Embed Size (px)
DESCRIPTION
Emergency Medicine Pearls. Steven M. Hochman, MD FACEP Dept of Emergency Medicine St. Joseph’s Regional Med Center October 28, 2009. Disclaimer. - PowerPoint PPT Presentation
Citation preview

Emergency Medicine Emergency Medicine PearlsPearls
Steven M. Hochman, MD FACEPSteven M. Hochman, MD FACEPDept of Emergency MedicineDept of Emergency Medicine
St. Joseph’s Regional Med CenterSt. Joseph’s Regional Med CenterOctober 28, 2009October 28, 2009

DisclaimerDisclaimer Any similarity between the information in this Any similarity between the information in this
lecture and any material published by the lecture and any material published by the American Board of Osteopathic Emergency American Board of Osteopathic Emergency Medicine is entirely coincidentalMedicine is entirely coincidental
Emergency medicine is in the public domain, Emergency medicine is in the public domain, and the dissemination of accurate, relevant and and the dissemination of accurate, relevant and up-to-date information about the evaluation and up-to-date information about the evaluation and care of emergency patients is in the best care of emergency patients is in the best interests of the medical community as well as interests of the medical community as well as the general publicthe general public

Part IPart IMnemonic ManiaMnemonic Mania

Altered Mental Status DDxAltered Mental Status DDx
Alcohol, other drugsAlcohol, other drugs AA Endo/exocrine, electrolytesEndo/exocrine, electrolytes EE Insulin (DM)Insulin (DM) II Oxygen (low), opiatesOxygen (low), opiates OO UremiaUremia UU Trauma, temperatureTrauma, temperature TT InfectionInfection II PsychiatricPsychiatric PP Space occupying lesions, stroke, shockSpace occupying lesions, stroke, shock SS

Substances Removed by HDSubstances Removed by HD
IsopropanolIsopropanol IISalicylatesSalicylates SSTheophyllineTheophylline TTUremiaUremia UUMethanolMethanol MMBarbsBarbs BBLithiumLithium LLEthylene glycol, ethanolEthylene glycol, ethanol EE

Cholinergic ToxidromeCholinergic Toxidrome(Muscarinic)(Muscarinic)
DiarrheaDiarrhea DDUrinationUrination UUMiosisMiosis MMBronchorrheaBronchorrhea BBBradycardiaBradycardia BBEmesisEmesis EELacrimationLacrimation LLSalivationSalivation SS

+AG Metabolic Acidosis+AG Metabolic Acidosis CO, CyanideCO, Cyanide CC AKAAKA AA TolueneToluene TT MethanolMethanol MM UremiaUremia UU DKADKA DD Paraldehyde, PhenphorminParaldehyde, Phenphormin PP INH, IronINH, Iron II Lactic AcidosisLactic Acidosis LL Ethylene glycolEthylene glycol EE SalicylatesSalicylates SS

(-)AG Metabolic Acidosis(-)AG Metabolic Acidosis
HyperalimentationHyperalimentation HHAcetazolamide, AmphoteracinAcetazolamide, Amphoteracin AARTARTA RRDiarrheaDiarrhea DDUreteral diversionsUreteral diversions UUPancreatic fistulasPancreatic fistulas PPSaline resuscitationSaline resuscitation SS

Elevated Osmolar GapElevated Osmolar Gap
MethanolMethanol MMEthanol, Ethylene GlycolEthanol, Ethylene Glycol EEDiuretics (glyc, mann, sorb)Diuretics (glyc, mann, sorb) DD IsopropanolIsopropanol II

Toxic Alcohols etc.Toxic Alcohols etc.
+AG+AG +OG+OG +Ketones+Ketones
EthanolEthanol -- ++ --
Eth GlycolEth Glycol ++ ++ --
IsopropylIsopropyl -- ++ ++
MethanolMethanol ++ ++++ --
ASAASA ++ - (slight)- (slight) ++

Serum OsmolaritySerum OsmolaritySSosmosm = 2 Na + BUN/2.8 + = 2 Na + BUN/2.8 +
Gluc/18 + Ethanol/4.6Gluc/18 + Ethanol/4.6Nl = 285 meq/LNl = 285 meq/L

Toxics Induced SeizuresToxics Induced Seizures(OTIS CAMPBELL)(OTIS CAMPBELL)
Oral hypoglycemics, organophosphates, Oral hypoglycemics, organophosphates, opiatesopiates
Theophylline, TCA’sTheophylline, TCA’s INH, insulinINH, insulinSalicylates, sympathomimeticsSalicylates, sympathomimeticsCamphor, CO, cocaine, cyanideCamphor, CO, cocaine, cyanideAmphetamines, anticholinergics, Amphetamines, anticholinergics,
antihistaminesantihistamines

Toxics Induced SeizuresToxics Induced Seizures(OTIS CAMPBELL)(OTIS CAMPBELL)
Methylxanthines, mushrooms (gyromitra)Methylxanthines, mushrooms (gyromitra)PCP, paraldehyde, plants (jimson, PCP, paraldehyde, plants (jimson,
belladonna alkaloids, water hemlock)belladonna alkaloids, water hemlock)B Blockers (propranolol), benzo/barb B Blockers (propranolol), benzo/barb
withdrawalwithdrawalEthanol withdrawalEthanol withdrawalLi, LidocaineLi, LidocaineLead, Lindane, LSDLead, Lindane, LSD

Abdominal Flat PlateAbdominal Flat Plate(CHIPES)(CHIPES)
Chloral HydrateChloral Hydrate CCHeavy Metals (Fe, Pb)Heavy Metals (Fe, Pb) HH IodineIodine IIPhenothiazines, Packets (cocainePhenothiazines, Packets (cocaine PP
heroine)heroine)Enteric-coated productsEnteric-coated products EESolventsSolvents SS

Substances Not Bound to ACSubstances Not Bound to AC
CausticsCaustics CCLithiumLithium LL IronIron IIMethanol, MetalsMethanol, Metals MMEthylene glycol, other alcoholsEthylene glycol, other alcohols EE

Multiple Dose ACMultiple Dose AC
TCA’sTCA’s TTTheophyllineTheophylline TTBarbiTuraTesBarbiTuraTes TTTegretolTegretol TTPhenyToinPhenyToin TTDigiTalisDigiTalis TTASA??ASA??

Whole Bowel IrrigationWhole Bowel Irrigation(PEG, 2L/hr, effluent clear)(PEG, 2L/hr, effluent clear)
Fe, heavy metalsFe, heavy metalsLithiumLithiumSustained release, enteric-coatedSustained release, enteric-coatedBody packers/stuffersBody packers/stuffersForeign bodies (batteries)Foreign bodies (batteries)

Sick of this yet??Sick of this yet??

More ToxicologyMore Toxicology

Carbon Monoxide PoisoningCarbon Monoxide Poisoning
Fires, propane, home heating (kerosine), Fires, propane, home heating (kerosine), engine exhaust (rare)engine exhaust (rare)
Extremes of age, pregnancy (FETUS), Extremes of age, pregnancy (FETUS), CAD/pulmonary diseaseCAD/pulmonary disease
CNS and CV systems most affectedCNS and CV systems most affectedCOHb level—Nl 1-2%, smokers 5-10%COHb level—Nl 1-2%, smokers 5-10%Levels correspond poorly to SxLevels correspond poorly to Sx

CO TreatmentCO Treatment
EliminationEliminationRoom air 21%Room air 21% 2-7 hrs (mean 4 hrs)2-7 hrs (mean 4 hrs)100% 1 Atm100% 1 Atm 90 min90 min100% 3 Atm100% 3 Atm 23 min23 min
HBO—indicationsHBO—indicationsEnd organ damage—LOC, coma, Sz, End organ damage—LOC, coma, Sz,
persistent Sxpersistent SxCoHb >25% or >15% in pregnancyCoHb >25% or >15% in pregnancyAbnl neuro exam, dysrhythmia, poor SaO2Abnl neuro exam, dysrhythmia, poor SaO2

Gastric LavageGastric Lavage
Ingestions potentially fatal or worsoning Ingestions potentially fatal or worsoning vital signs or MSvital signs or MS
TCA’s, CCB’s, LiTCA’s, CCB’s, LiPreferably within 1 hourPreferably within 1 hourProtect airway, L lateral decub positionProtect airway, L lateral decub positionAdults 36-40 French, Peds 22-24+ FrenchAdults 36-40 French, Peds 22-24+ French

Gastric LavageGastric Lavage
ContraindicationsContraindications Caustic ingestionsCaustic ingestions Large FB’s, sharp objectsLarge FB’s, sharp objects Inability to protect airwayInability to protect airway Drug not accessible in stomachDrug not accessible in stomach
ComplicationsComplications AspirationAspiration PerforationPerforation Tension PTX, empyemaTension PTX, empyema Impaired oxygenation/ventilationImpaired oxygenation/ventilation

Acetaminophen OverdoseAcetaminophen Overdose
Rule of 140’sRule of 140’s

Acetaminophen OverdoseAcetaminophen Overdose
Rule of 140Rule of 140Toxic dose 140 mg/kg Toxic dose 140 mg/kg 70 kg = 9.8 gms = 20 ES Tylenol70 kg = 9.8 gms = 20 ES Tylenol

Acetaminophen OverdoseAcetaminophen Overdose
Rule of 140Rule of 140Toxic level 140 mcg/ml (really 150) at 4 Toxic level 140 mcg/ml (really 150) at 4
hourshoursRumack-Matthew nomogram, single Rumack-Matthew nomogram, single
ingestion at known timeingestion at known time

Acetaminophen OverdoseAcetaminophen Overdose
Rule of 140Rule of 140Initial dose NAC 140 mg/kg poInitial dose NAC 140 mg/kg poThen 70 mg/kg q 4hrs X 17 dosesThen 70 mg/kg q 4hrs X 17 dosesOff label: 100 mg IV X3 doses over 20 Off label: 100 mg IV X3 doses over 20
hrshrs

Acetaminophen OverdoseAcetaminophen Overdose
Rule of 140Rule of 140Alternative: Acetadote 150 mg/kg IV Alternative: Acetadote 150 mg/kg IV
over 1 hour over 1 hour 2 more doses over next 20 hrs2 more doses over next 20 hrs

Acetaminophen OverdoseAcetaminophen Overdose
APAP, ASA level on all suicide attempt ptsAPAP, ASA level on all suicide attempt pts1/500 +tox level APAP without h/o APAP 1/500 +tox level APAP without h/o APAP
ingestioningestionGive AC to all; NAC if indicated (within Give AC to all; NAC if indicated (within
8hrs)8hrs)Potential toxic ingestionPotential toxic ingestionLate presentation, ongoing toxicityLate presentation, ongoing toxicityChronic overdose, ongoing toxicityChronic overdose, ongoing toxicity
Gastric lavage – only for coingestantsGastric lavage – only for coingestants

Acetaminophen OverdoseAcetaminophen Overdose
If potential toxicityIf potential toxicityLFT’s (AST, INR, Biliruben)LFT’s (AST, INR, Biliruben)Electrolytes, renal function studiesElectrolytes, renal function studies
New IV formulation: AcetadoteNew IV formulation: Acetadote21 hr protocol21 hr protocolCan use oral form IV ($18 vs. $416) – no Can use oral form IV ($18 vs. $416) – no
good datagood data

TCA OverdoseTCA Overdose -yline and -amine (nortriptyline,imipramine)-yline and -amine (nortriptyline,imipramine) Amitriptyline (Elavil)Amitriptyline (Elavil) Block reuptake of NE, DA, Seratonin at central Block reuptake of NE, DA, Seratonin at central
synapsessynapses ↑↑Catecholamines – initial HTNCatecholamines – initial HTN Anticholinergic – hot, dry, agitatedAnticholinergic – hot, dry, agitated Na Channel blockade – negative inotropyNa Channel blockade – negative inotropy Alpha blockade -- hypotensionAlpha blockade -- hypotension Antihistamine effects – sedationAntihistamine effects – sedation GABA antagonism -- seizuresGABA antagonism -- seizures

TCA OverdoseTCA Overdose
Na channel blockade - Type 1A Na channel blockade - Type 1A antiarrhythmic (quinidine-like) effectsantiarrhythmic (quinidine-like) effects
Prolonged Phase 0 depolarization Prolonged Phase 0 depolarization QRS QRS widening widening
EKG: Wide complex dysrhythmiasEKG: Wide complex dysrhythmiasSinus tachycardiaSinus tachycardiaTerminal 40 ms R axis deviation (Big R in Terminal 40 ms R axis deviation (Big R in
aVR and Big S in aVL)aVR and Big S in aVL)

TCA OverdoseTCA Overdose
EKG as screening toolEKG as screening toolQRS <100 ms – no significant toxicityQRS <100 ms – no significant toxicityQRS >100 ms – 1/3 had seizuresQRS >100 ms – 1/3 had seizuresQRS >160 ms – ½ had ventricular QRS >160 ms – ½ had ventricular
dysrhythmiasdysrhythmias

TCA OverdoseTCA Overdose
TreatmentTreatmentOrogastric lavage if timelyOrogastric lavage if timelyAC 1 gm/kgAC 1 gm/kgMDAC ½ dose q2 hrs X1-2MDAC ½ dose q2 hrs X1-2Ativan, Valium for seizuresAtivan, Valium for seizuresNaHCO3 for dysrhythmias – 1-2 amps (Peds: NaHCO3 for dysrhythmias – 1-2 amps (Peds:
1-2 mEq/kg), repeat EKG1-2 mEq/kg), repeat EKGHyperventilation (serum pH goal 7.45-7.55)Hyperventilation (serum pH goal 7.45-7.55) IVF, pressors for hypotensionIVF, pressors for hypotension

TCA OverdoseTCA Overdose
DispositionDisposition6 hour observation – no anticholinergic signs 6 hour observation – no anticholinergic signs
or seizures, nl MS and EKG, no Tx other than or seizures, nl MS and EKG, no Tx other than AC AC DISCHARGE DISCHARGE
Admit forAdmit forQRS ≥ 100 msQRS ≥ 100 msSeizure, dysrhythmia, MS changesSeizure, dysrhythmia, MS changesECG abnormalities ECG abnormalities MICU, bicarb tx X 12-24 hrs MICU, bicarb tx X 12-24 hrs

Zebras & Other Zebras & Other MinutiaeMinutiae

What’s the Diagnosis?What’s the Diagnosis?
28 yo male, painful joints, discharge from 28 yo male, painful joints, discharge from eyes, burning on urinationeyes, burning on urination

Reiter’s SyndromeReiter’s Syndrome
Triad: Arthritis, Urethritis , ConjunctivitisTriad: Arthritis, Urethritis , ConjunctivitisSpondyloarthropathy, reactive arthritisSpondyloarthropathy, reactive arthritisMechanism unclear – post infect, AI?Mechanism unclear – post infect, AI?Leading cause inflam arthritis, young menLeading cause inflam arthritis, young menDx: cervical/urethr swab (**Chlamydia), Dx: cervical/urethr swab (**Chlamydia),
arthrocentesis, CBC/D, ESRarthrocentesis, CBC/D, ESRTx: NSAIDs, sulfasalazine, Tx Tx: NSAIDs, sulfasalazine, Tx
cervicitis/urethritis; f/u Rheumatologycervicitis/urethritis; f/u Rheumatology

What’s the Diagnosis?What’s the Diagnosis?
45 yo white female45 yo white femaleRecurrent episodes of Recurrent episodes of
Eye pain, visual blurrinessEye pain, visual blurrinessRLE weakness RLE weakness UE paresthesiasUE paresthesias
Episodes last up to several hours, with Episodes last up to several hours, with incomplete resolutionincomplete resolution
Symptoms progressively worse over Symptoms progressively worse over monthsmonths

Multiple SclerosisMultiple Sclerosis
Myelin sheath destruction, ?causeMyelin sheath destruction, ?causeMost commonly periventricular white Most commonly periventricular white
mattermatterClinical Dx: 2+ episodes of neurological Clinical Dx: 2+ episodes of neurological
deficiencydeficiencyObjective clinical signs >1 CNS lesionObjective clinical signs >1 CNS lesionManagement: Refer to NeuroManagement: Refer to Neuro
MRI – periventricular plaquesMRI – periventricular plaques

Multiple Sclerosis – S&SMultiple Sclerosis – S&S
INO – deficiencies of abduct/adductionINO – deficiencies of abduct/adductionOptic neuritis – pain, visual impairmentOptic neuritis – pain, visual impairmentTransverse myelitis – spinal cord syndTransverse myelitis – spinal cord syndDiplopiaDiplopiaAtaxia, intention tremorAtaxia, intention tremorUMN signs – weakness, hyperreflex, UMN signs – weakness, hyperreflex,
Babinski’s signsBabinski’s signs

Multiple Sclerosis – S&SMultiple Sclerosis – S&S
Post column, spinothalamic involvementPost column, spinothalamic involvementUrinary Sx, constipation, sexual Urinary Sx, constipation, sexual
dysfunctiondysfunctionLhermitte’s sign – electric shock on flexion Lhermitte’s sign – electric shock on flexion
of neckof neck

What’s the Diagnosis?What’s the Diagnosis?
48 yo male, h/o lumbar disc disease48 yo male, h/o lumbar disc diseaseLower back pain, radiating down posterior Lower back pain, radiating down posterior
thighsthighsUrinary incontinenceUrinary incontinenceB/L numbness of feetB/L numbness of feetProgressive difficulty ambulatingProgressive difficulty ambulatingSx started 2 hours ago Sx started 2 hours ago

Cauda Equina SyndromeCauda Equina Syndrome
Compression of lumbar-sacral nerve rootsCompression of lumbar-sacral nerve rootsBelow conus medularis (L1-L2)Below conus medularis (L1-L2)
Disc herniation most common causeDisc herniation most common causeAlso: trauma, mass effect from tumor, Also: trauma, mass effect from tumor,
abscessabscess

Cauda Equina SyndromeCauda Equina SyndromePhysical ExamPhysical Exam
Bladder or rectal dysfunction – retention or Bladder or rectal dysfunction – retention or incontenenceincontenence
LE sensory/motor deficitsLE sensory/motor deficitsFoot dorsiflexion (L5-S1), quadriceps, DTR’sFoot dorsiflexion (L5-S1), quadriceps, DTR’s
Perineal sensation – saddle anesthesiaPerineal sensation – saddle anesthesiaReduced rectal tone (S3-4-5)Reduced rectal tone (S3-4-5)Absent anal winkAbsent anal winkStraight leg raise – sciaticaStraight leg raise – sciatica

Cauda Equina SyndromeCauda Equina SyndromeManagementManagement
Emergent MRI – Confirm Dx and levelsEmergent MRI – Confirm Dx and levelsBut do not delay treatmentBut do not delay treatment
Immediate Neurosurgery ConsultImmediate Neurosurgery ConsultMethylprednisolone 30+5.4 for traumaMethylprednisolone 30+5.4 for traumaEmergent decompression – improves Emergent decompression – improves
outcomesoutcomes6-24 hours – controversy6-24 hours – controversy>48 hours, ?still benefit>48 hours, ?still benefit

Optho Emergencies Optho Emergencies I-XI-X

Opthalmology IOpthalmology I
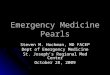
Teardrop-shaped pupil, pt felt something Teardrop-shaped pupil, pt felt something hit his eye while mowing lawnhit his eye while mowing lawn

Opthalmology IOpthalmology I
Teardrop-shaped pupil, pt felt something Teardrop-shaped pupil, pt felt something hit his eye while mowing lawnhit his eye while mowing lawn
ORBITAL RUPTUREORBITAL RUPTURE

Opthalmology IOpthalmology I
Teardrop-shaped pupil, pt felt something Teardrop-shaped pupil, pt felt something hit his eye while mowing lawnhit his eye while mowing lawn
ORBITAL RUPTUREORBITAL RUPTURE+Seidel test, NO TONOMETRY+Seidel test, NO TONOMETRYTX: Eye shield (not patch), keep pt still, TX: Eye shield (not patch), keep pt still,
ABXABXEmergent Optho consultEmergent Optho consult

Opthalmology IIOpthalmology II
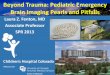
Sudden painless monocular vision lossSudden painless monocular vision lossPE: Afferent pupil defectPE: Afferent pupil defectFundoscopic: pale retina, cherry red spot Fundoscopic: pale retina, cherry red spot
at foveaat fovea

Opthalmology IIOpthalmology II
Sudden painless monocular vision lossSudden painless monocular vision lossPE: Afferent pupil defectPE: Afferent pupil defectFundoscopic: pale retina, cherry red spot Fundoscopic: pale retina, cherry red spot
at foveaat foveaCENTRAL RETINAL ARTERY CENTRAL RETINAL ARTERY
OCCLUSIONOCCLUSIONTX: Intermittant digital massageTX: Intermittant digital massageOPTHO CONSULT (paracentesis of OPTHO CONSULT (paracentesis of
anterior chamber) anterior chamber)

Opthalmology IIIOpthalmology III
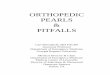
Sudden painless monocular vision lossSudden painless monocular vision lossLess severe than last caseLess severe than last caseFund: Blood and thunder retina (retinal Fund: Blood and thunder retina (retinal
hemorrhages, tortuous retinal veins)hemorrhages, tortuous retinal veins)

Opthalmology IIIOpthalmology III
Sudden painless monocular vision lossSudden painless monocular vision lossLess severe than last caseLess severe than last caseBlood and thunder retina (retinal Blood and thunder retina (retinal
hemorrhages, tortuous retinal veins)hemorrhages, tortuous retinal veins)CENTRAL RETINAL VEIN OCCLUSIONCENTRAL RETINAL VEIN OCCLUSIONRF’s: DM, HTN, hyperviscosityRF’s: DM, HTN, hyperviscosityRefer to Optho – confirm Dx and monitor Refer to Optho – confirm Dx and monitor
complications; Tx: most ineffectivecomplications; Tx: most ineffective

Opthalmology IVOpthalmology IV
Pt entered movie theater, then c/o eye Pt entered movie theater, then c/o eye pain, N/V, blurred vision, “halos” around pain, N/V, blurred vision, “halos” around lightslights
PE: Fixed, mid-dilated NR pupil, scleral PE: Fixed, mid-dilated NR pupil, scleral injection, injection, hazy corneahazy cornea

Opthalmology IVOpthalmology IV
Pt entered movie theater, then c/o eye Pt entered movie theater, then c/o eye pain, N/V, blurred vision, “halos” around pain, N/V, blurred vision, “halos” around lightslights
Fixed, mid-dilated NR pupil, scleral Fixed, mid-dilated NR pupil, scleral injection, hazy corneainjection, hazy cornea
ACUTE NARROW ANGLE GLAUCOMAACUTE NARROW ANGLE GLAUCOMA

Opthalmology IVOpthalmology IV
ACUTE NARROW ANGLE GLAUCOMAACUTE NARROW ANGLE GLAUCOMAShallow ant chamber, iris sits too tightly on Shallow ant chamber, iris sits too tightly on
lenslensResistance of flow of aquaeous humor, Resistance of flow of aquaeous humor,
elevated IOP (>40)elevated IOP (>40)Farsighted elderly womenFarsighted elderly women

Opthalmology IVOpthalmology IV
TREATMENT:TREATMENT: Acetazolamide, Beta blockers (timolol) Acetazolamide, Beta blockers (timolol)
(decrease production)(decrease production) Cholinergics (pilocarpine) (increase flow)Cholinergics (pilocarpine) (increase flow) Depress head (separates lens + iris)Depress head (separates lens + iris) E-F-Glycerol, Mannitol (hyperosmotics)E-F-Glycerol, Mannitol (hyperosmotics) Steroids (topical prednisolone) (antiinflamm)Steroids (topical prednisolone) (antiinflamm) EMERGENCY OPTHO CONSULTEMERGENCY OPTHO CONSULT

Opthalmology VOpthalmology V
Painful monocular central vision lossPainful monocular central vision lossPreservation of peripheral visionPreservation of peripheral visionPE: APD, +/- disc swellingPE: APD, +/- disc swelling

Opthalmology VOpthalmology V
Painful monocular central vision lossPainful monocular central vision lossPreservation of peripheral visionPreservation of peripheral visionPE: APD, +/- disc swellingPE: APD, +/- disc swellingOPTIC NEURITISOPTIC NEURITISAssociated with MS, Lyme, Neurosyphilis, Associated with MS, Lyme, Neurosyphilis,
Lupus, Sarcoid, ETOH, toxinsLupus, Sarcoid, ETOH, toxinsOPTHO consult, IV steroids OPTHO consult, IV steroids
(methylprednisolone)(methylprednisolone)

Opthalmology VIOpthalmology VI
Neonate, sticky discharge, conjunctival Neonate, sticky discharge, conjunctival inflammationinflammation
6-8 hrs after birth6-8 hrs after birth

Opthalmology VIOpthalmology VI
Neonate, sticky eye discharge, Neonate, sticky eye discharge, conjunctival inflammationconjunctival inflammation
6-8 hrs after birth6-8 hrs after birthCHEMICAL CONJUNCTIVITISCHEMICAL CONJUNCTIVITIS

Opthalmology VIOpthalmology VI
Neonate, sticky discharge, conjunctival Neonate, sticky discharge, conjunctival inflammationinflammation
6-8 hrs after birth6-8 hrs after birthCHEMICAL CONJUNCTIVITISCHEMICAL CONJUNCTIVITISTX: AgNO3, resolves 24-48 hrsTX: AgNO3, resolves 24-48 hrs

Opthalmology VIIOpthalmology VII
Neonate, sticky, Neonate, sticky, purulentpurulent discharge, discharge, conjunctival inflammationconjunctival inflammation
2-5 days after birth2-5 days after birth

Opthalmology VIIOpthalmology VII
Neonate, sticky Neonate, sticky purulentpurulent discharge, discharge, conjunctival inflammationconjunctival inflammation
2-5 days after birth2-5 days after birthGONONORRHEAL CONJUNCTIVITISGONONORRHEAL CONJUNCTIVITISAggressive, can ulcerate/perforate cornea Aggressive, can ulcerate/perforate cornea
in hrs/daysin hrs/days

Opthalmology VIIOpthalmology VII
Neonate, sticky Neonate, sticky purulentpurulent discharge, discharge, conjunctival inflammationconjunctival inflammation
2-5 days after birth2-5 days after birthGONONORRHEAL CONJUNCTIVITISGONONORRHEAL CONJUNCTIVITISAggressive, can ulcerate/perforate cornea Aggressive, can ulcerate/perforate cornea
in hrs/daysin hrs/daysTX: Topical erythro, IV ceftriaxone, TX: Topical erythro, IV ceftriaxone,
irrigationirrigationOptho consultOptho consult

Opthalmology VIIIOpthalmology VIII
Neonate, sticky discharge, conjunctival Neonate, sticky discharge, conjunctival inflammationinflammation
5-14 days after birth5-14 days after birth

Opthalmology VIIIOpthalmology VIII
Neonate, sticky discharge, conjunctival Neonate, sticky discharge, conjunctival inflammationinflammation
5-14 days after birth5-14 days after birthCHLAMYDIA CONJUNCTIVITISCHLAMYDIA CONJUNCTIVITISLeading cause of preventable blindness Leading cause of preventable blindness
worldwideworldwideMost common of last three; assoc Most common of last three; assoc
nasopharyngitisnasopharyngitis

Opthalmology VIIIOpthalmology VIII
Neonate, sticky discharge, conjunctival Neonate, sticky discharge, conjunctival inflammationinflammation
5-14 days after birth5-14 days after birthCHLAMYDIA CONJUNCTIVITISCHLAMYDIA CONJUNCTIVITISLeading cause of preventable blindness Leading cause of preventable blindness
worldwideworldwideMost common; assoc nasopharyngitisMost common; assoc nasopharyngitisTX: Oral and topical erythromycinTX: Oral and topical erythromycin

Opthalmology IXOpthalmology IX
Painless vision loss, spider webs across Painless vision loss, spider webs across visual field, curtain coming downvisual field, curtain coming down
Fund: retinal tears, vitreous hemorrhagesFund: retinal tears, vitreous hemorrhages

Opthalmology IXOpthalmology IX
Painless vision loss, spider webs across Painless vision loss, spider webs across visual field, curtain coming downvisual field, curtain coming down
Fund: retinal tears, vitreous hemorrhagesFund: retinal tears, vitreous hemorrhagesRETINAL DETACHMENTRETINAL DETACHMENT

Opthalmology IXOpthalmology IX
Painless vision loss, spider webs across Painless vision loss, spider webs across visual field, curtain coming downvisual field, curtain coming down
Fund: retinal tears, vitreous hemorrhagesFund: retinal tears, vitreous hemorrhagesRETINAL DETACHMENTRETINAL DETACHMENTTX: Keep pt still, Optho consultTX: Keep pt still, Optho consultRetinal attachment surgeryRetinal attachment surgery

Opthalmology XOpthalmology X
58 yo female, sudden monocular vision 58 yo female, sudden monocular vision loss, ipselateral headacheloss, ipselateral headache
PE: AFD; Fund: pale swollen optic discPE: AFD; Fund: pale swollen optic disc

Opthalmology XOpthalmology X
58 yo female, sudden monocular vision 58 yo female, sudden monocular vision loss, ipselateral headacheloss, ipselateral headache
PE: AFD; Fund: pale swollen optic discPE: AFD; Fund: pale swollen optic discTEMPORAL ARTERITISTEMPORAL ARTERITISVasculitis med-large arteries, can cause Vasculitis med-large arteries, can cause
optic nerve infarctionoptic nerve infarctionF>M, 50+ yoF>M, 50+ yo

Opthalmology XOpthalmology X
TX: IV methylprednisolone, Optho/IM TX: IV methylprednisolone, Optho/IM consultconsult
DX: Temporal artery biopsyDX: Temporal artery biopsyDO NOT DELAY TX PENDING DO NOT DELAY TX PENDING
DEFINITIVE DXDEFINITIVE DX

Most Common…Most Common…

Most Common:Most Common:
Metabolic abnormality in newborns:Metabolic abnormality in newborns:

Most Common:Most Common:
Metabolic abnormality in newborns:Metabolic abnormality in newborns:HypoglycemiaHypoglycemia

Most Common:Most Common:
Metabolic abnormality in newborns:Metabolic abnormality in newborns:HypoglycemiaHypoglycemia
Rhythm in pediatric cardiac arrest:Rhythm in pediatric cardiac arrest:

Most Common:Most Common:
Metabolic abnormality in newborns:Metabolic abnormality in newborns:HypoglycemiaHypoglycemia
Rhythm in pediatric cardiac arrest:Rhythm in pediatric cardiac arrest:BradycardiasBradycardias

Most Common:Most Common:
Metabolic abnormality in newborns:Metabolic abnormality in newborns:HypoglycemiaHypoglycemia
Rhythm in pediatric cardiac arrest:Rhythm in pediatric cardiac arrest:BradycardiasBradycardias
Site in pediatric esophagus where foreign Site in pediatric esophagus where foreign bodies trapped:bodies trapped:

Most Common:Most Common:
Metabolic abnormality in newborns:Metabolic abnormality in newborns:HypoglycemiaHypoglycemia
Rhythm in pediatric cardiac arrest:Rhythm in pediatric cardiac arrest:BradycardiasBradycardias
Site in pediatric esophagus where foreign Site in pediatric esophagus where foreign bodies trapped:bodies trapped:Cricopharngeal narrowing (C6)Cricopharngeal narrowing (C6)

Most Common:Most Common:
Cause of syncope during normal Cause of syncope during normal pregnancy:pregnancy:

Most Common:Most Common:
Cause of syncope during normal Cause of syncope during normal pregnancy:pregnancy:VasovagalVasovagal

Most Common:Most Common:
Cause of syncope during normal Cause of syncope during normal pregnancy:pregnancy:VasovagalVasovagal
Cause of maternal death in 1Cause of maternal death in 1stst trimester: trimester:

Most Common:Most Common:
Cause of syncope during normal Cause of syncope during normal pregnancy:pregnancy:VasovagalVasovagal
Cause of maternal death in 1Cause of maternal death in 1stst trimester: trimester:Ectopic pregnancy (1.5% of all pregnancies)Ectopic pregnancy (1.5% of all pregnancies)

Most Common:Most Common:
Cause of syncope during normal Cause of syncope during normal pregnancy:pregnancy:VasovagalVasovagal
Cause of maternal death in 1Cause of maternal death in 1stst trimester: trimester:Ectopic pregnancy (1.5% of all pregnancies)Ectopic pregnancy (1.5% of all pregnancies)
Medical cause of death in pregnant Medical cause of death in pregnant women (overall):women (overall):

Most Common:Most Common:
Cause of syncope during normal Cause of syncope during normal pregnancy:pregnancy:VasovagalVasovagal
Cause of maternal death in 1Cause of maternal death in 1stst trimester: trimester:Ectopic pregnancy (1.5% of all pregnancies)Ectopic pregnancy (1.5% of all pregnancies)
Medical cause of death in pregnant Medical cause of death in pregnant women (overall):women (overall):Pulmonary embolismPulmonary embolism

Most Common:Most Common:
Obstructive cardiac lesion in the elderly:Obstructive cardiac lesion in the elderly:

Most Common:Most Common:
Obstructive cardiac lesion in the elderly:Obstructive cardiac lesion in the elderly:Aortic stenosisAortic stenosis

Most Common:Most Common:
Obstructive cardiac lesion in the elderly:Obstructive cardiac lesion in the elderly:Aortic stenosisAortic stenosis
Valvular heart disease in industrialized Valvular heart disease in industrialized countries:countries:

Most Common:Most Common:
Obstructive cardiac lesion in the elderly:Obstructive cardiac lesion in the elderly:Aortic stenosisAortic stenosis
Valvular heart disease in industrialized Valvular heart disease in industrialized countries:countries:Mitral valve prolapse (3% of population)Mitral valve prolapse (3% of population)

Most Common:Most Common:
Obstructive cardiac lesion in the elderly:Obstructive cardiac lesion in the elderly:Aortic stenosisAortic stenosis
Valvular heart disease in industrialized Valvular heart disease in industrialized countries:countries:Mitral valve prolapse (3% of population)Mitral valve prolapse (3% of population)
Presenting symptom of L heart failure, MS, Presenting symptom of L heart failure, MS, AI, all other acute valvular disorders:AI, all other acute valvular disorders:

Most Common:Most Common:
Obstructive cardiac lesion in the elderly:Obstructive cardiac lesion in the elderly:Aortic stenosisAortic stenosis
Valvular heart disease in industrialized Valvular heart disease in industrialized countries:countries:Mitral valve prolapse (3% of population)Mitral valve prolapse (3% of population)
Presenting symptom of L heart failure, MS, Presenting symptom of L heart failure, MS, AI, all other acute valvular disorders:AI, all other acute valvular disorders:Dyspnea, especially on exertionDyspnea, especially on exertion

Most Common:Most Common:
Radiographic finding in aortic dissection:Radiographic finding in aortic dissection:

Most Common:Most Common:
Radiographic finding in aortic dissection:Radiographic finding in aortic dissection:Widened mediastinumWidened mediastinum

Most Common:Most Common:
Radiographic finding in aortic dissection:Radiographic finding in aortic dissection:Widened mediastinumWidened mediastinum
Top three cardiovascular diseases in US, Top three cardiovascular diseases in US, in order:in order:

Most Common:Most Common:
Radiographic finding in aortic dissection:Radiographic finding in aortic dissection:Widened mediastinumWidened mediastinum
Top three cardiovascular diseases in US, Top three cardiovascular diseases in US, in order:in order: (1) Ischemic HD (2) Hypertension (3) (1) Ischemic HD (2) Hypertension (3)
Cardiomyopathies (all combined)Cardiomyopathies (all combined)

Most Common:Most Common:
Radiographic finding in aortic dissection:Radiographic finding in aortic dissection:Widened mediastinumWidened mediastinum
Top three cardiovascular diseases in US, Top three cardiovascular diseases in US, in order:in order: (1) Ischemic HD (2) Hypertension (3) (1) Ischemic HD (2) Hypertension (3)
Cardiomyopathies (all combined)Cardiomyopathies (all combined)Symptom of acute pericarditis:Symptom of acute pericarditis:

Most Common:Most Common:
Radiographic finding in aortic dissection:Radiographic finding in aortic dissection:Widened mediastinumWidened mediastinum
Top three cardiovascular diseases in US, Top three cardiovascular diseases in US, in order:in order: (1) Ischemic HD (2) Hypertension (3) (1) Ischemic HD (2) Hypertension (3)
Cardiomyopathies (all combined)Cardiomyopathies (all combined)Symptom of acute pericarditis:Symptom of acute pericarditis:
Precordial or SS CP, described as sharp or Precordial or SS CP, described as sharp or stabbingstabbing

Most Common:Most Common:
Physical finding in acute pericarditis:Physical finding in acute pericarditis:

Most Common:Most Common:
Physical finding in acute pericarditis:Physical finding in acute pericarditis:Pericardial friction rub (??)Pericardial friction rub (??)
Cause of acute arterial occlusion in limb:Cause of acute arterial occlusion in limb:

Most Common:Most Common:
Physical finding in acute pericarditis:Physical finding in acute pericarditis:Pericardial friction rub (??)Pericardial friction rub (??)
Cause of acute arterial occlusion in limb:Cause of acute arterial occlusion in limb:Embolus (80-90% originate in heart)Embolus (80-90% originate in heart)

Most Common:Most Common:
Physical finding in acute pericarditis:Physical finding in acute pericarditis:Pericardial friction rub (??)Pericardial friction rub (??)
Cause of acute arterial occlusion in limb:Cause of acute arterial occlusion in limb:Embolus (80-90% originate in heart)Embolus (80-90% originate in heart)
Most common infection and 5Most common infection and 5thth leading leading COD in elderly:COD in elderly:

Most Common:Most Common:
Physical finding in acute pericarditis:Physical finding in acute pericarditis:Pericardial friction rub (??)Pericardial friction rub (??)
Cause of acute arterial occlusion in limb:Cause of acute arterial occlusion in limb:Embolus (80-90% originate in heart)Embolus (80-90% originate in heart)
Most common infection and 5Most common infection and 5thth leading leading COD in elderly:COD in elderly:PneumoniaPneumonia

Most Common:Most Common:
Viral agent implicated in post-transplant Viral agent implicated in post-transplant pulmonary infection:pulmonary infection:

Most Common:Most Common:
Viral agent implicated in post-transplant Viral agent implicated in post-transplant pulmonary infection:pulmonary infection:CytomegalovirusCytomegalovirus

Most Common:Most Common:
Viral agent implicated in post-transplant Viral agent implicated in post-transplant pulmonary infection:pulmonary infection:CytomegalovirusCytomegalovirus
Cause of abdominal pain in adults Cause of abdominal pain in adults presenting to ED:presenting to ED:

Most Common:Most Common:
Viral agent implicated in post-transplant Viral agent implicated in post-transplant pulmonary infection:pulmonary infection:CytomegalovirusCytomegalovirus
Cause of abdominal pain in adults Cause of abdominal pain in adults presenting to ED:presenting to ED:Nonspecific abdominal painNonspecific abdominal pain

Most Common:Most Common:
Viral agent implicated in post-transplant Viral agent implicated in post-transplant pulmonary infection:pulmonary infection:CytomegalovirusCytomegalovirus
Cause of abdominal pain in adults Cause of abdominal pain in adults presenting to ED:presenting to ED:Nonspecific abdominal painNonspecific abdominal pain
GI diagnosis in ED patients above age 50:GI diagnosis in ED patients above age 50:

Most Common:Most Common:
Viral agent implicated in post-transplant Viral agent implicated in post-transplant pulmonary infection:pulmonary infection:CytomegalovirusCytomegalovirus
Cause of abdominal pain in adults Cause of abdominal pain in adults presenting to ED:presenting to ED:Nonspecific abdominal painNonspecific abdominal pain
GI diagnosis in ED patients above age 50:GI diagnosis in ED patients above age 50:Biliary tract diseaseBiliary tract disease

Most Common:Most Common:
Surgical emergency in older patients with Surgical emergency in older patients with abdominal pain:abdominal pain:

Most Common:Most Common:
Surgical emergency in older patients with Surgical emergency in older patients with abdominal pain:abdominal pain:Acute cholecystitisAcute cholecystitis

Most Common:Most Common:
Surgical emergency in older patients with Surgical emergency in older patients with abdominal pain:abdominal pain:Acute cholecystitisAcute cholecystitis
Symptom of abdominal aortic aneurism:Symptom of abdominal aortic aneurism:

Most Common:Most Common:
Surgical emergency in older patients with Surgical emergency in older patients with abdominal pain:abdominal pain:Acute cholecystitisAcute cholecystitis
Symptom of abdominal aortic aneurism:Symptom of abdominal aortic aneurism:Abdominal painAbdominal pain

Most Common:Most Common:
Surgical emergency in older patients with Surgical emergency in older patients with abdominal pain:abdominal pain:Acute cholecystitisAcute cholecystitis
Symptom of abdominal aortic aneurism:Symptom of abdominal aortic aneurism:Abdominal painAbdominal pain
Diagnostic mistake in patients with AAA:Diagnostic mistake in patients with AAA:

Most Common:Most Common:
Surgical emergency in older patients with Surgical emergency in older patients with abdominal pain:abdominal pain:Acute cholecystitisAcute cholecystitis
Symptom of abdominal aortic aneurism:Symptom of abdominal aortic aneurism:Abdominal painAbdominal pain
Diagnostic mistake in patients with AAA:Diagnostic mistake in patients with AAA:Diagnosing renal colic in these ptsDiagnosing renal colic in these pts

Most Common:Most Common:
Rhythm disturbance in PE:Rhythm disturbance in PE:

Most Common:Most Common:
Rhythm disturbance in PE:Rhythm disturbance in PE:Sinus tachycardia (on Boards pts: S1Q3T3)Sinus tachycardia (on Boards pts: S1Q3T3)

Most Common:Most Common:
Rhythm disturbance in PE:Rhythm disturbance in PE:Sinus tachycardia (on Boards pts: S1Q3T3)Sinus tachycardia (on Boards pts: S1Q3T3)
ECG abnormality in PE:ECG abnormality in PE:

Most Common:Most Common:
Rhythm disturbance in PE:Rhythm disturbance in PE:Sinus tachycardia (on Boards pts: S1Q3T3)Sinus tachycardia (on Boards pts: S1Q3T3)
ECG abnormality in PE:ECG abnormality in PE:Non-specific ST-T wave changesNon-specific ST-T wave changes

Most Common:Most Common:
Rhythm disturbance in PE:Rhythm disturbance in PE:Sinus tachycardia (on Boards pts: S1Q3T3)Sinus tachycardia (on Boards pts: S1Q3T3)
ECG abnormality in PE:ECG abnormality in PE:Non-specific ST-T wave changesNon-specific ST-T wave changes
CXR abnormality in PE:CXR abnormality in PE:

Most Common:Most Common:
Rhythm disturbance in PE:Rhythm disturbance in PE:Sinus tachycardia (on Boards pts: S1Q3T3)Sinus tachycardia (on Boards pts: S1Q3T3)
ECG abnormality in PE:ECG abnormality in PE:Non-specific ST-T wave changesNon-specific ST-T wave changes
CXR abnormality in PE:CXR abnormality in PE: Infiltrate or atelectasis (50%), Elevated Infiltrate or atelectasis (50%), Elevated
hemidiaphragm +/- pleural effusion (40%), hemidiaphragm +/- pleural effusion (40%), NORMAL (30%)NORMAL (30%)

Thank you for Thank you for your Attentionyour Attention