Embed Size (px)
Citation preview

Accepted Manuscript
Endothelial function and dysfunction: impact of metformin
Asma Nafisa, Susan G. Gray, Yingnan Cao, Tinghuai Wang,Suowen Xu, Feroza H. Wattoo, Michael Barras, Neale Cohen,Danielle Kamato, Peter J. Little
PII: S0163-7258(18)30132-3DOI: doi:10.1016/j.pharmthera.2018.07.007Reference: JPT 7255
To appear in: Pharmacology and Therapeutics
Please cite this article as: Asma Nafisa, Susan G. Gray, Yingnan Cao, Tinghuai Wang,Suowen Xu, Feroza H. Wattoo, Michael Barras, Neale Cohen, Danielle Kamato, PeterJ. Little , Endothelial function and dysfunction: impact of metformin. Jpt (2018),doi:10.1016/j.pharmthera.2018.07.007
This is a PDF file of an unedited manuscript that has been accepted for publication. Asa service to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting proof beforeit is published in its final form. Please note that during the production process errors maybe discovered which could affect the content, and all legal disclaimers that apply to thejournal pertain.

ACC
EPTE
D M
ANU
SCR
IPT
P&T 23351
Endothelial function and dysfunction: impact of metformin
Asma Nafisa1,*
, Susan G Gray1, Yingnan Cao
2, Tinghuai Wang
2, Suowen Xu
3,
Feroza H. Wattoo4, Michael Barras
5, Neale Cohen
6, Danielle Kamato
1,2 and
Peter J Little1,2
1School of Pharmacy, University of Queensland, Pharmacy Australia Centre of Excellence,
Woolloongabba, QLD, Australia,
2Xinhua College of Sun Yat-sen University, Tianhe District, Guangzhou, China
3Aab Cardiovascular Research Institute, Department of Medicine, University of Rochester
School of Medicine and Dentistry, Rochester, New York, USA
*,4Department of Biochemistry PMAS Arid Agriculture University, Shamasabad, Muree
Road, Rawalpindi 4600, Pakistan.
5Dept. of Pharmacy, Princess Alexandra Hospital, 199 Ipswich Rd, Woolloongabba QLD
4102
6Baker Heart and Diabetes Institute, Melbourne, 3004, Victoria, Australia
Address correspondence to:
Professor Peter J. Little, AM School of Pharmacy, The University of Queensland,
Pharmacy Australia Centre of Excellence, 20 Cornwall Street, Woolloongabba,
QLD 4102, Australia Tel: +61 7 3346 1701 Email: [email protected]
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Author emails:
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Abstract
Cardiovascular and metabolic diseases remain the leading cause of morbidity and mortality
worldwide. Endothelial dysfunction is a key player in the initiation and progression of
cardiovascular and metabolic diseases. Current evidence suggests that the anti-diabetic drug
metformin improves insulin resistance and protects against endothelial dysfunction in the
vasculature. Hereby, we provide a timely review on the protective effects and molecular
mechanisms of metformin in preventing endothelial dysfunction and cardiovascular and
metabolic diseases.
Keywords : Metformin, mechanism of action, endothelium, hyperglycaemia, CVD,
endothelial dysfunction
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Abbreviations
AGE advanced glycation end-products
AngII Angiotensin II
AJ adherens junctions
Bcl6 B-cell lymphoma 6
BH4 tetrahydrobiopterin
CVD cardiovascular disease
cGMP cyclic guanosine 5’ monophosphate
DHAP dihydroxy acetone phosphate
ED endothelial dysfunction
EDHF endothelium derived hyperpolarizing factor
EDRF endothelium- derived relaxing factor
eNOS endothelial nitric oxide synthase
ER endoplasmic reticulum
ET-1 endothelin-1
eNOS endothelial nitric oxide synthase
FAD flavin adenine dinucleotide
FMN flavin adenine mononucleotide
G6PDH glucose-6-phosphatese dehydrogenase
GAPDH glyceraldehyde phosphate dehydrogenase
GCH1 GTP cyclohydrolase I
GTPCH1 guanosine 5’-triphosphate cyclohydrolase 1
H2S hydrogen sulphide
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
HSP90 heat shock protein 90
HUVECS human umbilical vein endothelial cells
ICAM1 intracellular adhesion molecule 1;
LOX-1 lectin-like oxidized LDL receptor 1
MAPK mitogen activated protein kinase
Mn-SOD manganese superoxide dismutase
MCP1 monocyte chemo attractant protein 1;
mTOR mammalian target of rapamycin
mPTP mitochondrial permeability transition pore
NF-kB nuclear factor kappa B;
NO nitric oxide
NOX NADPH oxidase
PAI-1 plasminogen activator 1
PAPP1 p, phosphorylation of poly-ADP-ribose polymerase 1
PEPCK phosphoenolpyruvate carboxykinase
PCOS polycystic ovary syndrome
PPARδ peroxisome proliferator-activated receptor δ
PGI2 prostacyclin I2
PGC1α PPARgamma Coactivator 1alpha
PKC protein kinase C
ROS reactive oxygen species
TJ tight junctions
t-PA tissue type plasminogen activator
TNFα Tumour necrosis factor - alpha
TRAF3IP2 TRAF3 interacting protein 2
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Sirt1 Sirtuin 1
u-PA urokinase plasminogen activator
VCAM1 vascular adhesion molecule 1
VEGF vascular endothelial growth factor
VSMCs vascular smooth muscle cells
vWF von willebrand factor
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
1. Introduction
Cardiovascular disease (CVD) is the largest cause of morbidity and mortality in modern
societies (Fang, Little, & Xu, 2017; Writing Group, et al., 2016). The major underlying
pathology of CVD is atherosclerosis (Libby, 2006; Little, Osman, & O'Brien, 2008; Ross,
1986; Tabas, Williams, & Boren, 2007). Atherosclerosis is accelerated by the diabetic milieu
but the mechanisms of this response are unclear. The impact of drugs which reverse the
diabetic state on preventing atherosclerosis and CVD is also controversial (Nigro, Osman,
Dart, & Little, 2006; S. N. Yang, et al., 2010). The phenomena of endothelial dysfunction
(ED) is closely associated with atherosclerosis. In this context, it is important to have a full
understanding of the action of drugs which treat the diabetic state and impact on ED for a full
appreciation of their potential role in reducing the development and progression of
atherosclerosis and hence CVD.
There are many risk factors for CVD most prominently hypertension, hyperglycaemia
and hyperlipidaemia which are modifiable by medical treatment. Risk factors are not of
concern in their own role but for their role in accelerating the onset or rate of development of
atherosclerosis. CVD in diabetes is traditionally divided into the microvascular diseases of
small vessels and the macrovascular disease of larger vessels where hyperglycaemia is the
cause of the former and it is closely associated with the latter.
Type 2 diabetes is now recognised as an important risk factor for CVD and in patients
with diabetes but without a previous cardiovascular event Type 2 diabetes carries a similar
risk of a future event to a subject without diabetes who has had a previous event (Haffner,
1997). The principal metabolic abnormalities of diabetes are insulin resistance, pancreatic
beta cell failure and abnormalities of the incretin system where early Type 2 diabetes is
characterized by insulin resistance and rising plasma insulin (relative insulin deficiency) and
in the later stages beta cell failure leads to an absolute deficiency of insulin and
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
hyperglycaemia. Incretins impact on these two parameters and can modify the progression of
disease and also serve as therapeutic targets (Cernea, 2011).
To be truly efficacious, lowering of risk factors for CVD must have effects on lowering
cardiovascular events and increase life expectancy. Medical treatments are often assessed for
their acute or short-term effects on risk factors but it is the ultimate outcomes on CVD that
are important. Therapeutic agents that are highly effective in reducing risk factors but this
may not always be sufficient to reduce the incidence of CVD. The action on risk factors may
be counteracted by their deleterious effects on the cardiovascular system such as occurred for
COX inhibitors (Fanelli, Ghisi, Aprile, & Lapi, 2017). Therefore, preferably agents should
have range of effects, known as pleiotropic effects directly on the cardiovascular system so
that these effects can work in tandem with the risk factor benefit to get an overall reduction in
CVD and mortality.
In Type 2 diabetes, it has been extremely difficult to discover agents which can reduce
hyperglycaemia and reduce cardiovascular events safely. Indeed, most agents for the
treatment of diabetes have not attained these criteria of efficacy and safety. One old agent
which had a mixed early therapeutic history is the biguanide, metformin. Metformin has
recently risen to the top of the relevant therapeutic armamentarium tree to become the first
line medical therapy for the treatment of the hyperglycaemia accompanying Type 2 diabetes
(Gray, McGuire, Cohen, & Little, 2017; Stumvoll, Nurjhan, Perriello, Dailey, & Gerich,
1995). As mentioned above, ED is thought to accelerate the development and progression of
atherosclerosis and accordingly targeting and reducing ED is hypothesized to reduce CVD.
The overall effect of metformin appears to be a reduction in cardiovascular events but the
topic is of some debate (UK Prospective Diabetes Study (UKPDS) Group, 1998).
Understanding the effects of metformin on ED would advance our understanding of the full
therapeutic potential of metformin. The effects of metformin, as other risk factor addressing
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
agents, arise from its primary effect on the risk factors (insulin resistance and
hyperglycaemia) and its associated direct effects on the vasculature, indeed the endothelium.
In this review, we address the use of metformin in diabetes and associated vascular
complications, and analyse the effects of metformin on the endothelium due to its anti-
hyperglycaemic and vasculoprotective actions. In these days of personalized medicine, a deep
understanding of effects of therapeutic agents may point to populations in which the balance
of unwanted and favourable effects is tipped in the desired direction and the use of drugs can
be optimised. Here we analyse the actions of metformin with a view to seeking optimum
patient outcomes for people treated with this ubiquitous agent.
2. Endothelial function and dysfunction
The endothelium is a single layer of cells which separates all tissues from circulating
blood (A Chistiakov, V Revin, A Sobenin, N Orekhov, & V Bobryshev, 2015; Minami &
Aird, 2005). Intact endothelium acts in an autocrine, paracrine and endocrine manner and
secretes a number of bioactive mediators that affect vascular tone (Muniyappa & Sowers,
2013). A seminal experiment by Robert Furchgott and colleagues (Furchgott & Zawadzki,
1980) demonstrated that removal of endothelium from isolated arteries prevents the ex vivo
vasodilatory response to acetylcholine; indeed denuded vessels constrict in response to
acetylcholine. Subsequently it was revealed that acetylcholine stimulates the endothelium to
release endothelium-derived relaxing factor (EDRF) which was later characterized as the
vasoactive gas, nitric oxide (NO) (Ignarro, Buga, Wood, Byrns, & Chaudhuri, 1987). Healthy
endothelium maintains a low level of oxidative stress and a relaxed vascular tone by releasing
several vasoactive mediators. Major vasodilators released by endothelial cells include NO,
prostacyclin I2 (PGI2) endothelium derived hyperpolarizing factor (EDHF), bradykinin,
histamine, serotonin, substance P while the key secreted vasoconstrictors include endothelin-
1 (ET-1), angiotensin II (ANG-II), thromboxane A2, prostacyclin H2 and reactive oxygen
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
species (ROS) (Endemann & Schiffrin, 2004; Just, Whitten, & Arendshorst, 2008; Lai &
Kan, 2015; Moncada, Gryglewski, Bunting, & Vane, 1976; R MoJ Palmer, Ferrige, &
Moncada, 1987; Yanagisawa, et al., 1988). The delicate balance between this plethora of
vasodilators and vasoconstrictors and pro- and anti-coagulation factors is crucial for
physiological functioning of the endothelium and an imbalanced production of these
molecules leads to failed vascular auto regulation and influences the structural and functional
integrity of the endothelium with pathophysiological consequences (Ghosh, Gao, Thakur,
Siu, & Lai, 2017).
3. Endothelial Dysfunction
The functional integrity of endothelium is important to vascular health. Imbalance
between vasodilators and vasoconstrictors as well as chronic disturbances in mechanical
shear stress caused by dyslipidaemia, hypertension and diabetes leads to endothelial
dysfunction. Endothelial dysfunction is not only an initiator but also could be an important
contributor to the progression of CVD (Barton & Haudenschild, 2001; Endemann &
Schiffrin, 2004; Félétou & Vanhoutte, 2006a). Endothelial dysfunction is characterised and
defined by one or more of following features: reduced production and bioavailability of NO,
impaired endothelium dependent vasorelaxation, impaired fibrinolytic ability, hemodynamic
dysregulation, enhanced expression of adhesion molecules and inflammatory genes,
increased generation of ROS and enhanced permeability of vascular endothelium (Ghosh, et
al., 2017; Gimbrone & García-Cardeña, 2016; Cristina M Sena, Ana M Pereira, & Raquel
Seiça, 2013). In disease states the endothelium undergoes functional and structural alterations
and loses its CVD protective role (Versari, Daghini, Virdis, Ghiadoni, & Taddei, 2009).
Several studies have linked endothelial dysfunction and resultant atherosclerosis to insulin
resistant states, such as obesity and diabetes (Bakker, Eringa, Sipkema, & van Hinsbergh,
2009; J.-a. Kim, Montagnani, Koh, & Quon, 2006; Nigro, et al., 2006).
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
4. Regulation of vascular tone
The endothelium regulates vascular tone by producing and releasing NO, and
prostacyclin and by hyperpolarising vascular smooth muscle cells (VSMCs). NO is the major
vasodilator synthesised by endothelial nitric oxide synthase (eNOS or NOS3) (Nishida, et al.,
1992). NO is synthesized from the oxidation of L-Arginine (Richard MJ Palmer, Ashton, &
Moncada, 1988), in a twostep process catalysed by eNOS through the generation of N-
hydroxyl-L arginine. eNOS is constitutively expressed in endothelial cells, closely associated
with caveolae where it binds caveolin-1 that restricts its activity (R MoJ Palmer, et al., 1987).
Other factors that influence the continuous synthesis of NO by endothelial cells include
plasma constituents (thrombin, sphingosine1-phosphate), autacoids (bradykinin, histamine,
prostaglandin), platelet products (adenosine phosphate, serotonin), neurohumoral mediators
such as acetylcholine and circulating hormones (catecholamines, vasopressin and
aldosterone) (Michel & Vanhoutte, 2010). Furthermore, mechanical forces regulate eNOS
gene expression differentially in areas of disturbed flow versus steady laminar flow.
Endothelial cells exposed to laminar flow possess enhanced NO forming capacity (Chiu &
Chien, 2011). Once produced, NO readily diffuses to VSMCs and activates soluble guanylate
cyclase system which in turn results in increased levels of cyclic guanosine-3’, 5 mono
phosphate (cGMP) and relaxation of VSMC (Rapoport & Murad, 1983). NO also exerts its
effects by reversible modification of proteins by adding NO group at cysthiol forming S-
nitrosylated proteins (Stamler, et al., 1992). S-Nitrosylation of proteins modulates many
important physiological processes in the cardiovascular system including cell proliferation,
apoptosis, ion channel activity, exocytosis, blood flow and systemic oxygen delivery. Apart
from being a key vasodilator, NO counteracts platelet aggregation, VSMC proliferation and
leukocyte adhesion to the endothelium (de Graaf, et al., 1992)(Cornwell, Arnold, Boerth, &
Lincoln, 1994). The endothelium also mediates the hyperpolarization of VSMCs by releasing
EDHF and directly by intercellular communication through gap junctions. NO and other
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
vasodilators act co-operatively and oppose the action of vasoconstrictors this maintaining the
normal arterial patency.
5. Endothelial transmigration by blood borne cells
Inflammation is a key player in both the development and acute activation of vascular
cells (Libby, Ridker, & Hansson, 2011). Under physiological conditions, the endothelium
resists attachment of leukocytes to its surface (Libby, et al., 2011). NO maintains the
endothelium in a quiescent, anti- inflammatory state and prevents leukocyte adhesion
(Widlansky, Gokce, Keaney, & Vita, 2003). However, the endothelium shows up regulated
expression adhesion molecules such as vascular adhesion molecule 1 (VCAM-1) and
intracellular adhesion molecule 1 (ICAM-1) (Libby, Ridker, & Maseri, 2002) in CVD risk
factors, such as dyslipidaemia, hypertension and increased proinflammatory mediators.
Consequently, the endothelium is rendered adhesive for circulating leukocytes, thereby
initiating an intriguing multistep process involving capturing, rolling, arrest, crawling (to the
site of injury) and transmigration through the barrier formed by endothelial cell monolayers
(Vestweber, 2015). The activated endothelium also expresses chemotactic factors such as
monocyte chemoattractant protein-1 (MCP-1) and proinflammatory cytokines such as
macrophage colony-stimulating factor, and tumour necrosis factor–alpha (TNFα) (Libby, et
al., 2002). Expression of these factors in the endothelium contributes to the development of
inflammation in the arterial wall and promotes atherogenesis.
6. The phenomenon of endothelial cell senescence
The phenomenon of cellular senescence is characterized by cell cycle arrest and pro-
inflammatory gene expression (Rodier & Campisi, 2011). Endothelial senescence occurs in
vivo and is a major contributor to vascular ageing (Erusalimsky, 2009; J. C. Wang & Bennett,
2012). Cellular senescence is driven by many factors including, high glucose, ROS,
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
inflammatory cytokines, telomere dysfunction, and ionizing radiation (Kojima, Kunimoto,
Inoue, & Nakajima, 2012; Minamino, et al., 2002; Rogers, Zhang, Azhar, Luo, & Wei, 2013;
Valenzuela, et al., 1997; Vasto, et al., 2007). Substantial evidence indicates that
hyperglycaemia–induced ROS formation and reduced bioavailability of NO promotes DNA
damage, shortening of telomeres, genomic instability and growth arrest in endothelial cells,
thus resulting in premature endothelial cell senescence (Hoffmann, et al., 2001; Matsui-Hirai,
et al., 2011; Ota, et al., 2008; Yokoi, et al., 2006). These phenotypically altered endothelial
cells are pro- inflammatory, pro-thrombotic and pro-atherosclerotic with diminished antigenic
and regenerative properties (Erusalimsky, 2009; Testa & Ceriello, 2007) and augmented
diabetes associated CVD .
7. Endothelial cell apoptosis in the functioning of the endothelium
Endothelial cell apoptosis is a crucial process for development of atherosclerosis (Peng,
et al., 2014). The hyperglycaemia of diabetes can induce apoptosis by one or more of the
following mechanisms: increased intracellular Ca2+, increased oxidative stress, mitochondrial
dysfunction, changed intracellular fatty acid metabolism, impaired phosphorylation of protein
kinase Akt and activation of mitogen activated protein kinase (Isoda, et al., 2006).
Hyperglycaemia increases Bax protein expression, but does not affect that of Bcl-2.
Elevated Bax/Bcl-2 ratio activates the cleavage of procaspase3 into active caspase-3 and
triggers apoptosis in Human Umbilical Vein Endothelial Cells (HUVECS) (Z. Yang, et al.,
2008). Intracellular ROS generation is an important cause of apoptotic cell death and is also
involved in the development of diabetic vascular disease (T. Yu, Sheu, Robotham, & Yoon,
2008). Hyperglycaemia induced intracellular ROS activate JNK and p38 pathway and
triggered subsequent apoptosis in HUVECS (Ho, et al., 2006). ROS accumulation in
mitochondria is a trigger for the intrinsic death pathway, subsequently leading to apoptosis
(Goyeneche, Harmon, & Telleria, 2006). There are many pathways involved in activating
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
endothelial cell apoptosis but a common mechanism causing endothelial dysfunction and
endothelial apoptosis is oxidative stress (Van den Oever, Raterman, Nurmohamed, & Simsek,
2010) .
8. Biochemical mechanisms associated with endothelial dysfunction in diabetes
8.1 Insulin resistance and endothelial cell dysfunction
In the diabetic milieu, the metabolic disturbances of insulin resistance, hyperglycaemia
and excessive circulating free fatty acids induces oxidative stress, low grade inflammation,
platelet hyperactivity and endothelial dysfunction in the vascular tissues (Cristina M. Sena,
Ana M. Pereira, & Raquel Seiça, 2013). Insulin resistance is linked with lipotoxicity,
glucotoxicity and inflammation, which initiates and accelerates atherogenesis and vascular
disease (Kamato, et al., 2014; Little, et al., 2008; Nigro, et al., 2006; Ouchi, Parker, Lugus, &
Walsh, 2011; S. N. Yang, et al., 2010). A decade ago we speculated that insulin resistance
was due to the action of an unknown lipophilic metabolite which attenuated insulin signalling
and this speculation remains valid to this day (Nigro, et al., 2006). Insulin signal transduction
occurs through two major and ubiquitous signalling pathways. PI3K is involved in mediating
the metabolic and hemodynamic effects while the Ras-Raf-mitogen-activated-protein kinase
(MAPK) pathway mediates gene expression, cell growth and differentiation (Avruch, 1998;
Nigro, et al., 2006). Under normal physiological conditions, insulin activates the PI3K
pathway, which phosphorylates eNOS at Serine 1177 site, thereby enhancing NO synthesis
by endothelial cells (Dimmeler, et al., 1999). In insulin resistant states, this pathway is
impaired and NO production is diminished. Alternatively, the MAPK pathway evokes the
synthesis of inflammatory markers PAI-1, ICAM-1, VCAM-1, and E-selectin resulting in
endothelial dysfunction (Montagnani, et al., 2002; Muniyappa & Sowers, 2013). An
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
imbalance between the PI3K and MAPK pathways provides a strong link between insulin
resistance and endothelial dysfunction (Hsueh & Quiñones, 2003)(J.-a. Kim, et al., 2006).
This relationship is accelerated by selective inhibition of insulin signalling to eNOS via PI3K,
whereas MAPK signalling to ET-1 is unaltered or increased (Z. Y. Jiang, et al., 1999).
Endothelial dysfunction due to impaired insulin signalling reduces agonist- induced
vasodilation and the vascular wall becomes more susceptible to atherosclerosis (Maeno, et
al., 2012; Rask-Madsen, et al., 2010). Furthermore insulin resistance also stimulates VSMC
proliferation, migration, and causes excessive release of free fatty acids from adipose tissue,
which elicits pathogenic gene expression through activation of protein kinase C (PKC) and
raised oxidative stress (Hajer, van Haeften, & Visseren, 2008).
8.2 Hyperglycaemia and endothelial dysfunction
Hyperglycaemia is an important factor in endothelial dysfunction and several theories
have been proposed to explain its adverse effects on the endothelium. These include the
advanced glycation end product hypothesis, hexosamine hypothesis, aldose reductase
hypothesis, the hyperperfusion hypothesis, PKC hypothesis and the oxidative stress
hypothesis (Giacco & Brownlee, 2010). These hypotheses have overlapping points that
potentiate each other but oxidative stress is most likely the common disturbance of
hyperglycaemia (Brownlee, 2001; Van den Oever, et al., 2010). ROS reduces glucose
metabolism via glycolysis, alternatively, there is increased flux through the hexosamine and
polyol pathways. Hyperglycaemia induced oxidative stress, causes DNA damage and
activates nuclear poly (ADP-ribose) polymerase which results in enhanced production of
polymers of ADP–ribose (PAR). Subsequently, these polymers of ADP-ribose cause
modification and inactivation of glyceraldehyde phosphate dehydrogenase (GAPDH) (X. Du,
et al., 2003; Giacco & Brownlee, 2010). Ultimately, the accumulation of upstream glycolytic
intermediates glycraldehyde-3-phosphate and dihydroxy acetone phosphate (DHAP), which
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
can be converted to diacylglycerol, activates classical and novel PKC pathways (Way, Katai,
& King, 2001) . There are at least 11 PKC isoforms and PKCβ is most frequently the
activated form in vascular cells. The pathogenic consequences of PKC activation include
dysregulated blood flow due to diminished eNOS activity and increased ET-1 synthesis and
(S. Chen, Apostolova, Cherian, & Chakrabarti, 2000), impaired vascular permeability in
VSMC due to induction of vascular endothelial growth factor (Williams, Gallacher, Patel, &
Orme, 1997), thickening of basement membranes through TGF-β mediated increased
synthesis of collagen IV and fibronectin, increased plasminogen activator inhibitor -1 (PAI-1)
expression which impairs fibrinolysis and activation of NADPH oxidase as well as increased
expression of superoxide producing uncoupled eNOS thus further increasing oxidative stress.
Glucotoxicity induces a low grade pro-inflammatory state due to activation of
transcription factors such as nuclear factor kappa B (NF-κB), a key regulator of pro-
atherosclerotic and pro-inflammatory gene targets in VSMC, endothelial cells and
macrophages (Avogaro, de Kreutzenberg, & Fadini, 2008; Brownlee, 2005; Creager,
Lüscher, Cosentino, & Beckman, 2003; Little, Chait, & Bobik, 2011). Endothelial cells
exposed to hyperglycaemic culture media show enhanced NF-κB activation with reduced NO
production, leukocyte recruitment and inflammatory gene expression (Ding, Vaziri, Coulson,
Kamanna, & Roh, 2000; X. L. Du, et al., 2001; Esposito, et al., 2001; Luppi, Cifarelli, Tse,
Piganelli, & Trucco, 2008; Piconi, et al., 2004; Piga, Naito, Kokura, Handa, & Yoshikawa,
2007).
8.3 Advanced Glycation End Products (AGEs) and endothelial dysfunction
Hyperglycaemia promotes non-enzymatic glycation of intracellular and extracellular
proteins, culminating in the formation of AGEs which subsequently accumulate in the
vascular wall and decrease NO activity and eNOS expression and increase the expression of
ET-1 (Avogaro, et al., 2008; Ballinger, et al., 2005; Quehenberger, et al., 2000; Soldatos,
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Cooper, & Jandeleit-Dahm, 2005). Modification of extracellular proteins, e.g. laminin and
collagen, increase fluid filtration and decreases vessel elasticity (Huijberts, et al., 1993). AGE
modification of intracellular and extracellular proteins affects their functions and receptor
binding properties. Binding of AGEs to their receptors (RAGE) increases intracellular
enzymatic superoxide production (Schmidt, Du Yan, Wautier, & Stern, 1999; Wautier, et al.,
2001). Excessive production of ROS by AGEs activates NF-κB and TNFα, which further
enhances the production of superoxide (J. Kim, Lee, Park, & Yoo, 2010; Roberge, et al.,
2014; Ungvari, et al., 2007).
Under hyperglycaemic conditions, a number of biochemically active substances such
as 3-deoxyglucosone, amadori products, diacylglycerol, methylglyoxal, ROS, AGE and
nitrosylated species are produced which contribute to and promote diabetes-associated
endothelial dysfunction (Cristina M Sena, et al., 2012). Thus, oxidative stress seems to be a
common alteration triggered by hyperglycaemia adjoined by hyperinsulinemia,
hyperlipidaemia and insulin resistance (Potenza, Gagliardi, Nacci, Carratu, & Montagnani,
2009).
8.4 Oxidative stress and endothelial dysfunction
Within the vessel wall, oxygen derived radicals like superoxide anions are generated
by a variety of enzymatic mechanisms. Molecular sources of ROS in the vasculature include
enzymes of the respiratory chain, specific NADPH oxidase (NOX) complexes, xanthine
oxidase, uncoupled eNOS, cyclooxygenase, lipoxygenase and cytochromeP450
monooxygenase (Cai & Harrison, 2000; Ježek & Hlavatá, 2005; Leopold & Loscalzo, 2009;
Ray & Shah, 2005; Rueckschloss, Duerrschmidt, & Morawietz, 2003; Soccio, Toniato,
Evangelista, Carluccio, & De Caterina, 2005; Turrens, 2003). NOXs are the only enzyme
with the primary function of generating ROS (Drummond, Selemidis, Griendling, & Sobey,
2011; Lassègue, San Martín, & Griendling, 2012). Under normal physiological conditions,
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
the detrimental effects of ROS are counter-balanced by vascular antioxidant enzymes
including catalases, superoxide dismutases, glutathione peroxidases,
glutathione S-transferases, glucose-6-phosphate dehydrogenases and heme oxygenase
(Leopold & Loscalzo, 2009). In a state of oxidative imbalance, excessive production of ROS
is implicated in the pathogenesis of various diseases including ageing, dementia,
ischemia-reperfusion injury and atherosclerosis (Madamanchi, Vendrov, & Runge, 2005).
Thus, increased oxidative stress is another important mechanism of endothelial dysfunctio n in
diabetes mellitus and associated conditions.
9. The biguanide anti-hyperglycaemic agent, metformin
Metformin is an old drug that has been used to treat diabetes for 60 years (Bailey &
Turner, 1996; Triggle & Ding, 2017). In recent times, it has evolved to be the first line
pharmacological choice for the treatment of Type 2 diabetes. Metformin is a member of the
biguanide family of drugs, which include phenformin and buformin. Phenformin and
buformin, showed a very high risk of severe lactic acidosis events, whilst the risk of lactic
acidosis with metformin remains low and was probably overstated in its earlier use.
As for many drugs, the use of metformin has occurred without a full understanding of
its mechanism of action, but recent investigations provide expanding knowledge in this area.
Metformin exerts its anti-hyperglycaemic effect in several ways. Metformin primarily lowers
glucose levels in blood by increasing insulin sensitivity and thus increasing uptake of glucose
by muscle cells and by reducing production in the liver. New studies investigated the effect of
metformin on the incretin and GLP1 systems (Zhao, et al., 2015), showing intestinal AMPK
pathways increasing secretion of GLP1 and related peptides (DeFronzo, et al., 2016). The gut
directed action is an important component of the anti-hyperglycaemic action of metformin.
In skeletal muscle, metformin improves the uptake of glucose into cells via activation
of the solute carriers (SLC2A4) and GLUT4 deployment. Inhibition of complex 1, in the
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
mitochondrial respiratory chain, decreases the ATP/AMP ratio (leading to increased
activation of AMPK). This action inhibits the production of glucose-6-phosphatase
dehydrogenase (G6PDH) (mimicking the normal feedback mechanism and reduces the
production of glucose) and phosphoenolpyruvate carboxykinase (PEPCK). It is the
interference with glycogenolysis and glycolysis by metformin that leads to the production of
lactic acid, where tissues are hypoperfused or hypoxic and the rare potential development of
lactic acidosis (Salpeter, Greyber, Pasternak, & Salpeter, 2003).
Metformin raises the tissue concentration of hydrogen sulphide (H2S), which is an
atheroprotective gasotransmitter (Hamidi Shishavan, et al., 2017; Xu, Liu, & Liu, 2014). H2S
functions as a vasculoprotective factor by sulfhydrating potassium channels and acting as an
EDHF (Félétou M. , 2011). EDHF-mediated responses are modified in various pathological
conditions (hypertension, atherosclerosis, hypercholesterolemia, heart fa ilure, ischemia–
reperfusion, angioplasty, eclampsia, diabetes, sepsis) and with aging (Feletou & Vanhoutte,
2004, 2006). This could be the mechanism for enhanced acetylcholine induced relaxation
seen when metformin was used (Marfella, et al., 2010).
Metformin attenuates fluctuating glucose-induced endothelial dysfunction through
enhancing guanosine 5′-triphosphate cyclohydrolase 1 (GTPCH1) mediated eNOS recoupling
and inhibiting NADPH oxidase (An, et al., 2016). Endothelial dysfunction, characterised by
reduced NO bioavailability, is involved in the initiation and progression of the vascular
complications of diabetes (Davignon & Ganz, 2004; Esper et al, 2006). eNOS is responsible
for most of the endothelial NO production. GTPCH1 is a rate limiting enzyme to
produce BH4, and if BH4 production falls then NO production is reduced.
Currently, G6PDH appears to be the mitochondrial target of action of metformin.
G6PDH is inhibited by the hyperglycaemia-mediated increase in protein kinase A and is the
rate limiting step in the pentose phosphate pathway (J. Zhang, et al., 2016). Reduced G6PD
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
activity reduces NADPH levels, the cells’ principal reductant molecule, leading to an increase
in oxidative stress. Metformin mediated increase in AMPK, will reduce PKA signalling
through phosphorylation of the CREB cycle, reversing hyperglycaemia induced inhibition of
G6PDH and reducing oxidative stress (C. H. Lee & Yu, 2016; Triggle & Ding, 2017).
Triggle et al (Triggle & Ding, 2017) identified a number of endothelium-specific micro
RNAs as regulators of endothelial function, and linked them to regulation of angiogenesis
(cell proliferation, aging and apoptosis) and the development of diabetes- induced endothelial
dysfunction and inflammation (Triggle & Ding, 2017). High glucose increases the levels of
miR34a in microvascular endothelial cells and this is prevented by metformin (Triggle &
Ding, 2017). Metformin is therefore thought to have a direct effect on endothelial function
through antioxidant effects via regulation of eNOS, improved NO production, inhibition of
mitochondrial complex 1, activation of AMPK and inhibition of apoptosis (Triggle & Ding,
2017). Regardless of the cell Type, AMPK activation can explain most, if not all of the
cellular actions of metformin.
Blood levels of metformin are obviously relevant to the actions of metformin. Importantly,
metformin is not metabolised in animals or humans and is eliminated intact via renal
mechanisms (He & Wondisford, 2015). One implication of this metabolic profile is that
metformin is less sensitive to metabolic drug interactions and interactions arise related to the
uptake and transport mechanisms that move metformin around the body. The maximum dose
of metformin orally in humans in most settings is 2.5-3 g per day which equates to
approximately 35-42 mg/kg (Davoren, 2014; He & Wondisford, 2015). This produces a
trough steady-state plasma concentration for metformin of between 54 to 4133ng/ml and is
highly dependent on the individual (Christensen, et al., 2011; Gong, Goswami, Giacomini,
Altman, & Klein, 2012). The difficulty of recognising therapeutic concentrations of
metformin has recently been reviewed (Kajbaf, De Broe, & Lalau, 2016). In humans
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
metformin concentrations after passage through the liver are usually in the range of 10 – 40
µM (He, 2015).
Plasma concentrations of metformin in animal studies are in the range of 10 -70 µM (He &
Wondisford, 2015; Wilcock & Bailey, 1994). Doses of metformin used in rat studies are
typically in the range of 100 mg/kg , in excess of doses attainable in human in vivo
studies(Pournaghi, Sadrkhanlou, Hasanzadeh, & Foroughi, 2012). Palmitic acid induced
endothelial dysfunction in HUVECS was attenuated by metformin at 0.5-1mM
concentrations (Ke, et al., 2017). Metformin has been used for in vitro studies at
concentrations up to 10 mM (Dallaglio, et al., 2014; Little, et al., 2007) which greatly
exceeds in vivo concentrations and such studies reveal actions of metformin that may be
interesting but are not clinically or therapeutically relevant.
10. Metformin and endothelial dysfunction
Clinical studies of metformin action on hyperglycaemia and associated insulin
resistance have addressed its effects on endothelial dysfunction. In 2001, Mather et al
(Mather, Verma, & Anderson, 2001) evaluated the effect of metformin on endothelial
function in patients with Type 2 diabetes and observed that metformin intake improves
insulin resistance and endothelium-dependent vasodilation assessed using forearm
plethysmography; endothelium-independent and nitrate-independent vasodilation remained
unaffected in these studies. These data indicate that metformin induced insulin sensitivity
associates with its vasodilatory effects. Since inflammation is a factor in different phases of
atherosclerosis, long-term treatment (4.3 years) with metformin added to insulin therapy
attenuates several inflammatory biomarkers of endothelial dysfunction (such as vWF and
soluble VCAM-1) in patients with Type 2 diabetes, indicating the potential utility of
metformin in reducing cardiovascular morbidity and mortality (de Jager, et al., 2014).
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Similarly, in 2005, Vitale et al (Vitale, et al., 2005) examined the effect of metformin (500
mg, b.i.d, 3 months) on endothelial function in 65 patients with metabolic syndrome and
observed that metformin treatment improved endothelium-dependent flow-mediated
dilatation in the brachial artery and insulin resistance (measured by homeostasis model
assessment- insulin resistance or HOMA-IR), indicating that insulin resistance and endothelial
dysfunction are interrelated and can be influenced by metformin. Metformin treatment also
improves flow-mediated dilation in patients with Type 1 diabetes (Pitocco, et al., 2013). The
REMOVAL trial in Type 1 diabetes showed no benefit in endothelial dysfunction from
glycaemic control, however, it did indicate benefit in cardiovascular risk (Petrie, et al.). Other
studies (Jensterle, et al., 2008; Naka, et al., 2011) involving women with polycystic ovary
syndrome (PCOS) treated with metformin or rosiglitazone, showed that metformin is as
effective as rosiglitazone in improving flow mediated vasodilation, without affecting
endothelium-independent relaxation. Metformin treatment is also associated with a decrease
in HOMA-IR. Metformin treatment for 3 months improves arterial stiffness and associated
endothelial dysfunction as well as reducing carotid intima media thickness in women with
PCOS (Agarwal, et al., 2010; Kaya, et al., 2015). There are several clinical trials
(https://clinicaltrials.gov) addressing the effects of metformin alone (NCT00169624) or in
combination with other anti-diabetic drugs in patients with Type 2 diabetes (NCT00169624)
and PCOS (NCT01459445). Therefore, metformin monotherapy or in combination with other
anti-diabetic strategies represents a useful therapeutic option for targeting the endothelial
dysfunction which accompanies hyperglycaemia and insulin resistance. The UKDPS data
from the aggregate of all the studies showed there were fewer diabetes-related endpoints
(RR 19% [2-33], p=0.033) in the metformin group (UK Prospective Diabetes Study
(UKPDS) Group, 1998).
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
11. Molecular mechanism(s) of metformin actions in improving endothelial dysfunction
11.1 Inhibition of inflammatory response and oxidative stress in endothelial cells
An earlier study in 2003 showed that metformin (0.1—2.5 µg/ml) inhibited monocyte
adhesion induced by advanced glycation end-products (AGE) by repressing endothelial cell
adhesion molecules (Mamputu, Wiernsperger, & Renier, 2003). This pharmacological effects
was also observed by Hattori et al (Hattori, Suzuki, Hattori, & Kasai, 2006) who showed that
metformin (2-10 mM), like the AMPK activator AICAR, inhibits endothelial cell
inflammation via AMPK-dependent inhibition of the IKK/IKBα/NF-KB pathway. The
consequence of metformin treatment is the inhibition of the TNF-α–induced gene expression
of VCAM-1, E-selectin, ICAM-1, and MCP1, which contribute to monocyte adhesion to
activated endothelial cells. Pro-inflammatory cytokines like VCAM1 and MCP1 are also
repressed by corepressor BCL6, and PARP1 suppresses BCL6 expression by binding to
intron 1 of BCL6. Metformin (1 mM) up regulates BCL6 expression via AMPK-dependent
phosphorylation of PARP1 at ser177 (Gongol, et al., 2013), suggesting that metformin could
be a useful agent in preventing monocyte adhesion to endothelial cells. Additional
mechanisms of action of metformin include the inhibition of LOX-1 signalling, which is an
important mediator in endothelial dysfunction and atherosclerosis (Xu, et al., 2013). By
ameliorating oxLDL-induced LOX-1 expression, metformin (20µM) decreases intracellular
oxidative stress (Hung, Chan, Chu, Lin, & Tsai, 2016). The anti-oxidative function of
metformin (10 µM- 1 mM) is also related to inhibition of TRAF3IP2 (Valente, Irimpen,
Siebenlist, & Chandrasekar, 2014).
11.2 Improved NO production and endothelium-dependent vasorelaxation
eNOS dependent NO production increases endothelium-dependent relaxation.
Metformin (60mg/kg/d) treatment restores endothelial function in the aorta of STZ-treated
rats (Type 1 diabetes model) as well as Goto-Kakizaki (GK) rats (Type 2 diabetes model) by
increasing NO bioavailability and normalizes endothelium-dependent vasorelaxation (C. M.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Sena, et al., 2011). In 2006, a landmark study by the Zou group identified that AMPK
activation by therapeutically relevant concentrations of metformin (50-500μM) increased NO
production via increasing eNOS phosphorylation and eNOS interaction with HSP90. Of
clinical relevance, metformin restored impaired eNOS-HSP90 interaction in endothelial cells
exposed to high glucose levels (Davis, Xie, Viollet, & Zou, 2006). The eNOS activating
effect of metformin (250 mg/kg/d) has also been demonstrated in endothelial progenitor cells
from STZ-induced diabetic mice (J. W. Yu, et al., 2016). In agreement with these data,
metformin (300 mg/kg/d) treatment also increase protein expression of GCH1 (the rate-
limiting enzyme in BH4 biosynthesis) in wild type as well as Ins2 (+/Akita) mice and
glomerular endothelial cells by slowing down the degradation rate of GCH1, without
affecting GCH1 gene expression. This suggests that the upregulation of GCH1 by metformin
occurs through a posttranslational mechanism (Kidokoro, et al., 2013). Metformin (300
mg/kg/d) mediated upregulation of GCH1 protein expression (but not gene expression) is also
seen in streptozotocin- induced diabetic mice and high glucose treated human endothelial cells
by preventing proteasome-mediated GCH1 degradation (S. Wang, Xu, Song, Viollet, & Zou,
2009). Since metformin induced GCH1 upregulation can be reversed by a dominant negative
mutant of AMPK (S. Wang, et al., 2009), it is highly possible that AMPK is involved in the
GCH1 upregulatory effects of metformin. Metformin (100 mg/kg/d) also increases NO
bioavailability by inhibiting ER stress and ROS generation via AMPK and PPARδ pathways
(Cheang, et al., 2014). These protective actions contribute to the improved endothelium-
dependent relaxation in mice under diabetic and obese conditions (Cheang, et al., 2014).
11.3 Inhibition of endothelial senescence and apoptosis
The senescence and apoptosis of endothelial cells is an important contributor to
endothelial dysfunction by increasing pro- inflammatory cytokine expression and cell cycle
arrest. High glucose induces endothelial cell senescence by repressing SIRT1 expression.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Metformin (50µM) improves endothelial senescence in high glucose treated endothelial cells
by increasing SIRT1 expression and activity, thereby repressing high glucose induced
endothelial cell aging and apoptosis (Arunachalam, Samuel, Marei, Ding, & Triggle, 2014).
In addition, metformin (50µM) also repressed senescent “memory” induced by high glucose
through increasing SIRT1 activity (E. Zhang, et al., 2015). Under diabetic conditions,
excessive high level of blood glucose causes endothelial injury and apoptosis. In this regard,
metformin (100µM) ameliorates high glucose induced cell death in endothelial cells from
multiple origins by suppressing mitochondrial permeability transition (Detaille, et al., 2005).
11.4 Improved vascular integrity
Increased vascular permeability causes endothelial leakage and the extravasation of
monocytes. Metformin (0.1-1 mM) decreases vascular permeability in brain endothelial cells
via AMPK, suggesting the utility of metformin in preventing the initiating event of
endothelial dysfunction in endothelial cells (Takata, et al., 2013). Endothelial glycocalyx is
an important Type of matrix structure that prevents vascular permeability. Metformin (0.33
mg/ml) treatment of db/db mice leads to improved glycocalyx barrier function and prevents
edema in the heart and kidney of the mice (Eskens, Zuurbier, van Haare, Vink, & van
Teeffelen, 2013). Metformin (5mM for in vitro studies, and 400mg/kg bid for in vivo studies)
decreases permeability in endothelial cells stimulated with high glucose and LPS as well as
improving lung barrier integrity in both STZ-induced diabetic and db/db mice models; the
mechanism is linked to the activation of the LKB1/AMPK pathway (Y. Yang, et al., 2017).
12. New mechanistic insights into the actions of metformin in cardiovascular and other
systems
12.1 Epigenetic effects of metformin
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Emerging evidence has shown that metformin also has epigenetic functions, which has been
reviewed elsewhere recently (Bridgeman, Ellison, Melton, Newsholme, & Mamotte, 2018).
Metformin can influence the activation of multiple epigenetic modifiers, mostly via AMPK,
since AMPK can phosphorylate multiple substrates, including histone acetyltransferases,
class II histone deacetylases (HDACs) and DNA/histone methyltransferases, thus leading to
their inhibition; Metformin can also increase SIRT1 activity and protect against high glucose
induced "memory" in endothelial cells (E. Zhang, et al., 2015). In addition, Metformin delays
endothelial senescence via AMPK-dependent upregulation of histone methyltransferse
DOTL1, thereby increasing binding of H3K79me3 to SIRT3 gene promoter (Karnewar, et al.,
2018). These epigenetic effects of metformin underlies its broad regulatory effects on gene
expression. More recently, Chen et al (Y. C. Chen, et al., 2018) have shown that metformin
(1-50 µM) has anti- inflammatory effects by reducing the expression IP-10, MCP-1 and NF-
kB phosphorylation in LPS-stimulated THP1 cells. Furthermore, the authors observed that
metformin reduces IL-10 expression by reducing the binding of global acetylated histones H3
and H4 to IP-10 gene promoter in LPS-stimulated THP-1 cell. In another study by Tang et al.
(Tang, et al., 2018), Metformin (2.5-10 mM) has been reported to inhibit the proliferation
and migration, and promotes apoptosis of ovarian cancer cells by increasing AMPK
phosphorylation, and reducing PRC2 components expression and associated H3K27
trimethylation. Moreover, EZH2 overexpression abrogated the anti-cancer effect
of metformin. This epigenetic effect of metformin is AMPK-dependent, since AMPK
inhibition by Compound C, abolishes the effect of metformin on reducing H3K27me3. In
light of recently evidence showing atherogenic role of PRC2 component EZH2 (Lv, et al.,
2016; Xiaoling, et al., 2016) and associated H3K27me3 (Xu, et al., 2018) in atherosclerosis,
it will be of interest whether metformin reduces PCR2 components and activity in endothelial
cells. Further research into this area will reveal a novel mode of action for metformin and
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
raises the possibility that metformin may be exploited as epigenetic drug that could affect
atherogenic processes, including endothelial dysfunction.
12.2. Metformin on autophagy
Decreased AMPK activity and associated defective autophagy is associated with
atherosclerosis. After incubating with in high glucose (25 mM) and subsequently with 0.4
mM palmitate, human aortic endothelial cells displayed decreased AMPK activation,
impaired autophagy and are prone to apoptosis and enhanced monocyte adhesion to
endothelial cells. These effects are reversed by autophagy activator rapamycin and AMPK
activators (AICAR, A769662, and phenformin). This study suggests that AMPK activation
could prevent glucose and palmitate induced AMPK uncoupling from autophagy in
endothelial cells (Weikel, Cacicedo, Ruderman, & Ido, 2015). In vivo, administration of
metformin (250 mg/kg/d) in ApoE-/- mice lead to significant reduction and stabilization of
atherosclerotic plaques, associated with increased content of smooth muscle cells, and
collagen, as well as reduced content of macrophages (Michiels, Apers, De Meyer, &
Martinet, 2016). Metformin treatment also induce autophagy by reducing SQSTM1/p62 and
increasing GFP-LC3 cleavage into free GFP in GFP-LC3 transgenic mice. In cultured
endothelial cells, 2 days treatment of metformin (10 mM) attenuates monocyte adhesion to
TNFa-activated endothelial cells via repressing ICAM1 and VCAM1. However, metformin
mediated protective effects was reversed by autophagy inhibition using Atg7 siRNA-
mediated depletion (Michiels, et al., 2016). It remains to be clarified whether AMPK is
involved in metformin mediated autophagy induction in endothelial cells.
12.3. Metformin on endothelial cell metabolism
Recently, endothelial cell metabolism (such as glucose, fatty acid, lipid etc) has been shown
to be critical for maintaining metabolic health. In 1996, Sasson et al. (Sasson, et al., 1996)
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
showed that metformin (1-5 mM) regulates hexose transport in both bovine endothelial cells
and smooth muscle cells. Glucose-starvation induces ER stress in mouse microvascular
endothelial cells, after treatment with metformin (50 μM and 2 mM), glucose-starvation
induced ER stress, was revered. This pharmacological action is exerted through an AMPK-
independent mechanism (Samuel, et al., 2017).
12.4. Metformin on other kinases and transcriptional factors
LKB1 is one of the upstream kinase of AMPK. Metformin (1 mM) increased the LKB1
phosphorylation at Ser428 and its subsequent nuclear export into the cytosols, and increases
AMPK/LKB1 association in ECs (Xie, Dong, Scholz, Neumann, & Zou, 2008). In addition,
Metformin has been shown to influence other kinase activity. For example, Metformin (500
µM) protects against free fatty acid (palmitate) induced endothelial apoptosis and
dysfunction, partially by reducing p38 MAPK phosphorylation. This inhibitory effects of
metformin on p38 is AMPK-dependent, since AMPK inhibition by compound C reverses the
p38 inhibiting effects of metformin (Eriksson & Nystrom, 2014). Metformin (1 mM) also
inhibits basal as well as VEGF-induced phosphorylation of ERK1/2 in an AMPK-dependent
manner (Dallaglio, et al., 2014).
Metformin also modulate gene expression via affecting multiple transcriptional factors, such
as PPARδ, carbohydrate response element-binding protein (ChREBP), forkhead box O1
(FOXO1), p53, and NF-kB (Hattori, et al., 2006). Specifically, PPARδ is critical for
metformin mediated protective effects against ER stress, oxidative stress, and high fat-diet
induced endothelial dysfunction (Cheang, et al., 2014). In endothelial cells, Metformin (1-2
mM) also decreases high glucose- induced upregulation of TXNIP by reducing the nuclear
transport of ChREBP and FOXO1, and their binding to TXNIP promoter. This effect was
reversed by AMPK inhibitor compound C, indicating that metformin impacts ChREBP and
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
FOXO1 in an AMPK-dependent manner (X. Li, et al., 2015). Metformin (2-10 mM) also
dose-dependently inhibits TNFα induced NF-kB (p65 and p50 subunit) activation in
HUVECs, which was reversed by AMPK siRNA, indicating an AMPK-dependent anti-
inflammatory effects (Hattori, et al., 2006). In addition, Metformin (50 µM) modulates
hyperglycaemia- induced endothelial senescence and apoptosis through SIRT1 (Arunachalam,
et al., 2014), thereby reducing FOXO1) and p53 acetylation, and decreasing high glucose-
induced premature senescence in endothelial cells.
13. Conclusions and future directions
Hyperglycaemia has deleterious effects on the cardiovascular system mostly the
vascular system where it is the cause of microvascular disease and is strongly associated with
the occurrence of macrovascular disease. The deleterious biochemical mechanisms of
hyperglycaemia are not completely understood at a molecular level but they are probably
related to the phenomenon of insulin resistance. Metformin improves insulin resistance and
therefore has an anti-hyperglycaemic and insulin- lowering action in patients with Type 2
diabetes. Metformin also has additional actions in the same way as the lipid lowering statins
have favourable pleiotropic, anti- inflammatory and anti-oxidative effects on the vasculature
beyond their lipid lowering actions. The main effect of metformin is on ED where the
integrity of the endothelium is a critical and long-term determinant of vascular health and
thus of the occurrence of CVD. We have reviewed the causes of ED and outlined the effects
of metformin to improve or to prevent deterioration of ED which potentially leads to reduced
CVD in patients with Type 2 diabetes and potentially other settings in which the use of
metformin is being proposed. Metformin has a very simple chemical structure. The dose of
metformin is relatively high and to some extent its actions might be considered alongside that
of nutrients. The simple structure means that it is unlikely that it will be possible to develop
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
new agents with similar or better properties and mechanisms of action so the future relies on
fully exploiting the pharmacokinetics, pharmacodynamics and therapeutic targeting to
achieve the full therapeutic potential of metformin. This approach has recently been
demonstrated by the description of the delayed release metformin product which acts in the
distal gut and reveals a gut hormone-dependent anti-hyperglycaemic action of metformin
Several important classes of drugs for the treatment of hyperglycaemia have shown in large
scale use to display serious unwanted effects such as the bone fractures and heart failure
associated with glitazones and the recent signs of the occurrence of amputations of digits
associated with the use of some SGLT2 inhibitors (S. Lee, 2017; Wu, Ding, Tanaka, &
Zhang, 2014). There does not appear to be a hidden unwanted effects profile for, metformin
so it has the potential to provide a really effective and safe future in the treatment of
hyperglycaemia and especially for its favourable CVD effects including beneficial effects on
ED.
Acknowledgments
We are grateful to the Government of Pakistan for supporting the placement of AN into the
Little Lab at UQ and which allowed her to lead the generation of this manuscript. Funding
supporting the studies in our laboratory and referenced in this review has been received from
the National Health and Medical Research Council of Australia, National Heart Foundation
of Australia, Diabetes Australia Research Trust, academic support packages from RMIT
University (PJL) and the University of Queensland (PJL) and Australian Government
Scholarships to numerous post-graduate students. Suowen Xu is a recipient of Career
Development Award of American Heart Association (18CDA34110359).
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
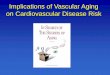
Figure 1
Role of metformin in endothelial dysfunction
Metformin improves endothelial dysfunction via the following aspects: (1) inhibiting
leukocyte adhesion; (2) increase nitric oxide production and inhibiting eNOS uncoupling; (3)
inhibiting vascular aging; (4) prevent endothelial cell injury and apoptosis. The
pharmacological effects of metformin were exerted through LKB1/AMPK and other targets.
Abbreviations: NF-kB, nuclear factor kappa B; ICAM1, intracellular adhesion molecule 1;
VCAM1, vascular adhesion molecule 1; MCP1, monocyte chemo attractant protein 1; Bcl6,
B-cell lymphoma 6; PAPP1-p, phosphorylation of poly-ADP-ribose polymerase 1; LOX-1,
lectin- like oxidized LDL receptor 1; TRAF3IP2, TRAF3 interacting protein 2; NOX,
NADPH oxidase; ROS, reactive oxygen species; Mn-SOD, manganese superoxide dismutase;
AGE, advanced glycation end-products; eNOS, endothelial nitric oxide synthase; eNOS-p,
phosphorylation of eNOS; HSP90, heat shock protein 90; GCH1, GTP cyclohydrolase I;
BH4, tetrahydrobiopterin; PPARδ, peroxisome proliferator-activated receptor δ; PGC1α,
PPARgamma Coactivator 1alpha; ER, endoplasmic reticulum; mTOR, the mammalian target
of rapamycin; Sirt1, Sirtuin 1, mPTP, mitochondrial permeability transition pore.
Conflict of Interest
The authors confirm we have no conflicts of interest of any kind to declare.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Figure 1.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Table. 1. Products modulating the state of the vascular endothelium.
Vasodilators NO (Ignarro, et al., 1987; R MoJ Palmer, et al., 1987)
PGI2 (Egan & FitzGerald, 2006; Moncada, et al., 1976)
Bradykinin (Drexler, 1998),
EDHF (Davignon & Ganz, 2004; Félétou & Vanhoutte,
2006b; Garland, Hiley, & Dora, 2011)
Serotonin
Histamine
Vasoconstrictors ET-1 (Yanagisawa, et al., 1988),
ThromoboxaneA2
AngiotensinII
Arachidonic acid
ProstaglandinH2
Thrombin
ROS
Adhesions molecules ICAM
VCAM
Endothelial cell adhesion molecule
Anticoagulants /
Antithromobotic factors
PAI-1(Kruithof, Nicolosa, & Bachmann, 1987),
t-PA
Thromobodulin,
u –PA (Libby, Aikawa, & Jain, 2006)
Inhibitors Bradykinin
heparin sulphate
Transforming growth factor – beta (TGFβ)
Promoters Platelet derived growth factor
fibroblast growth factor
insulin like growth factor
ET-1
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Table 2. Factors mediating and impacting on endothelial dysfunction.
Notorious stimuli Molecular changes leading to endothelial dysfunction
Hypercholesterolemia
Reduced endothelium dependent vasorelaxation (C. Sena, et al., 2008).
Up regulation of NOX and ROS reducing the bioavailability of
NO, eNOS uncoupling (Böger, et al., 2004; Speer, et al., 2014).
Insulin resistance
Increased production of ROS by NOX(J. Du, Fan, Mai, & Li,
2013)
over-expression of PKCβ and induction of ET-1 expression in
endothelium (Q. Li, et al., 2013) (Tabit, et al., 2012)
increased insulin receptor substrate
Phosphorylation at Ser 307 (Nemoto, Kobayashi, Taguchi, Matsumoto, & Kamata, 2011)
Up regulation of transcription factor forkhead boxO-1 FOXO-
1(Karki, et al., 2015).
Diabetes
Induced endothelial dysfunction
Advanced end glycation product (AGE)
ROS (Paneni, Beckman, Creager, & Cosentino, 2013).
Pro inflammatory
factors
Overexpression of TNFα and IL-1 which promotes leukocyte
adherence and migration (Barton, 2013)
Inflammatory cytokines induced endothelial cells express
VCAM, ICAM, MCP1, IL6, P-selectin and E –selectin and exacerbate the ED (Blake & Ridker, 2001)
C- reactive protein directly affects NO bioavailability acting through lectin like oxidised LDL receptor-1 which plays pivotal
role in oxLDL-induced ED in endothelial cells (L. Li, Roumeliotis, Sawamura, & Renier, 2004).
Hypertension
Reduced NO availability in response to endothelium dependent
stimuli in hypertension is attributed to higher levels of ADMA (Sasser, Cunningham, & Baylis, 2014).
Ageing
Aging results in diminished production of NO due
o Increased activity of arginase competing with eNOS for common substrate arginine (Santhanam, et al., 2007)
o Reduced expression and activity of eNOS (Lesniewski, et
al., 2011) o Decrease release of prostanide (Gano, et al., 2014)
o Increase release of ET-1.
Hemodynamic Forces Low sheer stress modulates gene expression through mechanoreception and mechanotransduction resulting in altered
atherogenic endothelial phenoytype and formation of atherosclerotic plaque (Pahakis, Kosky, Dull, & Tarbell, 2007)
Suppression of NO and prostacyclin, augmentation of ET-1, lipid
uptake and its catabolism induce plaque inflammation and oxidation in endothelial cells (White, et al., 2011)
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Environmental factors
Processes in smoking induce atherogenesis, endothelial dysfunction and damage,
Induction of inflammation, increase in oxidation of proatherogenic lipids and shift towards procoagulant state in
circulation (Messner & Bernhard, 2014)
Psychological stress Sleep deprivation decrease eNOS and cGMP levels indicating damaged eNOS/NO/cGMP / pathway(J. Jiang, et al., 2017).
Diet
High salt intake results in blunted endothelium dependent
vasodilation (Beyer, et al., 2014).
Oxidative Stress (H2O2)
Super oxide anions scavenge NO and form peroxynitrate resulting in reduced bioavailability of NO (Montezano & Touyz,
2012) .
ROS cause S-glutathionylation of eNOS and render it inactive
(Y. Zhang, Janssens, Wingler, Schmidt, & Moens, 2011)
Infectious Agents (e.g., bacteria l
endotoxins, viruses)
Infectious agents such as hepatitis A virus, herpes simplex virus-1, cytomegalovirus and bacteria (Helicobactor pylori,and
Chlamydia pneumonia) are reported to be associated with coronary artery disease
Life style (sedentary) Cardiac patients with lower physical activity levels exhibits ED
manifested by reduced flow mediated vasodilation (Luk, et al., 2012)
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
References
A Chistiakov, D., V Revin, V., A Sobenin, I., N Orekhov, A., & V Bobryshev, Y. (2015). Vascular endothelium: functioning in norm, changes in atherosclerosis and current dietary approaches to improve endothelial function. Mini reviews in medicinal chemistry, 15, 338-350.
Agarwal, N., Rice, S. P., Bolusani, H., Luzio, S. D., Dunseath, G., Ludgate, M., & Rees, D. A. (2010). Metformin reduces arterial stiffness and improves endothelial function in young women with polycystic ovary syndrome: a randomized, placebo-controlled, crossover trial. J Clin Endocrinol Metab, 95, 722-730.
An, H., Wei, R., Ke, J., Yang, J., Liu, Y., Wang, X., Wang, G., & Hong, T. (2016). Metformin attenuates fluctuating glucose-induced endothelial dysfunction through enhancing GTPCH1-mediated eNOS recoupling and inhibiting NADPH oxidase. J Diabetes Complications, 30, 1017-1024.
Arunachalam, G., Samuel, S. M., Marei, I., Ding, H., & Triggle, C. R. (2014). Metformin modulates hyperglycaemia-induced endothelial senescence and apoptosis through SIRT1. Br J Pharmacol, 171, 523-535.
Avogaro, A., de Kreutzenberg, S. V., & Fadini, G. (2008). Endothelial dysfunction: causes and consequences in patients with diabetes mellitus. Diabetes Res Clin Pract, 82, S94-S101.
Avruch, J. (1998). Insulin signal transduction through protein kinase cascades. Molecular and Cellular Biochemistry, 182, 31-48.
Bailey, C. J., & Turner, R. C. (1996). Metformin. N Engl J Med, 334, 574-579. Bakker, W., Eringa, E. C., Sipkema, P., & van Hinsbergh, V. W. (2009). Endothelial dysfunction and
diabetes: roles of hyperglycemia, impaired insulin signaling and obesity. Cell Tissue Res, 335, 165.
Ballinger, M. L., Thomas, M. C., Nigro, J., Ivey, M. E., Dilley, R. J., & Little, P. J. (2005). Glycated and carboxy-methylated proteins do not directly activate human vascular smooth muscle cells. Kidney Int, 68, 2756-2765.
Barton, M. (2013). Prevention and endothelial therapy of coronary artery disease. Current opinion in pharmacology, 13, 226-241.
Barton, M., & Haudenschild, C. C. (2001). Endothelium and atherogenesis: endothelial therapy revisited. Journal of Cardiovascular Pharmacology, 38, S23-S25.
Beyer, A. M., Raffai, G., Weinberg, B. D., Fredrich, K., Rodgers, M. S., Geurts, A. M., Jacob, H. J., Dwinell, M. R., & Lombard, J. H. (2014). Amelioration of salt-induced vascular dysfunction in mesenteric arteries of Dahl salt-sensitive rats by missense mutation of extracellular superoxide dismutase. American Journal of Physiology-Heart and Circulatory Physiology, 306, H339-H347.
Blake, G. J., & Ridker, P. M. (2001). Novel clinical markers of vascular wall inflammation. Circulation Research, 89, 763-771.
Böger, R. H., Tsikas, D., Bode-Böger, S. M., Phivthong-ngam, L., Schwedhelm, E., & Frölich, J. C. (2004). Hypercholesterolemia impairs basal nitric oxide synthase turnover rate: a study investigating the conversion of l-[guanidino-15 N 2]-arginine to 15 N-labeled nitrate by gas chromatography–mass spectrometry. Nitric Oxide, 11, 1-8.
Bridgeman, S. C., Ellison, G. C., Melton, P. E., Newsholme, P., & Mamotte, C. D. S. (2018). Epigenetic effects of metformin: From molecular mechanisms to clinical implications. Diabetes Obes Metab.
Brownlee, M. (2001). Biochemistry and molecular cell biology of diabetic complications. Nature, 414, 813-820.
Brownlee, M. (2005). The pathobiology of diabetic complications. Diabetes, 54, 1615-1625. Cai, H., & Harrison, D. G. (2000). Endothelial dysfunction in cardiovascular diseases: the role of
oxidant stress. Circulation Research, 87, 840-844.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Cernea, S. (2011). The Role of Incretin Therapy at Different Stages of Diabetes. The Review of Diabetic Studies : RDS, 8, 323-338.
Cheang, W. S., Tian, X. Y., Wong, W. T., Lau, C. W., Lee, S. S., Chen, Z. Y., Yao, X., Wang, N., & Huang, Y. (2014). Metformin protects endothelial function in diet-induced obese mice by inhibition of endoplasmic reticulum stress through 5' adenosine monophosphate-activated protein kinase-peroxisome proliferator-activated receptor delta pathway. Arterioscler Thromb Vasc Biol, 34, 830-836.
Chen, S., Apostolova, M. D., Cherian, M. G., & Chakrabarti, S. (2000). Interaction of endothelin-1 with vasoactive factors in mediating glucose-induced increased permeability in endothelial cells. Laboratory Investigation, 80, 1311.
Chen, Y. C., Kuo, C. H., Tsai, Y. M., Lin, Y. C., Hsiao, H. P., Chen, B. H., Chen, Y. T., Wang, S. L., & Hung, C. H. (2018). Suppressive effects of metformin on T-helper 1-related chemokines expression in the human monocytic leukemia cell line THP-1. Endocr Res, 1-7.
Chiu, J.-J., & Chien, S. (2011). Effects of disturbed flow on vascular endothelium: pathophysiological basis and clinical perspectives. Physiological reviews, 91, 327-387.
Christensen, M. M., Brasch-Andersen, C., Green, H., Nielsen, F., Damkier, P., Beck-Nielsen, H., & Brosen, K. (2011). The pharmacogenetics of metformin and its impact on plasma metformin steady-state levels and glycosylated hemoglobin A1c. Pharmacogenet Genomics, 21, 837-850.
Cornwell, T. L., Arnold, E., Boerth, N. J., & Lincoln, T. M. (1994). Inhibition of smooth muscle cell growth by nitric oxide and activation of cAMP-dependent protein kinase by cGMP. Am J Physiol, 267, C1405-1413.
Creager, M. A., Lüscher, T. F., Cosentino, F., & Beckman, J. A. (2003). Diabetes and vascular disease. Circulation, 108, 1527-1532.
Dallaglio, K., Bruno, A., Cantelmo, A. R., Esposito, A. I., Ruggiero, L., Orecchioni, S., Calleri, A., Bertolini, F., Pfeffer, U., Noonan, D. M., & Albini, A. (2014). Paradoxic effects of metformin on endothelial cells and angiogenesis. Carcinogenesis, 35, 1055-1066.
Davignon, J., & Ganz, P. (2004). Role of endothelial dysfunction in atherosclerosis. Circulation, 109, III-27-III-32.
Davis, B. J., Xie, Z., Viollet, B., & Zou, M. H. (2006). Activation of the AMP-activated kinase by antidiabetes drug metformin stimulates nitric oxide synthesis in vivo by promoting the association of heat shock protein 90 and endothelial nitric oxide synthase. Diabetes, 55, 496-505.
Davoren, P. (2014). Safe prescribing of metformin in diabetes. Australian Prescriber, 37, 2-5. de Graaf, J. C., Banga, J. D., Moncada, S., Palmer, R. M., de Groot, P. G., & Sixma, J. J. (1992). Nitric
oxide functions as an inhibitor of platelet adhesion under flow conditions. Circulation, 85, 2284.
de Jager, J., Kooy, A., Schalkwijk, C., van der Kolk, J., Lehert, P., Bets, D., Wulffele, M. G., Donker, A. J., & Stehouwer, C. D. (2014). Long-term effects of metformin on endothelial function in type 2 diabetes: a randomized controlled trial. J Intern Med, 275, 59-70.
DeFronzo, R. A., Buse, J. B., Kim, T., Burns, C., Skare, S., Baron, A., & Fineman, M. (2016). Once-daily delayed-release metformin lowers plasma glucose and enhances fasting and postprandial GLP-1 and PYY: results from two randomised trials. Diabetologia, 59, 1645-1654.
Detaille, D., Guigas, B., Chauvin, C., Batandier, C., Fontaine, E., Wiernsperger, N., & Leverve, X. (2005). Metformin prevents high-glucose-induced endothelial cell death through a mitochondrial permeability transition-dependent process. Diabetes, 54, 2179-2187.
Dimmeler, S., Fleming, I., Fisslthaler, B., Hermann, C., Busse, R., & Zeiher, A. M. (1999). Activation of nitric oxide synthase in endothelial cells by Akt-dependent phosphorylation. Nature, 399, 601-605.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Ding, Y., Vaziri, N. D., Coulson, R., Kamanna, V. S., & Roh, D. D. (2000). Effects of simulated hyperglycemia, insulin, and glucagon on endothelial nitric oxide synthase expression. American Journal of Physiology-Endocrinology And Metabolism, 279, E11-E17.
Drexler, H. (1998). Factors involved in the maintenance of endothelial function. The American journal of cardiology, 82, S3-S4.
Drummond, G. R., Selemidis, S., Griendling, K. K., & Sobey, C. G. (2011). Combating oxidative stress in vascular disease: NADPH oxidases as therapeutic targets. Nature reviews. Drug discovery, 10, 453.
Du, J., Fan, L. M., Mai, A., & Li, J. M. (2013). Crucial roles of Nox2‐derived oxidative stress in deteriorating the function of insulin receptors and endothelium in dietary obesity of
middle‐aged mice. British Journal of Pharmacology, 170, 1064-1077. Du, X., Matsumura, T., Edelstein, D., Rossetti, L., Zsengellér, Z., Szabó, C., & Brownlee, M. (2003).
Inhibition of GAPDH activity by poly (ADP-ribose) polymerase activates three major pathways of hyperglycemic damage in endothelial cells. Journal of Clinical Investigation, 112, 1049.
Du, X. L., Edelstein, D., Dimmeler, S., Ju, Q., Sui, C., & Brownlee, M. (2001). Hyperglycemia inhibits endothelial nitric oxide synthase activity by posttranslational modification at the Akt site. Journal of Clinical Investigation, 108, 1341.
Egan, K., & FitzGerald, G. (2006). Eicosanoids and the vascular endothelium. In The Vascular Endothelium I (pp. 189-211): Springer.
Endemann, D. H., & Schiffrin, E. L. (2004). Endothelial dysfunction. Journal of the American Society of Nephrology, 15, 1983-1992.
Eriksson, L., & Nystrom, T. (2014). Activation of AMP-activated protein kinase by metformin protects human coronary artery endothelial cells against diabetic lipoapoptosis. Cardiovasc Diabetol, 13, 152.
Erusalimsky, J. D. (2009). Vascular endothelial senescence: from mechanisms to pathophysiology. Journal of Applied Physiology, 106, 326-332.
Eskens, B. J., Zuurbier, C. J., van Haare, J., Vink, H., & van Teeffelen, J. W. (2013). Effects of two weeks of metformin treatment on whole-body glycocalyx barrier properties in db/db mice. Cardiovasc Diabetol, 12, 175.
Esposito, C., Fasoli, G., Plati, A., Bellotti, N., Conte, M. M., Cornacchia, F., Foschi, A., Mazzullo, T., Semeraro, L., & Dal Canton, A. (2001). Long-term exposure to high glucose up-regulates VCAM-induced endothelial cell adhesiveness to PBMC. Kidney International, 59, 1842-1849.
Fanelli, A., Ghisi, D., Aprile, P. L., & Lapi, F. (2017). Cardiovascular and cerebrovascular risk with nonsteroidal anti-inflammatory drugs and cyclooxygenase 2 inhibitors: latest evidence and clinical implications. Therapeutic Advances in Drug Safety, 8, 173-182.
Fang, J., Little, P. J., & Xu, S. (2017). Atheroprotective Effects and Molecular Targets of Tanshinones Derived From Herbal Medicine Danshen. Med Res Rev.
Feletou, M., & Vanhoutte, P. M. (2004). EDHF: new therapeutic targets? Pharmacol Res, 49, 565-580. Feletou, M., & Vanhoutte, P. M. (2006). Endothelial dysfunction: a multifaceted disorder (The
Wiggers Award Lecture). Am J Physiol Heart Circ Physiol, 291, H985-1002. Félétou, M., & Vanhoutte, P. M. (2006a). Endothelial dysfunction: a multifaceted disorder (the
Wiggers Award Lecture). American Journal of Physiology-Heart and Circulatory Physiology, 291, H985-H1002.
Félétou, M., & Vanhoutte, P. M. (2006b). Endothelium-derived hyperpolarizing factor. Arteriosclerosis, Thrombosis, and Vascular Biology, 26, 1215-1225.
Félétou M. . (2011). The Endothelium: Part 2: EDHF-Mediated Responses “The Classical Pathway” (Vol. Part 2: EDHF-Mediated Responses “The Classical Pathway”). California: Morgan & Claypool Life Sciences.
Furchgott, R., & Zawadzki, J. (1980). The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Nature, 288, 373-376.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Gano, L. B., Donato, A. J., Pasha, H. M., Hearon, C. M., Sindler, A. L., & Seals, D. R. (2014). The SIRT1 activator SRT1720 reverses vascular endothelial dysfunction, excessive superoxide production, and inflammation with aging in mice. American Journal of Physiology-Heart and Circulatory Physiology, 307, H1754-H1763.
Garland, C. J., Hiley, C. R., & Dora, K. A. (2011). EDHF: spreading the influence of the endothelium. British Journal of Pharmacology, 164, 839-852.
Ghosh, A., Gao, L., Thakur, A., Siu, P. M., & Lai, C. W. (2017). Role of free fatty acids in endothelial dysfunction. J Biomed Sci, 24, 50.
Giacco, F., & Brownlee, M. (2010). Oxidative stress and diabetic complications. Circulation Research, 107, 1058-1070.
Gimbrone, M. A., & García-Cardeña, G. (2016). Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circulation Research, 118, 620-636.
Gong, L., Goswami, S., Giacomini, K. M., Altman, R. B., & Klein, T. E. (2012). Metformin pathways: pharmacokinetics and pharmacodynamics. Pharmacogenetics and genomics, 22, 820-827.
Gongol, B., Marin, T., Peng, I. C., Woo, B., Martin, M., King, S., Sun, W., Johnson, D. A., Chien, S., & Shyy, J. Y. (2013). AMPKalpha2 exerts its anti-inflammatory effects through PARP-1 and Bcl-6. Proc Natl Acad Sci U S A, 110, 3161-3166.
Goyeneche, A. A., Harmon, J. M., & Telleria, C. M. (2006). Cell death induced by serum deprivation in luteal cells involves the intrinsic pathway of apoptosis. Reproduction, 131, 103-111.
Gray, S. G., McGuire, T., Cohen, N., & Little, P. J. (2017). The emerging role of metformin in gestational diabetes mellitus. Diabetes, Obesity and Metabolism.
Haffner, S. M. (1997). The scandinavian simvastatin survival study (4S) subgroup analysis of diabetic subjects: Implications for the prevention of coronary heart disease. Diabetes Care, 20, 469-471.
Hajer, G. R., van Haeften, T. W., & Visseren, F. L. J. (2008). Adipose tissue dysfunction in obesity, diabetes, and vascular diseases. European Heart Journal, 29, 2959-2971.
Hamidi Shishavan, M., Henning, R. H., van Buiten, A., Goris, M., Deelman, L. E., & Buikema, H. (2017). Metformin Improves Endothelial Function and Reduces Blood Pressure in Diabetic Spontaneously Hypertensive Rats Independent from Glycemia Control: Comparison to Vildagliptin. Scientific reports, 7, 10975.
Hattori, Y., Suzuki, K., Hattori, S., & Kasai, K. (2006). Metformin inhibits cytokine-induced nuclear factor kappaB activation via AMP-activated protein kinase activation in vascular endothelial cells. Hypertension, 47, 1183-1188.
He, L., & Wondisford, F. E. (2015). Metformin action: concentrations matter. Cell Metab, 21, 159-162.
Ho, F. M., Lin, W. W., Chen, B. C., Chao, C. M., Yang, C.-R., Lin, L. Y., Lai, C. C., Liu, S. H., & Liau, C. S. (2006). High glucose-induced apoptosis in human vascular endothelial cells is mediated through NF-κB and c-Jun NH 2-terminal kinase pathway and prevented by PI3K/Akt/eNOS pathway. Cell Signal, 18, 391-399.
Hoffmann, J., Haendeler, J., Aicher, A., Rössig, L., Vasa, M., Zeiher, A. M., & Dimmeler, S. (2001). Aging enhances the sensitivity of endothelial cells toward apoptotic stimuli. Circulation Research, 89, 709-715.
Hsueh, W. A., & Quiñones, M. J. (2003). Role of endothelial dysfunction in insulin resistance. The American Journal of Cardiology, 92, 10-17.
Huijberts, M., Wolffenbuttel, B., Boudier, H., Crijns, F., Kruseman, A., Poitevin, P., & Levy, B. I. (1993). Aminoguanidine treatment increases elasticity and decreases fluid filtration of large arteries from diabetic rats. Journal of Clinical Investigation, 92, 1407.
Hung, C. H., Chan, S. H., Chu, P. M., Lin, H. C., & Tsai, K. L. (2016). Metformin regulates oxLDL-facilitated endothelial dysfunction by modulation of SIRT1 through repressing LOX -1-modulated oxidative signaling. Oncotarget, 7, 10773-10787.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Ignarro, L. J., Buga, G. M., Wood, K. S., Byrns, R. E., & Chaudhuri, G. (1987). Endothelium-derived relaxing factor produced and released from artery and vein is nitric oxide. Proceedings of the National Academy of Sciences, 84, 9265-9269.
Isoda, K., Young, J. L., Zirlik, A., MacFarlane, L. A., Tsuboi , N., Gerdes, N., Schönbeck, U., & Libby, P. (2006). Metformin Inhibits Proinflammatory Responses and Nuclear Factor-κB in Human Vascular Wall Cells. Arteriosclerosis, Thrombosis, and Vascular Biology, 26, 611-617.
Jensterle, M., Sebestjen, M., Janez, A., Prezelj, J., Kocjan, T., Keber, I., & Pfeifer, M. (2008). Improvement of endothelial function with metformin and rosiglitazone treatment in women with polycystic ovary syndrome. Eur J Endocrinol, 159, 399-406.
Ježek, P., & Hlavatá, L. (2005). Mitochondria in homeostasis of reactive oxygen species in cell, tissues, and organism. Int J Biochem Cell Biol, 37, 2478-2503.
Jiang, J., Gan, Z., Li, Y., Zhao, W., Li, H., Zheng, J.-P., & Ke, Y. (2017). REM sleep deprivation induces endothelial dysfunction and hypertension in middle-aged rats: Roles of the eNOS/NO/cGMP pathway and supplementation with L-arginine. PLoS One, 12, e0182746.
Jiang, Z. Y., Lin, Y.-W., Clemont, A., Feener, E. P., Hein, K. D., Igarashi, M., Yamauchi, T., White, M. F., & King, G. L. (1999). Characterization of selective resistance to insulin signaling in the vasculature of obese Zucker (fa/fa) rats. Journal of Clinical Investigation, 104, 447.
Just, A., Whitten, C. L., & Arendshorst, W. J. (2008). Reactive oxygen species participate in acute renal vasoconstrictor responses induced by ET A and ET B receptors. American Journal of Physiology-Renal Physiology, 294, F719-F728.
Kajbaf, F., De Broe, M. E., & Lalau, J. D. (2016). Therapeutic Concentrations of Metformin: A Systematic Review. Clin Pharmacokinet, 55, 439-459.
Kamato, D., Rostam, M. A., Piva, T. J., Babaahmadi Rezaei, H., Getachew, R., Thach, L., Bernard, R., Zheng, W., Little, P. J., & Osman, N. (2014). Transforming growth factor beta-mediated site-specific Smad linker region phosphorylation in vascular endothelial cells. J Pharm Pharmacol, 66, 1722-1733.
Karki, S., Farb, M. G., Ngo, D. T., Myers, S., Puri, V., Hamburg, N. M., Carmine, B., Hess, D. T., & Gokce, N. (2015). Forkhead box O-1 modulation improves endothelial insulin resistance in human obesity. Arteriosclerosis, Thrombosis, and Vascular Biology, ATVBAHA. 114.305139.
Karnewar, S., Neeli, P. K., Panuganti, D., Kotagiri, S., Mallappa, S., Jain, N., Jerald, M. K., & Kotamraju, S. (2018). Metformin regulates mitochondrial biogenesis and senescence through AMPK mediated H3K79 methylation: Relevance in age-associated vascular dysfunction. Biochim Biophys Acta, 1864, 1115-1128.
Kaya, M. G., Yildirim, S., Calapkorur, B., Akpek, M., Unluhizarci, K., & Kelestimur, F. (2015). Metformin improves endothelial function and carotid intima media thickness in patients with PCOS. Gynecol Endocrinol, 31, 401-405.
Ke, J., Liu, Y., Yang, J., Lu, R., Tian, Q., Hou, W., Wang, G., Wei, R., & Hong, T. (2017). Synergistic effects of metformin with liraglutide against endothelial dysfunction through GLP-1 receptor and PKA signalling pathway. Sci Rep, 7, 41085.
Kidokoro, K., Satoh, M., Channon, K. M., Yada, T., Sasaki, T., & Kashihara, N. (2013). Maintenance of endothelial guanosine triphosphate cyclohydrolase I ameliorates diabetic nephropathy. J Am Soc Nephrol, 24, 1139-1150.
Kim, J.-a., Montagnani, M., Koh, K. K., & Quon, M. J. (2006). Reciprocal relationships between insulin resistance and endothelial dysfunction. Circulation, 113, 1888-1904.
Kim, J., Lee, S., Park, J., & Yoo, Y. (2010). TNF-[alpha]-induced ROS production triggering apoptosis is directly linked to Romo1 and Bcl-XL. Cell death and differentiation, 17, 1420.
Kojima, H., Kunimoto, H., Inoue, T., & Nakajima, K. (2012). The STAT3-IGFBP5 axis is critical for IL-6/gp130-induced premature senescence in human fibroblasts. Cell Cycle, 11, 730-739.
Kruithof, E., Nicolosa, G., & Bachmann, F. (1987). Plasminogen activator inhibitor 1: development of a radioimmunoassay and observations on its plasma concentration during venous occlusion and after platelet aggregation. Blood, 70, 1645-1653.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Lai, W. K. C., & Kan, M. Y. (2015). Homocysteine-induced endothelial dysfunction. Annals of Nutrition and Metabolism, 67, 1-12.
Lassègue, B., San Martín, A., & Griendling, K. K. (2012). Biochemistry, physiology, and pathophysiology of NADPH oxidases in the cardiovascular system. Circulation Research, 110, 1364-1390.
Lee, C. H., & Yu, H. S. (2016). Role of mitochondria, ROS, and DNA damage in arsenic induced carcinogenesis. Front Biosci (Schol Ed), 8, 312-320.
Lee, S. (2017). Update on SGLT2 Inhibitors-New Data Released at the American Diabetes Association. Crit Pathw Cardiol, 16, 93-95.
Leopold, J. A., & Loscalzo, J. (2009). Oxidative risk for atherothrombotic cardiovascular disease. Free Radical Biology and Medicine, 47, 1673-1706.
Lesniewski, L. A., Durrant, J. R., Connell, M. L., Folian, B. J., Donato, A. J., & Seals, D. R. (2011). Salicylate treatment improves age-associated vascular endothelial dysfunction: potential role of nuclear factor κB and forkhead Box O phosphorylation. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences, 66, 409-418.
Li, L., Roumeliotis, N., Sawamura, T., & Renier, G. (2004). C-Reactive Protein Enhances LOX-1 Expression in Human Aortic Endothelial Cells. Circulation Research, 95, 877-883.
Li, Q., Atochin, D., Kashiwagi, S., Earle, J., Wang, A., Mandeville, E., Hayakawa, K., d’Uscio, L. V., Lo, E. H., & Katusic, Z. (2013). Deficient eNOS phosphorylation is a mechanism for diabetic vascular dysfunction contributing to increased stroke size. Stroke, 44, 3183-3188.
Li, X., Kover, K. L., Heruth, D. P., Watkins, D. J., Moore, W. V., Jackson, K., Zang, M., Clements, M. A., & Yan, Y. (2015). New Insight Into Metformin Action: Regulation of ChREBP and FOXO1 Activities in Endothelial Cells. Mol Endocrinol, 29, 1184-1194.
Libby, P. (2006). Inflammation and cardiovascular disease mechanisms. Am J Clin Nutr, 83, 456S-460S.
Libby, P., Aikawa, M., & Jain, M. (2006). Vascular endothelium and atherosclerosis. In The Vascular Endothelium II (pp. 285-306): Springer.
Libby, P., Ridker, P. M., & Hansson, G. K. (2011). Progress and challenges in translating the biology of atherosclerosis. Nature, 473, 317-325.
Libby, P., Ridker, P. M., & Maseri, A. (2002). Inflammation and atherosclerosis. Circulation, 105, 1135-1143.
Little, P. J., Chait, A., & Bobik, A. (2011). Cellular and cytokine-based inflammatory processes as novel therapeutic targets for the prevention and treatment of atherosclerosis. Pharmacol Ther, 131, 255-268.
Little, P. J., Osman, N., de Dios, S. T., Cemerlang, N., Ballinger, M., & Nigro, J. (2007). Anti-proliferative activity of oral anti hyperglycemic agents on human vascular smooth muscle cells: thiazolidinediones (glitazones) have enhanced activity under high glucose conditions. Cardiovasc Diabetol, 6, 33.
Little, P. J., Osman, N., & O'Brien, K. D. (2008). Hyperelongated biglycan: the surreptitious initiator of atherosclerosis. Current Opinion in Lipidology, 19, 448-454.
Luk, T.-H., Dai, Y.-L., Siu, C.-W., Yiu, K.-H., Li, S.-W., Fong, B., Wong, W.-K., Tam, S., & Tse, H.-F. (2012). Association of lower habitual physical activity level with mitochondrial and endothelial dysfunction in patients with stable coronary artery disease. Circulation Journal, 76, 2572-2578.
Luppi, P., Cifarelli, V., Tse, H., Piganelli, J., & Trucco, M. (2008). Human C-peptide antagonises high glucose-induced endothelial dysfunction through the nuclear factor-κB pathway. Diabetologia, 51, 1534.
Lv, Y. C., Tang, Y. Y., Zhang, P., Wan, W., Yao, F., He, P. P., Xie, W., Mo, Z. C., Shi, J. F., Wu, J. F., Peng, J., Liu, D., Cayabyab, F. S., Zheng, X. L., Tang, X. Y., Ouyang, X. P., & Tang, C. K. (2016). Histone Methyltransferase Enhancer of Zeste Homolog 2-Mediated ABCA1 Promoter DNA Methylation Contributes to the Progression of Atherosclerosis. PLoS One, 11, e0157265.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Madamanchi, N. R., Vendrov, A., & Runge, M. S. (2005). Oxidative stress and vascular disease. Arteriosclerosis, Thrombosis, and Vascular Biology, 25, 29-38.
Maeno, Y., Li, Q., Park, K., Rask-Madsen, C., Gao, B., Matsumoto, M., Liu, Y., Wu, I.-H., White, M. F., & Feener, E. P. (2012). Inhibition of insulin signaling in endothelial cells by protein kinase C-induced phosphorylation of p85 subunit of phosphatidylinositol 3-kinase (PI3K). Journal of Biological Chemistry, 287, 4518-4530.
Mamputu, J. C., Wiernsperger, N., & Renier, G. (2003). Metformin inhibits monocyte adhesion to endothelial cells and foam cell formation. The British Journal of Diabetes & Vascular Disease, 3, 302-310.
Marfella, R., Barbieri, M., Grella, R., Rizzo, M. R., Nicoletti, G. F., & Paolisso, G. (2010). Effects of vildagliptin twice daily vs. sitagliptin once daily on 24-hour acute glucose fluctuations. J Diabetes Complications, 24, 79-83.
Mather, K. J., Verma, S., & Anderson, T. J. (2001). Improved endothelial function with metformin in type 2 diabetes mellitus. J Am Coll Cardiol, 37, 1344-1350.
Matsui-Hirai, H., Hayashi, T., Yamamoto, S., Ina, K., Maeda, M., Kotani, H., Iguchi, A., Ignarro, L. J., & Hattori, Y. (2011). Dose-dependent modulatory effects of insulin on glucose-induced endothelial senescence in vitro and in vivo: a relationship between telomeres and nitric oxide. Journal of Pharmacology and Experimental Therapeutics, 337, 591-599.
Messner, B., & Bernhard, D. (2014). Smoking and cardiovascular disease. Arteriosclerosis, Thrombosis, and Vascular Biology, 34, 509-515.
Michel, T., & Vanhoutte, P. M. (2010). Cellular signaling and NO production. Pflügers archiv-European journal of physiology, 459, 807-816.
Michiels, C. F., Apers, S., De Meyer, G. R. Y., & Martinet, W. (2016). Metformin Attenuates Expression of Endothelial Cell Adhesion Molecules and Formation of Atherosclerotic Plaques via Autophagy Induction Ann Clin Exp Metabol, 1, 1001.
Minami, T., & Aird, W. C. (2005). Endothelial cell gene regulation. Trends in cardiovascular medicine, 15, 174. e171-174. e124.
Minamino, T., Miyauchi, H., Yoshida, T., Ishida, Y., Yoshida, H., & Komuro, I. (2002). Endothelial cell senescence in human atherosclerosis. Circulation, 105, 1541-1544.
Moncada, S., Gryglewski, R., Bunting, S., & Vane, J. (1976). An enzyme isolated from arteries transforms prostaglandin endoperoxides to an unstable substance that inhibits platelet aggregation. Nature, 263, 663-665.
Montagnani, M., Golovchenko, I., Kim, I., Koh, G. Y., Goalstone, M. L., Mundhekar, A. N., Johansen, M., Kucik, D. F., Quon, M. J., & Draznin, B. (2002). Inhibition of phosphatidylinositol 3-kinase enhances mitogenic actions of insulin in endothelial cells. Journal of biological chemistry, 277, 1794-1799.
Montezano, A. C., & Touyz, R. M. (2012). Reactive oxygen species and endothelial function–role of nitric oxide synthase uncoupling and Nox family nicotinamide adenine dinucleotide phosphate oxidases. Basic & clinical pharmacology & toxicology, 110, 87-94.
Muniyappa, R., & Sowers, J. R. (2013). Role of insulin resistance in endothelial dysfunction. Reviews in Endocrine and Metabolic Disorders, 14, 5-12.
Naka, K. K., Kalantaridou, S. N., Kravariti, M., Bechlioulis, A., Kazakos, N., Calis, K. A., Makrigiannakis, A., Katsouras, C. S., Chrousos, G. P., Tsatsoulis, A., & Michalis, L. K. (2011). Effect of the insulin sensitizers metformin and pioglitazone on endothelial function in young women with polycystic ovary syndrome: a prospective randomized study. Fertil Steril, 95, 203-209.
Nemoto, S., Kobayashi, T., Taguchi, K., Matsumoto, T., & Kamata, K. (2011). Losartan improves aortic endothelium-dependent relaxation via proline-rich tyrosine kinase 2/Src/Akt pathway in type 2 diabetic Goto-Kakizaki rats. American Journal of Physiology-Heart and Circulatory Physiology, 301, H2383-H2394.
Nigro, J., Osman, N., Dart, A. M., & Little, P. J. (2006). Insulin Resistance and Atherosclerosis. Endocr Rev, 27, 242-259.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Nishida, K., Harrison, D., Navas, J., Fisher, A., Dockery, S., Uematsu, M., Nerem, R., Alexander, R., & Murphy, T. (1992). Molecular cloning and characterization of the constitutive bovine aortic endothelial cell nitric oxide synthase. Journal of Clinical Investigation, 90, 2092.
Ota, H., Eto, M., Kano, M. R., Ogawa, S., Iijima, K., Akishita, M., & Ouchi, Y. (2008). Cilostazol inhibits oxidative stress–induced premature senescence via upregulation of Sirt1 in human endothelial cells. Arteriosclerosis, Thrombosis, and Vascular Biology, 28, 1634-1639.
Ouchi, N., Parker, J. L., Lugus, J. J., & Walsh, K. (2011). Adipokines in inflammation and metabolic disease. Nature reviews. Immunology, 11, 85.
Pahakis, M. Y., Kosky, J. R., Dull, R. O., & Tarbell, J. M. (2007). The role of endothelial glycocalyx components in mechanotransduction of fluid shear stress. Biochemical and Biophysical Research Communications, 355, 228-233.
Palmer, R. M., Ashton, D., & Moncada, S. (1988). Vascular endothelial cells synthesize nitric oxide from L-arginine. Nature, 333, 664-666.
Palmer, R. M., Ferrige, A., & Moncada, S. (1987). Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature, 327, 524-526.
Paneni, F., Beckman, J. A., Creager, M. A., & Cosentino, F. (2013). Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. European Heart Journal, 34, 2436-2443.
Peng, N., Meng, N., Wang, S., Zhao, F., Zhao, J., Su, L., Zhang, S., Zhang, Y., Zhao, B., & Miao, J. (2014). An activator of mTOR inhibits oxLDL-induced autophagy and apoptosis in vascular endothelial cells and restricts atherosclerosis in apolipoprotein E-/-mice. Scientific reports, 4.
Petrie, J. R., Chaturvedi, N., Ford, I., Brouwers, M. C. G. J., Greenlaw, N., Tillin, T., Hramiak, I., Hughes, A. D., Jenkins, A. J., Klein, B. E. K., Klein, R., Ooi, T. C., Rossing, P., Stehouwer, C. D. A., Sattar, N., Colhoun, H. M., Nickerson, H., Lou, O., Dutta, S., Haw, J., Anderson, C., Kean, S., Thomson, E., Gillespie, L., Gibb, J., Greenlaw, N., Keech, A., Jenkins, A., March, K., Williams, S., Coady, E., Bots, M., Dreyer, J., Jan, T., Sheffy, K., Lusky, R., Peleg, S., Shore, A., Carty, D., Donnan, P., Witham, M., Adler, A., Lonn, E., Rauchhaus, P., Lindsay, R., Brouwers, M., Van-Melckebeke, J., Gillespie, L., Hamill, T., Cuthbertson, L., Murray, A., Jolly, L., Miller, E., Hair, J., Bell, A., Carmichael, S., Douglas, E., Surtees, P., Dinnett, E., Allan, J., Watson, C., McLaughlin, M., Brindley, G., Smillie, E., Motherwell, D., MacDonald, S., Ellis, P., Stuart, D., Travers, M., Brearley, S., Greig, L., Colman, P., Nankervis, A., Forulanos, S., West, D., Vaughan, S., Bjorasen, M., Donlan, J., Vrazas, J., O'Neal, D., Horsburgh, J., Pater, H., Kent, S., Twigg, S., Fulcher, G., Denner, R., Piotrowicz, A., Januszewski, A., Coy, A., Paul, T., McDonald, C., Tereschyn, S., Schmidt, N., Weingert, M., Heard, H., Burke, S., Ooi, T. C., Lochnan, H., Sorisky, A., Keely, E., Malcolm, J., Maranger, J., Favreau, C., Petherick, S., Boles, K., Rossing, P., Hansen, T. W., Lund, S., Hemmingsen, B., Thorogood, N., Green, K., Robinson, T., Abouglilia, K., Nayman, D., Miller, C., Warren, R., Aizawa, K., Balasubramani, M., Toth, S., Harvey, K., Birch, G., Atkin, S., Sathyapalan, T., James, A., Javed, Z., Wilding, J., Martin, B., Birch, S., Wilcox, A., Watson, N., Oliver, N., Jugnee, N., Rutter, M., Turgut, T., Shaju, A., Yau, S., Subin, S., Walker, M., Wake, D., Miller, C., Millward, A., Chong, P., Hibbert, M., George, J., Schaper, N., Pinxt, J., op het Roodt, J., Phillips, S., Murray, L., Sleigh, L., Collier, A., Sit, L. E., All an, K., Cook, J., Campbell, K., Hodge, L., Leese, G., Reekie, G., Jaap, A., Sudworth, A., White, A., McKnight, J., Steven, L., McKay, G., Llano, A., Currie, G., Lennon, E., Johnstone, J., & Shields, K. Cardiovascular and metabolic effects of metformin in patients with type 1 diabetes (REMOVAL): a double-blind, randomised, placebo-controlled trial. The Lancet Diabetes & Endocrinology, 5, 597-609.
Piconi, L., Quagliaro, L., Da Ros, R., Assaloni, R., Giugliano, D., Esposito, K., Szabo, C., & Ceriello, A.
(2004). Intermittent high glucose enhances ICAM‐ 1, VCAM‐ 1, E‐ selectin and
interleukin‐6 expression in human umbilical endothelial cells in culture: the role of poly
(ADP‐ribose) polymerase. Journal of Thrombosis and Haemostasis, 2, 1453-1459.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Piga, R., Naito, Y., Kokura, S., Handa, O., & Yoshikawa, T. (2007). Short-term high glucose exposure induces monocyte-endothelial cells adhesion and transmigration by increasing VCAM-1 and MCP-1 expression in human aortic endothelial cells. Atherosclerosis, 193, 328-334.
Pitocco, D., Zaccardi, F., Tarzia, P., Milo, M., Scavone, G., Rizzo, P., Pagliaccia, F., Nerla, R., Di Franco, A., Manto, A., Rocca, B., Lanza, G. A., Crea, F., & Ghirlanda, G. (2013). Metformin improves endothelial function in type 1 diabetic subjects: a pilot, placebo-controlled randomized study. Diabetes Obes Metab, 15, 427-431.
Potenza, M. A., Gagliardi, S., Nacci, C., Carratu, M. R., & Montagnani, M. (2009). Endothelial dysfunction in diabetes: from mechanisms to therapeutic targets. Current medicinal chemistry, 16, 94-112.
Pournaghi, P., Sadrkhanlou, R. A., Hasanzadeh, S., & Foroughi, A. (2012). An investigation on body weights, blood glucose levels and pituitary-gonadal axis hormones in diabetic and metformin-treated diabetic female rats. Vet Res Forum, 3, 79-84.
Quehenberger, P., Bierhaus, A., Fasching, P., Muellner, C., Klevesath, M., Hong, M., Stier, G., Sattler, M., Schleicher, E., & Speiser, W. (2000). Endothelin 1 transcription is controlled by nuclear factor-kappaB in AGE-stimulated cultured endothelial cells. Diabetes, 49, 1561-1570.
Rapoport, R. M., & Murad, F. (1983). Agonist-induced endothelium-dependent relaxation in rat thoracic aorta may be mediated through cGMP. Circulation Research, 52, 352-357.
Rask-Madsen, C., Li, Q., Freund, B., Feather, D., Abramov, R., Wu, I.-H., Chen, K., Yamamoto-Hiraoka, J., Goldenbogen, J., & Sotiropoulos, K. B. (2010). Loss of insulin signaling in vascular endothelial cells accelerates atherosclerosis in apolipoprotein E null mice. Cell Metab, 11, 379-389.
Ray, R., & Shah, A. M. (2005). NADPH oxidase and endothelial cell function. Clinical Science, 109, 217-226.
Roberge, S., Roussel, J., Andersson, D. C., Meli, A. C., Vidal, B., Blandel, F., Lanner, J. T., Le Guennec, J.-Y., Katz, A., & Westerblad, H. (2014). TNF-α-mediated caspase-8 activation induces ROS production and TRPM2 activation in adult ventricular myocytes. Cardiovascular Research, 103, 90-99.
Rodier, F., & Campisi, J. (2011). Four faces of cellular senescence. J Cell Biol, jcb. 201009094. Rogers, S. C., Zhang, X., Azhar, G., Luo, S., & Wei, J. Y. (2013). Exposure to high or low glucose levels
accelerates the appearance of markers of endothelial cell senescence and induces dysregulation of nitric oxide synthase. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences, 68, 1469-1481.
Ross, R. (1986). The pathogenesis of atherosclerosis. N Engl J Med, 314, 488-500. Rueckschloss, U., Duerrschmidt, N., & Morawietz, H. (2003). NADPH oxidase in endothelial cells:
impact on atherosclerosis. Antioxidants and Redox Signaling, 5, 171-180. Salpeter, S. R., Greyber, E., Pasternak, G. A., & Salpeter, E. E. (2003). Risk of fatal and nonfatal lactic
acidosis with metformin use in type 2 diabetes mellitus: systematic review and meta-analysis. Arch Intern Med, 163, 2594-2602.
Samuel, S. M., Ghosh, S., Majeed, Y., Arunachalam, G., Emara, M. M., Ding, H., & Triggle, C. R. (2017). Metformin represses glucose starvation induced autophagic response in microvascular endothelial cells and promotes cell death. Biochem Pharmacol, 132, 118-132.
Santhanam, L., Lim, H. K., Lim, H. K., Miriel, V., Brown, T., Patel, M., Balanson, S., Ryoo, S., Anderson, M., & Irani, K. (2007). Inducible NO synthase–dependent S-nitrosylation and activation of arginase1 contribute to age-related endothelial dysfunction. Circulation Research, 101, 692-702.
Sasser, J. M., Cunningham, M. W., & Baylis, C. (2014). Serelaxin reduces oxidative stress and asymmetric dimethylarginine in angiotensin II-induced hypertension. American Journal of Physiology-Renal Physiology, 307, F1355-F1362.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Sasson, S., Gorowits, N., Joost, H. G., King, G. L., Cerasi, E., & Kaiser, N. (1996). Regulation by metformin of the hexose transport system in vascular endothelial and smooth muscle cells. Br J Pharmacol, 117, 1318-1324.
Schmidt, A. M., Du Yan, S., Wautier, J.-L., & Stern, D. (1999). Activation of receptor for advanced glycation end products. Circulation Research, 84, 489-497.
Sena, C., Nunes, E., Louro, T., Proença, T., Fernandes, R., Boarder, M., & Seiça, R. (2008). Effects of α
‐lipoic acid on endothelial function in aged diabetic and high‐fat fed rats. British Journal of Pharmacology, 153, 894-906.
Sena, C. M., Matafome, P., Crisóstomo, J., Rodrigues, L., Fernandes, R., Pereira, P., & Seiça, R. M. (2012). Methylglyoxal promotes oxidative stress and endothelial dysfunction. Pharmacological Research, 65, 497-506.
Sena, C. M., Matafome, P., Louro, T., Nunes, E., Fernandes, R., & Seica, R. M. (2011). Metformin restores endothelial function in aorta of diabetic rats. Br J Pharmacol, 163, 424-437.
Sena, C. M., Pereira, A. M., & Seiça, R. (2013). Endothelial dysfunction—a major mediator of diabetic vascular disease. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease, 1832, 2216-2231.
Sena, C. M., Pereira, A. M., & Seiça, R. (2013). Endothelial dysfunction — A major mediator of diabetic vascular disease. Biochimica et Biophysica Acta (BBA) - Molecular Basis of Disease, 1832, 2216-2231.
Soccio, M., Toniato, E., Evangelista, V., Carluccio, M., & De Caterina, R. (2005). Oxidative stress and cardiovascular risk: the role of vascular NAD (P) H oxidase and its genetic variants. European Journal of Clinical Investigation, 35, 305-314.
Soldatos, G., Cooper, M. E., & Jandeleit-Dahm, K. A. (2005). Advanced-glycation end products in insulin-resistant states. Current hypertension reports, 7, 96-102.
Speer, T., Owala, F. O., Holy, E. W., Zewinger, S., Frenzel, F. L., Stähli, B. E., Razavi, M., Triem, S., Cvija, H., & Rohrer, L. (2014). Carbamylated low-density lipoprotein induces endothelial dysfunction. European Heart Journal, 35, 3021-3032.
Stamler, J. S., Simon, D. I., Osborne, J. A., Mullins, M. E., Jaraki, O., Michel, T., Singel, D. J., & Loscalzo, J. (1992). S-nitrosylation of proteins with nitric oxide: synthesis and characterization of biologically active compounds. Proceedings of the National Academy of Sciences, 89, 444-448.
Stumvoll, M., Nurjhan, N., Perriello, G., Dailey, G., & Gerich, J. E. (1995). Metabolic effects of metformin in non-insulin-dependent diabetes mellitus. N Engl J Med, 333, 550-554.
Tabas, I., Williams, K. J., & Boren, J. (2007). Subendothelial lipoprotein retention as the initiating process in atherosclerosis: update and therapeutic implications. Circulation, 116, 1832-1844.
Tabit, C. E., Shenouda, S. M., Holbrook, M., Fetterman, J. L., Kiani, S., Frame, A. A., Kluge, M. A., Held, A., Dohadwala, M., & Gokce, N. (2012). Protein kinase-C beta contributes to impaired endothelial insulin signaling in humans with diabetes mellitus. Circulation, CIRCULATIONAHA. 112.127514.
Takata, F., Dohgu, S., Matsumoto, J., Machida, T., Kaneshima, S., Matsuo, M., Sakaguchi, S., Takeshige, Y., Yamauchi, A., & Kataoka, Y. (2013). Metformin induces up-regulation of blood-brain barrier functions by activating AMP-activated protein kinase in rat brain microvascular endothelial cells. Biochem Biophys Res Commun, 433, 586-590.
Tang, G., Guo, J., Zhu, Y., Huang, Z., Liu, T., Cai, J., Yu, L., & Wang, Z. (2018). Metformin inhibits ovarian cancer via decreasing H3K27 trimethylation. Int J Oncol, 52, 1899-1911.
Testa, R., & Ceriello, A. (2007). Pathogenetic loop between diabetes and cell senescence. Diabetes Care, 30, 2974-2975.
Triggle, C. R., & Ding, H. (2017). Metformin is not just an antihyperglycaemic drug but also has protective effects on the vascular endothelium. Acta Physiol (Oxf), 219, 138-151.
Turrens, J. F. (2003). Mitochondrial formation of reactive oxygen species. The Journal of physiology, 552, 335-344.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
UK Prospective Diabetes Study (UKPDS) Group. (1998). Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet, 352, 854-865.
Ungvari, Z., Orosz, Z., Labinskyy, N., Rivera, A., Xiangmin, Z., Smith, K., & Csiszar, A. (2007). Increased mitochondrial H 2 O 2 production promotes endothelial NF-κB activation in aged rat arteries. American Journal of Physiology-Heart and Circulatory Physiology, 293, H37-H47.
Valente, A. J., Irimpen, A. M., Siebenlist, U., & Chandrasekar, B. (2014). OxLDL induces endothelial dysfunction and death via TRAF3IP2: inhibition by HDL3 and AMPK activators. Free Radic Biol Med, 70, 117-128.
Valenzuela, M. T., Núñez, M. I., Villalobos, M., Siles, E., McMillan, T. J., Pedraza, V., & Ruiz de Almodóvar, J. M. (1997). A comparison of p53 and p16 expression in human tumor cells treated with hyperthermia or ionizing radiation. International journal of cancer, 72, 307-312.
Van den Oever, I. A., Raterman, H. G., Nurmohamed, M. T., & Simsek, S. (2010). Endothelial dysfunction, inflammation, and apoptosis in diabetes mellitus. Mediators of inflammation, 2010.
Vasto, S., Candore, G., Balistreri, C. R., Caruso, M., Colonna-Romano, G., Grimaldi, M. P., Listi, F., Nuzzo, D., Lio, D., & Caruso, C. (2007). Inflammatory networks in ageing, age-related diseases and longevity. Mechanisms of ageing and development, 128, 83-91.
Versari, D., Daghini, E., Virdis, A., Ghiadoni, L., & Taddei, S. (2009). Endothelial dysfunction as a target for prevention of cardiovascular disease. Diabetes Care, 32, S314-S321.
Vestweber, D. (2015). How leukocytes cross the vascular endothelium. Nature reviews. Immunology, 15, 692.
Vitale, C., Mercuro, G., Cornoldi, A., Fini, M., Volterrani, M., & Rosano, G. M. (2005). Metformin improves endothelial function in patients with metabolic syndrome. J Intern Med, 258, 250-256.
Wang, J. C., & Bennett, M. (2012). Aging and atherosclerosis. Circulation Research, 111, 245-259. Wang, S., Xu, J., Song, P., Viollet, B., & Zou, M. H. (2009). In vivo activation of AMP-activated protein
kinase attenuates diabetes-enhanced degradation of GTP cyclohydrolase I. Diabetes, 58, 1893-1901.
Wautier, M.-P., Chappey, O., Corda, S., Stern, D. M., Schmidt, A. M., & Wautier, J.-L. (2001). Activation of NADPH oxidase by AGE links oxidant stress to altered gene expression via RAGE. American Journal of Physiology-Endocrinology And Metabolism, 280, E685-E694.
Way, K., Katai, N., & King, G. (2001). Protein kinase C and the development of diabetic vascular complications. Diabetic Medicine, 18, 945-959.
Weikel, K. A., Cacicedo, J. M., Ruderman, N. B., & Ido, Y. (2015). Glucose and palmitate uncouple AMPK from autophagy in human aortic endothelial cells. Am J Physiol Cell Physiol, 308, C249-263.
White, S. J., Hayes, E. M., Lehoux, S., Jeremy, J. Y., Horrevoets, A. J., & Newby, A. C. (2011). Characterization of the differential response of endothelial cells exposed to normal and elevated laminar shear stress. Journal of Cellular Physiology, 226, 2841-2848.
Widlansky, M. E., Gokce, N., Keaney, J. F., & Vita, J. A. (2003). The clinical implications of endothelial dysfunction. Journal of the American College of Cardiology, 42, 1149-1160.
Wilcock, C., & Bailey, C. J. (1994). Accumulation of metformin by tissues of the normal and diabetic mouse. Xenobiotica, 24, 49-57.
Williams, B., Gallacher, B., Patel, H., & Orme, C. (1997). Glucose-induced protein kinase C activation regulates vascular permeability factor mRNA expression and peptide production by human vascular smooth muscle cells in vitro. Diabetes, 46, 1497-1503.
Writing Group, M., Mozaffarian, D., Benjamin, E. J., Go, A. S., Arnett, D. K., Blaha, M. J., Cushman, M., Das, S. R., de Ferranti, S., Despres, J. P., Fullerton, H. J., Howard, V. J., Huffman, M. D., Isasi, C. R., Jimenez, M. C., Judd, S. E., Kissela, B. M., Lichtman, J. H., Lisabeth, L. D., Liu, S., Mackey, R. H., Magid, D. J., McGuire, D. K., Mohler, E. R., 3rd, Moy, C. S., Muntner, P., Mussolino, M.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
E., Nasir, K., Neumar, R. W., Nichol, G., Palaniappan, L., Pandey, D. K., Reeves, M. J., Rodriguez, C. J., Rosamond, W., Sorlie, P. D., Stein, J., Towfighi, A., Turan, T. N., Virani, S. S., Woo, D., Yeh, R. W., Turner, M. B., American Heart Association Statistics, C., & Stroke Statistics, S. (2016). Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation, 133, e38-60.
Wu, Y., Ding, Y., Tanaka, Y., & Zhang, W. (2014). Risk Factors Contributing to Type 2 Diabetes and Recent Advances in the Treatment and Prevention. International Journal of Medical Sciences, 11, 1185-1200.
Xiaoling, Y., Li, Z., ShuQiang, L., Shengchao, M., Anning, Y., Ning, D., Nan, L., Yuexia, J., Xiaoming, Y., Guizhong, L., & Yideng, J. (2016). Hyperhomocysteinemia in ApoE-/- Mice Leads to Overexpression of Enhancer of Zeste Homolog 2 via miR-92a Regulation. PLoS One, 11, e0167744.
Xie, Z., Dong, Y., Scholz, R., Neumann, D., & Zou, M. H. (2008). Phosphorylation of LKB1 at serine 428 by protein kinase C-zeta is required for metformin-enhanced activation of the AMP-activated protein kinase in endothelial cells. Circulation, 117, 952-962.
Xu, S., Liu, Z., & Liu, P. (2014). Targeting hydrogen sulfide as a promising therapeutic strategy for atherosclerosis. Int J Cardiol, 172, 313-317.
Xu, S., Ogura, S., Chen, J., Little, P. J., Moss, J., & Liu, P. (2013). LOX-1 in atherosclerosis: biological functions and pharmacological modifiers. Cell Mol Life Sci, 70, 2859-2872.
Xu, S., Xu, Y., Yin, M., Zhang, S., Liu, P., Koroleva, M., Si, S., Little, P. J., Pelisek, J., & Jin, Z. G. (2018). Flow-dependent epigenetic regulation of IGFBP5 expression by H3K27me3 contributes to endothelial anti-inflammatory effects. Theranostics, 8, 3007-3021.
Yanagisawa, M., Kurihara, H., Kimura, S., Tomobe, Y., Kobayashi, M., Mitsui, Y., Yazaki, Y., Goto, K., & Masaki, T. (1988). A novel potent vasoconstrictor peptide produced by vascular endothelial cells. Nature, 332, 411-415.
Yang, S. N., Burch, M. L., Tannock, L. R., Evanko, S., Osman, N., & Little, P. J. (2010). Transforming growth factor-beta regulation of proteoglycan synthesis in vascular smooth muscle: contribution to lipid binding and accelerated atherosclerosis in diabetes. J Diabetes, 2, 233-242.
Yang, Y., Dong, R., Hu, D., Chen, Z., Fu, M., Wang, D. W., Xu, X., & Tu, L. (2017). Liver Kinase B1/AMP-Activated Protein Kinase Pathway Activation Attenuated the Progression of Endotoxemia in the Diabetic Mice. Cell Physiol Biochem, 42, 761-779.
Yang, Z., Mo, X., Gong, Q., Pan, Q., Yang, X., Cai, W., Li, C., Ma, J.-x., He, Y., & Gao, G. (2008). Critical effect of VEGF in the process of endothelial cell apoptosis induced by high glucose. Apoptosis, 13, 1331-1343.
Yokoi, T., Fukuo, K., Yasuda, O., Hotta, M., Miyazaki, J., Takemura, Y., Kawamoto, H., Ichijo, H., & Ogihara, T. (2006). Apoptosis signal-regulating kinase 1 mediates cellular senescence induced by high glucose in endothelial cells. Diabetes, 55, 1660-1665.
Yu, J. W., Deng, Y. P., Han, X., Ren, G. F., Cai, J., & Jiang, G. J. (2016). Metformin improves the angiogenic functions of endothelial progenitor cells via activating AMPK/eNOS pathway in diabetic mice. Cardiovasc Diabetol, 15, 88.
Yu, T., Sheu, S.-S., Robotham, J. L., & Yoon, Y. (2008). Mitochondrial fission mediates high glucose-induced cell death through elevated production of reactive oxygen species. Cardiovascular Research, 79, 341-351.
Zhang, E., Guo, Q., Gao, H., Xu, R., Teng, S., & Wu, Y. (2015). Metformin and Resveratrol Inhibited High Glucose-Induced Metabolic Memory of Endothelial Senescence through SIRT1/p300/p53/p21 Pathway. PLoS One, 10, e0143814.
Zhang, J., Cao, M., Yang, W., Sun, F., Xu, C., Yin, L., & Pu, Y. (2016). Inhibition of Glucose-6-Phosphate Dehydrogenase Could Enhance 1,4-Benzoquinone-Induced Oxidative Damage in K562 Cells. Oxidative Medicine and Cellular Longevity, 2016, 3912515.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Zhang, Y., Janssens, S. P., Wingler, K., Schmidt, H. H., & Moens, A. L. (2011). Modulating endothelial nitric oxide synthase: a new cardiovascular therapeutic strategy. American Journal of Physiology-Heart and Circulatory Physiology, 301, H634-H646.
Zhao, L. P., Sheng, X. Y., Zhou, S., Yang, T., Ma, L. Y., Zhou, Y., & Cui, Y. M. (2015). Metformin versus insulin for gestational diabetes mellitus: A meta-analysis. British Journal of Clinical Pharmacology, 80, 1224-1234.
ACCEPTED MANUSCRIPT