Embed Size (px)
Citation preview
Emerging Treatment Strategies for Tuberous Sclerosis Complex
David Neal Franz, MDDirector, Tuberous Sclerosis ClinicCincinnati Children’s Hospital Medical CenterCincinnati, Ohio
Goals
• Describe the manifestations of tuberous sclerosis complex (TSC) in various organ systems and the most frequent causes of neurologic, renal, and pulmonary morbidity and mortality
• Review the molecular pathophysiology of TSC and how this forms the basis for novel therapeutic approaches
• Compare the rationale and initial clinical trial evidence for emerging treatment approaches for TSC
• Summarize ongoing clinical trials evaluating treatment approaches for TSC, including the goals of the trials, patient eligibility criteria, and other key factors
Pan D, et al. Trends Cell Biol. 2004;14:78-85.
Clinical Manifestations of TSC
• Brain: cortical tubers, subependymal nodules, subependymal giant cell astrocytomas
• Eye: retinal hamartomas
• Heart: cardiac rhabdomyomas
• Kidney: benign angiomyolipomas, cysts, malignant angiomyolipomas, renal cell carcinoma
• Lung: lymphangioleiomyomatosis, multifocal micronodular pneumocyte hyperplasia
• Skin: hypomelanotic macules, shagreen patches, periungual or subungual fibromas, facial angiofibromas
• Behavior: mental retardation, autism, bipolar disorder
Roach ES, Sparagana SP. J Child Neurol. 2004;19:643-649.
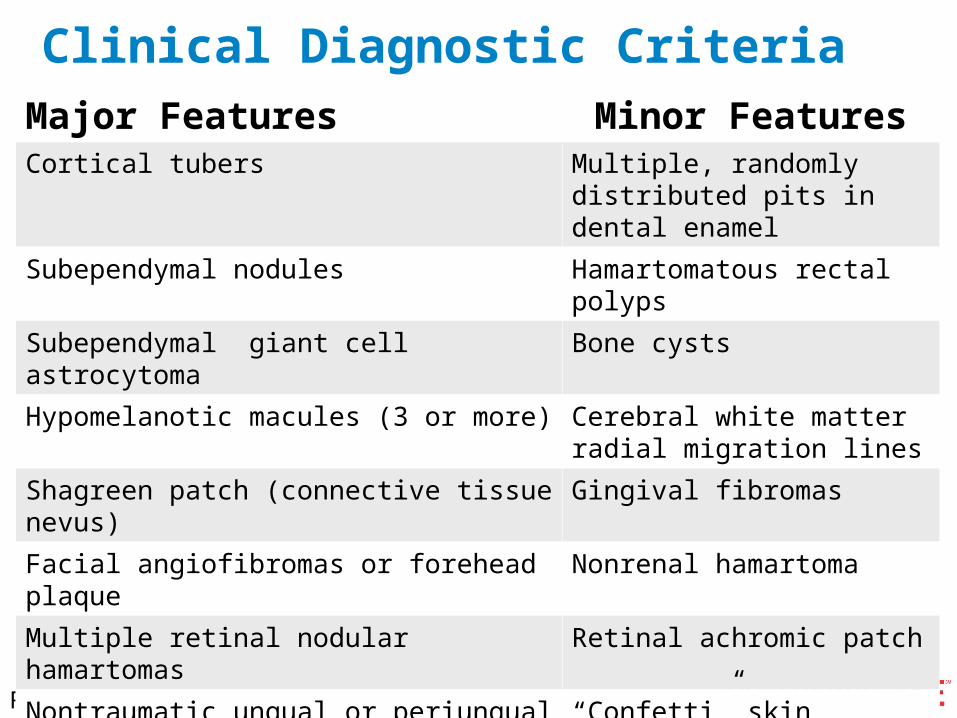
Clinical Diagnostic CriteriaMajor Features Minor FeaturesCortical tubers Multiple, randomly distributed
pits in dental enamel
Subependymal nodules Hamartomatous rectal polyps
Subependymal giant cell astrocytoma Bone cysts
Hypomelanotic macules (3 or more) Cerebral white matter radial migration lines
Shagreen patch (connective tissue nevus) Gingival fibromas
Facial angiofibromas or forehead plaque Nonrenal hamartoma
Multiple retinal nodular hamartomas Retinal achromic patch
Nontraumatic ungual or periungual fibromas “Confetti” skin lesions
Cardiac rhabdomyoma, single or multiple Multiple renal cysts
Pulmonary lymphangioleiomyomatosis and/or renal angiomyolipomas
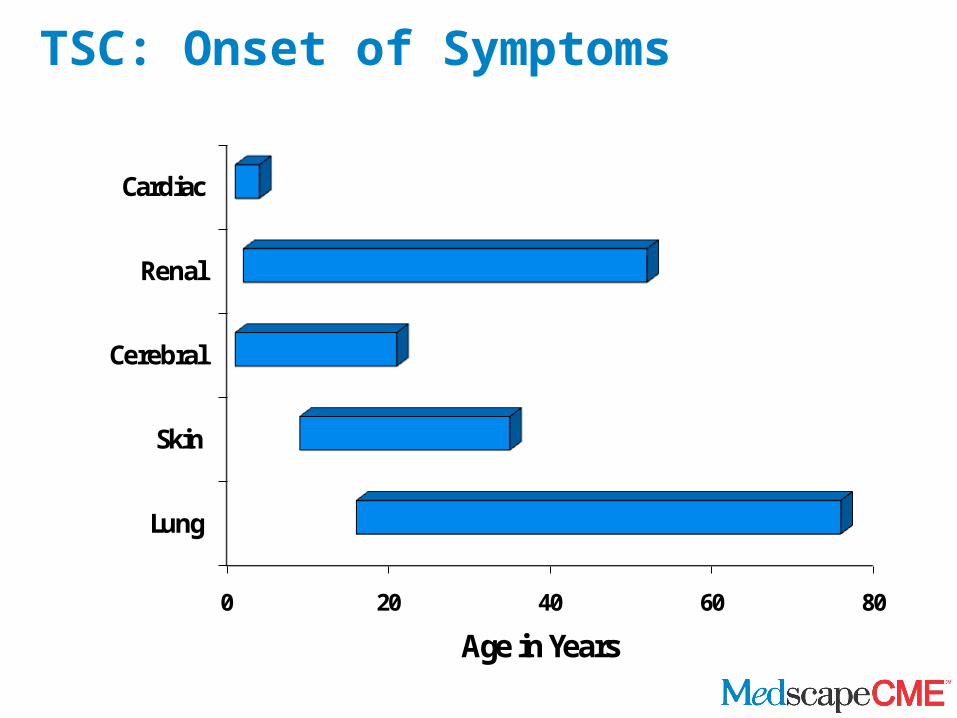
TSC: Onset of Symptoms
0 20 40 60 80
Lung
Skin
Cerebral
Renal
Cardiac
Age in Years

Hypopigmented Macule and Shagreen Patch

Facial Angiofibroma

Periungual Fibroma
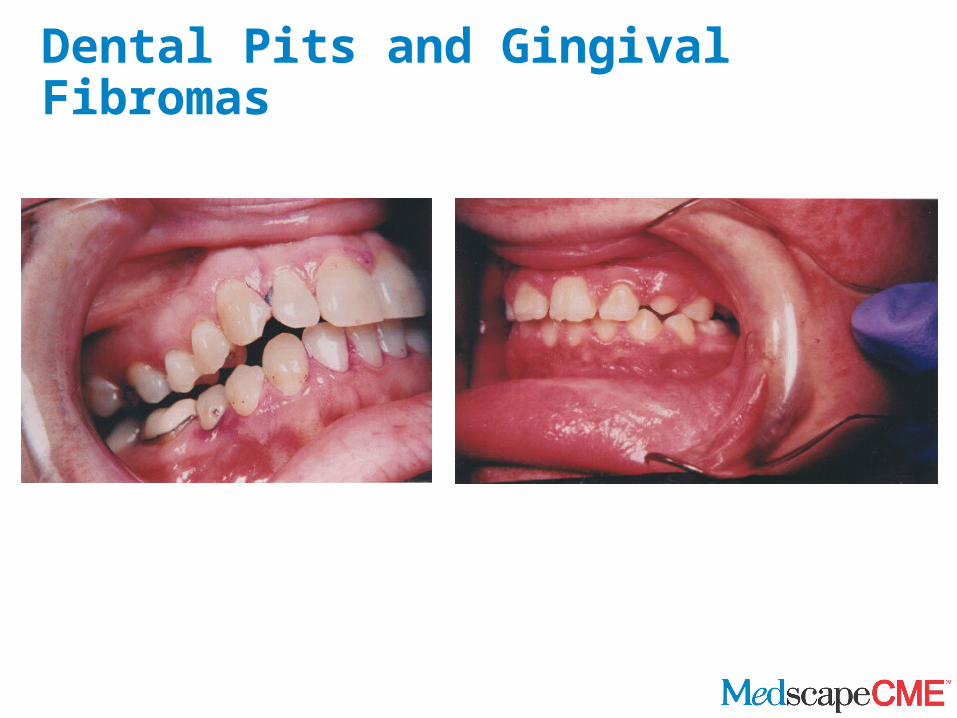
Dental Pits and Gingival Fibromas
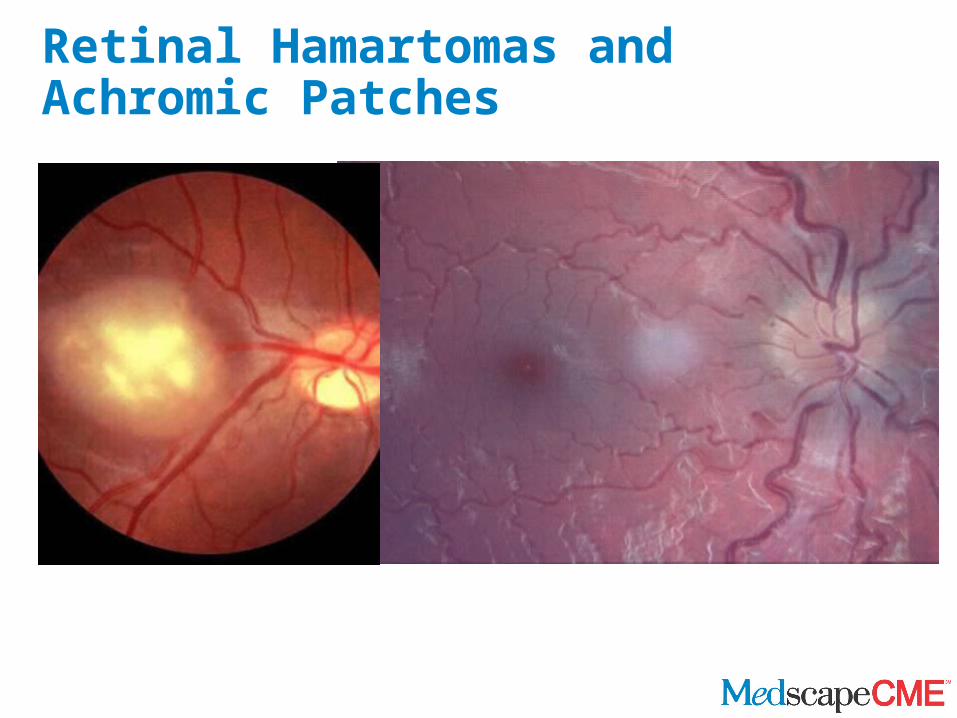
Retinal Hamartomas and Achromic Patches
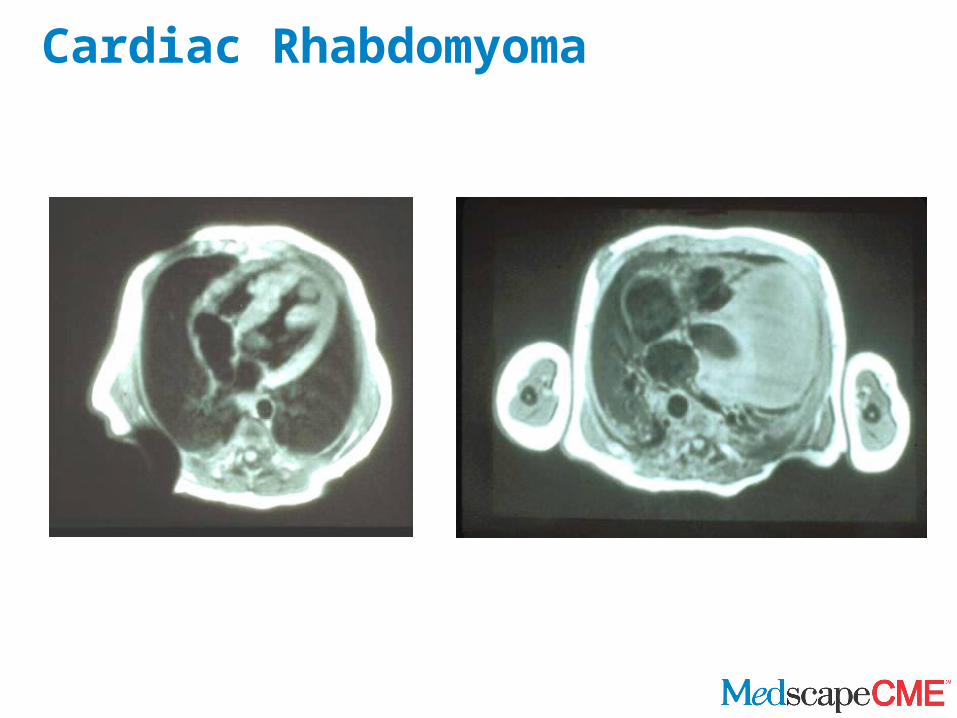
Cardiac Rhabdomyoma
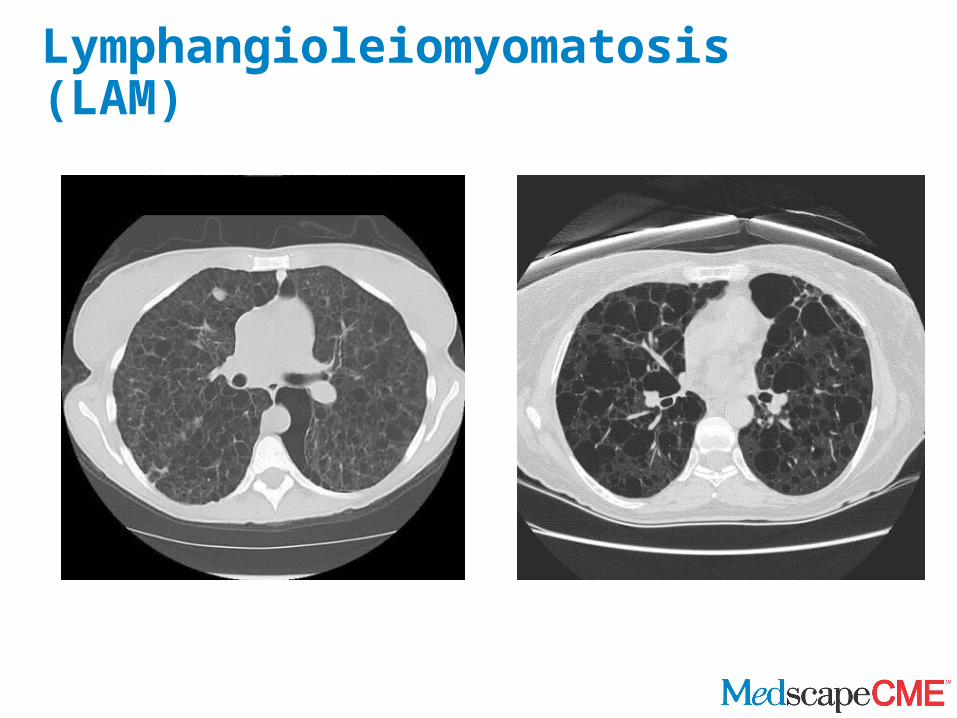
Lymphangioleiomyomatosis (LAM)
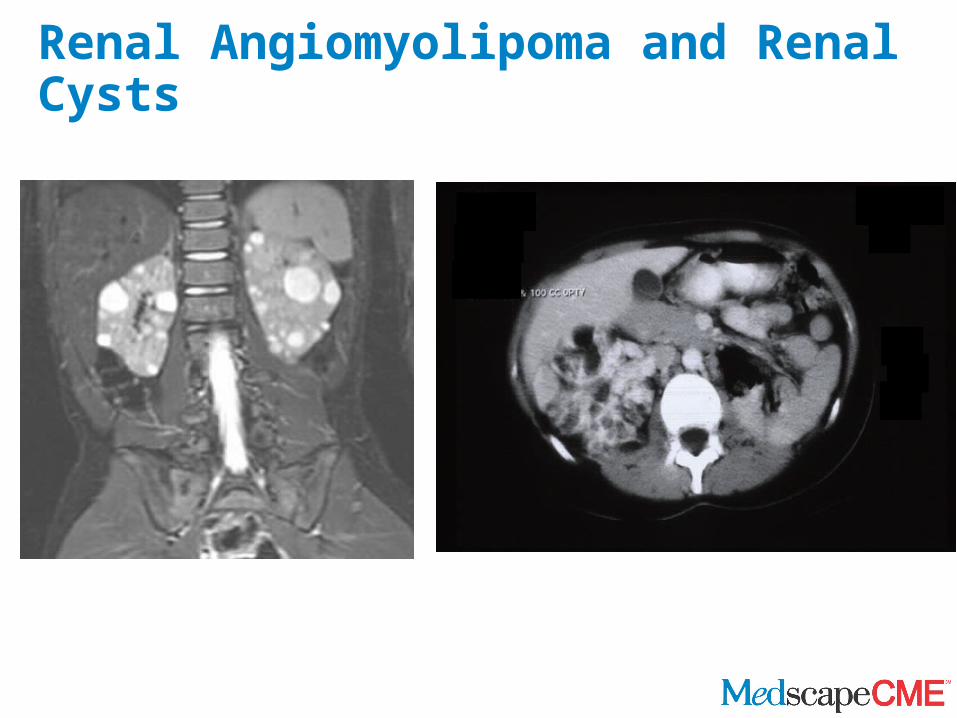
Renal Angiomyolipoma and Renal Cysts
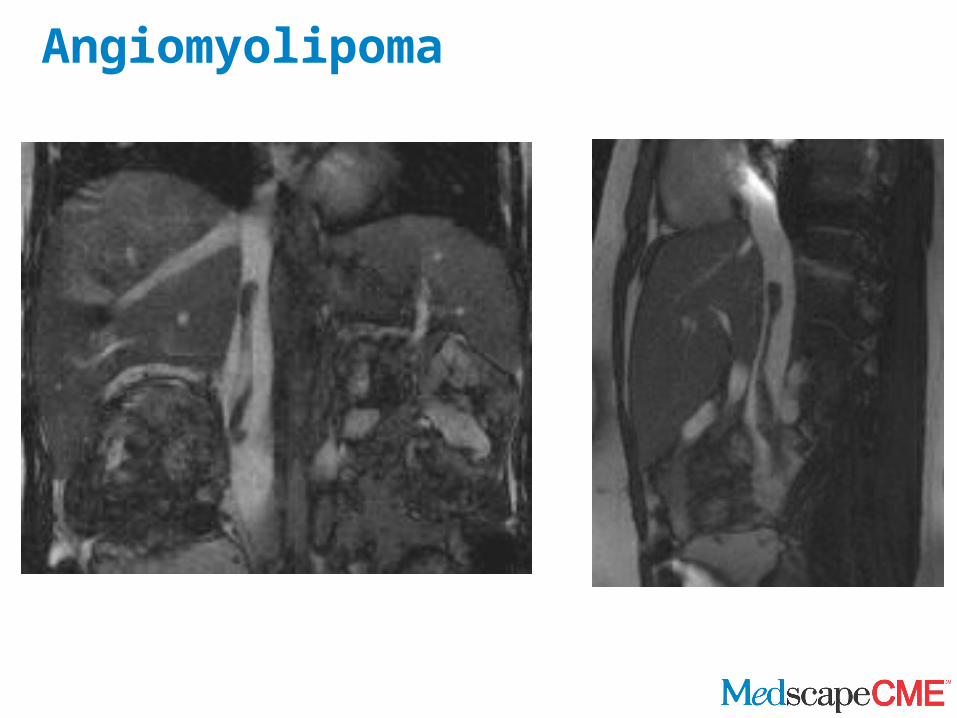
Angiomyolipoma
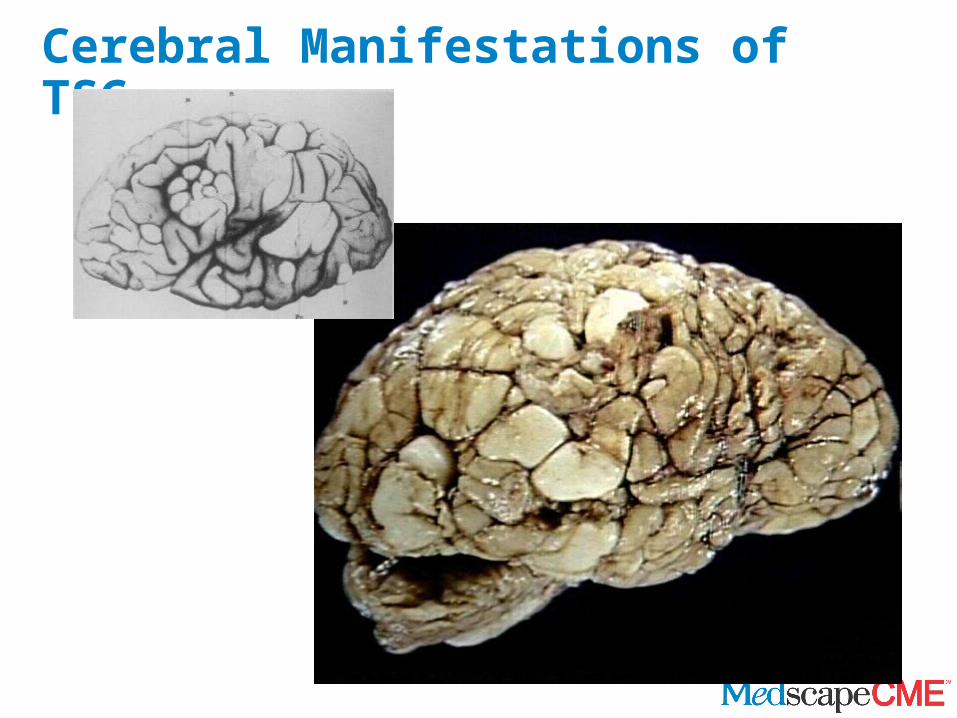
Cerebral Manifestations of TSC
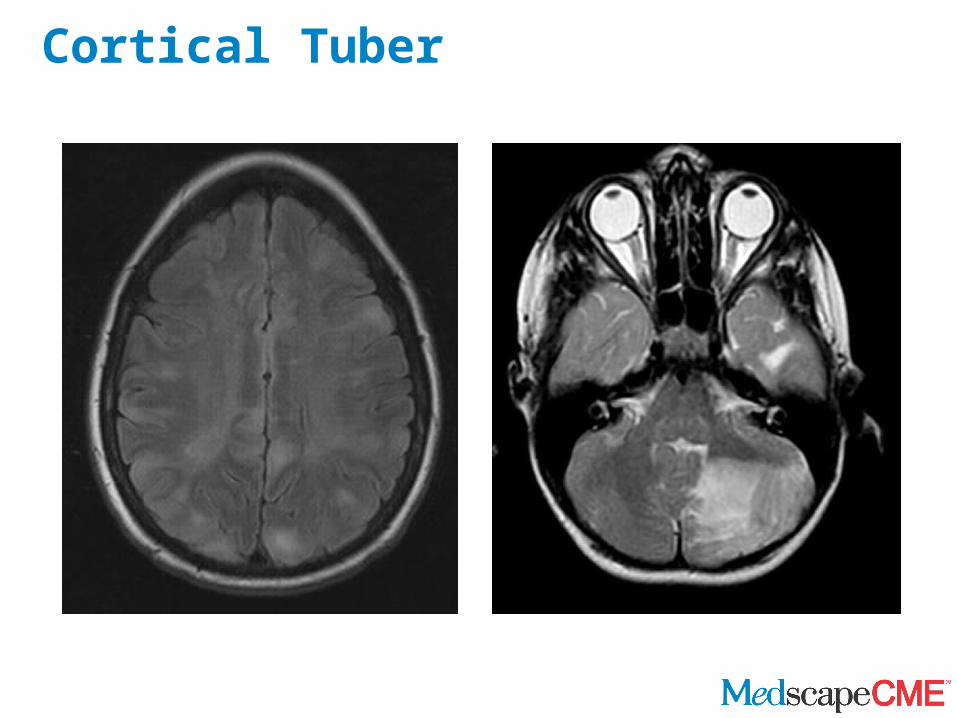
Cortical Tuber
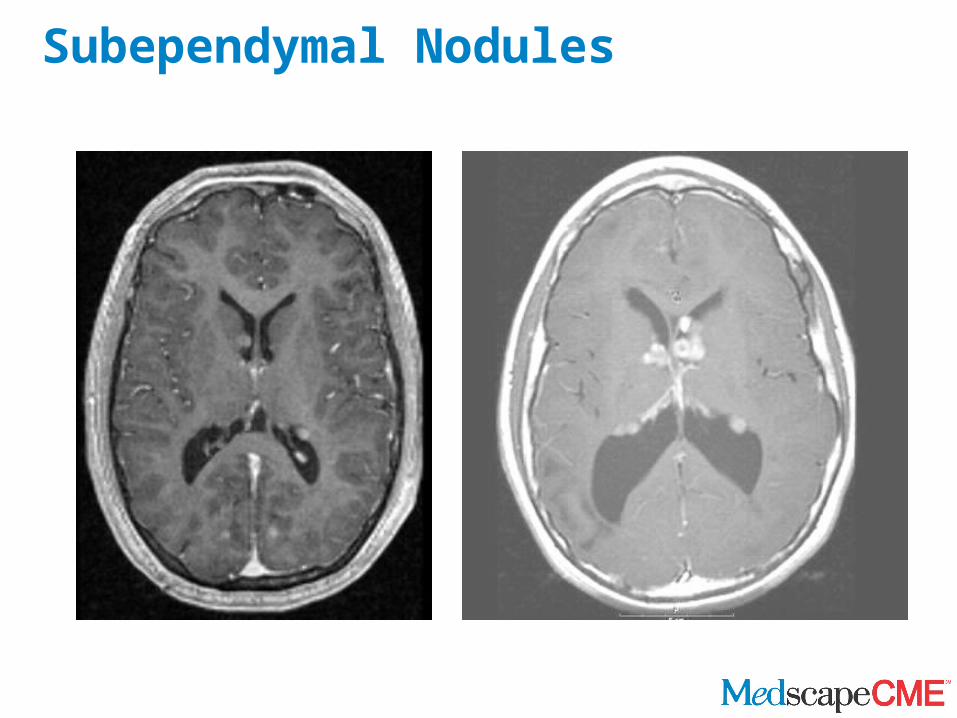
Subependymal Nodules
Neurologic/Behavioral Manifestations
• Seizures (90%)• Mental retardation and learning difficulties
(60%-70%)• Sleep disorders (60%)• Autism and behavioral difficulties (30%-50%)• Subependymal giant cell astrocytoma (15%-
20%)
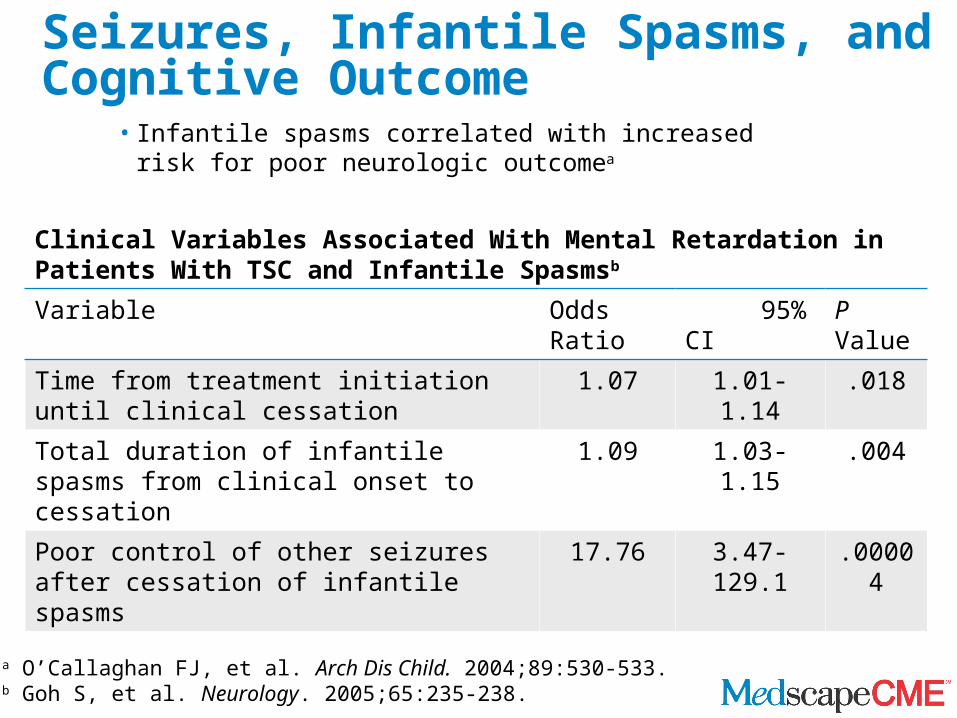
Seizures, Infantile Spasms, and Cognitive Outcome
• Infantile spasms correlated with increased risk for poor neurologic outcomea
a O’Callaghan FJ, et al. Arch Dis Child. 2004;89:530-533.b Goh S, et al. Neurology. 2005;65:235-238.
Clinical Variables Associated With Mental Retardation in Patients With TSC and Infantile Spasmsb
Variable Odds Ratio 95% CI P Value
Time from treatment initiation until clinical cessation
1.07 1.01-1.14 .018
Total duration of infantile spasms from clinical onset to cessation
1.09 1.03-1.15 .004
Poor control of other seizures after cessation of infantile spasms
17.76 3.47-129.1 .00004
Infantile Spasms in TSC
• Vigabatrin is the treatment of choice in TSC– Risk for adverse effect on peripheral vision – As high as 95% response rate in TSCa
• Steroids are second-line treatment (adrenocorticotropic hormone or oral prednisone)
• Valproate, topiramate, clonazepam minimally effective as single agents but may have beneficial adjunctive use
aHancock EC, Osborne JP. J Child Neurol. 1999;14:71-74.
Epilepsy in TSC
• About 90% of patients with TSC experience seizures• Virtually all seizure types have been reported (simple
partial, complex partial, generalized tonic-clonic, absence)
• Aggressive treatment is necessary to reduce risk for negative neurologic outcome (development, cognition, behavior)
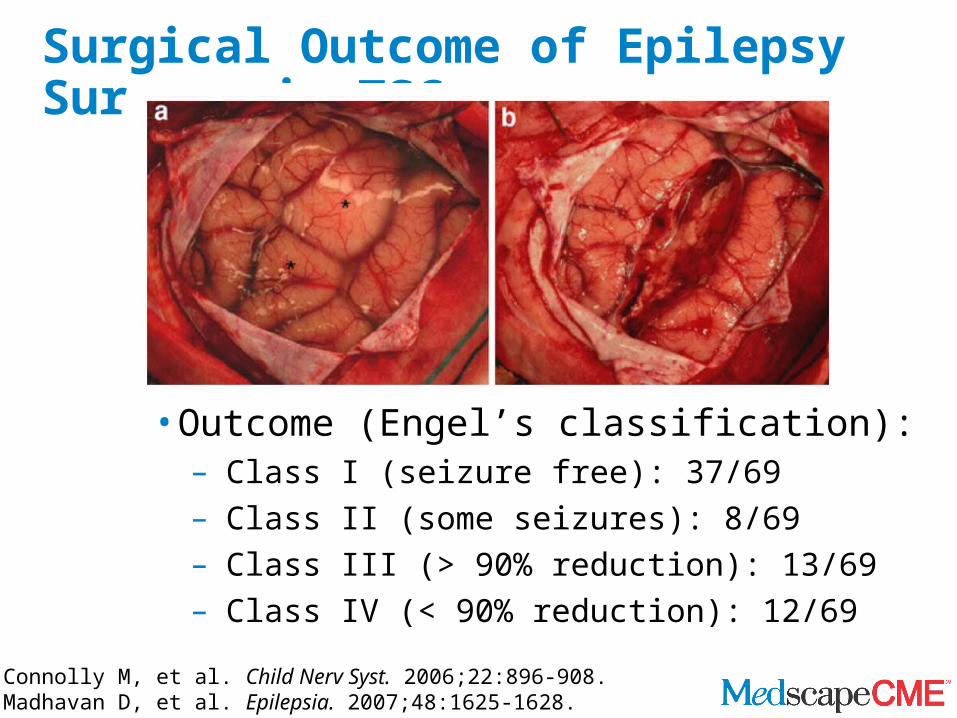
Surgical Outcome of Epilepsy Surgery in TSC
• Outcome (Engel’s classification):– Class I (seizure free): 37/69– Class II (some seizures): 8/69– Class III (> 90% reduction): 13/69– Class IV (< 90% reduction): 12/69
Connolly M, et al. Child Nerv Syst. 2006;22:896-908.Madhavan D, et al. Epilepsia. 2007;48:1625-1628.
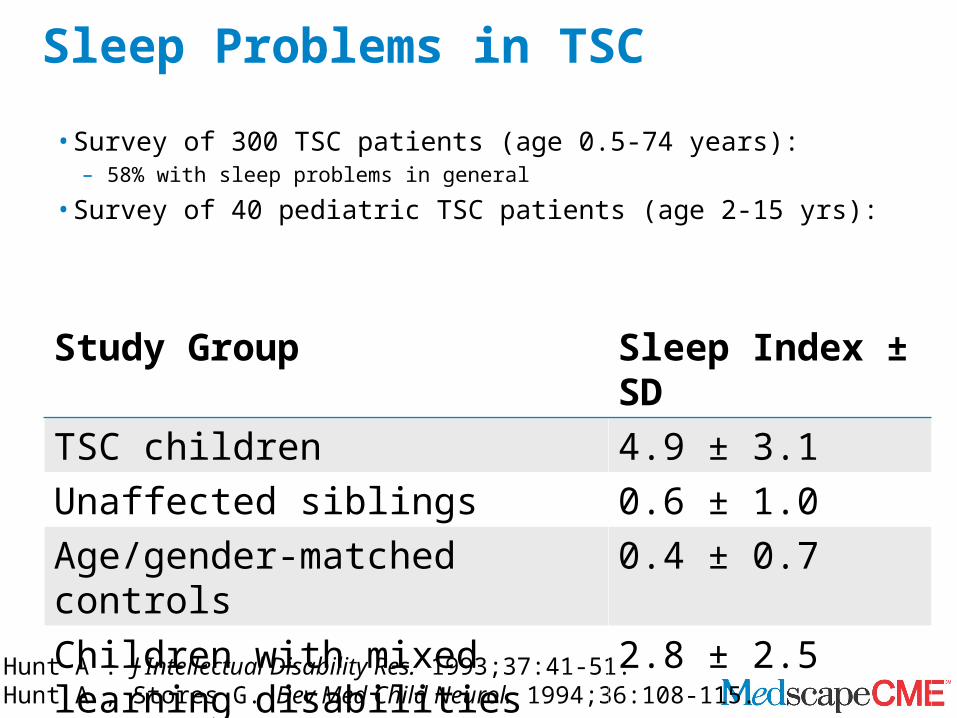
Sleep Problems in TSC
• Survey of 300 TSC patients (age 0.5-74 years):– 58% with sleep problems in general
• Survey of 40 pediatric TSC patients (age 2-15 yrs):
Hunt A . J Intellectual Disability Res. 1993;37:41-51. Hunt A , Stores G. Dev Med Child Neurol. 1994;36:108-115.
Study Group Sleep Index ± SDTSC children 4.9 ± 3.1Unaffected siblings 0.6 ± 1.0Age/gender-matched controls 0.4 ± 0.7Children with mixed learning disabilities
2.8 ± 2.5
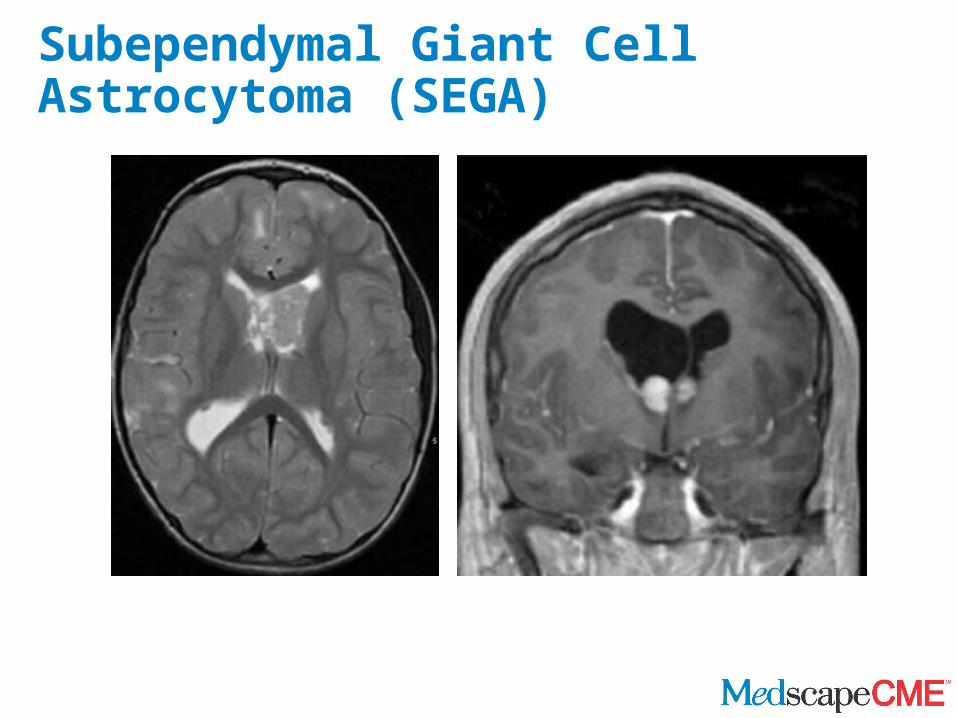
Subependymal Giant Cell Astrocytoma (SEGA)
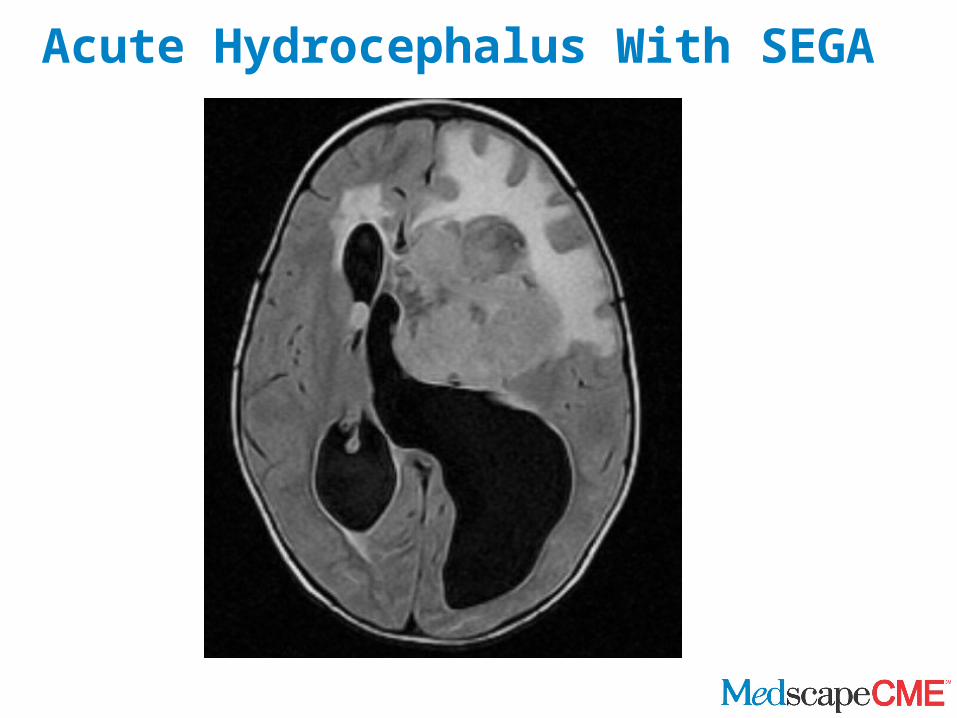
Acute Hydrocephalus With SEGA
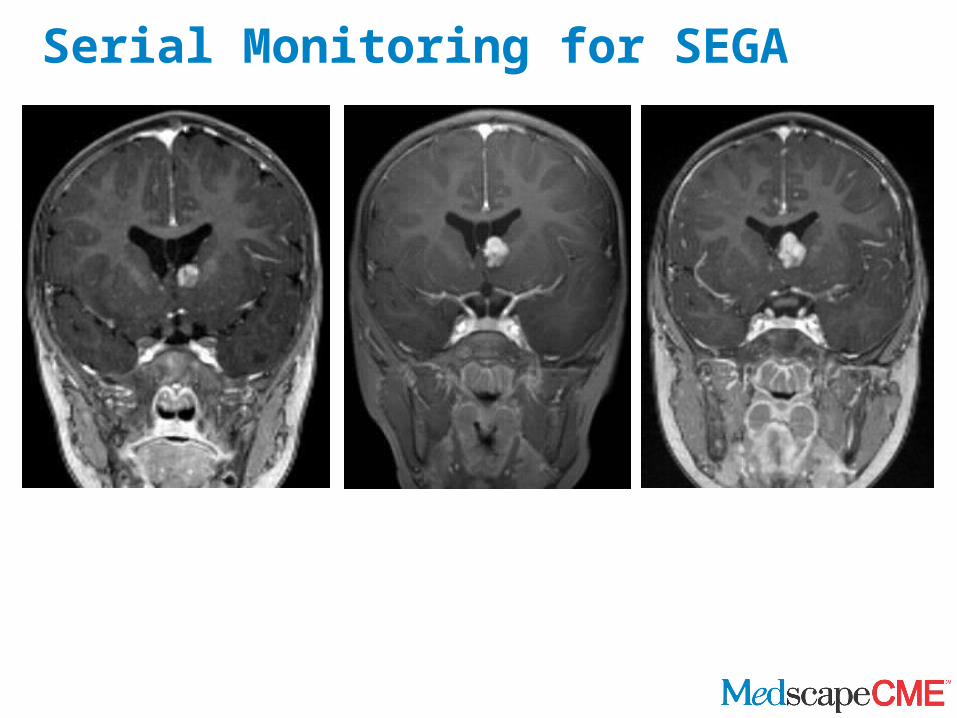
Serial Monitoring for SEGA
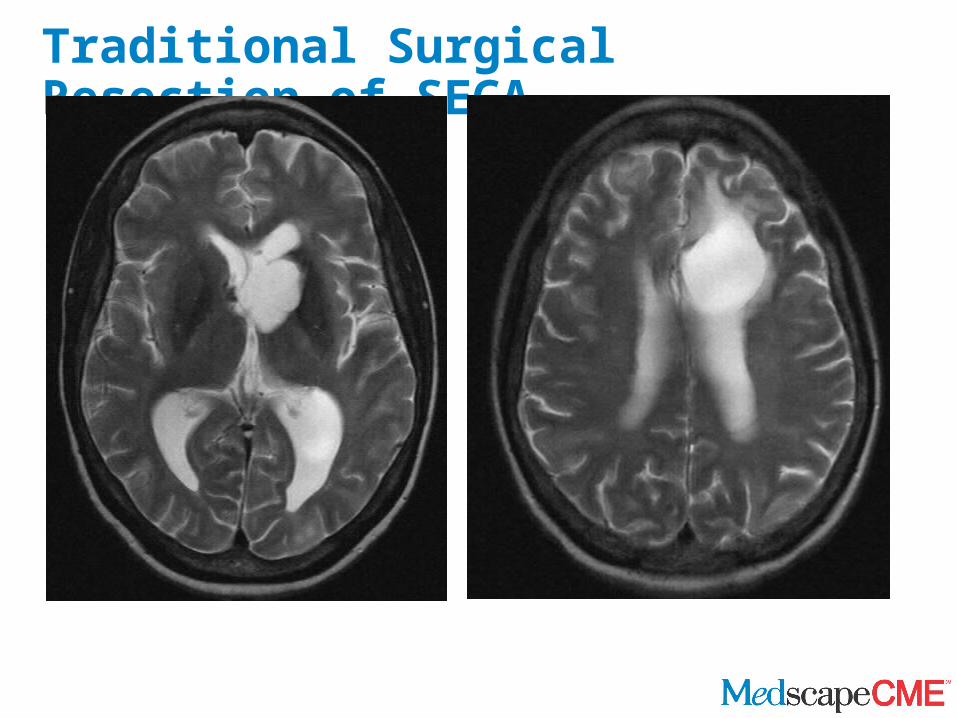
Traditional Surgical Resection of SEGA
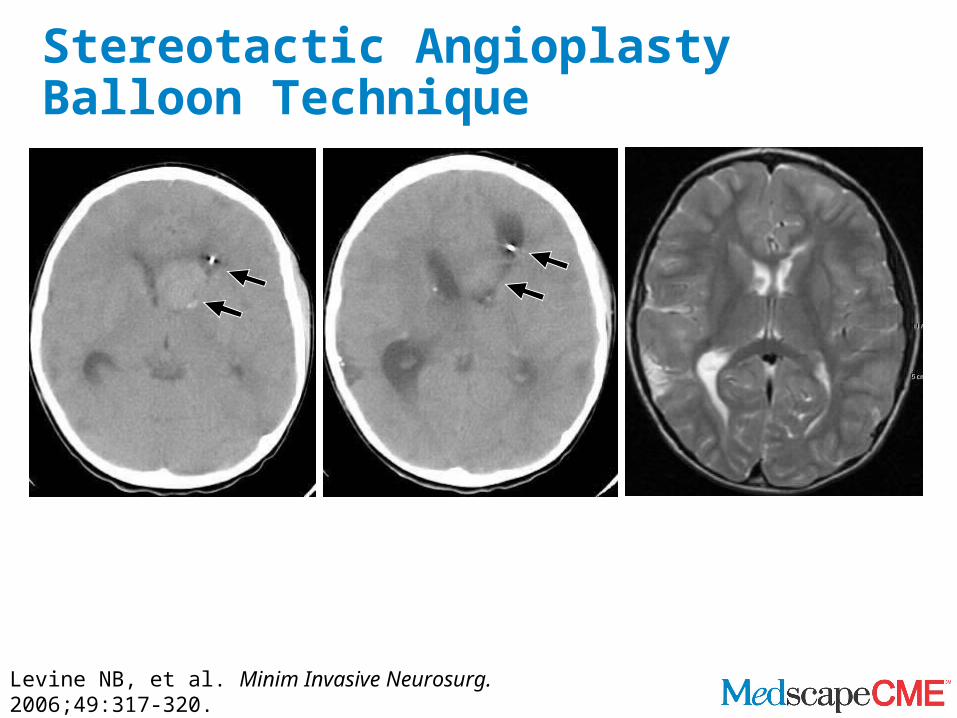
Stereotactic Angioplasty Balloon Technique
Levine NB, et al. Minim Invasive Neurosurg. 2006;49:317-320.
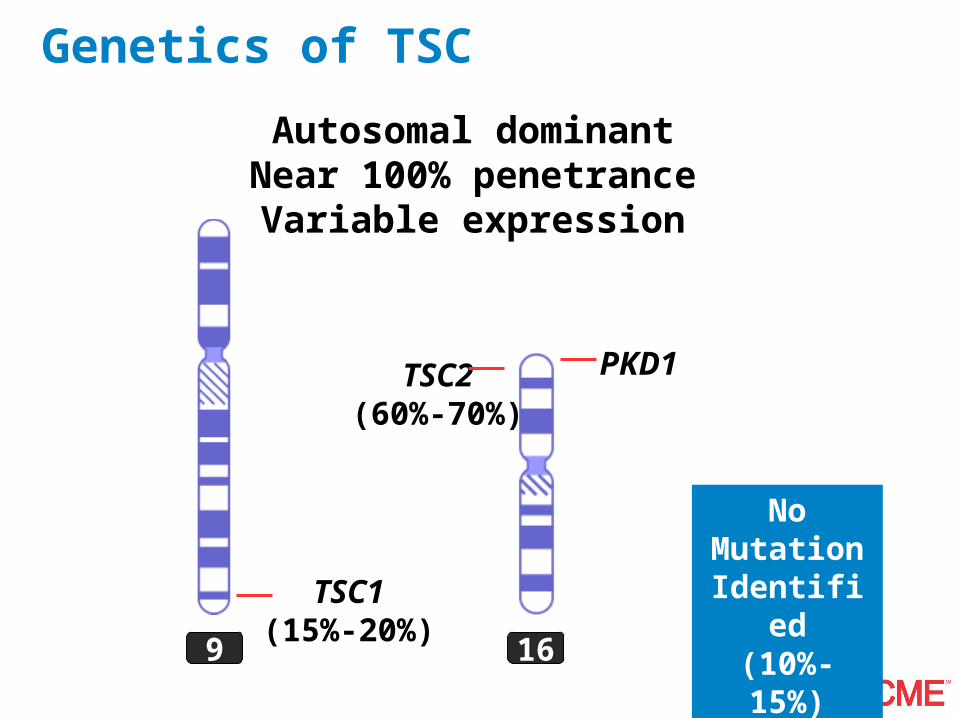
Genetics of TSC
9 16
TSC1(15%-20%)
TSC2(60%-70%)
PKD1
Autosomal dominantNear 100% penetrance
Variable expression
No Mutation Identified(10%-15%)
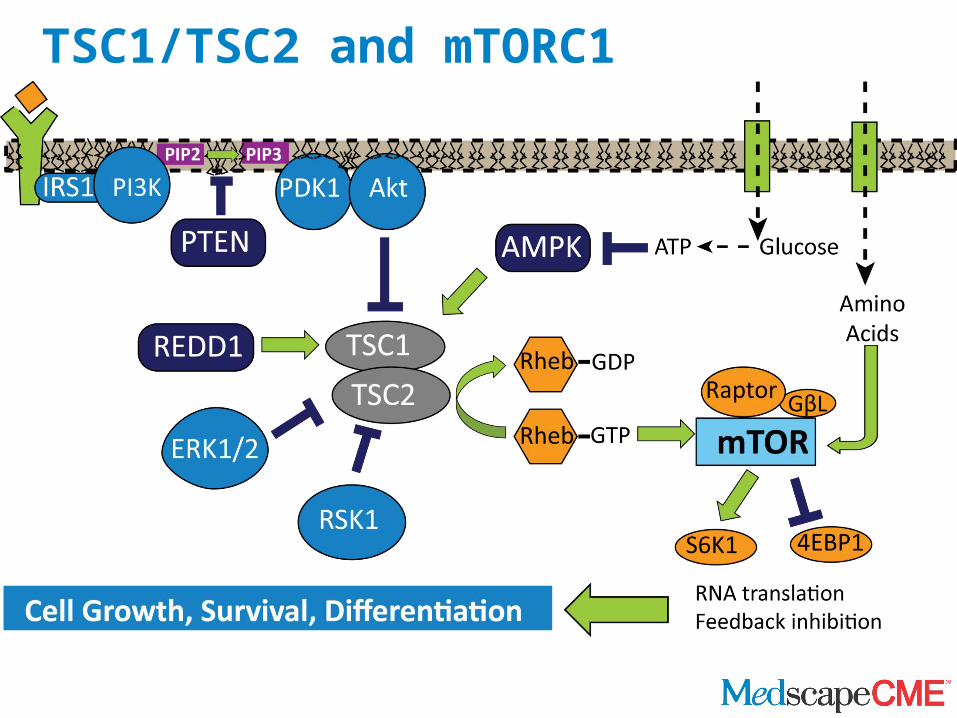
TSC1/TSC2 and mTORC1
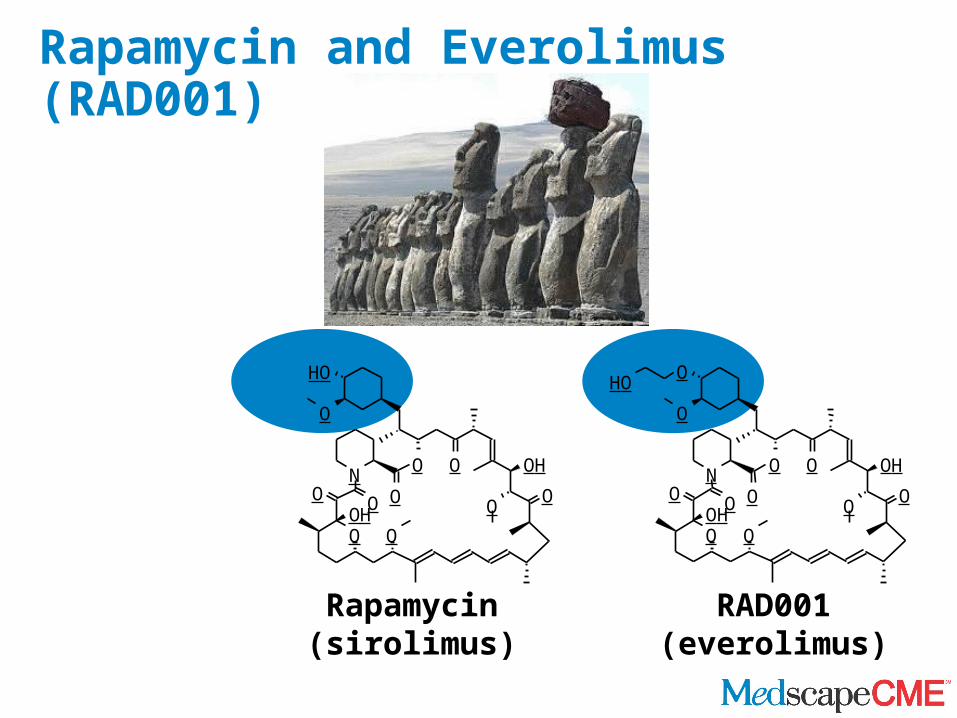
Rapamycin and Everolimus (RAD001)
Rapamycin(sirolimus)
RAD001(everolimus)
O O OH
O OON
OO
O O
OH
OH
O
O O OH
O OON
OO
O O
O
OH
O
OH
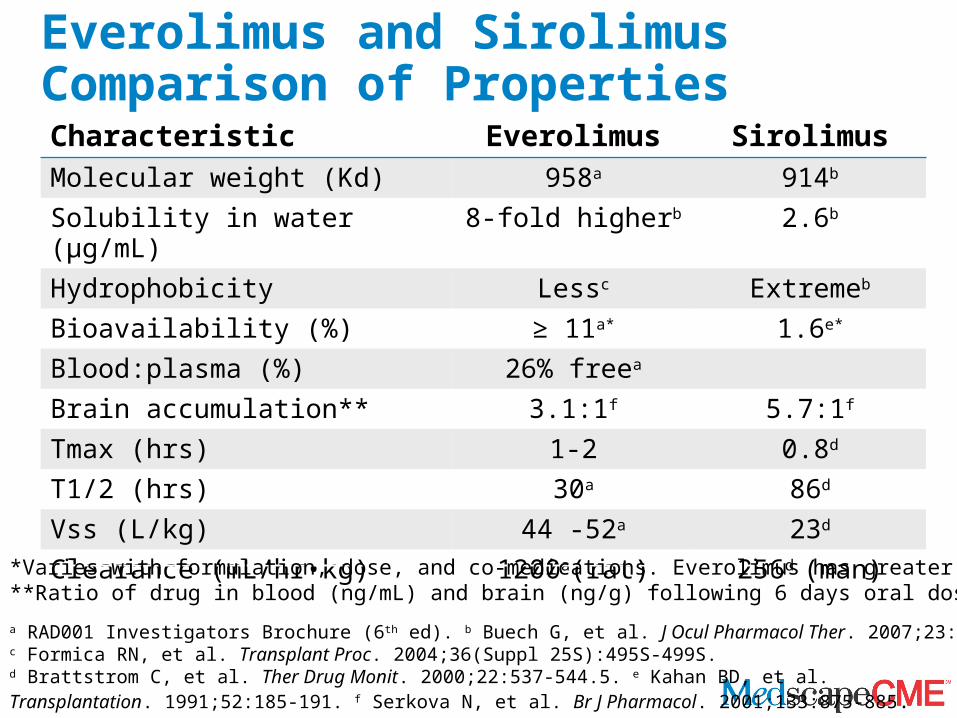
Everolimus and Sirolimus Comparison of PropertiesCharacteristic Everolimus SirolimusMolecular weight (Kd) 958a 914b
Solubility in water (μg/mL) 8-fold higherb 2.6b
Hydrophobicity Lessc Extremeb
Bioavailability (%) ≥ 11a* 1.6e*
Blood:plasma (%) 26% freea
Brain accumulation** 3.1:1f 5.7:1f
Tmax (hrs) 1-2 0.8d
T1/2 (hrs) 30a 86d
Vss (L/kg) 44 -52a 23d
Clearance (mL/hr•kg) 1200a(rat) 256d (man)
a RAD001 Investigators Brochure (6th ed). b Buech G, et al. J Ocul Pharmacol Ther. 2007;23:292.c Formica RN, et al. Transplant Proc. 2004;36(Suppl 25S):495S-499S. d Brattstrom C, et al. Ther Drug Monit. 2000;22:537-544.5. e Kahan BD, et al. Transplantation. 1991;52:185-191. f Serkova N, et al. Br J Pharmacol. 2001;133:875-885.
*Varies with formulation, dose, and co-medications. Everolimus has greater bioavailability than sirolimus.**Ratio of drug in blood (ng/mL) and brain (ng/g) following 6 days oral dosing at 3 mg/kg in rats. f
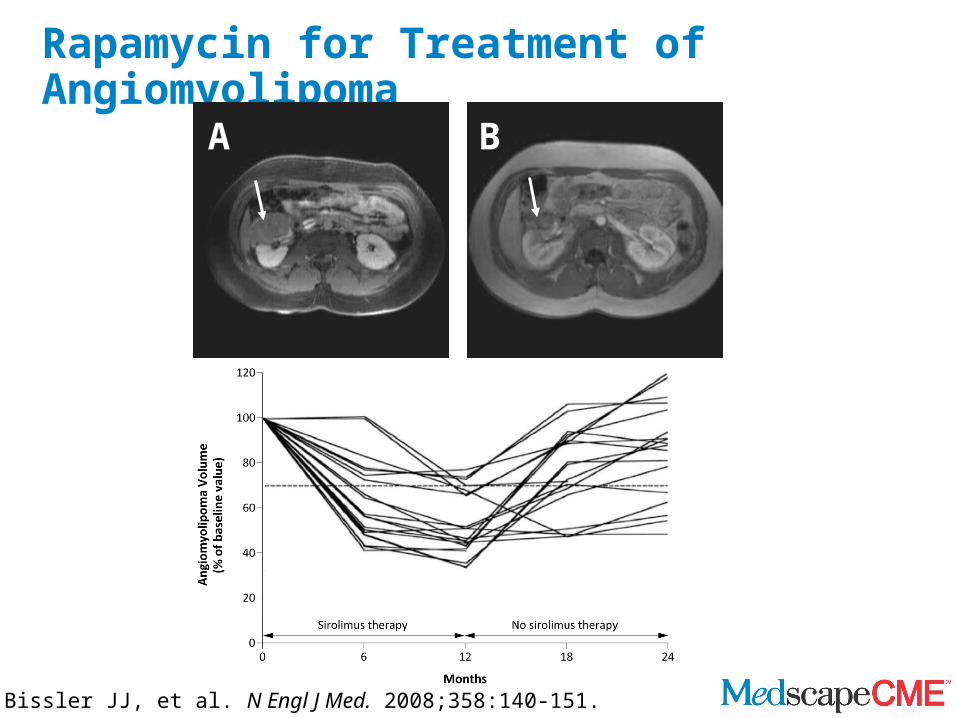
Rapamycin for Treatment of Angiomyolipoma
A B
Bissler JJ, et al. N Engl J Med. 2008;358:140-151.
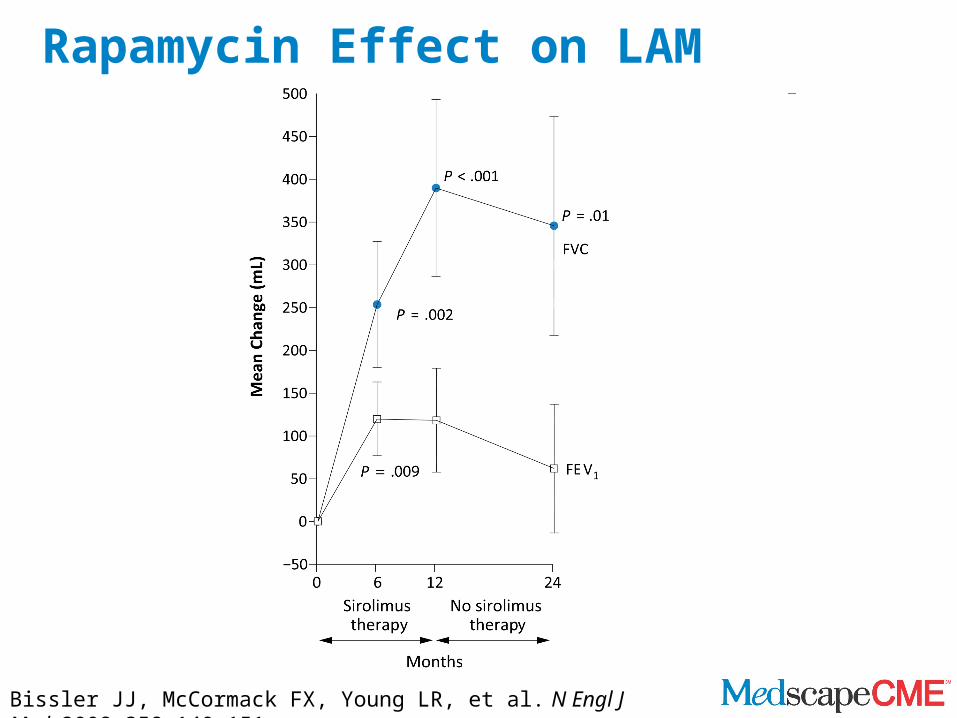
Rapamycin Effect on LAM
Bissler JJ, McCormack FX, Young LR, et al. N Engl J Med. 2008;358:140-151.
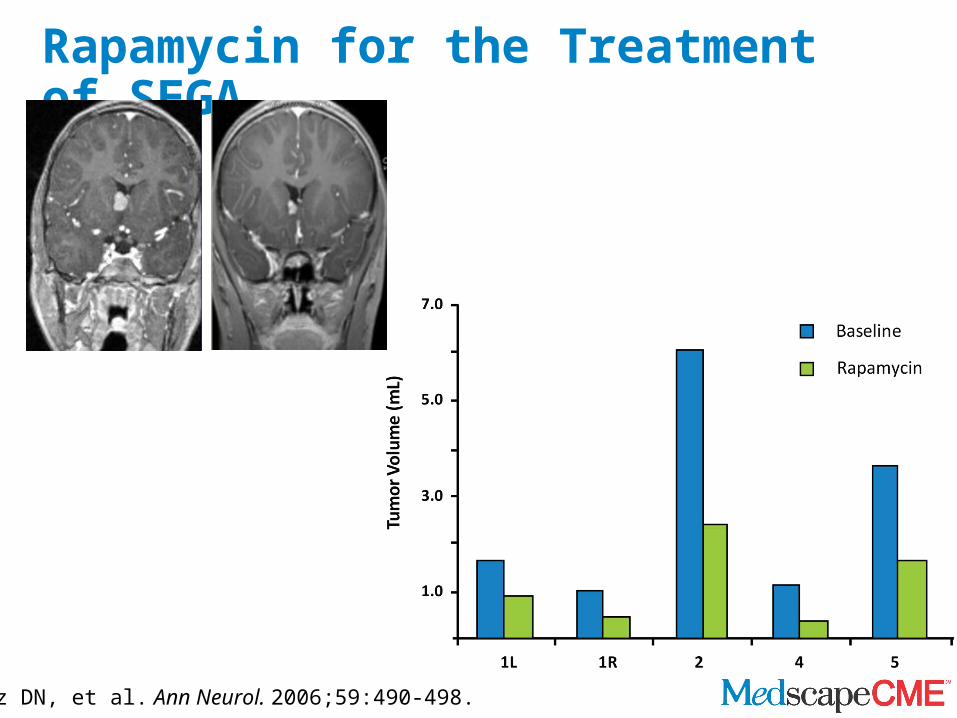
Rapamycin for the Treatment of SEGA
Franz DN, et al. Ann Neurol. 2006;59:490-498.
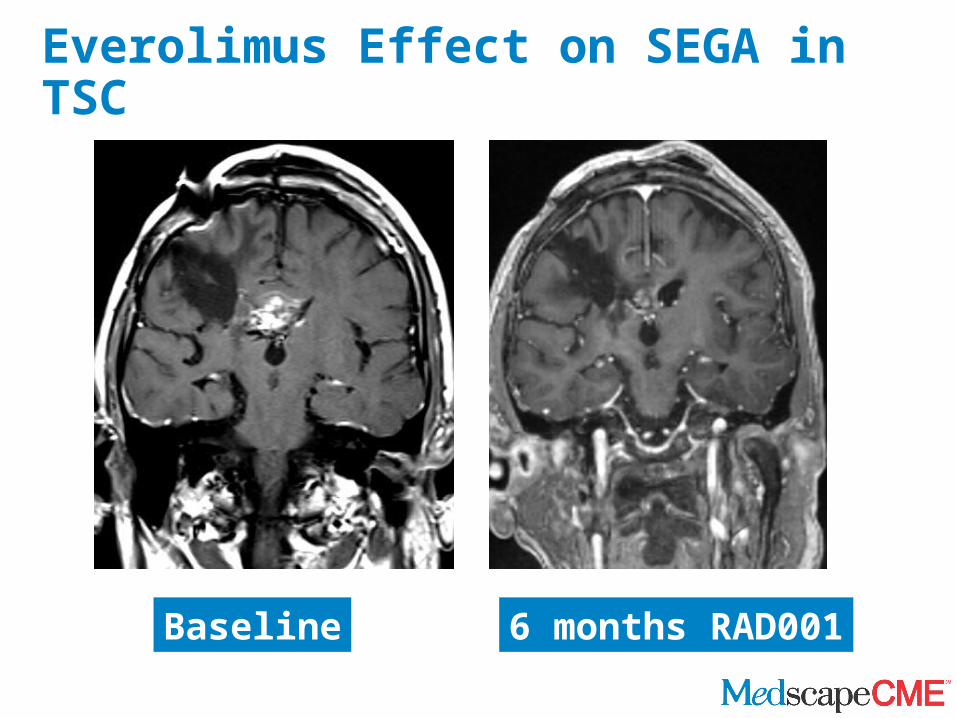
Everolimus Effect on SEGA in TSC
Baseline 6 months RAD001
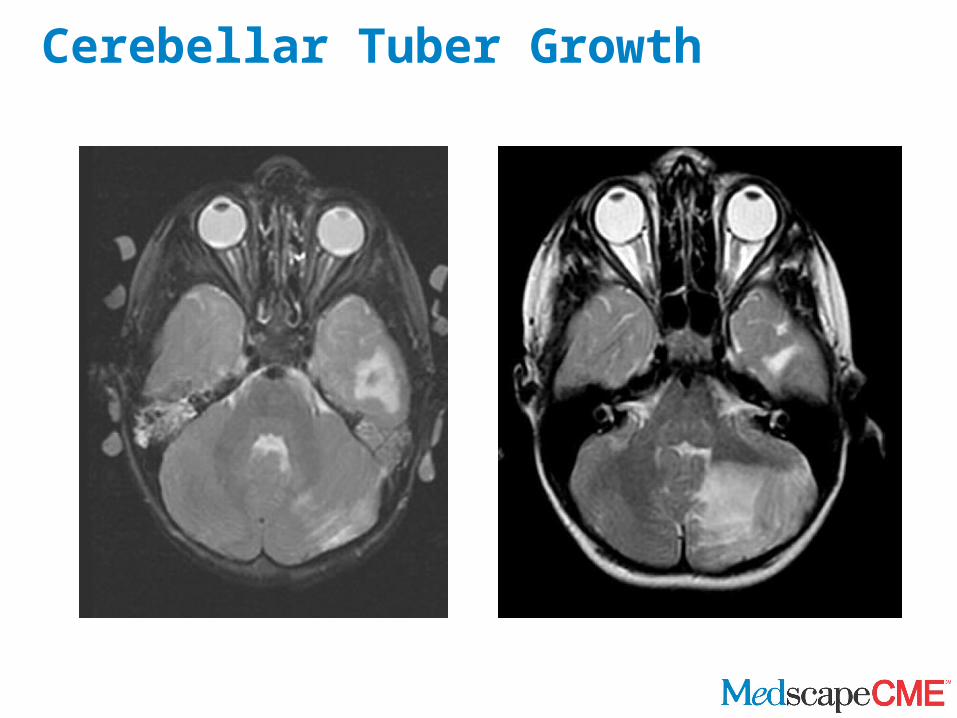
Cerebellar Tuber Growth
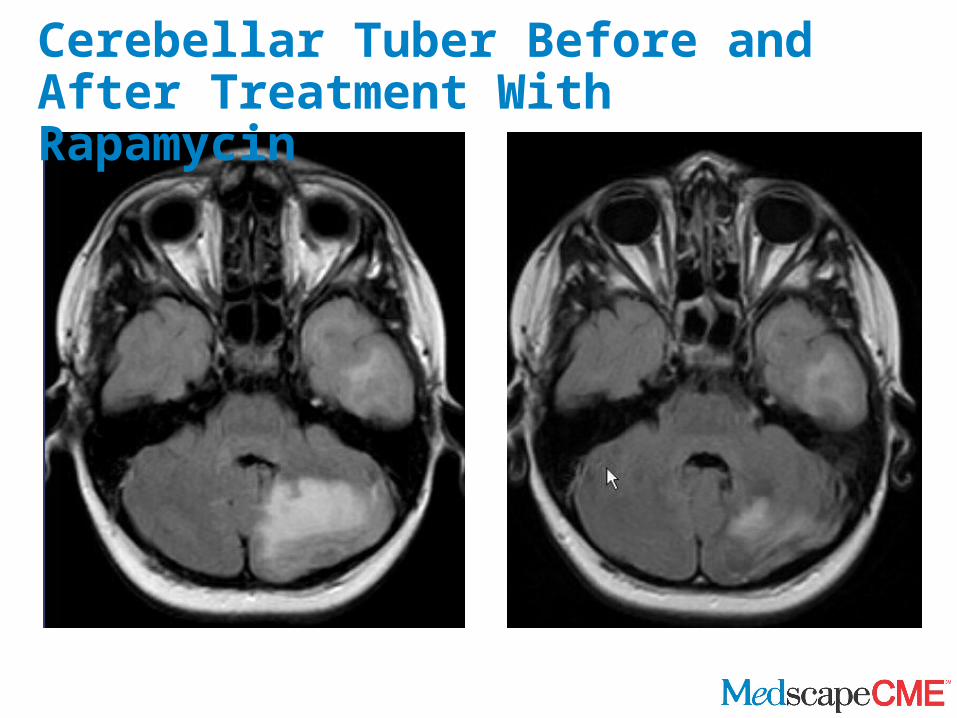
Cerebellar Tuber Before and After Treatment With Rapamycin
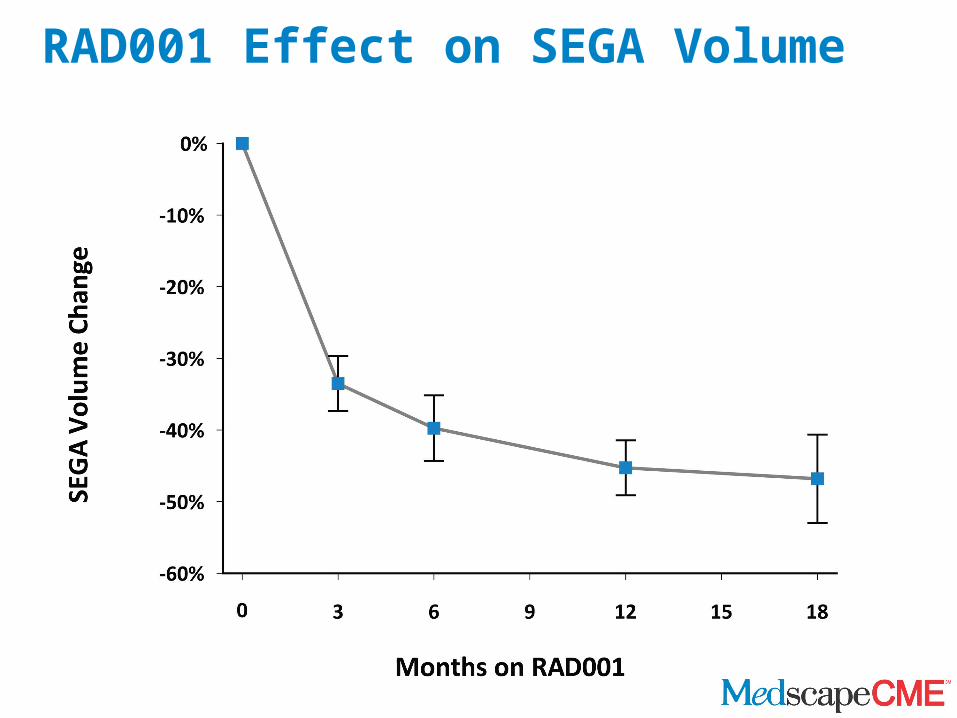
RAD001 Effect on SEGA Volume
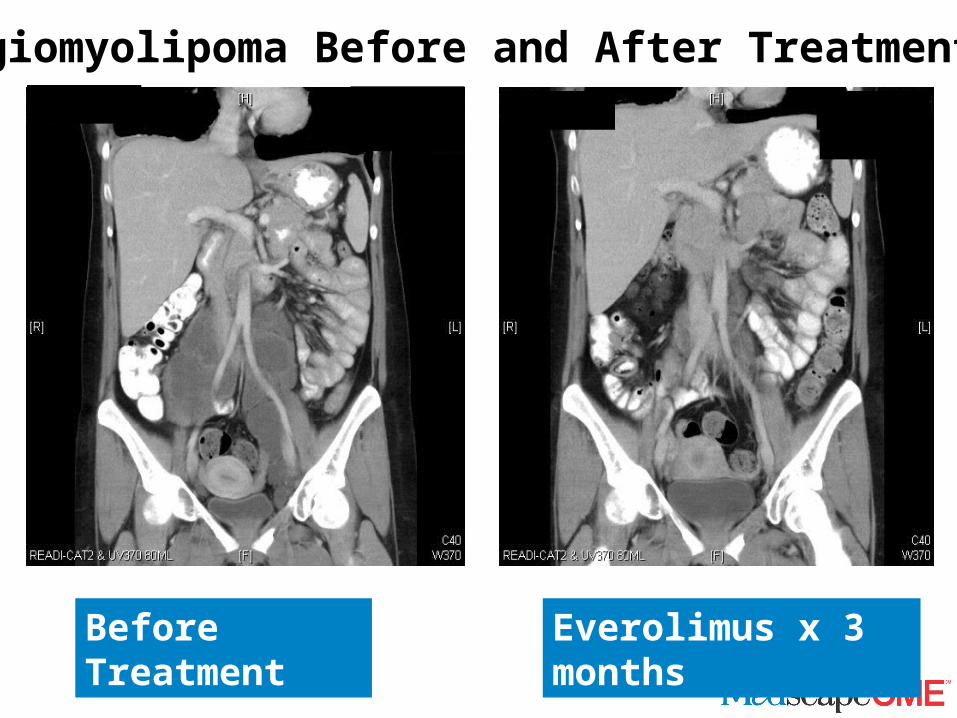
Before Treatment Everolimus x 3 months
Angiomyolipoma Before and After Treatment
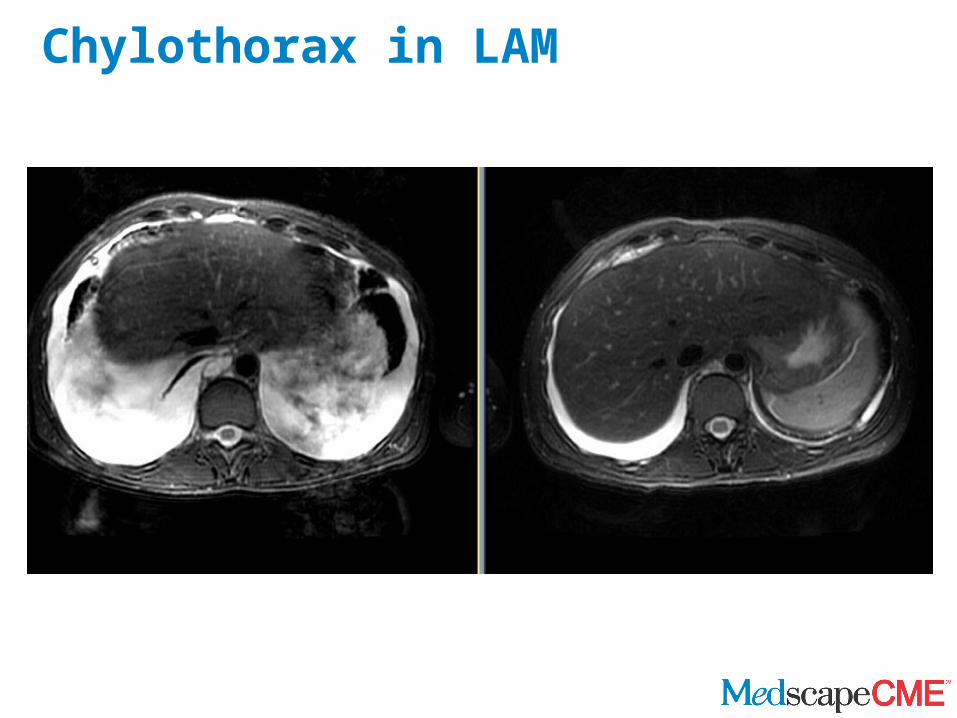
Chylothorax in LAM
Current Clinical Trials Related to TSC
• EXIST-1: Efficacy and Safety of RAD001 in Patients of All Ages With Subependymal Giant Cell Astrocytoma Associated With Tuberous Sclerosis Complex (TSC)
• EXIST-2: Efficacy and Safety of RAD001 in Patients 18 Years and Over With Angiomyolipoma Associated With Either Tuberous Sclerosis Complex (TSC) or Sporadic Lymphangioleiomyomatosis (LAM)
• MILES: Efficacy and Safety of Rapamycin in Patients with Tuberous Sclerosis Complex Lymphangioleiomyomatosis (TSC-LAM) or Sporadic Lymphangioleiomyomatosis (S-LAM)
• Long-term Follow-Up for RAD001 Therapy of Angiomyolipomata in Patients With Tuberous Sclerosis Complex (TSC) and Sporadic Lymphangioleiomyomatosis (LAM)
• Long-term Follow-Up for RAD001 Therapy of Subependymal Giant Cell Astrocytoma in Patients With Tuberous Sclerosis Complex (TSC)
Current Clinical Trials Related to TSC (cont)
• Efficacy and Safety of Aromatase Inhibition for Tuberous Sclerosis Complex Lymphangioleiomyomatosis (TSC-LAM) or Sporadic Lymphangioleiomyomatosis (S-LAM)
• Study of Skin Tumors in Tuberous Sclerosis• Tuberous Sclerosis Complex Natural History Study:
Renal Manifestations• Study of the Disease Process of Lymphangioleiomyomatosis• Effect of Fasting on the Size of Abdominal Lymphatic Tumors
in Women• Role of Genetic Factors in the Development of Lung Disease
Summary
• Tuberous sclerosis is a multiorgan disorder with variable penetrance and severity
• Highest disease morbidity is associated with cerebral, renal, and pulmonary manifestations
• Molecular-based therapies using mTOR inhibitors are showing promise in treating patients with TSC
Thank you for participatingin this activity.
To proceed to the online CME test, click on the Earn CME Credit link on this page.