Embed Size (px)
Citation preview

EPIDURAL OR EXTRADURAL HEMATOMA
(HAEMATOMA)
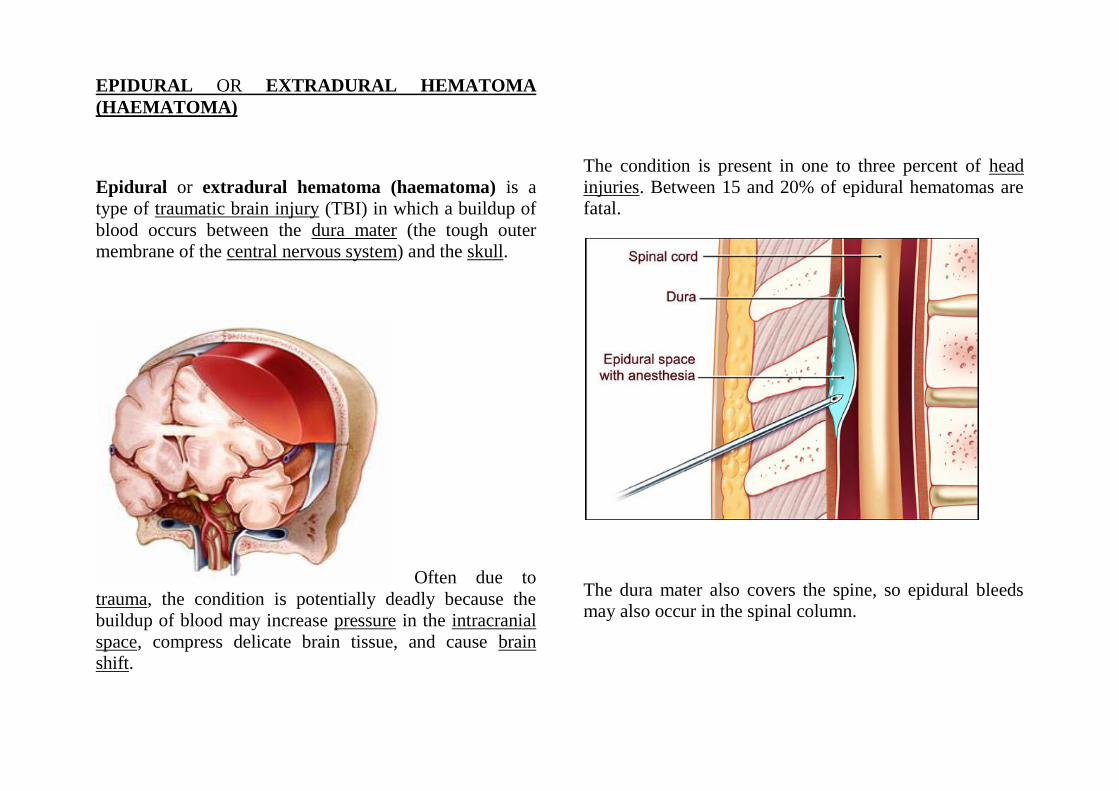
Epidural or extradural hematoma (haematoma) is a
type of traumatic brain injury (TBI) in which a buildup of
blood occurs between the dura mater (the tough outer
membrane of the central nervous system) and the skull.
Often due to
trauma, the condition is potentially deadly because the
buildup of blood may increase pressure in the intracranial
space, compress delicate brain tissue, and cause brain
shift.
The condition is present in one to three percent of head
injuries. Between 15 and 20% of epidural hematomas are
fatal.
The dura mater also covers the spine, so epidural bleeds
may also occur in the spinal column.
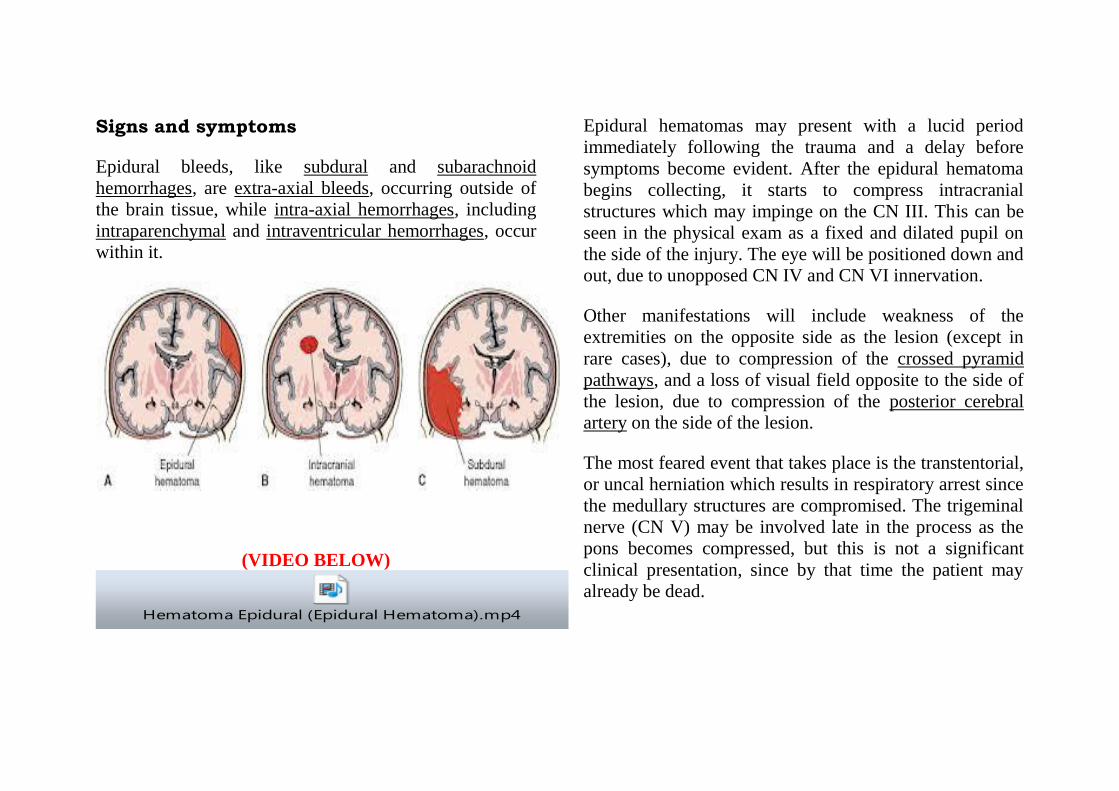
Signs and symptoms
Epidural bleeds, like subdural and subarachnoid
hemorrhages, are extra-axial bleeds, occurring outside of
the brain tissue, while intra-axial hemorrhages, including
intraparenchymal and intraventricular hemorrhages, occur
within it.
(VIDEO BELOW)
Hematoma Epidural (Epidural Hematoma).mp4
Epidural hematomas may present with a lucid period
immediately following the trauma and a delay before
symptoms become evident. After the epidural hematoma
begins collecting, it starts to compress intracranial
structures which may impinge on the CN III. This can be
seen in the physical exam as a fixed and dilated pupil on
the side of the injury. The eye will be positioned down and
out, due to unopposed CN IV and CN VI innervation.
Other manifestations will include weakness of the
extremities on the opposite side as the lesion (except in
rare cases), due to compression of the crossed pyramid
pathways, and a loss of visual field opposite to the side of
the lesion, due to compression of the posterior cerebral
artery on the side of the lesion.
The most feared event that takes place is the transtentorial,
or uncal herniation which results in respiratory arrest since
the medullary structures are compromised. The trigeminal
nerve (CN V) may be involved late in the process as the
pons becomes compressed, but this is not a significant
clinical presentation, since by that time the patient may
already be dead.
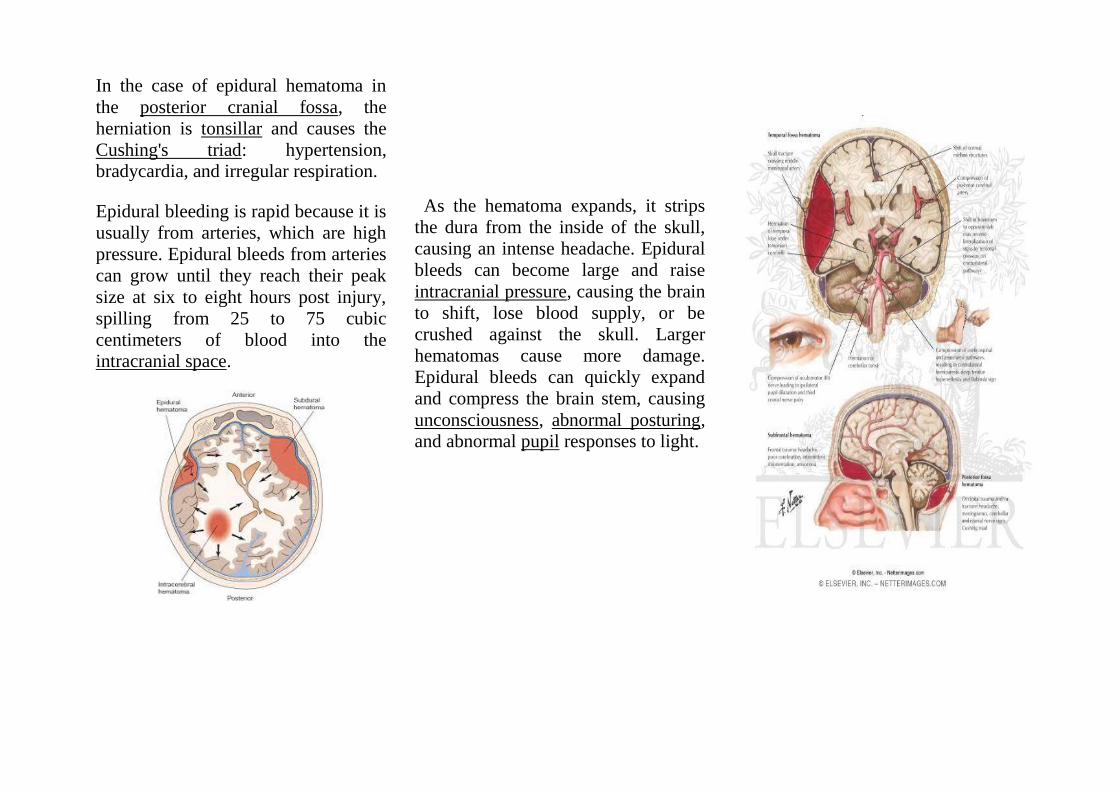
In the case of epidural hematoma in
the posterior cranial fossa, the
herniation is tonsillar and causes the
Cushing's triad: hypertension,
bradycardia, and irregular respiration.
Epidural bleeding is rapid because it is
usually from arteries, which are high
pressure. Epidural bleeds from arteries
can grow until they reach their peak
size at six to eight hours post injury,
spilling from 25 to 75 cubic
centimeters of blood into the
intracranial space.
As the hematoma expands, it strips
the dura from the inside of the skull,
causing an intense headache. Epidural
bleeds can become large and raise
intracranial pressure, causing the brain
to shift, lose blood supply, or be
crushed against the skull. Larger
hematomas cause more damage.
Epidural bleeds can quickly expand
and compress the brain stem, causing
unconsciousness, abnormal posturing,
and abnormal pupil responses to light.
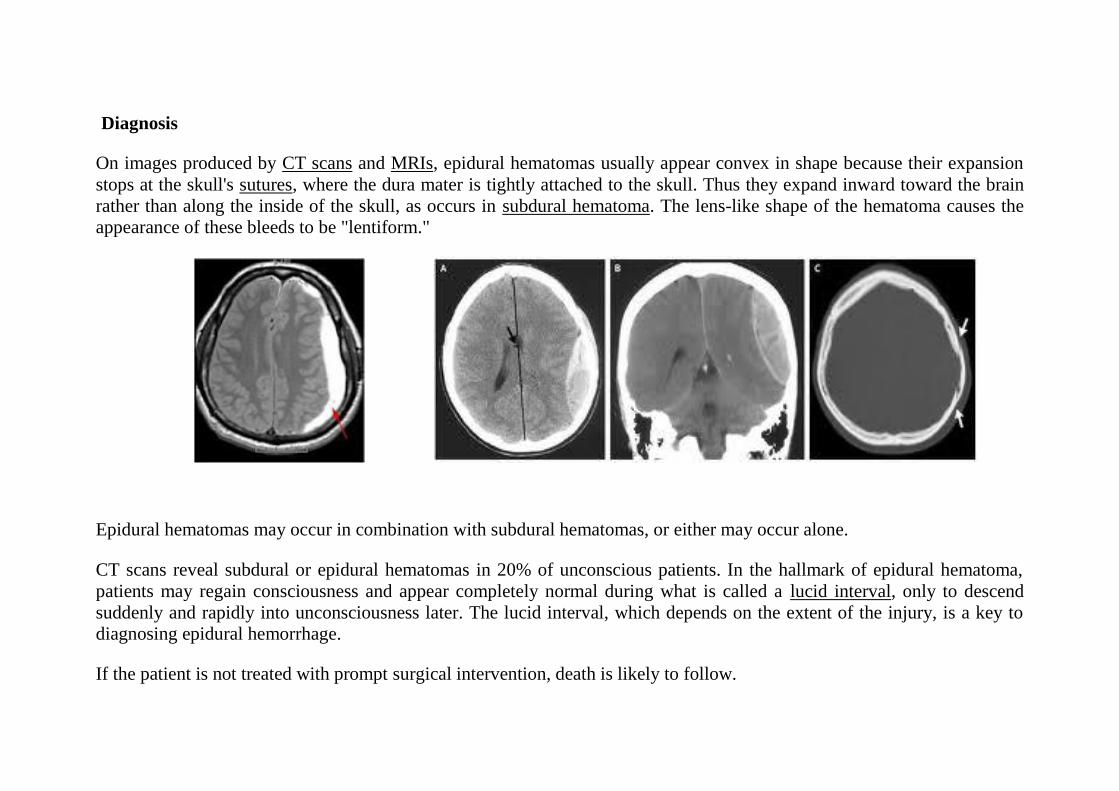
Diagnosis
On images produced by CT scans and MRIs, epidural hematomas usually appear convex in shape because their expansion
stops at the skull's sutures, where the dura mater is tightly attached to the skull. Thus they expand inward toward the brain
rather than along the inside of the skull, as occurs in subdural hematoma. The lens-like shape of the hematoma causes the
appearance of these bleeds to be "lentiform."
Epidural hematomas may occur in combination with subdural hematomas, or either may occur alone.
CT scans reveal subdural or epidural hematomas in 20% of unconscious patients. In the hallmark of epidural hematoma,
patients may regain consciousness and appear completely normal during what is called a lucid interval, only to descend
suddenly and rapidly into unconsciousness later. The lucid interval, which depends on the extent of the injury, is a key to
diagnosing epidural hemorrhage.
If the patient is not treated with prompt surgical intervention, death is likely to follow.
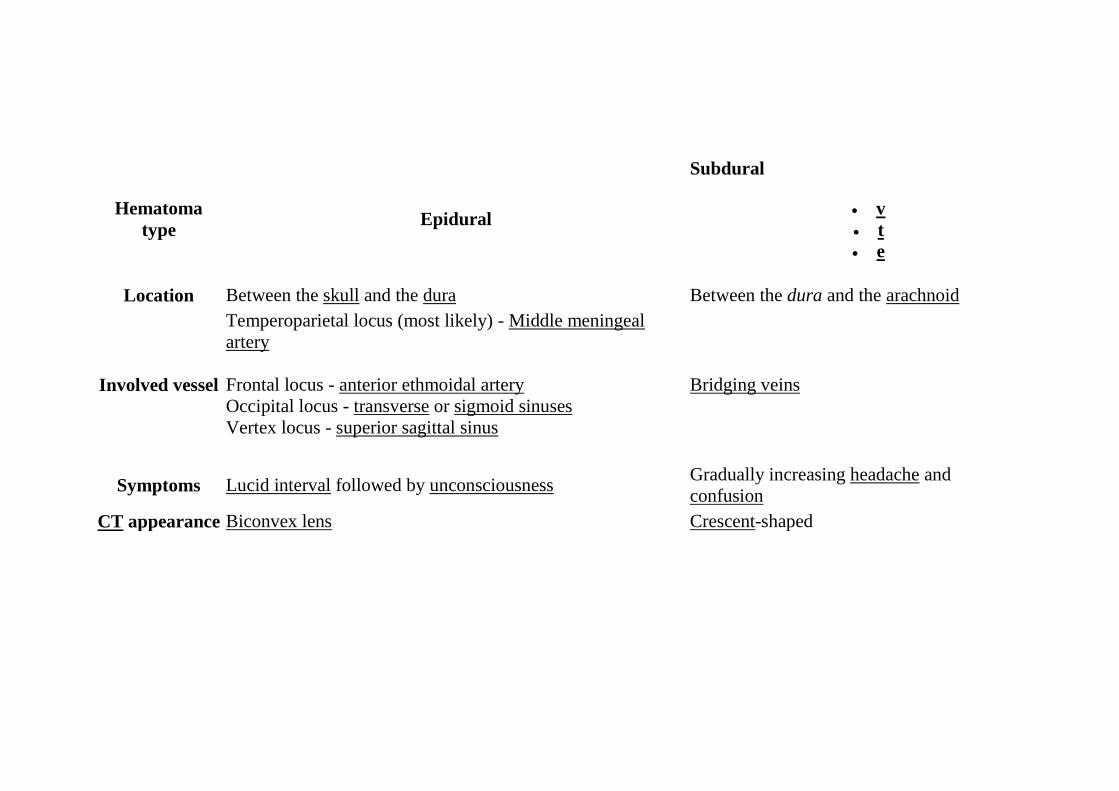
Hematoma
type Epidural
Subdural
v
t
e
Location Between the skull and the dura Between the dura and the arachnoid
Involved vessel
Temperoparietal locus (most likely) - Middle meningeal
artery
Frontal locus - anterior ethmoidal artery
Occipital locus - transverse or sigmoid sinuses
Vertex locus - superior sagittal sinus
Bridging veins
Symptoms Lucid interval followed by unconsciousness Gradually increasing headache and
confusion
CT appearance Biconvex lens Crescent-shaped
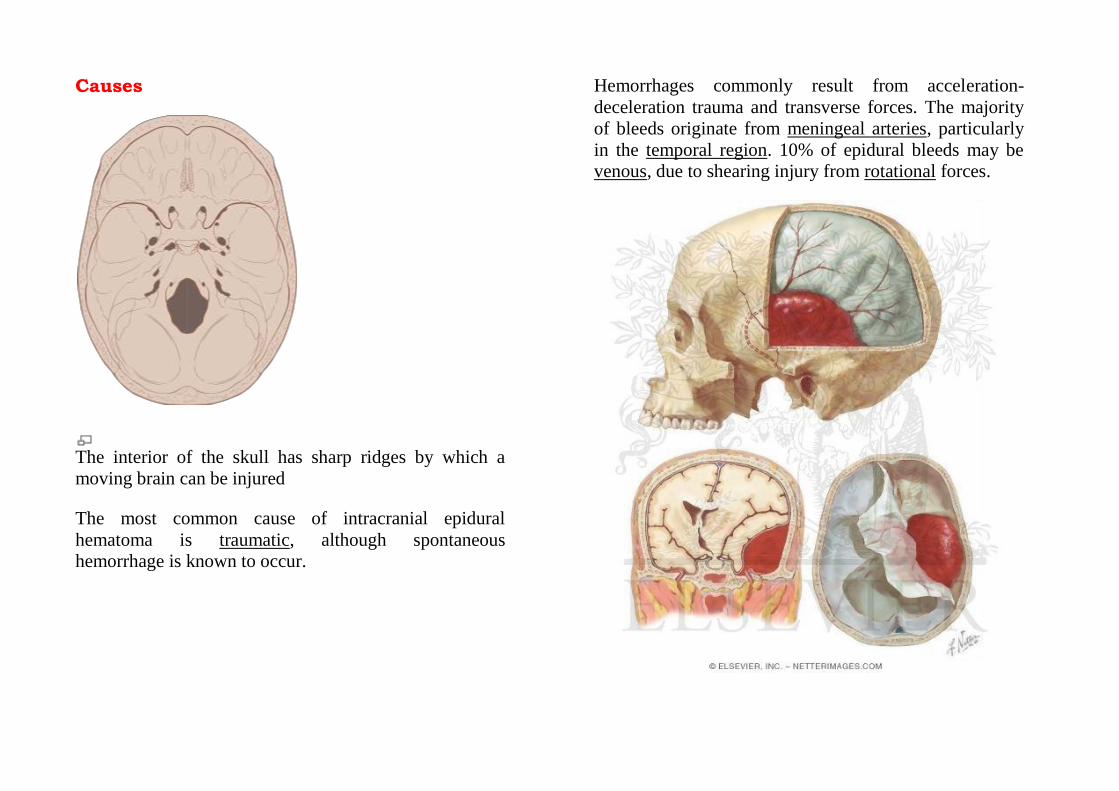
Causes
The interior of the skull has sharp ridges by which a
moving brain can be injured
The most common cause of intracranial epidural
hematoma is traumatic, although spontaneous
hemorrhage is known to occur.
Hemorrhages commonly result from acceleration-
deceleration trauma and transverse forces. The majority
of bleeds originate from meningeal arteries, particularly
in the temporal region. 10% of epidural bleeds may be
venous, due to shearing injury from rotational forces.
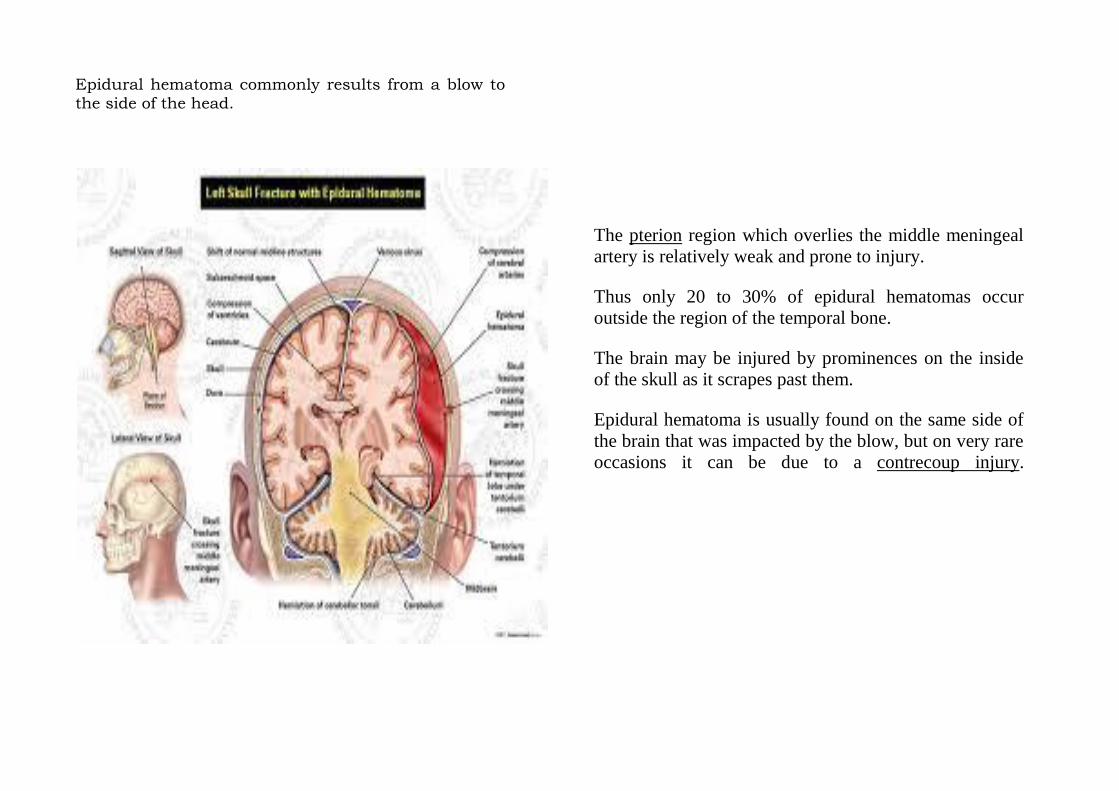
Epidural hematoma commonly results from a blow to
the side of the head.
The pterion region which overlies the middle meningeal
artery is relatively weak and prone to injury.
Thus only 20 to 30% of epidural hematomas occur
outside the region of the temporal bone.
The brain may be injured by prominences on the inside
of the skull as it scrapes past them.
Epidural hematoma is usually found on the same side of
the brain that was impacted by the blow, but on very rare
occasions it can be due to a contrecoup injury.
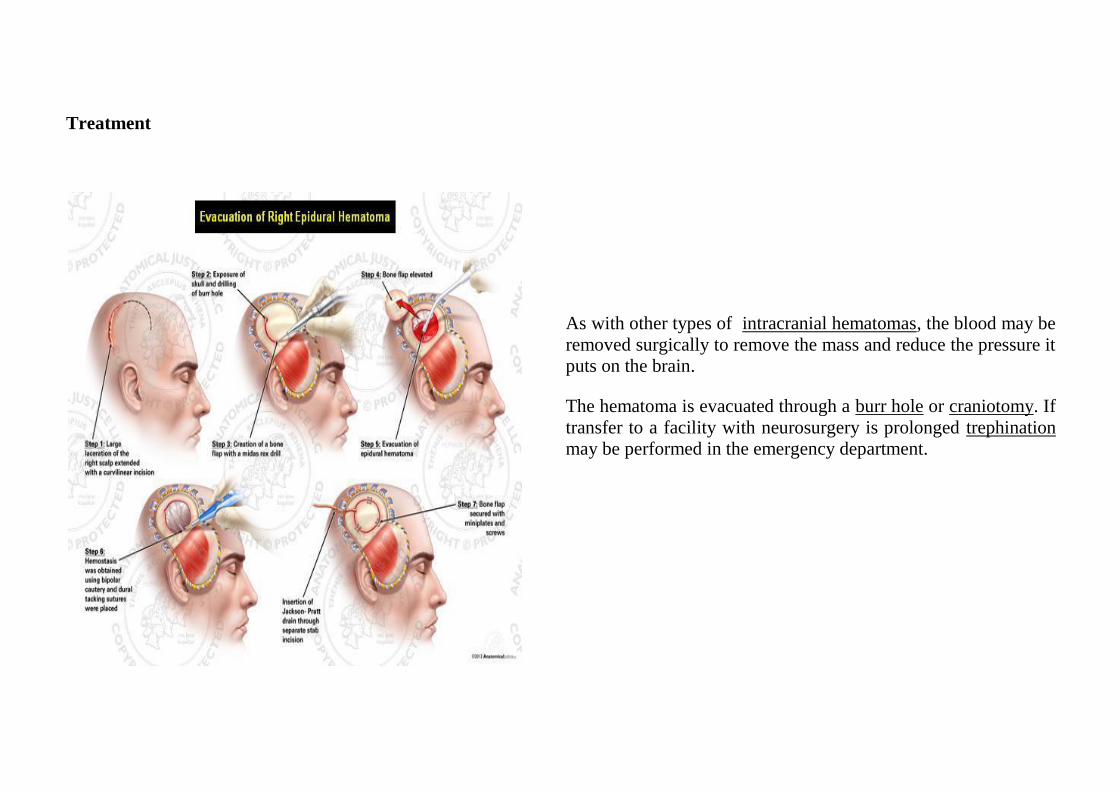
Treatment
As with other types of intracranial hematomas, the blood may be
removed surgically to remove the mass and reduce the pressure it
puts on the brain.
The hematoma is evacuated through a burr hole or craniotomy. If
transfer to a facility with neurosurgery is prolonged trephination
may be performed in the emergency department.
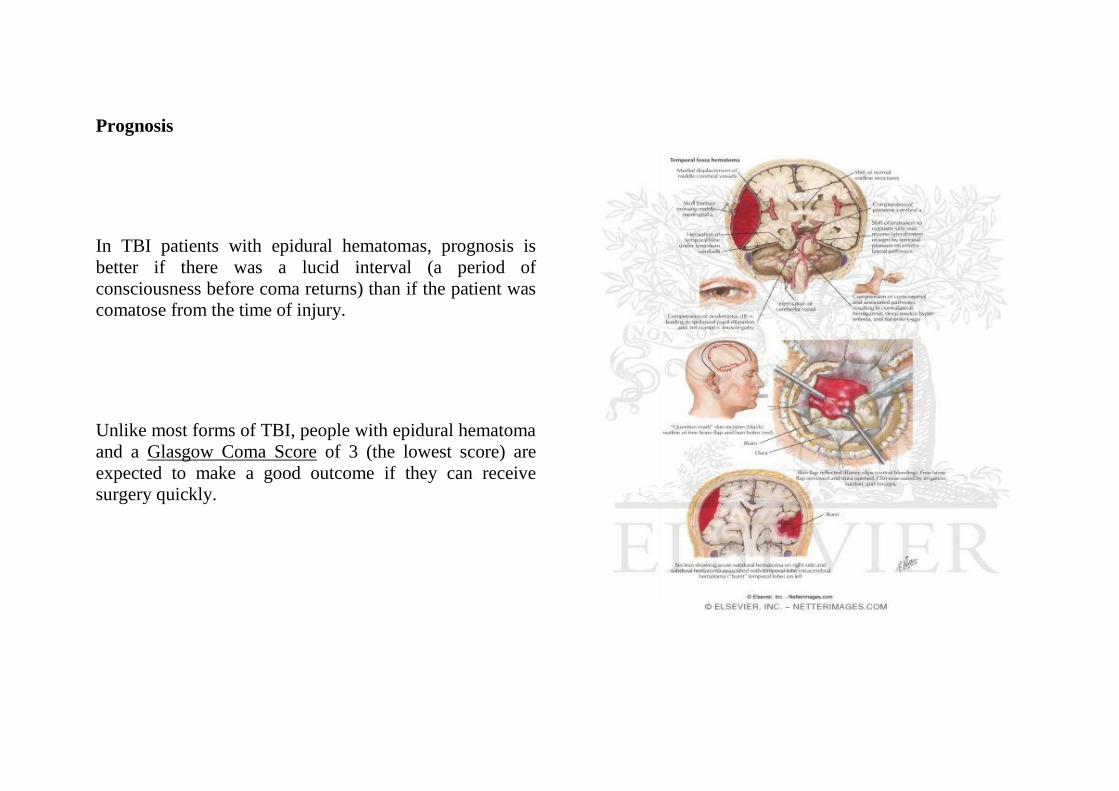
Prognosis
In TBI patients with epidural hematomas, prognosis is
better if there was a lucid interval (a period of
consciousness before coma returns) than if the patient was
comatose from the time of injury.
Unlike most forms of TBI, people with epidural hematoma
and a Glasgow Coma Score of 3 (the lowest score) are
expected to make a good outcome if they can receive
surgery quickly.

Of the spine
Bleeding into the epidural space in the spine may also
cause epidural hematoma. These may arise spontaneously
(e.g. during childbirth), or as a rare complication of
anaesthesia (such as epidural anaesthesia) or surgery (such
as laminectomy).
(VIDEO BELOW)
Epidural Hematoma.mp4
The anatomy of the epidural space means that spinal
epidural hematoma has a different profile from cranial
epidural hematoma.
In the spine, the epidural space contains loose fatty tissue,
and the epidural venous plexus, a network of large, thin-
walled veins.
This means that bleeding is likely to be venous.
Anatomical abnormalities and bleeding disorders make
these lesions more likely.
They may cause pressure on the spinal cord or cauda
equina, which may present as pain, muscle weakness, or
bladder and bowel dysfunction.
The diagnosis may be made on clinical appearance and
time course of symptoms.
It usually requires MRI scanning to confirm.
The treatment is surgical decompression.
The incidence of epidural hematoma following epidural
anaesthesia is extremely difficult to quantify; estimates
vary from 1 per 10,000 to 1 per 100,000 epidural
anaesthetics.
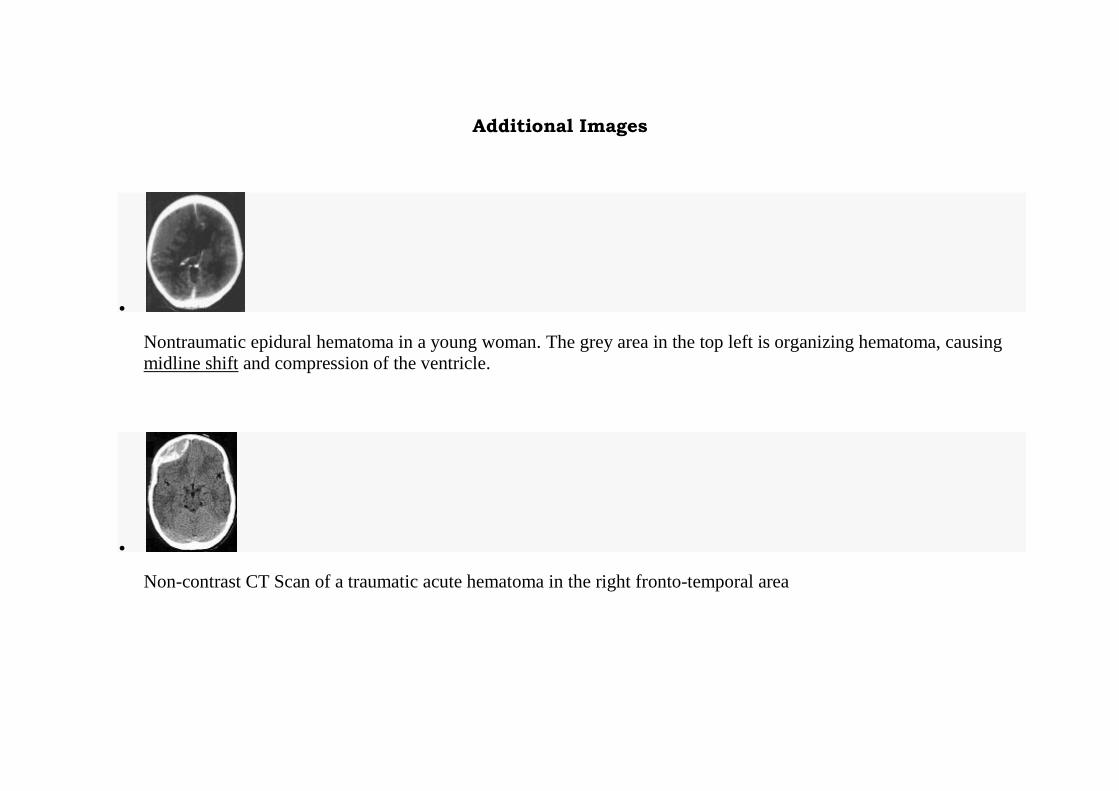
Additional Images
Nontraumatic epidural hematoma in a young woman. The grey area in the top left is organizing hematoma, causing
midline shift and compression of the ventricle.
Non-contrast CT Scan of a traumatic acute hematoma in the right fronto-temporal area