Embed Size (px)
Citation preview
9/21/15
1
S
EMDR as a Complement to Addiction Treatment
Updates & Insights
Jamie Marich, Ph.D., LPCC-‐S, LICDC-‐CS Director, Mindful Ohio
S
www.traumamadesimple.com/roadstorecovery2015
Jamie Marich, Ph.D., LPCC-‐S, LICDC-‐CS Director, Mindful Ohio

9/21/15
2
About Your Instructor
§ Humanitarian aid worker in post-war Bosnia & Hercegovina, 2000-2003 § Personal experience as an EMDR client § Certified Therapist, Approved Consultant and Education Provider by the
EMDR International Association § EMDRIA Research Award Winner in 2008 § Conducting EMDR sessions with appropriate clients since July 2006 § Multiple peer-reviewed publications and a book on the use of EMDR in
clinical settings § Author of EMDR Made Simple, Trauma Made Simple, & Trauma and the Twelve
Steps § Past volunteer for EMDR Humanitarian Assistance Programs § Reiki Master Teacher (RMT) § Creator of the Dancing Mindfulness Practice
Objectives
S Discuss the history of EMDR as a trauma intervention and briefly describe how it works
S Describe how EMDR can work as a relapse prevention/recovery enhancement measure
S Evaluate client appropriateness for EMDR and discuss logic for referral
S Evaluate professional readiness for formal training in EMDR
9/21/15
3
Disclaimer
Talking about issues of trauma, even in a professional setting, can be potentially triggering if you have experienced trauma yourself.
Please use your own discretion about staying in the lecture or participating in the group activity if you are feeling upset about your own issues.
S
EMDR?????
9/21/15
4
What Does EMDR Stand For?
§ Eye Movement Desensitization and Reprocessing
§ This name is actually a clinical misnomer, because it can be used with several forms of bilateral stimulation (BLS), not just eye movements
§ EMDR, according to founder Francine Shapiro, is more of a historical name, indicative of the therapy in its original form.
Shapiro compares it to Coca-Cola ©.
The “cocaine” was taken out in 1908, yet the name has still remained.
9/21/15
5
EMDR: The Story
S Developed serendipitously by California psychologist Francine Shapiro in 1987 during a “walk in the park”
S First study of her systematized protocol, EMD, published in 1989
S Switch to EMDR also made in 1989
S Other forms of BLS discovered and implemented in 1990
S EMDR is one of the most researched treatments for PTSD
S Dr. Shapiro currently considers EMDR to be a distinct approach to psychotherapy
EMDR: General Comments
Alan Moskovitz, M.D. (2001), a leading expert in treating borderline personality disorder has described EMDR as:
“An artful blend of several therapeutic techniques, including exposure therapy, cognitive therapy, and even an abbreviated form of the free association of psychoanalytic psychotherapy.”
9/21/15
6
EMDR is currently approved as a highly efficacious treatment for trauma by the:
§ American Psychiatric Association § American Psychological Association § Veterans Administration and the Department of the Defense
§ International Society of Traumatic Stress Studies § World Health Organization (2013 Practice Guidelines)
Bisson & Andrew (2007)
S Metanalysis of over 30 studies about PTSD over an 8 year period (1996-2004)
S Past-oriented PTSD treatments were far superior to coping skill only PTSD treatments
S Past-oriented or trauma-oriented treatments can include past-oriented cognitive behavioral therapy, exposure therapy, hypnosis, or EMDR
9/21/15
7
Benish, Imel, & Wampold (2008)
S A meta-analysis examining all studies on bona fide treatments for PTSD (e.g., desensitization, hypnotherapy, PD, TTP, EMDR, Stress Inoculation, Exposure, Cognitive, CBT, Present Centered, Prolonged exposure, TFT, Imaginal exposure) conducted between 1989-2007 found no statistical significance amongst the treatments (Benish, Impel, & Wampold, 2008).
World Health Organization (2013)
S Primary health care staff are also warned against certain popular treatments. For example, benzodiazepines, which are anti-anxiety drugs, should not be offered to reduce acute traumatic stress symptoms or sleep problems in the first month after a potentially traumatic event.
S Types of support offered can include psychological first aid, stress management and helping affected people to identify and strengthen positive coping methods and social supports.
S CBT and EMDR listed as two primary treatments of choice for referral following the psychological “first aid” stage
9/21/15
8
Trauma
Large-T and small-t
PTSD-qualifying and adverse life experiences
9/21/15
9
Etymological Origin
S Trauma comes from the Greek word meaning wound
An EMDR Client’s Perspective: Lily Burana (2009)
9/21/15
10
An EMDR Client’s Perspective: Lily Burana (2009)
“PTSD means, in ‘talking over beer’ terms, that you’ve got some crossed wires in your brain due to the traumatic event. The overload of stress makes your panic button touchier than most people’s, so certain things trigger a stress reaction- or more candidly- an over-reaction. Sometimes, the panic button gets stuck altogether and you’re in a state of constant alert, buzzing and twitchy and aggressive.”
An EMDR Client’s Perspective: Lily Burana (2009)
“Your amygdala- the instinctive flight, fight, or freeze part of your brain- reacts to a trigger before your rational mind can deter it. You can tell yourself,‘it’s okay,’ but your wily brain is already ten steps ahead of the game, registering danger and sounding the alarm. So you might say once again, in a calm, reasoned cognitive-behavioral-therapy kind of way, ‘Brain, it’s okay…’
9/21/15
11
An EMDR Client’s Perspective: Lily Burana (2009)
“But your brain yells back, ‘Bullshit kid, how dumb do you think I am? I’m not falling for that one again.’ By then, you’re hiding in the closet, hiding in a bottle, and/or hiding from life, crying, raging, or ignoring the phone and watching the counter on the answering machine go up, up, up, and up. You can’t relax, and you can’t concentrate because the demons are still pulling at your strings.”
An EMDR Client’s Perspective: Lily Burana (2009)
“The long-range result is that the peace of mind you deserve in the present is held hostage by the terror of your past.”
9/21/15
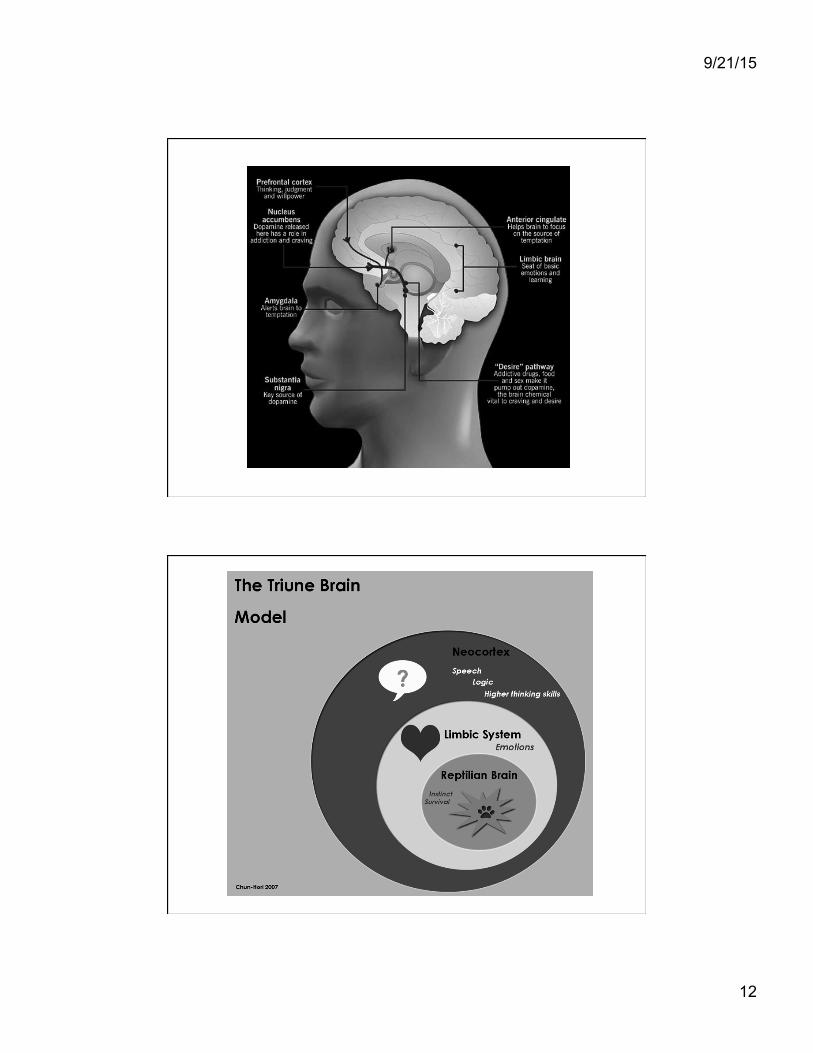
12
9/21/15
13
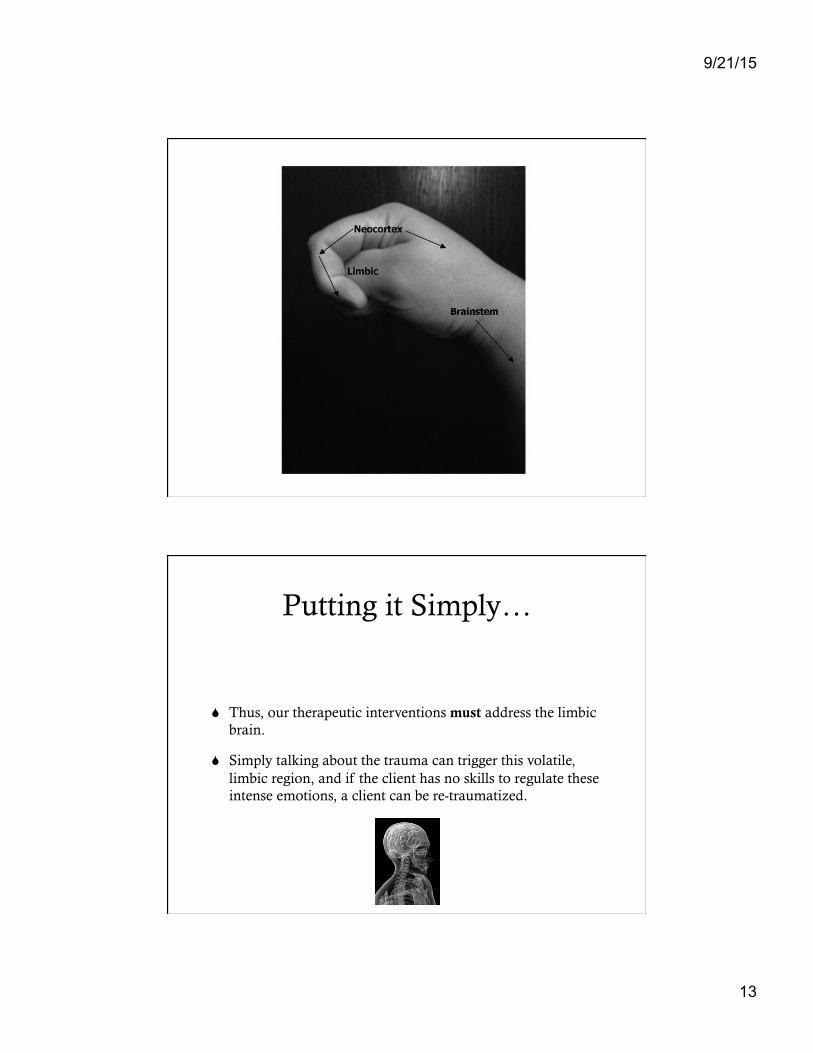
Putting it Simply…
S Thus, our therapeutic interventions must address the limbic brain.
S Simply talking about the trauma can trigger this volatile, limbic region, and if the client has no skills to regulate these intense emotions, a client can be re-traumatized.
9/21/15
14
Putting it Simply…
S What does not seem to change with traditional talk therapy is that uncomfortable experience of being triggered at a visceral level, (bottom of the brain) when the person is faced with reminiscent features of the original trauma in the present (Brown, 2003)
What does it mean to process something???
9/21/15
15
A Client’s Perspective: from Marich (2010)
Fadalia (pseudonym), a recovering heroin addict with complex trauma, reflected on where she was at before receiving the integrated treatment that led to her longest sobriety to date (3 years):
“Before [treatment], my feelings, thoughts and experiences were all tangled like a ball of yarn. I needed something to untangle them.”
è
9/21/15
16
EMDR Therapy (World Health Organization, 2013)
S Negative thoughts, feelings and behaviors are the result of unprocessed memories
S The treatment involves standardized procedures that include focusing simultaneously on:
u spontaneous associations of traumatic images, thoughts, emotions
and bodily sensations
u bilateral stimulation that is most commonly in the form of repeated eye movements.
So what is bilateral stimulation?
9/21/15
17
Primary Forms of Bilateral Stimulation Used in EMDR
S Eye movements (the original)
S Audio tones
S “Taps”/Tactile stimulation
- machine-generated or touch
- “Patty cake,” Butterfly Hug or Monkey Tap
- walking, drumming, dancing, other creative measures
Bilateral Stimulation
S Slow, short sets are used for client stabilization…similar to “driving slowly” through a pleasant scene
S Longer, faster sets are used for trauma processing and beyond…similar to “driving quickly” through a scary area
9/21/15
18
The EMDR Approach
§ EMDR does not bring up memories just for the sake of bringing them up.
§ The purpose of EMDR is to help people live a more adaptive
life.
The 3-Stage Consensus Model (ISTSS, 2012)
S Stabilization
• Building/Assuring a Strong Therapeutic Alliance
• Preparation
• Building Coping Skills
• Laying the Ground Work
S Processing of Traumatic Memories
S Reintegration Into Society
9/21/15
19
Eight Phases of EMDR (Shapiro, 2001)
1.) Client history
2.) Client preparation
3.) Assessment
4.) Desensitization
5.) Installation
6.) Body scan
7.) Closure
8.) Re-evaluation
STABILIZATION (RE)PROCESSING REINTEGRATION
Shapiro & Forrest (1997)
S EMDR is best implemented“as part of a system designed to make the client feel safe and supported. It works best when it is used in conjunction with counseling groups that provide a nurturing atmosphere, such as group therapy, Alcoholics Anonymous (AA), and Narcotics Anonymous (NA)” (p. 178).
9/21/15
20
EMDR as Organic Relapse Prevention Strategy
S Shapiro, Vogelmann-Sine, & Sine, 1994
S Henry, 1995
S Brown, 2003
S Zweben & Yeary, 2006
S Ricci, Shapiro, & Clayton, 2006; Ricci & Clayton, 2008
S Brown & Gilman, 2007
S Cox & Howard, 2007
S Marich, 2009 (a & b); 2010; 2011
EMDR as Organic Relapse Prevention Strategy
S Abel & O’Brien, 2010
S Tsoutsa, Fotopoulos, Zakynthinos, & Katsaounou, 2013
S Schweigerdt, 2014
S Jayatunge, 2014
S Meyer, 2014
9/21/15
21
Marich (2010)
S The thematic conclusions drawn from this study indicate that there is a place for EMDR as part of a comprehensive [addiction] recovery program when applied properly.
S EMDR experiences led to accessing of emotional core issues and shifting of perspectives that were relevant to lifestyle change
S The experiences of the women in the sample indicate that EMDR should not be used in isolation as a treatment intervention for addiction
Sasha
“I was a chronic relapser. And I think that was because, now that I have some awareness of a lot of that, I think it was because I didn’t get to none of my core issues… After I got to the core and knew what to identify with, that really helped me to look at me.”
9/21/15
22
Popky (2005)
S Developed an EMDR protocol for targeting addiction cravings, urges, or triggers called the Desensitization of Triggers and Urge Reprocessing (DeTUR)
S Solid theoretical components of the AIP with existing knowledge about addiction in the protocol; Popky’s protocol has been disseminated widely into the EMDR community despite lack of formal research validation
S For more info on DeTUR, see R. Shapiro (2005)
De TUR ® Basics
S Positive treatment goal:
Abstinence or controlled using is not a treatment goal, but the after product of a successful treatment plan (Popky, 2005)
The positive treatment goal is the focal point of the treatment plan. Such positive treatment goals should be:
stated in positive terms
time-related (not too distant future)
9/21/15
23
Hase (2006) Addiction Memory Protocol
S Incident: relapse (for example)
S Image: being in the grocery store ready to pick up the mouthwash
S Level of Urge (LOU): 10
S Negative Cognition: I am stupid.
S Positive cognition: I am making healthy choices
S VOC: 4
S Emotion: shame
S Body: core
Miller (2012): Feeling State Addictions Protocol (FSAP)
S The Feeling-State Addiction Protocol (FSAP), based on the feeling-state theory of behavioral and substance addiction, proposes that just as single-event traumas can become fixated with negative feelings, intensely positive events can become fixated with positive feelings. This fixated linkage between an event and a feeling is called a feeling-state (FS).
9/21/15
24
Miller (2012): Feeling State Addictions Protocol (FSAP)
1. Identify the exact behavior that has the most intense positive feeling.
2. Identify the exact feeling that underlies that behavior.
3. A modified form of EMDR is utilized to break the connection between the feeling and behavior.
4. The negative beliefs that underlie the compulsive fixation are processed.
Caution About These Protocols From a Traditional
Perspective
9/21/15
25
The Stages of Change:
An Addiction Field Classic
S Precontemplation
S Contemplation
S Preparation
S Action
S Maintenance
S Termination
SOURCES: Prochaska, Norcross, & DiClemente, 1994; Marich, 2011; Abel & O’Brien, 2011
Where a person is “at” in the stages of change is a useful guide for how deeply you can go with the EMDR.
Qualities of a Good EMDR Therapist Parnell (2007)
S Good clinical skills
S Ability to develop rapport with clients
S Comfort with trauma and intense affect
S Well-grounded
S Spacious
S Attuned to clients
9/21/15
26
Qualities of a Good EMDR Therapist Marich (2010/2012)
¡ caring ¡ trustworthy ¡ intuitive ¡ natural ¡ connected ¡ comfortable with trauma work ¡ skilled ¡ accommodating ¡ magical ¡ wonderful ¡ commonsensical ¡ validating ¡ gentle ¡ nurturing ¡ facilitating ¡ smart ¡ consoling
Butterfly Hug/Monkey Tap
9/21/15
27
Recommendations

9/21/15
28
Recommendations
Training Recommendations
9/21/15
29
References
Benish, S., Imel, Z., &Wampold, B. (2008). The relative efficacy of bona fide psychotherapies for treating posttraumatic stress disorder: A meta-analysis of direct comparisons. Clinical Psychology Review, 28,746-758. Bisson, J., & Andrew, M. (2007). Psychological treatment of post-traumatic stress disorder (PTSD). Cochrane Database of Systematic Reviews 2007, 3 Brown, S. (2003). The missing piece: The case for EMDR-based treatment for posttraumatic stress disorder and co-occurring substance use disorder. LifeForce Trauma Solutions. Retrieved June 4, 2008, from http://www.lifeforceservices.com/article_detail.php?recordid=5 Brown, S., & Gilman, S. (2007). Utilizing an integrated trauma treatment program (ITTP) in the Thurston County Drug Court program: Enhancing outcomes by integrating an evidence-based, phase trauma treatment program for posttraumatic stress disorder, trauma, and substance abuse. La Mesa, CA: Lifeforce Trauma Solutions. Cox, R.P., & Howard, M.D. (2007). Utilization of EMDR in the treatment of sexual addiction: A case study. Sexual Addiction & Compulsivity, 14, 1-20. Hase, M. (2006). Reprocessing of the addiction memory. Paper presented at the Annual EMDR International Conference. Philadelphia, PA. 9/2006. Hase, M., Schallmayer, S., & Sack, M. (2008). EMDR reprocessing of the addiction memory: Pretreatment, posttreatment, and 1-month follow-up. Journal of EMDR Practice and Research, 2 (3), 170–179.
References Henry, S.L. (1995). Pathological gambling: Etiologic considerations and treatment efficacy of eye movement desensitization/reprocessing. Journal of Gambling Studies, 12(4), 395-405. ISTSS: Cloitre, M., Courtois, C. A., Ford, J. D., Green, B. L., Alexander, P., Briere, J., … van der Hart, O. (2012). The ISTSS Expert Consensus Treatment Guidelines for Complex PTSD in Adults. . Retrieved from http://www.istss.org/AM/Template.cfm?Section=ISTSS_Complex_PTSD_Treatment_Guidelines&Template=/CM/ContentDisplay.cfm&ContentID=5185. Jayatunge, J. M. (2014, March). EMDR in the treatment of addiction. Lankaweb. Retrieved from http://www.lankaweb.com/news/items/2014/03/24/emdr-in-the-treatment-of-addictions. Marich, J. (2009a). EMDR in addiction continuing care: Case study of a cross-addicted female’s treatment and recovery. Journal of EMDR Practice and Research, 3(2), 98-106. Marich, J. (2009b). EMDR in addiction continuing care: A phenomenological study of women treated in early recovery. ProQuest Dissertations & Theses: Full Text. (UMI No. 3355347). Marich, J. (2010). EMDR in addiction continuing care: A phenomenological study of women in early recovery. Psychology of Addictive Behaviors, 24(3), 498-507. Marich, J. (2011). EMDR made simple: Four approaches to using EMDR with every client. Eau Claire, WI: Premiere Education & Media Marich, J. (2012). What makes a good EMDR therapist?: A phenomenological study of women in early recovery. Journal of Humanistic Psychology, 52(4), 401-422.
9/21/15
30
References
Meyer, J. L. (2014, May). EMDR for the co-occurring population. Counseling Today. Retrieved from http://ct.counseling.org/2014/05/emdr-for-the-co-occurring-population/ 6/23/2014. Miller, R. (2012). Treatment of behavioral addictions utilizing the feeling-state addiction protocol: A multiple baseline study. Journal of EMDR Practice and Research, 6(4), 159-169. Moskovitz, A. (2001). Lost in the mirror: An inside look at borderline personality disorder. (2nd ed.) Latham, MD: Taylor Trade Publishing. Parnell, L. (2007). A therapist’s guide to EMDR: Tools and techniques for successful treatment. New York: W.W. Norton. Parnell, L. (2008). Tapping in: A step-by-step guide to activating your healing resources through bilateral stimulation. Louisville, CO: Sounds True Books. Popky, A.J. (2005). DeTUR, an urge reduction protocol for addictions and dysfunctional behaviors. In R. Shapiro (Ed.), EMDR solutions: Pathways to healing (pp. 167-188). New York: Norton. Prochaska, J., Norcross, J., & DiClemente, C. (1994). Changing for good: The revolutionary program that explains the six stages of change and teaches you how to free yourself from bad habits. New York: William Morrow. Schweigerdt, B. (2014, February). Using eye movement desensitization and reprocessing (EMDR) as a therapeutic intervention for sex addicts. Available from Proquest Dissertations and Theses database. (UMI. No. 1539782).
References
Shapiro, F. (2001). Eye Movement Desensitization and Reprocessing: Basic principles, protocols, and procedures. (2nd ed.). New York: The Guilford Press. Shapiro, F. & Solomon, R. (2008). EMDR and the adaptive information processing model: Potential mechanisms of change. Journal of EMDR Practice and Research, 2(4), 315-325. Shapiro, F. (2012). Getting past your past. Emmaus, PA: Rodale Books. Shapiro, F. & Forrest, M. (1997). EMDR: The breakthrough “eye movement” therapy for overcoming stress, anxiety, and trauma. New York: Basic Books. Shapiro, F., Vogelmann-Sine, S., & Sine, L. (1994). Eye movement desensitization and reprocessing: Treating trauma and substance abuse. Journal of Psychoactive Drugs, 26(4), 379-391. Tsoutsa, A., Fotopoulos, D., Zakynthinos, S., & Katsaounou, P. (2013, December). Treatment of tobacco addiction using the feeling-state addiction protocol (FSAP) of the eye movement desensitization and reprocessing (EMDR) treatment. Tobacco Induced Diseases, 12(Supplement 1), A25. World Health Organization. (2013). Assessment and management of conditions specifically related to stress mhGAP Intervention Guide Module. Geneva, Switzerland: Author. Available at: http://apps.who.int/iris/bitstream/10665/85623/1/9789241505932_eng.pdf?ua=1 Zweben, J., & Yeary, J. (2006). EMDR in the Treatment of Addiction. Journal of Chemical Dependency Treatment, 8(2), 115-127.
9/21/15
31
To contact today’s presenter: Jamie Marich, Ph.D. Mindful Ohio [email protected] www.jamiemarich.com www.drjamiemarich.com www.mindfulohio.com www.dancingmindfulness.com www.TraumaTwelve.com www.TraumaMadeSimple.com Phone: 330-881-2944