Embed Size (px)
Citation preview

Employer On-Site Clinics as Medical Homes
Payors, Plans, and Managed Care Practice Group
Mid-Year Luncheon
November 8, 2010
PRESENTERS:
Richard M. Luceri, M.D. Elise Dunitz Brennan
VP of Health Care Services Partner
JM Family Enterprises Inc. Doerner Saunders Daniel & Anderson LLP
120 Jim Moran Blvd. 320 S. Boston Avenue, Suite 500
Deerfield Beach, FL 33442 Tulsa, OK 74103
Telephone: (954) 363-6068 Telephone: (918) 591-5214
Fax: (954) 363-4258 Fax: (918) 925-5214
Email: [email protected] Email: [email protected]

2
Overview of the Presentation
Defining medical homes and why on-site clinics are appropriate for medical homes
Describing why corporate clinics are proliferating
Legal issues
Ways JM Family Enterprises provides chronic care management and functions as a medical home

3
Definition of Medical Homes
Continuity of care
Clinical information systems
Delivery system design
Decision support
Patient/family engagement
Coordination of care across providers and settings
Improved access to care

4
Typical Characteristics of Medical Homes Are Easily Provided at Employer On-Site Clinics
Open scheduling
Expanded access hours
Email communication
Patient tracking
Chronic care management
Personal health assessments and wellness initiatives
Performance reporting and improvement

5
Increased Emphasis on Medical Homes
PPACA
Medicaid Demonstration Programs
Medicare Home Demonstration from Tax Relief and Healthcare Act
of 2006 and Medicare Improvement for Patients and Provider Act
of 2008
NCQA accreditation standards in existence
The Joint Commission accreditation standards are forthcoming

PPACA’s Emphasis on Employer Wellness Programs Promotes On-site Clinics as Medical Homes
Grants to small employers to provide comprehensive workplace wellness
programs for FY2011-2015.
Comprehensive workplace programs include health awareness initiatives
such as HRAs, efforts to maximize employee involvement, initiatives to
change unhealthy behaviors, and workplace policies to encourage healthy
lifestyles.
CDC to study and evaluate employer wellness programs including
comprehensive workplace chronic disease management and health
promotion programs.
6

Why Corporate Clinics are Proliferating
Healthcare costs are out of control
Healthcare delivery system is broken
7

8
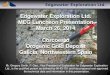
Employers View of Costs Associated with Reform
7.0%8.0%
8.9% 8.3%
Mean Median Mean Median
(2010 Sample Size=61; 2011 Sample Size=38)Source: National Business Group on Health, Large Employers’ 2011 Health Plan Design
Changes, August 2010.
2010 2011
3%
30%
12%
13%
28%
13%
N/A -- Already incompliance
Don't know
Increase by 5% or more
Increase by 3-4%
Increase by 1-2%
Increase by less than 1%
Source: Mercer, Health Care Reform – Sizing up the Challenge, 2010.
Budgeted Changes 2010-2011
Employer Estimates of Healthcare Costs

Even the Government Expects Higher Costs
The rate of increase in total U.S. healthcare spending will be little changed by the healthcare overhaul, according to federal economists
Healthcare spending as a percentage of GDP
CMS Office of the Actuary Sept. 8, 2010
Projected
With effects of HC reform
Prior to HC reform

10
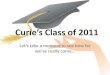
Employer Reactions to Healthcare Reform
Source: Towers Watson, Health Care Reform:, 2010.
88%
74%
33%
20%
12% 12%7%
11%
IncreaseEmployees'
Costs
Reduce healthbenefits and
programs
Absorb costs inthe business
Pass on increseto consumers
Eliminate orreduce
wellness/healthpromotionprograms
Reduceemployment
Reduce employercontributions toretirement plans
Reducesalaries/direct
compensations

U.S. Healthcare System is Broken
Care is fragmented and not coordinated Over-consumption of services
Patient side: no “skin in the game” (more is better) Physician side: fee-for-service rewards volume not quality; physicians are
paid for what they order not for what they know; fear of lawsuits; etc. Primary care physician shortage, projected to be even lower with ACA
No time to be the “trusted” physician No coordination with other providers, specialists Earlier referral to specialists (with regional differences based on local
expectations and sophistication) Lowest paid provider
IT deficiencies low rate of electronic record adoption and sharing, exaggerated HIPAA
interpretation, little interoperability, etc.
11

Reality: Patients Do Not Receive Recommended Care
12
McGlynn et al “The Quality of Health Care Delivered to Adults in the United States” NEJM June 26, 2003Health Study by the RAND Corporation (supported by the Robert Wood Johnson Foundation and the Veterans Affairs Health Administration);

Employers to the Rescue:Reasons for Success of Onsite Clinics
Better opportunities to control costs: Shift to less expensive but patient-oriented primary care Introduce “consumerism” in controlled setting:
Focus on generic drugs, annual physical exams, etc. Value-based health plan design
Good health is good for business: Physician-patient relationship is the cornerstone of care Emphasis on screening, wellness programs, chronic disease
management Reduced productivity losses and absence Employee retention, work-life balance, employer of choice, etc.
13

Legal Issues
Corporate practice of medicine issues
Licensing issues
Privacy issues
ERISA applicability
Relationship to HSAs
HRAs & GINA
Liability Issues
14

Corporate Practice of Medicine Issues
Medical home is a physician-driven model in which the physician
leads a team that takes collective responsibility for a patient.
Problem with employment of physicians in some states so there is a
need to link with a captive PC.
On-site clinics frequently rely on physician extenders (APNs and
PAs) to decrease costs.
On-site clinics need to balance reliance on physician extenders with
medical home concept that physicians are pivotal.
15

Licensing Issues Involving Physician Extenders
PAs are frequently licensed by medical licensing statutes, so corporate practice of medicine prohibition may apply.
APNs are typically the only type of nurses that can diagnose and treat.
APNs may not have prescriptive authority. Typically neither a doctor nor a physician extender can rely on the
patient assessment by an RN and make a medical diagnosis if he or she does not see the patient directly. Further, a RN can not take orders from a doctor unless: The doctor has seen the patient; and Has prepared a medical protocol.
16

Licensing Issues Involving Drug Distribution
Chronic disease management includes medication management
and employers are desiring to purchase and dispense drugs directly
to employees to lower costs.
Distribution of medication through employer facilities may
necessitate wholesale or distribution pharmacy licensing issues
depending on state law.
In some states, properly registered physicians can dispense
non-schedule medicine but on-site clinics frequently warehouse
drugs.
17

Privacy Issues
Covered entity status of employer health plan, but not
employer, so free exchange of PHI between on-site clinic
and health plan must be shielded from employer.
Ease of access to patients: emails and quick and
frequent meetings when healthcare providers reside at
patient’s place of location necessitates enhanced HIPAA
and HITECH responsibilities.
18

Privacy Issues
State privacy laws, Americans with Disabilities Act, and Family
and Medical Leave Act may apply to PHI.
Employer health plan and on-site clinics are both covered
entities, and this differs from typical arrangements when TPA
is business associate of employer health plan so aggregate
collection of PHI for plan administration purposes needs to be
carefully monitored.
19

Privacy Issues
Confidentiality obligations of the on-site provider differ for
the treatment of job related injuries versus other health
care needs. Most state workers compensation laws allow
employer access to treating physician report.
May need to consider enhanced or coordinated privacy
policies for “trust.”
20

ERISA Applicability
Maintenance on the premises of an employer facility of treatment for
minor injuries or illness or rendering first aid in the case of accidents
occurring during working hours is not an employee welfare benefit
plan pursuant to DOL section 2510.3-1(c).
A wellness program is any program designed to promote health or
prevent disease. DOL section 2590.702(f).
When an on-site clinic provides chronic care coordination it
becomes a wellness program subject to ERISA plan and notification
requirements, HIPAA nondiscrimination rules, and COBRA.
21

Applicability to HSAs
IRS Notice 2008-59 (Q&A 10) allows an employer or dependent to
have an HSA and use an employee on-site clinic that is either free
or charges below fair market value, if the employee or dependent
does not receive significant benefits in the nature of medical care.
A hospital that permits its employees to receive all medical care at
its facilities for no charge is providing significant care and the
employees are not eligible for HSAs.
22

Notice 2008-59 Guidance on Significant Benefits
Physicals and immunizations are not considered significant benefits.
Injecting antigens provided by employees is not considered significant benefits.
Providing aspirin and other non-prescription pain relievers is not considered significant benefits.
Query: Does the nature of a medical home necessitate a provision of more than significant benefits?
23

PPACA Increases Confusion
Query: Are preventive screenings broad enough to include annual
physicals, basic tests, and services typically provided in an
outpatient physician’s office to manage chronic conditions, which is
implicit in the medical home concept.
PPACA provides some indication that management of chronic
problems (such as regular blood pressure checks) fall within the
concept of preventive screenings but need further guidance.
24

PPACA Increases Confusion
Tests as to whether the services provided by on-site clinic are in the
nature of preventive and primary or treatment for injuries and
illnesses contracted at the employer’s worksite versus management
of specialist healthcare needs.
Once on-site clinics enter into employer direct service agreements
with hospitals or specialists movement to significant benefits.
For now most employees with an HSA are charged a nominal fee for
on-site clinic services, but this does not resolve the exemption from
ERISA issue.
25

Future Issue
On-Site medical clinics will be treated as a group health plan coverage for purposes of the excise tax that goes into effect in 2018 on “Cadillac Plans” if they offer more than a de minimus amount of medical care to employees in executive physical programs. This is in the technical explanation of the revenue provisions of
the Reconciliation Act of 2010 as amended, in combination with the Patient Protection and Affordable Care Act (JCX-18-10), 64 (March 21, 2010).
This explanation does not define de minimus medical care.
26

HRAs and GINA
Title I prohibits health plans from discriminating against covered
individuals based on genetic information.
Title II prohibits employers from discriminating against employees
based on genetic information.
Genetic Information includes family medical history and information
on individuals’ and family members’ genetic tests and genetic
services.
Federal regulations at 74 Fed Reg 51664 (October 7, 2009).
27

HRAs and GINA
Fundamental to the concept of Medical Home is collecting sufficient information through health risk assessments and/or biometric testing, which enable the provider to manage chronic illness or provide preventive care.
The Medical Home concept incorporates wellness initiatives which are governed by the HIPAA nondiscrimination rules that prohibit discrimination in the provision of wellness programs based on participant’s illness or medical condition (29 CFR § 2590).
28

HRAs and GINA Wellness programs that provide rewards for completing HRAs that
request genetic information, including family medical history, violate the prohibition against requesting genetic information for underwriting purposes. This is the result even if the rewards are not based on the outcome of the assessment, which otherwise would not violate the 2006 final HIPAA nondiscrimination rules regarding wellness programs. Some employers give rewards for completing HRAs that do not solicit genetic information.
Some employers make completion of HRAs completely voluntary. Query: When a turn-key on-site clinic or independent contractor
seeks completion of HRA, is this an action of the employer?
29

Professional Liability
The professional must render care with the same degree of care as a reasonable member of that profession in similar circumstances would render in the community.
Query: What is the community standard for on-site clinics? Is it a different standard?
Does the standard differ for independent contractor, employee, turn-key operation, or captive PC?
Possible apparent authority or ostensible agency issues as raised against non-staff model HMOs.
30

JM FAMILY EXPERIENCE WITH “MEDICAL HOME”
31

About JM Family Enterprises, Inc.
Diversified private automotive company
Founded in 1968 by automotive legend Jim Moran
Led by President and CEO Colin Brown
Approximately 4,000 associates
Headquarters in Deerfield Beach, FL
Major business operations throughout U.S. and Canada
32

Notable JM Family Rankings
No. 30 on list of America’s Largest Private
Companies
No. 28 on “100 Best Companies to Work For” list; ranked for 12 consecutive years
No. 2 on list of Florida’s Largest Private Companies
No. 3 on list of “100 Best Places to Work in IT”
33
About JM Family Enterprises, Inc.

On-site Health & Wellness Centers
Health & Wellness Centers
4,000 Associates10,000 Covered Lives
34

Our Leaders “Get It”
CEO
Total Rewards
Healthcare Services
CAO/HR
35

Overall Medical Home Strategy: Engagement, Wellness, Prevention
Core ProgramsWeight Management
Physical Activity
Smoking Cessation
Risk Reduction
Associate EngagementStay Healthy
Accept responsibility for one’s own health
Better understand how to consume healthcare
Coordinate Care
“Medical Home”Education
Coaching
Manage chronic disease
Prevention Promote healthy
lifestyle
Promote targeted screening
Health Risk Assessment
36

On-site Health & Wellness Centers
Staff: Primary care/IM physicians, gynecologists (full and part-time) Full-time registered nurses Physical therapist on-site or locally accessible in major facilities Contracted registered dietitians and fitness instructors
Patients served: Benefit plan members including associates, spouses, children >15 Wellness/prevention programs are open to all
Schedule options: By appointment “Fast Track” minor care (viewed as a “stay healthy” opportunity) Virtual waiting rooms
37

Wellness & Prevention Programs
Smoking cessation Weight management Cancer screening
Breast Prostate Colorectal others
Vaccinations Psychological counseling Nutritional consultations Onsite fitness programs tailored to location:
Gyms, swimming pool Exercise classes, Pilates, Boot Camp, etc.
38

Coordinated Care (DM) Programs
Core programs: Diabetes Hypertension Hyperlipidemia
Always available: Weight management Smoking cessation Behavioral health
Planned: Musculo-skeletal health
39

We “Drive” Associates and Families to Our Health & Wellness Centers
No-cost access to H&W Centers (except HAS plan) No deductibles
All services performed on company time “Free” ancillary lab and imaging services
Local vendor contracting High-touch/quality services
“Free” screening specialty visits Well-woman exams by GYN Dermatology checks
“Free” starter medications, course of antibiotics
40

“Modified” HRA with biometric data: 72% participation rate in pilot of > 1,000 associates without incentives Generated multiple annual and wellness visits, nurse coaching,
teachable moments
LifeSteps weight management program: 3-components: behavior modification, proper nutrition, and activity Remote locations tested first Mentoring from previous participants is maintaining engagement Success prompted “waiting list” for future enrollees and need for
additional personnel We pay for programs; participants maintain memberships through
continued engagement and commitment
We Test Our Programs Through Pilot Studies
41

Partnerships with area hospitals: Employers are good corporate community partners for hospitals Hospital revenue streams and margins are challenged Grants are possible and should be pursued:
We earned a fitness and smoking cessation grant in one location $1.5 M grant proposal is being submitted with another hospital system for
wellness partnerships Opportunities for integrated delivery systems (ACO) and other
opportunities through PPACA Local specialty networks
Reinforce coordinated care concept Assure quality Coordinated by our physicians
We Promote Partnerships WithLocal Hospitals and Provider Groups
42

Preliminary results We’ve begun bending the cost curve Associate engagement has increased
Future direction Continued focus on overall health and wellness of our
associates Expand onsite or near-site services Telehealth in certain locations
Modulate benefit design in conjunction with healthcare services
What’s Next?
43

44
Employer On-Site Clinics As Medical Homes © 2010 is published by the American Health Lawyers Association. All rights reserved. No part of this publication may be reproduced in any form except by prior written permission from the publisher. Printed in the United States of America. Any views or advice offered in this publication are those of its authors and should not be construed as the position of the American Health Lawyers Association. “This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is provided with the understanding that the publisher is not engaged in rendering legal or other professional services. If legal advice or other expert assistance is required, the services of a competent professional person should be sought”—from a declaration of the American Bar Association