Embed Size (px)
Citation preview

Effects of unilateral hyperinflation on the interpulmonary distribution of pleural pressure
ROLF D. HUBMAYR AND SUSAN S. MARGULIES (With the Technical Assistance of Steven B. Nelson and Mark A. Schroeder) Division of Thoracic Diseases and Internal Medicine, Mayo Clinic and Mayo Foundation, Rochester, Minnesota 55905
HUBMAYR, ROLF D., AND SUSAN S. MARGULIES. Effects of unilateral hyperinflation on the interpulmonary distribution of pleural pressure. J. Appl. Physiol. 73(4): 1650-1654, 199X- Motivated by single lung transplantation, we studied the me- chanics of the chest wall during single lung inflations in recum- bent dogs and baboons and determined how pleural pressure (Ppl) is coupled between the hemithoraces. In one set of experi- ments, the distribution of Ppl was inferred from known vol- umes and elastic properties of each lung. In a second set of experiments, costal pleural liquid pressure (Ppl,,,) was mea- sured with rib capsules. Both methods revealed that the in- crease in Ppl over the ipsilateral or inflated lung (APpli) is greater than that over the contralateral or noninflated lung ( APpl,). Mean d( APpl,) /d( APpli) and its 95% confidence inter- val was 0.7 t 0.1 in dogs and 0.5 t 0.1 in baboons. In a third set of experiments in three dogs and three baboons, we prevented sternal displacement and exposed the abdominal diaphragm to atmospheric pressure during unilateral lung inflation. These interventions had no significant effect on Ppl coupling between the hemithoraces. We conclude that lungs of unequal size and mechanical properties need not be exposed to the same surface pressure, because thoracic midline structures and the lungs themselves resist displacement and deformation.
chest wall mechanics; mediastinal compliance; single lung transplantation
MOTIVATED by the introduction of single lung transplan- tation into clinical practice, our aim is to define the mech- anisms that govern the interactions between two lungs with different mechanical properties. In trying to under- stand how lung-lung interactions affect the interpul- monary distribution of ventilation, we propose the hy- pothesis that under some circumstances the two lungs are exposed to different mean surface or pleural pres- sures (Ppl). One such condition may exist when a dynami- cally hyperinflated emphysematous lung operates in par- allel with a smaller implant. To test this hypothesis, we evaluated the interpulmonary distribution of Ppl during single lung inflations in normal recumbent dogs and ba- boons. Dogs were studied in anticipation of further ex- periments with a canine model of unilateral emphysema (14, 17, 19). In addition, we made measurements in ba- boons because of their greater anatomic similarity to hu- mans.
In this paper, we present the results of three sets of experiments to test the hypothesis that there are side-to- side differences in mean Ppl when lungs and chest wall
are deformed by single lung inflation. In the first set of experiments on seven dogs and three baboons, the inter- pulmonary distribution of Ppl was inferred from known volumes and elastic properties of each lung (indirect method). In the second set of experiments in four addi- tional dogs, we made direct measurements of costal pleural liquid pressure (Ppl,,,) during single lung infla- tions (20). In the third set of experiments on three dogs and three baboons, we evaluated whether anatomic pathways such as the rib cage and diaphragm-abdomen contribute to pressure coupling between the hemitho- races.
METHODS
Eleven dogs (20-35 kg) and three baboons (12-15 kg) were anesthetized with pentobarbital sodium (25-30 mg/ kg) and studied in the supine posture. Dogs were intu- bated translaryngeally with a Y-shaped dual-lumen en- dotracheal tube (Kottmeyer, Rusch). In baboons, the left main stem bronchus was intubated with a Robertshaw dual-lumen endotracheal tube through a tracheostomy. The position of the endotracheal tube was adjusted under endoscopic guidance to ensure patency of all lobar bronchi. The animals were mechanically ventilated with a Harvard pump. A balloon catheter was placed in the mid- to lower third of the esophagus for the measure- ment of intrathoracic pressure (Pes). The position of the esophageal balloon catheter was adjusted until the change in Pes during inspiratory efforts against an oc- cluded airway fell to within 1 cmH,O of the change in airway pressure (Pao) (2). Right and left Pao were re- corded from the proximal ends of the respective endotra- cheal tube lumina. Gas flow (V) to each lung was mea- sured with separate pneumotachographs (Fleisch no. 2) and differential pressure transducers (Validyne MP 45). Pressure and V signals were displayed on a strip chart recorder (Hewlett-Packard) and stored on a computer (DEC 11/70). The change in right and left lung volumes was determined by computer integration of the digitized flow signals. The relaxation volume (Vrel) of each lung was measured with an N, equilibration technique (5). The resident gas of the lung(s) at Vrel was equilibrated with a known volume of 0,. This was accomplished by five slow manual inflations and deflations of the lung(s) with a calibrated supersyringe. The N, concentration be- fore and after equilibration was measured with a mass
1650 0161-7567/92 $2.00 Copyright 0 1992 the American Physiological Society

EFFECTS OF UNILATERAL HYPERINFLATION 1651
spectrometer (Centronic, Croyton). By use of this tech- nique, Vrel values fell within 5% of those measured with plethysmography (15).
Rib capsule technique. In four dogs, Ppl,,, was mea- sured directly from rib capsules (20). Overlying tissue was removed from the third, fourth, and/or fifth ribs along both midaxillary lines. Small holes (2 mm diam) were drilled through the ribs, leaving the parietal pleura intact. A plastic intravenous tubing adapter was placed into the hole and glued to the rib. Polyethylene tubing was connected to the adapter, filled with methylene blue- colored saline, and capped with a rubber stopcock. The capsule was then anchored to the rib with screws and dental acrylic. An M-gauge needle attached to a fluid- filled catheter was introduced through the rubber stop- cock, and the parietal pleura was perforated. Then the polyethylene catheter was clamped to avoid air entry into the pleural space, the needle and rubber stopcock were removed, and the capsule was connected to a liquid-filled pressure transducer assembly (Cobe Lab, Lakewood, CO). Pressure recordings were taken only from rib cap- sules that met the following frequency-response criteria and gave reproducible readings. Ppl,,, tracings had to show cardiogenic oscillations and reach a new pressure plateau 10 s after a step change in lung volume. A lateral chest X-ray was taken during each experiment to guard against inclusion of data from dogs with a pneumo- thorax. In supine dogs, a pneumothorax causes the heart to drop away from the sternum toward the spine. The lungs were also inspected postmortem under water for needle puncture marks and air leaks.
Experimental protocol. After muscle paralysis was in- duced with pancuronium bromide (0.2 mg/kg), both lungs were inflated to total lung capacity (TLC) to pro- vide a constant volume history. TLC of each lung was defined as the volume at a Pao of 30 cmH,O. Subse- quently, the respiratory system was inflated from Vrel in small volume steps, exposing both lungs to the same al- veolar pressure. This was done with a calibrated super- syringe attached to a Y port that connected the two lumina of the endotracheal tube. From the recorded pressures and integrated flows, separate inflation pres- sure-volume curves were constructed for each lung. Only for maneuvers during which both lungs were inflated si- multaneously to a common airway pressure was trans- pulmonary pressure (PL) defined as the difference be- tween Pao and Pes.
After an inflation of both lungs to TLC, one lung was inflated from Vrel in small volume steps while the lumen of the endotracheal tube leading to the contralateral lung was occluded. Complete separation between ipsilateral (side of inflation) and contralateral airways was assumed if a constant pressure difference could be maintained at each inflation step. Right and left single lung inflations were repeated in random order.
Unilateral inflation measurements were repeated in three of the seven dogs and in all baboons after minimi- zation of possible contributions of rib cage and dia- phragm-abdomen pathways to pressure transmission be- tween the hemithoraces. First, two hooks were screwed into the sternum and rigidly attached to a stationary steel bar, preventing any sternal motion during single
lung inflation. Second, the abdomen was opened through a midline incision, and the abdominal contents were moved to expose a large portion of the abdominal surface of the diaphragm to atmospheric pressure.
Rationale for data handling (indirect method). It was necessary to make two assumptions to derive the Ppl distribution during single lung inflation from Pes, Pao, and lung volume measurements. Their validity is consid- ered in the DISCUSSION. The first assumption is that Ppl increases uniformly during bilateral lung inflations and that, under these conditions, the change in Pes (Apes) reflects the increase in average Ppl within both hemi- thoraces (3,21). On the basis of this assumption, we con- structed right and left lung PL-volume curves from the Pao, Pes, and bronchospirometric volume measurements during bilateral lung inflation and computed their re- spective inflation compliances (CL). The second assump- tion is that, at volumes near Vrel, the lungs are fluidlike and their elastic properties can be described by a single compliance (6). Consequently, each lung’s PL-volume curve can be used to predict its corresponding PL during bilateral and single lung inflations.
Specifically, the change in ipsilateral Ppl (APpli) dur- ing single lung inflation from Vrel was computed from the difference between the change in measured ipsilat- era1 airway pressure (APao;) and an estimated change in ipsilateral transpulmonary pressure ( APLi)
APpli = APao; - APLi (0
APLi was estimated from the known ipsilateral CL (CLi) and from the ipsilateral volume increase ( AVi) above Vrel
APLi = AVi/CLi (2)
Substitution of Eq. 2 into Eq. 1 results in the relationship used to estimate APpli during unilateral lung inflation
APpli = APaoi - AViICLi 0
Similarly, the change in contralateral Ppl (APpl,) is given by the relationship
APP4 = APao, - AVJCL, 0
However, the volume of the contralateral lung (V,) was held constant at Vrel (AVc = 0). Therefore
APPl, = APao, (5)
Statistical methods. The relative rates of change in Ppli and Ppl, during single lung inflations were computed us- ing a linear regression analysis. Regression slopes [d(Appl~)/d(APpli)] and their 95% confidence intervals were derived for both indirect and direct Ppl measure- ments in dogs and baboons. The effects of experimental interventions, such as sternal fixation, on the regression slopes were compared using a one-factor analysis of vari- ance for repeated measures.
RESULTS
Figure 1 shows a comparison of the indirect APpli and APpl, estimates from seven dogs. The slope of the re- gression line of 0.7 t 0.1 (significantly different from 1, P 5 0.05) underscores that in the recumbent dog the average rise in Ppl during single lung inflation is nonuni-
1652 EFFECTS OF UNILATERAL HYPERINFLATION
Of . I . I . I 4 0 2 4 6
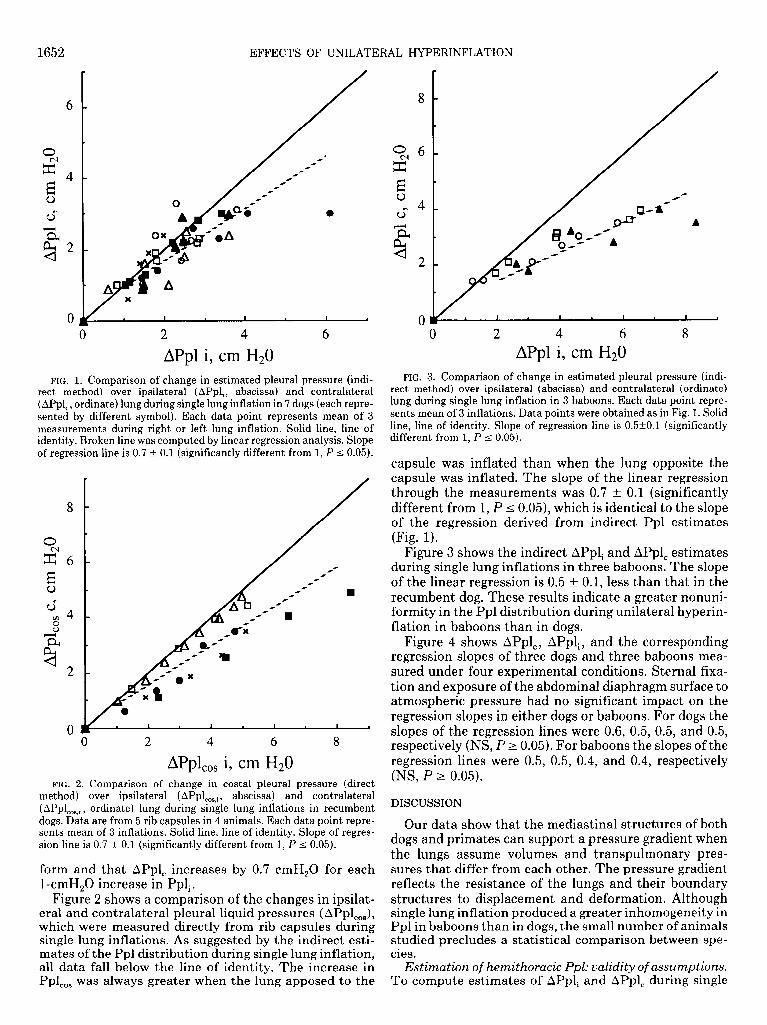
APpl i, cm Hz0 FIG. 1. Comparison of change in estimated pleural pressure (indi-
rect method) over ipsilateral ( APpli, abscissa) and contralateral ( APpl,, ordinate) lung during single lung inflation in 7 dogs (each repre- sented by different symbol). Each data point represents mean of 3 measurements during right or left lung inflation. Solid line, line of identity. Broken line was computed by linear regression analysis. Slope of regression line is 0.7 & 0.1 (significantly different from 1, P 5 0.05).
8
0 0 2 4 6 8
APpl,,, i, cm Hz0 FIG. 2. Comparison of change in costal pleural pressure (direct
method) over ipsilateral (APpl,,,,i, abscissa) and contralateral
( ~PPL3 c 9 ordinate) lung during single lung inflations in recumbent dogs. Data are from 5 rib capsules in 4 animals. Each data point repre- sents mean of 3 inflations. Solid line, line of identity. Slope of regres- sion line is 0.7 & 0.1 (significantly different from 1, P I 0.05).
form and that APpl, increases by 0.7 cmH,O for each l-cmH,O increase in Ppli.
Figure 2 shows a comparison of the changes in ipsilat- era1 and contralateral pleural liquid pressures ( APpl,,,), which were measured directly from rib capsules during single lung inflations. As suggested by the indirect esti- mates of the Ppl distribution during single lung inflation, all data fall below the line of identity. The increase in Ppl,,, was always greater when the lung apposed to the
8 -
94 6 - z E . 0 0” 4 -
n.
0 I a I . I . I 4
0 2 4 6 8
APpl i, cm Hz0 FIG. 3. Comparison of change in estimated pleural pressure (indi-
rect method) over ipsilateral (abscissa) and contralateral (ordinate) lung during single lung inflation in 3 baboons. Each data point repre- sents mean of 3 inflations. Data points were obtained as in Fig. 1. Solid line, line of identity. Slope of regression line is 0.5kO.l (significantly different from 1, P 5 0.05).
capsule was inflated than when the lung opposite the capsule was inflated. The slope of the linear regression through the measurements was 0.7 t 0.1 (significantly different from 1, P 5 0.05), which is identical to the slope of the regression derived from indirect Ppl estimates (Fig. 1).
Figure 3 shows the indirect APpli and APpl, estimates during single lung inflations in three baboons. The slope of the linear regression is 0.5 t 0.1, less than that in the recumbent dog. These results indicate a greater nonuni- formity in the Ppl distribution during unilateral hyperin- flation in baboons than in dogs.
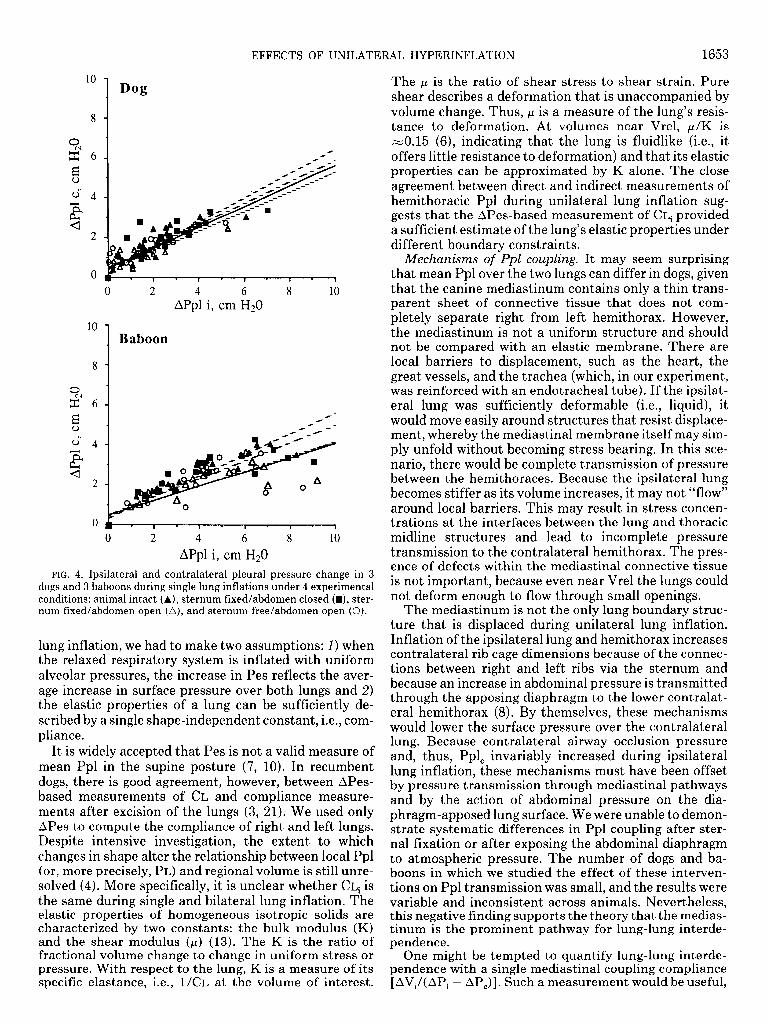
Figure 4 shows APpl,, APpli, and the corresponding regression slopes of three dogs and three baboons mea- sured under four experimental conditions. Sternal fixa- tion and exposure of the abdominal diaphragm surface to atmospheric pressure had no significant impact on the regression slopes in either dogs or baboons. For dogs the slopes of the regression lines were 0.6, 0.5, 0.5, and 0.5, respectively (NS, P 2 0.05). For baboons the slopes of the regression lines were 0.5, 0.5, 0.4, and 0.4, respectively (NS, P > 0.05).
DISCUSSION
Our data show that the mediastinal structures of both dogs and primates can support a pressure gradient when the lungs assume volumes and transpulmonary pres- sures that differ from each other. The pressure gradient reflects the resistance of the lungs and their boundary structures to displacement and deformation. Although single lung inflation produced a greater inhomogeneity in Ppl in baboons than in dogs, the small number of animals studied precludes a statistical comparison between spe- cles.
Estimation of hemithoracic Ppl: validity of assumptions. To compute estimates of APpli and APpl, during single
EFFECTS OF UNILATERAL HYPERINFLATION 1653
0
EC6
2
2 4 6 8 10
APpl i, cm Hz0
10
1 Baboon
0
$6 E 0
cJ 4 E u
2
I - I - I - I - 1
0 2 4 6 8 10
APpl i, cm Hz0
FIG. 4. Ipsilateral and contralateral pleural pressure change in 3 dogs and 3 baboons during single lung inflations under 4 experimental conditions: animal i ntact (A), sternum fixed/abdomen closed (H), ster- num fixed/abdomen open (A), and sternum free/abdomen open (0).
lung inflation, we had to make two assumptions: 1) when the relaxed respiratory system is inflated with uniform alveolar pressures, the increase in Pes reflects the aver- age increase in surface pressure over both lungs and 2) the elastic properties of a lung can be sufficiently de- scribed by a single shape-independent constant, i.e., com- pliance.
It is widely accepted that Pes is not a valid measure of mean Ppl in the supine posture (7, 10). In recumbent dogs, there is good agreement, however, between APes- based measurements of CL and compliance measure- ments after excision of the lungs (3, 21). We used only APes to compute the compliance of right and left lungs. Despite intensive investigation, the extent to which changes in shape alter the relationship between local Ppl (or, more precisely, PL) and regional volume is still unre- solved (4). More specifically, it is unclear whether CL, is the same during single and bilateral lung inflation. The elastic properties of homogeneous i sotropic solids are characterized by two constants: the bulk modulus 0 and the shear modulus (p) (13). The K is the ratio of fractional volume change to change in uniform stress or pressure. With respect to the lung, K is a measure of its specific elastance, i.e., ~/CL at the volume of interest.
The p is the ratio of shear stress to shear strain. Pure shear describes a deformation that is unaccompanied by volume change. Thus, p is a measure of the lung’s resis- tance to deformation. At volumes near Vrel, p/K is ~0.15 (6), indicating that the lung is fluidlike (i.e., it offers little resistance to deformation) and that its elastic properties can be approximated by K alone. The close agreement between direct and indirect measurements of hemithoracic Ppl during unilateral lung inflation sug- gests that the Apes-based measurement of CL, provided a sufficient estimate of the lung’s elastic properties under different boundary constraints.
Mechanisms of Ppl coupling. It may seem surprising that mean Ppl over the two lungs can differ in dogs, given that the canine mediastinum contains only a thin trans- parent sheet of connective tissue that does not com- pletely separate right from left hemithorax. However, the mediastinum is not a uniform structure and should not be compared with an elastic membrane. There are local barriers to displacement, such as the heart, the great vessels, and the trachea (which, in our experiment, was reinforced with an endotracheal tube). If the ipsilat- era1 lung was sufficiently deformable (i.e., liquid), it would move easily around structures that resist displace- ment, whereby the mediastinal membrane itself may sim- ply unfold without becoming stress bearing. In this sce- nario, there would be complete transmission of pressure between the hemithoraces. Because the ipsilateral lung becomes stiffer as its volume increases, it may not “flow” around local barriers. This may result in stress concen- trations at the interfaces between the lung and thoracic midline structures and lead to incomplete pressure transmission to the contralateral hemithorax. The pres- ence of defects within the mediastinal connective tissue is not important, because even near Vrel the lungs could not deform enough to flow through small openings.
The mediastinum is not the only lung boundary struc- ture that is displaced during unilateral lung inflation. Inflation of the ipsilateral lung and hemithorax increases contralateral rib cage dimensions because of the connec- tions between right and left ribs via the sternum and because an increase in abdominal pressure is transmitted through the apposing diaphragm to the lower contralat- era1 hemithorax (8). By themselves, these mechanisms would lower the surface pressure over the contralateral lung. Because contralateral airway occlusion pressure and, thus, Ppl, invariably increased during ipsilateral lung inflation, these mechanisms must have been offset by pressure transmission through mediastinal pathways and by the action of abdominal pressure on the dia- phragm-apposed lung surface. We were unable to demon- strate systematic differences in Ppl coupling after ster- nal fixation or after exposing the abdominal diaphragm to atmospheric pressure. The number of dogs and ba- boons in which we studied the effect of these interven- tions on Ppl transmission was small, and the results were variable and inconsistent across animals. Nevertheless, this negative finding supports the theory that the medias- tinum is the prominent pathway for lung-lung interde- pendence.
One might be tempted to quantify lung-lung interde- pendence with a single mediastinal coupling compliance
- APJ. Such a measurement would be useful,

1654 EFFECTS OF UNILATERAL HYPERINFLATION
however, only if it was independent of lung shape and This study was supported by National Heart, Lung, and Blood Insti-
stiffness, if it reflected only the displacement impedance tute Grant HL-38107.
of thoracic midline structures themselves, and if it was Address for reprint requests: R. D. Hubmayr, 4-411 Alfred Bldg.,
insensitive to the stress placed on the mediastinum be- Mayo Clinic, 200 First St. SW, Rochester, MN 55905.
fore its displacement. For example, tissue attachments Received 10 February 1991; accepted in final form 14 April 1992.
between diaphragm and thoracic midline structures may exert axial tension on the mediastinum. This would
REFERENCES l
make the “so-called” mediastinal compliance sensitive to changes in diaphragm activity and chest wall shape and limit its predictive value as a simple determinant of the interpulmonary Ppl distribution. Although our study does not offer insights into the relative importance of these mechanisms, it does underscore that lungs with unequal size and elastic properties need not be exposed to the same surface pressure.
BATES, D. The other lung. N. Engl. J. Med. 282: 277-278, 1970. BAYDUR, A., P. K. BEHRAKIS, W. A. ZIN, M. JAEGER, AND J. MILIC- EMILI. A simple method for assessing the validity of the esophageal balloon technique. Am. Rev. Respir. Dis. 126: 788-791, 1982. GILLESPIE, D. J., Y. L. LAI, AND R. E. HYATT. Comparison of esoph- ageal and pleural pressures in anesthetized dog. J. Appl. Physiol. 35: 709-713, 1973.
Implication of results to lung mechanics in disease. Ac- cording to the classic model of Milic-Emili et al. (ll), the lung is an isotropic homogeneous elastic solid that is ex- posed to a vertical gradient in surface pressure when the chest wall is intact. At Vrel, dependent lung units are exposed to a greater surface pressure and assume a smaller volume than nondependent units. Given the nonlinear relationship between volume and PL, the lung parenchyma of dependent units is less resistant to vol- ume expansion and deformation. Thus, when all lung regions are exposed to the same change in Ppl, the topo- graphical distribution of ventilation reflects primarily regional differences in lung elastic properties.
Stevens et al. (16) measured regional volumes and ventilation in two emphysematous patients who died shortly after single lung transplantation. They noted that the native emphysematous lung received a greater fraction of the inspired gas than the implant and con- cluded that this observation was produced by a parallel inhomogeneity in lung elastic properties. In an accom- panying editorial, Bates (1) assumed that, during breath- ing, intrathoracic pressure changes uniformly over both lungs, reducing the determinants of the interpulmonary distribution of gas flow to lung resistance and compli- ance (12). Because blood flow to the implant exceeded that of the native emphysematous lung, single lung transplantation for patients with chronic obstructive pul- monary disease (COPD) was abandoned on the basis of the belief that the procedure would invariably cause in- terpulmonary ventilation-perfusion mismatch.
The recent success of single lung transplantation in patients with COPD raises questions about Stevens’ ob- servations and conclusions (9, 18). The findings in this communication challenge the assumption that lung sur- face pressure changes uniformly when the lungs operate at different volumes and transpulmonary pressures. Such a condition may exist if an emphysematous lung with expiratory flow limitation hyperinflates and starts to “compress” the contralateral implant. The extent to which implant volume and ventilation are affected by dynamic hyperinflation depends on the degree of pneu- matic coupling between the hemithoraces.
The authors thank Dr. Theodore Wilson for insightful comments, Dr. Stephen Lai-Fook for help with the rib capsule technique, and Lori Oeltjenbruns for preparing the manuscript.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
HOPPIN, F. G., AND J. HILDEBRANDT. Mechanical properties of the lung. In: Bioengineering Aspects of the Lung, edited by J. B. West. New York: Dekker, 1977, vol. 3, p. 83-162. (Lung Biol. Health Dis. Ser.) KIERS, A., T. W. VAN DER MARK, M. G. WOLDRING, AND R. PESET. Determination of the functional residual capacity during exercise. Ergonomics 23: 955-959, 1980. LAI-FOOK, S. J., T. A. WILSON, R. E. HYATT, AND J. R. RODARTE. Elastic constants of inflated lobes of dog lungs. J. Appl. Physiol. 40: 508-513,1976. LINDERHOLM, H. Lung mechanics in sitting and horizontal pos- tures studied by body plethysmographic methods. Am. J. Physiol. 204: 85-91, 1963. LORING, S. H., AND J. MEAD. Action of the diaphragm on the rib cage inferred from a force-balance analysis. J. Appl. Physiol. 53: 756-760,1982. MAL, H., B. ANDREASSIAN, F. PAMELA, J. P. DUCHATTELLE, E. RONDEAU, F. DUBOIS, P. BALDEYROU, M. KITZIS, C. SLEIMAN, AND R. PARIENTE. Unilateral transplantation in end-stage pulmonary emphysema. Am. Rev. Respir. Dis. 140: 797-802, 1989. MEAD, J., AND E. A. GAENSLER. Esophageal and pleural pressures in man upright and supine. J. Appl. Physiol. 14: 81-83, 1959. MILIC-EMILI, J. J., A. M. HENDERSON, M. B. DOLOVIC, B. TROP, AND K. KANEKO. Regional distribution of inspired gas in the lung. J. Appl. Physiol. 21: 749-759, 1966. OTIS, A. B., C. B. MCKERROW, R. A. BARTLETT, J. MEAD, B. B. MCILROY, N. D. SELVERSTONE, AND E. P. RADFORD. Mechanical factors in the distribution of pulmonary ventilation. J. Appl. Phys- iol. 8: 587-594, 1956. RODARTE, J. R., AND Y. C. FUNG. Distribution of stresses within the lung. In: Handbook of Physiology. The Respiratory System. Me- chanics of Breathing. Bethesda, MD: Am. Physiol. Sot., 1986, sect. 3, vol. III, pt. 1, chapt. 15, p. 233-245. SCHLICK, W., G. SALEM, A. KEILER, I. GIBER, 0. M~SCHL, M. GL~CKLER, T. RADASZKIEWICZ, S. SZALAY, AND W. KREUZER. Pul- monary function tests following single lung homotransplantation in emphysematous dogs. Res. Exp. Med. 166: 283-294, 1975. SCHROEDER, M. A., H.-Y. TAO, AND G. A. FARKAS. Mechanical role of expiratory muscle recruitment during eupnea in supine anesthe- tized dogs. J. Appl. Physiol. 70: 2025-2031, 1991. STEVENS, P. M., P. C. JOHNSON, R. L. BELL, A. C. BEALL, JR., AND D. E. JENKINS. Regional ventilation and perfusion after lung trans- plantation in patients with emphysema. N. Engl. J. Med. 282: 245- 249,197o. TAKARO, T., AND S. M. WHITE. Unilateral severe experimental pul- monary emphysema. Am. Rev. Respir. Dis. 108: 334-342, 1973. TRULOCK, E. P., T. M. EGAN, N. T. KOUCHOUKOS, L. R. KAISER, M. K. PASQUE, N. ETTINGER, J. D. COOPER, AND THE WASHING- TON UNIVERSITY LUNG TRANSPLANT GROUP. Single lung trans- plantation for severe chronic obstructive pulmonary disease. Chest 96:738-742,1989. VEITH, F. J., S. K. KOERNER, S. S. SIEGELMAN, M. TORRES, P. A. BARDFELD, L. A. ATTAI, S. J. BOLEY, T. TAKARO, A.ND M. L. GLIEDMAN. Single lung transplantation in experimental and hu- man emphysema. Ann. Surg. 178: 463-476,1973. WEINER-KRONISH, J. P., M. A. GROOPER, AND S. J. LAI-FOOK. Pleural liquid pressure in dogs measured using a rib capsule. J. Appl. Physiol. 59: 597-602, 1985. WOHL, M. E. B., J. TURNER, AND J. MEAD. Static volume-pressure curves of dog lungs -in vivo and in vitro. J. Appl. Physiol. 24: 348- 354, 1968.