Embed Size (px)
Citation preview

Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Eur Neurol 2011;66:75–82 DOI: 10.1159/000329277
Effects of Medial Temporal Atrophy and White Matter Hyperintensities on the Cognitive Functions in Patients with Alzheimer’s Disease
Yong S. Shim a Young Chul Youn b Duk L. Na c Seong Yoon Kim d Hae-Kwan Cheong e So Young Moon f Kyung Won Park g Bon D. Ku h Jun-Young Lee i Jee H. Jeong j Heeyoung Kang k Eun-Joo Kim l Jung-Sun Lee d Seok Min Go m Sook Hui Kim n Kyung R. Cha o Sang Won Seo c
a Department of Neurology, Bucheon St. Mary’s Hospital, College of Medicine, Catholic University of Korea, Bucheon , b Department of Neurology, Chung-Ang University Hospital, College of Medicine, Chung-Ang University, Seoul , c Department of Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul , d Department of Psychiatry, Asan Medical Center, University of Ulsan, College of Medicine, Seoul , e Department of Social and Preventive Medicine, Sungkyunkwan University School of Medicine, Seoul , f Department ofNeurology, Ajou University School of Medicine, Suwon , g Department of Neurology, Dong-A Medical Center, Dong-A University College of Medicine, Busan , h Department of Neurology, Myongji Hospital, Kwandong University College of Medicine, Ilsan , i Department of Psychiatry, Seoul National University Boramae Hospital, Seoul , j Department of Neurology, Ewha Womans University Mokdong Hospital, Ewha Womans University School of Medicine, Seoul , k Department of Neurology, Gyeongsang National University School of Medicine, Jinju , l Department of Neurology, Pusan National University Hospital, Pusan National University School of Medicine and Medical Research Institute, Pusan , m Dr. Hwang’s Neurology Clinic, Suncheon , n Department of Neurology, Konkuk University Hospital, Konkuk University School of Medicine, Seoul , and o Department of Psychiatry, Mungyungjeil Hospital, Mungyeong , Korea
mains, and the interaction between MTA and WMH. Results: MTA independently correlated with scores of the Mini-Men-tal State Examination (MMSE), Clinical Dementia Rating scale (CDR), delayed recalls of the Seoul Verbal Learning Test (SVLT), the Boston Naming Test (BNT), and Word Fluency. WMH independently correlated with MMSE, CDR, Digit Span, and Stroop word reading, but not with delayed recall. There were interactions of WMH and MTA on CDR (p = 0.004), SVLT (p = 0.023), BNT (p = 0.002) and the semantic Word Fluency (p = 0.007). Conclusion: MTA and WMH independently af-fected cognitive deficits in AD patients, with somewhatdifferent patterns where MTA was associated mostly with memory and language, while WMH were associated withattention and frontal executive functions. This study also
Key Words
Medial temporal atrophy � White matter hyperintensities � Alzheimer’s disease
Abstract
Aims: We conducted this study to investigate the indepen-dent association of medial temporal atrophy (MTA) and white matter hyperintensities (WMH) with cognitive impair-ments of Alzheimer’s disease (AD) patients and the interac-tion between MTA and WMH. Methods: From 13 centers, a total of 216 AD patients were consecutively recruited and their MTA and WMH were visually rated. We evaluated the association of MTA and WMH with the various cognitive do-
Received: March 16, 2011 Accepted: May 9, 2011 Published online: July 22, 2011
Young Chul Youn, MD, PhD Department of Neurology Chung-Ang University Medical Center Heukseok-dong, Dongjak-gu, Seoul 156-755 (Korea) Tel. +82 2 6299 1501, E-Mail neudoc @ cau.ac.kr
© 2011 S. Karger AG, Basel0014–3022/11/0662–0075$38.00/0
Accessible online at:www.karger.com/ene

Shim et al. Eur Neurol 2011;66:75–82 76
showed interactions between MTA and WMH on some cog-nitive deficits and dementia severity, suggesting that they synergistically contribute to cognitive impairment in AD.
Copyright © 2011 S. Karger AG, Basel
Introduction
Medial temporal atrophy (MTA) is one of the early changes seen on magnetic resonance imaging (MRI) in the brains of patients with Alzheimer’s disease (AD),and its presence has proven to be a sensitive marker for the diagnosis of AD [1] . White matter hyperintensi-ties (WMH) are also commonly observed in patientswith AD, although their clinical relevance is not well de-fined [2] .
Several studies on the cognitive consequences of cere-brovascular disease (CVD)-related WMH have yielded contradictory results. Some have reported that patients with AD and WMH showed greater visuospatial dys-function and attention/concentration impairment, slow-er cognitive processing and greater executive dysfunction than those patients with AD alone [3, 4] . Other studies found no significant neuropsychological differences be-tween the two groups [5–7] . In contrast to the controver-sial cognitive correlates of WMH, atrophy measurements have shown a relatively consistent relationship with cog-nitive impairment. In individuals with cognitive impair-ment, MTA was correlated with impairments of both the verbal memory [8–10] and the general cognitive status [9] . Global brain atrophy has also been correlated with the severity of cognitive impairment [11, 12] .
Despite ample studies on cognitive impairment asso-ciated with either WMH or MTA, only a limited number of studies have evaluated the independent effects of atro-phy and WMH on cognition. In one study on AD pa-tients, gray matter volume and WMH were independent-ly correlated with global cognitive severity [13] . However, another study found no association of WMH with sever-ity of cognitive impairment or dementia, after control-ling for atrophy and demographic factors [14] . Further-more, these studies used global measures of cognitive im-pairment, without specifically examining memory or the executive function. Thus, the first goal of this study was to investigate if there is an independent effect of WMH or MTA on various cognitive deficits in AD patients.
Although pathologic studies have suggested that CVD plays a role in the neurodegenerative processes leadingto the clinical syndrome of AD [15] , there has been lit-tle clinical evidence of the relationship between WMH,
which may represent CVD, and MTA, which is known to be a marker for AD. A recent study showed an interaction between MTA and WMH in AD patients [16] , suggesting that the two factors synergistically increase the risk of AD. However, the study was not based on comprehensive neuropsychological assessments and did not look at in-teractions between WMH and MTA in various cognitive deficits of patients with AD. In contrast, another study reported that WMH may have a stronger association with global cortical atrophy than with MTA (entorhinal and hippocampal atrophy) [17] . Thus, the second goal of this study was to investigate if there is a relationship between WMH and MTA, and if there are interactive effects of WMH and MTA on various cognitive deficits in AD pa-tients.
Patients and Methods
The study participants were recruited from 13 centers for the Korean Multicenter MRI300 Study from March 2007 to April 2008. Among 292 consecutive patients, 16 patients with focal neu-rological signs, who could be diagnosed as subcortical ischemic vascular dementia, were excluded, and the 60 patients without MRI coronal image were also excluded. A total of 216 patients with AD were finally analyzed in this study. All the patients un-derwent a standardized workup involving history-taking, physi-cal and neurological examinations, blood tests (including hemo-globin, white cell count, serum electrolytes, glucose, urea, creati-nine, liver function tests, thyroid-stimulating hormone and free thyroid hormone, and vitamins B 1 , B 6 and B 12 ), the Korean version of the Mini-Mental State Examination (MMSE) [18] and the Clin-ical Dementia Rating scale (CDR) [19] . Comprehensive neuropsy-chological assessments were also performed to test for specific dysfunction in several cognitive domains. The tests consisted of the Seoul Verbal Learning Test (SVLT), which is the modified Ko-rean version of the Hopkins Verbal Learning Test [20] for ver-bal memory, the Digit Span Forward and Backward for attention and working memory, the Rey-Osterrieth Complex Figure Test (RCFT) for nonverbal, visuospatial memory, the Korean version of the Boston Naming Test (BNT) for language, the Stroop Test and the Word Fluency Test (semantic and phonemic fluency) for frontal lobe function and the RCFT copy for visuospatial function [21] . The diagnosis of probable AD was based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) [22] and the criteria of the National Institute of Neu-rological and Communicative Disorders and Stroke and the Alz-heimer’s Disease and Related Disorders Association (NINCDS-ADRDA) [23] . All the patients provided written informed consent to use their clinical data for research purposes, and this study was approved by the Institutional Review Boards of the participating hospitals.
The protocol of MRI acquisition for this study included the T 1 -weighted axial, T 2 -weighted axial, fluid-attenuated inversion recovery (FLAIR) and T 1 -weighted coronal images. On the T 1 -weighted axial, T 2 -weighted axial and FLAIR images, we evalu-

Cognitive Effects of MTA and WMH in AD
Eur Neurol 2011;66:75–82 77
ated the severity of WMH semiquantitatively according to the modified criteria of Fazekas et al. [24] or Scheltens et al. [25] . The periventricular WMH (PWMH) and the deep WMH (DWMH) were separately evaluated. The severity of DWMH was rated ac-cording to their largest diameter as the categories of D1 ( ! 10 mm), D2 ( 6 10 and ! 25 mm) and D3 ( 6 25 mm). The PWMH were rated as P1 if the cap and band were ! 5 mm, P2 if the cap or band was 6 5 and ! 10 mm, and P3 if the cap or band was 6 10 mm. Ac-cording to the combination of PWMH and DWMH ratings, as proposed by the Clinical REsearch for Dementia Of South Korea (CREDOS), the severity of WMH was classified into ‘minimal’, ‘moderate’ and ‘severe’ ( table 1 ). The MTA was rated on a 5-point scale (0–4) on a T 1 -weighted coronal image based on the width of the coronal fissure and the temporal horn and the height of the hippocampal formation [26] . We calculated the mean of the left and right MTA ratings, and then we re-classified them into MTA 1 (mean score 0, 0.5, 1), MTA 2 (mean score 1.5, 2, 2.5), and MTA 3 (mean score 3, 3.5, 4). The WMH including PWMH and DWMH were rated at the individual centers, and the MTA ratings were done by an experienced neurologist. For assessing the reliability, 138 MRI scans were randomly selected and rated by two neurolo-gists. The interrater reliabilities for the PWMH ( � = 0.595), DWMH ( � = 0.787), WMH ( � = 0.785), and MTA ( � = 0.569) were good, and the intrarater reliabilities of the WMH including PWMH and DWMH ( � = 0.874–0.979) and MTA ( � = 0.694–0.709) were also good.
Statistical analyses were performed using the SPSS software package version 13.0 (SPSS Inc., Chicago, Ill., USA). For all analy-ses, the statistical significance was accepted at p ! 0.05. First, we compared the distributions of age, years of education, gender and the results of comprehensive neuropsychological assessments, in-cluding the MMSE and CDR, among the groups according to the ratings of the WMH and MTA by using analysis of covariance (ANCOVA). The variables were adjusted for age and years ofeducation of the patients. Second, correlation analyses wereperformed with the partial correlation coefficient (r) and signifi-cance levels of p ! 0.05 to identify the association between the ratings of MTA and WMH, and to investigate the independent relations of MTA and WMH with the various cognitive domains, including the MMSE and CDR. In addition to age and years of education, variables were adjusted, respectively, for the ratings of the WMH or MTA. Next, ANCOVA was performed to investigate the interactions of MTA and WMH with the various cognitive domains.
Results
Clinical Findings according to the Ratings of WMH and MTA First, the patients were divided into three groups ac-
cording to the severity of WMH (107 with minimal WMH, 85 with moderate WMH, and 24 with severe WMH). The age of the patients significantly differed among the groups: the patients with severe WMH were older (p ! 0.001). The level of education was 5.94 8 4.67 years for the patients with minimal WMH, 5.20 8 4.92
years for the patients with moderate WNH, and 3.63 8 4.31 years for the patients with severe WMH (p = 0.089). After adjusting for age and education, the MMSE score was 19.31 8 5.48 in the patients with minimal WMH, 17.41 8 5.56 in the patients with moderate WMH, and 15.58 8 6.39 in the patients with severe WMH (p = 0.058). The CDR was 0.89 8 0.50 in the patients with minimal WMH, 0.99 8 0.52 in the patients with mod-erate WMH, and 1.31 8 0.62 in the patients with severe WMH (p = 0.028). Among the results of the neuropsy-chological assessments, there were no differences in the SVLT delayed recall scores and the RCFT delayed recall scores. The scores of the Digit Span Forward test were significantly different (p = 0.019). The Digit Span Back-ward test score was 2.53 8 1.35 in the patients with minimal WMH, 2.24 8 1.24 in the patients with mod-erate WMH, and 1.71 8 1.33 in the patients with severe WMH (p = 0.065). The differences of the semantic Word Fluency Test (p = 0.072) and the Stroop Test word read-ing (p = 0.063) also showed borderline significance ( ta-ble 2 ).
For the ratings of MTA, the patients with severe MTA had an older age (p ! 0.001). The distribution of gender was not different. As the left MTA, but not the right MTA, became severe, the years of education of the pa-tients were lower (p = 0.039). After adjusting for age and education, the MMSE score was lower (p = 0.001) and the CDR was more severe (p = 0.002) in the patients with se-vere MTA. For the neuropsychological assessments, the SVLT delayed recall (p = 0.001) and the RCFT delayed recall (p ! 0.001) were significantly different amongthe groups according to the rating of MTA. In addition,
Table 1. Rating of the WMH as proposed by CREDOS
D1(<10 mm)
D2(10–24 mm)
D3(≥25 mm)
P1 (capping/banding,both <5 mm) minimal moderate moderate
P2 (in between) minimal moderate moderateP3 (capping/banding,
either ≥10 mm) moderate moderate severe
T he periventricular hyperintensities and the deep WMH were separately evaluated and the results were combined to give a rep-resentative rating of the WMH as ‘minimal’, ‘moderate’ and ‘se-vere’.
D = Rating of the deep WMH; P = rating of the periventicular hyperintensities.

Shim et al. Eur Neurol 2011;66:75–82 78
Table 2. Demographic data of the study patients and the results of the neuropsychological assessments accord-ing to the severity of WMH
Minimal (n = 107) Moderate (n = 85) Severe (n = 24) p value
Age, years 72.0187.07 76.1686.34 76.7585.82 <0.001Gender (male:female) 33:74 28:57 3:21 0.366Education, years 5.9484.67 5.2084.92 3.6384.31 0.089MMSE 19.3185.48 17.4185.56 15.5886.39 0.058CDR 0.8980.50 0.9980.52 1.3180.62 0.028*SVLT delayed recall 1.3081.99 0.9681.75 0.7581.22 0.533RCFT delayed recall 2.8284.51 3.1085.44 2.7184.88 0.661Digit Span Forward 5.0681.55 4.6081.29 4.4281.41 0.019*Digit Span Backward 2.5381.35 2.2481.24 1.7181.33 0.065RCFT copy 18.86812.61 16.67812.39 13.25813.93 0.646BNT 28.95812.18 24.55810.45 21.7589.64 0.165Word Fluency Test semantic 17.7088.15 15.5686.72 13.0086.28 0.072Word Fluency Test phonemic 7.9788.70 6.8087.88 2.9085.19 0.292Stroop Test word reading 83.47839.47 74.53840.24 51.55845.99 0.063Stroop Test color reading 38.02824.90 31.76823.40 22.95824.56 0.264
M MSE = Mini-Mental State Examination; CDR = Clinical Dementia Rating scale; SVLT = Seoul Verbal Learning Test; RCFT = Rey-Osterrieth Complex Figure Test; BNT = Korean version of the Boston Naming Test.
Values represent the mean 8 SD. p values were calculated by analysis of covariance, and they were adjusted for age and education (* statistically significant).
Table 3. Demographic data of the study patients and the results of the neuropsychological assessments accord-ing to the ratings of MTA
MTA 1 (n = 89) MTA 2 (n = 77) MTA 3 (n = 50) p value
Age, years 71.8487.18 75.0486.42 76.9886.17 <0.001*Gender (male:female) 30:59 20:57 14:36 0.661Education, years 6.0785.07 5.2384.15 4.4284.98 0.138MMSE 19.8985.46 17.8185.41 15.5885.73 0.001*CDR 0.8280.40 1.0080.56 1.2380.62 0.002*SVLT delayed recall 1.7182.15 0.7981.63 0.5281.05 0.001*RCFT delayed recall 4.7586.40 1.7882.84 1.3682.88 <0.001*Digit Span Forward 4.8481.46 4.8481.51 4.6781.36 0.801Digit Span Backward 2.4981.31 2.2981.33 2.0681.33 0.379RCFT copy 20.12812.64 17.77812.40 11.92811.95 0.007*BNT 31.43811.94 23.6689.84 21.6189.73 <0.001*Word Fluency Test semantic 19.2687.66 14.6986.87 13.4686.56 <0.001*Word Fluency Test phonemic 9.0689.15 6.3787.22 3.6386.22 0.020*Stroop Test word reading 80.29839.95 77.23840.22 68.24846.22 0.800Stroop Test color reading 41.54825.65 30.63821.10 24.00823.60 0.008*
MMSE = Mini-Mental State Examination; CDR = Clinical Dementia Rating scale; SVLT = Seoul Verbal Learning Test; RCFT = Rey-Osterrieth Complex Figure Test; BNT = Korean version of the Boston Naming Test.
Values represent the mean 8 SD. p values were calculated by analysis of covariance and they were adjusted for age and education (* statistically significant).

Cognitive Effects of MTA and WMH in AD
Eur Neurol 2011;66:75–82 79
the BNT (p ! 0.001), the semantic (p ! 0.001) and pho-nemic (p = 0.020) Word Fluency Tests, the RCFT copy(p = 0.0073) and the Stroop Test color reading (p = 0.008) were also significantly different according to the rating of MTA ( table 3 ).
The age of the patients was correlated with WMH(r = 0.288, p ! 0.001) and MTA (r = 0.296, p ! 0.001) as well as the MMSE (r = –0.156, p = 0.011) and CDR (r = 0.243, p ! 0.001). The years of education of the patients
were also correlated with WMH (r = –0.145, p = 0.017) and MTA (r = –0.136, p = 0.023), as well as the MMSE(r = 0.527, p ! 0.011) and CDR (r = –0.210, p = 0.001).
Independent Association and the Interaction of WMH and MTA with Cognition The difference of the WMH ratings according to the
MTA ratings was significant even after adjusting for the age and years of education of the patients. The WMH rat-
0.00
0.50
1.00
1.50
2.00
MTA 1p < 0.001
MTA 2p = 0.976
MTA 3p = 0.725
CDRInteraction p = 0.004
Minimal WMHp = 0.076
Moderate WMHp = 0.013
Severe WMHp = 0.162
0.00
5.00
15.00
25.00
35.00
10.00
20.00
30.00
MTA 1p = 0.062
MTA 2p = 0.662
MTA 3p = 0.327
BNTInteraction p = 0.002
Minimal WMHp = 0.005
Moderate WMHp = 0.005
Severe WMHp = 0.401
0.00
5.00
15.00
25.00
10.00
20.00
MTA 1p = 0.054
MTA 2p = 0.817
MTA 3p = 0.474
Word fluency semanticInteraction p = 0.007
Minimal WMHp < 0.001
Moderate WMHp = 0.366
Severe WMHp = 0.919
0.00
0.50
1.00
1.50
2.00
MTA 1p = 0.401
MTA 2p = 0.887
MTA 3p = 0.264
SVLT delayed recallInteraction p = 0.023
Minimal WMHp = 0.002
Moderate WMHp = 0.165
Severe WMHp = 0.757
Colo
r ver
sion
ava
ilabl
e on
line
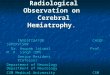
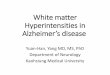
Fig. 1. Interaction of MTA and WMH on the CDR, SVLT delayed recall, BNT and semantic Word Fluency Test. For the SVLT de-layed recall, the BNT and the semantic Word Fluency Test, scores were decreased according to the MTA rating in the patients with minimal WMH. The CDR score significantly increased as the se-verity of WMH increased in patients with mild MTA (MTA 1), and the CDR significantly increased as the severity of MTA in-
creased in patients with moderate WMH. When Bonferroni cor-rection was applied, significance level for each testing was p ! 0.0083. CDR = Clinical Dementia Rating scale; SVLT = Seoul Ver-bal Learning Test; BNT = Korean version of the Boston Naming Test; MTA = medial temporal atrophy. p values were calculated by analysis of covariance and they were adjusted for age and educa-tion.

Shim et al. Eur Neurol 2011;66:75–82 80
ing was 1.42 8 0.58 for the patients with MTA 1, 1.74 8 0.71 for the patients with MTA 2, and 1.78 8 0.71 for the patients with MTA 3 (p = 0.037). Moreover, the WMH ratings correlated with the MTA ratings (r = 0.148, p = 0.015) even after adjusting for age and years of education of the patients.
For evaluating the independent cognitive relations of MTA and WMH, the MTA or WMH as well as such de-mographic variables as the age and years of education were adjusted on the partial correlation analysis. MTA independently correlated with the MMSE (r = –0.237, p ! 0.001), the CDR (r = 0.217, p ! 0.001), the BNT (r = –0.275, p ! 0.001), the RCFT copy (r = –0.196, p = 0.002), the pho-nemic (r = –0.210, p = 0.002) and semantic (r = –0.267,p ! 0.001) Word Fluency Tests, the Stroop Test color read-ing (r = –0.212, p = 0.003) and delayed recalls of the SVLT (r = –0.238, p ! 0.001) and RCFT (right: r = –0.282, p ! 0.001). WMH independently correlated with the MMSE (r = –0.129, p = 0.030), the CDR (r = 0.114, p = 0.048), the Digit Span Forward (r = –0.174, p = 0.006) and Backward (r = –0.152, p = 0.013), and Stroop Test word reading (r = –0.163, p = 0.016).
There were interactions of WMH and MTA on the CDR (p = 0.004), the SVLT delayed recalls (p = 0.023), the BNT (p = 0.002) and the semantic Word Fluency Test(p = 0.007). For the SVLT delayed recalls and semantic Word Fluency Test, those scores were decreased accord-ing to the MTA rating in the patients with minimal WMH. The score of the BNT was decreased as the MTA became severe in the patients with minimal and moder-ate WMH. The CDR became severe according to the se-verity of WMH in the patients with mild MTA (MTA 1), and became severe according to the MTA rating in the patients with moderate WMH ( fig. 1 ).
Discussion
One of the major findings of this study was that cogni-tive deficit profiles associated with MTA were somewhat different from those associated with WMH. We found that MTA correlated with memory impairment, as has been reported in previous studies [8–10] . In addition to the impairments of episodic memory, MTA was associ-ated with impairments of other cognitive functions such as language, visuospatial and frontal executive functions. On the other hand, WMH were not associated with epi-sodic memory, but with attention, working memory and parts of the frontal executive functions. In summary, MTA was more associated with memory, language, and
visuospatial function, while WMH were more associated with attention and frontal executive functions.
In addition to the domain-specific cognitive deficits, both MTA and WMH also correlated with general cogni-tive impairment as assessed by MMSE or CDR. It seems clear that MTA correlated with general cognitive impair-ment because MTA was associated with memory, lan-guage, and visuospatial functions that may contribute to general cognition. In contrast, WMH was mainly associ-ated with attention or frontal executive functions, which alone may not explain general cognitive impairment. However, the disruption of subcortical-cortical connec-tions by WMH may be detrimental to the integrity of the cortical gray matter and it may result in cognitive impair-ment [17] . Indeed, it has been demonstrated that patients with MCI or dementia associated with severe WMH have widespread cortical thinning including the frontal lobes [27] .
Another major finding of our study was that there was an association between MTA and WMH in AD pa-tients. One of the possible explanations for this link could be that the medial temporal lobe is disconnected from other cortical areas by the vascular white matter lesions in the white matter tracts that subserve the corti-cal association areas, and this leads to shrinkage of the medial temporal lobe due to wallerian degeneration [28, 29] . An alternative explanation is that amyloid deposi-tion could lead to both MTA and WMH. The predomi-nant pathology of AD even early in the course of disease is the presence of amyloid plaques [30] in medial tempo-ral areas, resulting in MTA, although MTA is also found in frontotemporal lobar degeneration such as fronto-temporal dementia and semantic dementia [31] . At the same time, amyloid angiopathy can lead to WMH, as has been indicated in the relationship between the level of plasma A � 1 to A � 42 and the presence of WMH [32] . A last finding may be that cerebral ischemia may cause not only WMH, but also MTA. Indeed, pathologic stud-ies have found microinfarcts in the medial temporal lobe of patients with AD [33] . In summary, as has been suggested in previous studies, a wide variety of neuro-pathological processes may link WMH with MTA, in-cluding incomplete infarction [34] , amyloid angiopathy [35, 36] and lipohyalinosis [37] .
Our study also demonstrated that there are even inter-actions between MTA and WMH with effects on cogni-tive deficits. Thus, our study based on a large sample is the first to demonstrate that MTA and WMH synergis-tically contribute to impairment of general cognition (CDR) as well as specific cognitive functions such as ver-

Cognitive Effects of MTA and WMH in AD
Eur Neurol 2011;66:75–82 81
bal memory (SVLT delayed recalls), confrontation (BNT) and generative naming (semantic Word Fluency). These findings are in line with previous studies [16] . Neuro-pathologic studies have suggested that the effect of the AD pathology on the cognitive decline in AD patients is amplified by vascular pathology [15] .
This study has the following limitations. First, it had no pathologic confirmation. There is the possibility that we included vascular dementia patients in the present study, although we excluded the patients with focal neu-rological signs among the patients with severe WMH. Next, we were unable to determine the impact of WMH on different regions because we only measured MTA and not the regional volume or global atrophy. A better re-search strategy might involve the association of MRI pix-el- or voxel-based measures of both the whole brain and the regional alterations, including the white and gray matter, with the neuropsychological test performance. Measurements of global cortical atrophy could have shown an association with WMH.
In conclusion, our results indicated that MTA and WMH independently cause cognitive impairments in pa-tients with AD, with MTA affecting primarily the mem-ory domain and WMH affecting attention and frontal networks. There was a correlation between MTA and WMH, suggesting that they may share common underly-ing mechanisms. Finally, MTA and WMH showed inter-actions in various cognitive domains, indicating that they synergistically contribute to cognitive impairment in AD patients.
Acknowledgements
This study was supported by a research grant of the Janssen Korea Ltd., a research fund (2007–2008) from the institute of Clinical Medical Research of Bucheon St. Mary’s Hospital and a grant of the Korea Health 21 R&D Project, Ministry of Health and Welfare, and Family Affairs, Republic of Korea (A050079).
References
1 Braak H, Braak E: Neuropathological stag-ing of Alzheimer-related changes. Acta Neu-ropathol 1991; 82: 239–259.
2 Barber R, Scheltens P, Gholkar A, Ballard C, McKeith I, Ince P, Perry R, O’Brien J: White matter lesions on magnetic resonance imag-ing in dementia with Lewy bodies, Alzhei-mer’s disease, vascular dementia, and nor-mal aging. J Neurol Neurosurg Psychiatry 1999; 67: 66–72.
3 Amar K, Bucks RS, Lewis T, Scott M, Wil-cock GK: The effect of white matter low at-tenuation on cognitive performance in de-mentia of the Alzheimer type. Age Ageing 1996; 25: 443–448.
4 Libon DJ, Bogdanoff B, Cloud BS, Skalina S, Giovannetti T, Gitlin HL, Bonavita J: Declar-ative and procedural learning, quantitative measures of the hippocampus, and subcorti-cal white alterations in Alzheimer’s disease and ischaemic vascular dementia. J Clin Exp Neuropsychol 1998; 20: 30–41.
5 DeCarli C, Grady CL, Clark CM, Katz DA, Brady DR, Murphy DG, Haxby JV, Salerno JA, Gillette JA, Gonzalez-Aviles A, Rapoport SI: Comparison of positron emission tomog-raphy, cognition, and brain volume in Alz-heimer’s disease with and without severe ab-normalities of white matter. J Neurol Neuro-surg Psychiatry 1996; 60: 158–167.
6 Doddy RS, Massman PJ, Mawad M, Nance M: Cognitive consequences of subcortical magnetic resonance imaging changes in Alz-heimer’s disease: comparison to small vessel
ischemic vascular dementia. Neuropsychia-try Neuropsychol Behav Neurol 1998; 11: 191–199.
7 Bartres-Faz D, Junque C, Clemente IC, Ser-ra-Grabulosa JM, Guardia J, Lopez-Alomar A, Sanchez-Aldeguer J, Mercader JM, Bar-gallo N, Olondo M, Moral P: MRI and ge-netic correlates of cognitive function in el-ders with memory impairment. Neurobiol Aging 2001; 22: 449–459.
8 Kohler S: Quantitative characterization of verbal learning deficits in patients with Alz-heimer’s disease. J Clin Exp Neuropsychol 1994; 16: 749–753.
9 Laakso MP, Soininen H, Partanen K, Helka-la EL, Hartikainen P, Vainio P, Hallikainen M, Hanninen T, Riekkinen PJ Sr: Volumes of hippocampus, amygdala and frontal lobes in the MRI-based diagnosis of early Alzhei-mer’s disease: correlation with memory functions. J Neural Transm Park Dis Dement Sect 1995; 9: 73–86.
10 Stout JC, Bondi MW, Jernigan TL, Archibald SL, Delis DC, Salmon DP: Regional cerebral volume loss associated with verbal learning and memory in dementia of the Alzheimer type. Neuropsychology 1999; 13: 188–197.
11 Brunetti A, Postiglione A, Tedeschi E, Ciarmiello A, Quarantelli M, Covelli EM, Milan G, Larobina M, Soricelli A, Sodano A, Alfano B: Measurement of global brain atro-phy in Alzheimer’s disease with unsuper-vised segmentation of spin-echo MRI stud-ies. J Magn Reson Imaging 2000; 11: 260–266.
12 Mungas D, Jagust WJ, Reed BR, Kramer JH, Weiner MW, Schuff N, Norman D, Mack WJ, Willis L, Chui HC: MRI predictors of cogni-tion in subcortical ischemic vascular disease and Alzheimer’s disease. Neurology 2001; 57: 2229–2235.
13 Stout JC, Jernigan TL, Archibald SL, Salmon DP: Association of dementia severity with cortical gray matter and abnormal white matter volumes in dementia of the Alzhei-mer type. Arch Neurol 1996; 53: 742–749.
14 Hirono N, Kitagaki H, Kazui H, Hashimoto M, Mori E: Impact of white matter changes on clinical manifestation of Alzheimer’s dis-ease: a quantitative study. Stroke 2000; 31: 2182–2188.
15 Snowdon DA, Greiner LH, Mortimer JA, Ri-ley KP, Greiner PA, Markesbery WR: Brain infarction and the clinical expression ofAlzheimer disease. The Nun Study. JAMA 1997; 277: 813–817.
16 Van der Flier WM, Middelkoop HA, Wever-ling-Rijnsburger AW, Admiraal-Behloul F, Spilt A, Bollen EL, Westendorp RG, van Bu-chem MA: Interaction of medial temporal lobe atrophy and white matter hyperintensi-ties in AD. Neurology 2004; 62: 1862–1864.
17 Du AT, Schuff N, Chao LL, Kornak J, Ezekiel F, Jagust WJ, Kramer JH, Reed BR, Miller BL, Norman D, Chui HC, Weiner MW: White matter lesions are associated with cortical at-rophy more than entorhinal and hippocam-pal atrophy. Neurobiol Aging 2005; 26: 553–559.

Shim et al. Eur Neurol 2011;66:75–82 82
18 Kang YW, Na DL, Hahn SH: A validity study on the Korean Mini-Mental State Examina-tion (K-MMSE) in dementia patients. J Ko-rean Neurol Assoc 1997; 15: 300–308.
19 Morris JC: The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology 1993; 43: 2412–2414.
20 Hogervorst E, Combrinck M, Lapuerta P, Rue J, Swales K, Budge M: The Hopkins Ver-nal Learning Test and screening for demen-tia. Dement Geriatr Cogn Disord 2002; 13: 13–20.
21 Kang YW, Na DL: Seoul Neuropsychological Screening Battery. Incheon, Human Brain Research & Consulting Co, 2003.
22 American Psychiatric Association (APA): Diagnostic and Statistical Manual of Mental Disorders, 4 ed. Washington, APA, 1994.
23 McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM: Clinical di-agnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Hu-man Services Task Force on Alzheimer’s Dis-ease. Neurology 1984; 34: 939–944.
24 Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA: MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am J Roentgenol 1987; 149: 351–356.
25 Scheltens P, Barkhof F, Leys D, Pruvo JP, Nauta JJ, Vermersch P, Steinling M, Valk J: A semiquantitative rating scale for the assess-ment of signal hyperintensities on magnetic resonance imaging. J Neurol Sci 1993; 114: 7–12.
26 Scheltens P, Leys D, Barkhof F, Huglo D, Weinstein HC, Vermersch P, Kuiper M, Steinling M, Wolters EC, Valk J: Atrophy of medial temporal lobes on MRI in ‘probable’ Alzheimer’s disease and normal ageing: di-agnostic value and neuropsychological cor-relates. J Neurol Neurosurg Psychiatry 1992; 55: 967–972.
27 Seo SW, Ahn J, Yoon U, Im K, Lee JM, Tae Kim S, Ahn HJ, Chin J, Jeong Y, Na DL: Cor-tical thinning in vascular mild cognitive im-pairment and vascular dementia of subcorti-cal type. J Neuroimaging 2010; 20: 37–45.
28 Masliah E, Miller A, Terry RD: The synaptic organization of the neocortex in Alzheimer’s disease. Med Hypotheses 1993; 41: 334–340.
29 Esiri MM, Pearson RC, Steele JE, Bowen DM, Powell TP: A quantitative study of the neu-rofibrillary tangles and the choline acetyl-transferase activity in the cerebral cortex and the amygdala in Alzheimer’s disease. J Neurol Neurosurg Psychiatry 1990; 53: 161–165.
30 Hardy J, Selkoe DJ: The amyloid hypothesis of Alzheimer’s disease: progress and prob-lems on the road to therapeutics. Science 2002; 297: 353–356.
31 Galton CJ, Gomez-Anson B, Antoun N, Scheltens P, Patterson K, Graves M, Sahaki-an BJ, Hodges JR: Temporal lobe rating scale: application to Alzheimer’s disease and fron-totemporal dementia. J Neurol Neurosurg Psychiatry 2001; 70: 165–173.
32 Van Dijk EJ, Prins ND, Vermeer SE, Hofman A, van Duijn CM, Koudstaal PJ, Breteler MMB: Plasma amyloid beta, apolipoprotein E, lacunar infarcts, and white matter lesions. Ann Neurol 2004; 55: 570–575.
33 Crystal HA, Dickson D, Davies P, Masur D, Grober E, Lipton RB: The relative frequency of dementia of unknown etiology increases with age and is nearly 50% in nonagenarians. Arch Neurol 2000; 57: 713–719.
34 Chui HC, Zarow C, Mack W, Ellis WG, Zheng L, Jagust WJ, Mungas D, Reed BR, Kramer JH, DeCarli CC, Weiner MW, Vin-ters HV: Cognitive impact of subcortical vas-cular and Alzheimer’s disease pathology. Ann Neurol 2006; 60: 677–687.
35 Englund E: Neuropathology of white matter changes in Alzheimer’s disease and vascular dementia. Dement Geriatr Cogn Disord 1998; 9: 6–12.
36 Scheltens P, Barkhof F, Leys D, Wolters EC, Ravid R, Kamphorst W: Histopathologic correlates of white matter changes on MRI in Alzheimer’s disease and normal aging. Neu-rology 1995; 45: 883–888.
37 Olichney JM, Hansen LA, Hofstetter CR, Grundman M, Katzman R, Thal LJ: Cerebral infarction in Alzheimer’s disease is associ-ated with severe amyloid angiopathy and hy-pertension. Arch Neurol 1995; 52: 702–708.