Embed Size (px)
Citation preview

3. EPIDEMIOLOGIC TRENDS OF
HEAD AND NECK CANCERS

25
3.0 EPIDEMIOLOGIC TRENDS OF HEAD AND NECK CANCERS
3.1 Introduction
Head and neck cancers are among the 10 most common cancers globally. In India, it
accounts for one fourth of male cancers and one tenth of female cancers (Yeole 2001).
The sub-site predilection of head and neck squamous cell carcinoma (HNSCC) reflects
the risk profile of a community and there are suggestions that these are changing over
time.
The risk factors in different countries are different. This leads to difference in risk of
HNSCC and sub-site predilection. With changes in risk profile, both the incidence and the
sub-site predilection may change. Among females the age-adjusted rates of India are the
highest in the world (Parkin 1997; Parkin 1998; Sankaranarayanan, Masuyer et al. 1998;
Parkin 2002). In India, oral cavity (ICD-9 141,143-5) is the predominant site, whereas
pharynx (ICD-9 146,148,149) is the common site in France (Coleman 1993). The
difference in disease predilection may be a reflection of the prevailing risk habits of the
population (Sankaranarayanan 1998; Menvielle 2004).
Globally the major cause for oral cancer is the use of tobacco products (Johnson 2001;
Winn 2001 ). Consumption of alcohol is synergistic as a risk factor; it is super-
multiplicative for the mouth, additive for the larynx and between additive and
multiplicative for the esophagus (Fioretti 1999 ). Tobacco smoke, smokeless tobacco,
alcohol, marijuana use, deficient diet, Human Papilloma virus infection have been
suggested as risk factors for head and neck cancers (Hashibe 2000; Iype 2001; Balaram
2002). The practice of different habits in different populations might account for the
difference in subsite predilection and the difference in the incidence observed.
3.2 Hypothesis
Changes in risk habits over the years may reflect in the incidence and sub-site
predilection of head and neck cancer.
3.3 Objectives
1. To determine the trends in incidence of head and neck squamous cell carcinoma
over a time period in India.

26
2. To compare change in the trends of head and neck squamous cell carcinoma of
India and US populations.
3. To evaluate etiologic basis for the change in trends (if any) of head and neck
squamous cell carcinoma.
The overall goal of this part of the project is to determine whether there is a change in the
trends of head and neck cancers in India and to find out if they are comparable between
urban and rural populations and those of the developed nations. We hypothesize that the
changes in risk habits and urbanization of rural population may cause alterations in the
patterns of HNSCC, like the age of onset and subsite predilection. To test the hypothesis
we conducted an in-depth analysis of cancer registry data representing one urban and one
rural population in India. We also compared the incidence trends in head and neck
cancers with data from developed countries to frame an etiological hypothesis if any.
Additionally we have investigated whether or not there has been a change in the risk
factor profile in comparison to historical data to the present time, and to determine
whether there are significant numbers of patients without any established risk factors in
our hospital set up.
3.4 Background
Head and Neck Squamous cell carcinoma (HNSCC), which constitutes the most common
upper aero digestive tract carcinomas, has a distinct geographical predilection. It accounts
for 3% of all cancers in the developed countries like USA whereas in developing
countries like India it accounts for 30% of all cancers.
3.4.1 Variation in incidence
3.4.1.1 Geographic
The age-adjusted rates of head and neck cancers are highest in countries like France,
India, Brazil, and USA (Blacks) (Fig. 3.1). The age adjusted rates of head and neck
cancers range from 45 in France to 5 in places like Costa Rica, Kuwait and Japan (Parkin
2002). There is also a distinct site predilection in different countries.

27
As far as oral cancers are concerned, the AAR range from as high as 21.5 among males in
South Karachi, Pakistan to as low as 0.8 in Ecuador, Quito (Curado 2007) (Fig 3.2).
AAR - Countries
<21.5 -Pakistan, India, France, Brazil, Spain, Australia,
<10.0 - USA Blacks, Germany, Thailand, Italy, Russia, USA Whites, Canada,
Switzerland
<5.0 – Netherlands, Finland, Ireland, Japan, Iceland, Sweden, Singapore, China
<2.5- Oman, Korea, Uganda, Malaysia, Algeria, Zimbabawe, Ecuador.
Among females it is as high as 19.3 in South Karachi, Pakistan to as low as 0.1 in Chile.
<19.3- Pakistan, India, Australia
<5.0 – Switzerland, USA Blacks, USA Whites, Thailand, Brazil, Canada, Switzerland
<2.5 - Austria, France, Germany, Italy, Malaysia, Spain, Finland, Japan
<1.0 – Korea, Israel, China, Algeria, Chile
3.4.2 Variations in risk factors
3.4.2.1 Smoking
Smoking of tobacco in the forms of cigarettes, bidis, cigars and cheroots and loose
tobacco in pipes is common. And previous literature gives good evidence of dose
response relationship for both tobacco and alcohol (Blot 1988; Blot 1992). Bidi smoking
is more hazardous than cigarette smoking. Reverse smoking with the lighted end inside


28
the mouth which is practised in rural Andhra Pradesh is linked with hard palate cancers
(Gupta 1980; van der Eb 1993).
3.4.2.2 Smokeless tobacco
It is more in use globally, being placed into contact with the mucous membrane. The practice of
placing snuff in the lower labial sulcus though has become less popular, but still in practice in
Scandinavia and USA is associated with oral cancers (Blot 1977; Winn 1981). Tobacco flakes is
used for chewing by North Americans (Johnson 2003). In Cuba, 82% of oral cancer cases were
attributable to tobacco smoking & 19% to smoking cigars or pipe only (Garrote 2001). Over 80%
of oral cancers in the United States (Blot 1988) and in Europe (Negri 1993) are attributable to
tobacco smoking and heavy alcohol consumption, with low intake of fresh fruit and vegetables
playing a smaller role. In the UK, cigarette, cigar and pipe smoking are the main forms of tobacco
use and all are causes of oral cancer (Warnakulasuriya 2005).
The primary cause of the very high incidence of oral cancer in South Asia is the widespread habit
of chewing betel quid (or paan) and related areca nut use (Bedi 1996). In India tobacco is mostly
combined with other ingredients like betel leaf, arecanut, slaked lime, etc.
Table 3.1: Common forms of oral smokeless tobacco in developing countries (Johnson 2003)
Habit Ingredients Population
Pan/paan/betel quid Areca nut, betel leaf, slaked lime, catechu,
condiments, with or without tobacco
Indian subcontinent, South-east Asia, Papua,
New Guinea, part of South America
Khaini Tobacco and lime Bihar –India
Mishri Burned tobacco Maharashtra-India
Zarda Boiled tobacco India and Arab countries
Gadakhu Tobacco and molasses Central India
Mawa Tobaco, lime and areca Bhavnagar –India
Nass Tobacco, ash, cotton or sesame oil Central Asia, Iran, Afghanistan, Pakistan
Naswar/niswar Tobacco, lime, indigo, cardamom, oil,
menthol,etc.
Central Asia, Iran, Afghanistan, Pakistan
Shammah Tobacco, ash, lime Saudi Arabia
Toombak Tobacco and sodium bicarbonate Sudan

29
Chewing of areca nut is common in India, SriLanka, Pakistan, Bangladesh, Myanmar,
Thailand, Cambodia, Malaysia, Indonesia, Singapore, Philippines, New Guinea, Taiwan
and China and in people emigrating from these countries.
A relation between oral cancer and sexual habits also exist, but information is limited
(Maden 1992; Schwartz 1998) A deficient diet also predisposes towards the development
of oral cancers and it has been estimated that this may be responsible for 10-15% of cases
in Europe (La Vecchia 1997). Use of Marijuana is linked to the development of oral
cancers in USA (Zhang 1999). Human Papilloma Viruses especially HPV-16 is the most
common type associated with oral cancers (Park 1991; Yeudall 1992; Sexton 1993;
Woods 1993; Mao 1995 ).
3.4.3 Relationship to the anatomical site of cancer
There is a strong association between the site of cancer and the site where the quid is
placed regularly. Pooling of carcinogens in saliva give rise to cancers in the floor of the
mouth and ventral and lateral tongue.
Smoking is more strongly associated with soft palate and larynx cancers and alcohol with
floor of the mouth and tongue lesions (Boffetta 1992). Lip cancer is most common in fair-
skinned races, particularly in rural areas and in men who work out of doors. Intraoral
cancer in western countries most commonly affects the lateral borders of the tongue and
the floor of the mouth, followed by the buccal mucosa, mandibular alveolus, retromolar
region and soft palate. By comparison, the hard palate and dorsum of the tongue are the
lowest risk sites. In the high-risk areas of south Asia, the buccal, retromolar and
commissural mucosae are the most prone sites. Cancers of the tongue as well as buccal
mucosa have been noted to be quite common in India, attributed to the local custom of
chewing pan, betel leaf with tobacco. In India, smoking is the most common form of
tobacco consumption in urban male population in India whereas in rural population,
chewing tobacco is more common. There are evidences to suggest that the tobacco habits
in populations are changing over time (National Sample Survey Organization NSS 50th
Round (1993-1994) 1998)
3.4.4 Age distribution
In most countries the incidence of oral cancer is low in people below the age of 45
(Ferlay 2001). The incidence of oral cancer increases with age, though the pattern differs
in different countries and with different risk factors. Over the last few decades there have

30
been reports suggesting an increase in incidence among young adults (<45 years). There
is an alarming rise in the incidence of oral cancers among young men due to the heavy
abuse of smokeless tobacco (Johnson 1991; Levi 1994) Davis and Severson (Davis 1987)
were among the first who pointed out an increasing incidence of tongue cancer in young
adults in the United States – with data from the 1970s to 1980s. They reported a 13-fold
increase in those aged 10-29 years (although very small numbers and no significant
trend), a 1.8-fold increase in those aged 30-39 years, no change in the 40-49 age-group
and a 1.2-fold increase in those aged 50 and over. These increases were all accounted for
by rises in male incidence. SEER data analysis by Schantz et al revealed a 7% increase in
tongue cancer incidence from 1973 to 1984 in those under 40 years, which then remains
stable through to the 1990s, while in those over 40 years the incidence increased only
marginally (Schantz 2002). Despite these increases in younger adults, the incidence rates
for older adults remain significantly higher in all of these studies. The explanations for
the increases in younger populations are generally unclear, with various hypotheses
around behavioral risk factors proposed.
3.4.5 Ethnic distribution
Ethnicity strongly influences prevalence due to social and cultural practices. Where such
habits represent risk factors, their continuation by emigrants from high prevalence regions
to other parts of the world results in comparatively high cancer incidence in immigrant
communities (Swerdlow 1995).
3.4.6 Gender distribution
In all countries men are affected almost twice as often as women, probably due to their
higher indulgence in risk factors such as alcohol and tobacco consumption, for intraoral
cancer and sunlight for lip cancer. The incidence of tongue and other intraoral cancer for
women is, however, greater than or equal to that for men in high prevalence areas such as
India, where chewing and smoking are also common among women. Men and women are
also almost equally affected in some of the ethnic groups in Singapore, Denmark and
Hawaii. The disparity between the sexes has decreased progressively especially in
younger age groups which probably could be due to social acceptance of habits among
females. Globally highest rates have been reported from South Karachi of Pakistan and
Trivandrum of India in men (Curado 2007). For females, the highest rate reported has
been in South Karachi of Pakistan and Karunagapally, Poona, Chennai, Trivandrum of

31
India (Curado 2007). In developing countries like India, oral cancer ranks the first most
common cancer in males and third most common cancer in rural Indian females (Mathew
2007).
3.4.7 Trends
Globally, overall there continues to be an increase of newly diagnosed oral cancers
particularly tongue cancers (Parkin 2001; Ferlay 2004; Parkin 2005) The rising trend in
tongue cancer in young men in western countries, is thought to be due to marked
increases in alcohol consumption, perhaps combined with increased use of oral smokeless
tobacco products, especially in the USA and Nordic countries (Macfarlane 1987;
Franchesci 1994; Shiboski 2000; Schantz 2002).
3.4.8 Migrant studies
Migrant studies related to oral cancer are few. McCredie and colleagues found migrants
from the Middle East to Australia have lower rates than native Australians (McCredie
1994). Migrants from Asia and China to London, UK have also been shown in several
descriptive case-series studies to bring with them a higher risk of oral cancer compared to
others in the area (Swerdlow 1995; Warnakulasuriya 1999). This risk was shown to be
passed down generations, and this was considered to be a result of cultural behaviors
including tobacco and betel quid use (Swerdlow 1995; Warnakulasuriya 1999;
Warnakulasuriya 2002). In one another survey it was reported that 80% of the
Bangladeshi community living in London reported using betel quid chewing while also
adopting the cigarette behaviors of the native Londoners (Ahmed 1997).
3.5 Materials & Methods
3.5.1 Population studied
Objective 1: The tumor registry data was taken from an urban South Indian cancer
registry (Chennai-1986-98) and from a rural (Barshi-1988-98) registry, which has data for
a long period since 1982 and 1987 respectively to identify the change in trends of head
and neck cancers. Chennai, a South Indian urban cancer registry caters to an area of
170sq.km and a population of 4.2 millions. The rural registry data was available only
from Barshi. It is the first rural registry in India that covers a total population of around
0.4 million in 346 villages spread over 3713 sq.km. in Solapur district of Maharashtra.
The National Cancer Registry Programme of the Indian Council of Medical Research

(ICMR) monitors these cancer registry data. The data from these two registries were used
to analyze change in trends within the country.
Objective 2: To compare change in trends from India to that of developed nation, data
was taken from the Surveillance, Epidemiology, and End Results (SEER) Program Public
Use (1973-97), National Cancer Institute, Cancer Surveillance Research Program, Cancer
Statistics Branch, of USA, released in April 2000. This data encompass 10% of the U.S.
population. Comparable data from India for this time period was obtained from Mumbai
Cancer Registry. Acceptable levels of reliability and completeness of data have been
reported for the Mumbai cancer registry (Yeole 2001). Mumbai cancer registry
established in 1963 became part of National Cancer Registry Program (NCRP) since
1981-82. It covers the area under the city of Greater Bombay with the area of about 603
sq.km. The data for this registry was taken from Cancer Incidence in 5 Continents vol. IV
to VIII (1973-97). The Descriptive Epidemiology Group of IARC (The International
Agency for Research on Cancer) monitors these data.
Objective 3: To investigate the risk factor profile of head and neck cancers, a
retrospective study was done with data obtained from AIMS Head and Neck tumour
board records between 1st January 2004 and 31st December 2006.
This retrospective study constituted data of 611 Head and Neck cancer patients.
Demographics, cancer sub-site and risk factors were recorded for each patient. The
number of tongue cancer patients with and without risk factors were statistically analysed,
using the Chi-Square test, against various other groups of sub-sites in the Head and Neck
region.
3.5.2 Statistical method adopted
Objectives 1 and 2
In this study we used Age Adjusted incidence Rate (AAR) for analyzing the trends.
Age Specific Incidence Rate (AspR) refers to the rate obtained by dividing the total
number of cancer cases by the corresponding estimated population in that age group and
sex/ site/ geographic area/ time period and multiplying by 100,000.
ASpR = New cases of cancer of a particular year in the given age group x 100,000
Estimated population of the same year for the given age group
32

33
As age increases the incidence of cancers also increases, therefore with an increase in the
median age of a population the cancer incidence also increases in the community. In order
to make the rates comparable between different populations, the age specific incidence
rates are adjusted to the five-year age distribution of the world standard population
(Plummer 1997) to obtain the age-adjusted rates (AAR). Age adjusted rates are calculated
for all age groups as well as for the young (20-44 years) age groups in this study and for
males and females separately.
AAR = Σ (ASpR) X No. of persons in Std. world population in that 5 yr. age group
100,000
Joinpoint regression program is a statistical software for analyzing the trends using
joinpoint models, where different lines are connected together at the joinpoints. The
joinpoint regression analysis involves fitting a series of joined straight lines on a log scale
to the trends in the annual age-adjusted cancer incidence rates. Line segments are joined
at points called joinpoints. Each joinpoint denotes a statistically significant (P = .05)
change in trend. The software takes trend data and fits the simplest joinpoint model that
the data allow. The program starts with the minimum number of joinpoint (e.g. 0
joinpoints, which is a straight line) and tests whether more joinpoints are statistically
significant and must be added to the model (up to that maximum number). This enables
us to test that an apparent change in trend is statistically significant. This is estimated by
the method of Least Squares and the regression equation is stated as Y = mX + b, where
Y is the outcome or the dependent variable- the age adjusted rate, X is the independent
variable- year of diagnosis, m is the annual percentage change, b is the Y-intercept. The
tests of significance use the Monte Carlo permutation method. In the final model, each
joinpoint indicates a statistically significant change in trend, and an estimated annual
percentage change (EAPC) is computed for each of those trends by means of generalized
linear models. A maximum number of 3 joinpoints was allowed for estimations. Once the
line segments are established, the estimated annual percent change is used to describe and
test the statistical significance of the trends in the model. Testing the hypothesis (two-
sided P value < .05) that the annual percent change is equal to zero is equivalent to testing
the hypothesis that the trend in the cancer rates is neither increasing nor decreasing.
Annual Percent Change (APC) gives a complete picture of the trend over time. A short
segment rising at a steep rate may not be statistically significant. Hence to summarize the
trend over a fixed predetermined interval, Average Annual Percent Change (AAPC) is

34
used which computes the summary measure over the fixed interval. This is advantageous
especially when the data is from a small geographic area like Barshi. Since each gives
different perspective, both APC and AAPC are given in the tables. Joinpoint software
version 3.3.1 was used.
Cumulative incidence risk percent and the lifetime risk of developing head and neck
cancers and other subsites were calculated for the urban and rural registry data.
Cumulative risk (Cu R) refers to the probability that the person will develop a particular
cancer during a certain age period in the absence of any other cause of death. The
Cumulative Rate is an approximation of the cumulative risk. It is obtained by adding the
annual age-specific incidence rates for each five-year age interval (for whatever age
group is to be used to calculate the cumulative risk) multiplied by 5 (representing the five
year age interval) times 100 divided by 100000
CuR = 5xΣ(ASpR) x100
100,000
The cumulative incidence rate has a useful probabilistic interpretation. This also removes
the arbitrariness of choosing a standard population. The confidence intervals are
calculated using the formula CIRP+/- (1.96X S.E.). The probability of getting a specific
cancer, expressed in terms of one in every ‘n’ persons is computed by reciprocating
estimated cumulative incidence rate expressed as a percentage.
Head and neck cancers in our study I constitute cancers of the oral cavity, pharynx, and
larynx (ICD-9, 141, 143-146, 148, 149, 161). As there are reports to suggest that the
incidence of tongue cancers is increasing in young adults (Schantz 2002; Stimson and
Guo-Pei 2002), we have separated tongue (ICD-9, 141) from the rest of oral cavity (ICD-
9, 143-5) in our analyses.
Head and neck cancers in our study II include cancers of the tongue, mouth, tonsil,
oropharynx, pyriform sinus, hypopharynx, pharynx unspecified, larynx and excludes
salivary glands, nasopharynx, eye/orbit. Mumbai: ICD-10, C 01-06, C 09-14, USA: ICD-
O-3, C 019-069, C 090-109, C 129, C 130-139, C 140, 142-148. See ICD coding in
annexure I.

35
Objective 3
The statistical test used to analyse the data was the Chi-Square test using the Epi-info
software. The number of tongue cancer patients with and without risk factors were
analyzed against those with cancers of the other head and neck sub sites.
In our retrospective study, 611 HNSCC patients, who presented at AIMS Hospital,
Cochin (Kerala) between 1st January 2004 and 31st December 2006, formed our study
group. The data was obtained from the department’s ‘Tumour Board’ records, which is a
collaboration of each patient’s full history and examination. The data collected for each
patient included:
• Demographics
• Risk factors (Smoking, Alcohol, Paan chewing, Pre-malignant lesions or None)
• Tumour sub-site
• Treatment received
• Follow-up status, where recorded.
The inclusion criteria, for the statistical analysis, were that the patient must have a cancer
of the oral cavity, oropharynx, hypopharynx or larynx. Oral cavity cancers included those
of tongue, buccal mucosa, floor of mouth, retromolar trigone, hard palate, lip and
alveolus. Oropharynx cancers included those of the soft palate, tonsils and other
unspecified oropharyngeal sites. Hypopharnyx cancers included those of the lateral and
posterior pharyngeal walls, pyriform sinus, post cricoid and other unspecified
hypopharyngeal sites. Larynx cancers included those of the glottis, supraglottis and other
unspecified laryngeal sites.
Patients excluded were those who suffered from any other head and neck cancer. Risk
factors were recorded if the patient had the habit at the time of, or within 1 month prior to,
their diagnosis.
The statistical test used to analyse the data was the Chi-Square test. The number of tongue
cancer patients with and without risk factors were analysed against those with cancers of
the previously mentioned sites. Our hypothesis was that there is significant difference
between the number of tongue cancer cases that present without the known associated

risk factors when compared to other subsites. A p value of 0.05 or less determined
significance.
3.6 Results
3.6.1 Objective 1
To determine the trends in incidence of head and neck squamous cell carcinoma over a
time period in India.
The urban registry recorded a total of 6857 head and neck cancers during the time period
1986 to 1998, out of which 4777 were males (23% of all male cancers), and 2080 were
females (9% of female cancers). In the rural registry, a total of 325 head and neck cancers
were registered during the time period 1988 to 1998, out of which 272 were males (28%
of all male cancers) and 53 were females (5% of all female cancers).
The overall male: female ratio of head and neck cancers in urban population is 2:1and in
rural population is 5:1. Table 3.2 gives the subsite distribution of cancers.
Table 3.2: Sub site distribution of total head and neck cancers in urban and rural Indian populations
Urban Rural
Male Female Young
male
Young
female
Male Female Young
male
Young
female
Site
n % n % n % n % n % n % n % n %
Tongue 1019 21 298 14 123 22 47 13 44 16 12 23 6 15 4 29
Oral
cavity
1252 26 1175 57 140 25 181 48 59 22 21 40 15 39 2 14
Larynx 863 18 104 5 100 18 24 6 43 16 5 9 5 13 3 21
Pharynx 1643 34 503 24 198 35 122 33 126 46 15 28 13 33 5 36
36

The AAR of the head and neck cancers and its subsites were analyzed in all and young
age groups in both males and females separately.
Age: To investigate whether there is any change in the incidence of head and neck
cancers in the young adults the AAR for age group 20-44 years were analyzed. In the
urban population, among males, 12% of the total head and neck cancers were from
younger age group (20-44 years) and among females it was 18%. In the rural population,
the contribution of young males was 14.5% and young females were 26%. It is interesting
to note that the young females contribute to nearly one fourth of all rural female head and
neck cancers. Among young adults, the male: female ratio in urban population was 1.5:1
and in rural population it was 3:1. In contrast in patients over 45 years old the male:
female ratio was 2.5:1 in the urban and 6:1 in the rural community.
Subsite: The sub-site distribution of all head and neck cancers in all ages and in young
adults is given in table.2. Oral cavity including tongue was the predominant site in the
urban and rural population except in rural males, where pharynx was the predominant
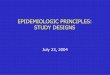
site. The age specific incidence rates of head and neck cancers showed the peak incidence
in 70-74 years in both urban and rural populations (Fig. 3.3)
020406080
100120140160180
0-4
10 to
14
20 to
24
30 to
3440
-4450
-5460
-6470
-74
1986-881989-911992-941995-98
Age groups
Age
Spe
cific
Inci
denc
e R
ate
Figure 3.3: Age Specific Incidence Rates of Head and Neck Cancers in India
The joinpoint analysis of the trends in the age-adjusted cancer incidence allows us to
more accurately interpret changes over time and, more importantly, to determine if those
changes are statistically significant. Figures 3.4 through 3.7 graphically display the results
of the joinpoint analysis shown in Tables 3.3 and 3.4.
37

38
The table below shows the best joinpoint fit for each site and the APC & AAPC of the
urban and rural registry data for all ages.
Table 3.3: Joinpoint analysis of the trends in the Age Adjusted Cancer Incidence
Rates of Urban and Rural registries -all ages
APC = Annual Percent Change; AAPC = Average Annual Percent Change
Chennai males-Joinpoint analysis 1986-98 trend 1 trend 2 trend 3 Cancer site: years APC years APC years APC
Head & Neck 1986-98 -1 Tongue 1986-98 -1.1
Other oral cavity 1986-98 -2.3 pharynx 1986-98 -1.76 larynx 1986-98 -0.21
Chennai females-Joinpoint analysis 1986-98 trend 1 trend 2 trend 3 Cancer site: years APC years APC years APC
Head & Neck 1986-98 -3.8
Tongue 1986-98 2.7
Other oral cavity 1986-98 -5.5
pharynx 1986-98 -3.5
larynx 1986-98 -1.4
Barshi males-Joinpoint analysis 1988-98 trend 1 trend 2 trend 3 Cancer site: years APC years APC years APC
Head & Neck 1988-98 -7.4
Tongue 1988-98 -4.3
Other oral cavity 1988-98 -0.2 1991-94 -37.11994-97 44.3
pharynx 1988-98 -8.2
larynx 1988-98 -9.6 Barshi females-Joinpoint analysis 1988-98 trend 1 trend 2 trend 3 Cancer site: years APC years APC years APC
Head & Neck 1988-98 7.7
Tongue 1988-98 24.3
Other oral cavity 1988-98 5.5
pharynx 1988-98 -3.3
larynx 1988-98 *61.9
AAPC=-3.3 last 10 observations

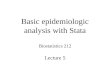
Fig.3.4. Trends in AAR of Head and Neck cancers and subsites – Chennai all ages
a b
c d
e f
g h

i j
a: Head and Neck cancers males, b: Head and Neck cancers females, c.Tongue cancers male, d. Tongue cancers female
e. Other oral cavity cancers male, f. Other oral cavity cancers female, g. Pharynx cancers male, h. Pharynx cancers female
i. Larynx cancers male, j. Larynx cancers female
Fig.3.5. Trends in AAR of Head and Neck cancers and subsites – Barshi all ages
a b
c d

e f
g h
i j
a: Head and Neck cancers males, b: Head and Neck cancers females, c.Tongue cancers male, d. Tongue cancers female
e. Other oral cavity cancers male, f. Other oral cavity cancers female, g. Pharynx cancers male, h. Pharynx cancers female
i. Larynx cancers male, j. Larynx cancers female

39
Table 3.4 shows the best joinpoint fit for each site and the APC & AAPC of the urban and
rural registry data for the younger age group.
Table 3.4: Joinpoint analysis of the trends in the Age Adjusted Cancer Incidence Rates of
Urban and Rural registries –young
Chennai males-Joinpoint analysis 1986-98 trend 1 trend 2 Cancer site: years APC years APC Head & Neck 1986-98 -3.8 Tongue 1986-98 -7 Other oral cavity 1986-98 -2.3 Pharynx 1986-98 -3.7 Larynx 1986-98 -2.3 Chennai females-Joinpoint analysis 1986-98 trend 1 trend 2 trend 3 trend 4 Cancer site: years APC years APC years APC years APC Head & Neck* 1986-98 19.2 1988-92 -15.3 1992-95 2.4 1995-97 -11.2 Tongue 1986-98 0.8 Other oral cavity 1986-98 -7.8 pharynx 1986-98 -7.7
larynx 1986-98 -
10.6 Barshi males-Joinpoint analysis 1988-98 trend 1 trend 2 Cancer site: years APC years APC Head & Neck 1988-98 -2.7 Tongue 1988-98 -24.5 Other oral cavity 1988-98 29.2 pharynx 1988-98 -45.3 larynx 1988-98 71.8 Barshi females-Joinpoint analysis 1988-98 trend 1 trend 2 Cancer site: years APC years APC Head & Neck 1988-98 50 Tongue 1988-98 50.8 Other oral cavity 1988-98 29.2 pharynx 1988-98 -3.3 larynx 1988-98 53.8
* - AAPC=-8.8 last 10 observations

Fig.3.6. Trends in AAR of Head and Neck cancers and subsites – Chennai young
a b
c d
e f
g h

i j
a: Head and Neck cancers males, b: Head and Neck cancers females, c.Tongue cancers male, d. Tongue cancers female
e. Other oral cavity cancers male, f. Other oral cavity cancers female, g. Pharynx cancers male, h. Pharynx cancers female
i. Larynx cancers male, j. Larynx cancers female
Fig.3.7. Trends in AAR of Head and Neck cancers and subsites – Barshi young
a b
c d

e f
g h
i j
a: Head and Neck cancers males, b: Head and Neck cancers females, c.Tongue cancers male, d. Tongue cancers female
e. Other oral cavity cancers male, f. Other oral cavity cancers female, g. Pharynx cancers male, h. Pharynx cancers female
i. Larynx cancers male, j. Larynx cancers female

40
Overall there was a reduction in the AAR of head and neck cancers in both urban and
rural population with APC of –1 among urban males, –3.8 among urban females and –7.4
among rural males. However among rural females the AAR of Head and Neck squamous
cell carcinoma had increased during the study period.
Among males, there was a decrease in the trends of oral cavity cancers (oral cavity
cancers other than tongue) with APC of –2.3 among urban males and –5.5 among urban
females. Among rural males it decreased during the time periods 1988-91, 1991-94 and
increased during 1994-97 with the AAPC of –3.3. Among rural females there was an
increase with the APC of 5.5. With respect to tongue cancers, it was found that there was
a decrease among urban and rural males but an increase among urban and rural females.
There was a decrease in the incidence of pharyngeal and laryngeal cancers in the urban
and rural population except for an increase among rural females.
Analysis of the incidence trends in young urban population revealed that there was a
decrease in the incidence of all cancers except for an increase in tongue cancers among
females. Among rural males there was a decrease in the incidence of head and neck,
tongue and pharynx cancers and an increase in other oral cavity and larynx cancers.
Among rural females, there was an increase in the incidence of all cancers of interest
except pharynx cancers, which showed a decrease. The increased AAPC in Barshi might
be due to the lower number of cancer cases reported.
The probability estimates showed that among urban population, one out of every 27men
and one out of every 64 women would contract head and neck cancer in their life span
(Table 3.5). Estimation of the cumulative incidence rate percentage showed that 3.7% of
the urban male population is estimated to develop head and neck cancer in their life span;
out of this 0.2% belong to 20-44 years age group. Of the urban female population 1.6% is
estimated to develop head and neck cancer in their life span; out of this 0.13% belong to
the younger age group.
Among rural population, one out of every 54 men and one out of every 494 women would
contract head and neck cancers in their lifespan. Estimation of the cumulative incidence
rate percentage showed that 2% of the rural male population is estimated to develop head
and neck cancer in their life span; out of this 0.2 % belongs to 20-44 years age group. Of
the rural female population 0.3% is estimated to develop head and neck cancer in their

life span; out of this 0.1 % belong to the younger age group. The probability estimates of
the sub sites are also given in Table 3.5.
Table 3.5: Probability estimates of the sub sites in urban and rural populations
LTR CIRP
Urban Rural Urban Urban Rural Rural Site
M F M F M F M F
Head &
neck 27 64 54 494
4%
(3.433-
4.036)
1.6%
(1.444-
1.716)
2%
(1.565-
2.438)
0.34%
(0.203-
0.463)
Tongue 136 458 459 1250
.76%
(0.657-
0.864)
.23%
(0.199-
0.259)
0.33%
(0.188-
0.483)
0.07%
(0.007-
0.138)
Oral cavity 102 111 422 1068
1%
(0.902-
1.102)
.94%
(0.816-
1.065)
0.33%
(0.213-
0.522)
0.12%
(0.079-
0.162)
Larynx 150 138
6 -* -*
.69%
(0.611-
0.766)
.08%
(0.064-
.092)
0.24%
(0.210-
0.451)
0.003%
(-.012-
.066)
Pharynx 80 313 130 1304
1.27%
(1.154-
1.413)
.3%
(0.287-
0.386)
0.97%
(0.676-
1.261)
0.11%
(0.055-
0.168)
*- Not enough cases for reliable estimation
LTR-Life time risk; CIRP-Cumulative Incidence Rate Percent 95% Confidence Intervals of the difference
for CIRP, the lower and upper limits are given in brackets.
3.6.2 Objective 2
To compare the change in trends of head and neck squamous cell carcinoma of India and
US populations.
41

In this study the trends in the age adjusted rates of the head and neck cancers and its
subsites from Mumbai cancer registry were compared with that of SEER data. Figures 3.8
through 3.11 graphically display the results of the joinpoint analysis shown in Tables 3.6
and 3.7. The table below shows the best joinpoint fit for each site and the APC & AAPC
of the Mumbai and SEER registry data for all ages and younger age group respectively.
Table 3.6: Joinpoint analysis of the trends in the Age Adjusted Cancer Incidence
Rates of Mumbai and SEER database -all ages
42
ALL AGES Mumbai males
Joinpoint analysis 1973-97 trend 1 trend 2 Cancer site years APC years APC
Head & Neck 1973-97 -9.4 Tongue 1973-97 -14
Other oral cavity 1973-97 -0.6 pharynx 1973-97 -12.6 larynx 1973-97 -13.2
Mumbai females Joinpoint analysis 1973-97 trend 1 trend 2 Cancer site years APC years APC
Head & Neck 1973-97 -10.5
Tongue 1973-97 -13.8
Other oral cavity 1973-97 -6.2
pharynx 1973-97 -12.6
larynx 1973-97 -17.7 SEER males Joinpoint analysis 1973-97
trend 1 trend 2 Cancer site years APC years APC
Head & Neck 1973-97 3.0 1983-97 -7.8
Tongue 1973-97 6.1 1983-97 -0.8 Other oral cavity 1973-97 3.7 1983-97 -11.6
pharynx 1973-97 9.27 1983-97 -10.01
larynx 1973-97 0.3 1983-97 -11.2 SEER females Joinpoint analysis 1973-97
trend 1 trend 2 Cancer site years APC years APC
Head & Neck 1973-97 -2
Tongue 1973-97 1.49
Other oral cavity 1973-97 -4.9
pharynx 1973-97 -3.6
larynx 1973-97 1.5
AAPC= -2.5 last 10 observations AAPC= +2.6 last 10 observations AAPC= -4.3 last 10 observations AAPC= -0.8 last 10 observations AAPC= -5.6 last 10 observations

Fig.3.8. Trends in AAR of Head and Neck cancers and subsites – Mumbai all ages
a b
c d
e f
g h

i j
a: Head and Neck cancers males, b: Head and Neck cancers females, c.Tongue cancers male, d. Tongue cancers female
e. Other oral cavity cancers male, f. Other oral cavity cancers female, g. Pharynx cancers male, h. Pharynx cancers female
i. Larynx cancers male, j. Larynx cancers female
X‐ axis‐‐‐ Year: 1=1973‐77, 2=1978‐82, 3=1983‐87, 4=1988‐92, 5= 1993‐97
Fig.3.9. Trends in AAR of Head and Neck cancers and subsites – SEER all ages
a b
c d

e f
g h
i j
a: Head and Neck cancers males, b: Head and Neck cancers females, c.Tongue cancers male, d. Tongue cancers female
e. Other oral cavity cancers male, f. Other oral cavity cancers female, g. Pharynx cancers male, h. Pharynx cancers female
i. Larynx cancers male, j. Larynx cancers female
X‐ axis‐‐‐ Year: 1=1973‐77, 2=1978‐82, 3=1983‐87, 4=1988‐92, 5= 1993‐97

Table 3.7: Joinpoint analysis of the trends in the Age Adjusted Cancer Incidence
Rates of Mumbai and SEER database -young
Mumbai males Joinpoint analysis 1973-97
trend 1 trend 2 Cancer site: years APC years APC
Head & Neck 1973-97 -7.7 Tongue 1973-97 -11.7
Other oral cavity 1973-97 1.2
pharynx 1973-97 4.6 1983-97 -36 larynx 1973-97 -15.6
Mumbai females Joinpoint analysis 1973-97 trend 1 trend 2 Cancer site: years APC years APC
Head & Neck 1973-97 -7.39
Tongue 1973-97 3.89
Other oral cavity 1973-97 -13.8
pharynx 1973-97 -8.11
larynx 1973-97 -4.32 SEER males Joinpoint analysis 1973-97
trend 1 trend 2 Cancer site: years APC years APC
Head & Neck 1973-97 16.7
Tongue 1973-97 45.7 1983-97 -1.8 Other oral cavity 1973-97 36.96
pharynx 1973-97 53.68
larynx 1973-97 -14.39 1983-97 -0.21 SEER females Joinpoint analysis 1973-97
trend 1 trend 2 Cancer site: years APC years APC
Head & Neck 1973-97 2.3
Tongue 1973-97 16.9
Other oral cavity 1973-97 -3.3
pharynx 1973-97 1.63 1983-97 -98.93
larynx 1973-97 -11.1
AAPC = +19.6 last 10 observations
AAPC= -18.1 last 10 observations
AAPC= -7.6 last 10 observations
AAPC= -6.7 last 10 observations
Analysis of the Mumbai registry data showed that there was an overall decrease in the
incidence of head and neck cancers and the subsites during the study period. SEER data
analysis also showed that there was a decrease in the incidence of head and neck cancers
43

Fig.3.10. Trends in AAR of Head and Neck cancers and subsites – Mumbai young
a b
c d
e f
g h

i j
a: Head and Neck cancers males, b: Head and Neck cancers females, c.Tongue cancers male, d. Tongue cancers female
e. Other oral cavity cancers male, f. Other oral cavity cancers female, g. Pharynx cancers male, h. Pharynx cancers female
i. Larynx cancers male, j. Larynx cancers female
X‐ axis‐‐‐ Year: 1=1973‐77, 2=1978‐82, 3=1983‐87, 4=1988‐92, 5= 1993‐97
Fig.3.11. Trends in AAR of Head and Neck cancers and subsites – SEER young
a b
c d

e f
g h
i j
a: Head and Neck cancers males, b: Head and Neck cancers females, c.Tongue cancers male, d. Tongue cancers female
e. Other oral cavity cancers male, f. Other oral cavity cancers female, g. Pharynx cancers male, h. Pharynx cancers female
i. Larynx cancers male, j. Larynx cancers female
X‐ axis‐‐‐ Year: 1=1973‐77, 2=1978‐82, 3=1983‐87, 4=1988‐92, 5= 1993‐97

44
except for the increase in the incidence of tongue cancers both among males and females
and larynx cancers among females.
Analysis of the Mumbai data among the younger age group showed similar results as that
of all ages except for the increase in incidence of other oral cavity among males and
tongue cancers among females.
SEER data analysis among the younger age group showed that there was an increase in
the incidence of head and neck especially tongue cancers both among males and females.
Other oral cavity and pharynx cancers showed an increase among young males and a
decrease among young females. There was a decrease in the incidence of laryngeal
cancers.
Proportion:
The SEER data showed that the Head and Neck Cancers formed around 6% (1977-82) to
4% (1993-97) of all cancers among males and around 2% (1977-82) to 1.7% (1993-97)
among females, whereas in Mumbai, they formed around 31% (1977-82) to 25% (1993-
97) of all cancers among males and 12% (1977-82) to 9% (1993-97) among females.
Cumulative rate and risk
Mumbai data showed that one out of every 16 men and one out of every 48 women would
contract head and neck cancers in their life span, whereas SEER data showed that one out
of every 25 men and one out of every 83 women would contract head and neck cancers in
their life span.
3.6.3 Objective 3
To evaluate etiologic basis for the change in trends (if any) of head and neck squamous
cell carcinoma.
The risk factors and cancer sub-site information was extracted from the raw data and the
information has been summarised in Table 3.8, and then used in the statistical analysis
(Table 3.9)
A total of 611 head and neck cancer patients (males=473-77%, females=138-33%)
reported at our hospital during the study period. Forty nine percent patients presented
with risk habits (n=298, males=93%, females=7%). Patients with cancers of tongue, oral
cavity, oropharynx, hypopharynx and larynx were included in the study. One hundred and

45
twenty nine patients with other head and neck cancers were excluded from the study.
Tongue cancer made up 151 patients of our study group, i.e. 25% of the patients. The
second most prevalent cancer at this institute within the last few years was cancer of the
glottis (82 patients), making up 13% of head and neck cancers. The raw data showed
quite a high proportion of tongue cancer patients who presented without any risk factors
(48%).
Table 3.8: Summarised risk factors vs. generalized cancer sub-sites
Risk Factors
Sub-sites
Sub-site
Proportion Presence % Absence %
Tongue 31% 78
(m=75, f=3) 52
73
(m=51, f=22) 48
Other Oral
Cavity 28%
73
(m=58, f=15) 54
62
(m=38, f=24) 46
Oropharyn
x 8%
29
(m=27, f=2) 78
8
(m=6, f=2) 22
Hypophary
nx 9%
28
(m=26, f=2) 62
17
(m=7, f=10) 38
Larynx 24% 68
(m=68, f=0) 60
46
(m=42, f=4) 40
Total 100% 276
(m=254, f=22)
57 206
(m=144, f=62)
43
Excluded
data
22
(m=22, f=0)
107
(m=53, f=54)
m-males, f-females

Chi-square analysis of tongue cancers against cancers of other subsites were analysed
using the Epi-info software. However, following the statistical analysis of tongue cancers
against cancers of the remainder of the oral cavity (135 patients), a P value of 0.77 was
obtained. This tells us that the number of tongue cancers presenting without any risk
factors, when compared to the rest of the oral cavity, is not of significance. Statistical
analysis of tongue cancers against the hypopharnyx (45 patients) and larynx (114
patients) also showed insignificance. However, a P value of 0.0058 was obtained when
analysing tongue cancer against the oropharnygeal cancers (37 patients). This tells us that
the prevalence of tongue cancer patients without risk factors is of a significant value,
when compared to oropharyngeal cancers.
Table.3.9: Statistical analysis results of tongue cancers against other subsites
46
Tongue vs Odds ratio P value
Oral cavity 0.91 0.77
Oropharynx 0.29 0.0058
Hypopharynx 0.65 0.28
Larynx 0.72 0.24
3.7 Discussion
In this study it is shown that that there is an overall reduction in the incidence of head and
neck cancers.
This is consistent with the previous studies published on head and neck cancer trends. A
slow and steady decline in the trend of head and neck cancers is seen in India (Yeole
2003 ). A study on the data from Mumbai cancer registry for 15 years from 1986-2000 on
time trends in the incidence and the risk of developing oral cancer has shown a decreasing
trend which was significant among males (Sunny 2004). In our study II it is shown that
the head and neck cancers showed a decline in the trend and accounted for 25% of male
cancers and 12% of female cancers in Mumbai. The overall incidence of head and neck
cancers was found to be stable among Americans during the time period 1973-97
(Schantz 2002). This reduction in head and neck cancer trends was not observed in young

47
Americans and rural Indian females. The increased incidence observed in rural females
might be due to very few cases reported there.
What is alarming is a consistent increase in the incidence of tongue cancers observed in
females- Indian urban, rural & SEER in both all age groups and younger age groups, in
young Mumbai females and in SEER males. Such increase was not found among Indian
males.
Oral cavity cancers showed a decline in the incidence in the study groups except for an
increase among rural females and young rural, Mumbai and SEER males. And there is an
overall reduction in the incidence of laryngeal cancers in all the study groups. This was
not observed among rural females and young rural males and young Americans, both
males and females as far as laryngeal cancers are concerned. With respect to pharyngeal
cancers there is a uniform reduction in the incidence except for an increase shown by
young SEER males.
The observed trends are a "tip-of-the-iceberg" phenomenon. Several factors like
prevalence of risk habits, awareness, screening, diagnosis and completeness of reporting
can affect the reported incidence of cancer.
There are strong epidemiological evidences to link tobacco habits with the occurrence of
head and neck cancers. A wide variety of tobacco habits like smoking, chewing, snuffing,
using burnt tobacco as powder or paste are prevalent in India, which is more so in the
rural population than in their urban counterparts (National Sample Survey Organization
1998). Among them, bidi smoking, tobacco chewing and cigarette smoking, in that order,
account for a large majority of head and neck cancers (Sanghvi 1989). Smoking is most
common form of tobacco consumption among males and chewing among females
(National Sample Survey Organization NSS 50th Round(1993-1994) 1998). Tobacco
related cancers (TRC) account for nearly 48.2% of all cancers in Indian men and 20.1%
in women (Gajalakshmi 1996). Other than tobacco, alcohol abuse and viral infection have
been implicated in head and neck carcinogenesis. In India, National Sample Survey
Organization (NSSO) collects data on the prevalence of tobacco use. The data on tobacco
consumption over the periods 1987-88 to 1993-94 has shown that it has decreased in both
urban and rural males and females. Contrary to the popular belief that the tobacco
consumption is increasing, this data shows that it has decreased in all sectors. According
to the National Health Interview Survey the prevalence of cigarette smoking and alcohol

48
use among Americans have markedly decreased (US Department of Health and Human
Services 1994; US Department of Health and Human Services 1998; The Gallup
Organization 2001). Possibly the decreased consumption could account for the decrease
in head and neck cancers, especially that of oral cavity. Though there is a decreasing
trend, the incidence of oral cavity cancers in India, is still one of the highest in the world
(Franceschi 2000). One of the possible reasons could be the easy availability of tobacco
products. Women appear to have a higher prevalence of chewing in many rural areas due
to the beliefs that tobacco has many magical and medicinal properties; keeping the mouth
clean, getting rid of a foul smell, curing toothache, controlling morning sickness, and
minimizing labor pains.
The sub-site predilection table shows that the reduction in incidence is obvious in tumors
where tobacco is the primary risk factor such as oral cavity (chewing of tobacco) and
larynx (smoking). Similar trends were observed in other parts of India (Coleman 1993;
Sunny 2004). The decreasing trend may be attributable to a decrease in the usage of pan
and tobacco. The increased incidence of oral cavity cancers in rural females and young
rural and Mumbai males might be attributed to the common habit of chewing in rural
population especially females and young Mumbai males. There are many reports from
Mumbai stating the increased prevalence of chewing among young males. In a study on
use of tobacco products among students and school personnel in India, it was found to be
14.1% among students-17.3% boys and 9.8% girls (Sinha 2007).
There are reports from Europe and United State of America to suggest that head and neck
cancers are increasing among young, particularly in tongue (Schantz 2002; Llewellyn
2004). Young Americans are diagnosed with increased rates of oral and tongue cancers
attributed to the use of smokeless tobacco and marijuana. This finding was not observed
in our study though there was an increased incidence of tongue cancers among both urban
and rural females as well as in young females in Mumbai.
There are not many reports from India about the awareness of these cancers among the
general public. Few reports from developed countries have shown an alarming lack of
awareness of oral cancer among the public (Warnakulasuriya 1999). In India
(unpublished data), there seems to be increased awareness of oral cancer and its factors,
which is discussed elaborately in chapter 5.

49
There is increased incidence of cancers in rural population especially females
emphasizing the need to target that population for health education. The increased
incidence might be due to the very few number of cases reported there. Indian data
showed an increase of tongue cancers among females and oral cavity cancers among
Mumbai males.
And in our study III, it was found that 48% of tongue cancers did not have any
established risk factors. It is fair to say from the statistical analysis that the number of
tongue cancer patients presenting without risk factors are not of a significant level,
especially when compared to the remainder of the oral cavity except oropharynx. But the
raw results of tongue cancer alone show quite a striking number of cases (48%) that
presented to the hospital without any of the known associated risk factors. As for the
possible aetiological factors for tongue cancers, firstly it should be reminded that 52% of
tongue cancer patients did indeed have one or more of the known associated risk factors.
Out of these, 62 were smokers, and from those 29 also drank alcohol. This suggests a
strong link between the risk factors of smoking and alcohol with tongue cancer. Alcohol
on its own seems not be a strong contributory factor, but its synergistic affect with
smoking is now widely accepted. Only 8 tongue cancer patients had the habit of chewing.
Paan chewing is generally associated with buccal mucosa cancers. Our results also show a
strong association between paan chewing as a habit and cancer of the buccal mucosa,
with 18 out of the 35 patients having the habit. This can be explained by the fact that the
paan is held in the buccal sulcus for an extensive period of time, so allowing the
carcinogens to act on the buccal mucosa more so than other regions of the oral cavity.
For the remaining 48% of the tongue cancer patients, who did not present with any risk
factors, alternative aetiological factors, if any, need to be proposed. This may suggest that
risk factor for these cancers may be different from that of other head and neck sub-sites.
Diverse risk factors other than tobacco, which could reflect changes in diet, nutritional
habits, food processing, sexual habits, need to be investigated for this subsite. In a study
by Shiboski et al in 2005, a paralleled increasing trend in tonsillar and tongue cancers was
found, against a general decline of other oral cavity cancers. Knowing that the association
between human papillomavirus (HPV) infection and tonsillar carcinoma is now well
established, this led to the suggestion that there may be a link between HPV and tongue
cancer (Shiboski 2005). However, a more recent study by Pintos et al concluded that this
aetiologic link is less clear for non-tonsillar oral cancers (Pintos 2008).

50
Diet, in terms of cancer prevention, has much ongoing research. The general consensus is
that the anti-oxidants available in fresh fruits and vegetables play a significant role in
protecting against cancer. These include vitamin C, vitamin E, carotenoids, and many
other phytochemicals. Little has been suggested regarding any particular dietary
ingredients that may be cancer causing. Those ingredients that have been suggested are
linked to cancers elsewhere in the body, for example high doses of soya and the increased
risk of estrogen-responsive cancers, such as breast or endometrial cancer. Any dietary
factors (other than paan, tobacco and alcohol) that may be associated with oral cavity
cancers are still to be found.
This was not a case-control study, but instead a study in which one cancer was compared
to a group of others. Carrying out this study with a control group of patients with the
same risk factors but not suffering from cancer may have resulted in a p value that would
have suggested a significant relationship. Hence, this study can be improved upon if it
were to be conducted prospectively, looking into the detailed dietary history of all
patients who present with oral cavity cancers, in an attempt to find a common ingredient
that could be proposed as a possible alternative aetiological factor in tongue cancer. Such
a study can then be expanded upon by investigating treatment outcomes and follow-up
details of each patient to find out whether there is any significant difference in the
prognosis of tongue cancer patients with and without risk factors.
3.8 Conclusion
A trend is emerging showing that the type of oral cancers that patients present with are
changing, with a definite increase in the number of patients presenting with tongue
cancer. We are also seeing that a considerable number of these patients are presenting
without the known associated risk factors. However, what might be causing these cancers
is still to be proven, with HPV and dietary factors being at the forefront of alternative
aetiological factors.