Embed Size (px)
Citation preview

lable at ScienceDirect
Manual Therapy 14 (2009) 679–684
Contents lists avai
Manual Therapy
journal homepage: www.elsevier .com/math
Original Article
Effects of posture on the thickness of transversus abdominis in pain-free subjects
Angelica Reeve a,*, Andrew Dilley b,c
a 19th Street Physiotherapy Clinic, Vancouver, V7M 1X5 Canadab Division of Clinical and Laboratory Investigation, Brighton and Sussex Medical School, University of Sussex, Brighton BN1 9PS, UKc Department of Physiology, University College London, Gower Street, London, UK
a r t i c l e i n f o
Article history:Received 30 April 2008Received in revised form1 February 2009Accepted 24 February 2009
Keywords:PostureTransversus abdominisSpinal stability
* Corresponding author. Tel.: þ1 604 988 5221; fax:9234 (mobile).
E-mail address: [email protected] (A. Reeve
1356-689X/$ – see front matter � 2009 Elsevier Ltd.doi:10.1016/j.math.2009.02.008
a b s t r a c t
The role of transversus abdominis (TrA) on spinal stability may be important in low back pain (LBP). Todate, there have not been any investigations into the influence of lumbo-pelvic neutral posture on TrAactivity. The present study therefore examines whether posture influences TrA thickness. A normativewithin-subjects single-group study was carried out. Twenty healthy adults were recruited and taughtfive postures: (1) supine lying; (2) erect sitting (lumbo-pelvic neutral); (3) slouched sitting; (4) erectstanding (lumbo-pelvic neutral); (5) sway-back standing. In each position, TrA thickness was measured(as an indirect measure of muscle activity) using ultrasound. In erect standing, TrA (mean TrA thickness:4.63� 1.35 mm) was significantly thicker than in sway-back standing (mean TrA thickness:3.32� 0.95 mm) (p¼ 00001). Similarly, in erect sitting TrA (mean thickness¼ 4.30 mm� 1.58 mm) wasfound to be significantly thicker than in slouched sitting (mean thickness¼ 3.46 mm� 1.13 mm)(p¼ 0002). In conclusion, lumbo-pelvic neutral postures may have a positive influence on spinal stabilitycompared to equivalent poor postures (slouched sitting and sway-back standing) through the recruit-ment of TrA. Therefore, posture may be important for rehabilitation in patients with LBP.
� 2009 Elsevier Ltd. All rights reserved.
1. Introduction
There has been much recent interest in the stability of thelumbar spine and its relation to low back pain (LBP; van Dieen et al.,2003; Hodges, 2003; Silfies et al., 2005). Transversus abdominis(TrA) has been of particular interest to many physiotherapists asa core stability muscle due to its anatomy (O’Sullivan, 2000;Hodges, 2003; Golby et al., 2006). A delayed muscular response ofTrA has been found in patients with a history of LBP (Hodges andRichardson, 1996, 1998; Ferreira et al., 2004), but it is still not clearif this delayed response is a predisposing factor to LBP or isa consequence of LBP (McGill et al., 2003; Hodges and Moseley,2003).
In a review on posture by Raine and Twomey (1994), it wasconcluded that there are still controversies and little evidencesupporting claims on the benefits of ideal posture or the suggestionthat poor posture will lead to musculoskeletal pain. However, ina more recent systematic review, Prins et al. (2008) concluded thatmusculoskeletal pain may be influenced by sitting posture inchildren and adolescents. Moreover, a correlation has been
þ1 604 984 4339, þ1 604 785
).
All rights reserved.
observed between spinal posture and LBP (O’Sullivan et al., 2006).There is also an increased risk of LBP in people who have sedentaryjobs, with symptoms increasing when sitting for long periods oftime (Pope et al., 2002). In a study by Yip et al. (2008), cervicalposture was correlated to cervical disability and pain.
The influence of lumbar stability on poor posture versus uprightposture has also been studied. It has been reported that there isa significant decrease in activity of the internal oblique (IO) andmultifidus muscles in poor sitting and standing postures (Snijderset al., 1998; O’Sullivan et al., 2002, 2007). In these studies however,the activity of TrA was not measured. The effect of sitting postureson TrA has been studied by Ainscough-Potts et al. (2006), buta lumbo-pelvic neutral spine appeared not to be controlled.
Deep needle electromyography (EMG) is an invasive techniquewhich has resulted in alternative methods of measuring muscleactivity. There is now growing evidence of real-time ultrasound asa valid tool to measure muscle thickness, with changes in thicknessshown to be correlated to changes in muscle activity at lower levelsof maximal voluntary contraction (McMeeken et al., 2004; Hodgeset al., 2003a).
The purpose of this study is to use ultrasound to examinechanges in thickness of TrA in slouched sitting and sway standing,which are commonly adopted poor standing and sitting postures(Arnold et al., 2000; O’Sullivan et al., 2006), and compare these toerect lumbo-pevic neutral standing and sitting positions.
A. Reeve, A. Dilley / Manual Therapy 14 (2009) 679–684680
2. Method
2.1. Subjects
Following ethical approval, by University College London’sCommittee on the ethics of non-NHS human research, consentwas obtained from 20 healthy subjects (10 male and 10 female)with a mean age of 29 years (range 20–51 years). Subjects wereexcluded if there was a history of abdominal surgery, a history ofLBP within the last two years, or a spinal deformity such asscoliosis. Subjects were also excluded if they were pregnant(Snijders et al., 1995).
2.2. Procedure
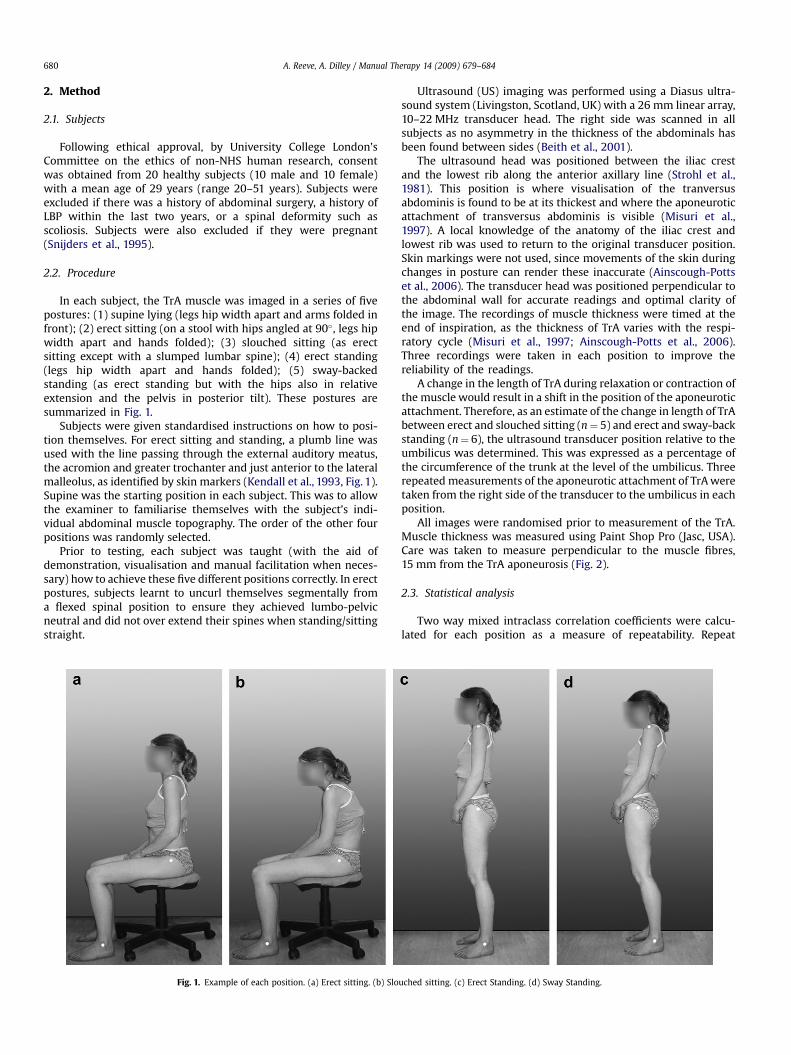
In each subject, the TrA muscle was imaged in a series of fivepostures: (1) supine lying (legs hip width apart and arms folded infront); (2) erect sitting (on a stool with hips angled at 90�, legs hipwidth apart and hands folded); (3) slouched sitting (as erectsitting except with a slumped lumbar spine); (4) erect standing(legs hip width apart and hands folded); (5) sway-backedstanding (as erect standing but with the hips also in relativeextension and the pelvis in posterior tilt). These postures aresummarized in Fig. 1.
Subjects were given standardised instructions on how to posi-tion themselves. For erect sitting and standing, a plumb line wasused with the line passing through the external auditory meatus,the acromion and greater trochanter and just anterior to the lateralmalleolus, as identified by skin markers (Kendall et al., 1993, Fig. 1).Supine was the starting position in each subject. This was to allowthe examiner to familiarise themselves with the subject’s indi-vidual abdominal muscle topography. The order of the other fourpositions was randomly selected.
Prior to testing, each subject was taught (with the aid ofdemonstration, visualisation and manual facilitation when neces-sary) how to achieve these five different positions correctly. In erectpostures, subjects learnt to uncurl themselves segmentally froma flexed spinal position to ensure they achieved lumbo-pelvicneutral and did not over extend their spines when standing/sittingstraight.
Fig. 1. Example of each position. (a) Erect sitting. (b) Slo
Ultrasound (US) imaging was performed using a Diasus ultra-sound system (Livingston, Scotland, UK) with a 26 mm linear array,10–22 MHz transducer head. The right side was scanned in allsubjects as no asymmetry in the thickness of the abdominals hasbeen found between sides (Beith et al., 2001).
The ultrasound head was positioned between the iliac crestand the lowest rib along the anterior axillary line (Strohl et al.,1981). This position is where visualisation of the tranversusabdominis is found to be at its thickest and where the aponeuroticattachment of transversus abdominis is visible (Misuri et al.,1997). A local knowledge of the anatomy of the iliac crest andlowest rib was used to return to the original transducer position.Skin markings were not used, since movements of the skin duringchanges in posture can render these inaccurate (Ainscough-Pottset al., 2006). The transducer head was positioned perpendicular tothe abdominal wall for accurate readings and optimal clarity ofthe image. The recordings of muscle thickness were timed at theend of inspiration, as the thickness of TrA varies with the respi-ratory cycle (Misuri et al., 1997; Ainscough-Potts et al., 2006).Three recordings were taken in each position to improve thereliability of the readings.
A change in the length of TrA during relaxation or contraction ofthe muscle would result in a shift in the position of the aponeuroticattachment. Therefore, as an estimate of the change in length of TrAbetween erect and slouched sitting (n¼ 5) and erect and sway-backstanding (n¼ 6), the ultrasound transducer position relative to theumbilicus was determined. This was expressed as a percentage ofthe circumference of the trunk at the level of the umbilicus. Threerepeated measurements of the aponeurotic attachment of TrA weretaken from the right side of the transducer to the umbilicus in eachposition.
All images were randomised prior to measurement of the TrA.Muscle thickness was measured using Paint Shop Pro (Jasc, USA).Care was taken to measure perpendicular to the muscle fibres,15 mm from the TrA aponeurosis (Fig. 2).
2.3. Statistical analysis
Two way mixed intraclass correlation coefficients were calcu-lated for each position as a measure of repeatability. Repeat
uched sitting. (c) Erect Standing. (d) Sway Standing.
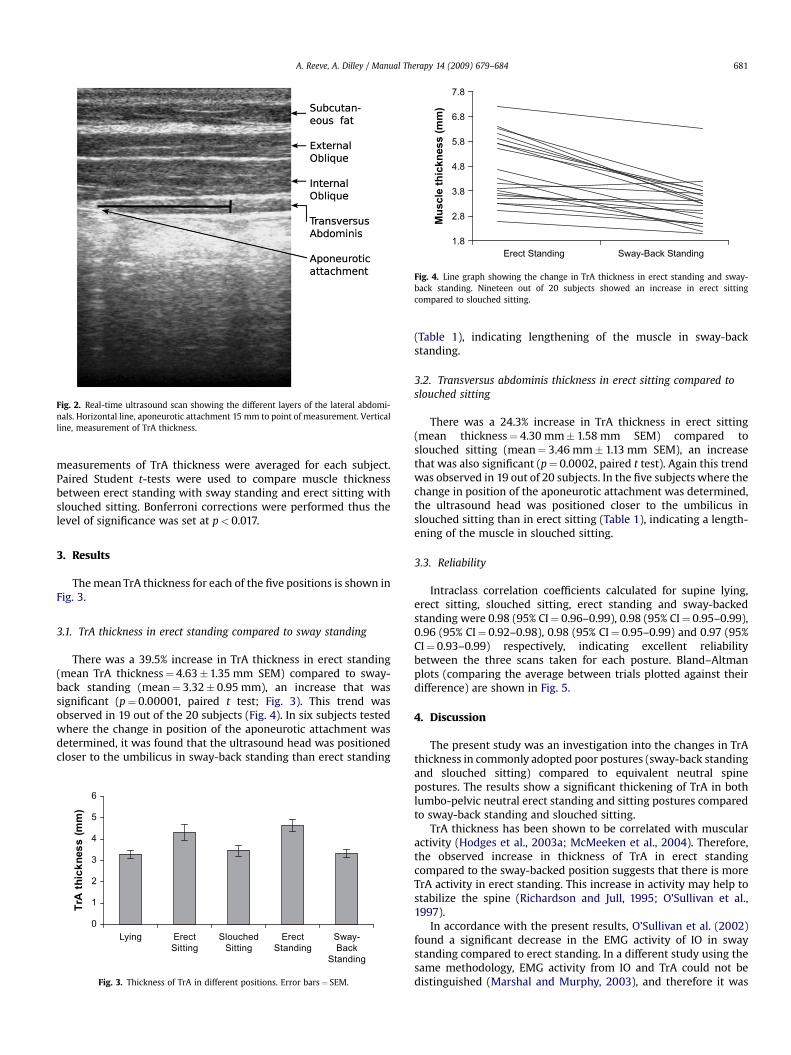
Fig. 2. Real-time ultrasound scan showing the different layers of the lateral abdomi-nals. Horizontal line, aponeurotic attachment 15 mm to point of measurement. Verticalline, measurement of TrA thickness.
Erect Standing Sway-Back Standing1.8
2.8
3.8
4.8
5.8
6.8
7.8
Mu
scle th
ickn
ess (m
m)
Fig. 4. Line graph showing the change in TrA thickness in erect standing and sway-back standing. Nineteen out of 20 subjects showed an increase in erect sittingcompared to slouched sitting.
A. Reeve, A. Dilley / Manual Therapy 14 (2009) 679–684 681
measurements of TrA thickness were averaged for each subject.Paired Student t-tests were used to compare muscle thicknessbetween erect standing with sway standing and erect sitting withslouched sitting. Bonferroni corrections were performed thus thelevel of significance was set at p< 0.017.
3. Results
The mean TrA thickness for each of the five positions is shown inFig. 3.
3.1. TrA thickness in erect standing compared to sway standing
There was a 39.5% increase in TrA thickness in erect standing(mean TrA thickness¼ 4.63�1.35 mm SEM) compared to sway-back standing (mean¼ 3.32� 0.95 mm), an increase that wassignificant (p¼ 0.00001, paired t test; Fig. 3). This trend wasobserved in 19 out of the 20 subjects (Fig. 4). In six subjects testedwhere the change in position of the aponeurotic attachment wasdetermined, it was found that the ultrasound head was positionedcloser to the umbilicus in sway-back standing than erect standing
0
1
2
3
4
5
6
Lying ErectSitting
SlouchedSitting
ErectStanding
Sway-Back
Standing
TrA
th
ic
kn
es
s (m
m)
Fig. 3. Thickness of TrA in different positions. Error bars¼ SEM.
(Table 1), indicating lengthening of the muscle in sway-backstanding.
3.2. Transversus abdominis thickness in erect sitting compared toslouched sitting
There was a 24.3% increase in TrA thickness in erect sitting(mean thickness¼ 4.30 mm� 1.58 mm SEM) compared toslouched sitting (mean¼ 3.46 mm� 1.13 mm SEM), an increasethat was also significant (p¼ 0.0002, paired t test). Again this trendwas observed in 19 out of 20 subjects. In the five subjects where thechange in position of the aponeurotic attachment was determined,the ultrasound head was positioned closer to the umbilicus inslouched sitting than in erect sitting (Table 1), indicating a length-ening of the muscle in slouched sitting.
3.3. Reliability
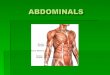
Intraclass correlation coefficients calculated for supine lying,erect sitting, slouched sitting, erect standing and sway-backedstanding were 0.98 (95% CI¼ 0.96–0.99), 0.98 (95% CI¼ 0.95–0.99),0.96 (95% CI¼ 0.92–0.98), 0.98 (95% CI¼ 0.95–0.99) and 0.97 (95%CI¼ 0.93–0.99) respectively, indicating excellent reliabilitybetween the three scans taken for each posture. Bland–Altmanplots (comparing the average between trials plotted against theirdifference) are shown in Fig. 5.
4. Discussion
The present study was an investigation into the changes in TrAthickness in commonly adopted poor postures (sway-back standingand slouched sitting) compared to equivalent neutral spinepostures. The results show a significant thickening of TrA in bothlumbo-pelvic neutral erect standing and sitting postures comparedto sway-back standing and slouched sitting.
TrA thickness has been shown to be correlated with muscularactivity (Hodges et al., 2003a; McMeeken et al., 2004). Therefore,the observed increase in thickness of TrA in erect standingcompared to the sway-backed position suggests that there is moreTrA activity in erect standing. This increase in activity may help tostabilize the spine (Richardson and Jull, 1995; O’Sullivan et al.,1997).
In accordance with the present results, O’Sullivan et al. (2002)found a significant decrease in the EMG activity of IO in swaystanding compared to erect standing. In a different study using thesame methodology, EMG activity from IO and TrA could not bedistinguished (Marshal and Murphy, 2003), and therefore it was
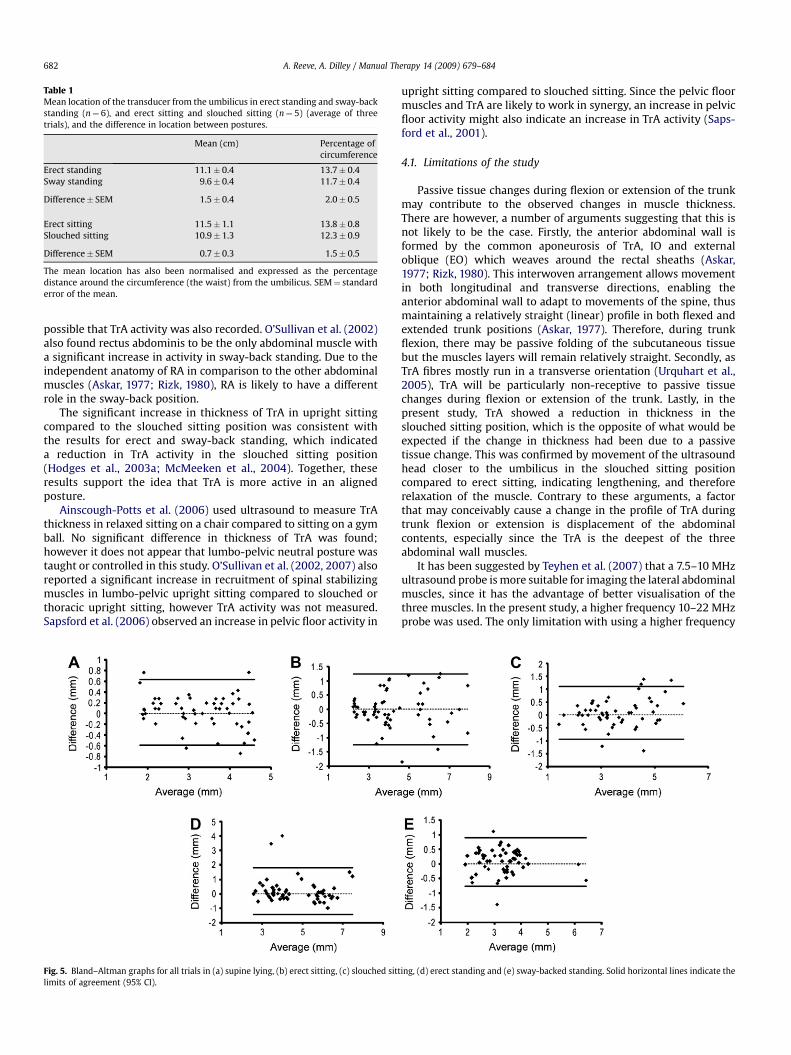
Table 1Mean location of the transducer from the umbilicus in erect standing and sway-backstanding (n¼ 6), and erect sitting and slouched sitting (n¼ 5) (average of threetrials), and the difference in location between postures.
Mean (cm) Percentage ofcircumference
Erect standing 11.1� 0.4 13.7� 0.4Sway standing 9.6� 0.4 11.7� 0.4
Difference� SEM 1.5� 0.4 2.0� 0.5
Erect sitting 11.5� 1.1 13.8� 0.8Slouched sitting 10.9� 1.3 12.3� 0.9
Difference� SEM 0.7� 0.3 1.5� 0.5
The mean location has also been normalised and expressed as the percentagedistance around the circumference (the waist) from the umbilicus. SEM¼ standarderror of the mean.
A. Reeve, A. Dilley / Manual Therapy 14 (2009) 679–684682
possible that TrA activity was also recorded. O’Sullivan et al. (2002)also found rectus abdominis to be the only abdominal muscle witha significant increase in activity in sway-back standing. Due to theindependent anatomy of RA in comparison to the other abdominalmuscles (Askar, 1977; Rizk, 1980), RA is likely to have a differentrole in the sway-back position.
The significant increase in thickness of TrA in upright sittingcompared to the slouched sitting position was consistent withthe results for erect and sway-back standing, which indicateda reduction in TrA activity in the slouched sitting position(Hodges et al., 2003a; McMeeken et al., 2004). Together, theseresults support the idea that TrA is more active in an alignedposture.
Ainscough-Potts et al. (2006) used ultrasound to measure TrAthickness in relaxed sitting on a chair compared to sitting on a gymball. No significant difference in thickness of TrA was found;however it does not appear that lumbo-pelvic neutral posture wastaught or controlled in this study. O’Sullivan et al. (2002, 2007) alsoreported a significant increase in recruitment of spinal stabilizingmuscles in lumbo-pelvic upright sitting compared to slouched orthoracic upright sitting, however TrA activity was not measured.Sapsford et al. (2006) observed an increase in pelvic floor activity in
Fig. 5. Bland–Altman graphs for all trials in (a) supine lying, (b) erect sitting, (c) slouched sittlimits of agreement (95% CI).
upright sitting compared to slouched sitting. Since the pelvic floormuscles and TrA are likely to work in synergy, an increase in pelvicfloor activity might also indicate an increase in TrA activity (Saps-ford et al., 2001).
4.1. Limitations of the study
Passive tissue changes during flexion or extension of the trunkmay contribute to the observed changes in muscle thickness.There are however, a number of arguments suggesting that this isnot likely to be the case. Firstly, the anterior abdominal wall isformed by the common aponeurosis of TrA, IO and externaloblique (EO) which weaves around the rectal sheaths (Askar,1977; Rizk, 1980). This interwoven arrangement allows movementin both longitudinal and transverse directions, enabling theanterior abdominal wall to adapt to movements of the spine, thusmaintaining a relatively straight (linear) profile in both flexed andextended trunk positions (Askar, 1977). Therefore, during trunkflexion, there may be passive folding of the subcutaneous tissuebut the muscles layers will remain relatively straight. Secondly, asTrA fibres mostly run in a transverse orientation (Urquhart et al.,2005), TrA will be particularly non-receptive to passive tissuechanges during flexion or extension of the trunk. Lastly, in thepresent study, TrA showed a reduction in thickness in theslouched sitting position, which is the opposite of what would beexpected if the change in thickness had been due to a passivetissue change. This was confirmed by movement of the ultrasoundhead closer to the umbilicus in the slouched sitting positioncompared to erect sitting, indicating lengthening, and thereforerelaxation of the muscle. Contrary to these arguments, a factorthat may conceivably cause a change in the profile of TrA duringtrunk flexion or extension is displacement of the abdominalcontents, especially since the TrA is the deepest of the threeabdominal wall muscles.
It has been suggested by Teyhen et al. (2007) that a 7.5–10 MHzultrasound probe is more suitable for imaging the lateral abdominalmuscles, since it has the advantage of better visualisation of thethree muscles. In the present study, a higher frequency 10–22 MHzprobe was used. The only limitation with using a higher frequency
ing, (d) erect standing and (e) sway-backed standing. Solid horizontal lines indicate the

A. Reeve, A. Dilley / Manual Therapy 14 (2009) 679–684 683
probe is that image quality is reduced at lower depths. However, inthis study the depth of TrA in all of the subjects was within thelimits of the probe.
Researchers have proposed a variety of different imaging loca-tions to measure the thickness of the lateral abdominals and as yet,no consensus as to the best location has been reached (Teyhen et al.,2007). In the present study the measurement of TrA thickness wastaken 15 mm from the aponeurosis. Fifteen millimetres wasconsidered suitable, since at this location the upper and lowerborders of TrA were parallel in all subjects.
Expiration has been suggested to be a more stable part of therespiratory cycle for taking images (Teyhen et al., 2007), althoughno study as yet has confirmed this. The excellent repeatabilitybetween the three individual trials in each position suggests thatthe inspiration phase of the respiratory cycle that was used in thepresent study was also sufficiently stable to produce reliableresults. Between day reliability was not tested.
4.2. Clinical implications
Since the increase in muscle thickness in neutral spine posturesduring sitting and standing most likely represents an increase inthe muscle activity in these postures, then this study supports theevidence that TrA functions as a postural muscle. The function ofTrA may help stabilize the lumbar spine by controlling inter-segmental motion either through increasing intra-abdominalpressure or its fascial attachments (Cresswell et al., 1992; Hodgesand Richardson, 1997; Hodges et al., 2003b). Patients with LBP havebeen found to have delayed activity of TrA (Hodges, 2003), withtreatment of LBP targeting the re-training of this muscle (O’Sullivanet al., 1997; Hides et al., 2001; Richardson et al., 2002; Stuge et al.,2004). The current research suggests that lumbo-pelvic neutralposture may influence the recruitment of TrA and thereforesupports the idea that posture re-education could be an importantpart of the rehabilitation process. Further research using deepneedle EMG of TrA may be justified to support the evidence foundin this study.
5. Conclusion
In both erect lumbo-pelvic neutral standing and sittingpostures there was an increase in TrA thickness compared tosway-back standing or slouched sitting, respectively. Should it beaccepted that the observed changes in thickness represent anincrease in muscular activity, these results support the evidence ofTrA as a postural muscle, possibly assisting in the provision ofstability to the spine. The present research also suggests that‘good’ posture may influence the recruitment of TrA. Therefore,posture re-education could be important in the rehabilitation ofTrA.
Acknowledgments
The assistance of Professor Bruce Lynn is most gratefullyacknowledged and also, many thanks to Dr Iain Beith for hisadvice.
References
Ainscough-Potts AM, Morrissey MC, Critchley D. The response of the transverseabdominis and internal oblique muscles to different postures. Manual Therapy2006;11(1):54–60.
Arnold CM, Beatty B, Harrison EL, Olszynski W. The reliability of five clinicalpostural alignment measures for women with osteoporosis. PhysiotherapyCanada 2000;52(4):286–94.
Askar OM. Surgical anatomy of the aponeurotic expansions of the anteriorabdominal wall. Annals of the Royal College of Surgeons of England1977;59(4):313–21.
Beith ID, Critchley DJ, Copeman E, Newman DJ. Changes in thickness of the left andright human abdominal muscles in standing and lying. Journal of PhysiologyProceedings 2001;531:147P.
Cresswell AG, Grundstrom H, Thostensson A. Observations on intra-abdominalpressure and patterns of abdominal intra muscular activity in man. ActaPhysiologica Scandinavica 1992;144:409–18.
van Dieen JH, Selen LPJ, Cholewicki J. Trunk muscle activation in low back painpatients, an analysis of the literature. Journal of Electromyography and Kine-siology 2003;13:333–51.
Ferreira PH, Ferreira ML, Hodges PW. Changes in recruitment of the abdominalmuscles in people with low back pain: ultrasound measurement of muscleactivity. Spine 2004;29:2560–6.
Golby LJ, Moore AP, Doust J, Trew MP. A randomized controlled trial investigatingthe efficiency of musculoskeletal physiotherapy on chronic low back paindisorder. Spine 2006;31(10):1083–93.
Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilizing exercisesfor first-episode low back pain. Spine 2001;26(11):E242–8.
Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbar spineassociated with back pain: a motor control evaluation of transverus abdominis.Spine 1996;21(22):2640–50.
Hodges PW, Richardson CA. Relationship between limb movement speed andassociated contraction of the trunk muscles. Ergonomics 1997;40(11):1220–30.
Hodges PW, Richardson CA. Delayed postural contraction of transversus abdominisin low back pain associated with movement of the lower limb. Journal of SpinalDisorders 1998;11(1):46–56.
Hodges P. Core stability exercise in chronic back pain. Orthopedic Clinics of NorthAmerica 2003;34:245–54.
Hodges P, Holm AK, Holm S, Ekstrom L, Cresswell A, Hansson T, et al. Intervertebralstiffness of the spine is increased by evoked contraction of the transversusabdominis and the diaphragm: in vivo porcine studies. Spine2003b;28(23):2594–601.
Hodges PW, Moseley GL. Pain and motor control of the lumbopelvic region: effectand possible mechanisms. Journal of Electromyography and Kinesiology2003;13:361–70.
Hodges PW, Pengel LHM, Herbert RD, Gandevia SC. Measurement of musclecontraction with ultrasound imaging. Muscle and Nerve 2003a;27:682–92.
Kendall FP, Kendall McCreary E, Provance PG. In: Muscle testing and function:with posture and pain. 2nd ed. Baltimore: Williams and Wilkins; 1993. pp.75–85.
Marshal P, Murphy B. The validity and reliability of surface EMG to assess theneuromuscular response of the abdominal muscles to rapid limb movement.Journal of Electromyography and Kinesiology 2003;13:477–89.
McGill SM, Grenier S, Kavcic N, Cholewicki J. Coordination of muscle activity toassure stability of the lumbar spine. Journal of Electromyography and Kinesi-ology 2003;13:353–9.
McMeeken J, Beith I, Newham D, Milligan P, Critchley D. The relationship betweenEMG and change in thickness of transversus abdominis. Clinical Biomechanics2004;19(4):337–42.
Misuri G, Colagrande S, Gorini M, Iandelli I, Mancini M, Duranti R, et al. In vivoultrasound assessment of respiratory function of abdominal muscles in normalsubjects. European Respiratory Journal 1997;10:2861–7.
O’Sullivan PB, Twomey LT, Garry T. Evaluation of specific stabilization exercise in thetreatment of chronic LBP with radiologic diagnosis of spondylolysis or spon-dylolisthesis. Spine 1997;22(24):2959–67.
O’Sullivan PB. Lumbar segmental ‘stability’: clinical presentation and specificstabilizing exercise management. Manual Therapy 2000;5(1):2–12.
O’Sullivan PB, Kirsty M, Kendell M, Lapenskie SC, Moller N, Richards K. The effect ofdifferent standing and sitting postures on trunk muscle activity in a pain-freepopulation. Spine 2002;27(11):1238–44.
O’Sullivan PB, Mitchell T, Bulich P, Waller R, Holte J. The relationship betweenposture and back muscle endurance in industrial workers with flexion-relatedlow back pain. Manual Therapy 2006;11(4):264–71.
O’Sullivan PB, Dankaerts W, Burnett A, Farrell G, Jefford E, Naylor CS, et al. The effectdifferent ‘upright’ sitting postures have on trunk muscle activation in pain-freesubjects. Physiotherapy 2007;93(S1):S96.
Pope MH, Goh KL, Magnusson ML. Spine ergonomics. Annual Review of BiomedicalEngineering 2002;4:49–68.
Prins Y, Crous L, Louw OA. A systematic review of posture and psychosocial factorsas contributors to upper quadrant musculoskeletal pain in children andadolescents. Physiotherapy Theory and Practice 2008;24(4):221–42.
Raine S, Twomey L. Attributes and qualities of human posture and their relationshipto dysfunction or musculoskeletal pain. Critical Reviews in Physical and Reha-bilitation Medicine 1994;6(4):409–37.
Richardson CA, Jull GA. Muscle control – pain control. What exercises would youprescribe? Manual Therapy 1995;1:2–10.
Richardson CA, Snijders CJ, Hides JA, Damen L, Pas MS, Storm J. The relationbetween the transversus abdominis muscles, sacroiliac joint mechanics, andlow back pain. Spine 2002;27(4):399–405.
Rizk NN. A new description of the anterior abdominal wall in man and mammals.Journal of Anatomy 1980;131(3):373–85.

A. Reeve, A. Dilley / Manual Therapy 14 (2009) 679–684684
Sapsford RR, Hodges PW, Richardson CA, Cooper DH, Markwell SJ, Jull GA. Co-activation of the abdominal and pelvic floor muscles during voluntary exercises.Neurourology Urodynamics 2001;20(1):31–42.
Sapsford RR, Richardson CA, Stanton WR. Sitting posture affects pelvic floor muscleactivity in Parous women: an observational study. Australian Journal of Phys-iotherapy 2006;52:219–22.
Silfies SP, Squillante D, Maurer P, Westcott S, Karduna AR. Trunk muscle recruitmentpatterns in specific chronic low back pain populations. Clinical Biomechanics2005;20:465–73.
Snijders CJ, Slagter AHE, van Strik R, Vlemming A, Stoeckart R, StamWhy legcrossing? HJ. The influence of common postures on abdominal muscle activity.Spine 1995;20(18):1989–93.
Snijders CJ, Vleeming A, Stoekart R, Mens JMA, Kleinrensink GJ. Biomechanicalmodelling of sacroiliac joint stability in different postures. Spine: State of theArt Reviews 1998;9:419–32.
Strohl KP, Mead J, Banzett RB, Loring SH, Kosch PC. Regional differences inabdominal muscle activity during various manoeuvres in humans. Journal ofApplied Sciences 1981;70:3044–54.
Stuge B, Veierod MB, Laerum E, Vollestad N. The efficacy of a treatment programmefocusing on specific stabilizing exercise for pelvic girdle pain after pregnancy:a two-year follow-up of a randomised clinical trial. Spine 2004;29(10):E197–203.
Teyhen DS, Gill NW, Whittaker JL, Henry SM, Hides JA, Hodges P. Rehabilitativeultrasound imaging of the abdominal muscles. Journal of Orthopaedic andSports Physical Therapy 2007;37(8):450–66.
Urquhart DM, Barker PJ, Hodges PW, Story IH, Biggs CA. Regional morphology of thetransversus abdominis and obliquus internus and externus abdominis muscles.Clinical Biomechanics 2005;20:233–41.
Yip HTY, Chui TTW, Poon ATK. The relationship between head posture and severityand disability of patients with neck pain. Manual Therapy 2008;13:148–54.

















![li Journal of Anesthesia Clinical Research - Longdom...oblique muscle and the transversus abdominis muscle [7,8]. In recent times, the transversus abdominis plane (TAP) block has been](https://img.pdfslide.net/doc/110x75/5f2868ff73bd59032d6d19c5/li-journal-of-anesthesia-clinical-research-longdom-oblique-muscle-and-the.jpg)










