Embed Size (px)
Citation preview
Epidemiology of Malaria
BY:
Hamad AldosariAwn AlqarniKhalid Alshahrani Fahad Alotaibi Abdullah Alenezi
OBJECTIVES:
Magnitude of Malaria; prevalence of the health problem Globally and in KSA.
To describe the disease pattern and trends. (person, place and time).
identify the risk factors and high risk groups.
Describe the process of communicable diseases transmission (Agent, Reservoir, Mode of transmission).
Identify the main methods for prevention and control.
Recognize the specific programs for prevention and control of Malaria in KSA.
Magnitude of malaria
The current and potential future impact of climate change on malaria is of major public health interest. The proposed effects of rising global temperatures on the future spread and intensification of the disease, and on existing malaria morbidity and mortality rates, substantively influence global health policy.
Global Prevalence of Malaria
According to the latest estimates, released in December 2013, there were about 207 million cases of malaria in 2012 and an estimated 627 000 deaths.
Malaria mortality rates have fallen by 42% globally since 2000, and by 49% in the WHO African Region.
Most deaths occur among children living in Africa where a child dies every minute from malaria. Malaria mortality rates among children in Africa have been reduced by an estimated 54% since 2000.
Estimated annual expenditure on malaria research and treatment: US$84million / year.
Malaria kills more people than AIDS
Malaria kills in one year what AIDS kills in 15 years.
For every death due to HIV/AIDS there are about 50 deaths due to malaria.
To add to the problem is there increasing drug resistance to the established drug.
Continues to be most important cause of fever and morbidity in the world.
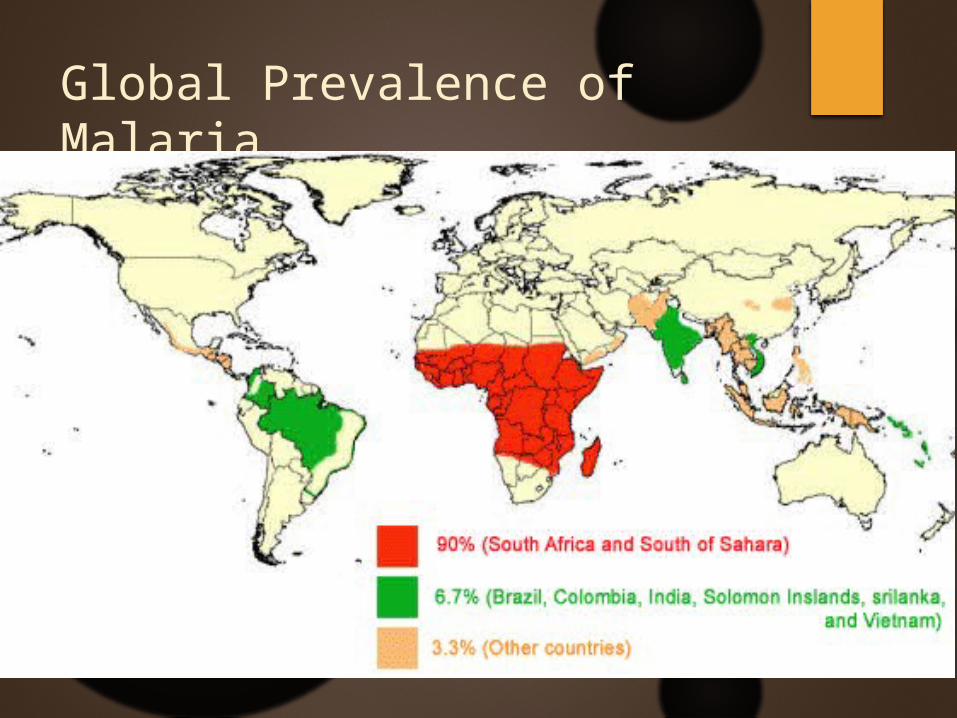
Global Prevalence of Malaria

Global Prevalence of Malaria
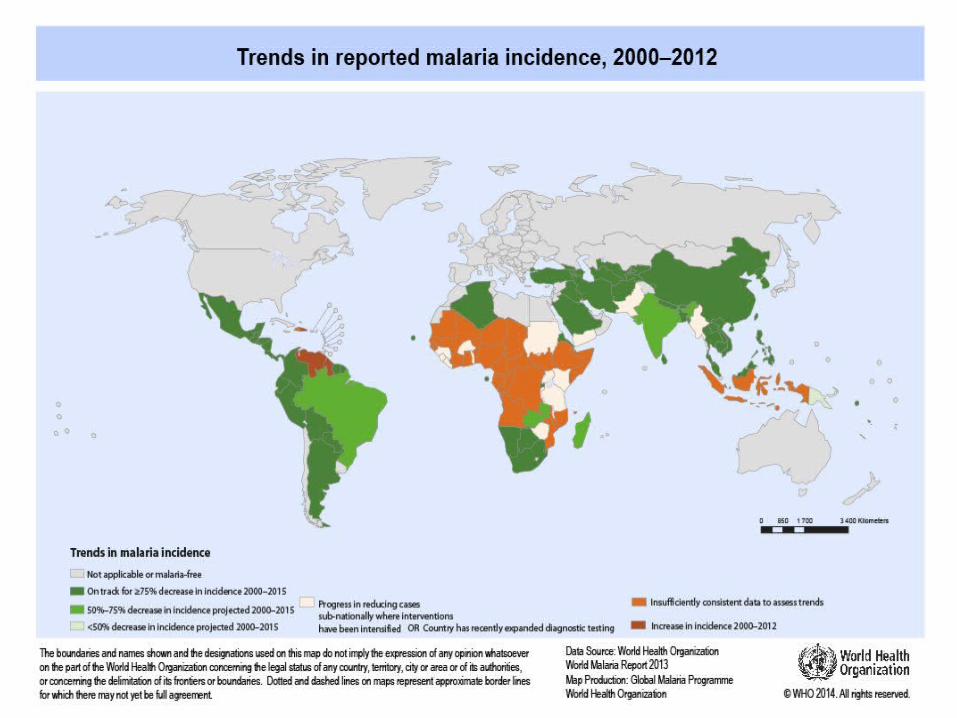
Since 2000, a tremendous expansion in the financing and coverage of malaria control programs has led to a wide-scale reduction in malaria incidence and mortality.
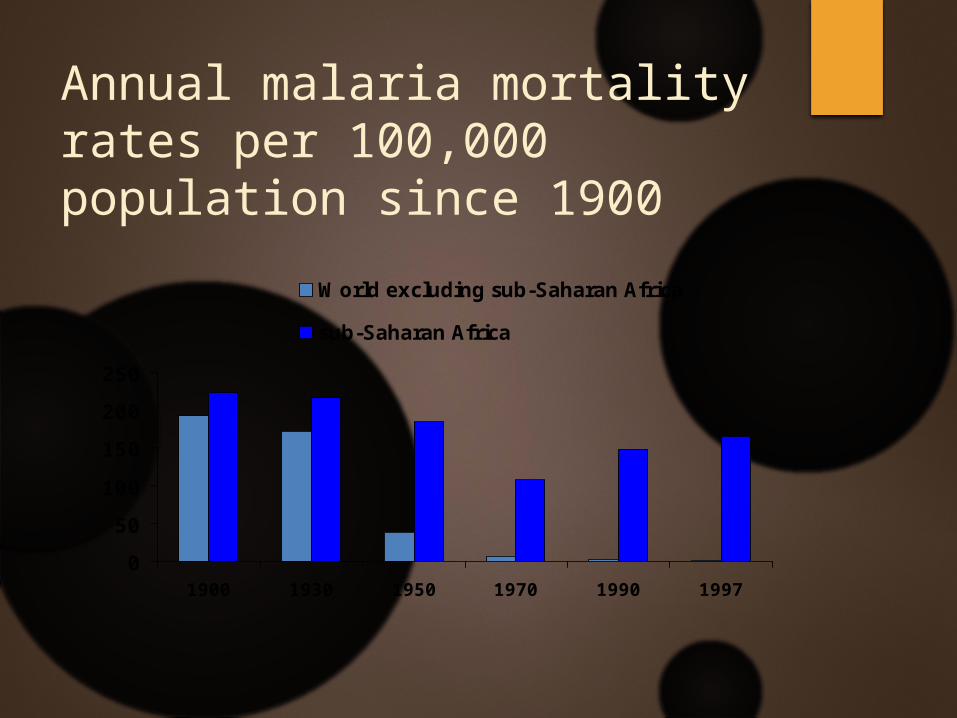
Annual malaria mortality rates per 100,000 population since 1900
0
50
100
150
200
250
1900 1930 1950 1970 1990 1997
World excluding sub-Saharan Africa
sub-Saharan Africa
The General Directorate of Statistics of the Ministry of Health has revealed the results of a study that reported 1,941 cases of malaria in Saudi Arabia 3 years ago. The vast majority of cases were concentrated in the Jizan and Asir regions. Other affected cities included Madina which had 145 cases, Makkah with 92 cases, and Jeddah with 66 cases.
The vast majority of malaria cases, 98.5 percent, were reported in people arriving from abroad, and the remaining 1.5 percent of cases were locally transmitted. With just under 2,000 reports in the year 2010, statistically the incidence of malaria in Saudi Arabia is considered almost non-existent with an occurrence rate of 0.2 cases in every 100,000 individuals in the country.
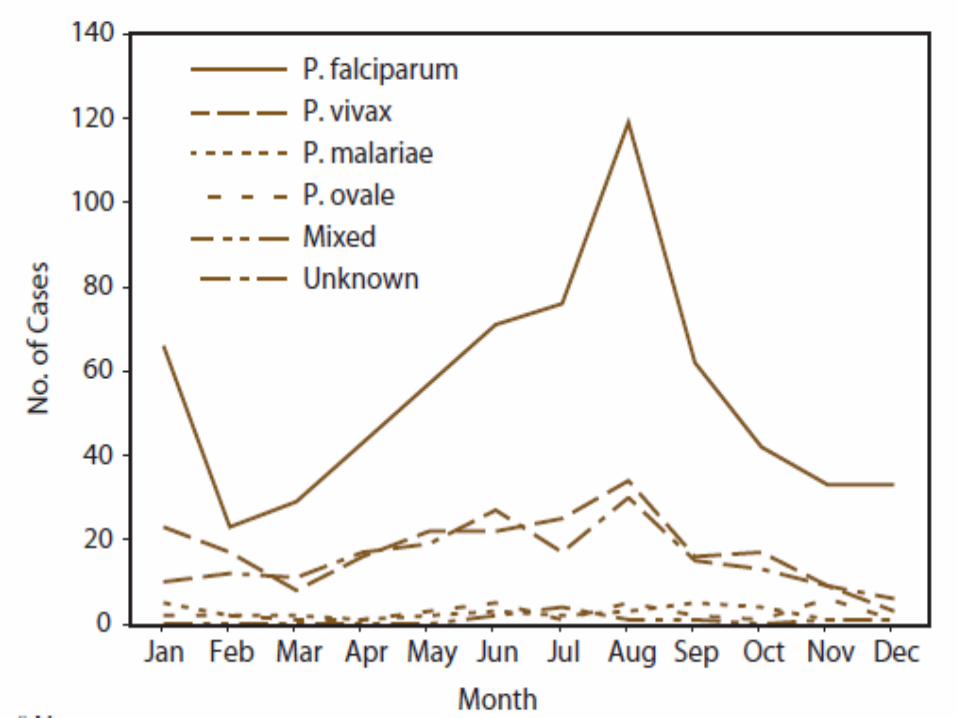
The highest incidence of malaria reports occurred during the months of January and February in the year 2010 in the southwestern regions of the Kingdom. A decline in malaria incidence was noticed starting from March, followed by an increase again in October and November. That is a normal pattern since these months coincide with the rainy season which contributes to the spread of malaria in these regions(3).
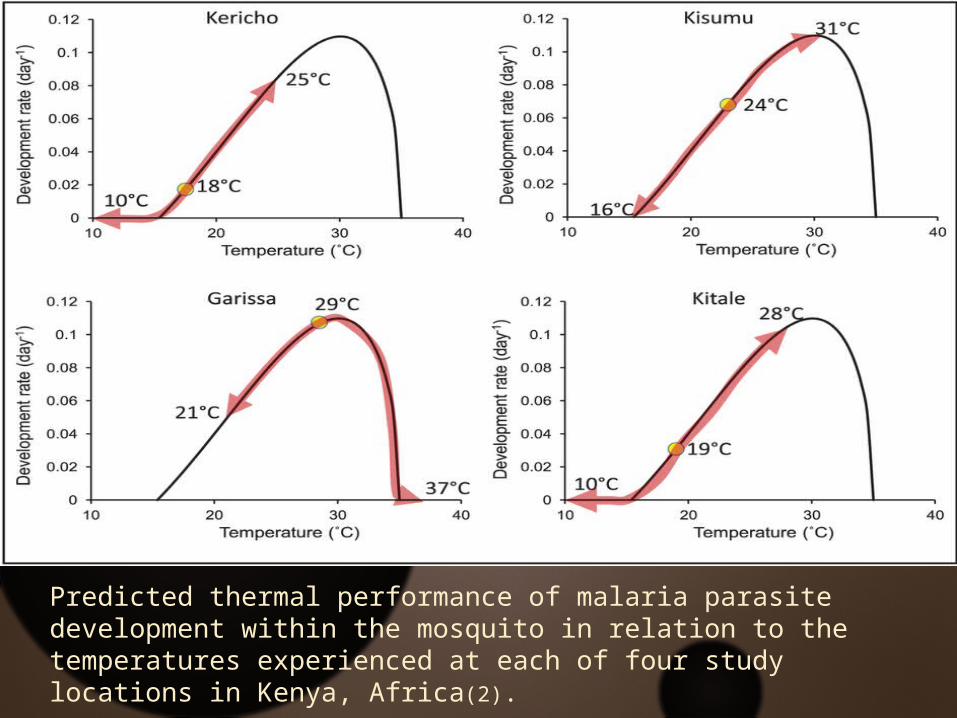
Predicted thermal performance of malaria parasite development within the mosquito in relation to the temperatures experienced at each of four study locations in Kenya, Africa(2).
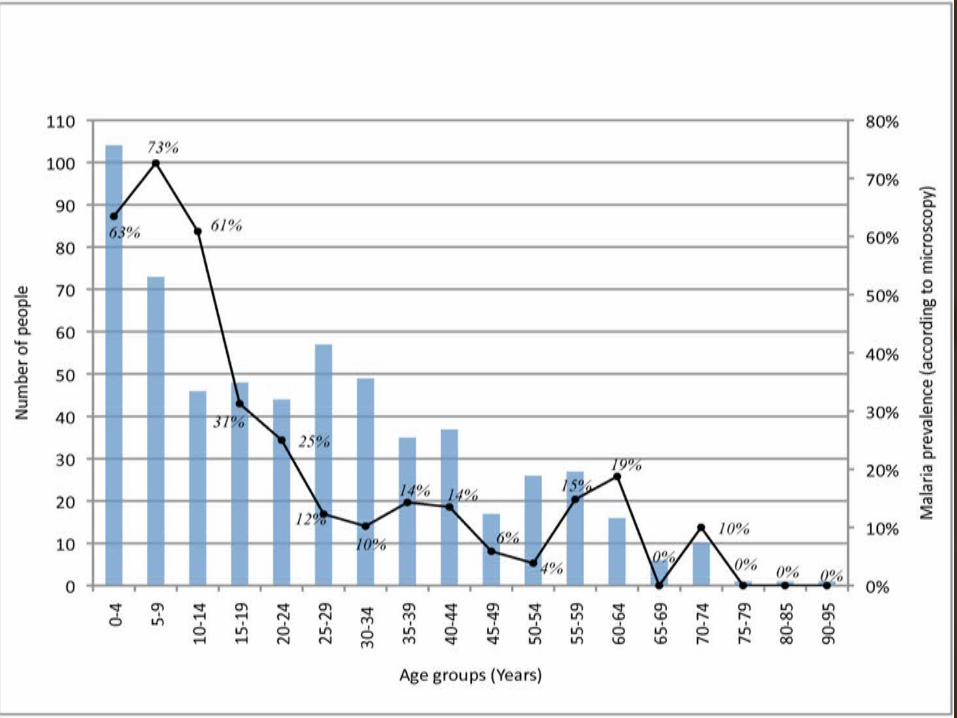
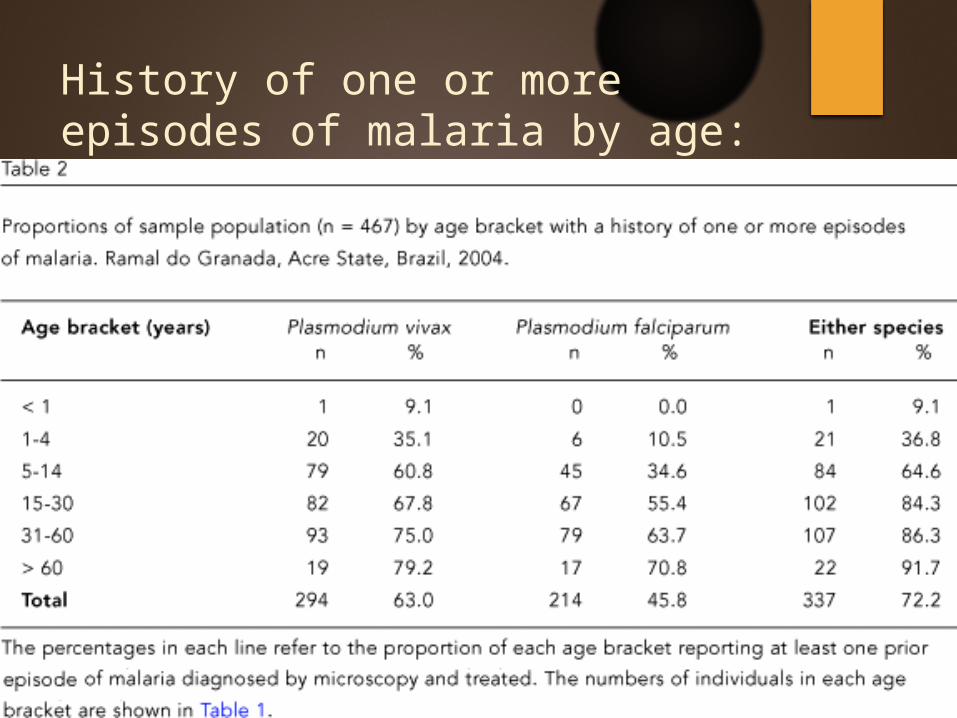
History of one or more episodes of malaria by age:
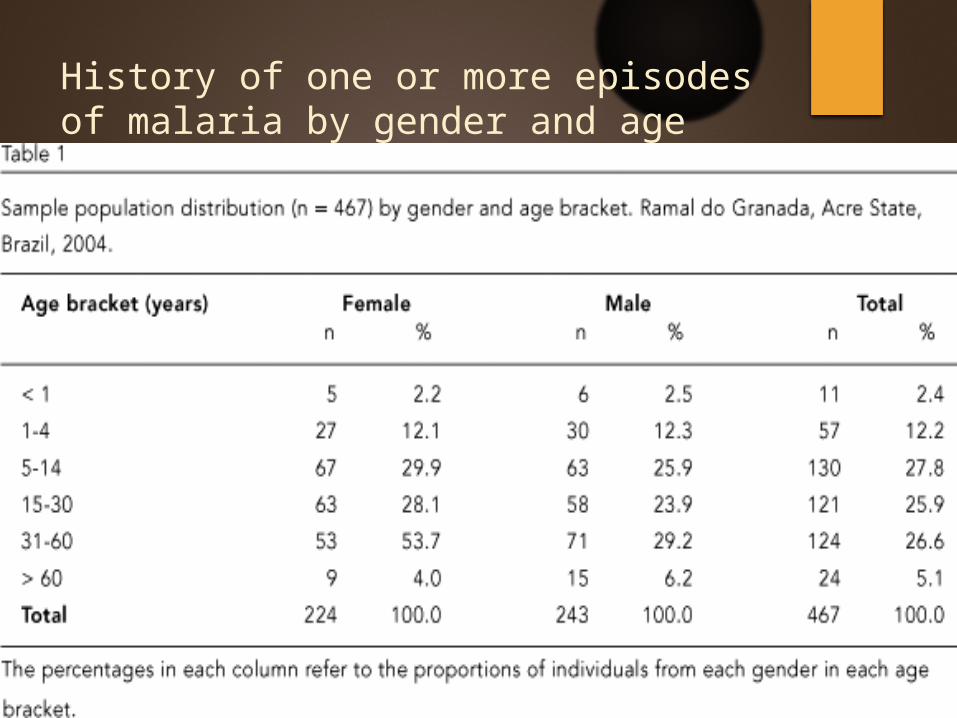
History of one or more episodes of malaria by gender and age bracket:
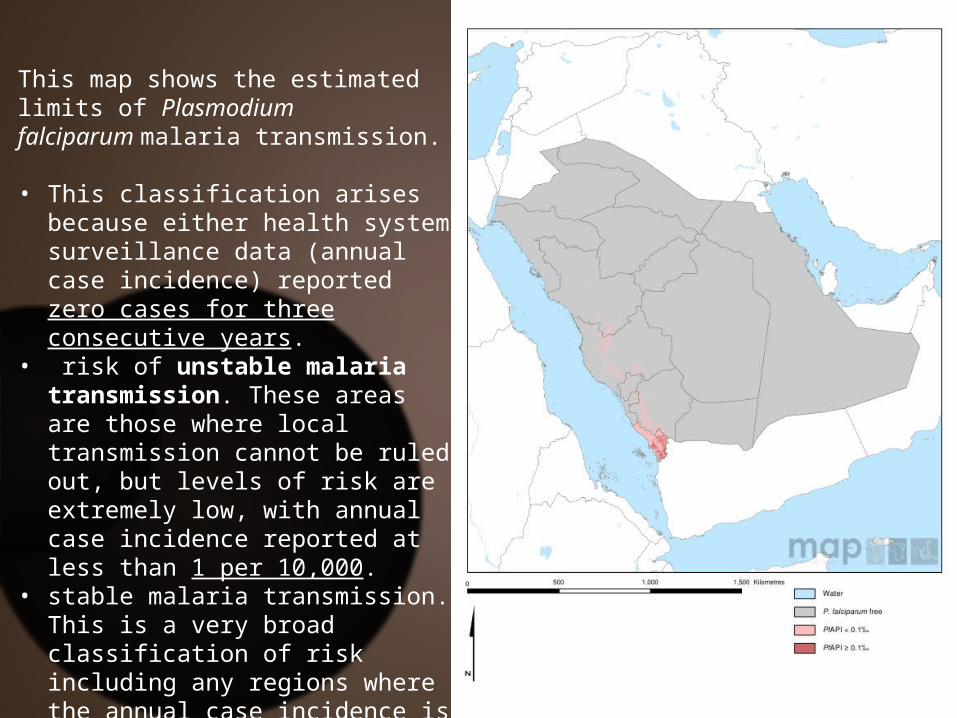
This map shows the estimated limits of Plasmodium falciparum malaria transmission.
• This classification arises because either health system surveillance data (annual case incidence) reported zero cases for three consecutive years.
• risk of unstable malaria transmission. These areas are those where local transmission cannot be ruled out, but levels of risk are extremely low, with annual case incidence reported at less than 1 per 10,000.
• stable malaria transmission. This is a very broad classification of risk including any regions where the annual case incidence is likely to exceed 1 per 10,000.
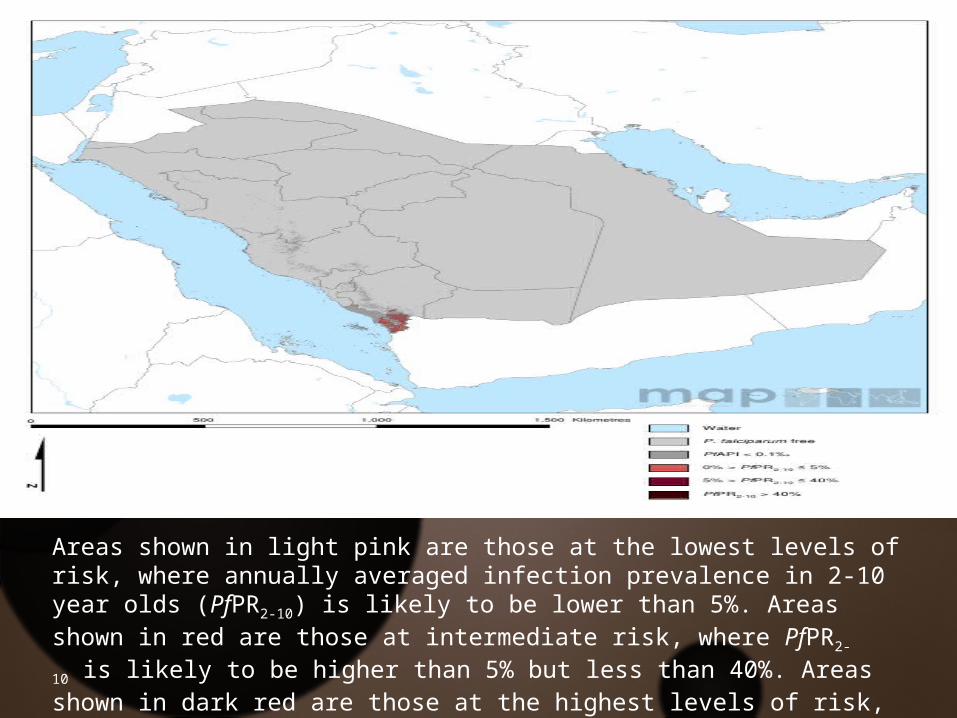
Areas shown in light pink are those at the lowest levels of risk, where annually averaged infection prevalence in 2-10 year olds (PfPR2-10) is likely to be lower than 5%. Areas shown in red are those at intermediate risk, where PfPR2-10 is likely to be higher than 5% but less than 40%. Areas shown in dark red are those at the highest levels of risk, wherePfPR2-10 is likely to exceed 40%.
Risk factors for getting malaria :
Living or traveling in a country or region where malaria is present.
Traveling in an area where malaria is common and: Not taking medicine to prevent malaria before,
during, and after travel, or failing to take the medicine correctly.
Being outdoors, especially in rural areas, between dusk and dawn (nighttime), when the mosquitoes that transmit malaria are most active.
Not taking steps to protect yourself from mosquito bites.
People at increased risk of serious disease include: Young children and infants
Travelers coming from areas with no malaria
Pregnant women and their unborn children
Malaria is more severe in people who have had their spleen removed (splenectomy).
Poverty, lack of knowledge, and little or no access to health care also contribute to malaria deaths worldwide.
overview
MALARIA IS A MOSQUITO-BORNE PARASITIC DISEASE CAUSED BY GENUS PLASMODIUM,
AFFECTING OVER 100 COUNTRIES OF THE TROPICAL
AND SUBTROPICAL REGIONS OF THE WORLD
Causative Agent
Malaria is caused by species of Plasmodium. The genus Plasmodium contains over 200 species
at least 11 species infect humans. Most important are: Plasmodium falciparum
Plasmodium malariae
Plasmodium ovale
Plasmodium vivax
Plasmodium knowlesi
Plasmodium parasites are highly specific with female Anopheles mosquitoes
Vector
Female mosquitos of genus Anopheles are primary hosts and transmission vectors.
Over 100 can transmit human malaria
Only 30–40 commonly transmit parasites of the genus Plasmodium
Anopheles gambiae is one of the best known which transmits Plasmodium falciparum
Vector
Only female mosquitoes feed on blood while the males feed on plant nectar and do not transmit the disease.
The females of Anopheles genus prefer to feed at night
Life Cycle & Pathogenesis
Life Cycle & Pathogenesis
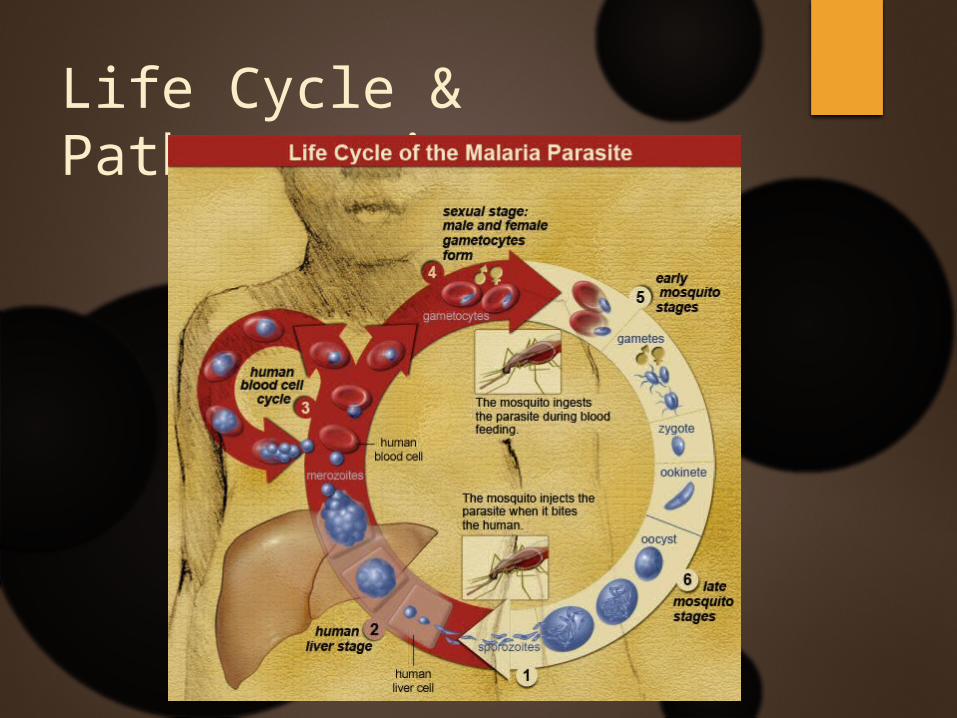
Inside the vector (sexual reproduction):
Young female mosquitoes ingest the malaria parasite by taking a blood meal from an infected human carrier
The ingested gametocytes will differentiate into male and female gametes and then unite to form a zygote (ookinete) in the mosquito’s gut
The resulting ookinete penetrates the gut lining to form an oocyst in the gut wall
The oocyst ruptures to release sporozoites that migrate in the mosquito’s body to the salivary glands and are ready to infect new human hosts
Life Cycle & Pathogenesis
Inside humans: Malaria develops via two phases:
Exoerythrocytic: involves infection of liver
Erythrocytic phase: involves infection of RBC (erythrocytes)
Life Cycle & Pathogenesis
A mosquito infects a person by taking a blood meal.
First, sporozoites enter the bloodstream, and migrate to the liver. They infect liver cells (hepatocytes), where they multiply into merozoites, rupture the liver cells, and escape back into the bloodstream.
Then, the merozoites infect red blood cells, where they develop into ring forms, trophozoites and schizonts which in turn produce further merozoites.
Sexual forms (gametocytes) are also produced, which, if taken up by a mosquito, will infect the insect and continue the life cycle.
Clinical diagnosis
Clinical diagnosis is based on the patient's symptoms and on physical findings at examination.
The first symptoms of malaria (most often fever, chills, sweats, headaches, muscle pains, nausea and vomiting) are often not specific and are also found in other diseases (such as the "flu" and common viral infections)
In severe malaria (caused by Plasmodium falciparum), clinical findings (confusion, coma, neurologic focal signs, severe anemia, respiratory difficulties) are more striking and may increase the index of suspicion for malaria.
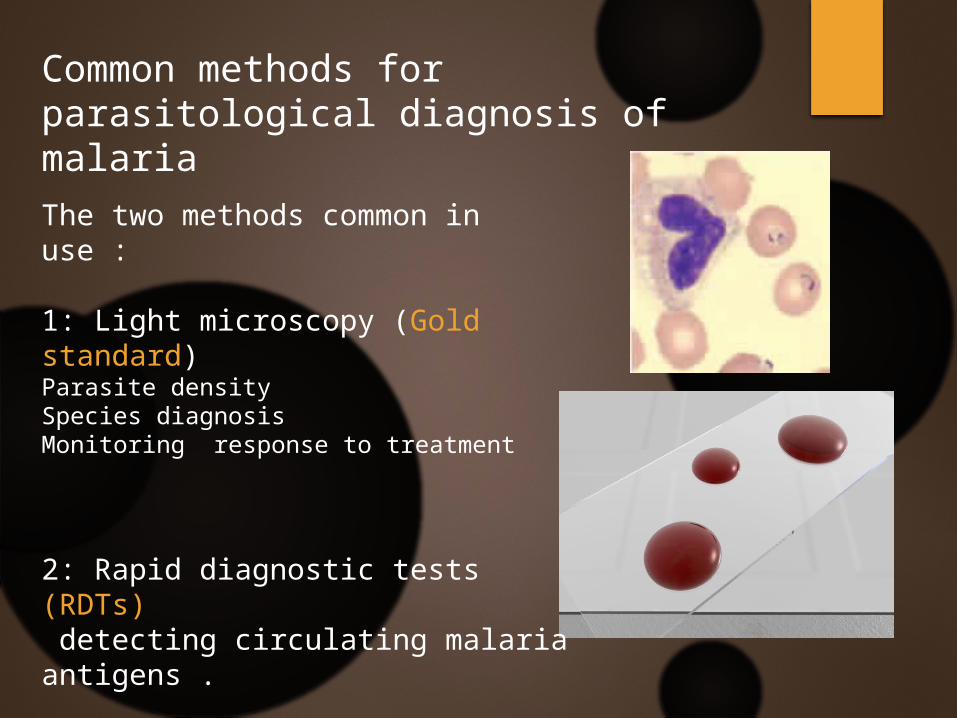
Common methods for parasitological diagnosis of malaria
The two methods common in use :
1: Light microscopy (Gold standard)Parasite densitySpecies diagnosisMonitoring response to treatment
2: Rapid diagnostic tests (RDTs) detecting circulating malaria antigens .
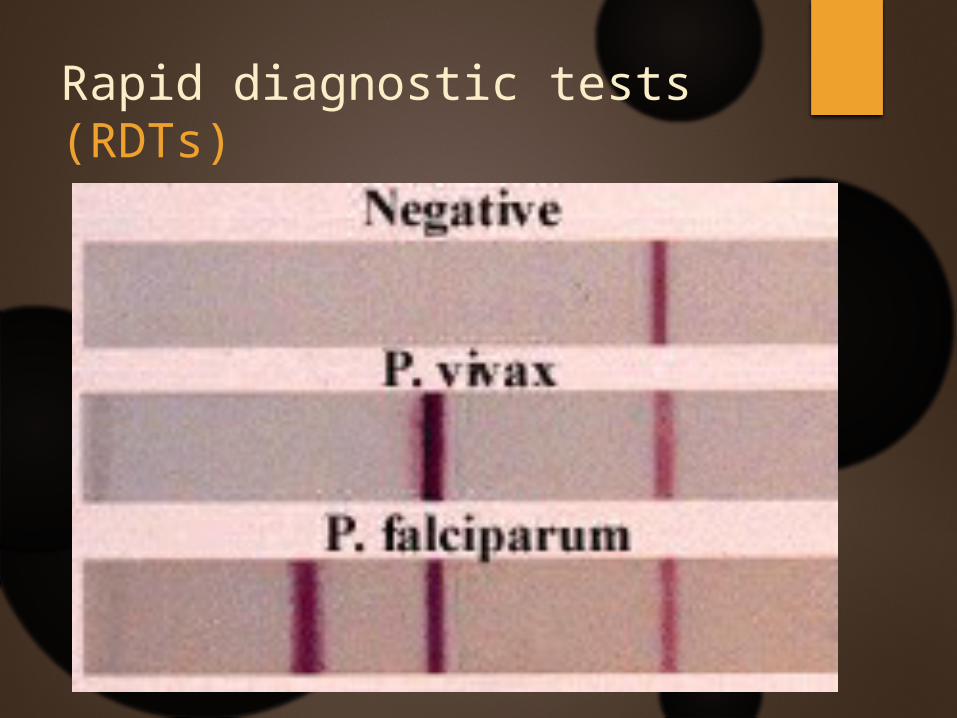
Rapid diagnostic tests (RDTs)
Malaria prevention and control
Control and prevention elements
The goal of the malaria control and elimination program is interruption of malaria transmission and this is can be done via
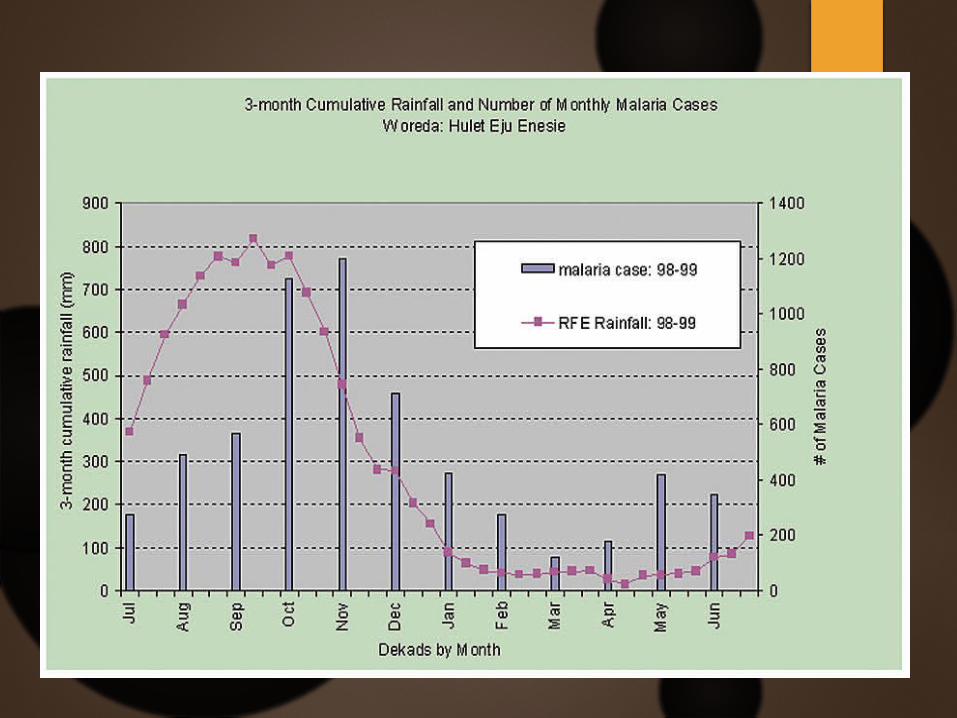
Malaria is prevalent in tropical and subtropical regions because rainfall, warm temperatures, and stagnant waters provide habitats ideal for mosquito larvae.
Vector control
is the main way to reduce malaria transmission at the community level. It is the only intervention that can reduce malaria transmission from very high levels to close to zero. For individuals, personal protection against mosquito bites represents the first line of defense for malaria prevention.
Types of vector control
1-Indoor spraying with residual insecticides:spraying of insecticides on the walls inside a home. After feeding, many mosquitoes rest on a nearby surface while digesting the bloodmeal, so if the walls of houses have been coated with insecticides, the resting mosquitoes can be killed before they can bite another person and transfer the malaria parasite
2- mosquito nets Bed nets are a sensible physical barrier precaution against malaria-transmitting mosquitoes since the major malaria vectors bite during the night
It contains many types:
1. Traditional bed nets
2. Insecticide-treated nets (ITNs)
3. Long-lasting insecticidal nets (LLINs)
Long-Lasting Insecticidal Nets (LLINs)
These are pretreated with insecticides.
They last about 3 to 5 years, and do not need to be retreated.
They are an effective and inexpensive way to prevent malaria.
They are recommended by the World Health Organization
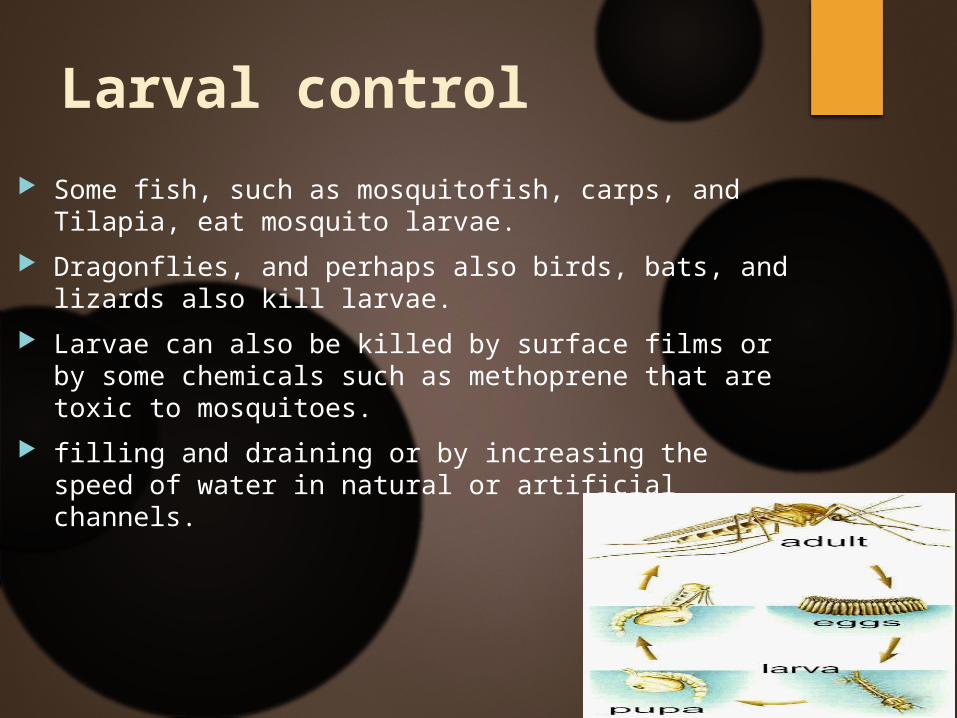
Larval control
Some fish, such as mosquitofish, carps, and Tilapia, eat mosquito larvae.
Dragonflies, and perhaps also birds, bats, and lizards also kill larvae.
Larvae can also be killed by surface films or by some chemicals such as methoprene that are toxic to mosquitoes.
filling and draining or by increasing the speed of water in natural or artificial channels.
Personal protection
When travelling in areas with malaria, wear loose-fitting long trousers and long sleeves in the evenings, as the mosquitoes that carry malaria are most active at this time.
Health education
strategies promoting awareness of malaria and the importance of control measures have been successfully used to reduce the incidence of malaria in some areas of the developing world.
Recognizing the disease in the early stages can stop the disease from becoming fatal. Education can also inform people to cover over areas of stagnant, still water, such as water tanks that are ideal breeding grounds for the parasite and mosquito, thus cutting down the risk of the
Prevention
Methods used to prevent malaria include medications, mosquito elimination and the prevention of bites. There is no vaccine for malaria.
Chloroquine-Doxycycline-Mefloquine-Primaquine-Atovaquone
Malaria control in KSA
n 1998, the Kingdom of Saudi Arabia (KSA) suffered its worst malaria epidemic. A total of 36,139 locally transmitted cases were recorded and incidence reached as high as 44/1000 in malarious regions
hese activities had a significant impact, in 2011 only 29 locally transmitted cases were recorded in the country, reducing incidence to <0.01/1000,
HOW ?
1- health education in endemic area
2- try to early diagnose and treat for malaria
3- establish central labs for diagnosing in endemic area
4- use all the control and prevention methods of WHO
1948 ARAMCO
1952 Cooperation between saudi government and Who
1970 no more cases in dammad and north saudi
1978 asir and jizan - Cooperation with yemeni government
1982 using insecticides in endemic areas
1983 activation of all the methods of WHO