Embed Size (px)
Citation preview

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 1
Timothy Kaja, MBA, CPCSenior Vice President, UnitedHealth GroupPresident, Provider and Network Service Operations, UnitedHealthcare
The Sixth HIPAA Summit West 2012
‘Eligibility and Claim Status Operating Rules'
October 12, 2012 9:30 am PST

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 2
• Mandatory Operating Rules Compliance Date – January 2013• Overview of UnitedHealth Group• Review of Operating Rules for Eligibility and Claim Status• UHG’s Transactions and Our Roadmap to Compliance• Moving the Industry to Adoption and Utilization• Future Considerations to drive Adoption and Utilization
UnitedHealthcare – Operating Rules and the Payer Experience
AGENDA

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 3
Meeting the Deadline – January 2013
THE JOURNEY TO COMPLIANCE• Administrative Simplification: Affordable Care Act
(ACA) Section 1104
• Payers must Certify Compliance by December 31, 2013
• Fines up to $20/per member per year

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 4
UnitedHealthcare
CAQH CORE Phase I and Phase II Operating Rulesand
CORE Certification Testing

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 5
UnitedHealth Group: Corporate Profile
OUR HEALTH BENEFITS BUSINESS: UNITEDHEALTHCARE OUR HEALTH SERVICES BUSINESS: OPTUM
Helping People Live Healthier Lives
UnitedHealthcare Community & State
UnitedHealthcare Employer & Individual
UnitedHealthcare Medicare & Retirement
Making the Health Care System Work Better for Everyone
OptumInsight
OptumHealth
OptumRx
“Health in Numbers”• Serving 35 million Americans at every stage of life• Innovation-driven growth• Exceptionally well positioned to evolve and grow through
health care reform
“Good for the System”A dedicated and independent business providing services to:
6,000 hospital facilities, 250,000 health care professionals, 60 million consumers
• Health care information technology• Consumer engagement and support• Integrated care delivery• Pharmacy • Health financial services
FOUNDATIONAL COMPETENCIES
• Domain knowledge around care management and care resources• Actionable health care information and intelligence• Advanced, enabling technology

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 6
• A Phase I and Phase II v5010 CORE-certified health plan
• CAQH Member and CORE Participant – Current CAQH Board Member and CORE Transition Committee Member.
• Current CAQH Board Chair: David S. Wichmann, Executive VP, UnitedHealth Group and President, UnitedHealth Group Operations and Technology
• UnitedHealth Group is an active collaborator on industry initiatives that simplify healthcare adminstration for health plans and providers, resulting in better care experience for patients and caregivers
United Healthcare: CAQH/CORE Involvement

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 7
UnitedHealthcare: Transaction Services Profile
• Health Plan Operations– Our customer servicing center handled more than 28 million Benefit/Eligibility
and Claim Status calls in 2011– Over 300 million claims were processed in 2011
• Eligibility and Benefits– Currently support the electronic exchange of eligibility transactions both in
real-time and batch– 2012 electronic eligibility inquiries volumes are approximately 170 million
annually– 95% of these eligibility transactions are handled in real-time
• Claim Status– Currently supporting the electronic exchange of claim status transactions both
in real-time and batch– Real-time claim status inquiry volumes in 2012 averaging ~260,000/day
Operational Objective: Collaborate with our provider network to transition phone calls and paper to electronic transactions, and transition batch to real-time.

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 8
Scope of CAQH CORE Operating Rules:Phase I and Phase II

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 9
CAQH CORE Rules 154 and 260 require that health plans and information sources that create a ASC X12 271 response to a generic ASC X12 270 inquiry must include:
• The name of the health plancovering the individual (if available)
• Provide patient financials for the static financials of co-insurance, co-payment, and deductible, and return the remaining deductible amount; include in-network and out-of-network coverage and financials for 48 required service types (benefits)
For more detail, see CORE Rules 154 and 260
Improve Eligibility Verification Plus
Financials
CAQH CORE Rule 258 requires health plans to normalize submitted and stored last name before using the submitted and stored last names:
• If normalized name validated, return ASC X12 271 with CORE-required content
• If normalized name validated but un-normalized names do not match, return last name as stored by health plan and specified INS segment
• If normalized name not validated, return specified AAA code
For more detail, see CORE Rule 258
Enhanced Error Reporting and Patient Identification
CAQH CORE Rule 259 requires health plans to return a unique combination of one or more AAA segments along with one or more of the submitted patient identifying data elements in order to communicate the specific errors to the submitter
The receiver of the ASC X12 271 response is required to detect all error conditions reported and display to the end user text that uniquely describes the specific error conditions and data elements determined to be missing or invalid
For more detail, see CORE Rule 259
Eligibility v5010 270/271:Transactional Data Content
© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 10
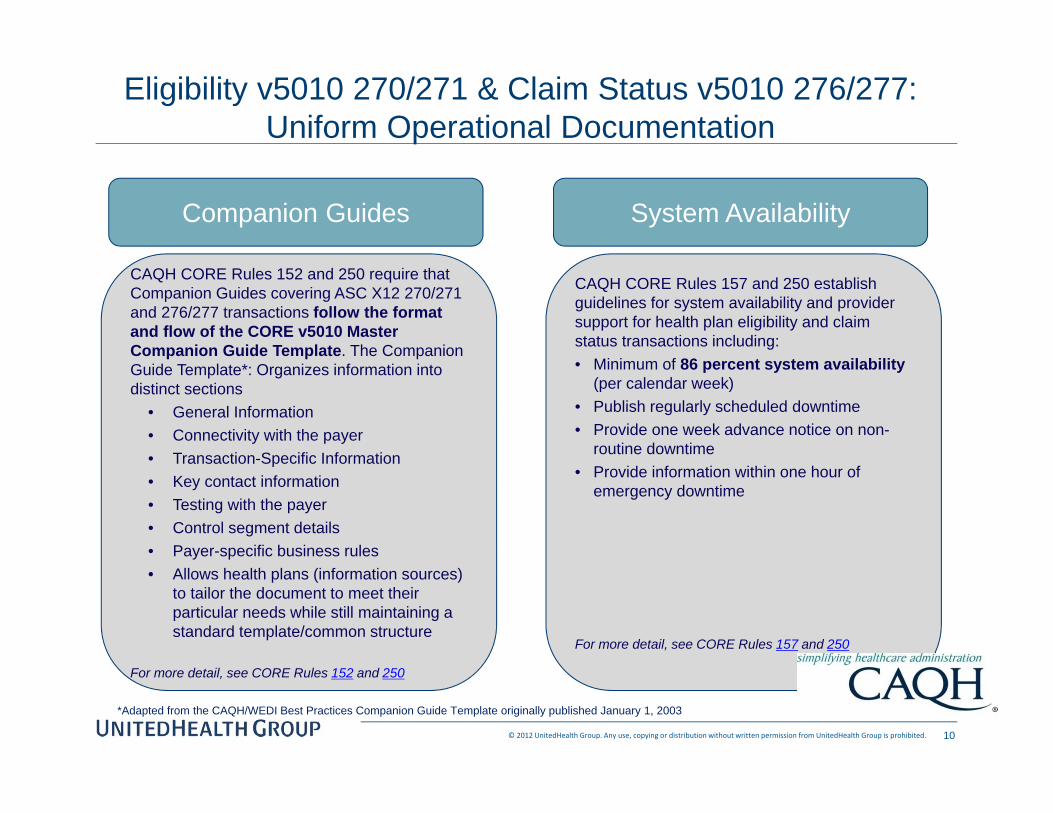
*Adapted from the CAQH/WEDI Best Practices Companion Guide Template originally published January 1, 2003
CAQH CORE Rules 152 and 250 require that Companion Guides covering ASC X12 270/271 and 276/277 transactions follow the format and flow of the CORE v5010 Master Companion Guide Template. The Companion Guide Template*: Organizes information into distinct sections
• General Information • Connectivity with the payer• Transaction-Specific Information • Key contact information• Testing with the payer• Control segment details• Payer-specific business rules• Allows health plans (information sources)
to tailor the document to meet their particular needs while still maintaining a standard template/common structure
For more detail, see CORE Rules 152 and 250
Companion Guides
CAQH CORE Rules 157 and 250 establish guidelines for system availability and provider support for health plan eligibility and claim status transactions including:• Minimum of 86 percent system availability
(per calendar week)• Publish regularly scheduled downtime• Provide one week advance notice on non-
routine downtime• Provide information within one hour of
emergency downtime
For more detail, see CORE Rules 157 and 250
System Availability
Eligibility v5010 270/271 & Claim Status v5010 276/277: Uniform Operational Documentation
© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 11
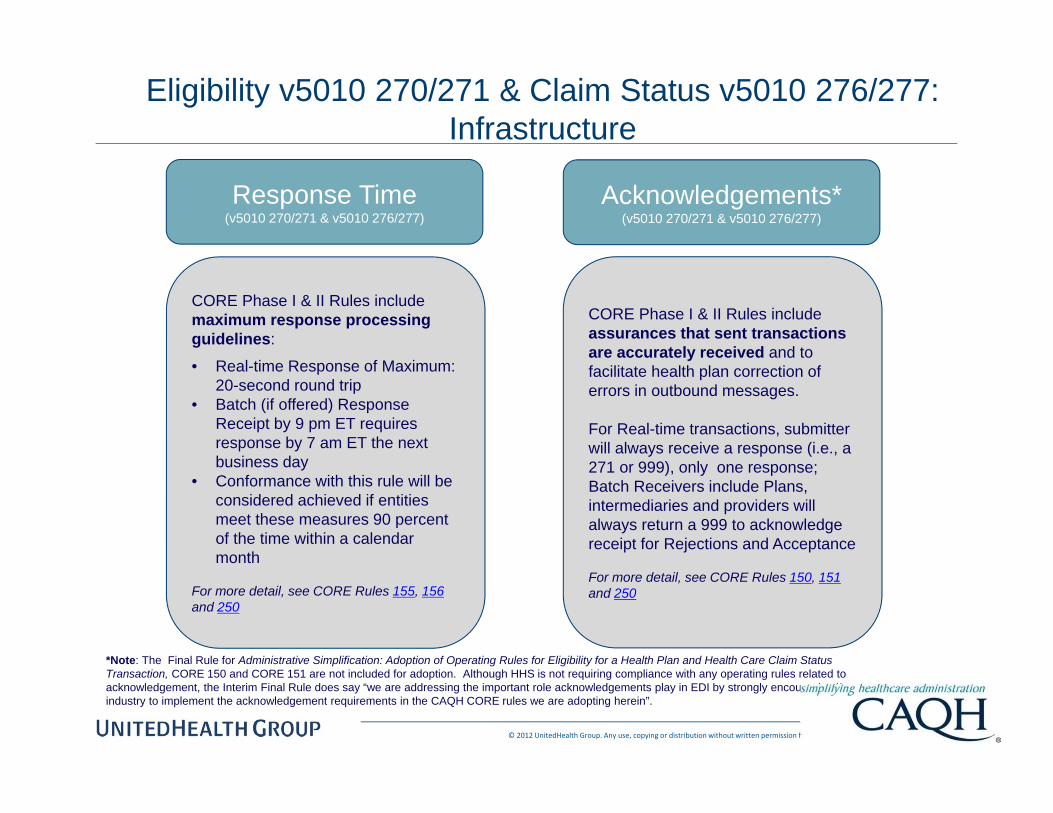
Eligibility v5010 270/271 & Claim Status v5010 276/277: Infrastructure
*Note: The Final Rule for Administrative Simplification: Adoption of Operating Rules for Eligibility for a Health Plan and Health Care Claim Status Transaction, CORE 150 and CORE 151 are not included for adoption. Although HHS is not requiring compliance with any operating rules related to acknowledgement, the Interim Final Rule does say “we are addressing the important role acknowledgements play in EDI by strongly encouraging the industry to implement the acknowledgement requirements in the CAQH CORE rules we are adopting herein”.
CORE Phase I & II Rules include maximum response processing guidelines:
• Real-time Response of Maximum: 20-second round trip
• Batch (if offered) Response Receipt by 9 pm ET requires response by 7 am ET the next business day
• Conformance with this rule will be considered achieved if entities meet these measures 90 percent of the time within a calendar month
For more detail, see CORE Rules 155, 156and 250
Response Time(v5010 270/271 & v5010 276/277)
CORE Phase I & II Rules include assurances that sent transactions are accurately received and to facilitate health plan correction of errors in outbound messages.
For Real-time transactions, submitter will always receive a response (i.e., a 271 or 999), only one response; Batch Receivers include Plans, intermediaries and providers will always return a 999 to acknowledge receipt for Rejections and Acceptance
For more detail, see CORE Rules 150, 151and 250
Acknowledgements*(v5010 270/271 & v5010 276/277)
© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 12
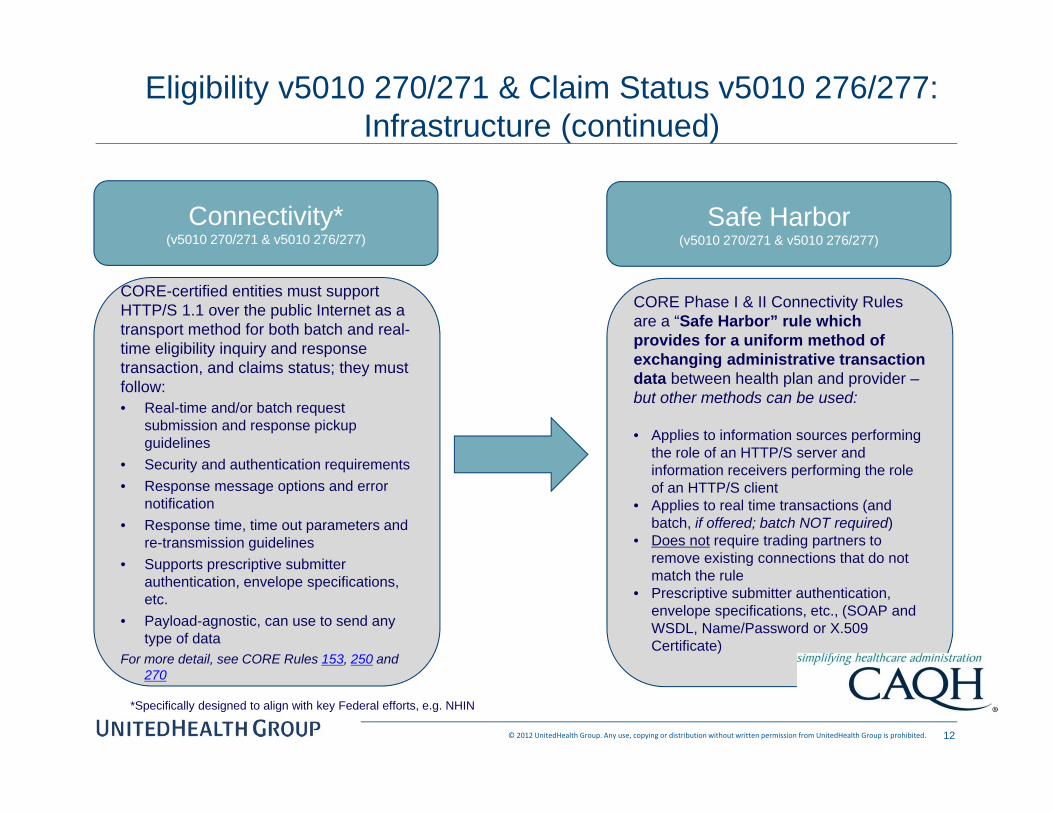
Eligibility v5010 270/271 & Claim Status v5010 276/277: Infrastructure (continued)
CORE-certified entities must support HTTP/S 1.1 over the public Internet as a transport method for both batch and real-time eligibility inquiry and response transaction, and claims status; they must follow:• Real-time and/or batch request
submission and response pickup guidelines
• Security and authentication requirements• Response message options and error
notification• Response time, time out parameters and
re-transmission guidelines• Supports prescriptive submitter
authentication, envelope specifications, etc.
• Payload-agnostic, can use to send any type of data
For more detail, see CORE Rules 153, 250 and 270
Connectivity*(v5010 270/271 & v5010 276/277)
CORE Phase I & II Connectivity Rules are a “Safe Harbor” rule which provides for a uniform method of exchanging administrative transaction data between health plan and provider –but other methods can be used:
• Applies to information sources performing the role of an HTTP/S server and information receivers performing the role of an HTTP/S client
• Applies to real time transactions (and batch, if offered; batch NOT required)
• Does not require trading partners to remove existing connections that do not match the rule
• Prescriptive submitter authentication, envelope specifications, etc., (SOAP and WSDL, Name/Password or X.509 Certificate)
Safe Harbor(v5010 270/271 & v5010 276/277)
*Specifically designed to align with key Federal efforts, e.g. NHIN

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 13
OptumInsight
Clearinghouse
UnitedHealthcare: Transaction Flow and Channels
Providers
External Customer Gateway
B2B UFE Claims Engines
ConnectivityDirector
Providers
ClearingHouses
DirectConnects
64%
1%
35%
CHANNEL*TRADINGPARTNERS
SYSTEMS INFRASTRUCTURE
Electronic channels support the following HIPAA ASC X12 transactions: • Real-Time eligibility (270/271), claim status (276/277) – using v5010 • Batch eligibility, claim status, referrals (278), payment advice (835), and claim (837)
LabCorpQuest
Large Facilities
Note: UnitedHealthcare (UHC) also supports web portal inquiries but is encouraging the adoption of electronic transaction processing

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 14
• Results from an internal research analysis indicated as many as 30% of call center service requests could be resolved by adopting the CORE Operating Rules for eligibility response transactions.
• Management’s interest in leveraging voluntary CORE Operating Rules to gain valuable experience and insight about the benefits associated with implementing industry operating rules prior to federal and state mandates
CORE Certification: Project Rational
© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 15
• United Healthcare Executive Management supported CORE certification as a critical organizational priority
• Enterprise-wide requirements were created for the HIPAA v5010 compliance project as well as for the implementation of Phase I and II CORE Operating Rules
• These requirements were shared with the different business segments for incorporation into their own business segment specific requirements
• Any issues or questions regarding the enterprise requirements where handled by one team to ensure consistency across the enterprise
• Majority of the CORE requirements were rigorously tested internally prior to conducting testing on the CORE Certification platform
CORE Certification: Project Approach

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 16
CORE Certification: Key Project Decisions
• CORE Operating Rules implementation was managed as its own project. The timeframe for implementing CORE Operating Rules ran concurrently with the organization’s HIPAA v5010 implementation.
Rationale– CORE Operating Rule requirements were deemed to be
approximately 10% of the total HIPAA v5010 implementation total effort.
– Project resources were shared between the CORE Certification and HIPAA v5010 implementation project teams with the goal of reducing project costs and ensuring availability of subject matter experts.
• Pursue Phase I and II CORE Certification concurrentlyRationale– The estimated cost of implementing Phase I and II together is less
than pursuing each phase separately– Planning, analysis, design, coding and testing are best handled as a
whole– The requirements for Phase I and Phase II CORE Certification
impacted the same IT systems– The need for rigorous internal testing required focused effort
© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 17
Lessons Learned: Test Planning & Systems Evaluation
• A full understanding of CORE Operating Rules requirements and how they impact your organization’s IT systems is essential
• Upfront business/systems planning and analysis is a major component of the project
• Technical and business analyst resources must be available and work closely together throughout the full lifecycle of the project
• Need somebody who really knows your health benefits products and how they are implemented in your systems
• If you rely on vendors, make sure they are involved early-on in the planning process

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 18
• Consider early on how CORE Master Test Bed Data (for testing eligibility rule) will be loaded and used within the context of your system environment. Advanced planning for test data setup is very critical.
– It took approximately 8 weeks to setup the data due to complexity of the UnitedHealthcare claim platforms
– Detailed understanding of the CORE Master test data along with your external interfaces/dependencies, and the data flow between applications is very critical
– Test data setup needs to include more test scenarios than what is specified when selecting your testing option
• Majority of the CORE requirements were rigorously tested internally before executing first test script
• Execute the test scripts first that you have concerns with as you can run the test scripts as many times as you want and this will give you more lead time to fix any problem areas
• Weekly staff meetings to assess progress once testing began were important
Lessons Learned: Certification Testing
© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 19
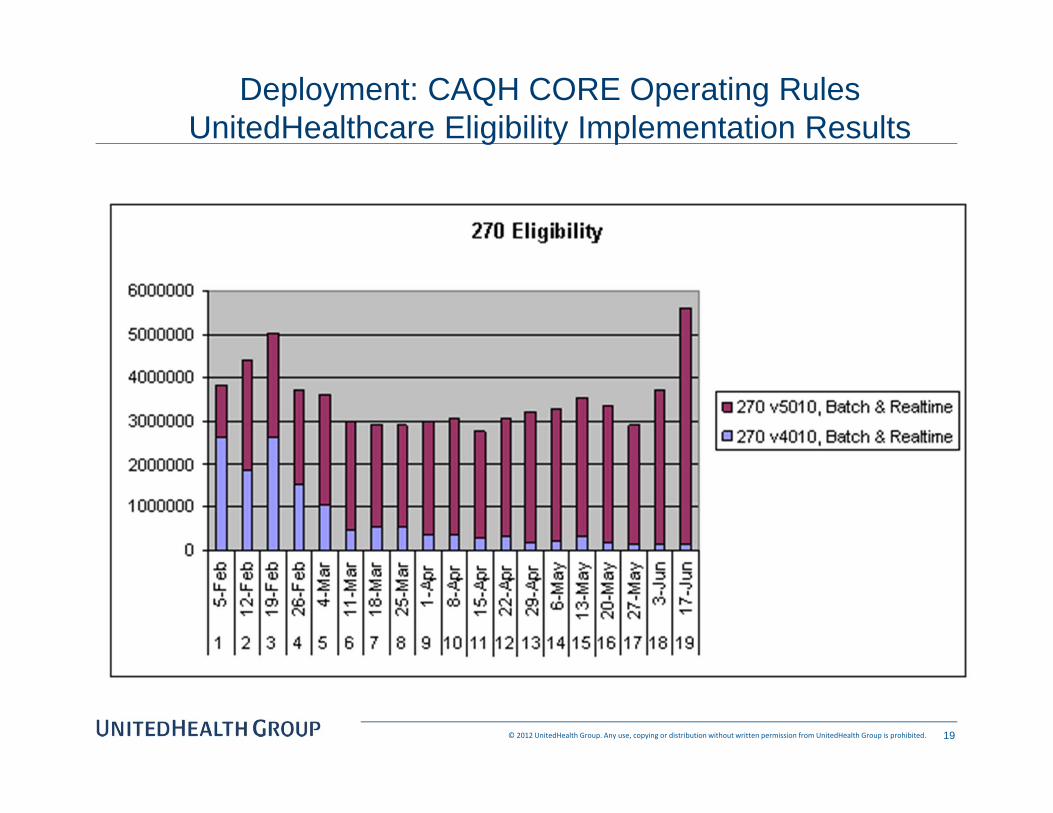
Deployment: CAQH CORE Operating RulesUnitedHealthcare Eligibility Implementation Results

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 20
Deployment: CAQH CORE Operating RulesUnitedHealthcare Claim Status Implementation Results

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 21
Deployment: CAQH CORE Operating RulesUnitedHealthcare Claim Status Implementation Results

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 22
System Monitoring5010 Volumes and Response Time
Total 4010 vs. 5010 Transaction Volumes and Response Time: B2B weekly report of 4010 vs. 5010 transaction types and volumes: Week of 06.11.12 - 06.17.12.
Overall transaction volume distribution v5010 = 93% - v4010 = 7%
June 17, 2012
Weekly Monitoring Seconds270 Batch 1.354270 Real Time 2.134276 Batch 1.456276 Real Time 2.186
4 Seconds per “hop” – 20 Seconds total

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 23
Adoption to Utilization
• What is nirvana?• The Shift • How do we shift Provider behavior
• Can we influence new Operating Rules development
• Are there alternative uses of the Transactions and Operating Rules that fit into the Provider’s workflow

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 24
100% AUTOMATION
Vision of Administrative Simplification
Pre-Service1. Patient uses mobile device to make appointment2. Insurance is verified in the Practice Management System (PMS)3. COB Information returned and updated in the PMS4. Expected Co-Pay for visit delivered to patient via email/text
Care Delivery1. Patient arrives – Insurance Re-Verified (via PMS)2. Patient Examined and visit documented in EMR
Referral/Prior Authorization required – Auto-generated from EMR to Payer
No additional services required – Encounter recorded via EMR and sent to Practice Management System and sent to Payer
Post-Service1. Patient checks out of office - Claim generated to payer
– 835 received and patient responsibility identified2. F/U appointment scheduled and emailed to patient3. Patient EOB received electronically clearly identifying
member responsibility and amount applied to patients FSA, etc.
As simple as 1 – 2 – 3

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 25
Industry Context: A Spectrum of Change
ClaimAdjudication
“277” Status Response
“834” Enrollment
“820” Premium PaymentSponsor
Provider
Charge CaptureClinical O/EUtilization Review
“278 “Referral Request
Billing“837” Claim/Encounter
“277” Request for Info
“275” Claim Attachment
A/Rand Treasury
“ 276” Status Inquiry
Health Plan Enrollment
“278” Referral ResponsePre-Adjudication
“270” Eligibility InquiryMembership
“271” Eligibility Response
“835” Remittance A/P
BankCCD+ (EFT)
© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 26
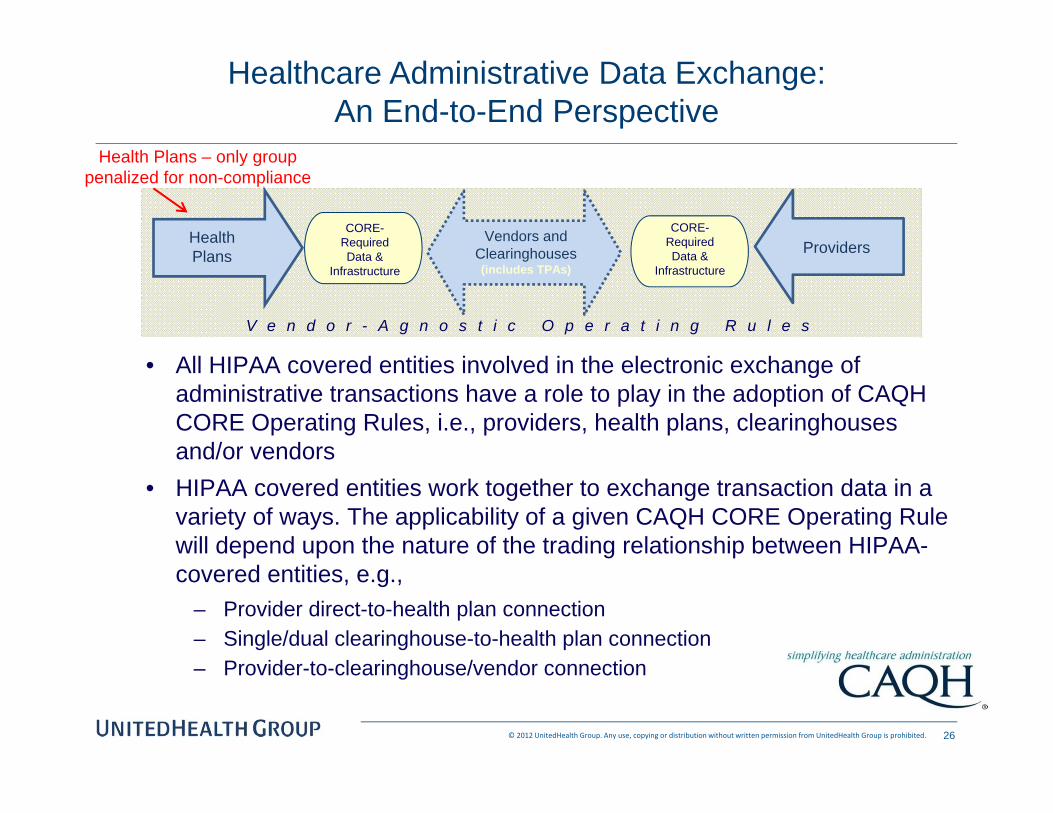
Healthcare Administrative Data Exchange: An End-to-End Perspective
CORE-RequiredData &
Infrastructure
V e n d o r - A g n o s t i c O p e r a t i n g R u l e s
ProvidersVendors and
Clearinghouses (includes TPAs)
CORE-RequiredData &
Infrastructure
HealthPlans
• All HIPAA covered entities involved in the electronic exchange of administrative transactions have a role to play in the adoption of CAQH CORE Operating Rules, i.e., providers, health plans, clearinghouses and/or vendors
• HIPAA covered entities work together to exchange transaction data in a variety of ways. The applicability of a given CAQH CORE Operating Rule will depend upon the nature of the trading relationship between HIPAA-covered entities, e.g.,
– Provider direct-to-health plan connection– Single/dual clearinghouse-to-health plan connection– Provider-to-clearinghouse/vendor connection
Health Plans – only group penalized for non-compliance

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 2727Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
27Confidential Property of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Patient MakesAppointment1
PMS/EMR(CH)
EDI, Phone, Portal, Fax
Verify Claim Status, Post Payment & ManageAccounts Receivable
Benefit & EligibilityVerification
Submit Pre-Auth/ Notification
Patient Arrives atAppointment
Patient Visit
Provider Enters Information intoPMS/EMR
PMS/EMR(CH)
EDI, Phone, Portal, Fax
EDI, Paper
Submit Pre-Auth / Referral/ Notification
Claim Submission
PMS/EMR(CH)
ED
I, P
aper
ED
I, P
hone
, Por
tal,
Fax
Rec
eive
Cla
imR
emitt
ance
Cla
im S
tatu
s, In
quiry
,&
Med
ical
Not
es
Contract Match Rate
Provider Contract Execution & Contract/Demographic Configuration Loaded Separately into Practice Mgmt System & UHC Systems
2 3
45
Scheduling / Registration Solutions1. Link provider network status to B&E verification
2. Clarify copay / deductible information
3. Provide clearer member product information on card
4. Simplify what is provided back in a 271 response
5. Link auth/referrals required to B&E verification
6. View network providers for scheduling purposes
Claim Resolution1. Better transparency on claim denials2. Ability to correct claims online3. Electronic attachments4. Tracking claim reconsiderations / appeals5. Downloadable Fee Schedule6. Consistency on recoupment process7. Lookup Policy / Authorization by code8. View list of claims denials and reasons
General Administrative Functions1. Customize portal views by specialty2. View provider letters / member forms online3. Chat capability versus phone
Touch Point ProjectFuture Opportunities – Voice of the Provider

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 28
Touch Point ProjectRelease 2: Scheduling / Registration Workflow
Patient MakesAppointment
Patient Arrives atAppointment
Objective: Build out an application to streamline the patient scheduling and registration process by matching provider and patient information to confirm eligibility and benefit coverage while ensuring authorizations are obtained prior to patient seeing the physician. The goal is to eliminate any calls a provider has to make prior to service being rendered.
Provider’s PMIS
Confirms Patient Eligibility / COB
Validates Provider Benefit Level
Validates Benefit Coverage
Determines if Auth is Required
Summarizes Product Information
Captures Patient Responsibility
Patient eligibility status and effective datesIdentify secondary coverage (COB) *
Provider’s network status with Patients plan *Determines patient’s out of pocket
Verifies coverage in general or at code levelCaptures patients lifetime / benefit max *
Determine if authorization is required *Auto links next steps to capture auth online
Identifies Patient’s plan / product informationVerifies if referral is required *Provide copy of patient’s ID card
Challenge: Providers work across multiple practice management systems that provide inconsistent tools to leverage EDI transactionspreventing providers to utilize this within their practice workflow.
UHC Systems
Prior authorizationrequests via online
Provider’s PMIS
OptumX Desktop
271
270
Ideal link betweenProvider’s PMISand OptumX Desktop
Workflow Tool
* Not provided through Core 5010 Transactions
Provider referralobtained
Goal: Simplify scheduling and registration process by capturing key information up front prior to patient arriving in the office to validate patient’s eligibility, services are covered, and financial responsibility
Did you know?Provider offices are 20% successful in collecting patient responsibility once a patient leaves the office.
© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 29Any use, copying or distribution without written permission from UnitedHealth Group is prohibited.
Monthly Transaction VolumesElectronic vs. Manual
Current Monthly Transaction Volumes:
270 Eligibility Inquiry – 12,342,000+
276 Claims Inquiry – 3,468,000+
Current Monthly Call Volumes:
Eligibility Inquiry – 691,000+
Claims Inquiry – 388,000+

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 30
Continuing the Push for Adoption and Utilization
• Recently deployed enhanced EDI reporting to provide additional visibility around who is using the transactions and who is not (and could benefit)
• Result will be targeted outreach toward “heavy hitters”
• We have seen a reduction in calls to date
• Exact reduction attributable to CAQH CORE certified transactions unclear (but enhanced EDI reporting will help confirm)
• Provider Relations organization continues to emphasize value and encourage utilization

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 31
Next Phase of Operating Rules – Can we get the next 30%
Cumulative IsolatedCurrent 32.21%Benefits ‐ Vendor #'s 35.21% 3.00%Benefits ‐ Notifications Req'd? 38.95% 2.62%Benefits ‐ Not Covered 41.20% 2.25%Benefits ‐ Spec Proc Code 58.05% 1.87%Benefits ‐ Pre‐X Timeframes 59.55% 1.50%Benefits ‐ Lifetime Max 62.17% 0.75%Benefits ‐ Referral Req'd 64.42% 0.75%
Current 23.97%All Additional Information Requests 35.62% 11.56%All Processing Details 52.05% 9.96%Check Information 58.90% 5.82%TAT 65.75% 3.08%Requested EOB 70.55% 1.37%
Call Obviation Potential
Benefits and Eligibility
Claim Status

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 32
UnitedHealth Group: Challenges Going Forward
“If you build it they will come.” May work in baseball, but not the case here…
• Provider Readiness/Willingness to Adopt• Providers are not as engaged as health plans
– THIS IS A RISK!• Practice Management Systems: Will vendors find value in supporting?
– Vendors are not HIPAA covered entities; clearinghouses are covered
• Expectation around HHS ACA-mandated certification and maintenance• Lack of consistent expectations across stakeholders • In many instances legislative language needs clarification• Given the non-compliance penalty for health plans, it is critical to establish achievable
dates for deployment• Clinical and Administrative data share the same challenges
• Periodic reviews • Is there a better approach than what is currently used; current process can be
cumbersome and lengthy• Health plans assume much risk & expense adopting when providers and vendors may not
be willing/capable of adopting

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 33
Phase III OR – ERA/EFT Enrollment Today
Distribution of Providers Paid by Health Plans
Cla
ims
Volu
me
per P
rovi
der
Low Claims Volume
High Claims Volume
Few Providers Many Providers
Current Level of EFT Adoption
• EFT adoption typically concentrated among select group of high claims volume providers.
• May represent more than ~50% of claims volume but only ~20% of providers in network.
• Typical national health plan pays claims to 250-300k providers (Tax ID level).
• Rate of enrollment for typical national health plan is ~1-2k providers per month.
EFT Adoption by Claims Volume and Provider Size

© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. 34© 2012 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited.
Timothy Kaja, MBA, [email protected]
Questions???