Embed Size (px)
Citation preview

Effects of Pulmonary Rehabilitation on the Surv of Emphysema Patients
va I
Receivincr Lon cr -term J J
Oxygen Therapy
Summary Aims: The purpose of this study was to investigate the effect of pulmonary rehabilitation on the long-term survival rate of 1 16 elderly emphysema patients (average age 70.1 years) undergoing long-term oxygen therapy (LTOT), as well as to consider the influence on length of survival of additional factors such as LTOT starting age, nutrition (body mass index; BMI), and one-second forced expiratory volume (FEVI).
Method: The Kaplan-Meier method and the log-rank chi-square test were used to analyse the survival rate, and multiple regression analysis using Cox's proportional hazards model was employed to assess the relationship between the survival rate and a number of factors including BMI, percentage vital capacity (VC), FEVI, and i m plemen t a t ion of pu I mona ry re ha bi I i t a t i on,
Results: The survival rate for the 20 patients who received pulmonary rehabilitation was significantly higher than that of the 96 patients who did not, suggesting that pulmonary rehabilitation is effective in the care of elderly LTOT patients with emphysema. Moreover, the relative risk was found to be 4.5 times less for those who received pulmonary rehabilitation, showing its influence on the survival rate to be significant, and confirming the role of pulmonary rehabilitation as a treatment of major importance for emphysema patients.
Senjyu, H, Moji, K, Takemoto, T, Kiyama, T and Honda, S (1999).'Effects of pulmonary rehabiliLation on the survival of' emphysema patients receiving long-term oxygen therapy', Physiolhwupy, 85, 5 , 251-258.
Introduction Long-term oxygen therapy (LTOT) was first reported to be effective in the treatment of patients with chronic obstructive pulmonary disease (COPD) by the Nocturnal Oxygen Therapy Trial Group (NOTT, 1980), and by the Medical Research Council Working Party (MRCWP, 1981). These studies showed that LTOT, self-administered on an outpatient basis for 15 hours or more per day, improved survival in hypoxaemic COPD patients (Oswald-Mammosser et al, 1995). S' ince then, many studies have been published concerning factors which tend to affect survival rates, including sex, age, smoking, FEV,, arterial oxygen partial pressure (PaO,) , pulmonary hypertension and nutrition (Wilson rt al, 1989; Dubois et al, 1990; Wuertemberger et al, 1990; Skwarski P t
Key Words 251
al, 1991; Strom et al, 1993; Oswald- Mammosser et al, 1995; Gorecka et al, 1996).
The importance of pulmonary rehabilit- ation in the long-term management of COPD has also been extensively rrported (Connors and Hilling, 1993; Wijkstra et al, 1994; Lacasse et al, 1996; Hodgkin, 1997; Reina-Rosenbaum et al, 1997), showing improvements in terms of exercise tolerance, quality of life (QL) and decreased dyspnoea, as well as reduced frequency and/or costs of hospitalisation (Barandun, 199'7), and it is gradually being adopted as an accepted treatment to supplement LTOT as well as bronchodilators and o the r medications.
On the other hand, some authors have suggested that clinical evidence in favour of pulmonary rehabilitation for COPD patients is far from conclusive (Smith et al, 1992; Albert, 1997). Certainly, the effectiveness of pulmonary rehabilitation from the standpoint of survival rates has not been satisfactorily demonstrated. We believe that this is largely due to the difficulty in conducting long-term studies of effectiveness which use rigid statistical controls. Ethical considerations tend to hinder the creation of control groups (ie potentially beneficial treatment should not be withheld from patients who could be helped by its application), and a number of other problems in terms of experiment construction have been suggested (Petty, 1993).
Furthermore, existing research aimed at confirmation of the effectiveness of pulmonary rehabilitation for LTOT patients has tended to examine heterogeneous groups of subjects experiencing a diverse range of pulmonary irregularities, making it difficult to use the results. In addition, studies asserting the effectiveness of p u 1 m o n a r y re h a b i 1 i tat i o n h ave be e n conducted mainly on groups of patients in
Physiotherapy May IYYS/vol %/no 5

252
Authors and Contribution Hideaki Senjyu BS RPT, ;I pliysiothcrapixt a i i d
associatr pi-olbssor at tlir School of' Allicd Medical Scieiicrs, Nagasaki
Kazuhiko Moji PhD, an iissocixtc pi-ofrssor iit tlic lkpiirtiiiciit ol' I'ublic I l ra l th , Nagasaki [Jiiiversity Scliool of Mrdicinc, a i d Taiichiro Takemoto MD, a prol'rssor iit tlie same iiistitution, both provided coiisultativr input.
Taishou Kiyama MD, head of tlic Department of' liespiratory Disease at Killllilllloto (:lluou € iospi till, observed patients ;ind collectrd cla t a ;I t t I1 c I<rr mairio to location.
Sumihisa Honda MS, lkpai-tirielit ol' liatliation Epidemiology, Atomic Borril) Discasc Iiistitute, Nagasaki Ilnivcrsity School 01' Mrdicinc, c.onducted thr stat isticill a 1 ialys is.
Address for Correspondence MI. I Tidealti Sei!jyii, lkpartrriciit of l'hysical 'l'hci.apy, School of Allicd Medical Sciences, Nagasaki IJriiv(:rsity, 7-1 Sakainoto 1 - d i o r r i r , Nagxaki 852-8520, Japm.
their 50s and early 60s. Very little research in this area has been published concerning patients in their late 60s and 70s, although a study of patients aged .75 and older by Couser e t a1 (1995) did conclude that pulmonary rehabilitation is as beneficial for older COPD patients as for younger ones. Accordingly, there remains some doubt in the profession as to whether pulmonary rehabilitation is effective for such older patients, and there is only scant evidence available regarding the effects of pulmonary rehabilitation in conjunction with LTOT.
In Japan, largely due to a lack of pulmonary therapists and physiotherapists involved in pulmonary rehabilitation, comprehensive rehabilitation has not been generally available to LTOT patients (Senjyu and Katsuno, 1997). As of 1994, pulmonary rehabilitation programmes were available in only 20% of hospitals in Tokyo, as opposed to 56% in North America and 74% in Europe (Kida et al, 1998). This factor has allowed us to make retrospective com- parative observations of the effectiveness of rehabilitation, using a group that did not receive rehabilitation as an indicative 'historical control'.
T h e retrospective multi-centre study presented here considers the effects of pulmonary rehabilitation on a relatively homogeneous group of older LTOT patients, observed from the standpoint of survival rates, as more direct evidence of a clear relationship between pulmonary rehabilitation and survival rates is desirable to stimulate more active interest among physiotherapists and doctors, and to encourage corroborative research.
The Studv Participants A total of 116 Japanese subjects (88 men and 28 women) diagnosed with emphysema were taken from a total of 481 LTOT cases recorded at two hospitals from April 1985 to August 1996; three patients who died of o ther causes (ie traffic accidents and suicide) during this period were excluded from the results. Because emphysema patients comprise roughly one-third of all LTOT patients in Japan, and because comparison of generally similar cases is preferable in terms of the reliability of the data obtained, we limited our study to emphysema patients, and the average age of the cases available for retrospective examination was 70.1 years. All diagnoses of emphysema had been confirmed by means
of selective alveolobronchography and/or computerised tomography.
All subjects met the following criteria established in Japan for LTOT treatment (typically referred to in Japan as home oxygen therapy ( H O T ) , and typically prescribed for 24 hours a day) : W Stable condition for at least one month
following prescription of appropriate drugs. PaOp of less than 55 mm Hg when resting and on room air.
W Diagnosis of pulmonary heart disease with a PaOn of between 55 and 60mm Hg inclusive. And/or diagnosis of pulmonary hyper- tension with a mean pulmonary arterial pressure of over 20 mm Hg. And/or noticeable hypoxaemia (PaOs < 55 mm Hg during sleeping or exercise. Of the 116 subjects observed beginning at
various points from April 1985, 64 were still living at the conclusion of the 11-year study in August 1996.
Prescription of Pulmonary Rehabilitation Pulmonary rehabilitation (described below) was prescribed by the physicians attending 20 of the subjects, but was not prescribed for the remaining 96 patients. The rehabilit- ation prescribed was supervised by trained physiotherapists. The basis for decisions as to whether or not to prescribe pulmonary rehabilitation in Japan is related primarily to the availability of rehabilitation services at the institutions concerned (Senjyu and Katsuno, 1997; Kida et al, 1998). The former group received rehabilitation-linked education in addition to medication, while the latter group was treated with medication alone. The education programme for the former group included weekly classes and individualised instruction on a range of topics including pulmonary physiology, emphysema and its treatment, exercise, and the dangers associated with smoking.
Physiotherapy Service At the time this study was performed, Japanese guidelines required all LTOT candidates to undergo preliminary inpatient observation in order to confirm stability of condition and the appropriate amount of oxygen to be prescribed. Chest physio- therapy for the rehabilitation group was initiated during this inpatient treatment period lasting two to four weeks before the start of home-based LTOT, and was continued indefinitely on an outpatient basis.
Physiotherapy May 1999/vol85/no 5

Prof essiona I a r t ides 253
Walking
Orientation a t initial eva I uat ion
*-
Postu ra I 71 drainage I
+
I I
Respiratory muscle training
Relaxation 3 Positioning
Assisted breathing
;Breafhing - exercises
Purs’ed lips Diaphragmatic Supine
Self-drainage Percussion Vibration -1 Huffing Coughing I I I I
exercise
Chest mobilisation
+I Education I
Walking exercise
Treadm i I I and/or bicycle exercise
I I
For all patients * * * * - * * * * * * Based on individual needs
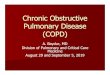
Fig 1: Chest physiotherapy programme
The physiotherapy programme (fig 1) included breathing exercises, drainage and therapeutic exercises. Inpatient physio- therapy was conducted three to four times a week in sessions of 30 to 50 minutes. Subsequent outpatient physiotherapy sessions were of the same length, but were conducted at a frequency of between twice a week and twice a month, depending on the supervising physiotherapists’ assessment of patients’ needs. Exercise was performed both in small groups (five or six people) and individually (ie the exercise programme called for both group and individual activities).
Spec i f i call y, breathing exercises were initiated with pursed lips breathing, followed by diaphragmatic breathing in the supine position, sitting, standing, walking, and in some cases stair-climbing. The muscle strengthening and endurance exercise programme consisted of walking, upper/lower extremity and respiratory muscle training exercises, and occasional use of a treadmill and/or stationary bicycle set at a low intensity, subject to individual needs. Individualised home exercise
programmes were prescribed to maintain and build on the achievements of the inpatient sessions, and were monitored through continuing outpatient sessions. All patients exercised while receiving enough supplementary oxygen to maintain arterial oxygen saturation (SaOz) of at least 90%.
Procedure and Data Analysis Information was retrieved from the subjects’ medical records concerning age at the start of LTOT, height, weight and BMI (weight in kilograms divided by the square of height in metres; kg/m‘), grade on the Medical Research Council breathlessness scale (MRC scale) (Mahler et al, 1997), percentage of predicted normal value of vital capacity (%VC), FEV,, implementation of pulmonary rehabilitation, and survival period.
The subjects were divided into two groups on the basis of whether or not they received physiotherapy - PR (pulmonary rehabilitation), and NR (non-recipients). The group averages with respect to age at starting LTOT, BMI, FEV,, and survival period were then compared using a two- sample t-test with Welch’s correction. The
Physiotherapy May 1999/vol85/no 5

survival rates of three, five, and seven years after starting LTOT are shown for the purpose of comparison with other studies. Survival rates were analysed using a log-rank chi-square test for all 116 cases, and differences were examined by comparing the subjects according to salient categorical divisions, ie implementation of pulmonary rehabilitation; sex; LTOT starting age (< 70, - 2 70); BMI (< 18, 2 18); FEV, (< 0.8 litres, - 2 0.8 litres); and their grade on the MRC scale (I1 and 111, IV and V) .
These cut-off points were selected for the following reasons: = T h e average BMI of COPD patients in
Japan is reported as 18.4 (Narita et al, 1997). The cut-off point of 0.8 litres for FEV, is in reference to a study by Strom (1993).
W There are apparent differences in the activities of daily living (ADL) between grades 111 and IV of the MRC scale. The mean age of the subjects on
starting LTOT was just over 70 years. The length of the survival period was
adopted as the standard variable, while pulmonary rehabilitation, sex, LTOT starting age, BMI, FEV,, and grade on the MRC scale were all taken as risk factors. The relationship between the survival period and each factor was assessed by multiple regression analysis using Cox’s proportional hazards model, and a t ime-dependent explanatory variable was added to the model to assess the validity of the constant proportional hazard assumption. Statistical analyses were conducted using the SAS. For all cases a significance level of 5% was adopted.
Limitations to the Study The hospital functions and the overall characteristics of the patients at the two hospitals concerned are very similar, except
for the extent of availability of respiratory rehabilitation. As is shown below, the major characteristics of the two groups at the start of LTOT did not differ significantly. Nevertheless, there may be possible confounding effects of the research design on the results, as random allocation to treatment with prospective data collection could not be applied. The small number of the subjects, especially of those who received pulmonary rehabilitation, is the other major weakness of the study, caused mainly by the limited availability of pulmonary rehabilit- ation in Japan.
Results In the NR group, 48 of the 96 subjects died; while in the PR group, four of the 20 subjects died over the course of the study, showing a significant difference (p < 0.001). The four deaths occurred at 2’7, 59, 59, and 62 months after the start of LTOT. All of the deaths were due to respiratory failure, as those who died of unrelated causes were excluded from retrospective analysis. The average survival period (SD in parentheses) after the start of LTOT was 39 (24) months for the NR group and 52 (23) months for the PR group, the latter exhibiting a significantly longer survival period a t p < 0.05 (see table 1).
As also indicated in table 1, the mean age for starting of LTOT (SD in parentheses) was 71.8 (8.5) years for the NR group and 72.7 (6.4) years for the PR group. Mean BMI was 18.9 (3.4) kg/m2 for the NR group and 19.0 (3.0) kg/m‘ for the PR group. There was no significant difference in either the age o r the BMI of the two groups. Average percentage VC was 66.6 (18.6) for the NR group and 74.6 (21.9) for the PR group, while average FEVI was 0.75 (0.31) litres for the NR group and 0.65 (0.27) litres for the PR group. Average FEVI% was 46.5
Table 1: Demographic data of non-recipients and those receiving pulmonary rehabilitation (PR)
Non-recipien ts PR recipients
Mean SD Mean SD (n = 96) (n = 20) p value
Age (years) 71 .O 8.5 72.7 6.4 ns Men (%) 79 60 BMI (kglm’) 18.9 3.4 19.0 3.0 ns FEV1 (litres) 0.75 0.31 0.65 0.27 ns Survival (months) 39 24 52 23 < 0.05
BMI =Weight in kilograms divided by the square of height in metres; kg/m’ FEVl = Forced one-second expiration volume ns = Non-significant

Professiona I articles 255
NR
........ PR
.... 60 -
...................................... 40 - I l l
I 1 1 I 1
20 -
I I I I I I I I I I 1 2 3 4 5 6 7 8 9 10
Su rviva I ti me (years)
NR = Not receiving rehabilitation. PR = Receiving pulmonary rehabilitation
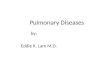
Fig 2: Comparison of survival curves in NR and PR patients
(9.5) for the NR group and 41.5 (11.0) for the PK group. Although the PR group exhibited higher %VC and the NR group higher FEV,, the differences were no t significant. With regard to MRC scale, the NR group featured 36 cases of grade I11 and 60 cases of grade IV, while the PR group was composed of five cases of grade 111, 12 cases of grade IV, and three cases of grade V.
Figure 2 indicates the survival rates of the PK and NR groups calculated by the Kaplan- Meier method (Kaplan and Meier, 1958) with clarification of censored observation. The NK group had a three-year survival rate of 7O%, a five-year survival rate of 4776, and a seven-year survival rate of 41%. The PR group, which was given respiratory rehabilitation and patient education in addition to LTOT, had a three-year survival rate of 94%, a five-year survival rate of 63%, and seven-year and ten-year survival rates of 47%. The result of the log-rank chi-square test showed that the PR survival rate was significantly higher than that of the NR group (p < 0.02).
Although slightly higher survival rates tended to be respectively associated with a LTOT starting age of under 70 years, BMI of 18 or over, FEV, of 0.8 litres or over, and grade of I1 or I11 on the MRC scale, no significant differences were identified. Neither was any significant difference observed with regard to the subjects' sex.
As shown in table 2, the implementation of pulmonary rehabilitation had by far the
strongest influence on the survival period, with a relative risk of 0.224 (p = 0.016), significantly extending the time the subjects survived. The relative risk was 0.519 ( p = 0.123) for FEV, (FEVI< 0.8 litres, FEV, 2 0.8 litres), and 1.575 (p = 0.170) for LTOT commencement age (< 70, 2 70 years).
The regression coefficient of the time- dependent explanatory variable was not significant (p = 0.16), indicating the validity of the present analysis for the constant proportional hazards assumption.
Although the survival period tended to be longer for subjects with FEV, of 0.8 litres or greater and for those under 70 years of age, the correlation was not significant. There were also no significant correlations between survival period and sex, BMI, or grade on the MRC scale.
Table 2: Relative risk estimation from regression analysis using Cox's proportional hazards model
Variable Category Relative risk p value
Age (years) 0; < 70, 1; 2 70 1.575 0.17 NR/PR 0; NR, 1; PR 0.224 0.01 6 BMI (kg/m2) 0; BMI < 18. 1; BMI 2 18 0.698 0.273 MRC 0; MRC 5 111, 1; MRC 2 IV 1.222 0.599 FEV,(litres) 0; FEVI < 0.8, 1; FEVl 2 0.8 0.519 0.123 Sex 0; Male, 1; Female 0.898 0.786
BMI =Weight in kilograms divided by square of height in metres; kg/m2 MRC = Grade on Medical Research Council breathlessness scale FEVl = Forced one-second expiration volume
Physiotherapy May 1999/vol85/no 5

256
Discussion The present study considered the efficacy of pulmonary rehabilitation for older emphysema patients receiving LTOT, specifically from the standpoint of survival rates. Our results suggest a much higher rate of survival for those who received pulmonary rehabilitation as compared with those who did not, as measured up to five years from the start of LTOT. Specifically, the relative risk was 0.224 (p = 0.016) for the PR group, or 4.5 times less than that of the NR group.
The results of roughly comparable exist- ing research are summarised in table 3. However, only a few such studies (ie considering survival rates with pulmonary rehabilitation) have been conducted, and direct comparison is made difficult by the fact that average ages a n d / o r starting respiratory function (as measured by FEV,) of patient groups differ among these few studies. Bebout et al (1983) reported the longest survival rate with pulmonary rehabilitation thus far established (86% for a five-year period and 64% for a ten-year period), but their patients were compar- atively young (average age of 59.9 years) and healthy (average FEV, of 1.53 litres). Sahn et a1 (1980) and Petty (1993) reported the shortest such survival rates (41% and 17% for five-year and ten-year periods, respectively), although the fact that the study was conducted at a rather high altitude in the city of Denver was cited as a contributing factor, and treatment was not continued as an outpatient service after release from hospital.
Our results correspond most closely with those of Burns et al (1989), who found five-year and ten-year survival rates of 58% and 38% among chronic bronchitis o r
Table 3: Summary of studies comparing survival
No of Age FEV, Cumulative survival rate (“A) Investigator patients (years) (litres) 3-year 5-year 7-year 10-year
Pulmonary rehabilitation
Hodgkin (1997) 75 59.9 1.53 86 64 Petty (1 993) 182 61 0.94 41 17 Burns e ta / (1989) 240 64.5 0.89 58 38 Our PR 20 70.1 0.65 94 63 47* 47*
Non-rehabilitation
Oswald-Marnmosser
Our NR 96 69.1 0.75 70 47 41 * e t a / (1995) 84 63 0.85 71 48 28
*No significant difference between PR and NR groups in our study
emphysema patients with a mean age of 64.5 years and FEV, of 0.89 litres.
As an example of studies examining patients not receiving pulmonary rehab- ilitation (where there is considerably more research), Oswald-Mammosser et al (1995) reported respective three-year and five-year survival rates of 71% and 48% in a study conducted on COPD patients with an average age of 63.0 years and FEV, of 0.85 litres. Corresponding figures for our NR group were 70% and 47%, even though our subjects were about six years older than those in the Oswald-Mammosser study. This may be related to the fact that our patients were specifically emphysema patients, and/or to o ther possible differences between the groups.
We found a relative risk of 0.519 (p = 0.123) for those with FEV, of at least 0.8 litres, which was 1.9 times less than that for subjects with FEV, of less than 0.8 litres, and a corresponding figure of 1.575 (p = 0.170) for subjects under 70 years at the start of LTOT, or 1.7 times less than that for subjects aged over 70. However, while a tendency to influence the length of survival can be seen, the correlations were not significant. Furthermore, no correlation was observed between the survival period and BMI, grade on the MRC scale, or sex. In contrast, the implementation of pulmonary rehabilitation did significantly influence the survival period. Also, the fact that significant differences in survival rates were not observed between the PR and NR groups for seven-year and ten-year periods is probably related to the nature of the eventual progress of emphysema.
Needless to say, there are serious limitations to the present study. Given the research design featuring non-randomised allocation of patients to pulmonary rehabilitation, as well as the smallness of the PR group and the relatively large number of censored observations, the conclusions of the study must be taken as tentative. While it would have been preferable to work with a larger number of sub.jects receiving pulmonary rehabilitation, this was simply not possible a t the time this study was conducted due to the low rate of implementation of pulmonary rehabilitation in Japan. Also, while prospective studies might provide better evidence of the benefits of pulmonary rehabilitation, retrospective studies will probably have to suffice in light of the previously mentioned ethical and design difficulties. In addition,
Physiotherapy May 1999/vol %/no 5

Prof essi ona I articles 257
existing research does not typically provide percentage figures for FEVI, making i t difficult to compare directly data on .Japanese and Western patients. The inclusion of these percentages in future reports would ease this difficulty. Although the results of the present study are mostly in accordance with the results of previous research, fur ther studies in Japan are obviously necessary.
. . . . . . Conclusion We believe that the mechanism influencing the survival rate as observed in the present study depends on the deceleration of the negative snowball effect accompanying COPD. COPD patients experience dyspnoea d 11 ring activities , there by 1 i ni i t i n g their overall activity of daily living (ADL). As activity declines, muscle power and endurance also decline, and the general condition of such patients deteriorates accordingly. This causes a negative spiral of events whereby patients tire easily, often fail to get sufficient nutrition, suffer reduced immunocompetence, and become in- creasingly susceptible to infection and/or cor pulmonale. Reduced survival rates are the predictable outcome. Pulmonary rehabilitation and associated educational programmes, however, can be seen to be effective in slowing the pace of this cycle by contributing to increased self-care ability (eg prevention of infection), reduced dyspnoea
References
Albert, R K (1997). ‘Is piilrrioiiary rrhidilitation i u i cl’li~ct i\.c t i’r:atmcnt Ior cliron ic obstriictivc piilrnonary disease? No’, Amcr~c~n,/olo.rrnl o /
cicl ( h ~ /Medicine, 155, 781-783.
Ambrosino, N, Paggiaro, P L, Macchi, M, Filieri, M, Toma, G, Lambardi, F A, Del Cesta, F, Parlanti, A, Loi, AM and Baschieri, L (19810. ‘A st i i t ly of’ stior[-icrtii (.f’kc( of rchabilitativc. t licrxpy in chronic: obstriictivr piilmonai-y tlisciwc:’, / h $ i . ~ - ~ ~ / z o ~ i , 41, I , 1-0-44.
Barandun, J (1997). ‘Value a i i d c o s t s of‘ pi l i i io i ia ry wlialil I ~ i i i i t l s c . / r c r i c , / i i r M P ~
Belbout, D E, Hodgkin, J E, Zorn, E G, Yee, A R and Sammer, E A (1983). ‘(Xni(:al and pliysiological oii(c:otncs of‘ a iiriivrrsity-hospital pl1lrrionitl-y rcliahilitation program’, 1ksl)irci~ory (;ewe, 28, I I , 146i8-73.
Belman, M J (1993). ‘Exercise in patierits with cliimiic olnt i-iiclivc pdiiioiiary disease’, ii’liorax. 48, 9, !13(i-946.
(Goldstein P t al, 1994; Ramirez et al, 199’1), increased maximum oxygen uptake and walking distance, as well as improved exercise endurance (Belman, 1993) and higher levels of ADL and QL (Reina- Rosenbaum el al, 1997), increased exercise ability (Carter PL al, 1988; Swerts et al, 1990), and reduced length of hospital stays (Hudson el al, 1976).
Although a few reports have noted improvements in FEVl over time in COPD patients (Ambrosino el al, 1981), it is generally felt that such improvement cannot be expected in the great majority of cases (Connors and Hilling 1993), ie that decline is associated with the normal pattern of ageing in general and with the progress of COPD in particular. Thus, the standard by which the efficacy of pulmonary therapy should be judged is not improvement in prognostic indicators, but rather improve- ment as measured in more general terms such as ADL and QL, and ultimately in terms of survival rates. Although o u r experimental group is small in comparison to ou r ‘historical control’ , ou r results unmistakably point towards the effectiveness of pulmonary rehabilitation in the care of elderly LTOT patients with emphysema. As pulmonary rehabilitation in Japan becomes more widespread, we will be able to assemble more balanced groups for continued study.
Burns, M R, Sherman, B, and Madison, R (1989). ‘l’ulnionary rehabilitation ourc:orne’, Rapirulory
Carter, R, Nicotra, B, Clark, L, Zinkgraf, S, Williams, J, Peavler, M, Fields, S and Berry, J (1988). ‘Excrcise conditioning in thc rchahilitation 0 1 patients with chronic pulrrionary disease’, Archim ojI-’hy.sical Medicin,(: and I~PheLhililalion., 69, 2, 1 18-122.
Connors, G and Hilling, L (eds) (1993). (;uid(4i)i(~,F ,/i)r I’ul~rnonr~ry lihabililnlion I’ro,grurns, American Association of (:;rrdiovascular and Pulmonary Kehabilitation, Tokyo.
Cower, J I, Guthmann, R, Hamadeh, M A and Kane, C S (1995). ‘Pirlrrioriary rekiabilitation
capacity in older elderly patients with COPD’, C ~ L , 107, 3, 730-734.
Dubois, P, Machiels, J, Smeets, F, Delwiche J P and Lulling, J (1990). ‘(XI transfer capacity as a tletrrrriiriing fiictor of survival tor srvere hypoxacinic (:Ol’D patienls undcr loiig-tern1 oxygen t hcr.apy ’ , ~:urol,a,c?a,/ou~n-ilo/’ Re,s$imtory
Y%rrlll,y, 2, 25.
l)i.Y(~eL,sP, 3, 1042-47.
Physiotherapy May 1999/vol85/no 5

258
Goldstein, R S, Gort, E H, Stubbing, D, Avendano, M A and Guyatt, G H ( I 994). ‘l<aritlorniscd coritrollcd trial of’ rc.spimtoi-y rcii~~l)ilit~~tioii’, I,crncP/, 19, 314 (8!134), 1394-97.
Gorecka, D, Czajkowska-Malinowska, M, Jedrzejczak, M, Filipowska, M, Sokolowska, L, Sporna, E, Nykiel, E, Malosek, D, Tobiasz, M, Sliwinski, P and Pulka, M J (1996). ‘Evaluation or‘ prognostic factors arid progress of disease in paticnts with (:OPD t i catcd with loiig-rcrm ox ygc n ’ , 1’nnP~Limt)rrolo~z~i A l ( v y d o ~ i ~ ~ Po Itha, 64, 9-10, 544-553.
Hodgkin, J E (1997). ‘Benefits of piilinonary rehabilitation’ in: Fishrnan, A 1’ (ctl) Pulmortaty RPhabalilntion, Marcel Dekkrr Inc, New York, chap 3.
Hudson, L D, Tyler, M L and Petty, T L (1976). ‘I Iospitalisatiori net:ds tlrrring an out-patient rcliabilitation program for severe chronic airway obstruction’, (,‘/it:,tt, 70, 5, 606-6IO.
Kaplan, E L and Meier, P (1958). ‘Non- parametric estimation Crorri incomplete observat ion ’ , Jowrnnl /I/’ bht Avwicriwt Stulir l i e d A , s , s o c ~ ( L ~ ~ o ~ ~ , 53, 457-48 1 .
Kda, K, Jinno, S, Nomura, K, Yamada, K, Katsura, H and Kudoh, S (1998). ‘Pulnionary rcha\,ilitation.progr‘~m siirvcy in North Airirrica, Europc, a i i d Tokyo’, , fourr id 0/’ ~~~~rrl iol ,ulvrio~zary Kehnbilitation, 18, /1, 30 1-308.
Lacasse, Y, Wong, E, Guyatt, G H, King, D, Cook, D J and Goldstein, R S (1996). ‘Mcta.-arial respiratory rehabilitation in chronic obstruc:tivc pulnioriary disease’, I.ancul, 348, 10, 1 I 15-19.
Mahler, D A, Guyatt, G H and Jones, P W (1997). ‘<:liriical nicasiirrinent ol’t1yspnoc;i’ in: Fishman, A 1’ (cd) /J7~lm(iv,(~t-y I(c.hnt,%lilalion, Marcel Deltker Iric, New York, chap 5.
Medical Research Council Working Party (1981). ‘I mng-term dorriicili;try oxygen therapy in chronic: hypoxic cor pulrrionale complicating chronic: kironchitis and ctuphysema’, I.ancc!t, 28, 3, 682-685.
Narita, T, Otsuto, A, Takenaka, H, Yoneda, N, Yoshikawa, M, Tsukapchi, K, Tokuyama T, Okamoto, Y, Yamamoto, T, Nakatani, M, Kobayashi, A, Kawashiro T and Konno, K (1997). Nabiorird S u r w y ort Nulrilionnl S l n l u . ~ oJ’ / ’ U L I I L O ~ L ~ L ~ Y l~ , ir i~i~i ,y ,s tJi i i [ i . Keport of’ I Irc M O t l Working Group o n I’tilrnoriary Empliyscrria (in ,Jqxiricst-) Ministry of Health, ‘ lokyo.
Nocturnal Oxygen Therapy Trial Group (1980). ’(hntinuous o r nocturnal oxygen therapy in hypoxcmic chronic obstructive hing disease’, Aii’trnO 01 lr/~lernrcl M~licivre, 93, 3, 3!9 1-398.
Oswald-Mammosser, M, Weitzenblum, E, Quoix, E, Moser, G, Chaouat, A, Charpentier, C and Kessler, R (1995). ‘l’rogiiostic t8ctor.s in (:01’D patients rrcciving long-term oxygen therapy: Importancr of’ piilnioiiary artcry pressiirc’, Che,.tl, 107, 5, 1193-!)8.
Petty, T L (1993). ‘I’ulnlonary ri:habjlitation i i i
pcxrspec:1ivc: 1Iistoric:al roots, present status, a r i d fiitrirc projrctions’, ‘Ihomx, 48, 8, 855-862.
Ramirez-Venegas, V R, Ward, J L, Olmstead, E M, Tosteson, A N and Mahler, D A (1997). ‘Effi-cl of’ exrrcisc training on dysprioea nicasures i i i
pt icnts with clironic obstriictivc pulrrionary disrascs’ , ,j)uwml o/ (:c~rrlio~~c*/7rio*l1/,r~ R~hahilillilion, 17, 2, 103-109.
Reina-Rosenbaum, R, Bach, J R and Penek, J (1997). ‘The cost/hcriefits of outpatient-basctl pulmonary rel-iabilit;itiori’, Archivrc (!ff’hy.ticnl Mrdit:i.nw a n d Rehahililation, 78, 3, 240-244.
Sahn, S A, Nett, L M and Petty, T L (1980). “ I r r i - year follow-up of a corriprehcirsivc: rt:liabilitatiori prograrri for sevcrc COI’D’, C 31 1-314.
Senjyu, Hand Katsuno, K (1997). ‘Piilrrionary reh abil ita tiori i r i Japan ’ , lie!iab%lilalion Ma.nngemen / Z~ZlPrnnlional, 7, 30-3 I .
Skwarski, K, MacNee, W, Wraith, P K, Sliwinski, P and Zielinski, J (1991). ‘l’redictors of‘ siirvival iri patients wilt1 clironic obstruct ive pulrriotlary disease treated with long- tcriri oxygen therapy’, C h , s l , 100, 6, 1522-27.
Smith, K, Cook, D, Guyatt, G H, Madhavan, J and Oxman, AD (1992). ‘Respiratory mtrscle training in chronic airflow liniitation: A rnera-analysis’,
I . Amtricnn I i w i u w of l&q%rato~ l~i,toa.w, 145,
Strom, K (1993). ‘Survival ofpatieiits with chronic obstructive p iho r l a ry disease receiving l o r ig-te r in tlc ) ni i cil i ary ()xyge n t h e ra p y ’ , Anic.)ic:a 17,
I<e71irro ?JI<i~,sI~ir(.to~y I)iseases, 147, 3, 585-591.
Swerts, P M J, Kretzers, L M J, Terpstra-Lindeman, E, Verstappen, F T J and Wouters, E F M (1990). ‘Exercise reconditioning i n thc rchabilitation of‘ patients with chronic: obstructive piilmonary disease: A short- arid lorig- term analysis’, l~v‘chi~~.). OJ‘Physiccil Mediccnr and 12eh%abilibalion, 71, 57-73.
Wijkstra, P J, Van Altena, R, Kraan, J, Otten, V, Postma, D S and Koeter, G H (1994). ‘Quality of lift: in patients with chronic obstructive piilmonary disease improves after rehabilitation at home’, I:‘ur(ifieaia, Jourmd of fi,sf)iralory I)i,si?u.w, 7,2,2ii9-27:1.
Wilson, D 0, Rogers, R M, Wright, E C and Anthonisen, N R (1989). ‘Body weight in chronic obstructive pulmonary disease: The National Institutes of’ Health intermittent positive pressure l)reathing trial’, ii’meiimn h ~ i e w i fI&q?ir~~hry Di,sea.te,~, 139, 6, 1435-35.
Wuertemberger, G, Zielinsky, J, Sliwinsky, P, Auw-Haedrick, C and Matthys, H (1990). ‘Survival in chronic obstrrictivc pulmonary disease after diagnosis of pulmonary hypertension related to long-term oxygen therapy’, I,ung, 168 (suppl), 762--769.
Physiotherapy MAY 1OSS/vol X5/na 5