-
Epidemiology of gastric and duodenal ulcers
Sarah Bowman
April 2008
-
What is an ulcer?
Acid breaks through protective substances on gut wall Duodenum (1st
part small intestine) most common site Gastric ulcers in stomach
Pain, bloating, nausea, fullness, weight loss, tiredness
Complications: bleeding, perforation, obstruction
The duodenum is the first part of the small intestine, through
which hydrochloric acid and pepsin flow to help digest food (1, 2).
The duodenum makes chemicals (bicarbonate), mucus and
prostaglandins which cover the inside lining and protect it from
acid. Mucosal blood flow is also protective (3). An ulcer occurs
where the acid breaks through the protection, not by
over-production of acid (1). The duodenum is the most common site
for a peptic ulcer - gastric ulcers are those occurring in the
stomach (1).
Symptoms
Pain in the upper abdomen just below the sternum (breastbone) is
the common symptom. It comes and goes and may occur mostly before
meals. It may be eased on eating food, or taking antacid medicines
(1)
Other symptoms may include: bloating, retching, nausea,
particular 'fullness' after meals, food, weight loss and tiredness
(2).
Complications develop in a small number of cases, but can be
serious. These include:
Bleeding from the ulcer. Can range from a 'trickle' to a
life-threatening bleed (1).
Perforation - the ulcer goes right through the wall of the
duodenum. Food and acid in the duodenum leak into the abdominal
cavity causing severe pain. This is a medical emergency. (1)
Narrowing and obstruction
Ulcers located at the end of the stomach where the duodenum is
attached, can cause swelling and scarring which can narrow / close
the intestinal opening. This obstruction can prevent food from
leaving the stomach and entering the small intestine, resulting in
vomiting (2)
-
Diagnosis
Endoscopy (>55yrs, first time). Capture all cases?Faecal /
breath tests for H. pyloriGI series (rare)
False positive tests
Missed cases? risk of transmission / disease progression
Tests
Endoscopy (1). The NICE guidelines on Management of Dyspepsia in
Adults states endoscopy is not required unless the patient is
presenting for the first time above the age of 55 or unless there
are other warning signs e.g. GI bleeding, dysphagia, unintentional
weight loss, abdominal swelling and persistent vomiting" (3). There
is a risk associated with endoscopy.
Faecal / breath tests for the H. pylori bacterium or from a
biopsy sample taken during endoscopy (1)
A GI series (X-ray through swallowing barium) (2) (now v. rare
(3)
There is a high frequency of false positive tests (14).
Cases may be missed if latent in the system for some time, and
patient is asymptomatic / does not present. Particularly if faecal
test does not detect bacteria but endoscopy not indicated
(according to NICE)???
-
Why are they important?
HPA infectious disease but main effects are from chronic
burdenPotential medical emergencyChronic symptoms health and
economic costsH. pylori also linked to:Functional dypepsiaCancer
(2-6x more likely, though still rare)Differential clinical outcome
- interaction between bacterial properties (phenotypic variation),
genetics and environmental / behavioural factors
Complications can be dangerous. Costs to the patient and the
health service result.
Chronic symptoms costs to individuals health and wellbeing;
economic costs in sickness absence
Other problems of having H. pylori:
Functional dyspepsia (4)
H. pylori is sometimes found in people with recurrent bouts of
indigestion (dyspepsia) not caused by an ulcer or inflammation.
Cancer (4)
The risk of developing stomach cancer is thought to be slightly
increased with long-term infection with H. pylori. However >25%
of people in the UK become infected with H. pylori, and the vast
majority do not get stomach cancer. Risk may be greater if person
has H. pylori in addition to having a first degree relative
diagnosed with stomach cancer.
Interventions may influence clinical outcome of infection. Some
evidence exists for phenotypic variation in H. pylori bacteria,
which may enable development of screening for bad bacteria in
future, though this is not yet sufficiently understood (5).
-
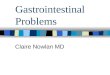
Emergency admission for perforation
Rates per million resident population. Three-year moving
averages
Implications for care of older people
(Bardhan et al. 2004, Digestive & Liver Disease 36(9),
577-588)
Rates are: higher for duodenal ulcer; higher with age.
-
Causes?
Ulcers are only found in white people, usually in long thin
types given to worry and irritability (Robinson & Bruce
1940)
-
Causes & Risk Factors
Helicobacter pylori 90% duodenal ulcers70-75% gastric
ulcersNSAIDsLifestyle factors increase risk smoking, physical
stress, salt (GU)Genetic susceptibility / protection against H.
pylori infection (twin studies, mouse
models)RarelyZollinger-Ellison syndrome & others
Causes
Infection with H. pylori (1) in 90% of duodenal cases. The
bacterium affects the duodenal lining by producing substances that
weaken the protective mucus and produce more acid (2). H. pylori
causes 70-75% of gastric ulcers (2, 3).
Anti-inflammatory medicines (NSAIDs non-steroidal
anti-inflammatory drugs) taken for joint pain, etc. e.g. aspirin
and ibuprofen sometimes affect the duodenal lining (1). Patients
taking NSAIDs have 2 to 4 times the risk of ulceration if H. pylori
is positive. Testing patients for H pylori and eradication before
starting NSAIDs reduces the incidence of ulcers (3).
Lifestyle factors: smoking, stress, and drinking heavily may
increase risk. However, these are not the underlying cause of
ulcers (1). Smoking increases the chances of getting an ulcer,
slows the healing process of existing ulcers and contributes to
ulcer recurrence (2). Caffeine seems to stimulate acid secretion in
the stomach, which can aggravate the pain of an existing ulcer.
However, the stimulation of stomach acid cannot be attributed
solely to caffeine (2). Although no proven link has been found
between alcohol consumption and peptic ulcers, ulcers are more
common in people who have cirrhosis of the liver, a disease often
linked to heavy alcohol consumption (2). Although emotional stress
is no longer thought to be a cause of ulcers, people with ulcers
often report that emotional stress increases ulcer pain. Physical
stress, however, may increase the risk of developing ulcers,
particularly in the stomach. For example, people with injuries such
as severe burns and people undergoing major surgery often require
rigorous treatment to prevent ulcers and ulcer complications (2).
High salt is implicated in GU (7).
Genetic:
Traditional family and twin studies have shown that concordance
for H. pylori infection and duodenal ulcer is more common in
monozygotic (identical) twins than in dizygotic (non-identical)
twins (26, 27 in 7]. One study calculated the inherited component
to be greater than the environmental component (27 in 7).
The second line of evidence is factors known to be genetically
determined have been shown to be associated with disease. For
example individuals with blood group O have a higher risk of
duodenal ulcer, while blood group A is more common in those with
gastric cancer (7). Some specific disease associations with HLA
type have also been identified (7).
The third line of evidence is extremely convincing and comes
from mouse models. Researchers have found the whole spectrum of
possible conditions (including various degrees of gastritis,
ulcers, cancer and lymphoma) can be produced by infecting
genetically different mice with the same strain of Helicobacter
felis (7). Preliminary evidence suggests that a variety of genes
involved in the inflammatory response affect the likelihood of
Hpylori infection progressing to duodenal ulcer disease (5).
Rare causes e.g. Zollinger-Ellison syndrome where more acid than
usual is made by the stomach (1). Other rare causes include Crohns
disease, gastric secreting tumours, hypergastinaemia, idiopathic
gastrinoma and hyperparathyroidism (5).
-
Treatment & Outcome (NICE)
10% cases fail treatment (HPA)1 course of combination therapy
clears most cases (74% duodenal ulcers)Relapse greater for gastric
ulcers (affected by lifestyle factors). At 3-12 months:Duodenal
ulcers: 39% clear (acid suppression only); 91% (combination
therapy)Gastric ulcers: 45% clear (acid suppression only); 77%
(combination therapy)
Treatment
H. pylori is the cause
Combination therapy: two antibiotics and an anti-acid medicine
to allow the antibiotics to function. One course of therapy clears
infection in up to 90% cases. Further tests may be done after a
course of combination therapy if: symptoms do not go, or if they
return; there is a complication e.g. perforation. Rarely surgery
may be considered in cases not responding to treatment or
developing complications (2). Anti-acid treatments only common
since 1970s and 1980s (8).
NSAIDs are the cause
Stop the anti-inflammatory medicine. Where this is not possible,
take acid-suppressing medicine daily (1).
Lifestyle modification
No need for "ulcer diets" since the introduction of effective
acid suppression but reduction of alcohol intake, coffee and spicy
foods may be needed. Smoking cessation is advised. The new COX2
inhibitors are less likely to cause ulcers than NSAIDs but it is
dangerous to assume they have no risk. This advantage is nullified
if the patient also takes even low dose aspirin (3).
Effectiveness of interventions
Effectiveness is important because it has an impact on
prevalence and disease burden. NICE guidelines give the following
data (3):
In duodenal ulcer, acid suppression for 4 to 8 weeks produces
healing of the ulcer in 69%. This rises by an extra 5.4% with
eradication therapy. NNT=18.
In duodenal ulcer relapse at 3 to 12 months after treatment is
39% after short term acid suppression alone but eradication
increases this by 52% to 91%. NNT=2.
In gastric ulcer, supplementation of acid suppression with
eradication therapy does not improve healing rates but it does
reduce relapse so that 3 to 12 months later 45% are free of ulcers
after just acid suppression but eradication raises this by 32% to
77%. NNT=3.
In patients taking NSAIDs, eradication did not improve ulcer
healing rate but it did halve the number of endoscopically proven
ulcers 6 months later from 18 to 9%.
The recurrence rate was significantly higher in gastric ulcer.
Recurrence rates of patients who smoked, consumed alcohol, and used
NSAIDs were significantly higher in those with gastric ulcer
recurrence compared to duodenal ulcer. Relapsed ulcers tended to
recur at the same or adjacent sites as the previous ulcers (3).
Mass eradication of Hpylori is impractical because of the cost and
the danger of generating antibiotic resistance, so we need to know
how to target prophylaxis. (5)
-
Consequences
Primary care GP consultations, drug costs (increasing
resistance)Secondary care complications, surgeryTertiary care
rarely neededSocio-economic cost: Standardised average annual years
of life lost (up to age 75) = 2.6 (per 10,000) (Females=1.8;
Males=3.5) (1999 & 2001 pooled data, ONS)
High persistent morbidity. Burden is on primary care. Resistance
to metronidazole occurs in approximately 50% of infected
individuals in many European countries with significantly higher
levels of up to 90% in developing countries. Resistance to
clarithromycin is currently less common with levels below 10% in
many European countries although there is evidence that rates may
be increasing. Significantly, a recent meta-analysis has shown that
pretreatment resistance to clarithromycin can reduce the
effectiveness of therapy by 55%.
Socio-economic cost work days lost; discomfort and pain; quality
of life / disability. HTA (2003) did not estimate cost per QALY.
USA analysis (in NICE guidance) found significant cost-savings from
a societal perspective on treatment more so for DU than GU.
-
Consequences
Mass eradication of Hpylori is impractical because ofgenerating
antibiotic resistance, so we need to know how to target
prophylaxis. (Calam & Baron 2001)Ulcers occurring in absence of
H. pylori or NSAIDs / aspirin. Combination therapies less effective
in absence of H. pylori data neededScreening? Cost-effective
cost/LYS < 10,000 over 80yrs. But effects of eradication on
morbidity / mortality?
Bardhan et al. (2004): Ulcers occurring in absence of H. pylori
or NSAIDs / aspirin. Combination therapies less effective in
absence of H. pylori data needed. Implications for services as
ulcer surgery no longer practiced.
Screening
Roderick et al. (2003): HTA. Population screening H. pylori
cost-effective: cost/LYS < 10,000 over 80yrs. Once-only
screening at age 40
Major uncertainty re: effect of H.pylori eradication on gastric
cancer and complicated ulceration risk; and antibiotic resistance.
Favourable comparison with other screening programmes. Long follow
up period therefore more evidence needed before can be recommended.
The cost-effectiveness of screening would be reduced if extensive
opportunistic screening of all dyspeptic patients presenting in
primary care
-
Time, Person, Place
-
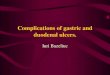
Barron & Sonnenberg (2002)
UK Incidence & Prevalence (Time)
Increases due to:
Increase in H.pylori? Different strain of H. pylori? Another
concurrent gut infection?
But what about differing temporal changes of CU and DU and
between men and women?
Graph shows admissions for gastric (GU) and duodenal (DU)
ulcers, and dyspepsia in all 12 London hospitals associated with a
medical school. Gastric ulcer, duodenal ulcer, and dyspepsia
(including indigestion, gastralgia, and gastritis) are presented as
mean rates per 10, 000 admission in each five year period. To
further smooth out missing time periods and various lengths of data
availability from individual hospitals, the data were plotted as
the moving average of three consecutive time periods.
Peptic ulcer disease was comparatively rare until the
mid-nineteenth century following which its incidence rose steadily,
peaking 1940-1960. Since then there has been a slight decline,
particularly in gastric ulcer (7).
These increases in peptic ulcer in the 19th century have been
attributed to a postulated increase in an (cross) infectious
disease (H pylori) in childhood, spread perhaps by the overcrowding
and poor sanitation of early urbanisation. Or there may have been a
new and more pathogenic strain of H pylori, a change in host
susceptibility, or even a concurrent enteric infection modulating
gastric inflammation and immune responses. However, these
suggestions remain as yet untestable hypotheses, and do not explain
the temporal changes in gastric versus duodenal ulcer and men
versus women described (9).
-
UK Incidence & Prevalence (Time)
Evidence of cohort effect 1970-1986: (Primatesta et al.
1994)
Decreased hospitalized morbidity and mortalityRelated more to
changes in risk factors (e.g. smoking) in different cohorts than
new pharmacological treatments? - implications for public health!
OR: Genetic factors may be more important (Malaty et al.
1994)
-
UK Incidence & Prevalence (Person)
H. pylori infection
Incidence: 1-3% of adults p.a. (HPA)Prevalence infection: 40%
population (HPA: >50% of 50+yr olds)
Ulceration
Incidence: DU in 30-50yrs old; higher incidence in men GU in
>60yr olds; higher incidence in womenLow prevalence in younger
age groupsDuodenal ulcer: up to 10% of population
In the UK around 40% of the population are infected and the
possible clinical outcomes of this infection are diverse. The
majority of individuals will have no symptoms and will not develop
any related problems throughout their lives (7). 1% of the 40% will
have an endoscopy and 13% of those will have ulcer disease
annually.
There are differential outcomes, which are incompletely
understood:
- Ulcers are rare among teenagers and children (2)
- Duodenal ulcers usually first occur between the ages of 30 and
50 (2)
- Duodenal ulcers occur more frequently in men than women
(2)
- Stomach ulcers are more likely to develop in people over age
60 (2)
- Stomach ulcers develop more often in women than men (2)
-
UK Incidence & Prevalence (Person)
Current trends:
Annual age-standardized period prevalence decreased 1994-1998,
particularly deprived areas (men 3.3/1000 - 1.5/1000; women
1.8/1000 - 0.9/1000)Sex incidence evening out decreasing incidence
in young men; increasing in older womenBut emergency admission
rates for complications unchanged in last 30yrs Kang et al. (2006)
increase in case fatality for DU. Due to concomitant comorbidity /
increasing ulceration (NSAIDs) / H.pylori (i.e. changing natural
history)?Future decrease in prevalence?
Frequency decreasing (H. pylori decreasing), particularly in
deprived areas
Increase in older women could be due to increased use of NSAIDs
(non-steroidal anti-inflammatory drugs). Reason for little change
in emergency admissions could be increase in use of aspirin and
anti-coagulants, especially in older people Scottish data showed
many admissions are for bleeding (8 Kang et al. 2006; 11)
More research needed re: potential changing natural history of
ulceration.
Future decreasing prevalence? Current older cohorts were
children when H. pylori was more common and are also now at an age
where they are exposed to more NSAIDs and anti-platelet drugs.
Additive effect could mean higher prevalence of ulcers in that
cohort and high rates of complications (bleeding) (15).
-
International prevalence (Place)
Rates infection higher in less developed countries. Quite large
variation.
-
Place
Worldwide. Prevalence 100% in developing countriesPotential for
re-spread in UK through travel?H. pylori - oral / faeco-oral
transmission associated with poverty / overcrowding in
childhoodIncreased prevalence in children with history of ulcer in
the mothers due to common environmental factors?Variation between
ethnic groups even within countries
Precise mode of transmission of H.pylori unknown
Clustering?: study by Brenner et al. (1998) (6)
Variation between ethnic groups (14)
-
Place Regional variation (NCHOD)
2004-06 pooled data from ONSSMRDirectly standardised age specific
death rates (per 100,000 European standard population) - regional
centres higher than national average High rates affected by
lifestyle factors & e.g. aspirin in deprived areas (raised CVD
risk)? Lowest = E. Midlands (89). Highest = London (112) Industrial
areas = 114, London suburbs = 111, London cosmopolitain = 153
E&W
NE
All
Males
Females
99 (97-101)
100 (97-103)
99 (96-101)
111 (102-121)
124 (110-139)
100 (88-113)
NCHOD = National Centre for Health Outcomes Development
2004-06 pooled data all age groups: age specific death rates
(per 100,000) = 6.2 (E&W) (females =6.5; males = 6.0). NE (GONE
/ SHA)= 7.0 (males 7.6; females 6.4). Centres with industry 6.4
(thriving London periphery 5.3); industrial hinterland 6.8; coastal
& countryside 8.4; regional centres 6.7. High due to older
popn? Age- specific data for age bands removed for anonymity due to
small numbers.
Directly standardised all age groups: age specific death rates
(per 100,000 European standard population) = 3.88 (CI 3.80 3.96)
(E&W) (males=4.70, CI=4.56-4.83; females=3.18, CI=3.08-3.27).
GONE / NE SHA= 4.44 (CI=4.05-4.84); males=5.81 (CI=5.11-6.50);
females=3.35 (CI=2.90-3.79). Centres with industry 4.68 (thriving
London periphery 3.68); industrial hinterland 4.33; coastal &
countryside 3.69; regional centres 4.29. Industrial centres /
hinterland associated. Fit with effect of lifestyle factors and use
of e.g. aspirin due to raised risk CVD in deprived areas? London
cosmopolitain=6.25! Highest. Why?
Indirectly standardised: SMR (2004-2006 pooled). E&W=99
(97-101) males =100 (97-103), females=99 (96-101). NE=111 (102-121)
(males=124 (110-139), females=100 (88-113)). Lowest = E. Midlands
(89). Only 1 higher London +112. Industrial areas come out badly
(114) but London suburbs 111 and London cosmopolitain=153!!
-
NCHOD data - critique
Based on original underlying cause of death (death
certification)Numerator - mortality data 1993-2006 (ONS) with codes
assigned using postcode of usual residenceChanges to coding causes
of death in England & Wales. Data based on new coding
Denominator data - latest revisions of ONS mid-year population
estimates, current at Oct 2007 - quite accurateNCHOD regularly
updated
-Death certificate problems particularly if older people with
co-morbidities
- Comments on numerator data - Mortality data for years
1993-2006 were extracted by ONS in June 2007 with organisational
codes assigned using the postcode of usual residence and the
November 2006 edition of the National Statistics Postcode
Directory
- In January 2001, the ONS implemented a change from ICD-9 to
ICD-10 for coding causes of death in England & Wales. As part
of an exercise to investigate the effects of this change, the ONS
also re-coded all deaths registered in 1999. Deaths for years prior
to 1999 and for year 2000 have not been re-coded.
For current analysis, therefore, all data are based on ICD-10.
- Denominator data based on latest revisions of ONS mid-year
population estimates for respective years, current as at Oct 2007.
So quite accurate
- NCHOD regularly updated
-
Data sources
Other potential sources: HES, primary care records, prescribing
database
Data
sourceValid?Reliable?Complete?Timely?Accessible?Relevant?Cochrane
reviews (RCTs / meta-analyses) (RCTs / meta-analyses) Treatment
focus PartialPubMed articles Some small studies Some small studies
Epidemiol focus NEPHO ONS data ONS data Regional life years lost
data London only 1999 & 2001
-
Data sources
Data sourceValid?Reliable?Complete?Timely?Accessible?Relevant?NCHOD
ONS data. Updated though based on death certification ONS data.
Updated though based on death certification Age-specific rates not
split by sex (small numbers) Updated 2007 NEPHO website HPA Based
on reporting from primary care Testing & trend monitoring. No
routine publications
-
Data sources
Data
sourceValid?Reliable?Complete?Timely?Accessible?Relevant?Patient UK
NICE guidance & review articles. Written by clinicians.
Reviewed 18monthly NICE guidance & review articles. Written by
clinicians. Reviewed 18monthly Patient info. Based on recent
guidance & articles Patient Plus Peer reviewed. Based on NICE
guidance & review articles. Written by clinicians. Peer
reviewed. Based on NICE guidance & review articles. Written by
clinicians. Clinical focus diagnosis and management Based on recent
guidance & articles Partial
-
Conclusion
Disease mechanism / transmission poorly understoodRisk factors
multiple & interactingH. pylori is main cause but has changing
natural historyEach generation has carried its own particular risk
of bearing ulcers throughout adult life (Susser & Stein
1962)Current pattern = exposure to H. pylori + genetics + exposure
to drugs + environmental / behavioural factorsDU / GU likely to
continue causing significant chronic disease burden and personal /
societal cost. Predicting future pattern difficult
-
Questions?
References
Bardhan, K. D., Williamson, M., Royston, C., Lyon, C. (2004)
Admission rates for peptic ulcer in the Trent Region, UK,
1972-2000: Changing pattern, a changing disease? Digestive and
Liver Disease, 36, 577-588
Barron & Sonnenberg, Gut (2002), 50(4), 568-570
Malaty, H., Engstrand, L., Pederson, N., Graham, D. (1994),
"Helicobacter pylori infection genetic and environmental
influences, a study of twins", Annals of Internal Medicine, Vol.
120 pp.982-6
Primatesta et al. (1994), Int. J. Epidemiol. 23(6),
1206-1217
Robinson, S.C., Bruce, R.M. (1940), "The body build of the ulcer
patient", American Journal of Digestive Diseases, Vol. 7
Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Patel P.
The cost-effectiveness of screening for Helicobacter pylori to
reduce mortality and morbidity from gastric cancer and peptic ulcer
disease: a discrete-event simulation model. Health Technol Assess,
2003;7(6). Available at:
http://www.cinahl.com/cexpress/hta/summ/summ706.pdf
-
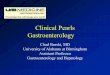
Bardhan et al. 2004
Elective surgery. Rates per million resident population. Three-year
moving averages.
The number of elective anti-ulcer operations has declined, and more
markedly so for DU. The greatest decline for both groups was in
younger men, 3564 years, in whom such operations were most commonly
performed (Fig. 4). The rate of decline, however, was no greater in
the era of modern medical treatment (Table 3).