

72
5.4.4. Dynamic ankle range of movement showed a mean ankle angle
change of 11.31 ± 3.56 degrees (between pre-swing to mid-swing phase)
as shown in table 12. This was nearly two-third of the normal ankle angle
change of 18 ± 2 (as determined in our gait lab for the normal subjects.)
Table 12: Ankle angle change before and during the stimulation
(degrees)
Sl.no. Maximum Drop Maximum Lift Difference
1 -30.08 -15.95 14.13
2 -23.2 -12.03 11.17
3 -26.08 -14.27 11.81
4 -7.88 2.74 10.62
5 -16.49 -2.29 14.2
6 -20.61 -16.41 4.2
7 -19.66 -12 7.66
8 -18.19 -7.62 10.52
9 -26.33 -9.3 17.03
10 -25.02 -13.24 11.78
Mean 11.312
S.D 3.56663801

73
IC LR MST PSW ISW MSW
Angle Chan
ge
GAIT PHASES
ANKLE ANGLE
Graph 1: Trend of ankle angle change in PS group patient
The graph above illustrates the trend of the ankle angle change seen in
one of the patients in the PS group. The graph nearly matches the
trajectory of the ankle angle change during gait cycle of a normal
individual.
Graph 2: Ankle angle change during normal gait cycle

74
5.5. Additional analysis:
Additional analysis was done to correlate the duration of stroke and
MMSE with the outcome measures.
5.5.1. Duration of the stroke:
The 6 minute walk test was found to have a statistically significant
inverse co-relation with duration of the stroke for the stimulator group
and no statistically significant difference for the AFO group (Graph 3).
The 10 meter walk test (Graph 4) and the spatial asymmetry (Graph 5)
was found to be non- significant for both stimulator and AFO group.
The ankle angle change (Graph 6) had a statistically significant
correlation with duration of the stroke in the PS group; i.e., in patients
with longer duration from the event of stroke, there was more increase in
the dynamic ankle angle change observed during the application of PS.
5.5.2. MMSE:
Change in the speed as noted with 10 meter walk test (Graph 8) was
better in patients with MMSE > 21 in the PS group as compared to the
patients with MMSE < 21. This was statistically significant. Similar
changes were not seen with AFO group.

75
The 6 minute walk test (Graph 7) and the spatial asymmetry (Graph 9)
was found to be non- significant for both stimulator and AFO group.
The ankle angle change (Graph 10) had a statistically significant
correlation with MMSE. Patients with MMSE > 23 had changes in the
ankle angle significantly better than patients with MMSE < 23 in PS
group.
5.6. User feedback:
Of the 10 patients in the stimulator group, 5 patients preferred PS over
AFO, 3 patients liked AFO and 2 patients could not decide which of the
two is better.
No adverse effects or harms were seen throughout the study.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
6 MIN PRE 6 MIN POST
Graph 3: Correlation of duration of stroke with 6 minute walk test pre
and post intervention

76
0
0.2
0.4
0.6
0.8
1
1.2
10 M PRE 10 M POST
AFO
PS
Graph 4: Correlation of duration of stroke with 10 meter walk test pre
and post intervention
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
SPAs Pre SPAs Post
AFO
PS
Graph 5: Correlation of duration of stroke with spatial asymmetry test
pre and post intervention

77
0
0.01
0.02
0.03
0.04
0.05
ANGLE
CHANGE
AFO
PS
AFO
PS
Graph 6: Correlation of duration of stroke with ankle angle changet pre
and post intervention
0
5
10
15
20
25
30
35
40
45
6 MIN PRE 6 MIN POST
AFO
PS
Graph 7: Correlation of MMSE with 6 minute walk test pre and post
intervention

78
‐0.8
‐0.6
‐0.4
‐0.2
0
0.2
0.4
0.6
0.8
10 M PRE 10 M POST
AFO
PS
Graph 8: Correlation of MMSE with 10 meter walk test pre and post
intervention
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
SPAs Pre SPAs Post
AFO
PS
Graph 9: Correlation of MMSE with spatial asymmetry pre and post
intervention

79
0
0.005
0.01
0.015
0.02
0.025
ANGLE
CHANGE
AFO
AFO
PS
Graph 10: Correlation of MMSE with ankle angle change pre and post
intervention

80
6. Discussion
This study aimed to study the orthotic effect of a user controlled hand
switch based peroneal nerve stimulator and compare it with the ankle foot
orthosis in patients with stroke having foot drop. After three weeks of
training with either PS or AFO, no statistically significant difference was
observed ‘between the two groups’ in terms of walking speed, walking
endurance and gait parameters including spatial asymmetry, stride length
and stance percentage. The results for ‘within group’ comparison also did
not reveal any statistically significant difference for the above parameters.
A number of factors could be attributed to the ‘no difference’ seen for
‘between the groups’ analysis. Firstly, patients in PS group received only
1 hour of training with PS and the remaining 6-7 hours of gait training
was with AFO. This was mainly due to the fact that patient was planned
to be discharged with AFO since the PS was still in the pilot phase and
also due to the technical constraints of a single PS device. Hence, the
training with AFO had to be continued for the intervention group as well.
Besides, the control group also received electrical stimulation for muscle
strengthening during the routine physiotherapy sessions. A small sample
size of 10 patients in each arm could also possibly contribute to the lack
of difference ‘between the two groups’.

81
A number of recent trials support similar findings. P. Kluding et al
conducted a 30 week multicentre randomised controlled single blinded
trial comparing the in-shoe pressure sensor based PS and AFO for stroke
patients more than 3 months duration with foot drop and found no
significant difference in the gait speed ‘between the two groups’ at the
end of 30 weeks(8). Similar findings were replicated by Richard B. Stein
et al in their initial 6 week phase 1 trial with AFO and foot drop
stimulator in terms of the gain in walking speed. After this, in the phase
2, cross over trial of 6 weeks duration was done and the orthotic effect of
AFO was found to be better than the PS though values were not
statistically significant(7). Sheffler et al too demonstrated absence of
significant difference in walking speed ‘between the two groups’.
However, the study used quantitative gait analysis for assessment of
speed instead of the 10 meters walk test, as used in our study(9).
In a within-subject study of 26 community dwellers with stroke using
AFO, the PS for 8 weeks did not show any difference in walking speed in
comparison to the AFO(28). A randomised control trial by Kottink et al
using an implantable PS indicated comparable results for 6 minutes walk
test between the two groups at 12 weeks, but showed a significant
difference at 26 weeks. For 10 meters walk test, an improvement of 10 %
was observed at the end of 26 weeks for FES group and no change in

82
control group. However, this study included a mixed ‘control’ population
wherein the patients were allowed to use an AFO, walking aid and even,
no device(29). Both the randomised control studies done by Kottnik et al
and Kluding et al have a shown a within group improvement in terms of
walking speed and other gait parameters at 30 weeks and 26 weeks.
Among the limited Indian trials, Sabut et al performed an uncontrolled
trial of FES application as an orthosis and revealed an improved walking
velocity and endurance after 12 weeks of FES based rehabilitation(23).
This ‘within group’ improvement was not demonstrated in our study.
This may be because the follow-up evaluation was a short time period of
3 weeks.
It has been observed in our rehab set-up that the patients with stroke
usually require a stipulated time of 3-4 weeks to complete gait training
with AFO with or without the walking aid once they have started
ambulating 5 meters within the parallel bar. Hence a follow up period
was kept in accordance with this protocol of finishing training within the
3 week time frame. Besides, the accommodation phase of getting
accustomed to the device was also a short period of 4 days. The previous
studies have had a follow-up of minimum 8 to 12 weeks to demonstrate a
change or improvement in either of the arms with an accommodation
time of 2 weeks or more.

83
Prior clinical studies have shown that PS has advantages over the AFO in
terms of gait pattern and other kinematic and kinetic parameters. A single
case report by van Swigchem in a chronic stroke patient with an
implantable system showed normalised knee and hip movements with
increased knee and hip flexion angles, increased movement symmetry,
increased ankle push-off and ability to avoid sudden obstacles(22).
Kottink et al randomised 23 chronic stroke patients to receive either
implantable PS or conventional treatment (AFO, no device, shoes) and
found the stance period and double limb support to be normalised for the
paretic side and single limb support normalised for the non-paretic side.
The rest of the gait parameters of stride length, step length, stride time
and walking speed did not show any significant changes ‘within the
group’ as well as ‘between the groups’(30).
Sheffler et al observed improved stride length with both AFO and the PS
group compared to no device in a case series of 12 patients. There was no
difference in other gait parameters of cadence, double limb support
within and between the groups(9). The data in our study does not show
any ‘within group’ or ‘between the group’ differences for stance
percentage, stride length and spatial asymmetry. The probable reasons for
the same have been mentioned earlier.

84
A significant finding of the study is the dynamic ankle angle change in
the PS group. The database for the normal subjects in our gait lab have
shown a mean ankle ROM of 13 ± 2 in the pre-swing phase to the mean
ROM of 5 ± 2 in the mid-swing phase making the total ankle angle
change from the pre-swing to mid-swing is noted to be 18 ± 2 degrees.
This gait phase corresponds to the application of PS device. The PS group
was able to achieve ankle angle change of 11 ± 3 degrees during this
phase of gait cycle. This finding is essential for proving the feasibility of
the PS as an orthotic device and for its immediate orthotic effect. The
above values were deduced from the video gait analysis where all the 10
participants were observed to obtain a sufficient foot lift and achieve
ground clearance preventing any foot/ toe drag.
Most of the studies have measured the ankle active and passive ROM
using a goniometer and only few kinematic and kinetic studies so far have
studied the dynamic ankle dorsiflexion in the swing phase and plantar
flexion in the stance phase. The case series by Sheffler et al did not find
any device effect on the peak dorsiflexion in swing with statistically
insignificant values for the transcutaneous PS, AFO and no device
group(9). Kottink et al noted a significant change in the minimum ankle
dorsiflexion angle achieved in the swing phase and thereby, a
significantly reduced ankle plantar flexion during swing in the PS group.

85
Hence, they concluded that implantable PS is an effective option in
providing the ankle dorsiflexion during the swing phase of gait cycle(30).
These findings are similar to those found in our study.
This study brings forth a noteworthy perspective regarding the AFO as
well. Inspite of the AFO being considered the conventional therapy mode
for stroke rehabilitation, the AFO group did not reveal any ‘within the
group’ improvement at the end of 3 weeks of training in terms of walking
speed, endurance and gait asymmetry. A quasi-experimental study of 16
hemiplegic stroke patients demonstrated that the walking speed was
unaffected by the use of AFO and there was no significant difference
‘between the control group’ with no AFO and the three arms using the
different AFOs. The study also revealed that the AFO use decreased the
plantar flexion at the initial contact and the mid swing phase(31). These
results were comparable to those obtained by S. J. Mulroy et al in a study
assessing the effect of AFO design on ambulation in 30 stroke patients.
Walking with or without AFO had a minimal impact on gait speed. On
the contrary, rigid AFO reduced the speed in some of the patients with
neutral or some ankle dorsiflexion. Irrespective of the different AFO
designs used in the study, all AFOs prevented the excess plantar flexion
during the swing phase and increased dorsiflexion at initial contact(32).
These are consistent with the findings in our study. However, there are

86
numerous studies which are at odds with these results including a recent
systemic review which showed that the AFO improved the balance and
walking in patients with stroke. Studies have also shown that step length
and stride length are also enhanced with use of AFO for the paretic limb.
However, the results in our study did not show any ‘within group’
improvements for the kinematic assessment.
A notable feature is the therapeutic affects related to PS. PS has been
found to bring about changes in the properties of stimulated muscle as
observed by alteration in the electromyographical activity. It has been
speculated that electrical stimulation enhances the cortical excitability
and facilitates neuromuscular activity(33,34). These properties are not
seen with an AFO. Nevertheless, the study did not involve investigating
the therapeutic effects of PS since the PS is still in the preliminary stages
of trial.
Additional analysis of the data suggested a significant inverse correlation
of the 6 minute walk test with the duration of the stroke within the PS
group. This implied that the PS group patients who were within 3 months
of stroke (subacute phase) had better improvement in walking endurance
than those who used the PS in the chronic phase (more than 6 months).
However, there was an unequal distribution of the patients in the PS
group for the three time durations taken (within 3 months, 3-6 months

87
and more than 6 months). As per the random allocation, the subgroup of
within 3 months duration had 6 patients, 1 patient for 3-6 months duration
and 3 patients were in more than 6 months category. This could have
possibly influenced the result. The control group had a more uniform
distribution in terms of duration with 4, 3, 3 patients in the respective
three time periods. The study by Sabut et al who compared various gait
parameters between the subacute and chronic period found that ‘within
each group’, significant improvements in walking parameters was seen.
However, no statistically significant difference was noted for ‘between
the group’ comparison(23). The authors interpreted the results as
facilitation of recovery and functional gains with early intervention with
FES in rehabilitation for stroke patients on the basis of a previous study
by K Dunning et al(24).
Another finding is the significant association between the MMSE score
and 10 meter walk test in PS group. This proved that the patients with
better cognitive ability (as determined by MMSE in our study) were able
to perform better with the device in terms of ambulation speed. This is
unsurprising because the device requires voluntary co-ordination of the
stimulation with the appropriate gait phase.
An essential aspect of the study was to the patient’s perception about the
device. This was done through a questionnaire assessing the difficulties

88
with the device and their preference for the device. Of the 10 patients, 6
did not feel any difficulty in using the device. 3 patients felt the co-
ordination of the switch with the ambulation as a difficult feature and the
remaining 1 patient found it difficult to re-learn a new walking pattern
after having been trained with the AFO. These 4 patients also felt that the
accommodation time of 4 days was too short to adjust to the device.
Overall, 5 patients preferred the device over the AFO, 3 participants
preferred the AFO and 2 patients could not decide their preference.
The feedback from the patients included several other noteworthy points.
Though there were no adverse effects of the surface stimulation seen or
any untoward events throughout the study, one patient experienced ankle
pain with stimulation throughout walking for initial 2 weeks which later
subsided spontaneously. There were two patients who were gradually
weaned off the walking aid in the therapy and hence, the switch had to be
hand held for rest of the therapy. Another patient had significant
spasticity of the dorsiflexors and hence, the stimulation was effective in
causing sufficient ankle lift only after few initial steps. Repeated training
and instructions had to be given to the patients including visual and
verbal feedback and a step-wise task analysis to teach the co-ordination
to these patients.

89
One of the patients brought forth the point that the device made walking a
conscious effort since every step had to be synchronised with stimulation.
However, this point was considered prior to the designing of the device
and it was believed that the co-ordination would be a learnt motor task as
any other learnt motor behaviour in our day to day activities and this
would improve with greater duration of training and use of the device.
Another feature was muscle fatigability experienced by one patient on
continuous use of the stimulator. A possible explanation for that could be
the presence of more of the type 2 fibres (fast fatiguing) in the ankle
dorsiflexors probably as a result of disuse atrophy. However, further
evaluation of the muscle changes and the therapeutic effects of the device
were beyond the scope of the current pilot study.
One patient had greater fear of falling with the device than with the AFO.
This could be due to the ability of the AFO to provide mediolateral
stability during the stance and also prevention of hyperextension. AFO
prevents posterior tibial rotation in relation to the foot and reduces the
large internal flexor moment generated at the hyperextended knee during
the first half of stance phase, thereby limiting the hyperextension of the
knee.
During the study, the device enabled the patients to walk bare foot or
choose a foot wear according to their convenience. This is the more

90
socially and culturally acceptable option in an Indian scenario. The study
did not explore the functional independence in terms of ADL and
advanced gait training and community use as these were beyond the
scope of this study at present.
The device had certain technical drawbacks. The stimulation used a
simple ON/OFF of 20Hz stimulation, and hence transition of movement
was abrupt. This was noted as a jerking movement of the foot with
stimulated foot lift. Also since the device was wired, there was frequent
detachment and breakage of wires, requiring re attachment, an average of
2 times per patient during the 3 week usage. The device also did not have
an indicator to show the discharging and recharging status of the battery.
Thus, the insufficient generation of ankle lift and gradual decrease in
dorsiflexion was taken as an indication for discharging of the battery.
In spite of these flaws, the novelty of the study lies in an attempt to
explore a user controlled hand switch based peroneal stimulator for
which, to our knowledge, no randomised control trials in the clinical
settings have been done. Literature mentions experiments with a similar
device designed in 1990’s by E. Ott et al(10). However, application of
this device under clinical set-up has not been mentioned. In view of the
lack of evidence, the results obtained in our study have been compared to
other studies using different sensors (either foot switches or automatic

91
sensors) and using different electrodes (either transcutaneous or
implantable). Therefore, results of the current preliminary design of PS
may not be expected to yield the same results as for the previous devices
which have undergone recurrent technical improvements.
It is notable that even with the limited training for a short duration and
time; the stimulator did not show worse results as compared to the
standard therapy of AFO in terms of its walking ability. It also had the
advantage of a more physiological form of ground clearance due to the
ankle angle change achieved. The mixed acceptability of the device
among the patients was anticipated in such a pilot study. In view of these
results, the manually controlled Peroneal Nerve Stimulator can be offered
as an alternative option for a selected group of hemiplegic population
with good cognitive abilities and in their initial phase of training,
following the acute event. The device definitely requires further
modifications in terms of the technical designing to obtain smooth
movements and also training of longer duration to prove or disprove its
efficacy.

92
7. Limitations
• Small sample size of 20 participants with 10 in each arm.
• Absence of blinding in the study.
• Non uniform distribution of patients in PS group in terms of
duration of the stroke.
• Influence of gender difference could not be detected since there
was only 1 female participant.
• Continued use of the AFO in the intervention group.
• Short duration of follow-up of 3 weeks.
• Manual calculations of the kinematic parameters from patient 7 to
patient 14 with a probable error of ± 5.
• Technical drawbacks of the device (wired device, battery charging
status, graded current generation).
• Device suitability to selected hemiplegic patients with a certain
level of cognitive ability for learning the co-ordination and
synchronization with gait cycle and cannot be used by patients with
more cognitive deficits.
• Non validated questionnaire used for patient feed-back.

93
8. Recommendations for further study
• Trial of a radiofrequency wireless hand switch for making the
device less cumbersome
• Comparison of the user based hand switch PS to an automatic PS
incorporating automatic stimulation control using accelerometers
and gyroscopes to determine the swing phase of gait.
• Trial of the PS for longer duration of therapy allowing the
intervention group patients to use the device for equivalent number
of hours as the control group using the AFO
• Trial involving longer accommodation phase with PS and longer
follow-up period (minimum 12 weeks)
• Trial with increased sample size and blinding
• Trials exploring the therapeutic effects of the PS
• Trials exploring the feasibility of PS in community and studying
the functional independence in ADL and other vocational tasks
while using the device.
• Usage of a validated questionnaire for patient’s feedback for
further studies

94
9. Conclusion
1. The study suggests some orthotic effect of a user controlled PS but
in comparison to an AFO, it was inconclusive. The assessments
were made after rehabilitation training of one hour daily for 3
weeks. The orthotic effect was measured in terms of walking
speed, endurance and kinematic gait parameters.
2. The orthotic effect of the PS when measured in terms of dynamic
ankle angle change achieved during the ambulation showed a
significant change with nearly two-third of normal angle change
during the swing phase of the gait phase.
3. The stimulator had a better orthotic effect in patients in the
subacute phase of rehabilitation as compared to those in the
chronic phase.
4. The stimulator proves a useful option for hemiplegic patients with
good cognitive abilities.
5. The stimulator received a mixed response from the patients
regarding its effectiveness as an orthosis with 50 % patients
preferring the device over the AFO and 60% claiming no difficulty
in use of the device.

95
6. The study has demonstrated a user operated hand switch PS as an
alternative to an AFO for foot drop correction, in the Indian
rehabilitation setting. This needs to be further technically
improved and its efficacy investigated on a larger scale.

Bibliography
1. Mukherjee D, Patil CG. Epidemiology and the global burden of
stroke. World Neurosurg. 2011 Dec;76(6 Suppl):S85–90.
2. Mishra NK, Khadilkar SV. Stroke program for India. Ann Indian
Acad Neurol. 2010;13(1):28–32.
3. Norrving B, Kissela B. The global burden of stroke and need for a
continuum of care. Neurology. 2013 Jan 15;80(3 Suppl 2):S5–12.
4. Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation.
Lancet. 2011 May 14; 377(9778):1693–702.
5. Walter R. Frontera, JAD. D E L I S A’ S Physical Medicine &
Rehabilitation PRINCIPLES AND PRACTICE. Fifth Edition.
LIPPINCOTT WILLIAMS & WILKINS;
6. Lyons GM, Sinkjaer T, Burridge JH, Wilcox DJ. A review of
portable FES-based neural orthoses for the correction of drop foot.
IEEE Trans Neural Syst Rehabil Eng Publ IEEE Eng Med Biol Soc.
2002 Dec;10(4):260–79.
7. Everaert DG, Stein RB, Abrams GM, Dromerick AW, Francisco
GE, Hafner BJ, et al. Effect of a foot-drop stimulator and ankle-foot
orthosis on walking performance after stroke: a multicenter
randomized controlled trial. Neurorehabil Neural Repair. 2013
Sep;27(7):579–91.

8. Kluding PM, Dunning K, O’Dell MW, Wu SS, Ginosian J, Feld J,
et al. Foot drop stimulation versus ankle foot orthosis after stroke:
30-week outcomes. Stroke J Cereb Circ. 2013 Jun;44(6):1660–9.
9. Sheffler LR, Bailey SN, Wilson RD, Chae J. Spatiotemporal,
kinematic, and kinetic effects of a peroneal nerve stimulator versus
an ankle foot orthosis in hemiparetic gait. Neurorehabil Neural
Repair. 2013 Jun;27(5):403–10.
10. Ott E, Munih M, Kralj A. Voluntary controlled peroneal stimulator.
Eng Med Biol 1999 21st Annu Conf 1999 Annu Fall Meetring
Biomed Eng Soc BMESEMBS Conf 1999 Proc First Jt. 1999. p.
661 vol.1–.
11. Microsoft Word - Stroke.doc -
bod_cerebrovasculardiseasestroke.pdf [Internet]. [cited 2013 Oct
13]. Available from:
http://www.who.int/healthinfo/statistics/bod_cerebrovasculardisease
stroke.pdf
12. Walter R. Frontera JAD. D E L I S A ’ S Physical Medicine &
Rehabilitation PRINCIPLES AND PRACTICE. Fifth.
LIPPINCOTT WILLIAMS & WILKINS;
13. Khattar B, Banerjee A, Reddi R, Dutta A. Feasibility of Functional
Electrical Stimulation-Assisted Neurorehabilitation following

Stroke in India: A Case Series. Case Reports Neurol Med.
2012;2012:830873.
14. RANDALL L. BRADDOM. Physical Medicine and Rehabilitation.
Fourth. Elsevier Saunders;
15. Jauch EC, Saver JL, Adams HP, Bruno A, Connors JJ (Buddy),
Demaerschalk BM, et al. Guidelines for the Early Management of
Patients With Acute Ischemic Stroke A Guideline for Healthcare
Professionals From the American Heart Association/American
Stroke Association. Stroke. 2013 Jan 31;STR.0b013e318284056a.
16. Cynthia C. Norkin PKLN. Joint Structure and Function: A
Comprehensive Analysis. Fourth Edition. F. A. Davis Company;
17. B.D. Chaurasia. Human Anatomy, Regional and Applied. CBS;
18. Stroke rehabilitation: Long term rehabilitation measures, NICE
guidelines [Internet]. [cited 2013 Oct 14]. Available from:
http://www.nice.org.uk/nicemedia/live/14182/64098/64098.pdf
19. Walter R. Frontera JAD. D E L I S A ’ S Physical Medicine &
Rehabilitation PRINCIPLES AND PRACTICE. Fifth.
LIPPINCOTT WILLIAMS & WILKINS;
20. 9. Mobility and the Lower Extremity [Internet]. [cited 2013 Oct 14].
Available from: http://www.ebrsr.com/uploads/Module-
9_mobility.pdf

21. Elizabeth Orton, Linda Ward. Orthotic Functional Electrical
Stimulation (FES) for “drop foot” of neurological origin. East
Midlands Specialised Commissioning Group; 2010.
22. Van Swigchem R, Weerdesteyn V, van Duijnhoven HJ, den Boer J,
Beems T, Geurts AC. Near-normal gait pattern with peroneal
electrical stimulation as a neuroprosthesis in the chronic phase of
stroke: a case report. Arch Phys Med Rehabil. 2011 Feb;92(2):320–
4.
23. Sabut SK, Sikdar C, Kumar R, Mahadevappa M. CLINICAL USE
OF FUNCTIONAL ELECTRICAL STIMULATION FOR
CORRECTION OF FOOT DROP: A COMPARISON BETWEEN
SUBACUTE AND CHRONIC STROKE PATIENTS. J Mech Med
Biol. 2011 Dec;11(05):1165–77.
24. Dunning K, Black K, Harrison A, McBride K, Israel S.
Neuroprosthesis peroneal functional electrical stimulation in the
acute inpatient rehabilitation setting: a case series. Phys Ther. 2009
May;89(5):499–506.
25. Rehab Measures - 10 Meter Walk Test [Internet]. Rehabil. Meas.
Database. [cited 2013 Oct 13]. Available from:
http://www.rehabmeasures.org/Lists/RehabMeasures/PrintView.asp
x?ID=901

26. Rehab Measures - 6 Minute Walk Test [Internet]. Rehabil. Meas.
Database. [cited 2013 Oct 13]. Available from:
http://www.rehabmeasures.org/Lists/RehabMeasures/DispForm.asp
x?ID=895
27. The CONSORT Group > CONSORT Statement > Flow Diagram
[Internet]. [cited 2013 Oct 14]. Available from: http://www.consort-
statement.org/consort-statement/flow-diagram0/
28. Van Swigchem R, Vloothuis J, den Boer J, Weerdesteyn V, Geurts
ACH. Is transcutaneous peroneal stimulation beneficial to patients
with chronic stroke using an ankle-foot orthosis? A within-subjects
study of patients’ satisfaction, walking speed and physical activity
level. J Rehabil Med Off J UEMS Eur Board Phys Rehabil Med.
2010 Feb;42(2):117–21.
29. Kottink AI, Hermens HJ, Nene AV, Tenniglo MJ, van der Aa HE,
Buschman HP, et al. A randomized controlled trial of an
implantable 2-channel peroneal nerve stimulator on walking speed
and activity in poststroke hemiplegia. Arch Phys Med Rehabil. 2007
Aug;88(8):971–8.
30. Kottink A, Tenniglo M, de Vries W, Hermens H, Buurke J. Effects
of an implantable two-channel peroneal nerve stimulator versus
conventional walking device on spatiotemporal parameters and
kinematics of hemiparetic gait. J Rehabil Med. 2012;44(1):51–7.

31. Fatone S, Gard SA, Malas BS. Effect of ankle-foot orthosis
alignment and foot-plate length on the gait of adults with poststroke
hemiplegia. Arch Phys Med Rehabil. 2009 May;90(5):810–8.
32. Mulroy SJ, Eberly VJ, Gronely JK, Weiss W, Newsam CJ. Effect of
AFO design on walking after stroke: impact of ankle plantar flexion
contracture. Prosthet Orthot Int. 2010 Sep;34(3):277–92.
33. Israel S, Kotowski S, Talbott N, Fisher K, Dunning K. The
therapeutic effect of outpatient use of a peroneal nerve functional
electrical stimulation neuroprosthesis in people with stroke: a case
series. Top Stroke Rehabil. 2011 Dec;18(6):738–45.
34. Kottink AI, Hermens HJ, Nene AV, Tenniglo MJ, Groothuis-
Oudshoorn CG, IJzerman MJ. Therapeutic Effect of an Implantable
Peroneal Nerve Stimulator in Subjects With Chronic Stroke and
Footdrop: A Randomized Controlled Trial. Phys Ther. 2008 Apr
1;88(4):437–48.

Annexure
1. Institutional Review Board Acceptance letter.
2. Patient Information Sheet and Consent Form
3. Case Sheet
4. Database for all patients

Institutional Review Board Acceptance letter


PATIENT INFORMATION SHEET
Title of the study: Effectiveness of peroneal stimulator for foot drop in
hemiplegic patients during subacute phase of rehabilitation
Principal Investigator: Dr. Kriti Mishra
Department: Physical Medicine and Rehabilitation (PMR), CMC, Vellore
There are certain diseases which affect normal walking patterns. Foot
drop is a condition where a patient is unable to clear the foot off the
ground mainly due to weakness of some ankle muscles and overactivity
of certain muscles. This is seen in patients with stroke wherein there is
also some minimal weakness of hip muscles and tightness in knee
muscles. The conventional rehabilitation method used has been AFO
along with physiotherapy. AFO is used to keep foot straight and helps in
ground clearance during walking. There is another alternative where the
patient wears a device just below the knee and this device stimulates the
nerve directly and causes muscle to contract and hence helps in lifting the
foot off ground. Since usage of this device permits ankle to be free during
rest of walking phase, it is more physiological. However, this needs co-
ordination between different components and is more user dependent
unlike the AFO. Besides, patient may also experience some unpleasant
sensations due to stimulation.

The PMR department of CMC is conducting a study to compare between
AFO and this device in stroke patients in sub acute phase, mainly in terms
of walking speed and distance patient can walk without stopping
(endurance). The stimulator being used involves a cane based switch gait
sensor making it a simpler and more adaptable device for use, the sensor
being first of its type.
The study will recruit hemiplegic patients with foot drop and suitable
physical and cognitive abilities. If you are willing to be part of study, you
will be randomly allocated into any of the two groups, first group using
device and other group receiving standard treatment of AFO.
Initially both groups will receive training in parallel bar with AFO, and
later will be randomly allocated into two groups. Each group will receive
therapy with respective mode for 3 weeks and will be assessed in terms of
walking speed, endurance, ankle ROM, other walking parameters
(cadence, step length, stride length) and also difficulties in usage and
satisfaction level. Post interventional analysis for both groups will be
done to see for statistically significant results in above parameters.
Participation in this study is not likely to cause harm to your health in any
foreseeable manner. If there is any skin changes or abnormal intolerable
sensory changes as experienced by patient, it will medically sorted out
cost being borne by the department.

All your personal information obtained by us from you will be kept
completely confidential. If you do not want to participate in this study,
you are free to say so. You can also choose to withdraw from the study at
any time without being obliged to provide an explanation. This will not
affect the treatment to be received by you in this hospital in any way.
If you need additional information, you are welcome to contact us.
Contact information is available below. Additional information on
peroneal stimulator and the assessment tests that will be used in this study
will be provided on request.
Dr. Kriti Mishra
Department of Physical Medicine and Rehabilitation
Christian Medical College,
Vellore, Tamil Nadu – 632002, INDIA
Phone: +91 –7639831201 (mobile)
E-mail: [email protected]

INFORMED CONSENT
Title of the study: Effectiveness of peroneal stimulator for foot drop in
hemiplegic patients during subacute phase of rehabilitation
Principal Investigator: Dr. Kriti Mishra
Department: Physical Medicine and Rehabilitation (PMR), CMC, Vellore
I, ________________ have been explained the details of the proposed
study to me. I have understood what has been said including the
following:
1. If I give consent to participate in this study, I may be randomly
allocated into any of the two groups, first group using peroneal
stimulator device and other group receiving standard treatment of
AFO . I am willing to take part in study irrespective of the group I
am allocated to.
2. Usage of stimulator is not likely to adversely affect my health in
any foreseeable manner.
3. I can choose not to give consent to be part of this study. I can also
choose to withdraw myself from the study at any time without
being obliged to provide an explanation. In any case, my decision
will not affect the treatment given to me in this hospital.

I am willing to give consent to be part of this study voluntarily and
without any coercion from the investigators of this project.
Signature of patient
Signature of investigator
Signature of witness
Date:

CASE SHEET
Sl. No.
Name Hospital No.:
Sex: M / F Age: Date of Onset:
Type of CVA: Haemorrhage
Ischemic : Thrombic / embolic
Vessel involved: Right / Left , MCA / ACA
Management: _____________________________________
__________________________________________________
Deficits: __________________________________________
______________________________________________________
______________________________________________________
__________________________________________
Examination:

CNS:
HMF: MMSE:
Cranial Nerves:
Motor system: Right Left
Tone : UL
LL
Voluntary Control:
Shoulder
Elbow
Wrist
Hand
Hip
Knee
Ankle

Sensory system: ____________________________________
Cortical sensation:
Reflexes:
Superficial:
Plantars:
Deep tendon reflexes: BJ TJ SJ KJ AJ
Right
Left
Cerebellar signs:___________________________________
Skull & spine:
Other systems:
CVS/RS/PA:
Musculoskeletal: _________________________________

ROM:
MMSE: Procedure Maximum
Score
Orientation
What are the day, date, month, season, and year? ___/5
Where are we? Country, state, city, hospital, floor? ____/5
Registration
Name three objects: 1 second to say each. Then ask patient to
repeat all three. Give 1 point for each correct answer. Then repeat
until all three are registered.
_____/3
Attention and calculation
Serial 7s.( one point for each correct) Stop after five answers.
Alternatively, spell world backward.
______/5
Recall
Ask for the three objects repeated above. Give 1 point for each
correct. ______/3

Language
Name a pencil and a watch. (2 points)
______/2
Repeat the following: “No ifs, ands, or buts.” (1 point)
______/1
Follow a three-stage command: “Take a piece of paper in your
right hand, fold it in half, and put it on the floor.” (3 points)
_______/3
Read and obey the following: “Close your eyes.” (1 point)
______/1
Write a sentence. (1 point)
_______/1
Copy design. (1 point)
_______/1
From: Folstein MF, Folstein S, McHugh P. “Mini-mental state”: a
practical method for grading the cognitive state of patients for the
clinician. J Psychiatr Res 1975;12:189-198.

6 min walk(meters)
Sl. No AFO Stimulator
Pre Post Post-Pre Pre Post Post-Pre
1 52 95 43 20.5 47.35 26.85 2 150.8 142 -8.8 72 85.2 13.2 3 26 59 33 70.75 66 -4.75 4 61 138 77 54.8 50 -4.8 5 27 55 28 45 46 1 6 23 32 9 66 192 126 7 70 53 -17 74 121.3 47.3 8 36.4 43 6.6 66 59 -7 9 61 95 34 62.6 38 -24.6 10 36.7 26 -10.7 64 74 10
Mean 54.39 73.8 19.41 59.56 77.88
5 18.32 SD 37.72 41.71 29.14 16.19 46.89 42.75
Within t-test 0.064 0.28 group
p-value 0.95 0.784
Inter t-test pre 0.69 t-test post 0.84
group
p-value
pre 0.503 p-value post 0.423
AFO Stim Total
Fisher Exact Test Bette
r 7 6 13 Wors
e 3 4 7 Total 10 10 20
p-
value 1

10 m walk(meters/seconds))
Sl. no AFO Stimulator
Pre Post Post-Pre Pre Post Post-Pre
1 11 22 11 5 8 3 2 30 28 -2 11 14 3 3 5 11 6 12 12 0 4 12 28 16 10 9 -1 5 5 11 6 8 7 -1 6 4 6 2 15 36 21 7 11 9 -2 13 21 8 8 3.45 7 3.55 9 9 0 9 10 16 6 11 6 -5 10 7 6.3 -0.7 9 11 2
Mean 9.845 14.43 4.585 10.3 13.3 3
SD 7.77 8.65 5.77 2.79 9.06
8 7.18
within t-test 0.033 t-test 0.27
p-value 0.97 p-value 0.79
4
Inter t-test pre 0.86 t-test post 0.78 p-value
pre 0.41 p-value post 0.45
6
AFO Stim Fisher Exact
Test Better 7 7 14 Worse 3 3 6
10 10 20 p-
value 1

Spatial Asymmetry AFO Stimulator
Pre Post Post-Pre Pre Post
Post-Pre
1 0 0 0 0 0 0 2 0 0 0 0 0 0 3 0 0 0 0 0 0 4 0 0.048 0.048 -0.85 0.65 1.5 5 -0.4 -0.46 -0.06 0.51 0.725 0.215 6 0.83 0.6 -0.23 0.19 -0.068 -0.258 7 0 0 0 0.512 0.31 -0.202 8 0 0 0 0.44 0.65 0.21 9 0 0 0 0 0 0 10 -0.2 0.725 0.925 0 0 0
Mean 0.023 0.0913 0.0683 0.0802 0.226 0.146 SD 0.313 0.336 0.310 0.395 0.326 0.49
within t-test 0.504 t-test 0.38
p-value 0.626 p-value 0.713
Inter t-test pre 0.724 t-test post 0.372
p-value pre 0.487
p-value post 0.718
AFO Stim total Fisher Exact Test Better 2 2 4
Worse 8 8 16 Total 10 10 20
p-value 1

Stride Length(meters) Sl.no AFO Stimulator
Pre Post Post-Pre Pre Post Post-Pre
1 44 64 20 77 20 -57 2 66 48 -18 68 49 -19 3 37 61 24 43 22 -21 4 32 84 52 34 43 9 5 33 57 24 61 51 -10 6 33 46 13 54 101 47 7 46 18 -28 61 93 32 8 47 38 -9 57 39 -18 9 53 44 -9 52 45 -7 10 60 53 -7 41 42 1
Mean 45.1 51.3 6.2 54.8 50.5 -4.3 SD 11.81 17.44 24.40 12.99 26.65 29.16
within t-test 0.44 t-test 0.85
p-value 0.668 p-value 0.417
Inter t-test pre 0.098 t-test post 0.94
p-value pre 0.924
p-value post 0.373
AFO Stim Total Fisher Exact Test Better 5 4 4
Worse 5 6 6 Total 10 10 10
p-value 1

Stance % Sl.no AFO Stimulator
Pre Post Post-Pre Pre Post
Post-Pre
1 93 80 -13 80 86 6 2 71 62 -9 77 79 2 3 91 95 4 76 72 -4 4 77 59 -18 72 87 15 5 74 75 1 79 77 -2 6 85 86 1 78 55 -23 7 77 82 5 85 66 -19 8 94 88 -6 77 76 -1 9 82 82 0 80 87 7 10 82 73 -9 75 80 5
Mean 82.6 78.2 -4.4 77.9 76.5 -1.4
SD 8.071 11.25 7.75 3.48 10.1
2 11.69
within t-test 0.106 t-test 0.59
6
p-value 0.917 p-value 0.56
5
Inter t-test pre 0.116 t-test post 0.72
6 p-value
pre 0.91 p-value
post 0.48
6
AFO Stim Total
Fisher Exact Test Better 5 5 5 Worse 5 5 5 Total 10 10 10
p-
value 1