Embed Size (px)
Citation preview

Clin Biochem, Vol. 20, pp. 329-332, 1987 0009-9120/87 $3.00 + .00 Printed in Canada. All rights reserved. Copyright © 1987 The Canadian Society o£ Clinical Chemists.
Enzymatic Determination Index of
of Red Cell Hemolysis
Creatine as an
H. CRAMER, H. DAUWALDER, H. MEIER, and J. P. COLOMBO
Departments of Clinical Chemistry and Hematology, Inselspital, University of Berne, Berne, Switzerland
An enzymatic assay for creatine, depending on the creatine kinase reaction, has been modified for the determination of creatine in packed erythrocytes, using a centrifugal analyzer (COBAS BIO). The method is precise, sensitive and shows excellent accuracy in recovery experiments when compared to the diacetyl-e-naphthol method. The enzymatic red cell creatine correlates with the erythrooyte survival time determined with the radioactive chromium method. It can be used as a rapidly available parameter for the quantification of he- molytic processes.
S P E C I M E N
Whole blood specimens were collected in tubes con- taining heparin or EDTA (1 mg/ml). Packed erythro- cytes can be stored at 4°C for 10 d (5) but were mostly analyzed within 2 d.
R E A G E N T S
KEY WORDS: creatine; hemolytic anemia.
T he erythropoietic activity, the mean age of red cell population, and the intensity of the hemolytic pro-
cess are usual ly evaluated by the ~tCr-erythrocyte sur- vival time. It has been shown that creatine in eryth- rocytes is chiefly related to the mean age of the red cell population but it is not conditioned by the degree of anemia (1). Creat ine has, therefore, been used to eval- uate the above-mentioned conditions (2, 3).
Red cell creatine can be measured with the diacetyl-(~- naphthol reaction by a continuous flow method (4). The specificity of this method was improved by Li et al. by eliminating the glutathione interference (5). For our studies, we adapted a specific enzymatic method to mea- sure red cell creatine using the centrifugal analyzer COBAS BIO ®. The method is based on the following reaction principles (6, 7):
Creatine + ATP C K creatine phosphate + ADP
ADP + PEP PK) ATP + Pyruvate
Pyruvate + NADH + H ÷ L D H Lactate + NAD ÷
We compared this method with the diacetyl-~-naphthol method, which is still widely used.
Mater ia l a n d m e t h o d s
A P P A R A T U S
Cobas Bio (Roche Ltd., Basel, Switzerland), Hamil ton Dilutor.
Correspondence: J. P. Colombo, M.D., Department of Clini- cal Chemistry, Inselspital, 3010 Berne, Switzerland.
Manuscript received February 9, 1987; revised April 22, 1987; accepted May 4, 1987.
Abbreviations: CK, creatine kinase (ATP: creatine N-phos- photransferase, EC 2.7.3.2); PEP, phosphoenolpyruvate; PK, pyruvate kinase (ATP: pyruvate 2-0-phosphotransferase, EC 2.7.1.40); LDH, lactate dehydrogenase (L-lactate: NAD ~ oxidoreductase, EC 1.1.1.27).
Deproteinization: Ba(OH)2"8H20 solution 0.15 mol/L and ZnSO4.7H~O solution 0.15 mol/L were used as de- scribed (5).
E N Z Y M A T I C ASSAY
Glycine-phosphate buffer
Solution of 350 mmol/L glycine p.a., 360mmol /L K2HPO4"3H20 p.a., pH 8.5.
ATP-PEP-MgS04 solution
ATP 198 mmol/L (adenosine-5' t r iphosphate diso- dium salt '3H20) pH 7.5; PEP 66mmol /L (phospho- enolpyruvate t r icyclohexylammonium salt), pH 7.5 (Boehringer Mannheim AG, Rotkreuz, Switzerland). Aliquots were stored frozen. MgSO4 300 mmol /L was stored at 4°C. Equal parts of each solution were mixed before use.
NADH
Nicotinamide-adenine dinucleotide reduced, diso- dium salt 12 mmol/L (Boehringer-Mannheim) in water, prepared daily.
Auxiliary enzymes
PK, pyruvate kinase 200 U/mg (10 mg/ml) and LDH, lactate dehydrogenase 5 5 0 U / m g (10mg/ml) from rabbit muscle (Boehringer Mannheim nr 109045 and 1272307). Suspensions were mixed 3 : 2 before use.
Working solution
Nine millilitres of glycine-phosphate buffer were added to 0.4 ml ATP-PEP-MgSO4 solution, 0.2 ml PK- LDH suspension, and 0.4 ml NADH2 solution.
CLINICAL BIOCHEMISTRY, VOLUME 20, OCTOBER 1987 329

CRAMER, DAUWALDER, MEIER, AND COLOMBO
TABLE 1 Hematological Findings in Fourteen Patients with Hemolytic Anemia
Reference 2 + SD Range interval
Red cell count (1012/L) 3.3 ± 0.79 2.8-4.6 4.3-5.9 ~ Reticulocytes (%) 7.0 ± 4.9 1.8-17 0.5-2.0 a Hemoglobin (g/L) 108 ± 25 60-140 135-168 a Haptoglobin (g/L) 0.17 ± 0.24 0.1-0.9 0.3-2.0 b Red cell survival time 33 ± 12 17-59 90-130 b
Ref. (10). b Ref. (8).
Starting reagent
CK, creatine kinase from rabbi t muscle, 380 U / m g (lyophilized) 5 rag/10 ml.
Concentration in the assay mixture (mmol/L)
Glycine 145, Phosphate 109, ATP 0.2, PEP 0.40, MgSO4 1.8, NADH 0,22; LDH 18.4 kU/L, PK 11.0 kU/L , CK 25 kU/L.
CONTROL SOLUTIONS
Several dilutions of aqueous stock solutions of 6104 mmol /L creatine monohydra te p.a. (Merck AG, Zfirich, Switzerland) were used as controls. Aliquots were kept frozen.
Number of patients with
abnormal results
12 13 12 13 14
various types (au to immune type, hypersplenic syn- drome of unknown origin, heredi tary spherocytosis) were included in the study. Their hematological data are summarized in Table 1. The diagnosis of hemolyt ic disease was based on a reduced red cell count, increased reticulocyte count, decreased hemoglobin and hapto- globin concentration, and diminished red cell life span. The la t ter sign was present in all the pat ients , whereas the others were normal in one or two individual sub- jects. A reduced red cell life span was a prerequis i te for the diagnosis in combination with three of the other signs, abnormal cell morphology in the per iphera l blood smear , and the clinical picture.
Results
METHOD COMPARISON
ENZYMATIC METHODS Linearity
Preassay t r ea tmen t of specimens was carried out according to Li et al. (5). After the protein precipitat ion, creatine was measured in the supe rna tan t wi th an enzymatic endpoint method on the COBAS BIO. The complete conversion t ime of creat ine to creat ine phos- phate was determined by moni tor ing the consumption of NADH spectrophotometrical ly at 340 nm. The sam- ple volume was 0.03 ml, the final volume 0.185 ml. For comparison, the improved diacetyl-a-naphthol method of Li et al. described for the centrifugal analyzer was used on the COBAS BIO (5).
For the es t imat ion of the red cell life span, the ra- dioactive chromium technique was used (8). The ref- erence values are 90-130 d.
STATISTICAL ANALYSIS
The stock solution described above was diluted with water to give known concentrations from 3.0 ~mol /L up to 1.22 mmol/L. Each solution was analyzed with both methods. Using 12 different concentrations the enzy- mat ic assay was l inear from 6 .1~mol /L - 760 ~mol /L and the diacetyl-~-naphthol reaction from 3.0 ~mol/L - 611 ~mol/L. Samples exceeding tha t range were diluted with water.
Precision
For the within-day precision samples were assayed on one day and for the day-to-day precision over a period of 10 d. Both methods showed an acceptable wi thin-day precision, whereas the enzymatic method performed bet ter from day to day (Table 2).
Range and median are used to describe the reference interval because no normal distr ibution was observed in the small number of control individuals. For the method comparison a regression analysis was used. The preci- sion data and the hematological findings were calcu- lated on the basis of a normal distr ibution using the mean and s tandard deviation (9).
PATIENT SELECTION
Fourteen pat ients suffering from hemolyt ic anemia of
Recovery
The recovery of creatine was assessed af ter addition of aqueous solutions containing 76, 228, and 331 ~mol/L creat ine to three different concentrations of packed erythrocytes (235,327, and 350 ~mol /L creatine) before the precipitat ion step (5). The creatine concentrat ion was measured with both methods in triplicate. At the concentrations studied, the mean recovery was 97.2% (range 92-105) for the enzymatic method and for the diacetyl-~-naphthol reaction 101% (range 96-103) .
330 CLINICAL BIOCHEMISTRY, VOLUME 20, OCTOBER 1987
RED CELL CREATINE
TABLE 2 Precision of Creatine Assay ~
-+ SD CV% 2 _+ SD CV% ~ _+ SD CV%
Within day (n = 10) Enzymatic method Diacetyl-~-naphthol
Day to day (n = 10) Enzymatic method Diacetyl-a-naphthol
213 -+ 7.0 3.3 506 -+ 5.0 0.98 1037 _+ 29.7 2.9 261 +- 9.1 3.5 550 -+ 8.8 1.6 1077 _+ 20.9 1.9
194 -+ 6.8 3.5 488 -+ 14.1 2.9 944 - 34.7 3.7 241 -+ 16.0 6.6 538 -+ 27.0 5.0 1000 + 65.9 6.6
a ~mol/L packed red cells.
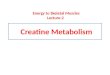
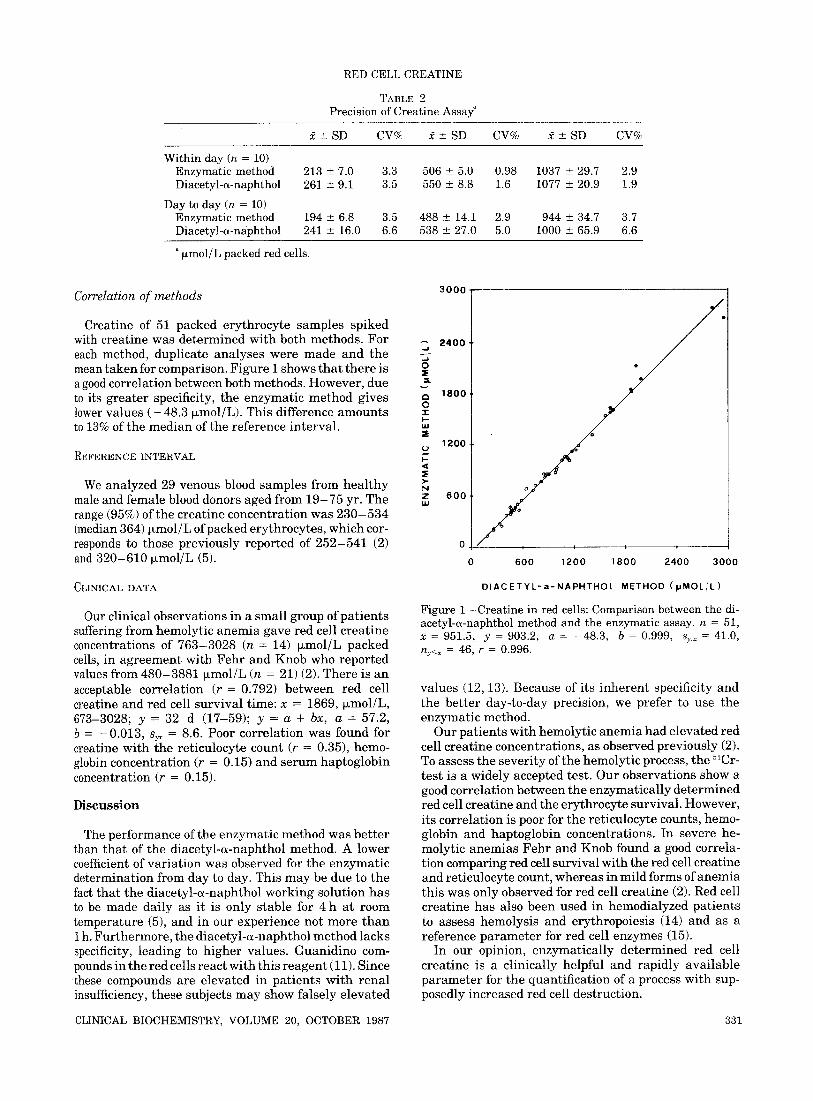
Correlation o f m e t h o d s
Creatine of 51 packed erythrocyte samples spiked with creatine was determined with both methods. For each method, duplicate analyses were made and the mean taken for comparison. Figure I shows that there is a good correlation between both methods. However, due to its greater specificity, the enzymatic method gives lower values ( - 48.3 ~mol/L). This difference amounts to 13% of the median of the reference interval.
REFERENCE INTERVAL
We analyzed 29 venous blood samples from heal thy male and female blood donors aged from 19-75 yr. The range (95%) of the creatine concentration was 230 -534 (median 364) jxmol/L of packed erythrocytes, which cor- responds to those previously reported of 252-541 (2) and 320-610 ~mol/L (5).
CLINICAL DATA
Our clinical observations in a small group of patients suffering from hemolytic anemia gave red cell creatine concentrations of 763-3028 (n = 14) ~mol/L packed cells, in agreement with Fehr and Knob who reported values from 480-3881 ~mol/L (n = 21) (2). There is an acceptable correlation (r = 0.792) between red cell creatine and red cell survival time: x = 1869, ~mol/L, 673-3028; y = 32 d (17-59); y = a + bx, a = 57.2, b = -0 .013, syx -- 8.6. Poor correlation was found for creatine with the reticulocyte count (r = 0.35), hemo- globin concentration (r = 0.15) and serum haptoglobin concel~tration (r = 0.15).
Discussion
The performance of the enzymatic method was better than that of the diacetyl-~-naphthol method. A lower coefficient of variation was observed for the enzymatic determination from day to day. This may be due to the fact that the diacetyl-~-naphthol working solution has to be made daily as it is only stable for 4 h at room temperature (5), and in our experience not more than 1 h. Furthermore, the diacetyl-~-naphthol method lacks specificity, leading to higher values. Guanidino com- pounds in the red cells react with this reagent (11). Since these compounds are elevated in patients with renal insufficiency, these subjects may show falsely elevated
3000 1
2400~ .-i .J o =E ,,s
CI
o -r ,>- U.l
I-
>-
N Z ~u
1800
1200
6 0 0
0
0
"e
" o o e
6 0 0 1 2 0 0 1 8 0 0 2 4 0 0 3 0 0 0
D I A C E T Y L - a - N A P H T H O L METHOD ( N M O L / L )
Figure 1--Creatine in red cells: Comparison between the di- acetyl-(~-naphthol method and the enzymatic assay, n = 51,
= 951.5, y = 903.2, a = -48.3, b = 0.999, s~.x = 41.0, ny<x = 46, r = 0.996.
values (12, 13). Because of its inherent specificity and the better day-to-day precision, we prefer to use the enzymatic method.
Our patients with hemolytic anemia had elevated red cell creatine concentrations, as observed previously (2). To assess the severity of the hemolytic process, the ~lCr- test is a widely accepted test. Our observations show a good correlation between the enzymatically determined red cell creatine and the erythrocyte survival. However, its correlation is poor for the reticulocyte counts, hemo- globin and haptoglobin concentrations. In severe he- molytic anemias Fehr and Knob found a good correla- tion comparing red cell survival with the red cell creatine and reticulocyte count, whereas in mild forms of anemia this was only observed for red cell creatine (2). Red cell creatine has also been used in hemodialyzed patients to assess hemolysis and erythropoiesis (14) and as a reference parameter for red cell enzymes (15).
In our opinion, enzymatically determined red cell creatine is a clinically helpful and rapidly available parameter for the quantification of a process with sup- posedly increased red cell destruction.
CLINICAL BIOCHEMISTRY, VOLUME 20, OCTOBER 1987 331

CRAMER, DAUWALDER, MEIER, AND COLOMBO
Acknowledgement
This project was supported by the Swiss National Science Foundation, grant hr. 3.879.0.83.
References
1. Opalinski A, Beutler E. Creatine, 2,3-diphosphoglycerate and anemia. N Engl J Med 1971; 285: 483-6.
2. Fehr J, Knob M. Comparison of red cell creatine level and reticulocyte count in appraising the severity of hemolytic processes. Blood 1979; 53: 966-76.
3. Smith BJ, Mohler DN, Wills MR, Savory J. Erythrocyte creatine levels in anemia. Ann Clin Lab Sci 1982; 12: 439-46.
4. Griffith WJ. The determination of creatine in body fluids and muscle, and of phosphocreatine in muscle, using the AutoAnalyzer. Clin Chim Acta 1964; 9: 210-13.
5. Li PK, Lee JT, Li CS, Deshpande G. Improved method for determination of erythrocyte creatine by the diacetyl-a- naphthol reaction: elimination of endogenous glutathione interference. Clin Chem 1982; 28: 92-6.
6. Tanzer ML, Gilvarg C. Creatine and creatine kinase mea- surement. J Biol Chem 1959; 234: 3201-4.
7. Wahlefeld AW, Siedel J. Creatine and creatinine. In: Berg- meyer HU Ed. Methods of enzymatic analysis, 3rd ed. Vol. VIII. Pp 488-507. Weinheim: Verlag Chemie, 1985.
8. Dacie J, Lewis SM. Practical haematology, 6th ed. P. 298 Edinburgh: Churchill, 1984.
9. Richterich R, Colombo JP. Clinical Chemistry. P. 29 New York: John Wiley & Sons, 1981.
10. Bucher U, Beck EA. Die einfachen h~imatologischen Laboruntersuchungen Pp. 49, 69, 130. Berne: H. Huber, 1978.
11. WongT. Studies on creatine determination by a-naphthol- diacetyl reaction. Anal Biochem 1971; 40: 18-28.
12. CohenBD. Guanidinosuccinicacidinuremia.ArchIntern Med 1970; 126: 846-50.
13. Shainkin-Kestenbaum R, Giat Y, Berlyne GM. The tox- icity of guanidino compounds in the red blood cell in uremia and the effects ofhemodialysis. Nephron 1982; 31: 20-3.
14. Eggert W, Syllm-Rapoport I, Daniel A, Wolf S. Das Ver- hal ten des Kreatins in roten Blutzellen und im Plasma von Kindern mit chronischer Niereninsuffizienz. Helv PaediatActa 1983; 38: 281-90.
15. Brewster MA, Berry DH. Detection of G6PD and pyruvate kinase deficiencies in reticulocytosis by reference to eryth- rocyte creatine. Clin Biochem 1981; 14: 132-4.
332 CLINICAL BIOCHEMISTRY, VOLUME 20, OCTOBER 1987