Embed Size (px)
Citation preview
Epidemiological evidence for a protective role for statins in
Community Acquired Pneumonia
British Thoracic Society Winter Meeting 2012 , London
Yana Vinogradova
Background
• Statins – common medications, 24% in 45+ age group.
• CAP – common infection, 230 per 100,000 person-years, 670 for 60+ age group.
• Evidence from lab data that statins may benefit in cases of infectious diseases

Figure Legend:
Pleiotropic effects of statins. eNOS = endothelial nitric oxide synthase; PAI-1 = plasminogen activator inhibitor-1; NADPH = nicotinamide adenine dinucleotide phosphate hydrogen;
MCP1 = monocytic chemoattractant protein 1; TNF = tumor necrosis factor; LFA-1 = lymphocyte function-associated antigen-1.
From: Does Statin Use Improve Pneumonia Outcomes?
Chopra, Flanders, CHEST. 2009;136(5):1381-1388. doi:10.1378/chest.09-0941

Pharmacoepidemiology
and Prescription Kwok et al. Eur J Clin Pharmacol (2012) 68, 747-755
Fig. 3 Meta-analysis of adjusted risk of pneumonia with statin therapy
From: Statins and associated risk of pneumonia: a systematic review and meta-
analysis of observational studies

• QResearch– 660 GP practices
• Currently largest database in the UK
• 537 UK practices• > 6 practices in every SHA• > 9 million patients including
those who died, left and still registered
• > 30 million person years of observation
Patient level data
from GP clinical records
Anonymised
Longitudinal data for 20+ years
Validated externally and internally
Industry independent

Methods: Study design and analysis
• Nested case control study• Study period Jan 1996-Dec 2005 • Cases were incident CAP patients• 5 controls matched by age, sex, practice• analysis restricted to subjects with at least 2 years
of prescribing data• Conditional logistic regression, odds ratios 95%CI

Methods: Assessment of Exposure• use:
at least 2 scripts in 12 months prior to the index date• different types of statins
atorvastatin pravastatin cerivastatinsimvastatin fluvastatin rosuvastatin
• time before the index date: 28 days29-89 days90-365 days

Methods: Confounding factors
•Socio-economic status
•Townsend quintiles
•Smoking status
•Non-smoker
•Smoker
•not recorded
•Vaccinations
•Influenza
•pneumococcal
•Morbidities
•List of co-morbidities recommended
for pneumococcal vaccination
•Additional co-morbidities limiting
mobility or suppressing immune
system
•Medications
•Acid-lowering drugs

Results: Sample and statin use in the last year
17,757 cases
with 2 years of medical records
2231 cases (12.6%) statin users
80,484 controls with 2 years of
medical records
8759 controls (10.9%) statin
users
0
5
10
15
20
25
%
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005Index year
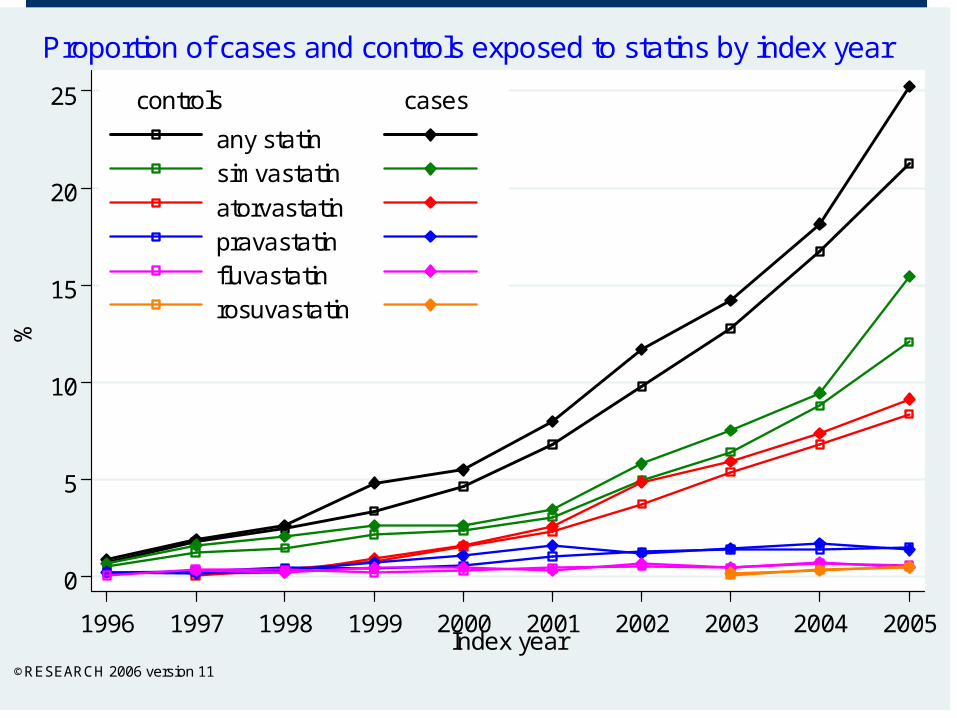
any statin simvastatin
atorvastatin pravastatin fluvastatin rosuvastatin
controls cases
©RESEARCH 2006 version 11
Proportion of cases and controls exposed to statins by index year

0
200
400
600
800
1000
1200
1400
1600
rate
pe
r 1
00.0
00 p
opul
atio
n/ y
ear
45- 50- 55- 60- 65- 70- 75- 80- 85- 90+Age groups
Men Women
©QRESEARCH 2006 version 11
Pneumonia episode rates by age and gender in 2005

0
5
10
15
20
25
45 50 55 60 65 70 75 80 85 90 95 45 50 55 60 65 70 75 80 85 90 95
Women Men
cases controls
%
Age at index date
©RESEARCH 2006 version 11
Proportion of cases and controls exposed to statinsby age and sex
Crude OR, 95%CI 1.23, 1.13 – 1.33 Crude OR, 95%CI 1.25, 1.16 – 1.34

0
5
10
15
20
45 50 55 60 65 70 75 80 85 90 95 45 50 55 60 65 70 75 80 85 90 95
cases controls
3 to 12 months
1 to 3 monthsup to 28 days
%
Age at index date
©QRESEARCH 2006 version 11
Last use of statin before the index date
Crude OR, 95%CI
1.27, 1.20 – 1.34
1.14, 1.08 – 1.20
1.03, 0.98 – 1.09
13%
55%
11%
9%
37%30%
62%
7%

0
1
2
3
4
5
6
7
8
%
cases controls
28days29-89days
90-365days28days
29-89days90-365days
©QRESEARCH 2006 version 11
Proportion of cases and controls and number of prescriptionsby the last prescription time
2-67-12
12+
Number ofprescriptions
69%
63%
48%
70%
60%
38%

0
10
20
30
40
50
60
45 50 55 60 65 70 75 80 85 90 95 45 50 55 60 65 70 75 80 85 90 95
cases controls
not on statinon statin
%
Age at index date
©QRESEARCH 2006 version 11
Proportion of cases and controls with heart disease and strokeand their use of statin
CHD and stroke
Crude OR, 95%CI
2.18, 2.10 – 2.27
Statin use, OR, 95%CI
Crude 1.24, 1.18 – 1.31
Adjusted 0.81, 0.77 – 0.86
37%23%
26% 31%

3 months ago (190) 0.89 (0.75 to 1.06)
1 to 3 months (819) 0.97 (0.88 to 1.06)
in 28 days (1222) 0.68 (0.63 to 0.73)
by time of use
overall use (2231) 0.78 (0.74 to 0.83)
Last year use (N of cases) OR (95%CI)
.5 .75 1 1.25Odds ratios are adjusted for co-morbidities, deprivation, smoking status,acid lowering drugs and influenza and pneumococcal vaccinations©QRESEARCH 2006 version 11
OR and 95%CIRisk of pneumonia and use of statin in the last year
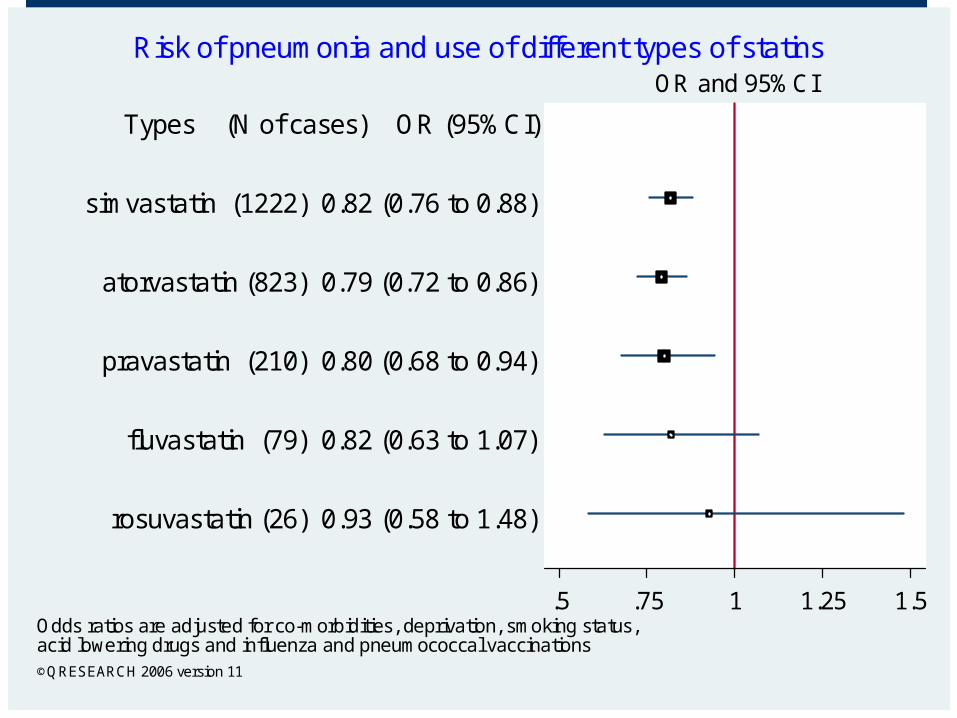
rosuvastatin (26) 0.93 (0.58 to 1.48)
fluvastatin (79) 0.82 (0.63 to 1.07)
pravastatin (210) 0.80 (0.68 to 0.94)
atorvastatin (823) 0.79 (0.72 to 0.86)
simvastatin (1222) 0.82 (0.76 to 0.88)
Types (N of cases) OR (95%CI)
.5 .75 1 1.25 1.5Odds ratios are adjusted for co-morbidities, deprivation, smoking status,acid lowering drugs and influenza and pneumococcal vaccinations©QRESEARCH 2006 version 11
OR and 95%CIRisk of pneumonia and use of different types of statins

3 months ago (37) 0.88 (0.60 to 1.30)
1 to 3 months (70) 1.06 (0.79 to 1.41)
in 28 days (103) 0.65 (0.52 to 0.82)
pravastatin
3 months ago (99) 0.98 (0.78 to 1.25)
1 to 3 months (292) 0.89 (0.77 to 1.02)
in 28 days (432) 0.70 (0.62 to 0.78)
atorvastatin
3 months ago (131) 0.86 (0.70 to 1.06)
1 to 3 months (442) 1.02 (0.91 to 1.15)
in 28 days (649) 0.70 (0.63 to 0.77)
simvastatin
Last use (N of cases) OR (95%CI)
.5 .75 1 1.25 1.5Odds ratios are adjusted for co-morbidities, deprivation, smoking status,acid lowering drugs and influenza and pneumococcal vaccinations©QRESEARCH 2006 version 11
OR and 95%CIRisk of pneumonia and use of most common types of statin

Limitations
• Residual confounding as no information – on X-ray– on microbiological tests– on severity of pneumonia
• Information on prescriptions only
• Over-the-counter statin use
• Missing data
Strengths
• Large sample size and representative population
• Data electronically collected – unlikely misclassification bias
• Data collected before diagnosis – no recall bias
• All cases used – no selection bias


Further research
•RCT in 26 countries
•Randomisation in 2003-2006, last visit in 2008
•17802 participants with no history of CVD and diabetes
•Rosuvastatin 20mg or placebo
•Incidence of infections during the trial

Figure 2:
Kaplan–Meier estimates from intention-to-treat analysis showing cumulative incidence of first pneumonia adjusted for competing risk of cardiovascular events. Participants
were censored at the time of a cardiovascular event.
HR (95%CI) 1st
CAP 0.81 (0.67 – 1.97)

Further research
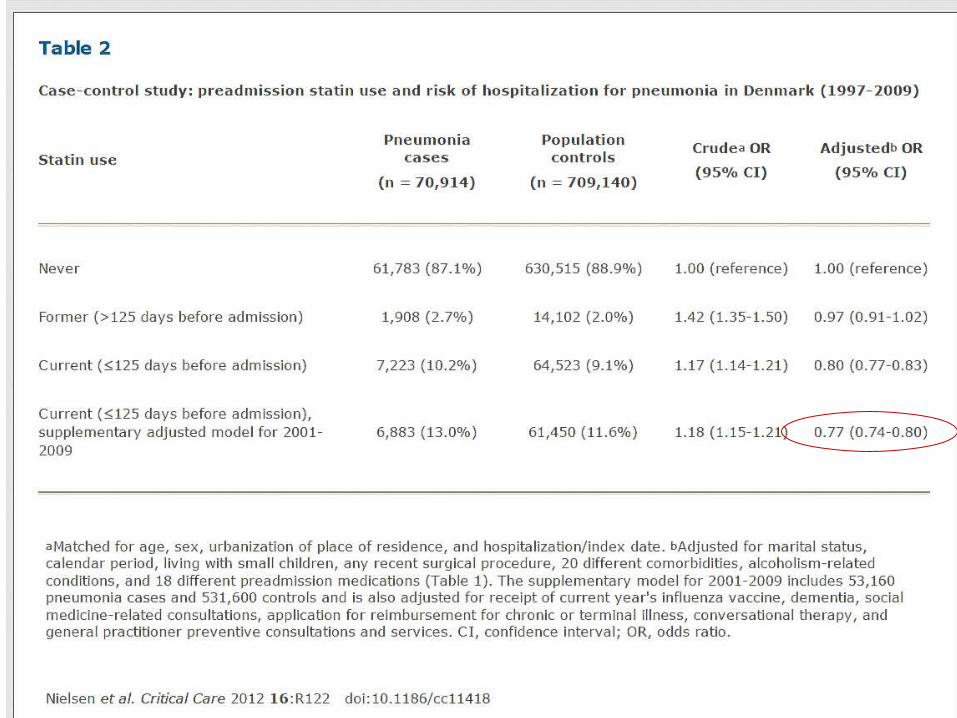
• Danish National Registry• 1997-2009, additional analysis for 2001-2009• 70,914 patients hospitalised with pneumonia• Matched to up to 10 controls• Current statin use: at least 1 prescription in last 125 days• Adjusted for co-morbidities, medications, smoking, demographics...

Conclusions
There is an association between use of statins and decreased risk of pneumonia, more pronounced for patients having recent statin use.• It may be due to anti-inflammatory and
immunomodulatory properties of statins• It may also be due to reduced rate of CVD
events and rates of associated complication such as pneumonia
Thank you
Questions?