Embed Size (px)
Citation preview

2011; 33: e22–e26
WEB PAPER
Effects of interprofessional education onpatient perceived quality of care
KARIN HALLIN, PETER HENRIKSSON, NILS DALEN & ANNA KIESSLING
Karolinska Institutet, Sweden
Abstract
Background: Active patient-based learning by working together at an interprofessional clinical education ward (CEW) increases
collaborative and professional competence among students.
Aim: To assess the patients’ perceptions of collaborative and communicative aspects of care when treated by interprofessional
student teams as compared to usual care.
Method: Patients treated by student teams (medical, nurse, physiotherapy and occupational therapy students) at a CEW
comprised the intervention group. Patients treated at a regular ward were taken as controls. The patients answered a questionnaire
representing collaborative and communicative aspects of care. Questionnaires from CEW (n¼ 84) and control (n¼ 62) patients
were obtained (82% vs 73% response rates).
Results: CEW patients rated a significantly higher grade of own participation in decisions regarding treatment as compared to
controls (p¼ 0.006). They did further rate a higher grade of satisfaction with information regarding need of help at home
(p¼ 0.003) and perceived that the CEW staff had taken their home situation into account at a higher grade in the preparation of
discharge (p¼ 0.0002). Finally, CEW patients felt better informed (p¼ 0.02).
Conclusion: Patients perceived a higher grade of quality of care as compared to controls with no signs of disadvantages when
treated and informed by supervised interprofessional student teams.
Introduction
The main aim of clinical education is to develop a competence
to perform high-quality health care. However, it has been
difficult to assess to what extent this mission is fulfilled.
In traditional disciplinary clinical education, the different
professions learn very little from and about one another.
However, in shared learning, students are enabled to acquire
knowledge, skills and attitudes that they would not be able to
acquire effectively in uniprofessional education (Funnell
1995). Interprofessional education (IPE) occurs when two or
more professions learn with, from and about each other in
order to improve collaboration and the quality of practice
(CAIPE 2002). IPE increases the students’ ability to look at the
task from the perspective of other professions as well as from
the perspective of their own profession (Barr 1996). Clinical
interprofessional education wards (CEWs) were established in
1998 in Sweden and in 1999 in the United Kingdom. These
clinical practice wards are platforms of clinical IPE. They
provide an opportunity to pre-qualified health care students to,
under supervision, systematically develop, e.g. collaborative
skills (Mogensen et al. 2002; Reeves & Freeth 2002; Reeves
et al. 2002; Ponzer et al. 2004; Hallin et al. 2008).
We have previously shown that active patient-based
learning by working together at a CEW was an effective
means for the students to increase their collaborative and
professional competence. All four student categories at our
CEW improved their knowledge of other professions’ work,
their own professional role and the educational period
profoundly contributed to the students’ understanding of the
importance of communication and teamwork to the quality of
patient care (Hallin et al. 2008). However, there is a paucity of
studies assessing effects at patient level when patients are
treated by supervised students (O’Malley et al. 1997). This is
true in particular as regards studies assessing the patients’
perceptions and experiences of the quality of care when
treated by interprofessional student teams.
The aim of this was to assess the patients’ perceptions of
collaborative and communicative aspects of care when treated
at a CEW as compared to usual care.
Practice points
. To evaluate outcome of medical education at patient
level is important, complicated, but possible.
. We have shown that from a patient perspective the CEW
provides increased quality of communication and col-
laboration as compared to usual care.
. We found no signs of disadvantages when patients were
treated and informed by supervised interprofessional
student teams.
. A more structured interprofessional team-based care
may be beneficial even in usual care.
Correspondence: K. Hallin, Capio Artro Clinic AB, Box 5605, SE 11486 Stockholm, Sweden. Tel: 46 701684849 or 46 709605827; fax: 46 84062691;
email: [email protected]
e22 ISSN 0142–159X print/ISSN 1466–187X online/11/010022–5 � 2011 Informa UK Ltd.
DOI: 10.3109/0142159X.2011.530314
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cam
brid
ge o
n 10
/29/
14Fo
r pe
rson
al u
se o
nly.

Methods
Patients and study design
The CEW at Danderyd University Hospital, Stockholm,
Sweden, was incorporated as a part of a regular orthopaedic
ward during the period of this study (2004–2005), where CEW
consisted of eight patient beds and the rest of the ward had 12
patient beds. The patients treated at the ward represented a
wide variety of orthopaedic diagnoses. They were admitted
both from the emergency room and for elective surgery. A
majority of the patients were elderly and presented – besides
the orthopaedic diagnosis – a wide range of other diagnoses
such as cardiovascular diseases, diabetes and malnutrition.
Patients were randomly allocated to the CEW or to the regular
part of the ward depending on patient beds available at the
moment. Only patients in need of a single room or with
dementia were excluded from care at the CEW. A staff nurse –
at the arrival to the CEW – informed all patients about the CEW
concept. They had an option to be treated by regular staff.
Very few patients used this option. The occupational therapy
supervisor was placed at CEW solely and the regular ward had
another occupational therapist at their service. The rest of the
staff had rotating schedules at the entire ward, including both
CEW and the regular ward. Due to pedagogic skills and
interest, some of the staff had their main placement at CEW.
The staff were not instructed to alter their clinical practice
when they changed between the regular part of the ward and
the CEW. During weekends and other periods, with no
students at the ward, regular staff treated all patients.
Accordingly, the ward context with facilities, personnel and
medical profile was equivalent in the two parts of the ward and
the main difference was the participation of students at the
CEW. Supervised IP pre-qualification student teams consisting
of 1–2 medical students, 3 nurse students, 1 physiotherapy
student and 1 occupational therapy student per team treated
patients at the CEW. The 2-week CEW course was mandatory
to the medical students during their eight term (out of 11) and
to the other three student categories during their last (sixth)
term. The main objectives of the students were to provide the
patients independently, but under supervision, with good
medical care, nursing care and rehabilitation activities; to
develop their own professional role; to enhance their under-
standing of the other professions and to highlight the
importance of good communication to teamwork and to
patient care. The supervisors, representing all four professions,
supported the students but kept to the background to give the
students’ all opportunities to get involved. The cooperation
and communication with patients as well as direct patient care
were thus mainly performed by the students. Further details
regarding intended learning outcomes, teaching and learning
activities of the students, etc., have been presented earlier
(Ponzer et al. 2004).
Patients at the regular part of the ward were also treated by
interprofessional teams but with qualified professional staff.
However, these teams were less structured and did not include
IP student attendance.
We assessed all patients who were treated and prepared for
discharge to their homes at the ward during the study period.
Patients discharged to another clinic or to inpatient aftercare
were excluded. Furthermore, patients in need of a single room,
usually due to serious illness or at high risk to acquire an
infection and patients suffering from dementia were excluded.
The reason was that care of such patients could not be
performed at the CEW. We excluded patients discharged from
the ward during weekends and on holidays when no students
were present. In addition, patients readmitted to the hospital
within 4 weeks after discharge were excluded.
Thus the CEW group consisted of patients treated and
prepared for discharge by supervised IPE student teams at the
CEW. The control group consisted of equivalent patients
treated by ordinary staff without participation of students.
Outcome measures
All patients included in the study were asked to fill out a
questionnaire after they had been prepared for discharge, i.e.
after all information had been given to the patients by the
students at the CEW or by the ordinary staff at the regular
ward. In order to diminish any bias, only two persons handed
out or mailed the questionnaires to the patients. Seven
questions were chosen from a valid patient satisfaction
questionnaire (Jenkinson et al. 2002) regularly used by the
hospital for quality assurance purposes. The questions con-
cerned the collaborative and communicative aspects of care –
areas were student involvement could have a positive or
negative impact. The patients had the option to fill out the
questionnaire and put it in a sealed envelope at the ward or
they could fill it out at home and use regular mail service.
Patients who did not get a questionnaire at the ward had one
sent to their homes within a week after discharge. In case of a
missing answer, one reminder was mailed within 4 weeks after
discharge. All patients had given written informed consent to
participate and were informed that the answers were to be
analysed at group level with no possibility to identify the
answers of a particular individual.
Statistical analysis
The aim of the analysis was to assess the effects of the IPE
initiative on patient perceived quality of care. The assessments
by patients at the CEW were compared to those of the control
patients treated by qualified professional staff teams (usual
care). Nonparametric and Chi-square analyses were per-
formed. The patient characteristics are given as n (%) or
n� SD. The results were considered significant at p5 0.05. All
analyses were performed with the STATISTICA Stat Soft, Inc
8.0 package.
Results
The study population consisted of 102 patients in the CEW
group, treated by the student teams and 85 patients in the
control group (usual care), treated by regular staff. A total of 35
reminders were mailed to patients in the CEW group and 26 to
the controls. A total of 84 patients filled out the questionnaire
in the CEW group and 62 patients in the control group. The
response rates were 82% and 73%, respectively. There were no
Quality of care by interprofessional learning
e23
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cam
brid
ge o
n 10
/29/
14Fo
r pe
rson
al u
se o
nly.

significant differences between the groups of responding
patients regarding gender, age, length of the hospital stay or
whether the patients were planned or acutely admitted to the
ward. There were 62% women in the CEW group versus 60%
women in the controls. The mean age was 64 years in the CEW
group versus 62 years in the control group. The length of
hospital stay was 5� 2 days in the CEW group and 5� 3 days
in the controls. In the CEW group 43% of the patients were
acutely admitted to hospital versus 58% in the controls.
Furthermore, there was no significant difference between the
groups as regards the distribution of the patients’ diagnoses.
Forty per cent of the patients in both groups were attended
due to fractures, where hip fractures dominated. Nine per cent
of the patients were admitted due to other acute orthopaedic
lesions than fractures. Thirty-four per cent of the patients were
admitted to receive elective joint replacements, with hip
replacement as the dominant procedure. Six per cent of the
patients were admitted due to other elective orthopaedic
procedures and a further 11% of the patients were tended due
to lumbar spine disorders.
Perceived quality of care
As shown in Table 1, the patients treated and prepared for
discharge by student teams rated a higher grade of participa-
tion in the decisions regarding their care as compared to
controls (p¼ 0.006). They also rated a higher grade of
satisfaction with information regarding possible home assis-
tance as compared to controls (p¼ 0.003). Furthermore, they
stated in a higher grade that the CEW staff had taken their
family and home situation into account when preparing for
discharge as compared to usual care (p¼ 0.0002). In addition,
CEW patients felt more well-informed as regards the results of
their treatment than the controls (p¼ 0.02). No unfavourable
effects or trends were noted in the CEW patients.
Reliability and validity analysis of the patientquestionnaire
The reliability of the questionnaire was good with a high
internal consistency. The Cronbach alpha-coefficient of total
satisfaction with the collaborative and communicative aspects
of care (items 1–7) was 0.73.
Discussion
We assessed the effects of this IPE intervention through the
patients’ perceptions of the collaborative and communicative
aspects of the quality of care. We found that patients with
orthopaedic disorders treated by IPE students at a CEW
perceived a higher quality of care compared to patients at a
regular orthopaedic ward. Our results are in line with O’Malley
et al. (1997). However, our study was, in contrast to theirs,
performed in a setting with acute in-patient care and with an
IPE team-based care with four professions in each team.
Interprofessional collaboration (IPC) in teams is assumed to
be beneficial because it allows a more holistic approach to
patient care than what is possible in uniprofessional care
(Funnell 1995). IPC has been defined as an activity that
involves members of more than one health- and or social-care
profession interacting together with the explicit purpose to
improve IPC (Zwarenstein et al. 2009).
IPE has, according to Barr et al. (2006), three foci: to
prepare individuals, to cultivate collaboration and to improve
services. These three foci could be seen as three cogs where
the first drives the second, which in turn drives the third.
Translated into effects of IPE, the hypothesis is that preparation
of individuals should lead to effective collaborative teamwork
resulting in beneficial changes of service and care. This
understanding has led to more and more patient centred IPE
initiatives in pre-qualification health-care education. However,
some worries regarding patient safety and quality of care have
been posed if inexperienced students are allowed to inde-
pendently take care of patients. The contention that IPE
student care at a CEW should result in unfavourable effects,
such as a reduced well-being of the patients, insufficient
information to patients or a decreased patient involvement,
could not be supported in this study. One plausible explana-
tion to our positive results could be the competent and always
present supervisors. In the CEW concept, this is a prerequisite
for IPE learning.
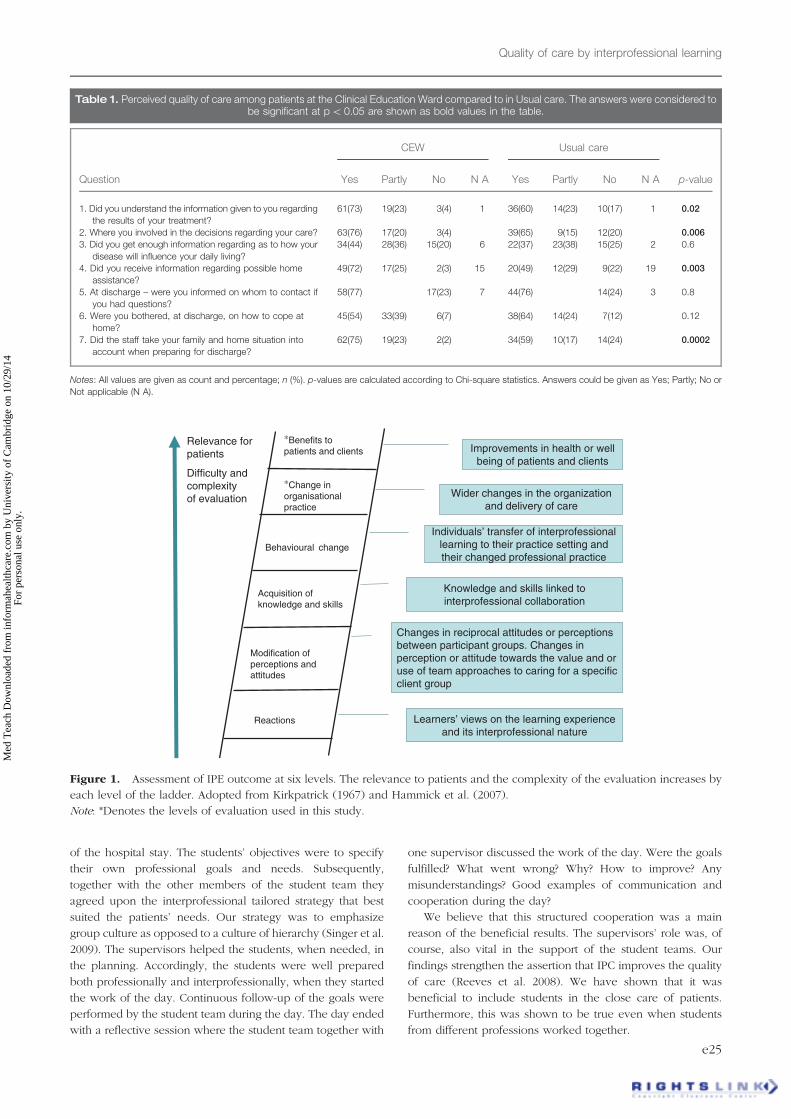
Patient outcome and quality of practice is important but
intricate fields of IPE research (Barr et al. 2006). According to
Kirkpatrick (1967), the outcome of educational interventions
could in principle be evaluated at four levels: reaction,
knowledge, behaviour/performance and result levels
(Hutchinson 1999). The relevance to patients and also the
complexity of the evaluation increases by each level. Barr et al.
(2000) have revised Kirkpatrick’s levels as regards to classifi-
cation of IPE outcomes and have added two levels (Hammick
et al. 2007). Figure 1 shows an illustration including these two
new outcome levels. The illustration is inspired from
Kirkpatrick (1967) and Hammick et al. (2007).
We assessed and found positive effects at two levels;
both concerning service delivery and patient perceived
quality of care. To our knowledge, this has not previously
been shown in prequalification IPE. A weakness of our
study is, of course, that only patient perceived quality of
care was assessed. However, patients’ perceptions concern-
ing disease and illness have been shown to be a sensitive
marker that in many instances contains prognostic informa-
tion that could not be assessed by conventional objective
markers. An indication that the CEW patients had at least the
same prognosis as the control patients was that there was
no difference in readmission rate between the two groups.
Another weakness was that it was not possible to make a
strict randomisation because patients were allocated where
there were empty beds.
One could of course speculate that patients should be
bothered by an anticipated less distinct and coherent infor-
mation by the student teams but our results did not support
such a contention. An explanation of the present results could
be that one of the intended learning outcomes of students at
CEW was to acquire skills on how to professionally inform
patients. Each working session started with a team conference
where all the students of the team and the supervisors of each
profession gathered. The students discussed each patient’s
relevant goals of the day and also the patient’s appointed goals
K. Hallin et al.
e24
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cam
brid
ge o
n 10
/29/
14Fo
r pe
rson
al u
se o
nly.
of the hospital stay. The students’ objectives were to specify
their own professional goals and needs. Subsequently,
together with the other members of the student team they
agreed upon the interprofessional tailored strategy that best
suited the patients’ needs. Our strategy was to emphasize
group culture as opposed to a culture of hierarchy (Singer et al.
2009). The supervisors helped the students, when needed, in
the planning. Accordingly, the students were well prepared
both professionally and interprofessionally, when they started
the work of the day. Continuous follow-up of the goals were
performed by the student team during the day. The day ended
with a reflective session where the student team together with
one supervisor discussed the work of the day. Were the goals
fulfilled? What went wrong? Why? How to improve? Any
misunderstandings? Good examples of communication and
cooperation during the day?
We believe that this structured cooperation was a main
reason of the beneficial results. The supervisors’ role was, of
course, also vital in the support of the student teams. Our
findings strengthen the assertion that IPC improves the quality
of care (Reeves et al. 2008). We have shown that it was
beneficial to include students in the close care of patients.
Furthermore, this was shown to be true even when students
from different professions worked together.
Reactions
Acquisition ofknowledge and skills
Behavioural change
Relevance for patients
Difficulty and complexityof evaluation
Modification ofperceptions andattitudes
*Change inorganisationalpractice
*Benefits topatients and clients Improvements in health or well
being of patients and clients
Wider changes in the organization and delivery of care
Individuals’ transfer of interprofessional learning to their practice setting and their changed professional practice
Knowledge and skills linked to interprofessional collaboration
Changes in reciprocal attitudes or perceptions between participant groups. Changes in perception or attitude towards the value and or use of team approaches to caring for a specific client group
Learners’ views on the learning experience and its interprofessional nature
Figure 1. Assessment of IPE outcome at six levels. The relevance to patients and the complexity of the evaluation increases by
each level of the ladder. Adopted from Kirkpatrick (1967) and Hammick et al. (2007).
Note: *Denotes the levels of evaluation used in this study.
Table 1. Perceived quality of care among patients at the Clinical Education Ward compared to in Usual care. The answers were considered tobe significant at p5 0.05 are shown as bold values in the table.
CEW Usual care
Question Yes Partly No N A Yes Partly No N A p-value
1. Did you understand the information given to you regarding
the results of your treatment?
61(73) 19(23) 3(4) 1 36(60) 14(23) 10(17) 1 0.02
2. Where you involved in the decisions regarding your care? 63(76) 17(20) 3(4) 39(65) 9(15) 12(20) 0.006
3. Did you get enough information regarding as to how your
disease will influence your daily living?
34(44) 28(36) 15(20) 6 22(37) 23(38) 15(25) 2 0.6
4. Did you receive information regarding possible home
assistance?
49(72) 17(25) 2(3) 15 20(49) 12(29) 9(22) 19 0.003
5. At discharge – were you informed on whom to contact if
you had questions?
58(77) 17(23) 7 44(76) 14(24) 3 0.8
6. Were you bothered, at discharge, on how to cope at
home?
45(54) 33(39) 6(7) 38(64) 14(24) 7(12) 0.12
7. Did the staff take your family and home situation into
account when preparing for discharge?
62(75) 19(23) 2(2) 34(59) 10(17) 14(24) 0.0002
Notes: All values are given as count and percentage; n (%). p-values are calculated according to Chi-square statistics. Answers could be given as Yes; Partly; No or
Not applicable (N A).
Quality of care by interprofessional learning
e25
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cam
brid
ge o
n 10
/29/
14Fo
r pe
rson
al u
se o
nly.

The patient care at the regular part of the ward was also
performed by interprofessional teams but not as structured as
at the CEW. The rounds included a nurse and an orthopaedic
surgeon and at times also a physiotherapist, an occupational
therapist and a nurse’s aid. At most times, the patient
information was shared by only two professions – usually a
nurse and one of the other professions. The regular part of the
ward had more patients to tend to and some of the patients
had more severe conditions, not appropriate to the CEW. It can
thus be argued that shortage of time made it difficult to
implement structured teamwork and communication.
However, we would suggest that the present result implies
that a more structured IPC should have been beneficial also at
a regular ward. There are several studies evaluating an
association between organizational culture, collaboration,
quality of care and patient safety (Singer et al. 2009). It is
reported that beneficial strategies in this respect are reduced
hierarchy and increased group orientation, well in accord with
our results.
Conclusion
From a patient’s point of view we found no signs of
disadvantages in terms of collaborative and communicative
aspects of care when care was performed by supervised IPE
student teams at a CEW. By contrast, we found several
indications that the patients perceived a higher grade of quality
of care when cared by the supervised IPE student teams. A
more structured interprofessional team-based care may be
beneficial even in usual care. Our findings should be
reassuring and be a further support in the future development
of CEWs.
Ethical aspects
The investigation conforms to the principles outlined in the
‘Declaration of Helsinki; 1964’. The Regional Ethical Review
Board in Stockholm, Sweden, approved the study.
Acknowledgements
We would like to thank all patients for their willingness to
share their experiences and attitudes with us. We would also
like to thank all professional staff at the CEW and at the regular
ward for their support during this study.
Funding was provided through the regional agreement on
medical education and clinical research (ALF) between
Stockholm County Council and Karolinska Institutet.
Declaration of interest: The authors report no conflicts of
interest. The authors alone are responsible for the content and
writing of this paper.
Notes on contributors
KARIN HALLIN, MD, was during the study Consultant at the Orthopaedic
clinic and Director, Clinical Education Ward at Danderyd Hospital and is at
present Orthopaedic Consultant, Capio Artro Clinic at Sophiahemmet,
Stockholm, Sweden.
PETER HENRIKSSON, MD, PhD, is a Professor and Director of studies at
Karolinska Institutet and an experienced medical educator.
NILS DALEN, MD, PhD, is a Professor and Orthopaedic surgeon and an
experienced Senior lecturer.
ANNA KIESSLING, MD. PhD, is an experienced medical educator and
Director, Centre for Clinical Education of North East Stockholm at
Karolinska Institutet.
References
Barr H. 1996. Strategies for change: End and means in interprofessional
education: Towards a typology. Educ Health 9(3):341–352.
Barr H, Freeth D, Hammick M. 2000. Evaluations of interprofessional
education: A United Kingdom review for health and social care.
London: British Educational Research Association.
Barr H, Freeth D, Hammick M, Koppel I, Reeves S. 2006. The evidence base
and recommendations for interprofessional education in health and
social care. J Interprof Care 20(1):75–8.
CAIPE. 2002. Interprofessional Education – A definition. [Accessed 3
November 2010]. Available from: http://www.caipe.org.uk/
Funnell P. 1995. Exploring the value of interprofessional learning.
In: Soothill K, Mackay L, Webb C, editors. Interprofessional relations
in health care. London: Edward Arnold. pp 163–171.
Hallin K, Kiessling A, Waldner A, Henriksson P. 2009. Active interprofes-
sional education in a patient-based setting increases perceived
collaborative and professional competence. Med Teach 31:1–7.
Hammick M, Freeth D, Koppel I, Reeves S, Barr H. 2007. A best evidence
systematic review of interprofessional education: BEME Guide no. 9.
Med Teach 29(8):735–751.
Hutchinson L. 1999. Evaluating and researching the effectiveness of
educational interventions. BMJ 318(7193):1267–1269.
Jenkinson C, Coulter A, Bruster S, Richards N, Chandola T. 2002. Patients’
experiences and satisfaction with health care: Results of a questionnaire
study of specific aspects of care. Qual Saf Health Care 11(4):335–339.
Kirkpatrick DL. 1967. Evaluation of training. In: Craig R, Bittel I, editors.
Training and development handbook. New York: McGraw-Hill.
pp 87–112.
Mogensen E, Elinder G, Widstrom AM, Winbladh B. 2002. Centres for
clinical education (CCE): Developing the health care education of
tomorrow – A preliminary report. Educ Health (Abingdon) 15(1):10–18.
O’Malley PG, Omori DM, Landry FJ, Jackson J, Kroenke K. 1997. A
prospective study to assess the effect of ambulatory teaching on patient
satisfaction. Acad Med 72(11):1015–1017.
Ponzer S, Hylin U, Kusoffsky A, Lauffs M, Lonka K, Mattiasson AC,
Nordstrom G. 2004. Interprofessional training in the context of clinical
practice: Goals and students’ perceptions on clinical education wards.
Med Educ 38(7):727–736.
Reeves S, Freeth D. 2002. The London training ward: An innovative
interprofessional learning initiative. J Interprof Care 16(1):41–52.
Reeves S, Freeth D, McCrorie P, Perry D. 2002. ‘It teaches you what to
expect in future . . .’: Interprofessional learning on a training ward for
medical, nursing, occupational therapy and physiotherapy students.
Med Educ 36(4):337–344.
Reeves S, Zwarenstein M, Goldman J, Barr H, Freeth D, Hammick M,
Koppel I. 2008. Interprofessional education: Effects on professional
practice and health care outcomes. Cochrane Database Syst Rev
23(1):CD002213.
Singer SJ, Falwell A, Gaba DM, Meterko M, Rosen A, Hartmann CW,
Baker L. 2009. Identifying organizational cultures that promote patient
safety. Health Care Manage Rev 34(4):300–311.
Zwarenstein M, Goldman J, Reeves S. 2009. Interprofessional collaboration:
Effects of practice-based interventions on professional practice and
healthcare outcomes. Cochrane Database Syst Rev Jul 8; (3):CD000072.
K. Hallin et al.
e26
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cam
brid
ge o
n 10
/29/
14Fo
r pe
rson
al u
se o
nly.





























