Embed Size (px)
Citation preview

Service de Gynécologie Obstétrique 2 et Médecine de la Reproduction
Université Paris Descartes, Groupe Hospitalier Cochin, AP-HP
Département Génétique, Développement, Cancer, Institut Cochin
INSERM, CNRS
Paris, France
Endométriose et infertilité:
physiopathologie et stratégiesPr Bruno BORGHESE, Dr Pietro SANTULLI, Dr Isabelle STREULI,
Pr Dominique de ZIEGLER, Pr Charles CHAPRON

Superficial OSIS
Adhesions
Ovarian endometriomas
Deep endometriosis

Hum Reprod (2010)
JC Noel (2010)
JC Noel (2010)
Invasion of
the muscularis
propria

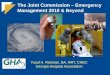
Pathogenesis
Hormonal
Histological
Symptoms
Lesions
Lymph node with
endometriotic focus
PROGINS
polymorphisms
YES
NO
Pain Infertility
SUP OMA DIE

CC Chemokines
CXC
Chemokines
Reis. Hum Reprod Update 2013,376:730-8

Cholesterol
Androstenedione
STAR
CYP11A1
CYP17
EstroneCYP19A1
NR5A1 Estradiol
PGE2PTGS2
+
+
+
+
VEGF
+
MMP
INSL3
Proliferation
Inflammation
Steroidogenesis
Adhesion-Migration
Angiogenesis
PGTE
adapated form Bulun SE. N Engl J Med 2009

de Ziegler D, Borghese B, Chapron C. Lancet 2010,376:730-
8

Inflammation-related processes impairs sperm-
oocyte interactions
Reduced chances of in vivo fertilization
1
de Ziegler D, Borghese B, Chapron C. Lancet 2010,376:730-
8

2Decreased ovarian response to COH:
More FSH/hMG needed
Less oocytes obtained
de Ziegler D, Borghese B, Chapron C. Lancet 2010,376:730-
8

de Ziegler D, Borghese B, Chapron C. Lancet 2010,376:730-
8
Alteration of eutopic endometrium
Activation of CYP-19
Resistance to P4 (PR-D)
Endometrial receptivity & implantation
3

Kunz. Hum Reprod 2005

Chapron, Millischer in press
Ballester. Hum Reprod 2012
JZ ≤ 12 mm JZ > 12 mm P-value OR (95% CI)
N total DIE lesions > 3 29 (54%) 13 (87%) 0.018 25.6 (1.2 –
27.3)

Surgery improves natural conception
Medical treatment of no value for natural
conception
Surgery of no value for ART
Medical treatment favors ART outcome

Vercellini P et al. Hum Reprod 2009,24:254-69
50%

≥ 12 months
< 12 months
Pregnancy: 0.79 (95% CI: 0.46–1.35)
Vercellini et al., RBMO 2010 Vercellini P et al. RBMO 2010

ConsiderSx + 6-18 Mo
in vivoCumulative PR
50%
Time (months)6 18
N=222Stages I-IV
Vercellini P et al. Hum Reprod 2009,24:254-69

Web Appendix: Effects of surgery on infertility associated with endometriosis. Laparoscopic excision of endometrioma (OMA) N # IUP % IUP
Daniell et al., 1991 32 12 37.5
Marrs et al., 1991 23 7 30.4
Bateman et al., 1994 21 9 42.8
Crosignani et al., 1996 22 6 27.3
Montanino et al., 1996 11 5 45.5
Donnez et al., 1996 814 414 50.8
Sutton et al., 1997 66 30 45.5
Beretta et al., 1998 9 6 66.7
Milingos et al., 1998 32 17 53.1
Busacca et al., 1999 67 39 58.2
Jones and Sutton, 2002 39 15 38.5
Alborzi et al., 2004 32 19 59.4
Fedele et al., 2006 90 29 32.2
Vercellini et al., 2006 237 128 54.0
Total 1495 736 49.2
Deep infiltrating endometriosis (DIE) N # IUP % IUP
Coronado et al., 1990 33 13 39.4
Nehzat et al., 1994 8 1 12.5
Bailey et al., 1994 49 24 48.9
Jerby et al., 1999 7 3 42.8
Chapron et al., 1999 30 15 50.0
Possover et al., 2000 15 8 53.3
Redwine and Wright, 2001 23 7 30.4
Kavallaris et al., 2003 38 18 47.4
Fedele et al., 2004 50 17 34.0
Thomassin et al., 2004 15 4 26.7
Chopin et al., 2005 78 42 53.8
Daraï et al., 2005 22 10 45.5
Fleisch et al., 2005 17 4 23.5
Keckstein et al., 2005 95 47 49.5
Mohr et al., 2005 58 23 39.6
Lyons et al., 2006 3 3 100.0
Vercellini et al., 2006 44 15 34.1
Ferrero et al., 2009 46 22 47.8
Meuleman et al., 2009 33 16 48.5
Stepniewska et al., 2009 30 12 40.0
Total 694 304 43.8
IUP: Intrauterine pregnancy
Adapted and updated from Vercellini et al., 2009, with permission.
References
1. Daniell JF, Kurtz BR, Gurley LD. Laser laparoscopic management of large endometriomas. Fertil Steril 1991; 55: 692-95.
2. Marrs RP. The use of potassium-titanyl-phosphate laser for laparoscopic removal of ovarian endometrioma. Am J Obstet Gynecol
1991; 164: 1622-26.
3. Bateman BG, Kolp LA, Mills S. Endoscopic versus laparotomy management of endometriomas. Fertil Steril 1994; 62: 690-95.
4. Crosignani PG, Vercellini P, Biffignandi F, Costantini W, Cortesi I, Imparato E. Laparoscopy versus laparotomy in conservative
surgical treatment for severe endometriosis. Fertil Steril 1996; 66: 706-11.
5. Montanino G, Porpora MG, Montanino Oliva M, Gulemì L, Boninfante M, Cosmi EV. Laparoscopic treatment of ovarian
endometrioma. One year follow-up. Clin Exp Obstet Gynecol 1996; 23: 70-72.
6. Donnez J, Nisolle M, Gillet N, Smets M, Bassil S, Casanas-Roux F. Large ovarian endometriomas. Hum Reprod 1996; 11: 641-
46.
7. Sutton CJ, Ewen SP, Jacobs SA, Whitelaw NL. Laser laparoscopic surgery in the treatment of ovarian endometriomas. J Am
Assoc Gynecol Laparosc 1997; 4: 319-23.
8. Beretta P, Franchi M, Ghezzi F, Busacca M, Zupi E, Bolis P. Randomized clinical trial of two laparoscopic treatments of
endometriomas: cystectomy versus drainage and coagulation. Fertil Steril 1998; 70: 1176-80.
49.2%
de Ziegler D, Borghese B, Chapron C. Lancet 2010,376:730-
8

Web Appendix: Effects of surgery on infertility associated with endometriosis. Laparoscopic excision of endometrioma (OMA) N # IUP % IUP
Daniell et al., 1991 32 12 37.5
Marrs et al., 1991 23 7 30.4
Bateman et al., 1994 21 9 42.8
Crosignani et al., 1996 22 6 27.3
Montanino et al., 1996 11 5 45.5
Donnez et al., 1996 814 414 50.8
Sutton et al., 1997 66 30 45.5
Beretta et al., 1998 9 6 66.7
Milingos et al., 1998 32 17 53.1
Busacca et al., 1999 67 39 58.2
Jones and Sutton, 2002 39 15 38.5
Alborzi et al., 2004 32 19 59.4
Fedele et al., 2006 90 29 32.2
Vercellini et al., 2006 237 128 54.0
Total 1495 736 49.2
Deep infiltrating endometriosis (DIE) N # IUP % IUP
Coronado et al., 1990 33 13 39.4
Nehzat et al., 1994 8 1 12.5
Bailey et al., 1994 49 24 48.9
Jerby et al., 1999 7 3 42.8
Chapron et al., 1999 30 15 50.0
Possover et al., 2000 15 8 53.3
Redwine and Wright, 2001 23 7 30.4
Kavallaris et al., 2003 38 18 47.4
Fedele et al., 2004 50 17 34.0
Thomassin et al., 2004 15 4 26.7
Chopin et al., 2005 78 42 53.8
Daraï et al., 2005 22 10 45.5
Fleisch et al., 2005 17 4 23.5
Keckstein et al., 2005 95 47 49.5
Mohr et al., 2005 58 23 39.6
Lyons et al., 2006 3 3 100.0
Vercellini et al., 2006 44 15 34.1
Ferrero et al., 2009 46 22 47.8
Meuleman et al., 2009 33 16 48.5
Stepniewska et al., 2009 30 12 40.0
Total 694 304 43.8
IUP: Intrauterine pregnancy
Adapted and updated from Vercellini et al., 2009, with permission.
References
1. Daniell JF, Kurtz BR, Gurley LD. Laser laparoscopic management of large endometriomas. Fertil Steril 1991; 55: 692-95.
2. Marrs RP. The use of potassium-titanyl-phosphate laser for laparoscopic removal of ovarian endometrioma. Am J Obstet Gynecol
1991; 164: 1622-26.
3. Bateman BG, Kolp LA, Mills S. Endoscopic versus laparotomy management of endometriomas. Fertil Steril 1994; 62: 690-95.
4. Crosignani PG, Vercellini P, Biffignandi F, Costantini W, Cortesi I, Imparato E. Laparoscopy versus laparotomy in conservative
surgical treatment for severe endometriosis. Fertil Steril 1996; 66: 706-11.
5. Montanino G, Porpora MG, Montanino Oliva M, Gulemì L, Boninfante M, Cosmi EV. Laparoscopic treatment of ovarian
endometrioma. One year follow-up. Clin Exp Obstet Gynecol 1996; 23: 70-72.
6. Donnez J, Nisolle M, Gillet N, Smets M, Bassil S, Casanas-Roux F. Large ovarian endometriomas. Hum Reprod 1996; 11: 641-
46.
7. Sutton CJ, Ewen SP, Jacobs SA, Whitelaw NL. Laser laparoscopic surgery in the treatment of ovarian endometriomas. J Am
Assoc Gynecol Laparosc 1997; 4: 319-23.
8. Beretta P, Franchi M, Ghezzi F, Busacca M, Zupi E, Bolis P. Randomized clinical trial of two laparoscopic treatments of
endometriomas: cystectomy versus drainage and coagulation. Fertil Steril 1998; 70: 1176-80.
43.8%
de Ziegler D, Borghese B, Chapron C. Lancet 2010,376:730-
8

Patients
operated
Wishing to
conceive
Pregnant
127 94 (74%) 48 (51%)
76 54 (71%) 27 (50%)
44%
58%
1 Y
ea
r
2 Y
ea
rs
3 Y
ea
rs
73%
Meuleman C et al. Ann Surg 2013

41% conceived spontaneously
Bowel resection p
Yes No
Recurrence 2/76 (3 %) 6/127 (5%) <0.05
Meuleman C et al. Ann Surg 2013

Time after surgery (days)
Bowel resection Residual bowel
endometriosis
Bowel
resection
Residuel bowel
endometriosis
No bowel
endometriosisP
regnancie
s (
%)
Bowel resection Residual bowel
endometriosisNo bowel
endometriosis
IVF treatment
No bowel
endometriosis
Spontaneous conception
P=0.03
P=0.005
12/30 7/23 24/34
5/13 1/13 4/6
No Conception
1 year
Conception
2 years 4 years
Stepniewska et al. Hum Reprod
2009

of conservative surgery for rectovaginal endometriosis in which the
reproductive outcome in operated patients was compared with that
observed in women undergoing expectant management (Vercellini
et al., 2006b). Amongthe 44 women who had resection of rectovaginal
endometriosis at laparotomy, 15 (34.1%) became pregnant, as com-
pared with 22 of the 61 (36.1%) women who choose expectant man-
agement. The 12-month cumulative probability of conception was
20.5%in the former group and 34.7%in the latter (P¼ 0.12). Corre-
sponding figures at 24-month survival analysis were, respectively, 44.9
and 46.8%(P¼ 0.38). However, a statistically significant longer time to
recurrence of moderate or severe pain recurrence wasobserved in the
surgery group compared with the expectant management group for all
of the symptoms considered. The benefit of surgery was particularly
evident with regard to deep dispareunia and dyschezia.
The above data suggest that excision of rectovaginal plaques does
not improve the likelihood of pregnancy nor reduces the
time-to-conception in women with endometriosis-associated inferti-
lity. These findingsmay be explained by a process of ‘pseudoretroper-
itonealization’ of implants leading to a reduction of the biochemical
impact of deep lesions on fertilization processes. In fact, adhesion
between the anterior rectal wall and the posterior vaginal fornix or
uterine isthmus results in exclusion of the deepest portion of the
pouch of Douglas, where infiltrating endometriosis originates and
develops (Vercellini et al., 1996, 2000; Vercellini, 1997). Excision of
deep endometriotic implants is unlikely to influence the probability
of conception to a major extent if their burial limits the inflammatory
consequences on the pelvic environment. Consequently, the
........................................................................................
T able I Major int ra- and post -operat ive complicat ions
of radical surgery for rectovaginal endomet r iosis
Complicat ion Observed incidence
(%)
Neurogenic bladder dysfunction 4–10
Rectovaginal fistula formation 2–10
Blood transfusion 2–6
Inadvertent rectal perforation 1–3
Anastomotic leakage 1–2
Pelvic abscess 1–2
Temporary diverting loop ileostomy/
colostomy
0.5–1.5
Intraoperative ureteral lesion 0.5–1
Post-operative ureteral fistula formation 0.5–1
Post-anastomotic rectal stenosis 0.5–1
Post-anastomotic ureteral stenosis 0.5–1
From Vercellini et al. (2009, in press). Literature data, 2000–2008: Possover et al.
(2000), Anaf et al. (2001), Chapron et al. (2001), Redwine and Wright (2001), Wright
and Shafic (2001), Duepree et al. (2002), Fedele et al. (2004a), Ford et al. (2004),
Thomassin et al. (2004), Volpi et al. (2004), Campagnacci et al. (2005), Chopin et al.
(2005), Darai et al. (2005), Fleisch et al. (2005), Keckstein and Weisinger (2005), Mohr
et al. (2005), Vignali et al. (2005), Angioni et al. (2006), Dubernard et al. (2006), Landi
et al. (2006), Langebrekke et al. (2006), Lyons et al. (2006), Ribeiro et al. (2006),
Vercellini et al. (2006b), Brouwer and Woods (2007), Kristensen and Kjer (2007),
Mereu et al. (2007), Secchiaroli et al. (2007) and Zanetti-Dallenbach et al. (2008).
Figur e 5 Pregnancy rates observed after excisional surgery of rectovaginal endometriosis at laparotomy or laparoscopy.Diamonds represent per-
centage point estimates and horizontal lines 95% CIs. Modified from Vercellini et al. (2006b), with permission.
Surgery for endometriosis and infertility 259
Vercellini et al., Hum Reprod (2009)

Surgery improves natural conception
Medical treatment of no value for natural conception
Surgery of no value for ART
Medical treatment favors ART outcome

Hughes E et al., Cochrane Database 2007

Vercellini, Obstet Gynecol Clin North Am 2003, 30:163-80.
Conception rate: 22.9% 18.1%

All options are contraceptive

Surgery improves natural conception
Medical treatment of no value for natural
conception
Surgery of no value for ART
Medical treatment favors ART outcome

Garcia-Velasco J et al. Fertil Steril 2004,81:1194-7No impact on IVF
outcome

Impact on
pregnancy rate
Somigliana E et al. Hum Reprod 2008;23:1526-30.

Benaglia et al., Hum Reprod (2010)
Absence of follicular growth:Operated ovary = 12 cases (12%)
Contralateral ovary = 0 cases (0%)
(p < 0.001)
Severe ovarian damage:13% (95% CI 7% - 21%)
N = 93
Operated ovary Non operated ovary

Streuli I et al. Hum Reprod 2012,27:3294-303
** **

Pre op
AMH levels
≥ 3.1ng/ml
Raffi et al., JCEM (2012)

Tang et al., Fertil Steril (2013)

Variable Inexperienced
surgeon
Experienced
surgeon
p
Antral follicule count 7.53.8 9.66.6 0.015
Implantation rate (%) 13.9 18.5 NS
Clinical pregnancy rate per cycle (%) 26.3 41.1 NS
Live-born rate per cycle (%) 9.3 32.9 < 0.001
Yu et al., EJOGRB (2010)
Muzii et al., Fertil Steril (2011)

Endometriosis and IVF Fears
Pain progression Post retrieval infection
Obstetrical Risks Cancer risk

OMAs and ART Pelvic infection after oocyte retrieval
ART in global population Oocyte
retrieval
Post procedure
infection
Bennett SJ et al. J Assist Reprod Genet (1993) 2 670 18 (0.67%)
Dicker D et al. Fertil Steril (1993) 3 656 9 (0.24%)
Moini A et al. J Assist Reprod Genet (2005) 5 958 10 (0,16%)
TOTAL 12 284 37 (0.30%)
ART in endometriotic women Oocyte
retrieval
Post procedure
infection
Tsai YC et al. J Assist Reprod Genet (2005) 108 2 (1.9%)
Benaglia L et al. Fertil Steril (2008) 214 0 (0.0%)
de Ziegler et al. In press (2013) 513 2 (0.38%)
TOTAL 835 4 (0.48%)

22ds – 25wks
intervalAspirated
14 cases described
despite using
prophylactic antibiotics
in at least 11 cases.
Endometrioma infection
following oocyte
retrieval can occur.
Prophylactic AB
may reduce this risk but
cannot abolish it.
Cyst
aspiration/puncture is a
definite risk factor.
Somigliana HRU 2015
OMAs and ART Pelvic infection after oocyte retrieval
Risk of conservative management of women with endometriomas

OMAs and ART Follicular fluid contamination
Risk of conservative management of women with endometriomas
Controversial and paradoxical findings: Numerous toxic substances (free iron)
Animal study: Brief exposure to OMA fluid did not affect mouse emb develop but reduced the blast hatching rate.
Benaglia et al. 2014: In 19 cases of contamination vs 38 matched controls w/ OMABut w/o contamination: Fert rate and top quality emb rates were higher but pregnancy rates were significantly lower.

Somigliana HRU 2015
OMAs and ART Risk of cancer
Risk of conservative management of women with endometriomas
Missing an occult malignancy at IVF
Cancer development after IVF
Mostoufizadeh and Scully (1980): Ca in 8/950 operated endometriomas (0.8%, 95% CI: 0.4–1.6%)
Stern et al. (2001): 9/1000 (0.9%; 95% CI: 0.4–1.6%).
Overestimation, as are pathological findingsMost should have been picked up by imaging.
Complex issue concerning the rarity of ovarian cancer (lifetime risk of ~1%) and possible links of COS/ART and/infertility w/ ov cancer.

Importance of preoperative work-up
QuestionningPelvic
examination
Biochemical
markers
MRI Uro-MRI
Trans-vaginal
US
Trans-rectal
US
Kidney scintigraphy

Endo and ART Painful symptoms
progression
4 cases of severe digestive complications under ovarian stimulation

Endo and ART Painful symptoms
progression
Benaglia et al., Hum Reprod (2011)

Endo and ART Painful symptoms
progression
• Pain during ART :
endometriosis Women
• Endometriosis complaints before
and after ART treatment
• Moderate to severe surgically
proven endometriosis
• IUI (n=25) / IVF (n=25) / IVF
ultra long (n=25)
Van der Houwen Gynecol Endocrinol 2014

Prospective cohort study : 1058 Oocyte retrievals
Ludwig et al, 2006, Human Reproduction
Pain assessment after oocytes retrieval

Fertility and Sterility 2012
The Prepregnancy Uterine Milieu as a Risk Factor of Placental Bed Disorders
ENDOMETRIOSIS
Altered eutopic
endometrium

Vascular & ureteral complications
Maignien 2013
Autor, year Origin of
bleeding site
Number
of cases
Gestational
age at diagnosis
(Noack and Hohlweg-Majert,
1984)
Pelvic 1 3rd trimester
(Inoue et al., 1992) Anterior uterus 1 29
(Mizumoto et al., 1996)
Uterine vessels 28
(Leung et al.,
1998) Right uterine artery 1 33
(Ismail and
Shervington, 1999)
Vascular area of the Douglas
2 33 / PP
(Aziz et al., 2004) Left uterine artery 1 20 Wu (Wu et al.,
2007)
Superficial posterior venous of uterus
1 32
(Katorza et al.,
2007)
Anterior uterin wall, Right Adnexe
Posterior wall of the uterus
3 25 /26 / 29
(Passos et al.,
2008)
Large ligament, right uterine venous
2 32 / 31
(Roche et al.,
2008) Right uterine artery 1 33
(Chiodo et al.,
2008)
Right uterine artery and
right ureter 1 31
(Gonzalez Rosales
et al., 2008) Right uterine artery 1 22
(Tourette et al.,
2011)
Posterior face of the
uterus
(Lajtman et al.,
2011) - 1 -
(Maignien et al.,
2014) Left ovary 1 15
(Berlac et al.,
2014)
Anterior varicous of
uterus 1 28
Marcellin et al. Seud 2015

Ovarian responsiveness to COS
Oocyte competence
Technical difficulties during oocyte retrieval
Infection of endometrioma
Follicular fluid contamination w/ endometrioma content
Risk of conservative management of women with endometriomas
Infertility and ART in women with
endometriosisPregnancy complications
Somigliana HRU 2015;10:1-14.

AuthorStudy
design
Cohort
size
Study
period
(years)
SIR, OR, RR or SMR (95% CI)
Small for
Gestational age
Hypertensive
pathology
Preterm birth
(< 37)
Kortelahti,
2003Case-control 137 1.09 (0.46 – 2.57) - 0.34 (0.88 – 1.88)
Fernando,
2009Case-control 95 13 1.95 (1.06 – 3.60) - 1.98 (1.09 – 3.62)
Stephansson
,
2012
Cohort 13,090 14 1.17 (1.05 – 1.30) 1.17 (1.06 – 1.29) 1.39 (1.30 – 1.49)
Benaglia,
2012Case-control 61 4 0.56 (0.12 – 2.56) 0.56 (0.12 – 2.56) 0.47 (0.14 – 1.54)
Carassou-
Maillan
2014
Case-control 227 5 - 0.69 (0.30 - 1.55) 1.68 (1.11 - 2.53)
Lin,
2015Case-control 249 18 1.75 (0.41–7.49) 0.78 (0.31–2.00) 2.42 (1.05–5.57)
Endometriosis and Obstetrical Outcomes

Inflammation
Interface Materno-fœtale pathologique

AuthorStudy
design
Cohort
size
Study
period
(years)
SIR, OR, RR or SMR (95% CI)
Cesarean sectionPlacenta
preaviaAntepartal bleeding
Kortelahti,
2003Case-control 137 1.03 (0.62 - 1.72) 1.52 (0.42 - 5.52) -
Stephansson,
2012Cohort 13,090 14 1.76 (1.69 – 1.84) - 1.95 (1.75 – 2.18)
Benaglia,
2012Case-control 61 4
1.25 (0.63 – 2.50) - -
Carassou-
Maillan
2014
Case-control 227 5 1.16 (0.84 - 1.60) 5.47 (2.24 - 13.38) 2.54 (1.23-5.24)
Lin,
2015Case-control 249 18 1.93 (1.31–2.84) 4.51 (1.23–16.50) -
Endometriosis and Obstetrical Outcomes


Surgery improves natural conception
Medical treatment of no value for natural
conception
Surgery of no value for ART
Medical treatment favors ART outcome

Canada
2004
Australia
2009
France
2001-2005
USA
2009
IVF ICSI IVF + ICSI IVF + ICSI IVF + ICSI
Primary
diagnosis
Pregnancies
(% per
retrieval)
Pregnancies
(% per
retrieval)
Pregnancies
(% per initiated
cycle)
Pregnancies
(% per initiated
cycle)
Live births
(% per
aspiration)
Male factor 31.0% 37.7% 24.9% 20.1% 37.6%
Tubal factor 33.5% 29.4% 23.5% 21.0% 32.2%
Idiopathic 36.4% 34.7% 23.7% 21.6% 33.7%
Endometriosis 37.8% 41.4% 25.7% 23.7% 35.3%
Ovulatory
disorder
35.6% 36.3% 23.2% 22.6% 40.4%
Other 37.6% 27.9% 18.5%% 27.7%
Gunby J et al. Fertil Steril (2008)
Yueping A et al. Assisted Reproductive technology in Australia and New Zeland (2009)
FIVNAT (2001-2005)
USA, 2009 aspirations: National Center for Chronic Disease Prevention and Health Promotion Division of Reproductive Health

Harb et al. BJOG
2013

Results: Effects of GnRH-a IVF outcome
The 3 trials retained for study indicate that the administration of GnRH-a for 3-6 months prior to IVF/ICSI in women w/
endometriosis increases the odd of pregnancy > 4 fold.
2006

0
10
20
30
40
50
controls OSIS IV OMA present
with OC pretreatment
425 57 28**
P <0.01
83 52 31
*
P <0.05
OC pretreatment (6-8 wk) in ovarian
endometriosis
No pretreatment
* **
Effects of pre-ART treatment with OC
pre-ART OC x6-8 wks
Center I & 2
De Ziegler et al. Fertil Steril 2010,94:2796-9

with OC pretreatment pre-ART OC x6-8 wks
De Ziegler et al. Fertil Steril 2010,94:2796-9
OC pretreatment (6-8 wk) in ovarian
endometriosis

Unoperated bilateral OMAs ART outcome
Benaglia et al., Fertil Steril, (2013)
Characteristics Case n = 39 Control n = 78 p

Operated bil Omas
n = 68
No prior ovarian
surgery n = 136pCharacteristics
Somigliana et al., Hum Reprod (2008)
Operated bilateral OMAs ART outcome

Relationship between « oocyte quantity and quality »
Oocytes
Cumul PR Life birth rate
Amp FSH
OMA
OMA
Tubal infertility
Tubal infertility
NS NS
Al-Azemi et al., Hum Reprod (2000)

37
reg. ART
donor-egg ART
37

Streuli I et al. Hum Reprod 2012,27:3294-303
** **

Endometriosis Age
Quantity
Quality
FSH < 8 mIU/ml 8-12 mIU/ml > 12 mIU/ml
AFC > 8 total 5-7 total < 5 total
AMH > 1ng/ml 0.5-1 ng/ml < 0.5 ng/ml
de Ziegler and Chapron, IFFS Newsletter (2013)
Ovarian reserve testing in ART patients
AMH, AFC and FSH/E2 predict
magnitude of ovarian response
in ART but not fecundity
Ovarian reserve predicts the number of oocytes
responding to COS, not their quality
Ovarian reserve reflects the efficacy of ART as infertility
treatment
Endo has an impact on
quantity but not quality
(≠ age)

Multidisciplinary management
Endometriosis
and
Patients
Pelvic pain
Infertility
Global approach
Surgery
Medical Ttt
ART
SUP OMAs DIE
Adenomyosis

Global approach of endometriosis
Avoid that the choosing of surgery or ART
reflects the primary activity
of the doctor first consulted

Ovarian reserve
Adenomyosis
Infertility Pelvic pain
A
Referral center
VAS < 7:
Moderate DIE
VAS ≥ 7:
Severe DIE
Classical center
B
« Emergency ART »
ART
Without surgery
Fertility preservation ?
Previous surgery
Endometrioma
OC