Embed Size (px)
Citation preview

267
ABSTRACT. Bariatric surgery is nowadays an effective thera-peutic option for morbid obesity. Endocrinologists may thushave a growing opportunity to diagnose and treat obese pa-tients eligible for surgery in pre- and post-operative phase.This requires a better understanding of endocrine changescaused by either obesity or weight loss surgery. Despite thelarge number of studies available in literature, only limitedwell-designed clinical trials have been performed so far toinvestigate changes of endocrine axes following bariatric pro-cedures. There are still areas of unclear results such as fe-
male and male fertility, however, weight loss after bariatricsurgery is considered to be associated with favorable effectson most endocrine axes. The aim of this clinical review is tooverview the available literature on the effects of weight lossafter bariatric surgery on the endocrine systems to suggestthe most appropriate pre- and post-operative managementof obese patients undergoing bariatric surgery in terms of“endocrine” health.(J. Endocrinol. Invest. 36: 267-279, 2013)©2013, Editrice Kurtis
INTRODUCTION
Obese patients are affected with several endocrine ab-normalities (1). A recent survey reported that, apart fromType 2 diabetes mellitus, the overall prevalence of en-docrinopathy was 47.4% in morbidly obese patientsscheduled for bariatric surgery, with 16.3% of newly di-agnosed endocrine diseases (2). Though most of theendocrine changes are secondary to obesity, and thusreversible (partially or totally) after substantial and sta-ble weight loss, there is increasing evidence that en-docrine alterations may also contribute to the develop-ment of obesity as part of a maladaptive homeostaticmechanism that promote weight gain and hamperweight loss (3-5).Bariatric surgery, associated to a careful pre- and post-operative management (6), has shown so far to be amore effective therapeutic option than conventionaltreatment in eligible obese patients in terms of sus-tained weight loss, improvement of the quality of life,and reduction of morbidity and mortality (7). Techniquesof bariatric surgery can be divided into two groups: mal-absorptive procedures, such as biliopancreatic diver-sion (BPD), and restrictive procedures, such as laparo-scopic adjustable gastric banding (LAGB), and sleevegastrectomy, with a growing variety of procedures usingboth malabsorptive and restrictive over the years, suchas the Roux-en-Y gastric bypass (RYGB) and BPD withduodenal switch. Malabsorptive procedures induce de-
creased absorption of nutrients and calories by short-ening the functional length of the small intestine. Re-strictive procedures induce weight loss by reducing thefood storage capacity of the stomach; in particular,sleeve gastrectomy provides rapid improvement ofType 2 diabetes mellitus with a very low rate of com-plications (8), and is thought to provide additional ben-efit by decreasing secretion of the appetite-stimulatinghormone Ghrelin (9).The efficacy of bariatric surgery in ameliorating main obe-sity-related comorbidities, such as Type 2 diabetes, hy-pertension, dyslipidemia, and cancer, has so far provenlargely based on both randomized controlled trials (RCT)and cohort studies (10, 11). The favorable effects ofbariatric surgery on insulin sensitivity has been exten-sively reviewed in a previous issue of this Journal (12).Conversely, despite the large number of studies avail-able in literature, relatively few well-designed clinical tri-als have been performed to investigate the endocrinechanges after bariatric procedures. However, given theworldwide success of bariatric surgery, a better under-standing of these mechanisms is becoming particularlycompelling for endocrinologists and other physicians be-ing challenged by pre- and post-operative managementof obese patients eligible for surgery. Moreover, the eval-uation of accompanying endocrine changes after restric-tive or malabsorptive procedures may offer to investiga-tors an interesting opportunity to increase knowledge onthe endocrine effects on metabolism and body compo-sition, as well as adding to obese patients a motivation toopt for surgical weight loss.The aim of this clinical review is to analyze available lit-erature on the effects of weight loss after bariatric surgeryon the endocrine systems, attempting to suggest themost appropriate pre- and post-operative managementof obese patients undergoing bariatric surgery in terms of“endocrine” health.
Key-words: Bariatric surgery, endocrine axes.
Correspondence: S. Savastano, MD, Dipartimento di Medicina Clinica e Chirurgia,Sezione di Endocrinologia, Università Federico II di Napoli, Via S. Pansini 5 – 80131Napoli (Italy).
E-mail: [email protected]
Accepted January 14, 2013.
First published online February 27, 2013.
Endocrine changes (beyond diabetes) after bariatric surgeryin adult life
J. Endocrinol. Invest. 36: 267-279, 2013DOI: 10.3275/8880
S. Savastano1, C. Di Somma2, R. Pivonello1, G. Tarantino3, F. Orio4, V. Nedi1, and A. Colao1
1Sezione di Endocrinologia, Dipartimento di Medicina Clinica e Chirurgia, Università Federico II di Napoli; 2IRCCS FondazioneSDN Napoli; 3Sezione di Medicina Interna, Dipartimento di Medicina Clinica e Chirurgia, Università Federico II di Napoli;4Sezione di Endocrinologia, Università Parthenope di Napoli, Naples, Italy
SHORT REVIEW

Endocrine changes after bariatric surgery
268
LOW GH STATUS AND SURGICAL WEIGHT LOSSThe GH/IGF-I axis in obesityObesity and GH status shows multiple and bidirectionalrelationships (13). Adult patients with GH deficiency(GHD) have changes in body composition, glucose andlipid metabolism, cardiovascular risk profile, and bonemineral density (14), which are successfully reversed afterGH replacement therapy (15). On the other hand, obesi-ty, mainly abdominal obesity, is associated with a “func-tional” low GH status, with IGF-I levels normal, subnormalor even elevated (4, 5). The pathophysiological mecha-nism responsible for reduced GH secretion in obesity ismultifactorial. There are many data suggesting that, apartfrom overeating per se (16), a chronic state of somato-statin or insulin hypersecretion results in inhibition of GHrelease, whereas increased free fatty acid levels, as wellas a deficient ghrelin secretion, probably contribute tothe impaired GH secretion (17). We have previously re-ported that about 30% of morbidly obese patients, with-out any evidence of organic pituitary disease had a lowGH secretory status (5), using appropriate testing for di-agnosing GHD in obese subjects (18). Moreover, in-creased intra-myocellular and intra-hepatic lipid contenthas been accounted as further possible pathogeneticmechanism (19), consistent with the evidence of the as-sociation between low IGF-I status and hepatic steatosisin overweight/obese females (20).Although reversed after significant and sustained weightloss (21), the low GH status correlates with the obesephenotype, in that morbidly obese GHD patients showedsignificantly different body composition (5) and metabol-ic abnormalities (22) compared with their obese non-GHDcounterparts. Finally, in unselected obese adult patientsGH therapy at replacement doses has been shown to bebeneficial in decreasing visceral adiposity, increasing leanbody mass, improving lipid profile, without inducing sig-nificant weight loss or altering glucose tolerance in thelong term (23).
The GH/IGF-I axis after bariatric surgeryAfter bariatric surgery, GH secretion is expected to berestored based on the “functional” nature of low GH sta-tus in obesity. However, among the post-surgical en-
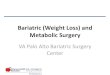
docrine changes, those related to the GH/IGF-I axis havebeen poorly studied. Valera Mora et al. (24) found bothfasting and stimulated GH levels significantly increased18 months after BPD. Accordingly, Camastra et al. (25)reported that low GH levels increased to near-normallevels 6 months after BPD in severely obese non-diabeticpatients. Partial recovery of GH secretion was observedalso after RYGB (26). In contrast, IGF-I secretion wasshown to persist at low levels, likely due to the post-op-erative state of semi-starvation (27) and/or to thecatabolic state induced by malabsorptive surgical pro-cedure such as BPD (28). Similarly, Engström et al. (29)found that surgically induced weight loss after RYGB on-ly partially restored IGF-I secretion. In a prospectivestudy that we conducted in 72 pre-menopausal obesewomen 6 months after LAGB, when the initial catabolicstate should have already been overcome, about 20%of obese women were found to be GH and IGF-I defi-cient and another fifth had IGF-I levels still below thenormal range calculated according with age normativeranges (30).Interestingly, excess of both weight loss and fat mass losswere higher in patients who normalized their GH/IGF-Iaxis after surgery than in those who did not. The dissoci-ation between GH and IGF-I, shown after non-surgicalweight loss (21), has been confirmed by our group in alarger series of patients who have undergone LAGB(Table 1) (31), and by others (27). In particular, Mitter-berger et al. (27) found that 4 yr of severe caloric restric-tion induced LAGB and diet led to significantly lower IGF-I serum levels in formerly obese women compared withnormal-weight women, although they reported that fast-ing GH serum levels were considerably lower comparedwith both normal weight and overweight controls. Thus,the possibility that subtle but persistent failures of theGH/IGF-I axis as a possible maladaptive epiphenomenon,might negatively influence the response to any surgicalprocedure for obesity, should be considered.Based on the impairment of GH/IGF-I status afterbariatric surgery, the potential favorable influence of GHreplacement was investigated in a group of morbidlyobese female patients who underwent LAGB (32). Theaim of treatment was to prevent loss of lean body mass
GH GH p IGF-I IGF-I pdeficient sufficient deficient/insufficient normal
No. (%) 26 (25.0) 78 (75.0) 32 (30.8) 72 (69.2)
Body mass indexkg/m² 37.4±3.4 35.3±5.7 0.079 36.6±4.0 35.5±5.8 0.33Percent change –15.8±3.2 –19.6±4.9 <0.0001 –16.3±3.7 –19.7±4.9 <0.0001
Waist circumferencecm 115.1±8.1 104.9±9.2 <0.0001 112.9±7.7 105.0±9.9 <0.0001Percent change –6.5±2.5 –13.2±7.0 <0.0001 –7.4±4.1 –13.3±7.1 0.49
Excess body weight losskg 18.6±3.7 22.2±5.9 0.004 19.0±4.3 22.3±5.8 0.0005Percent change 31.9±7.1 41.0±12.4 <0.0001 34.1±8.9 40.8±12.2 0.0006
Fat mass (%) 48.8±7.0 41.0±9.7 0.003 47.8±6.9 40.8±10.0 <0.0001
Free fat mass (%) 51.2±7.0 58.9±9.7 0.003 52.2±6.9 59.2±10.0 <0.0001
Data drawn from (31).
Table 1 - The persistence of a low GH/IGF-I status 6 months after bariatric surgery is associated to lower post-operative percent changein body mass index, waist circumference, excess of body weight loss, and with higher fat mass and lower free fat mass percentages.

S. Savastano, C. Di Somma, R. Pivonello, et al.
269
during the early post-operative period, a crucial eventto ensure an optimal outcome of surgery in terms oflong-lasting body weight loss (32). Indeed, at the endof the study we found the same amount of excess ofweight loss in patients treated with GH as in those whodid not, but in the former the weight loss was mainly dueto fat mass loss, with a significant sparing of lean bodymass. The beneficial effects of GH treatment were alsoaccompanied by improvements of lipid profile and in-sulin sensitivity. These data prompt the exploration ofGH replacement in those patients with subnormal GHand IGF-I secretion after bariatric surgery to optimize fatloss while presenving lean mass. Of note, it is relevant toreport a case of an acromegalic woman with a long con-dition of morbid obesity who presented a worsening ofbiochemical GH/IGF-I axis after BPD along with the res-olution of obesity, likely secondary to the resolution ofType 2 diabetes and sleep apnea syndrome, or tochanges in ghrelin levels (33).
ConclusionsThe low GH/IGF-I secretion in obesity may partially berestored after bariatric surgery. The evaluation of theGH/IGF-I axis may be a reliable method to identify pre-operatively those patients who have a worse obese phe-notype and will not ensure an optimal surgery outcome.Thus, the “functional” low GH/IGF-I axis status in obesi-ty could represent the rationale to replace with GH obesesubjects, at least until improvement of body compositionand obesity-related metabolic sequelae might reversethe central and/or peripheral alterations in GH secretion.
THYROID FUNCTION AND SURGICAL WEIGHT LOSSThyroid dysfunction in obesityDespite the critical role of thyroid hormones in regulat-ing body weight mainly via energy metabolism and ther-mogenesis, glucose and lipid metabolism, food intake,and the oxydation of fatty acids, studies on thyroid func-tion in obesity yielded conflicting results. A possible ex-planation accounting for this evidence might be that,besides iodine intake, age, and sex, the reference rangefor serum concentration of thyroid hormones does nottake into account a number of adjunctive confounders,like body weight and the caloric content as well as thecomposition of the diet, specifically, the carbohydratecontent (34), that are commonly modified among diet-ing patients. Thus, “new” reference ranges might beconsidered, almost adjusted for the subject’s weight.An increase in TSH levels was observed among the par-ticipants of the Framingham Offspring Study in bothsexes along with body weight gain, although within thereference range (35). Overall, there is an agreement thatin euthyroid obese individuals not only serum TSH, butalso free T3 (FT3) levels are usually in the upper limit (orslightly over it) of the normal range, whereas free T4(FT4) remains unchanged (36). The increase in TSH andFT3 levels, that is independent of iodine deficiency orautoimmune thyroiditis (37), is positively associated withbody mass index (BMI), waist circumference, and fat ac-cumulation as well (38), and may represents an adap-tive phenomenon to supply the high thermogenesis re-
quired by the augmented fat amount (39). Moreover,an impaired regulation of TSH secretion by FT3 is asso-ciated in obese individuals as a result of abnormalitiesin leptin regulatory effect on TSH secretion and the re-setting of their central thyrostat (36), or as a conse-quence of leptin-mediated increased susceptibility todevelop thyroid autoimmunity (40). Furthermore, a con-dition of peripheral thyroid hormone resistance hasbeen described due to a reduced expression of bothTSH and thyroid hormone receptor on adipocytes ofobese vs lean individuals with subsequent down-regu-lation thyroid hormone action (41).Overall, as expected, the 24-h TSH secretion and FT3 lev-els in obese women are reduced after weight loss in-duced by caloric restriction. This evidence, indirectly sup-porting that obesity causes TSH elevation rather than viceversa, has been also related to post-operative changesin leptin secretion (42). The decline of TSH release andFT3 concentrations may contribute to the compensatoryreductions of 24-h energy expenditure and catabolismthat typically accompany weight loss (42). However, al-though protective against the perils of famine in ancienttimes, these adaptive changes may contribute to ham-per weight loss attempts in current times of plenty (42).
Thyroid axis after bariatric surgeryLimited studies evaluated thyroid function after surgicalweight loss and reported conflicting results. Vettor et al.(43) observed a fall in both FT3 and FT4 in spite of no sig-nificant changes in TSH levels 18 months after BPD, alongwith the decline in leptin levels. Additionally, changes inboth FT3 and lean body mass were significantly correlat-ed with lower 24-h energy expenditure, one of the mech-anisms implicated in weight regain after weight loss (44).In line with this study, Dall’Asta et al. (45) reported thatweight loss 2 yr after LAGB, a procedure that does not al-ter iodine absorption, induced a decrease in FT3 andFT3/FT4 ratio of 15% and 20%, respectively, while TSHremained steady. To explain these results, the authorssuggested that increased hypothalamic activity of type-2 deiodinase may account for the lack of TSH response toFT3 decline, similarly to findings reported during caloricrestriction (46). More recently, a large survey in 433 con-secutive morbidly obese patients before and after dif-ferent bariatric surgery confirmed that TSH levels de-creased during the post-operative follow-up though re-maining in the reference range (47).
L-T4 replacement therapy after bariatric surgeryA relevant issue is played by possible changes in ab-sorption and metabolism of replacement dose of L-T4 informerly hypothyroid patients following bariatric surgery.Despite the expected increase due to a possible post-operative malabsorption, Segal et al. (48) reported thathypothyroid patients after bariatric surgery required asmall decrease in daily dose of L-T4. In this respect, tak-ing also into account the stronger association betweenL-T4 dose with lean body mass than with fat mass (49), itis conceivable that post-operative lower daily L-T4 dosedepends on combined effect of changes in energy re-quirement and loss of lean mass that almost constantly isassociated to weight loss.

Endocrine changes after bariatric surgery
270
ConclusionsIncreased TSH and FT3 levels in obese individuals couldidentify a form of hormone resistance similar to insulinresistance. Changes in TSH and FT3 levels may also resultfrom the persistent effects of the caloric restriction ratherthan from loss of body weight. The understanding ofthese changes, as expression of complex adaptive mech-anisms contributing for the compensatory reduction of24-h energy expenditure associated with weight loss, iscrucial to prevent weight regain and further supports theimportance of the association of a moderately caloric re-striction in the post-operative management patients whohave undergone bariatric surgery. Fine-tuning adjust-ments of L-T4 replacement may be required as the com-bined consequence of possible changes in oral drug ab-sorption and reduction in lean body mass after surgicalweight loss.
HYPOTHALAMIC-PITUITARY-ADRENAL AXISAND SURGICAL WEIGHT LOSSAdrenal dysfunction in obesityThere are well-recognized similarities between obesityand Cushing´s syndrome. However, circulating levels ofcortisol, the natural ligand activating the glucocorticoidreceptor, are not consistently elevated in obese subjects,whereas elevated free urinary cortisol excretion are fre-quently found (50). In fact, obesity is associated to an in-crease in cortisol production rate, with a likely contribu-tion of stress-related (51) and inflammatory mechanisms(52). In addition, obese subjects have demonstrated anenhanced metabolic clearance rate (53), and an increasedreactivation of cortisone to cortisol shift mediated by 11β-hydroxysteroid dehydrogenase (HSD) type 1 in adiposetissue, a hormone known to cause obesity in both humanand animal studies (54).Apart the well-known effects on glucose and fatty acidmetabolism, cortisol exerts major effects either on adi-pose tissue, by increasing both lipid accumulation andmobilization, and on lean body mass, by enhancing pro-tein catabolism. Cortisol increases visceral fat more thansubcutaneous fat because of increased cell density andmore glucocorticoid receptors in abdominal adipose tis-sue (55). This generates a vicious circle, where the in-creased production of cortisol in the visceral adipose isresponsible for either higher differentiation of localadipocytes and enhanced delivery of glucocorticoids tothe liver via the portal vein, generating a condition knownas “Cushing’s disease of the omentum” (56). Althoughcortisol metabolism abnormalities are considered to be aconsequence rather than a cause of obesity, these alter-ations have been implicated as pathophysiological me-diators in idiopathic obesity and its detrimental metabol-ic consequences, including metabolic syndrome (50) andincreased cardiovascular mortality (57). The frequent clus-tering of obesity with other long-term consequences ofcortisol excess, i.e. diabetes, hypertension, and osteo-porosis, suggests the presence in obese subjects of asubclinical hypercortisolism, a condition of biochemicalcortisol excess without the classical signs or symptomsof overt hypercortisolism (58). It is well known also thatlow levels of DHEA-S, the major steroidal products of the
adrenal gland, may be frequently found in obesity (59),due to the selective insulin-dependent impairment of the17,20 lyase activity, the key enzyme in the conversion ofpregnenolone into DHEA (60). In this context, due to theanti-glucocorticoid properties of DHEAS associated withits weak androgenic effects in females, cortisol andDHEAS have also been proposed to act as an agonistand antagonist pair in the control of body composition,being higher cortisol/DHEAS ratio associated with in-creased protein catabolism (61).Despite that a chronic calorie restriction might enhanceglucocorticoid production as part of its potent anti-in-flammatory effect (62), long-term weight loss is mainlyassociated to beneficial changes in glucocorticoid metab-olism (63).
Adrenal axis after bariatric surgeryAlthough changes in glucocorticoid metabolism couldhave been expected after bariatric surgery, no conclu-sive data are so far available, likely owing to possiblevariables, such as methodological bias and periopera-tive stress affecting baseline measures of cortisol, dif-fering surgery procedures, degree of caloric restriction,and rate of post-operative weight loss. Plasma cortisollevels have been found to decrease significantly 6months after LAGB, without any further change at 14months, despite the progressive reduction in BMI,whereas DHEA-S remained at steady levels (64). In linewith this study, data from our group have confirmed thatin pre-menopausal morbidly obese women weight loss24 months after LAGB and a well-balanced low-caloriediet was associated with a significant decrease in corti-sol and insulin levels; by contrast, circulating levels ofDHEA-S showed a remarkable rise, being the highestpre-operative cortisol/DHEAS ratio a reliable marker ofthe most favorable post-operative changes in body com-position (65). Manco et al. (66) evidenced that after BPDfree cortisol, an indirect measure of biologically activefraction of total cortisol (67), increased in associationwith a simultaneous decrease in cortisol-binding globu-lin levels, as an adaptive mechanism related to the post-operative environmental changes, including the im-provement of the low-grade inflammatory status trig-gered by the sustained weight loss induced by BPD. Re-cently, Rask et al. (53) found that stable weight loss af-ter RYGB was followed by a reduced glucocorticoid pro-duction but also by a significant decrease excretion ofcortisol and cortisone metabolites, reflecting a down-regulation of the net activities of the cortisol-activatingenzyme 11β-HSD type 1. In this respect, the reducedglucocorticoid exposure in obese subjects may repre-sent a further possible contribution to the health bene-fits of bariatric surgery.In this overall reassuring scenario, it is interesting to re-port a case of unexplained adrenal insufficiency in a 35-yr-old woman with morbid obesity and amenorrhea oc-curring 5 yr later BPD. This patient presented with multi-ple vitamin and mineral deficiency, including vitamin D,and without any evidence of adrenal antibodies or alter-ation of the adrenal morphology at computed tomogra-phy scan. The authors speculated that the marked mal-absorption of bile acids following ileal bypass may have

S. Savastano, C. Di Somma, R. Pivonello, et al.
271
partly accounted for severe deficiencies in both vitaminD and steroid hormones due to a relative cholesterol de-ficiency resulting by the compensatory increase in hepaticbile acid synthesis, further highlighting the need for long-term follow-up post-BPD (68).A final consideration regards the role of the endocrinol-ogists in diagnosing a Cushing’s syndrome as a possibleendocrine disorder underlying simply obesity. Besidesthe obesity-related alterations in glucocorticoid metabo-lism, it has been recently reported that a proportion(9.3%) of patients with simple obesity were found to haveCushing’s syndrome (69); thus, taken into account theepidemic proportion of obesity throughout the world, anincreasing number of undiagnosed patients with Cush-ing’s syndrome might seek bariatric surgery. On the oth-er hand, two recently published surveys (2, 47) reporteda prevalence of undiagnosed Cushing’s syndrome below1% in morbidly obese patients scheduled for bariatricsurgery. Although rare, this prevalence is greater thanthat reported in the general population (70), undiagnosedCushing’s syndrome can present several major problemsboth in pre- and post-operative management of patientsundergoing a contra-indicated bariatric surgery (71). Infact, any delay in the diagnosis and the treatment ofthese patients may result in severe and irreversible co-morbidities owing to the combined harmful effects ofmalabsorption of a contraindicated and excess in en-dogenous glucocorticoid exposure (72).
ConclusionsAlthough the effects of surgical weight loss on glucocor-ticoid metabolism need to be better investigated, theevaluation of HPA axis in bariatric patients can contributeto add new insight also into the complex and bidirec-tional mechanisms linking HPA activity to obesity. Con-cerning the pre-operative management of patients un-dergoing bariatric surgery, endocrinologists should con-sider that the recommended diagnostic procedures forscreening Cushing’s syndrome includes a series of teststhat cannot be routinely applied to patients with simpleobesity (73), but the awareness of the risk of a “hidden”Cushing’s syndrome among the growing population ofobese patients should advise a careful evaluation in se-lected patients.
GONADAL FUNCTION IN OBESE WOMENAND SURGICAL WEIGHT LOSSFemale gonadal dysfunction in obesityObesity is frequently associated to a state of hyperinsu-linemia, resulting in hyperandrogenism, amenorrhea, andendocrine infertility (74-76). The reproductive health his-tory of obese women clearly indicates that obese wom-en are more likely to experience infertility and delay toconception than the general population and normalweight women (77). On the other hand, maternal obesi-ty poses significant short- and long-term risks for all as-pects of pregnancy, either to the mother and to the new-born (78, 79). In particular, obese women are at increasedrisk of miscarriage, pregnancy-induced hypertension, andpre-eclampsia, gestational diabetes, and post partumweight retention. The enhanced maternal morbidity ac-
counts for more frequent operative delivery, with highcesarean section rate, associated with difficulty of anes-thesia and post-operative thromboembolic disorders. Fi-nally, an overall increased perinatal mortality is commonlyreported, while offspring of obese women may have in-creased prevalence of macrosomia, congenital malfor-mation, and juvenile obesity.A large survey, part of the multi-center Longitudinal As-sessment of Bariatric Surgery (LABS-2), showed that41.9% of obese women who had tried to conceive ex-perienced infertility, and those who were obese by theage of 18 yr were more likely to report polycystic ovarysyndrome (PCOS) and infertility and less likely to haveever been pregnant compared to women who becameobese later in their life (80).Due to the impressive increase of the prevalence of obe-sity in the general population, it has been estimated thatthe prevalence of maternal obesity is rising up to 20%(79), and approximately 6% of women entering preg-nancy are categorized as morbidly obese, some of whomundergo bariatric surgery to lose weight (81). Weightloss should be considered as a first option for womenwho are infertile and obese, as a loss of 5 to 10% in over-all body weight can result per se in resumption of regu-lar cycles and ovulation in 66% and 55% of the women,respectively, with increased rate of spontaneous preg-nancy (82).
Female gonadal function and fertilityafter bariatric surgeryA growing body of evidence indicates that menstrual cy-cle disorders, infertility, and adverse pregnancy outcomeamong obese women of reproductive age may satisfac-torily be improved following bariatric surgery-inducedweight loss (83). Consequently, such women may be atgreater risk of unintended pregnancy, and pregnancy orcontraception in obese women who have undergone abariatric procedure may represent an evolving publichealth challenge. In a survey involving women under theage of 40, 71.4% of patients who were anovulatory pre-operatively regained normal menstrual cycles aftersurgery, being their weight loss higher than those whoremained anovulatory (84). Moreover, weight loss as wellas the BMI achieved at pregnancy appeared to be inde-pendent from the surgical techniques in determining theincrease in the pregnancy rate (85). Thus, infertility due toanovulation among morbidly obese women could havepotentially been viewed as an additional indication forbariatric surgery (84).Maternal obesity may affect also obstetric outcomes af-ter in vitro fertilization (IVF) treatment, with higher risk fordecreased pregnancy and live birth rates, and increasesin dose, duration of gonadotropin stimulation, andoocyte retrieval time (86). Recently, a small case-seriesstudy reported that 3 out 5 patients undergoing IVF afterRYGB conceived with their first IVF cycle, and all experi-enced no complications during their IVF cycles or preg-nancy (87). A close monitoring for signs and symptomsof ovarian hyperstimulation syndrome was strongly rec-ommended because of the possible difficulty in distin-guishing between this condition and the possible internalherniation in RYGB procedures.

Endocrine changes after bariatric surgery
272
Neonatal and maternal outcome in pregnancyafter bariatric surgeryThe risk of adverse maternal and neonatal outcomescould be reduced in women who become pregnant afterbariatric surgery compared with rates in pregnant wom-en who are obese (73, 83, 88). However, the incidenceof intra-uterine growth restriction (IUGR) were increased,the risk for cesarian section did not appear to be re-duced, whereas that for pre-term labor and miscarriageremained undetermined (78, 83). Despite some contro-versies (89, 90), a large survey on adverse perinatal out-come after both restrictive and malabsorptive proceduresreported that there were no significant differences in peri-natal mortality and congenital malformations comparedto general population (0.3% and 5% vs 1.5% and 4.0%,respectively) (91).Malabsoptive procedures may result in nutritional defi-ciencies in subsequent pregnancy. The most severe com-plications reported as case reports were: oligohydram-nios, electrolyte imbalances, cerebral hemorrhages dueto vitamin K deficiency, bilateral micropthalmia, perma-nent retinal damage due to vitamin A deficiency, neona-tal hypocalcemia, anemia due to vitamin B12 deficiency,congenital abnormalities, IUGR, small for gestational age(SGA), failure to thrive, and even fetal deaths (78). As ex-pected, the mean birth weight might be significantly re-duced compared with pre-operative pregnancies afterboth malabsortive and mixed malabsortive/restricitive(92, 93), whereas no differences were reported afterLAGB (94). Conversely, a 3-fold increased incidence ofIUGR and SGA appeared more consistently reportedacross studies (78), but this increase was not significant-ly different from obese (2.6%) and severely obese pa-tients (3.7%) (93). Besides low birth weight (<10th per-centile), the post-natal growth of the baby may be sig-nificantly influenced by the energy content of breast milkdepending on fat malabsorption in the mother or to vi-tamin B12 deficiency in breast milk (78).Otherwise, it is noteworthy to consider among the ben-efits of bariatric surgery that a sustained maternal weightloss may contribute to reduce the transmission of obesi-ty and severe obesity in the offspring of both genders by52% and 45.1%, respectively, thus reducing the preva-lence of overweight to current population levels, and in-directly demonstrating the importance of potentiallymodifiable epigenetic factors in the cause of obesity (95).A maternal post-operative complication commonly oc-curring with the LAGB is an increased risk for intestinalhernias, likely due to the frequent occurrence of emesisduring pregnancy, or the increased abdominal pressureand anatomical repositioning of the intra-abdominal or-gans during pregnancy. In particular, while no mechanicalcomplications were reported in some studies (96), in oth-er studies vomiting, severe dehydration, electrolyte dis-turbances, and band leakage might results from band mi-gration in up to 29% of cases (97), requiring the removalof the LAGB at laparotomy in 4% of the patients (98). Fi-nally, considering the high prevalence of gestational dia-betes among obese women, clinicians should be awarethat in women having a RYBG, the physiologic changesof pregnancy may precipitate clinically significant hypo-glycemia in asymptomatic patients, and that the standard
50-g glucose challenge test for gestational diabetes cancause per se symptoms of a dumping syndrome (99).Due to nutritional deficiencies, women are currently ad-vised to delay conception for up to 2 yr after surgery, theperiod when the majority of weight loss occurs (88, 100),also considering that the mother’s potential poor nutritionalstatus can be exacerbated by serious vomiting or nauseaduring the pregnancy. However, early post-operative preg-nancy may not be as dangerous in terms of the rate of mis-carriage and fetal growth as once thought (101), althougha close follow-up of fetal growth during pregnancy andbreastfeeding by a well-trained multidisciplinary team ofbariatric specialists are strongly recommended (78).
Contraception after bariatric surgeryAlthough women are suggested to avoid pregnancy af-ter surgery, the vast majority of women undergoingbariatric surgery are not using very effective contraceptivemethods or any contraception. In particular, a recent self-administered survey showed that only 21.2% of patientswere referred to an obstetrician/gynecologist for contra-ceptive counseling, with condoms (30.6%) or oral con-traceptives (16.3%) as the most common contraceptivemethods used (102). Gerrits et al. (103) reported that twowomen who have undergone BPD, with subsequentlong-lasting post-operative diarrhea, became pregnantpost-operatively while were using the same oral contra-ceptive they used pre-operatively. Despite the possiblerisk of interferences in oral contraceptive absorption andmetabolism, Paulen et al. (104) did not find any evidenceon failure rates or safety for contraceptive methods. Upto now the World Health Organization’s (WHO) MedicalEligibility Criteria for Contraceptive Use has not yet in-cluded bariatric surgery as a contraindication (105). How-ever, as the incidence of post-operative venous throm-boembolism among bariatric surgical patients is between0.4 and 3.1% (106), according to the above-mentionedWHO’s Criteria, the use of oral contraceptives in obesewomen planning major surgery involving prolonged im-mobilization should not recommended (80, 102).
PCOS and bariatric surgeryA particular attention has been paid to morbidly obesepatients with PCOS. PCOS is very common among mor-bidly obese pre-menopausal women, with a 6- to 7-foldincrease in its prevalence compared to general popula-tion (107). Obesity may contribute to the pathogenesisof the syndrome by increasing some features of PCOS,such as hyperandrogenism, hirsutism, infertility, and preg-nancy complications (108). The clinical consequence ofthis contribution is a vicious circle between androgen ex-cess, abdominal adiposity, adipose tissue dysfunction,and insulin resistance, which markedly increase the car-dio-metabolic risk of obese women with PCOS (109).Bariatric surgery has been claimed to represent, in se-lected cases, an extremely efficient treatment for changesin the PCOS phenotype, as it may restore insulin sensi-tivity and fertility, and avoiding the long-term risks asso-ciated with PCOS and morbid obesity (107, 110). How-ever, although the remarkable improvement of metabol-ic dysfunctions in PCOS after bariatric surgery was re-cently confirmed by a large retrospective analysis (111),

S. Savastano, C. Di Somma, R. Pivonello, et al.
273
these beneficial effects are still largely debatable (112).Up to now, there are no published RCT assessing the ef-fectiveness of bariatric surgery specifically in PCOS wom-en, and more scientific research is required (113).
ConclusionsBariatric surgery may improve reproductive hormone pro-file, sexuality, fertility status, safety, and outcomes of preg-nancies in morbid obese women. A summary of the mostrecently published review articles is given in Table 2. Thus,women’s health practitioners may have a growing chanceto encounter a substantial number of women in reproduc-tive age who conceive after bariatric surgery. Women un-dergoing bariatric surgery require careful clinical and nu-tritional supervision, in combination with specific supple-mentation of micronutrients. The counseling should be car-ried out before, during and after a pregnancy followingbariatric surgery. Moreover, a close follow-up of the moth-er and the newborn during the breastfeeding is stronglyrecommended. Endocrinologists should be cautious whencounseling morbidly obese women in reproductive agewho plan to undergo the bariatric surgery. On the otherhand, as the maternal overnutrition can alter the fetalepigenome through epigenetic mechanisms (114), the re-duced risk of obesity in the offspring of obese mothersshould be considered among the possible benefit ofbariatric surgery performed in reproductive age.
GONADAL FUNCTION IN OBESE MENAND SURGICAL WEIGHT LOSSMale gonadal dysfunction in obesityIn contrast to obese women who frequently may experi-ence androgen excess, in male subjects obesity results
in low levels of testosterone with inappropriately low lev-els of LH (115), and in impaired fertility (116, 117). A num-ber of other associated co-morbidities are likely to con-tribute to hypotestosteronemia in obesity, such as Type2 diabetes (118), but there is a large consensus that theboth obesity and diabetes appear to exert independenteffects on the prevalence of low free testosterone con-centrations in addition to age (119). Due to the increasedconversion of androgens into estrogens, mediated by thearomatase normally present in the white adipose tissue,obese males usually express a characteristic gonadal dys-function described as “hyperestrogenic hypogonado-tropic hypogonadism” (120). However, as estrogens andinsulin exert opposite effects on SHBG levels and on itsaffinity for circulating testosterone, the peculiar associa-tion of increased testosterone-to-estradiol conversionwith insulin resistance may result in methodological prob-lems for the evaluation of total and free testosterone lev-els in obese males (121). As a consequence of the alteredsex hormone production, there is also definite evidenceof sexual dysfunction and reduced reproductive potentialin male obesity, due to a number of different factors, in-cluding erectile dysfunction, increased DNA fragmenta-tion, oxydative stress, and scrotal hyperthermia (117, 122,123). In addition, the increased release of adipose-de-rived hormones and adipokines associated with obesity(124) and systemic low-grade inflammation (125) repre-sent further mechanisms for explaining the effect of obe-sity on male gonadal function and fertility.Consequently, as reported in a cohort study in a Danishpopulation of adult obese males (126), weight loss pro-grams, based on healthy diet and daily exercise, are as-sociated with favorable effects on male gonadal functionand increases in total sperm count and semen volume.
Authors Study BariatricReproductive Adverse Adverse
Cesarianand cohort design procedure hormone Fertility Miscarriage fetal maternal
sectionprofile outcomes outcomes
Maggard et al, Systematic review (Medline, Malabsorptive Unclear ↑ ↓ macrosomia ≅,↓ obstetrical Unclear2008 (88) EMBASE, Controlled Clinical and restrictive ≅ congenital complications
Trials Register Database, malformation ↑ nutritionaland the Cochrane Database deficiencyof Reviews of Effectiveness)
Guelinckx et al, Systematic review Malabsorptive ↑ ≅, ↑ ↓ ↓ obstetrical ≅2009 (78) (PubMed) and restrictive complications
↑ nutritionaldeficiency
Brewer et al, Current literature Malabsorptive Restored ↑ ↓ ↓ obstetrical2010 (75) and restrictive complications
↑ nutritionaldefeciency
Escobar-Morreale, Current literature Malabsorptive ↓ Androgen ↑ ↓ ↓ obstetrical2012 (107) and restrictive excess complications
Maqdaleno et al, Systematic review Malabsorptive ↑ ↓ macrosomia ↓ obstetrical unclear2012 (83) (PubMed) and restrictive ↑ IUGR complications
↑ SGA ↑ nutritionaldefeciency
BPD: biliopancreatic diversion; IUGR; intra-uterine growth restriction; SGA: small for gestational age.
Table 2 - Summary of relevant data on bariatric surgery and reproduction in women that are obtained from the analysis of some ofthe most recently published review articles reported in the text and in References 75, 78, 83, 88, 107.

Endocrine changes after bariatric surgery
274
Male gonadal function after bariatric surgeryThe vast majority of patients who undergo bariatricsurgery are women (127). Thus, data on the effects ofbariatric surgery in men are underevaluated and, in somecases, unexpectedly controversial. However, there iscommon agreement that both obesity and weight lossdeeply affect the hypothalamic-pituitary-gonadal axis(128) and the reproductive potential in males (125).Bariatric surgery has been recently defined the most ef-fective treatment of hypotestosteronemia and sexual dys-function in obese men (129, 130). Pellitero et al. (131) re-ported that the hypotestosteronemia in males with mor-bid obesity was mostly reversed after 12 months of sus-tained weight loss induced by bariatric surgery, with aprevalence of persistently reduced testosterone levels aslow as 6-15% depending on the different definition ofhypogonadism. Interestingly, after bariatric surgery cir-culating testosterone in obese men increases in parallelwith the improvement in insulin sensitivity (132), althoughit has been reported that the recovery in testosteronelevels at 6 months from surgery becomes statistically sig-nificant only when considering age ≤35 yr (133).
Male fertility after bariatric surgeryData proving that weight loss reverses male infertilityare surprisingly scarce and controversial. Currently, nostudy investigated birth rate as primary end-point in theevaluation of male fertility after bariatric surgery. Sec-ondary azoospermia with complete spermatogenic ar-rest has been reported in previously fertile male sub-jects with morbid obesity after RYGB surgery, as possi-ble metabolic consequence of a severe post-operativemalabsorption (134). Nutritional deficiencies and releaseof toxic substances are also considered the underlyingmechanism responsible for the worsening of semen pa-rameters after bariatric surgery, including extremeoligoastheno-teratozoospermia, respectively in two (135)
and three patients (136). Nevertheless, this is clearly incontrast with the current literature on the overall favor-able effects of bariatric surgery on testosterone levels.As a matter of fact, Reis et al. (137) evaluated prospec-tively 20 morbidly obese men randomized for RYGB upto 24 months, and concluded that surgery did not in-terfere with sperm quality, while it increased the quali-ty of sexual function. Thus, the negative impact ofbariatric surgery on male fertility remains still unclear,and requires to be confirmed by well-structured trials,based on solid outcomes, such as birth rates, and con-trolled for confounders, including female factors or in-correct nutrition management of the post-bariatricsurgery patient. Nevertheless, these preliminary obser-vations prompt the need for an accurate pre-operativecounseling of patients about the potential reproductiveconsequences of a massive and rapid weight loss, andsome authors have also suggested that sperm cryop-reservation before surgery should be proposed (136). Asummary of the relevant data from recent articles is giv-en in Table 3.
ConclusionsEndocrinologists should be careful in interpreting the ef-fects of surgical induced weight loss on male gonadalfunction, weighing the differences in surgical procedures,follow-up time and number of cases, the possiblemethodological bias in diagnosing hypogonadism inobese males, and the effects of confounding factors ofpersistent co-morbidities or concomitant treatments. Al-though potentially reversible after weight loss, hypotes-tosteronemia in long-term obesity exerts negative effectsnot only on the quality of life of men with morbid obesi-ty, affecting numerous aspects their sexual life (138), butalso on metabolism and body composition (139), with in-creased risk to develop Type 2 diabetes and cardiovas-cular disorders (140). Thus, the functional hypotestos-
Authors Study Bariatric Reproductive Quality Fertility Sperm Testosterone SHBG Estradioland cohort design procedure hormone profile of life quality levels levels levels
Hammoud et al, Prospective RYGB Restored ↑ ↑ ↑ ↓2009 (130) controlled study
Rao et al, Systematic review Malabsorptive Restored ↑ ↑2011 (129) (Medline) and restrictive
Pellitero et al, Prospective RYGB Restored ↑2012 (131) Sleeve (including Sertoli
gastrectomy function)
Botella-Carretero et al, Prospective Malabsorptive Restored2012 (132) and restrictive
Facchiano et al, Prospective Malabsorptive Restored2012 (133) and restrictive
Di Frega et al, Case report RYGB Secondary2005 (134) (6 patients) azoospermia
Lazaros et al, Case report BPD Secondary2012 (135) (2 patients) azoospermia
Sermondade et al, Case report BPD Oligo-astheno2012 (136) (3 patients) teratozoospermia
Reis et al, Prospective RYGB Restored ↑ ↑ Unchanged2012 (137) controlled study
RYGB: Roux-en-Y gastric bypass; BPD: biliopancreatic diversion.
Table 3 - Summary of relevant data on bariatric surgery and reproduction in men that are obtained from the analysis of some of thearticles reported in the text and in References 129-137.

S. Savastano, C. Di Somma, R. Pivonello, et al.
275
teronemia in obese males might be added in the cate-gory of modifiable co-morbidities associated to obesity,and its improvement may be considered a further bene-fit yielded by bariatric surgery, beyond weight loss. Theclinical consequence of the strong correlation betweenpatients’ age at surgery and post-operative increase intestosterone levels may be that patients who better ben-eficiate of the surgical induced weight loss are theyounger ones. It is tempting to suggest that male go-nadal dysfunction could be added among the new crite-
ria for bariatric surgery of NIH based apart from BMI(141), along with age, fitness, gender, body composition,and co-morbidities (142). Young age or longer life-ex-pectancy should be considered carefully in the cost-ben-efit analysis of obese male patients with low testosteroneundergoing bariatric surgery.
FINAL CONSIDERATIONS
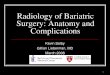
This review gives an updated glance on function of theendocrine axes in obese patients undergoing bariatricsurgery, pinpointing some of the challenge issues mostfrequently encountered. Though the authors are awarethat many questions remain still unsolved, the take-homemessage is that the beneficial effects of bariatric surgeryon metabolism and body composition might be also dueto the favorable reversal of the obesity-related endocrinechanges, summarized in Table 4, beyond improvement ofType 2 diabetes, while a flow chart indicating some ofthe possible strategies in the diagnostic and therapeuticmanagement of post-operative endocrine changes is pro-posed in Figure 1. However, the careful and long-lifemonitoring of the post-operative nutrition deficiencies iscrucial in avoiding the detrimental effects of malnutrition,which can potentially overcome the benefits of thesechanges. The complexity of the endocrine mechanismstriggered by surgical weight loss poses the need to im-prove our knowledge on still unsolved problems, such asthe most appropriate timing when obese subjects shouldbe offered a surgical option to lose weight. Optimizingthe surgical outcome, also in terms of “endocrine” health,
Before bariatric surgery After bariatric surgery
Hormonal References Hormonal Referenceschanges changes
GH ↓ (4, 5) ↑ (24-26, 29, 31)
IGF-I ↓ (4, 5, 20) = (28, 30, 31)↑ (29)
TSH ↑ (35-40) = (43, 45)↓ (47)
FT3 ↑ (35-40) ↓ (43, 45)
FT4 = (35, 36, 40) ↓ (43, 45)
Cortisol = (50) ↓ (64, 65)↑ (54-56, 58, 61)
Free urinary ↑ (50) ↓ (53)cortisol
DHEA-S ↓ (59-61) = (64)↑ (65)
n
Table 4 - Summary of main endocrine changes after bariatricsurgery that are obtained from the analysis of some of the articlesreported in the text and in the References shown in parentheses.
Pre-bariatric surgery Post-bariatric surgery
Endocrineaxis
evaluation
=
=
TSHFT3
Exclude CS
DHEA-S
=
Fertility
=
Check at6 months
GH/IGF-Iaxis
HPT axis
HPA axis
FemaleHPG axis
MaleHPG axis
Check during early3 monthsCheck L-T4 dosage
CheckDHEA-S/Cortisolratio at 6 months
Contraceptivemethods for atleast 2 years
Check during early3 months: TRT ?
Spermcryopreservation ?
Fig. 1 - Suggested flow chart indicatingsome of the possible diagnostic and ther-apeutic strategies in the management ofthe most common post-operative en-docrine changes. HPT axis: hypothalam-ic pituitary thyroid axis; HPA axis: hy-pothalamic pituitary adrenal axis; HPG ax-is: hypothalamic pituitary gonadal axis;CS: Cushing’s syndrome; TRT: testos-terone replacement therapy; FT3: free T3.

Endocrine changes after bariatric surgery
276
could be of particular concern in obese subjects under-going bariatric surgery during their transitional age. Inthese patients, the balance between the detrimental ef-fects of long lasting nutritional deficiency and the long-term metabolic and endocrine consequences of obesityon body composition, and fertility should be carefullyevaluated. On the other hand, endocrinologists shouldalso consider that, in the same way, the progressive fail-ure of β-cells could affect the possible remission of Type2 diabetes after bariatric surgery, an excessive waitingtime for bariatric surgery may be crucial in increasing thedetrimental effects of combined endocrine dysfunctionand in amplifying the cardio-metabolic risk of obese sub-jects.
ACKNOWLEDGMENTSWe are very grateful to Prof. P. Forestieri (Department of General, Geri-atric, Oncologic Surgery and Advanced Technologies, University Federi-co II, Naples, Italy), Prof. L. Angrisani (General and Laparoscopic SurgeryUnit, San Giovanni Bosco Hospital, Naples, Italy), Prof. L. Docimo (XI Di-vision of General and Obesity Surgery, Second University of Naples,Naples, Italy), Prof. M. Musella (Department of Surgical Sciences, Or-thopaedics, Trauma and Emergency, General Surgery, University Fed-erico II, Naples, Italy), and Dr. C. Giardiello (Mininvasive and MetabolicSurgery Unit, University, Pineta Grande Hospital, Castelvolturno (CE),Italy) for their long lasting enthusiastic cooperation in sharing with us thedifficult task to investigate the endocrine changes in obese patients eli-gible for surgery.
Competing interestsThe authors declare that they have no competing interests.
REFERENCES1. Park H, Ahima RS. Classical Hormones Linked to Obesity. In: Ahima
RS (ed). Metabolic Basis of Obesity. New York: Springer Science& Business Media, LLC. 2011, 139-54.
2. Fierabracci P, Pinchera A, Martinelli S, et al. Prevalence of en-docrine diseases in morbidly obese patients scheduled for bariatricsurgery: beyond diabetes. Obes Surg 2011, 21: 54-60.
3. Björntorp P, Rosmond R. Neuroendocrine abnormalities in viscer-al obesity. Int J Obes Relat Metab Disord 2000, 24 (Suppl): S80-5.
4. Franco C, Bengtsson BA, Johannsson G. The GH/IGF-1 axis in obe-sity: physiological and pathological aspects. Metab Syndr RelatDisord 2006, 4: 51-6.
5. Savastano S, Di Somma C, Belfiore A, et al. Growth hormone sta-tus in morbidly obese subjects and correlation with body compo-sition. J Endocrinol Invest 2006, 29: 536-43.
6. Buchwald H, Ikramuddin S, Dorman RB, Schone JL, Dixon JB.Management of the metabolic/bariatric surgery patient. Am J Med2011, 124: 1099-105.
7. Colquitt JL, Picot J, Loveman E, Clegg AJ. Surgery for obesity.Cochrane Database Syst Rev 2009, 2: CD003641.
8. Angrisani L, Cutolo PP, Buchwald JN, et al. Laparoscopic reinforcedsleeve gastrectomy: early results and complications. Obes Surg2011, 21: 783-93.
9. Papailiou J, Albanopoulos K, Toutouzas KG, Tsigris C, Nikiteas N,Zografos G. Morbid obesity and sleeve gastrectomy: how does itwork? Obes Surg 2010, 20: 1448-55.
10. Sjöström L, Gummesson A, Sjöström CD, et al; Swedish ObeseSubjects Study. Effects of bariatric surgery on cancer incidence inobese patients in Sweden (Swedish Obese Subjects Study): aprospective, controlled intervention trial. Lancet Oncol 2009, 10:653-62.
11. Dorman RB, Serrot FJ, Miller CJ, et al. Case-matched outcomes inbariatric surgery for treatment of type 2 diabetes in the morbidlyobese patient. Ann Surg 2012, 255: 287-93.
12. Castagneto-Gissey L, Mingrone G. Insulin sensitivity and secretion
modifications after bariatric surgery. J Endocrinol Invest 2012, 35:692-8.
13. Kreitschmann-Andermahr I, Suarez P, Jennings R, Evers N, BrabantG. GH/IGF-I regulation in obesity mechanisms and practical con-sequences in children and adults. Horm Res Paediatr 2010, 73:153-60.
14. Prodam F, Pagano L, Corneli G, et al. Update on epidemiology,etiology, and diagnosis of adult growth hormone deficiency. JEndocrinol Invest 2008, 31: 6-11.
15. Hazem A, Elamin MB, Bancos I, et al. Body composition and qual-ity of life in adults treated with GH therapy: a systematic reviewand meta-analysis. Eur J Endocrinol 2012, 166: 13-20.
16. Cornford AS, Barkan AL, Horowitz JF. Rapid suppression of growthhormone concentration by overeating: potential mediation by hy-perinsulinemia. J Clin Endocrinol Metab 2011, 96: 824-30.
17. Vijayakumar A, Yakar S, Leroith D. The intricate role of growth hor-mone in metabolism. Front Endocrinol (Lausanne) 2011, 2: 32-42.
18. Di Somma C, Savastano S, Rota F, et al. Appropriate use of stim-ulation tests and insulin-like growth factor-I in obesity. J EndocrinolInvest (Suppl) 2008, 31: 21-6.
19. Bredella MA, Torriani M, Thomas BJ, et al. Peak growth hormone-releasing hormone-arginine-stimulated growth hormone is inverselyassociated with intramyocellular and intrahepatic lipid content inpremenopausal women with obesity. J Clin Endocrinol Metab2009, 94: 3995-4002.
20. Savastano S, Di Somma C, Pizza G, et al. Liver-spleen axis, insulin-like growth factor-(IGF)-I axis and fat mass in overweight/obese fe-males. J Transl Med 2011, 9: 136-43.
21. Rasmussen MH. Obesity, growth hormone and weight loss. MolCell Endocrinol 2010, 316: 147-53.
22. Di Somma C, Pivonello R, Pizza G, et al. Prevalence of the metab-olic syndrome in moderately-severely obese subjects with andwithout growth hormone deficiency. J Endocrinol Invest 2010, 33:171-7.
23. Mekala KC, Tritos NA. Effects of recombinant human growth hor-mone therapy in obesity in adults: a meta analysis. J Clin EndocrinolMetab 2009, 94: 130-7.
24. Valera Mora ME, Manco M, Capristo E, et al. Growth hormone andghrelin secretion in severely obese women before and afterbariatric surgery. Obesity (Silver Spring) 2007, 15: 2012-8.
25. Camastra S, Manco M, Frascerra S, Iaconelli A, Mingrone G, Ferran-nini E. Daylong pituitary hormones in morbid obesity: effects ofbariatric surgery. Int J Obes (Lond) 2009, 33: 166-72.
26. Mancini MC, Costa AP, de Melo ME, et al. Effect of gastric bypasson spontaneous growth hormone and ghrelin release profiles.Obesity (Silver Spring) 2006, 14: 383-7.
27. Mitterberger MC, Mattesich M, Klaver E, Piza-Katzer H, ZwerschkeW. Reduced insulin-like growth factor-I serum levels in formerlyobese women subjected to laparoscopic-adjustable gastric band-ing or diet-induced long-term caloric restriction. J Gerontol A BiolSci Med Sci 2011, 66: 1169-77.
28. De Marinis L, Bianchi A, Mancini A, et al. Growth hormone secre-tion and leptin in morbid obesity before and after biliopancreaticdiversion: relationships with insulin and body composition. J ClinEndocrinol Metab 2004, 89: 174-80.
29. Edén Engström B, Burman P, Holdstock C, Ohrvall M, SundbomM, Karlsson FA. Effects of gastric bypass on the GH/IGF-I axis in se-vere obesity--and a comparison with GH deficiency. Eur JEndocrinol 2006, 154: 53-9.
30. Di Somma C, Angrisani L, Rota F, et al. GH and IGF-I deficiencyare associated with reduced loss of fat mass after laparoscopic-ad-justable silicone gastric banding. Clin Endocrinol (Oxf) 2008, 69:393-9.
31. Savastano S, Angrisani L, Di Somma C, et al. Relationship betweengrowth hormone/insulin-like growth factor-1 axis integrity and vol-untary weight loss after gastric banding surgery for severe obesi-ty. Obes Surg 2010, 20: 211-20.
32. Savastano S, Di Somma C, Angrisani L, et al. Growth hormone treat-ment prevents loss of lean mass after bariatric surgery in morbidlyobese patients: results of a pilot, open, prospective, randomized,controlled study. J Clin Endocrinol Metab. 2009, 94: 817-26.
33. Lecube A, Vilallonga R, Sturniolo G, Obiols G, Fort JM. Renaissanceof acromegaly after bariatric surgery. Endocrine 2013, 43: 239-41.

S. Savastano, C. Di Somma, R. Pivonello, et al.
277
34. Pasquali R, Parenti M, Mattioli L, et al. Effect of dietary carbohy-drates during hypocaloric treatment of obesity on peripheral thy-roid hormone metabolism. J Endocrinol Invest 1982, 5: 47-52.
35. Fox CS, Pencina MJ, D’Agostino RB, et al. Relations of thyroidfunction to body weight: cross-sectional and longitudinal obser-vations in a community-based sample. Arch Intern Med 2008, 168:587-92.
36. Biondi B. Thyroid and obesity: an intriguing relationship. J ClinEndocrinol Metab 2010, 95: 3614-7.
37. Rotondi M, Leporati P, La Manna A, et al. Raised serum TSH levelsin patients with morbid obesity: is it enough to diagnose subclini-cal hypothyroidism? Eur J Endocrinol 2009, 160: 403-8.
38. De Pergola G, Ciampolillo A, Paolotti S, Trerotoli P, Giorgino R.Free triiodothyronine and thyroid stimulating hormone are direct-ly associated with waist circumference, independently of insulin re-sistance, metabolic parameters and blood pressure in overweightand obese women. Clin Endocrinol (Oxf) 2007, 67: 265-9.
39. Iacobellis G, Ribaudo MC, Zappaterreno A, Iannucci CV, LeonettiF. Relationship of thyroid function with body mass index, leptin,insulin sensitivity and adiponectin in euthyroid obese women. ClinEndocrinol (Oxf) 2005, 62: 487-91.
40. Marzullo P, Minocci A, Tagliaferri MA, et al. Investigations of thy-roid hormones and antibodies in obesity: leptin levels are associ-ated with thyroid autoimmunity independent of bioanthropomet-ric, hormonal, and weight-related determinants. J Clin EndocrinolMetab 2010, 95: 3965-72.
41. Nannipieri M, Cecchetti F, Anselmino M, et al. Expression of thy-rotropin and thyroid hormone receptors in adipose tissue of pa-tients with morbid obesity and/or type 2 diabetes: effects of weightloss. Int J Obes (Lond) 2009, 33: 1001-6.
42. Kok P, Roelfsema F, Langendonk JG, et al. High circulating thy-rotropin levels in obese women are reduced after body weight lossinduced by caloric restriction. J Clin Endocrinol Metab 2005, 90:4659-63.
43. Vettor R, Mingrone G, Manco M, et al. Reduced expression of un-coupling proteins-2 and -3 in adipose tissue in post-obese patientssubmitted to biliopancreatic diversion. Eur J Endocrinol 2003, 148:543-50.
44. Ravussin E, Lillioja S, Knowler WC, et al. Reduced rate of energy ex-penditure as a risk factor for body-weight gain. N Engl J Med 1988,318: 467-72.
45. Dall’Asta C, Paganelli M, Morabito A, et al. Weight loss throughgastric banding: effects on TSH and thyroid hormones in obesesubjects with normal thyroid function. Obesity (Silver Spring) 2010,18: 854-7.
46. Lechan RM, Fekete C Role of thyroid hormone deiodination in thehypothalamus. Thyroid 2005, 15: 883-97.
47. Jankovic D, Wolf P, Anderwald CH, et al. Prevalence of endocrinedisorders in morbidly obese patients and the effects of bariatricsurgery on endocrine and metabolic parameters. Obes Surg 2012,22: 62-9.
48. Segal JB, Clark JM, Shore AD, et al. Prompt reduction in use ofmedications for comorbid conditions after bariatric surgery. ObesSurg 2009, 19: 1646-56.
49. Santini F, Pinchera A, Marsili A, et al. Lean body mass is a major de-terminant of levothyroxine dosage in the treatment of thyroid dis-eases. J Clin Endocrinol Metab 2005, 90: 124-7.
50. Andrew R, Gale CR, Walker BR, Seckl JR, Martyn CN. Glucocorti-coid metabolism and the Metabolic Syndrome: associations in anelderly cohort. Exp Clin Endocrinol Diabetes 2002, 110: 284-90.
51. Björntorp P. Do stress reactions cause abdominal obesity and co-morbidities? Obes Rev 2001, 2: 73-86.
52. Classen JB. Review of evidence that epidemics of type 1 diabetesand type 2 diabetes/metabolic syndrome are polar opposite re-sponses to iatrogenic inflammation. Curr Diabetes Rev 2012, 8:413-8.
53. Rask E, Simonyte K, Lönn L, Axelson M. Cortisol metabolism afterweight loss- associations with 11 β-HSD type 1 and markers of obe-sity in women. Clin Endocrinol (Oxf) 2012, Jan 10 [Epub ahead ofprint]; doi: 10.1111/j.1365-2265.2012.04333.x.
54. Mariniello B, Ronconi V, Rilli S, et al. Adipose tissue 11beta-hy-droxysteroid dehydrogenase type 1 expression in obesity andCushing’s syndrome. Eur J Endocrinol 2006, 155: 435-41.
55. Drapeau V, Therrien F, Richard D, Tremblay A. Is visceral obesitya physiological adaptation to stress? Panminerva Med 2003, 45:189-95.
56. Bujalska IJ, Kumar S, Stewart PM. Does central obesity reflect“Cushing’s disease of the omentum”? Lancet 1997, 349: 1210-3.
57. Vogelzangs N, Beekman AT, Milaneschi Y, Bandinelli S, Ferrucci L,Penninx BW. Urinary cortisol and six-year risk of all-cause and car-diovascular mortality. J Clin Endocrinol Metab 2010, 95: 4959-64.
58. De Leo M, Cozzolino A, Colao A, Pivonello R. SubclinicalCushing’s syndrome. Best Pract Res Clin Endocrinol Metab 2012,26: 497-505.
59. De Pergola G, Zamboni M, Sciaraffia M, et al. Body fat accumula-tion is possibly responsible for lower dehydroepiandrosterone cir-culating levels in premenopausal obese women. Int J Obes RelatMetab Disord 1996, 20: 1105-10.
60. Nestler JE.Regulation of human dehydroepiandrosterone metabo-lism by insulin. Ann NY Acad Sci 1995, 774: 73-81.
61. Kalimi M, Shafagoj Y, Loria R, Padgett D, Regelson W. Anti-gluco-corticoid effects of dehydroepiandrosterone (DHEA). Mol CellBiochem 1994, 131: 99-104.
62. Fontana L. Neuroendocrine factors in the regulation of inflamma-tion: excessive adiposity and calorie restriction. Exp Gerontol 2009,44: 41-5.
63. Tomlinson JW, Finney J, Hughes BA, Hughes SV, Stewart PM.Reduced glucocorticoid production rate, decreased 5alpha-re-ductase activity, and adipose tissue insulin sensitization after weightloss. Diabetes 2008, 57: 1536-43.
64. Ram E, Vishne T, Diker D, et al. Impact of gastric banding on plas-ma ghrelin, growth hormone, cortisol, DHEA and DHEA-S levels.Obes Surg 2005, 15: 1118-23.
65. Savastano S, Belfiore A, Guida B, et al. Role of dehydroepiandros-terone sulfate levels on body composition after laparoscopic ad-justable gastric banding in pre-menopausal morbidly obese wom-en. J Endocrinol Invest 2005, 28: 509-15.
66. Manco M, Fernández-Real JM, Valera-Mora ME, et al. Massiveweight loss decreases corticosteroid-binding globulin levels andincreases free cortisol in healthy obese patients: an adaptive phe-nomenon? Diabetes Care 2007, 30: 1494-500.
67. le Roux CW, Sivakumaran S, Alaghband-Zadeh J, Dhillo W, KongWM, Wheeler MJ. Free cortisol index as a surrogate marker forserum free cortisol. Ann Clin Biochem 2002, 39: 406-8.
68. Stephens JW, Boregowda K, Barry J, Price DE, Eyre N, Baxter JN.Adrenal insufficiency following bariatric surgery. Obes Rev 2012,13: 560-2.
69. Tiryakioglu O, Ugurlu S, Yalin S, et al. Screening for Cushing’s syn-drome in obese patients. Clinics (Sao Paulo) 2010, 65: 9-13.
70. Newell-Price J, Bertagna X, Grossman AB, Nieman LK. Cushing’ssyndrome. Lancet 2006, 367: 1605-17.
71. Fleseriu M, Ludlam WH, Teh SH, Yedinak CG, Deveney C,Sheppard BC. Cushing’s syndrome might be underappreciated inpatients seeking bariatric surgery: a plea for screening. Surg ObesRelat Dis 2009, 5: 116-9.
72. Savastano S, Pivonello R, Colao A. Bariatric surgery for obesity andhidden Cushing syndrome. Surg Obes Relat Dis 2009, 5: 121-2.
73. Nieman LK, Biller BM, Findling JW, et al. The diagnosis ofCushing’s syndrome: an Endocrine Society Clinical PracticeGuideline. J Clin Endocrinol Metab 2008, 93: 1526-40.
74. Pasquali R, Patton L, Gambineri A. Obesity and infertility. Curr OpinEndocrinol Diabetes Obes 2007, 14: 482-7.
75. Brewer CJ, Balen AH. The adverse effects of obesity on conceptionand implantation. Reproduction 2010, 140: 347-64.
76. Ehrmann DA, Liljenquist DR, Kasza K, Azziz R, Legro RS, GhazziMN; PCOS/Troglitazone Study Group. Prevalence and predictorsof the metabolic syndrome in women with polycystic ovary syn-drome. J Clin Endocrinol Metab 2006, 91: 48-53.
77. Practice Committee of American Society for Reproductive Medi-cine. Obesity and reproduction: an educational bulletin. Fertil Steril2008, 90: S21-9.
78. Guelinckx I, Devlieger R, Vansant G. Reproductive outcome afterbariatric surgery: a critical review. Hum Reprod Update 2009, 15:189-201.

Endocrine changes after bariatric surgery
278
79. Tsoi E, Shaikh H, Robinson S, Teoh TG. Obesity in pregnancy: amajor healthcare issue. Postgrad Med J 2010, 86: 617-23.
80. Gosman GG, King WC, Schrope B, et al. Reproductive health ofwomen electing bariatric surgery. Fertil Steril 2010, 94: 1426-31.
81. Bergholt T, Lim LK, Jørgensen JS, Robson MS. Maternal body massindex in the first trimester and risk of cesarean delivery in nulli-parous women in spontaneous labor. Am J Obstet Gynecol 2007,196: 163.e1-5.
82. Crosignani PG, Vegetti W, Colombo M, Ragni G. Resumption offertility with diet in overweight women. Reprod Biomed Online2002, 5: 60-4.
83. Magdaleno R jr, Pereira BG, Chaim EA, Turato ER. Pregnancy afterbariatric surgery: a current view of maternal, obstetrical and peri-natal challenges. Arch Gynecol Obstet 2012, 285: 559-66.
84. Teitelman M, Grotegut CA, Williams NN, Lewis JD. The impact ofbariatric surgery on menstrual patterns. Obes Surg 2006, 16:1457-63.
85. Musella M, Milone M, Bellini M, Sosa Fernandez LM, Leongito M,Milone F. Effect of bariatric surgery on obesity-related infertility.Surg Obes Relat Dis 2012, 8: 445-9.
86. Dokras A, Baredziak L, Blaine J, Syrop C, VanVoorhis BJ, SparksA. Obstetric outcomes after in vitro fertilization in obese and mor-bidly obese women. Obstet Gynecol 2006, 108: 61-9.
87. Doblado MA, Lewkowksi BM, Odem RR, Jungheim ES. In vitro fer-tilization after bariatric surgery. Fertil Steril 2010, 94: 2812-14.
88. Maggard MA, Yermilov I, Li Z, et al. Pregnancy and fertility follow-ing bariatric surgery: a systematic review. JAMA 2008, 300: 2286-96.
89. Dalfrà MG, Busetto L, Chilelli NC, Lapolla A. Pregnancy and foetaloutcome after bariatric surgery: a review of recent studies. J MaternFetal Neonatal Med 2012, 25: 1537-43.
90. Friedman D, Cuneo S, Valenzano M, et al. Pregnancies in an 18-year follow-up after biliopancreatic diversion Obes Surg 1995, 5:308-13.
91. Sheiner E, Levy A, Silverberg D, et al. Pregnancy after bariatricsurgery is not associated with adverse perinatal outcome. Am JObstet Gynecol 2004, 190: 1335-40.
92. Marceau P, Kaufman D, Biron S, et al. Outcome of pregnancies af-ter biliopancreatic diversion. Obes Surg 2004, 14: 318-24.
93. Patel JA, Patel NA, Thomas RL, Nelms JK, Colella JJ. Pregnancyoutcomes after laparoscopic Roux-en-Y gastric bypass. Surg ObesRelat Dis 2008, 4: 39-45.
94. Dixon JB, Dixon ME, O’Brien PE. Birth outcomes in obese womenafter laparoscopic adjustable gastric banding. Obstet Gynecol2005, 106: 965-72.
95. Kral JG, Biron S, Simard S, et al. Large maternal weight loss fromobesity surgery prevents transmission of obesity to children whowere followed for 2 to 18 years. Pediatrics 2006, 118: 1644-9.
96. Ducarme G, Revaux A, Rodrigues A, Aissaoui F, Pharisien I, Uzan M.Obstetric outcome following laparoscopic adjustable gastric band-ing. Int J Gynaecol Obstet 2007, 98: 244-7.
97. Bar-Zohar D, Azem F, Klausner J, Abu-Abeid S. Pregnancy after la-paroscopic adjustable gastric banding: perinatal outcome is fa-vorable also for women with relatively high gestational weight gain.Surg Endosc 2006, 20: 1580-3.
98. Skull AJ, Slater GH, Duncombe JE, Fielding GA. Laparoscopic ad-justable banding in pregnancy: safety, patient tolerance and ef-fect on obesity-related pregnancy outcomes. Obes Surg 2004,14: 230-5
99. Wax JR, Heersink D, Pinette MG, Cartin A, Blackstone J. Symp-tomatic hypoglycemia complicating pregnancy following Roux-en-Y gastric bypass surgery. Obes Surg 2007, 17: 698-700.
100. Beard JH, Bell RL, Duffy AJ. Reproductive considerations and preg-nancy after bariatric surgery: current evidence and recommenda-tions. Obes Surg 2008, 18: 1023-7.
101. Dao T, Kuhn J, Ehmer D, Fisher T, McCarty T. Pregnancy outcomesafter gastric-bypass surgery. Am J Surg 2006, 192: 762-6.
102. Mody SK, Hacker MR, Dodge LE, Thornton K, Schneider B, HaiderS. Contraceptive counseling for women who undergo bariatricsurgery. J Womens Health (Larchmt) 2011, 20: 1785-8.
103. Paulen ME, Zapata LB, Cansino C, Curtis KM, Jamieson DJ. Contra-ceptive use among women with a history of bariatric surgery: a sys-tematic review. Contraception 2010, 82: 86-94.
104. Gerrits EG, Ceulemans R, van Hee R, Hendrickx L, Totté E. Contra-ceptive treatment after biliopancreatic diversion needs consensus.Obes Surg 2003, 13: 378-82.
105. World Health Organization. Medical eligibility criteria for contra-ceptive use: 2008 update. http://www.who.int/reproductive-health/publications/mec/mec update 2008.pdf.
106. Bult MJ, van Dalen T, Muller AF. Surgical treatment of obesity. EurJ Endocrinol 2008, 158: 135-45.
107. Escobar-Morreale HF. Surgical management of metabolic dys-function in PCOS. Setroids 2012, 77: 312-6.
108. Motta AB. The role of obesity in the development of polycysticovary syndrome. Curr Pharm Des 2012, 18: 2482-91.
109. Fauser BC, Tarlatzis BC, Rebar RW, et al. Consensus on women’shealth aspects of polycystic ovary syndrome (PCOS): theAmsterdam ESHRE/ASRM-Sponsored 3rd PCOS ConsensusWorkshop Group. Fertil Steril 2012, 97: 28-38.
110. Malik SM, Traub ML. Defining the role of bariatric surgery in poly-cystic ovarian syndrome patients. World J Diabetes 2012, 3: 71-9.
111. Gomez-Meade C, Lopez-Mitnik G, Arheart KL, et al. Effect ofbariatric surgery on cardiometabolic disease risk factors among amultiethnic sample of women with polycystic ovary syndrome. 9th
Annual Meeting of the Androgen Excess & PCOS Society, Orlando,FL, 2011, p.73.
112. Costello MF, Ledger WL. Evidence-based management of infertil-ity in women with polycystic ovary syndrome using surgery or as-sisted reproductive technology. Womens Health (Lond Engl) 2012,8: 291-300.
113. Moran LJ, Pasquali R, Teede HJ, Hoeger KM, Norman RJ. Treat-ment of obesity in polycystic ovary syndrome: a position statementof the Androgen Excess and Polycystic Ovary Syndrome Society.Fertil Steril 2009, 92: 1966-82.
114. Heerwagen MJ, Miller MR, Barbour LA, Friedman JE. Maternalobesity and fetal metabolic programming: a fertile epigenetic soil.Am J Physiol Regul Integr Comp Physiol 2010, 299: R711-22.
115. Allan CA, McLachlan RI. Androgens and obesity. Curr OpinEndocrinol Diabetes Obes. 2010, 17: 224-32.
116. Pasquali R, Patton L, Gambineri A. Obesity and infertility. Curr OpinEndocrinol Diabetes Obes 2007, 14: 482-7.
117. Sermondade N, Faure C, Fezeu L, Lévy R, Czernichow S; Obesity-Fertility Collaborative Group. Obesity and increased risk for oligo-zoospermia and azoospermia. Arch Intern Med 2012, 172: 440-2.
118. Dandona P, Dhindsa S. Update: Hypogonadotropic hypogonadismin type 2 diabetes and obesity. J Clin Endocrinol Metab 2011, 96:2643-51.
119. Dhindsa S, Miller MG, McWhirter CL, et al. Testosterone concen-trations in diabetic and nondiabetic obese men. Diabetes Care2010, 33: 1186-92.
120. Hammoud AO, Gibson M, Peterson CM, Meikle AW, Carrell DT.Impact of male obesity on infertility: a critical review of the currentliterature. Fertil Steril 2008, 90: 897-904.
121. Rosner W, Auchus RJ, Azziz R, Sluss PM, Raff H. Position statement:Utility, limitations, and pitfalls in measuring testosterone: anEndocrine Society position statement. J Clin Endocrinol Metab2007, 92: 405-13.
122. Shayeb AG, Bhattacharya S. Male obesity and reproductive po-tential. Br J Diabetes Vasc Dis 2009, 9: 7-12.
123. MacDonald AA, Herbison GP, Showell M, Farquhar CM. The im-pact of body mass index on semen parameters and reproductivehormones in human males: a systematic review with meta-analy-sis. Hum Reprod Update 2010, 16: 293-311.
124. Hofny ER, Ali ME, Abdel-Hafez HZ, et al. Semen parameters andhormonal profile in obese fertile and infertile males. Fertil Steril2010, 94: 581-4.
125. Lotti F, Corona G, Colpi GM, et al. Elevated body mass index cor-relates with higher seminal plasma interleukin 8 levels and ultra-sonographic abnormalities of the prostate in men attending an an-drology clinic for infertility. J Endocrinol Invest 2011, 34: 336-42.

S. Savastano, C. Di Somma, R. Pivonello, et al.
279
126. Håkonsen LB, Thulstrup AM, Aggerholm AS, et al. Does weight lossimprove semen quality and reproductive hormones? Results from acohort of severely obese men. Reprod Health 2011, 8: 24-31.
127. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: sur-gical treatment of obesity. Ann Intern Med 2005, 142: 547-59.
128. Saad F, Aversa A, Isidori AM, Gooren LJ. Testosterone as potentialeffective therapy in treatment of obesity in men with testosteronedeficiency: a review. Curr Diabetes Rev 2012, 8: 131-43.
129. Rao SR, Kini S, Tamler R. Sex hormones and bariatric surgery inmen. Gend Med 2011, 8: 300-11.
130. Hammoud A, Gibson M, Hunt SC, et al. Effect of Roux-en-Y gastricbypass surgery on the sex steroids and quality of life in obese men.J Clin Endocrinol Metab 2009, 94: 1329-32.
131. Pellitero S, Olaizola I, Alastrue A, et al. HypogonadotropicHypogonadism in Morbidly Obese Males Is Reversed After BariatricSurgery. Obes Surg 2012, Aug 25 [Epub ahead of print]; doi:10.1007/s11695-012-0734-9.
132. Botella-Carretero JI, Balsa JA, Gómez-Martin JM, et al. Circulatingfree testosterone in obese men after bariatric surgery increases inparallel with insulin sensitivity. J Endocrinol Invest 2012, Jun 25[Epub ahead of print]; doi: 10.3275/8469.
133. Facchiano E, Scaringi S, Veltri M, et al. Age as a predictive factorof testosterone improvement in male patients after bariatricsurgery: preliminary results of a monocentric prospective study.Obes Surg 2013, 23: 167-72.
134. di Frega AS, Dale B, Di Matteo L, Wilding M. Secondary male fac-
tor infertility after Roux-en-Y gastric bypass for morbid obesity:case report. Hum Reprod 2005, 20: 997-8.
135. Lazaros L, Hatzi E, Markoula S, Takenaka N, et al. Dramatic reduc-tion in sperm parameters following bariatric surgery: report of twocases. Andrologia 2012, 44: 428-32.
136. Sermondade N, Massin N, Boitrelle F, et al. Sperm parameters andmale fertility after bariatric surgery: three case series. ReprodBiomed Online 2012, 24: 206-10.
137. Reis LO, Zani EL, Saad RD, Chaim EA, de Oliveira LC, Fregonesi A.Bariatric surgery does not interfere with sperm quality--a prelimi-nary long-term study. Reprod Sci 2012, 19: 1057-62.
138. Sarwer DB, Lavery M, Spitzer JC. A review of the relationships be-tween extreme obesity, quality of life, and sexual function. ObesSurg 2012, 22: 668-76.
139. Lunenfeld B. The relationship between sex hormones and themetabolic syndrome. Acta Biomed 2010, 81 (Suppl): 79-84.
140. Traish AM, Kypreos KE. Testosterone and cardiovascular disease:an old idea with modern clinical implications. Atherosclerosis 2011,214: 244-8.
141. Gastrointestinal surgery for severe obesity. National Institutes ofHealth Consensus Development Conference Draft Statement.Obes Surg 1991, 1: 257-66.
142. Pories WJ, Dohm LG, Mansfield CJ. Beyond the BMI: the search forbetter guidelines for bariatric surgery. Obesity (Silver Spring) 2010,18: 865-71.