Embed Size (px)
Citation preview
Equine Dermatology
Stephen D. White, DVM, Diplomate ACVD; andAnthony A. Yu, DVM, MS, Diplomate ACVD
Authors’ addresses: Department of Medicine and Epidemiology, School of Veterinary Medicine,University of California at Davis, Davis, CA 95616 (White); and Department of Clinical Studies,Ontario Veterinary College, University of Guelph, Guelph, Ontario N1G 2W1, Canada (Yu); e-mails:[email protected] (White) and [email protected] (Yu). © 2006 AAEP.
I. Diagnosis and Treatment of the Pruritic Horse
Pyoderma (Bacterial Skin Infections)
Stephen D. White, DVM, Diplomate ACVD
1. Introduction
Bacterial folliculitis (superficial pyoderma) is usu-ally caused by a coagulase positive Staphylococcusspecies. Both S. aureus and S. intermedius havebeen isolated.1,2 In one study, S. aureus accountedfor twice as many isolates as S intermedius; thesame study isolated some strains of S. hyicus aswell.3 Interestingly, in another study, lysozymesfrom equine neutrophils were only slightly bacteri-cidal for S. aureus.4 Many isolates are resistant topenicillin G3. Occurrence of pyoderma has beenlinked to poor nutrition and husbandry in somecases.5
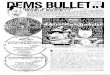
Clinical signs of staphylococcal pyoderma aremost often crusts, usually in a circular pattern sug-gestive of dermatophytosis (this may be the reasonthat equine pyoderma is underdiagnosed), epider-mal collarettes (circular skin lesions with an exfoli-
ative border as seen in dogs with superficialpyoderma; Figs. 1 and 2), or encrusted papules sim-ilar to the miliary dermatitis reaction pattern incats.6 These infections tend to be variable in theirintensity of pruritus. Histology usually shows fol-liculitis and/or furunculosis, but bacterial coloniesare not always seen. A truncal form of bacterialfolliculitis (contagious acne, contagious pustulardermatitis, or Canadian horsepox) is often associ-ated with poor grooming, trauma from tack andsaddle, warm wet weather, and heavy work. It ispainful and interferes with working and riding.It is usually caused by a coagulase positive Staphy-lococcus species but may also be caused by Coryne-bacterium pseudotuberculosis.7 This organism ismore commonly a cause of deep pyoderma, as dis-cussed below (Fig. 3). In horses, folliculitis oftendevelops in the saddle and lumbar region, particu-larly in the summer. The affected area initiallymay be swollen and very sensitive; this is followedby formation of follicular papules and pustules.These may become confluent or rupture, forming
AAEP PROCEEDINGS � Vol. 52 � 2006 457
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
NOTES
plaques and crusts. Deep pyoderma followed byulceration may develop over large areas of the body,especially on the neck, sides of the thorax, innersurface of the thighs, or the prepuce.
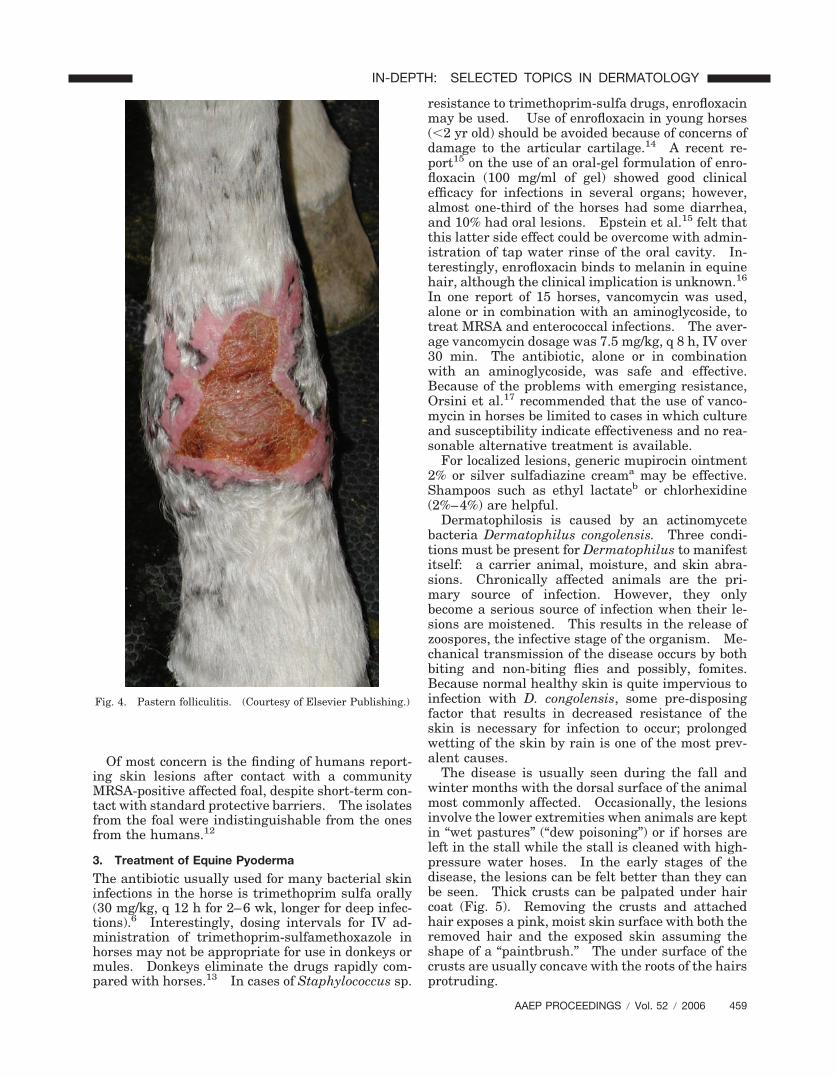
A pastern bacterial infection (pastern folliculitis)is often seen. Again, the causative agent is usuallya coagulase positive Staphylococcus species. Aswith most “primary pyodermas,” the mechanism(s)whereby the organism gains its foothold is unknown(not contagion and not poor sanitary conditions).The lesions are usually limited to the posterior as-pect of the pastern and fetlock regions; one or morelimbs may be involved. The initial lesions consistof papules and pustules (Fig. 4). If left untreated,the lesions coalesce and may produce large areas ofulceration and suppuration, which may be quite
painful. The disease is usually not associated withsystemic signs, and the general health of the horse isnot affected.
A relatively uncommon nodular disease termed“botryomycosis” mimics actinomycosis or a deep fun-gal infection, but it is most often caused by Staphy-lococcus species in the horse. These may requiresurgical excision as well as long-term antibiotics.
2. Public Health Considerations�Staphylococcus spp.
In a 2000 study, methicillin-resistant coagulase-negative staphyloccal species were cultured fromhealthy horses in Japan; Yusada et al.8 concludedthat “[t]hese organisms must be considered a poten-tial threat to horses and veterinarians who care forthem.” In a 2006 study from the Netherlands, me-thicillin-resistant coagulase-negative staphylococciwere found frequently.9 The organism was usuallyS. sciuri, not S. epidermidis, which was found in thehumans in close contact with these horses. No me-thicillin-resistant S. aureus (MRSA) was found inhealthy horses.
In contrast, a single strain of MRSA was isolatedfrom both humans (13%) and horses (4.7%) on horsefarms in Canada and New York state.10 In lookingat horses admitted to a university teaching hospital(Ontario Veterinary College, University of Guelph,Guelph, Ontario, Canada), MRSA was isolated from120 (5.3%) of 2,283 horses. Of these 120 horses,50.8% were positive at the time of admission, andclinical infections attributable to MRSA werepresent or developed in 14 horses. Horses colo-nized at admission were more likely to develop clin-ical MRSA infection. Administration of ceftiofur oraminoglycosides during hospitalization was the onlyrisk factor associated with nosocomial MRSA colo-nization. Another strain of MRSA was isolatedfrom a small number of horses at the VeterinaryUniversity in Vienna, Austria.11
Fig. 1. Staphylococcal folliculitis: crusts in a circular pattern.(Courtesy of Elsevier Publishing.)
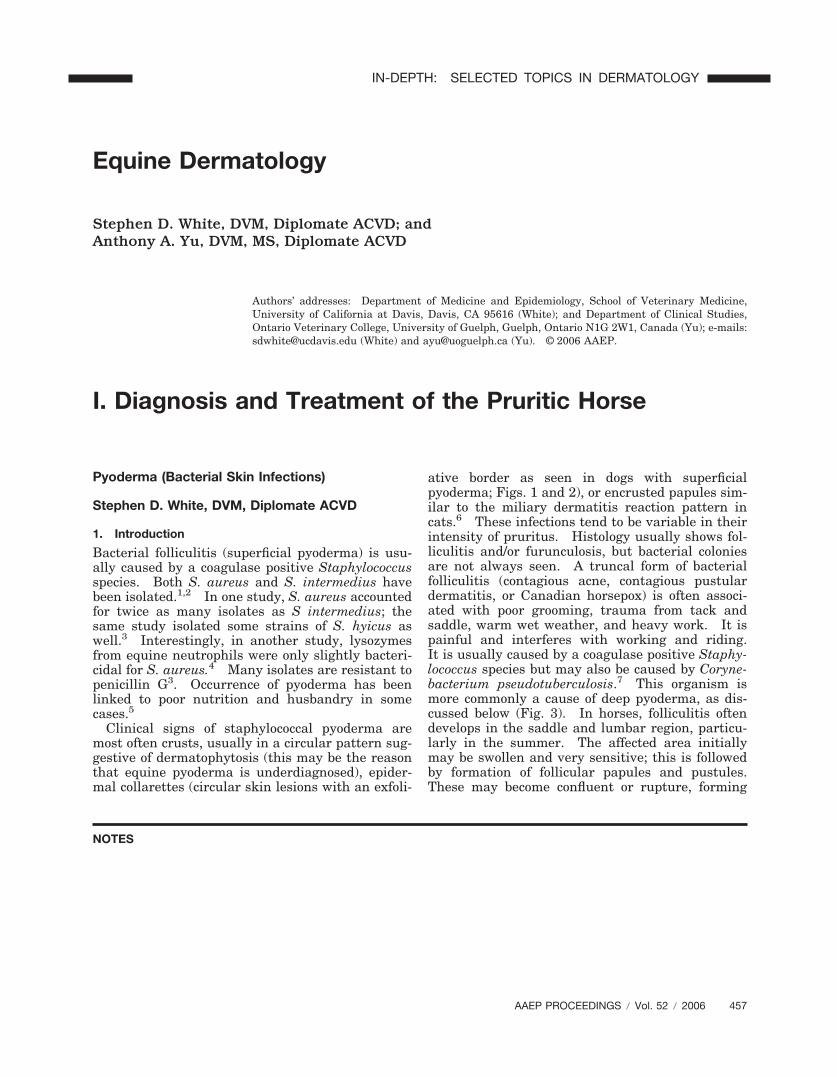
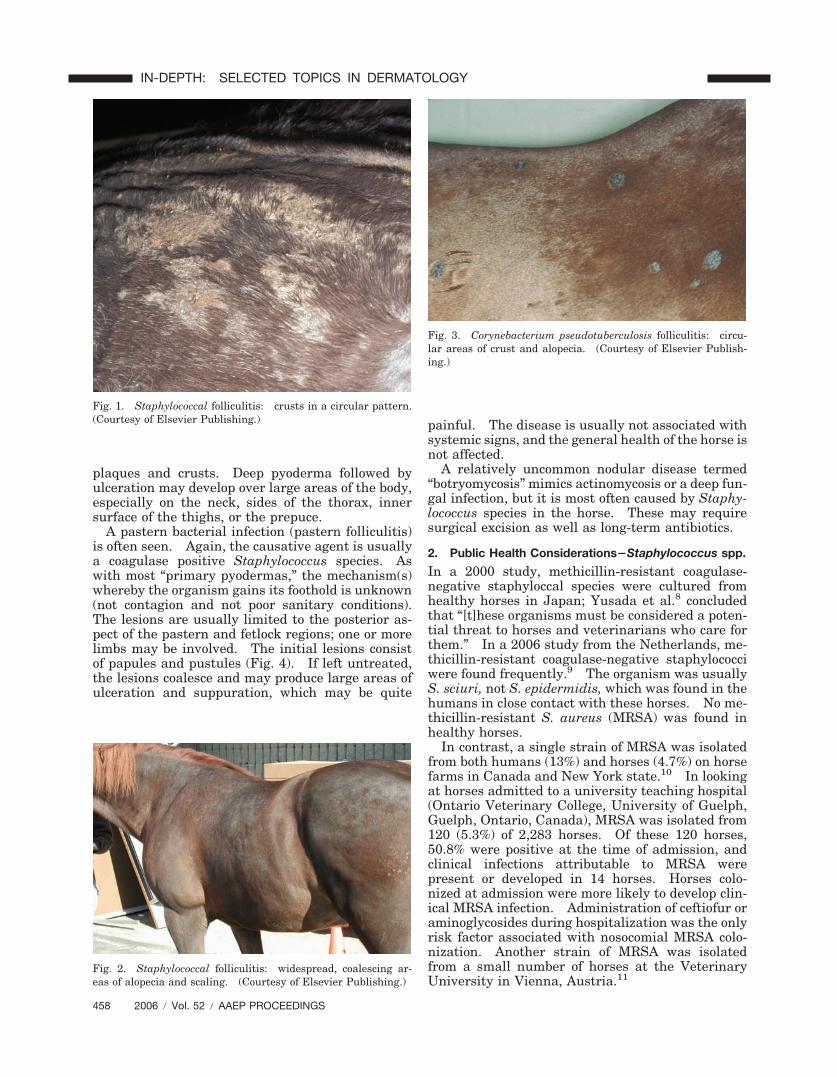
Fig. 2. Staphylococcal folliculitis: widespread, coalescing ar-eas of alopecia and scaling. (Courtesy of Elsevier Publishing.)
Fig. 3. Corynebacterium pseudotuberculosis folliculitis: circu-lar areas of crust and alopecia. (Courtesy of Elsevier Publish-ing.)
458 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
Of most concern is the finding of humans report-ing skin lesions after contact with a communityMRSA-positive affected foal, despite short-term con-tact with standard protective barriers. The isolatesfrom the foal were indistinguishable from the onesfrom the humans.12
3. Treatment of Equine Pyoderma
The antibiotic usually used for many bacterial skininfections in the horse is trimethoprim sulfa orally(30 mg/kg, q 12 h for 2–6 wk, longer for deep infec-tions).6 Interestingly, dosing intervals for IV ad-ministration of trimethoprim-sulfamethoxazole inhorses may not be appropriate for use in donkeys ormules. Donkeys eliminate the drugs rapidly com-pared with horses.13 In cases of Staphylococcus sp.
resistance to trimethoprim-sulfa drugs, enrofloxacinmay be used. Use of enrofloxacin in young horses(�2 yr old) should be avoided because of concerns ofdamage to the articular cartilage.14 A recent re-port15 on the use of an oral-gel formulation of enro-floxacin (100 mg/ml of gel) showed good clinicalefficacy for infections in several organs; however,almost one-third of the horses had some diarrhea,and 10% had oral lesions. Epstein et al.15 felt thatthis latter side effect could be overcome with admin-istration of tap water rinse of the oral cavity. In-terestingly, enrofloxacin binds to melanin in equinehair, although the clinical implication is unknown.16
In one report of 15 horses, vancomycin was used,alone or in combination with an aminoglycoside, totreat MRSA and enterococcal infections. The aver-age vancomycin dosage was 7.5 mg/kg, q 8 h, IV over30 min. The antibiotic, alone or in combinationwith an aminoglycoside, was safe and effective.Because of the problems with emerging resistance,Orsini et al.17 recommended that the use of vanco-mycin in horses be limited to cases in which cultureand susceptibility indicate effectiveness and no rea-sonable alternative treatment is available.
For localized lesions, generic mupirocin ointment2% or silver sulfadiazine creama may be effective.Shampoos such as ethyl lactateb or chlorhexidine(2%–4%) are helpful.
Dermatophilosis is caused by an actinomycetebacteria Dermatophilus congolensis. Three condi-tions must be present for Dermatophilus to manifestitself: a carrier animal, moisture, and skin abra-sions. Chronically affected animals are the pri-mary source of infection. However, they onlybecome a serious source of infection when their le-sions are moistened. This results in the release ofzoospores, the infective stage of the organism. Me-chanical transmission of the disease occurs by bothbiting and non-biting flies and possibly, fomites.Because normal healthy skin is quite impervious toinfection with D. congolensis, some pre-disposingfactor that results in decreased resistance of theskin is necessary for infection to occur; prolongedwetting of the skin by rain is one of the most prev-alent causes.
The disease is usually seen during the fall andwinter months with the dorsal surface of the animalmost commonly affected. Occasionally, the lesionsinvolve the lower extremities when animals are keptin “wet pastures” (“dew poisoning”) or if horses areleft in the stall while the stall is cleaned with high-pressure water hoses. In the early stages of thedisease, the lesions can be felt better than they canbe seen. Thick crusts can be palpated under haircoat (Fig. 5). Removing the crusts and attachedhair exposes a pink, moist skin surface with both theremoved hair and the exposed skin assuming theshape of a “paintbrush.” The under surface of thecrusts are usually concave with the roots of the hairsprotruding.
Fig. 4. Pastern folliculitis. (Courtesy of Elsevier Publishing.)
AAEP PROCEEDINGS � Vol. 52 � 2006 459
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

Diagnosis is made by the “railroad track” cocci onimpression smears: a portion of one of the crustsshould be minced and mixed with a few drops ofsterile water on a glass slide, gram stained, andexamined microscopically (Fig. 6). Alternatively,bacterial culture or histopathology may be used fordiagnosis. A thick crust composed of alternatinglayers of parakeratotic stratum corneum, dried se-
rum, and degenerating neutrophils is the most char-acteristic change. A superficial folliculitis may be aprominent feature of the disease.1 In sectionsstained with gram stain, the branching, filamentousorganisms can be observed in the crusts and in thefollicles. Treatment is removal from the wet envi-ronment, removal of crusts (with care because thesemay be painful), washing with iodophors or limesulfur, and use of antibiotics (penicillin at 22,000mg/kg procaine pen G, q 12 h, IM or trimethoprimsulfa orally with the same dosage used for staphy-lococcal pyoderma) for 7 days.18 As the crusts areimportant in contagion, these should be disposed ofrather than brushed on to the ground.
4. Dermatophytes and Malassezia
Dermatophyte infections, like pyoderma, can bevariably pruritic. The most common equine der-matophyte species isolated from horses are Tricho-phyton equinum, M. equinum, T. mentagrophytes,and T. verrucosum.1,3,19 Tack (bridles, halters, andsaddle blankets) often act as fomites. The lesionsusually appear first on the axillary/girth area andmay spread over the trunk, rump, neck, head, andlimbs (Fig. 7). Initial lesions may be urticarial innature and can progress to multi-focal, sharply de-marcated scaling and crusting areas (Figs. 8 and 9).Lesions may be superficial or deep. Superficial in-fections are more common and are manifested by thedevelopment of thick crusts or more generally, adiffuse moth-eaten appearance with desquamationand alopecia. Less commonly, deeper structuresare infected through the hair follicles, which causessmall foci of inflammation and suppuration. Asmall crust forms over the follicle, and the hair islost. However, extensive alopecia and crust forma-tion do not occur; some irritation and itching may becaused by this type. Rarely, dermatophytosis maybe limited to the coronary band (Fig. 10).
Fig. 5. Dermatophilosis: severe scaling and alopecia. (Cour-tesy of Dr. V. Fadok and Elsevier Publishing.)
Fig. 6. Dermatophilosis: branching chains of cocci (“railroadtracks”) modified Wright’s stain times 100. (Courtesy of Dr. V.Fadok and Elsevier Publishing)
Fig. 7. Dermatophytosis: circular alopecia and scaling causedby Trichophyton mentagrophytes infection. (Courtesy ofElsevier Publishing.)
460 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
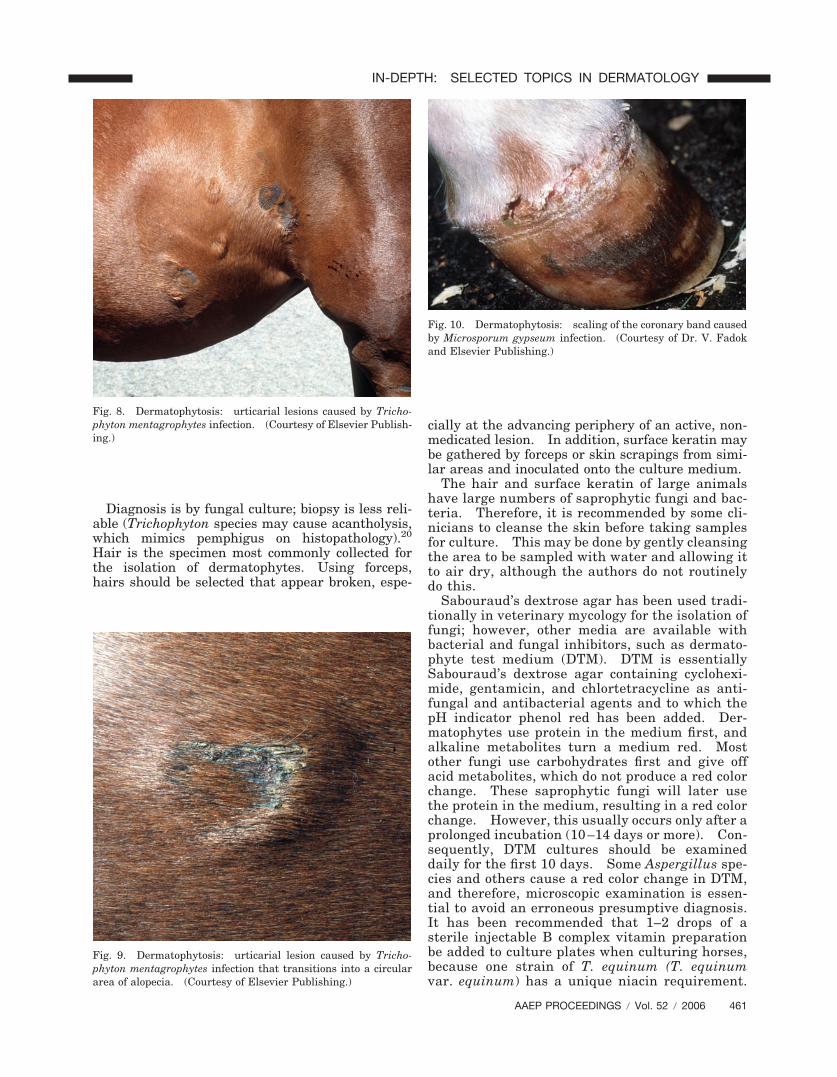
Diagnosis is by fungal culture; biopsy is less reli-able (Trichophyton species may cause acantholysis,which mimics pemphigus on histopathology).20
Hair is the specimen most commonly collected forthe isolation of dermatophytes. Using forceps,hairs should be selected that appear broken, espe-
cially at the advancing periphery of an active, non-medicated lesion. In addition, surface keratin maybe gathered by forceps or skin scrapings from simi-lar areas and inoculated onto the culture medium.
The hair and surface keratin of large animalshave large numbers of saprophytic fungi and bac-teria. Therefore, it is recommended by some cli-nicians to cleanse the skin before taking samplesfor culture. This may be done by gently cleansingthe area to be sampled with water and allowing itto air dry, although the authors do not routinelydo this.
Sabouraud’s dextrose agar has been used tradi-tionally in veterinary mycology for the isolation offungi; however, other media are available withbacterial and fungal inhibitors, such as dermato-phyte test medium (DTM). DTM is essentiallySabouraud’s dextrose agar containing cyclohexi-mide, gentamicin, and chlortetracycline as anti-fungal and antibacterial agents and to which thepH indicator phenol red has been added. Der-matophytes use protein in the medium first, andalkaline metabolites turn a medium red. Mostother fungi use carbohydrates first and give offacid metabolites, which do not produce a red colorchange. These saprophytic fungi will later usethe protein in the medium, resulting in a red colorchange. However, this usually occurs only after aprolonged incubation (10 –14 days or more). Con-sequently, DTM cultures should be examineddaily for the first 10 days. Some Aspergillus spe-cies and others cause a red color change in DTM,and therefore, microscopic examination is essen-tial to avoid an erroneous presumptive diagnosis.It has been recommended that 1–2 drops of asterile injectable B complex vitamin preparationbe added to culture plates when culturing horses,because one strain of T. equinum (T. equinumvar. equinum) has a unique niacin requirement.
Fig. 8. Dermatophytosis: urticarial lesions caused by Tricho-phyton mentagrophytes infection. (Courtesy of Elsevier Publish-ing.)
Fig. 9. Dermatophytosis: urticarial lesion caused by Tricho-phyton mentagrophytes infection that transitions into a circulararea of alopecia. (Courtesy of Elsevier Publishing.)
Fig. 10. Dermatophytosis: scaling of the coronary band causedby Microsporum gypseum infection. (Courtesy of Dr. V. Fadokand Elsevier Publishing.)
AAEP PROCEEDINGS � Vol. 52 � 2006 461
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

However, the authors do not routinely do this.Skin scrapings and hair should be inoculated ontoSabouraud’s dextrose agar and/or DTM and incu-bated at 30°C with 30% humidity. A pan of waterin the incubator will usually provide enough hu-midity. Cultures should be checked every day forgrowth. DTM may be incubated for 21 days, butcultures on Sabouraud’s agar should be allowed 30days to develop. The authors usually use Derm-Duet,c which has DTM on one side, rapid sporu-lating media (RSM) on the other side, and a well ofwater in the center. It is routinely incubated atroom temperature. T. verrucosum has been re-ported not to grow on DTM.21
Topical treatment alone is often cura-tive. Although 50% captan (2 tablespoons of thepowder in 1 gallon of water) has been touted in thepast, and while certainly safe for tack, its effective-ness has been questioned. Lime Sulfurd (1 cup to 1gallon of water) or bleach (1:10 with water) are botheffective but messy and odiferous. Miconazole orketoconazole veterinary shampoos are becomingmore widely used and may be as effective. In Eu-rope and Canada, an enilconazole rinsee is highlyeffective.
Systemic treatment is occasionally need-ed. Griseofulvin’s efficacy in horses (as well as aneffective dose) has not been thoroughly re-searched. However, a dosage of 100 mg/kg dailyfor 7–10 days has been advocated and has beenused with good success on a small number ofhorses by the authors. Griseofulvin is a terato-gen and should not be used in pregnant mares.Additionally, it is no longer available. Alterna-tively, 20% NaI may be given IV (250 ml/500 kghorse every 7 days, 1–2 times). This also is con-traindicated in pregnant mares, because it maycause abortion. Although medications such asitaconazole and fluconazole have been used totreat horses with systemic mycotic infections suchas coccidioidomycosis and aspergillosis, therehave not been any studies on their effectiveness indermatophytosis. However, the safety record inhorses in the face of the doses used (2–5 mg/kg, q12 h) are encouraging.22–24 Vaccination to T.equinum may reduce the incidence of new infec-tions and protect a high percentage (�80%) ofvaccinates from infection. This data is based onresults with an inactivated vaccine containingboth conidia and mycelial elements.25
The exact species of Malassezia growing on horses’skin is just beginning to be investigated.26 In onestudy, the Malassezia sp. isolated were identified asM. furfur, M. slooffiae, M. obtusa, M. globosa, and M.restricta.27 The authors have examined severalmares with Malassezia infections between theirmammary glands that were intensely pruritic.The mares rubbed their tails and ventral abdomens.Physical examinations showed dry, greasy-to-the-touch exudate. Cytology of the exudate showed nu-merous yeast organisms, which were identified on
culture as Malassezia species (Fig. 11). Treatmentwith a topical 2% miconazole/chlorhexidine shampoowas curative. The authors are aware of other sim-ilar cases. However, healthy non-pruritic maresmay also have large numbers of yeasts in the intra-mammary area.28
References and Footnotes1. Scott DW, Manning TO. Equine folliculitis and furunculo-
sis. Equine Pract 1980;2:11–32.2. Shimizu A, Kawano J, Ozaki J, et al. Characteristics of
Staphylococcus aureus isolated from lesions of horses. J VetMed Sci 1991;53:601–606.
3. Chiers K, Decostere A, Devriese LA, et al. Bacteriologicaland mycological findings, and in vitro antibiotic sensitivity ofpathogenic staphylococci in equine skin infections. Vet Rec2003;152:138–141.
4. Pellegrini A, Waiblinger S, Von Fellenberg R. Purification ofequine neutrophil lysozyme and its antibacterial activityagainst gram-positive and gram-negative bacteria. Vet ResCommun 1991;15:427–435.
5. Inokuma H, Kanaya N, Fujii K, et al. Equine pyodermaassociated with malnutrition and unhygienic conditions dueto neglect in a herd. J Vet Med Sci 2003;65:527–529.
6. White SD. Equine bacterial and fungal skin diseases:a diagnostic and therapeutic update. Clin Tech EquinePract 2005;4:302–310.
7. Heffner KA, White SD, Frevert CW, et al. Corynebacteriumfolliculitis in a horse. J Am Vet Med Assoc 1988;193:89–90.
8. Yasuda R, Kawano J, Onda H, et al. Methicillin-resistantcoagulase-negative staphylococci isolated from healthyhorses in Japan. Am J Vet Res 2000;61:1451–1455.
9. Busscher JF, van Duijkeren E, Sloet van Oldruitenborgh-Oosterbaan MM. The prevalence of methicillin-resistantstaphylococci in healthy horses in the Netherlands. Vet Mi-crobiol 2006;113:131–136.
10. Weese JS, Rousseau J, Traub-Dargatz JL, et al. Commu-nity-associated methicillin-resistant Staphylococcus aureusin horses and humans who work with horses. J Am Vet MedAssoc 2005;226:580–583.
11. Cuny C, Kuemmerle J, Stanek C, et al. Emergence of MRSAinfections in horses in a veterinary hospital: strain charac-terisation and comparison with MRSA from humans. EurSurveill 2006;11:44–47.
12. Weese JS, Caldwell F, Willey BM, et al. An outbreak ofmethicillin-resistant Staphylococcus aureus skin infectionsresulting from horse to human transmission in a veterinaryhospital. Vet Microbiol 2005;114:160–164.
Fig. 11. Cytology of Malassezia sp. from intermammary debrisfrom a healthy mare. (Courtesy of Elsevier Publishing.)
462 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
13. Peck KE, Matthews NS, Taylor TS, et al. Pharmacokineticsof sulfamethoxazole and trimethoprim in donkeys, mules,and horses. Am J Vet Res 2002;63:349–353.
14. Egerbacher M, Edinger J, Tschulenk W. Effects of enro-floxacin and ciprofloxacin hydrochloride on canine and equinechondrocytes in culture. Am J Vet Res 2001;62:704–708.
15. Epstein K, Cohen N, Boothe D, et al. Pharmacokinetics,stability, and retrospective analysis of use of an oral gelformulation of the bovine injectable enrofloxacin in horses.Vet Ther 2004;5:155–167.
16. Dunnett M, Richardson DW, Lees P. Detection of enrofloxa-cin and its metabolite ciprofloxacin in equine hair. Res VetSci 2004;77:143–151.
17. Orsini JA, Snooks-Parsons C, Stine L, et al. Vancomycin forthe treatment of methicillin-resistant staphylococcal and en-terococcal infections in 15 horses. Can J Vet Res 2005;69:278–286.
18. Outerbridge CA, Ihrke PJ. Folliculitis: staphylococcalpyoderma, dermatophilosis, dermatophytosis. In: Robin-son NE, ed. Current therapy in equine medicine, 5th ed. St.Louis: W.B. Saunders, 2003;197–200.
19. Kane J, Padhye AA, Ajello L. Microsporum equinum inNorth America. J Clin Microbiol 1982;16:943–947.
20. Scott DW. Marked acantholysis associated with dermato-phytosis due to Trichophyton equinum in two horses. VetDermatol 1994;5:105–110.
21. Scott DW, Miller WH. Equine dermatology. St. Louis:W.B. Saunders, 2003;96.
22. Foley JP, Legendre AM. Treatment of coccidioidomycosisosteomyelitis with itraconazole in a horse. A brief report.J Vet Int Med 1992;6:333–334.
23. Korenek NL, Legendre AM, Andrews FM, et al. Treatmentof mycotic rhinitis with itraconazole in three horses. J VetInt Med 1994;8:224–227.
24. Taintor J, Crowe C, Hancock S, et al. Treatment of conid-iobolomycosis with fluconazole in two pregnant mares. J VetInt Med 2004;18:363–364.
25. Pier AC, Zancanella PJ. Immunization of horses againstdermatophytosis caused by Trichophyton equinum. EquinePract 1993;15:23–27.
26. Nell A, James SA, Bond CJ, et al. Identification and distri-bution of a novel Malassezia species yeast on normal equineskin. Vet Rec 2002;150:395–398.
27. Crespo MJ, Abarca ML, Cabanes FJ. Occurrence ofMalassezia spp. in horses and domestic ruminants. Mycoses2002;45:333–337.
28. White SD, Vandenabeele SIJ, Drazenovich N, et al.Malassezia species isolated from the intermammary and pre-putial fossa areas of horses. J Vet Int Med 2006;20:395–398.
aSilvadene, Monarch Pharmaceuticals, Inc., Bristol, TN 37620.bEtiderm, VIRBAC, Ft. Worth, TX 76137.cDermDuet, Bacti-Labs, Mountain View, CA 94042.dLymDyp, Miami, FL 33169.eImaveral, Janssen-Cilag Animal Health 1 rue Camille, Des-
moulins, France.
Insect Hypersensitivity
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
Insect hypersensitivity is the most common cause ofequine pruritus. There are four contributingcauses of pruritus.
1. The bite itself, which is painful because ofthe chewing mouthparts of these flies.
2. An immediate (i.e., type 1) hypersensitivityto salivary antigens of biting insects or inhala-tion of desiccated insects, which is supportedby the increased immunohistochemicalpresence of IgE in skin of horses with insecthypersensitivity and detection of IgG and IgEserum antibodies to Culicoides salivary glandantigens in horses with insect dermalhypersensitivity.1,2
3. A delayed (i.e., type 4) and cutaneous baso-phil hypersensitivity reaction that is similarto flea-allergy dermatitis in dogs and cats.
4. Langerhans’ cells and T-lymphocytes cyto-kine production.3–5
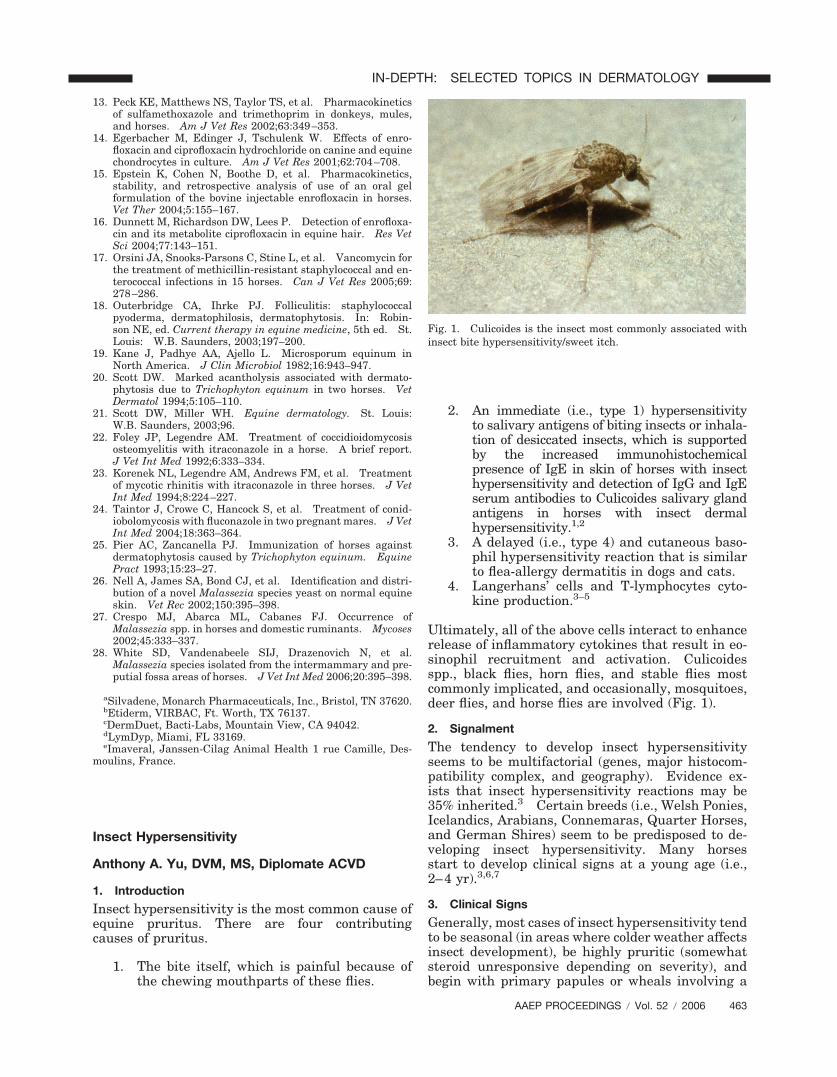
Ultimately, all of the above cells interact to enhancerelease of inflammatory cytokines that result in eo-sinophil recruitment and activation. Culicoidesspp., black flies, horn flies, and stable flies mostcommonly implicated, and occasionally, mosquitoes,deer flies, and horse flies are involved (Fig. 1).
2. Signalment
The tendency to develop insect hypersensitivityseems to be multifactorial (genes, major histocom-patibility complex, and geography). Evidence ex-ists that insect hypersensitivity reactions may be35% inherited.3 Certain breeds (i.e., Welsh Ponies,Icelandics, Arabians, Connemaras, Quarter Horses,and German Shires) seem to be predisposed to de-veloping insect hypersensitivity. Many horsesstart to develop clinical signs at a young age (i.e.,2–4 yr).3,6,7
3. Clinical Signs
Generally, most cases of insect hypersensitivity tendto be seasonal (in areas where colder weather affectsinsect development), be highly pruritic (somewhatsteroid unresponsive depending on severity), andbegin with primary papules or wheals involving a
Fig. 1. Culicoides is the insect most commonly associated withinsect bite hypersensitivity/sweet itch.
AAEP PROCEEDINGS � Vol. 52 � 2006 463
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
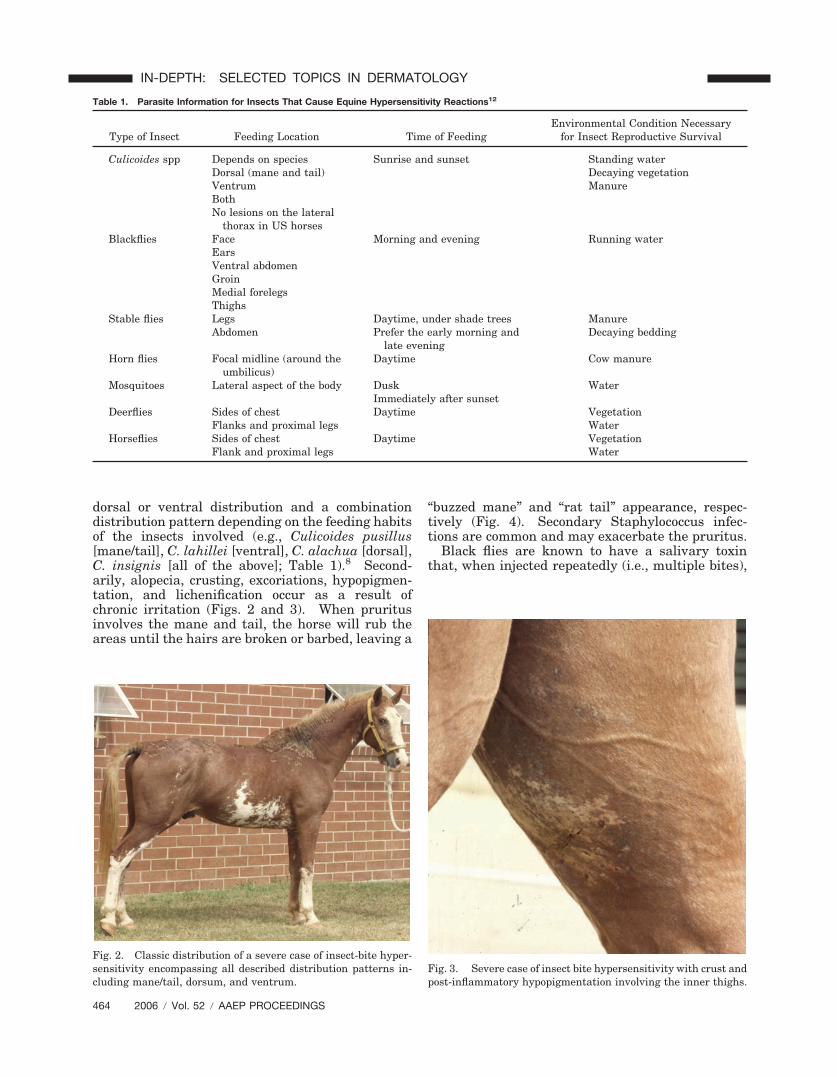
dorsal or ventral distribution and a combinationdistribution pattern depending on the feeding habitsof the insects involved (e.g., Culicoides pusillus[mane/tail], C. lahillei [ventral], C. alachua [dorsal],C. insignis [all of the above]; Table 1).8 Second-arily, alopecia, crusting, excoriations, hypopigmen-tation, and lichenification occur as a result ofchronic irritation (Figs. 2 and 3). When pruritusinvolves the mane and tail, the horse will rub theareas until the hairs are broken or barbed, leaving a
“buzzed mane” and “rat tail” appearance, respec-tively (Fig. 4). Secondary Staphylococcus infec-tions are common and may exacerbate the pruritus.
Black flies are known to have a salivary toxinthat, when injected repeatedly (i.e., multiple bites),
Fig. 2. Classic distribution of a severe case of insect-bite hyper-sensitivity encompassing all described distribution patterns in-cluding mane/tail, dorsum, and ventrum.
Table 1. Parasite Information for Insects That Cause Equine Hypersensitivity Reactions12
Type of Insect Feeding Location Time of FeedingEnvironmental Condition Necessary
for Insect Reproductive Survival
Culicoides spp Depends on species Sunrise and sunset Standing waterDorsal (mane and tail) Decaying vegetationVentrum ManureBothNo lesions on the lateral
thorax in US horsesBlackflies Face Morning and evening Running water
EarsVentral abdomenGroinMedial forelegsThighs
Stable flies Legs Daytime, under shade trees ManureAbdomen Prefer the early morning and
late eveningDecaying bedding
Horn flies Focal midline (around theumbilicus)
Daytime Cow manure
Mosquitoes Lateral aspect of the body Dusk WaterImmediately after sunset
Deerflies Sides of chest Daytime VegetationFlanks and proximal legs Water
Horseflies Sides of chest Daytime VegetationFlank and proximal legs Water
Fig. 3. Severe case of insect bite hypersensitivity with crust andpost-inflammatory hypopigmentation involving the inner thighs.
464 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

is capable of causing capillary permeability leadingto shock and even death.6 Horsefly and deerflybites differ from those of other insects in that theytypically cause nodular lesions that ulcerate.3,6
Respiratory signs (i.e., recurrent airway obstructionthat is similar to reactions noted in humans withasthma and arthropod hypersensitivity) have beenassociated with positive skin-test reactions to onlyCulicoides spp. and mosquitoes.7,9,10
4. Differential Diagnoses
The primary differentials for insect hypersensitiv-ity include atopy, food allergy, and a stable vice.Secondary bacterial infections are common. Pri-mary or secondary dermatophytosis should alwaysbe considered, particularly if multiple horses areaffected in the same environment. Some species(e.g., C. variipennis) transmit the filarid parasite,Onchocerca cervicalis, which in itself may resultin similar clinical signs with ventral crusting/pru-ritus. A regular deworming protocol with iver-mectin would minimize the likelihood of
onchocerciasis. Other ectoparasites such as lice,Chorioptes, and Psoroptes should be ruled out be-fore pursuing extensive diagnostics.
5. Diagnosis
Diagnosis of insect hypersensitivity is based on his-tory (single horse involvement and seasonality; e.g.,spring [C. niger/alachua], summer [C. stellifer], andfall [C. insignis] depending on the region), distribu-tion pattern (e.g., horn flies focus on the umbilicalregion), and an inspection of the patient’s environ-ment for evidence of insect breeding grounds (for-ested area or ponds/still water within a mile; Table1). Skin scrapings are helpful in ruling out ecto-parasite problems (e.g., Chorioptes and psoroptes).Skin cytologies and/or cultures are useful in deter-mining whether a bacterial (Staphylococcus or Der-matophilus) and/or fungal infection (Trichophytonmentagrophytes, Microsporum canis, or Microspo-rum gypseum) is present.
There are diagnostic tests for insect hypersensi-tivity.
1. A stringent ectoparasiticidal trial usingKnockout L.A.a up to every other day de-pending on the severity of the condition andparasite load in the environment. Onestudy noted significant improvement withevery other week application in cases of sus-pected Culicoides hypersensitivity.11
2. Intradermal skin testing with several insectsincluding Culicoides variipennis, whichcrossreacts with other species of Culicoides,stable flies, mosquitoes, deer flies, horse flies,and black flies, because several types of in-sects can cause allergies in horses; however,many have cross-reactive antigens (Fig.5).3,6,7,12–14
3. In vitro testing is not reliable in horses.15
Fig. 4. Characteristic rubbed tail of a horse with insect-bitehypersensitivity.
Fig. 5. Trans-illuminated positive intradermal reactions to in-sect allergens in a horse with suspected insect bite hypersensi-tivity.
AAEP PROCEEDINGS � Vol. 52 � 2006 465
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
4. Dermatopathology is supportive but not con-clusive of insect hypersensitivity.3,6
6. Conclusion
Insect hypersensitivities can manifest as a singlecondition or as part of a spectrum of allergic condi-tions including atopy, food allergy, and contact hy-persensitivity. To successfully manage any equinepatient with allergies, every effort should be made tobecome familiar with the feeding habits and envi-ronmental requirements for reproduction for in-sects. This will help to successfully eliminate theircontribution to the allergen load.
References and Footnote1. van der Haegen A, Griot-Wenk M, Welle M, et al. Immuno-
globulin-E-bearing cells in skin biopsies of horses with insectbite hypersensitivity. Equine Vet J 2001;33:699–706.
2. Wilson AD, Harwood LJ, Bjornsdottir S, et al. Detection ofIgG and IgE serum antibodies to Culicoides salivary glandantigens in horses with insect dermal hypersensitivity (sweetitch). Equine Vet J 2001;33:707–713.
3. Scott DW, Miller WH. Insect hypersensitivity. In: ScottDW, Miller WH, eds. Equine dermatology. Philadelphia:W.B. Saunders, 2003;458–467.
4. Kurotaki T, Narayama K, Arai Y, et al. Langerhans cellswithin the follicular epithelium and the intradermal sweatduct in equine insect hypersensitivity “Kasen.” J Vet MedSci 2002;64:539–541.
5. McKelvie J, Foster AP, Hamblin AS, et al. Culicoides anti-gen extract stimulates equine blood mononuclear (BMN) cellproliferation and the release of eosinophil adherence-induc-ing factor(s). Res Vet Sci 2001;70:115–122.
6. Pascoe R, Knottenbelt DC. Immune-mediated/allergic dis-eases. In: Pascoe R, Knottenbelt DC, eds. Manual of equinedermatology. London: W.B. Saunders, 1999;155–181.
7. Fadok VA. Update on equine allergies. Vet Allergy ClinImmunol 1997;15:69–76.
8. Greiner EC, Fadok VA, Rabin EB. Equine culicoides hyper-sensitivity in Florida: biting midges aspirated from horses.Med Vet Entomol 1990;4:375–381.
9. Baur X, Liebers V. Insect immunoglobulins (Chi t I) of theDiptera genus chironomus are relevant environmental, occu-pational and hobby-related allergens. Int Arch Occup Envi-ron Health 1992;64:185–188.
10. Bernton HS, Browne H. Insect allergy: preliminary stud-ies of the cockroach. J Allergy Clin Immunol 1992;25:506–513.
11. Bourdeau PJ, Beis C, Chouilly C, et al. Evaluation of per-methrin and pyriproxyfen containing spray in the treatmentof sweet itch in 25 horses, in Proceedings. 15th AnnualMember’s Meeting of the American Academy of VeterinaryDermatology/American College of Veterinary Dermatology1999;13–14.
12. Rees C. Diagnosing and managing equine pruritus: insecthypersensitivity. Compend Cont Educ Pract Vet 2005;27:629–636.
13. Morris DO, Lindborg S. Determination of ‘irritant’ thresh-old concentrations for intradermal testing with allergenicinsect extracts in normal horses. Vet Dermatol 2003;14:31–1436.
14. Grier TJ, Willis EL, Esch RE, et al. Canine insect hyper-sensitivity: immunochemical evidence for common or cross-reactive antigens. Vet Dermatol 1994;5:129–130.
15. Lorch G, Hillier A, Kwochka KW, et al. Comparison of im-mediate intradermal test reactivity with serum IgE quanti-tation by use of a radioallergosorbent test and two ELISAs inhorses with and without atopy. J Am Vet Med Assoc 2001;218:1314–1322.
aKnockout L.A., Virbac, Peakhurst, NSW 2210, Australia.
Atopy
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
Manifestations of equine allergies include derma-toses (hives, pruritus, scale/crust, leukotrichia, ornodules) as well as respiratory conditions (recur-rent airway obstruction [RAO]). Currently, thepathomechanism is not completely understoodboth in human and veterinary medicine. Aller-gies seem to be a multifactorial condition involv-ing immunoglobulins, major histocompatibilitycomplex (MHC-II), cytokines, chemokines, and theneuroendocrine system. The classic type I hyper-sensitivity pathway continues to play an intrinsicrole in the production of an allergic response.The inherited predisposition to form sensitizingantibodies to environmental allergens such asmolds, dust, and pollens of grasses, weeds, andtrees results in the production of antigen specificimmunoglobulin E (IgE), which then fixes to tissuemast cells. Cross linking of mast cell bound IgEresults in release of inflammatory mediators,which culminates in pruritus, urticaria, and anallergic bronchitis. Other genes, such as the betachain of the high affinity IgE receptor found onmast cells and basophils, may also regulate sus-ceptibility to atopy. We now realize that this tra-ditional type-I allergic response is only the tip ofthe iceberg, and its role still remains controversialin the horse, especially in cases of RAO.1–3
In humans, the allergic response has been furtherelaborated to involve T lymphocytes, particularlythe T helper cell paradigm. The T helper 2 cell(Th2), in fact, produces cytokines such as interleu-kins (IL) 4, 5, 6, 10, and 13, of which IL4 and IL13are essential for the B-cell immunoglobulin classswitching to IgE. In non-atopic individuals, the Thelper 1 cell line (Th1) produces interferon (IFN)and IL2, which in turn suppress the proliferation ofallergy promoting Th2 cells, and are responsible forthe local immune defense system.
Recently, bronchoalveolar lavage fluid harvestedfrom antigen challenged allergen induced RAOhorses had increased numbers of Th2 cells that pro-duced the classic allergic profile (increased IL4 andIL5 and decreased IFN).4 Many studies show thehorse’s ability to react to allergens introduced intra-dermally; however, controversy surrounds the sig-nificance of these reactions.5–13 It is obvious thatfurther studies are necessary to delineate the aller-gic behavior of the equine immune system.
2. Signalment
Two recent studies from California revealed a me-dian age of onset of 5–6.5 yr of age with a range of2–12 yr.14,15 Cannon cautions that horses are oftensold during the “good” season and develop allergiestheir next “bad” season, which makes age of onsetdifficult to determine. As well, pre-disposed breeds
466 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
include Thoroughbreds, Quarter Horses, Warm-bloods, Arabians, and Morgans, and males (usuallygeldings) were almost twice as likely as mares tohave atopy. However, the study populations weresmall, regional, and potentially, socio-economicallyinfluenced. It will take a multicenter (general andreferral practice) study or verifiable survey of thou-sands of allergic horses to get a true picture of thesignalment of equine allergic dermatoses.
3. Clinical Signs
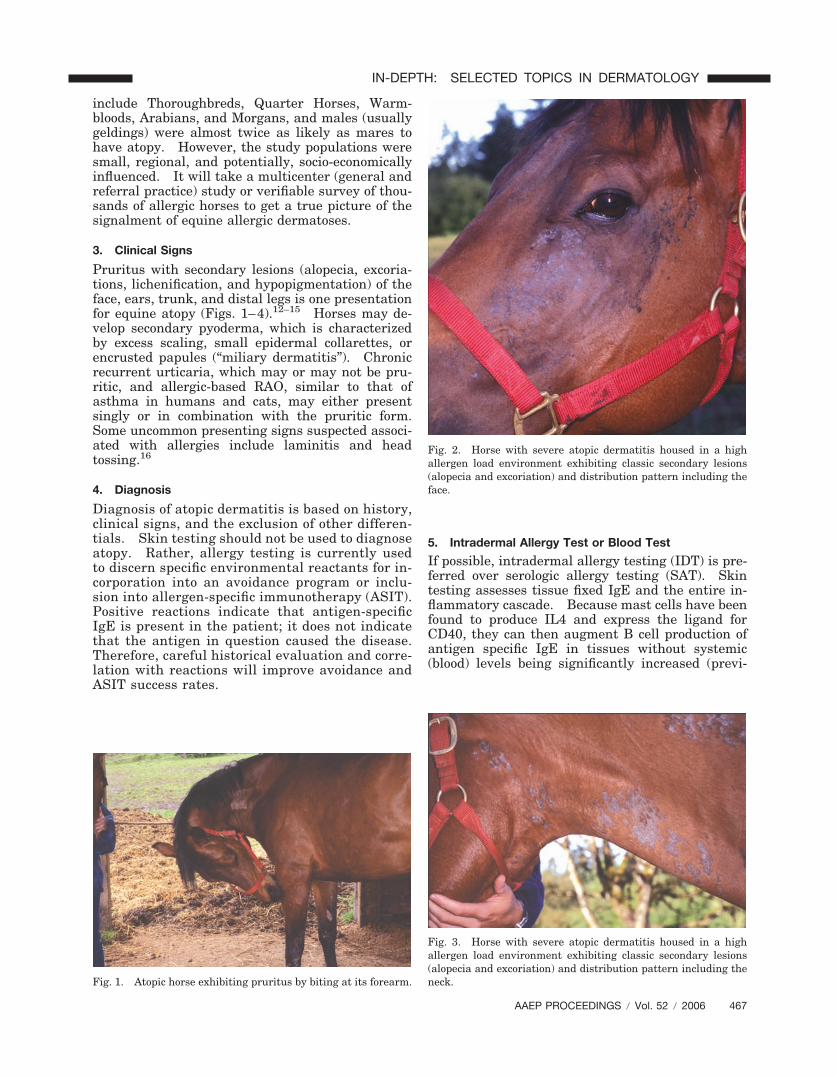
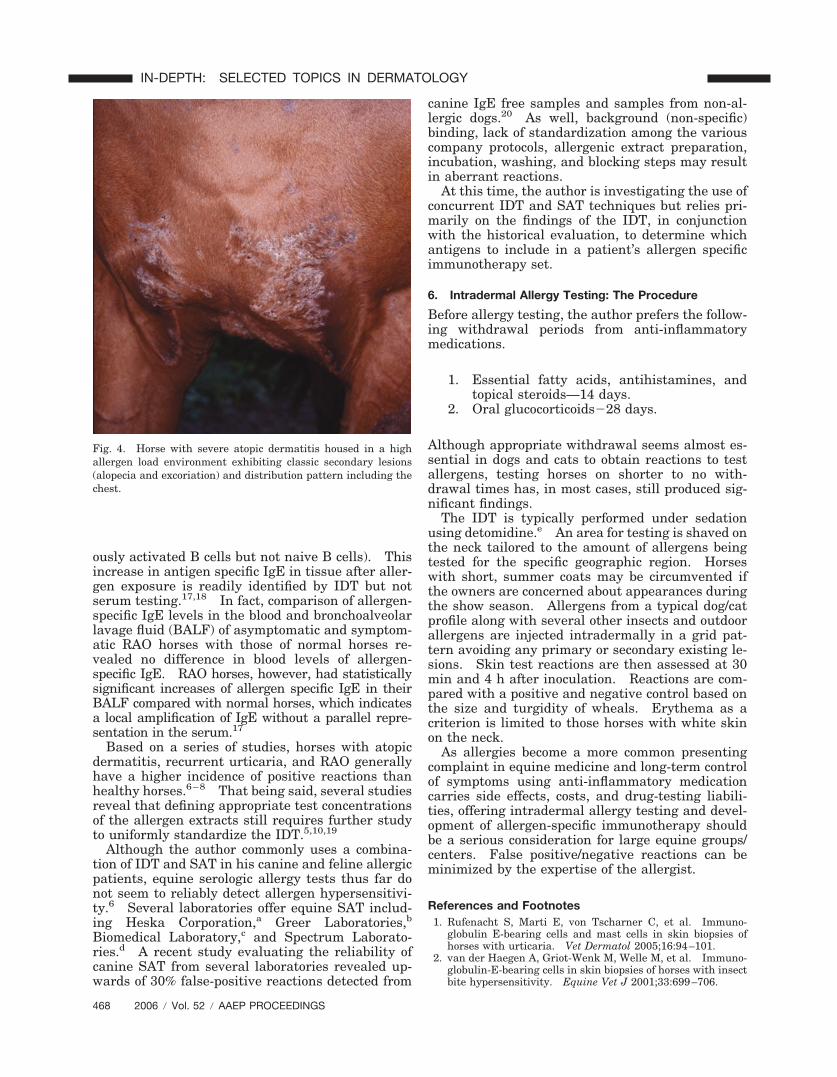
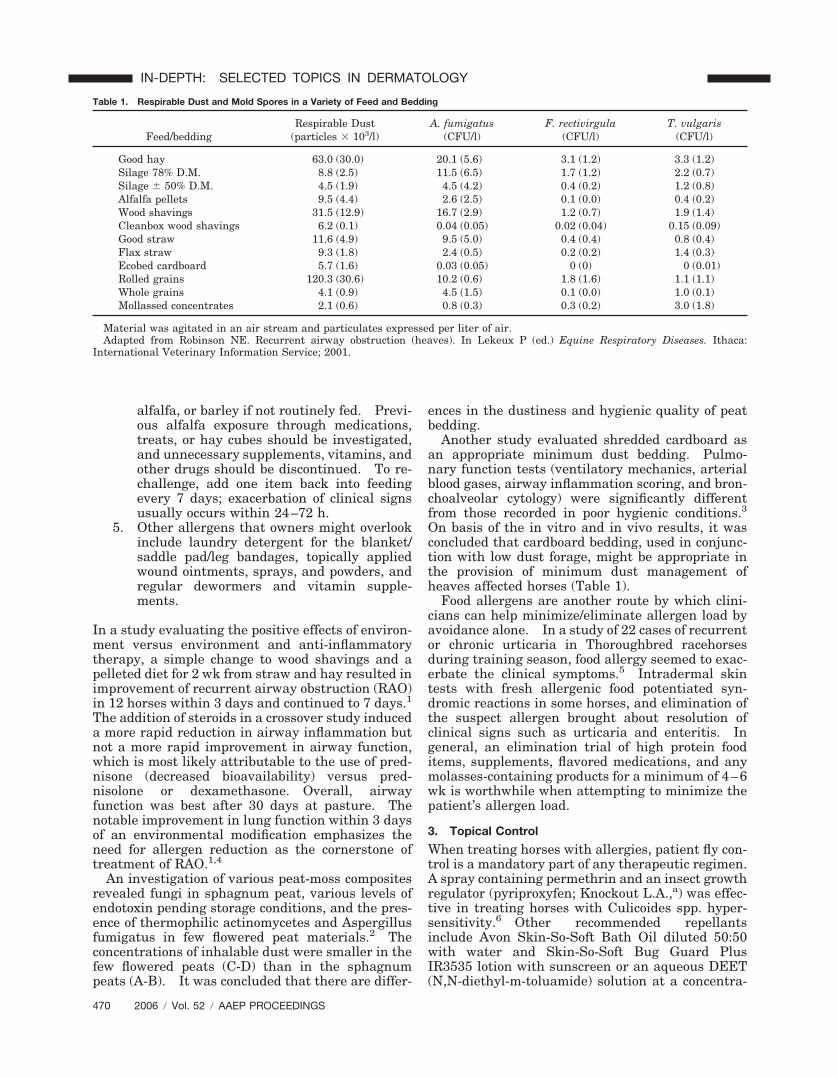
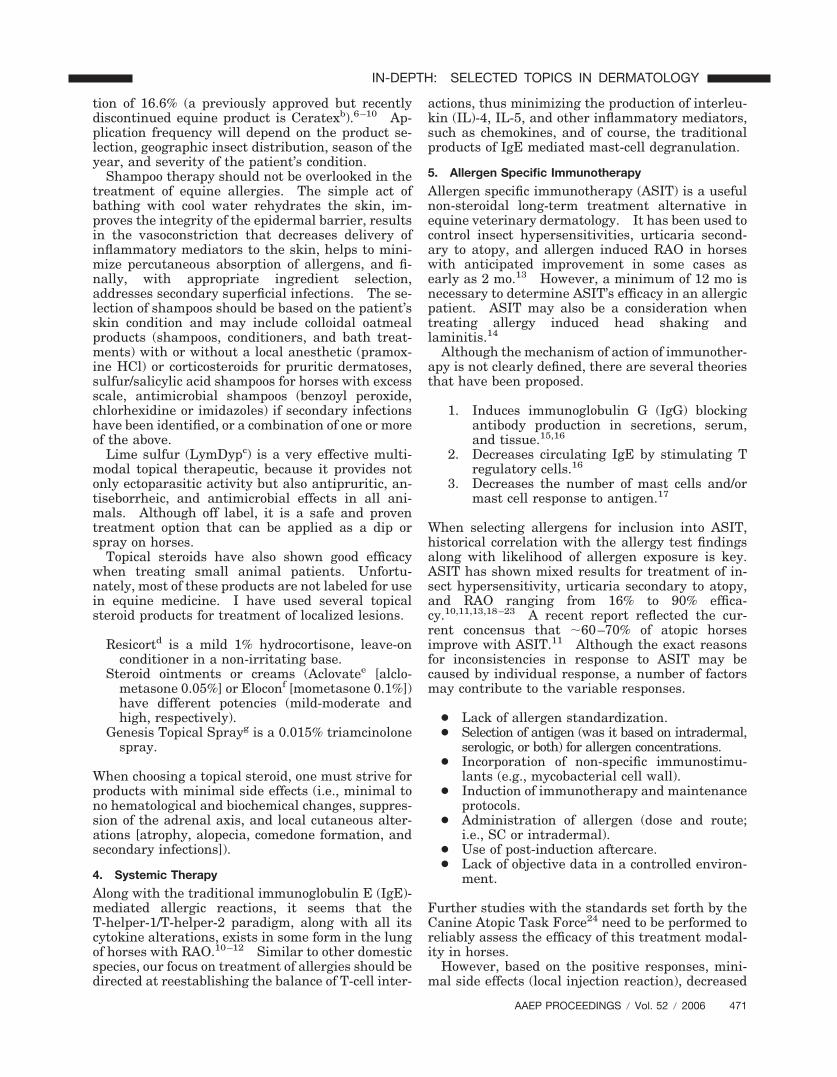
Pruritus with secondary lesions (alopecia, excoria-tions, lichenification, and hypopigmentation) of theface, ears, trunk, and distal legs is one presentationfor equine atopy (Figs. 1–4).12–15 Horses may de-velop secondary pyoderma, which is characterizedby excess scaling, small epidermal collarettes, orencrusted papules (“miliary dermatitis”). Chronicrecurrent urticaria, which may or may not be pru-ritic, and allergic-based RAO, similar to that ofasthma in humans and cats, may either presentsingly or in combination with the pruritic form.Some uncommon presenting signs suspected associ-ated with allergies include laminitis and headtossing.16
4. Diagnosis
Diagnosis of atopic dermatitis is based on history,clinical signs, and the exclusion of other differen-tials. Skin testing should not be used to diagnoseatopy. Rather, allergy testing is currently usedto discern specific environmental reactants for in-corporation into an avoidance program or inclu-sion into allergen-specific immunotherapy (ASIT).Positive reactions indicate that antigen-specificIgE is present in the patient; it does not indicatethat the antigen in question caused the disease.Therefore, careful historical evaluation and corre-lation with reactions will improve avoidance andASIT success rates.
5. Intradermal Allergy Test or Blood Test
If possible, intradermal allergy testing (IDT) is pre-ferred over serologic allergy testing (SAT). Skintesting assesses tissue fixed IgE and the entire in-flammatory cascade. Because mast cells have beenfound to produce IL4 and express the ligand forCD40, they can then augment B cell production ofantigen specific IgE in tissues without systemic(blood) levels being significantly increased (previ-
Fig. 1. Atopic horse exhibiting pruritus by biting at its forearm.
Fig. 2. Horse with severe atopic dermatitis housed in a highallergen load environment exhibiting classic secondary lesions(alopecia and excoriation) and distribution pattern including theface.
Fig. 3. Horse with severe atopic dermatitis housed in a highallergen load environment exhibiting classic secondary lesions(alopecia and excoriation) and distribution pattern including theneck.
AAEP PROCEEDINGS � Vol. 52 � 2006 467
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
ously activated B cells but not naive B cells). Thisincrease in antigen specific IgE in tissue after aller-gen exposure is readily identified by IDT but notserum testing.17,18 In fact, comparison of allergen-specific IgE levels in the blood and bronchoalveolarlavage fluid (BALF) of asymptomatic and symptom-atic RAO horses with those of normal horses re-vealed no difference in blood levels of allergen-specific IgE. RAO horses, however, had statisticallysignificant increases of allergen specific IgE in theirBALF compared with normal horses, which indicatesa local amplification of IgE without a parallel repre-sentation in the serum.17
Based on a series of studies, horses with atopicdermatitis, recurrent urticaria, and RAO generallyhave a higher incidence of positive reactions thanhealthy horses.6–8 That being said, several studiesreveal that defining appropriate test concentrationsof the allergen extracts still requires further studyto uniformly standardize the IDT.5,10,19
Although the author commonly uses a combina-tion of IDT and SAT in his canine and feline allergicpatients, equine serologic allergy tests thus far donot seem to reliably detect allergen hypersensitivi-ty.6 Several laboratories offer equine SAT includ-ing Heska Corporation,a Greer Laboratories,b
Biomedical Laboratory,c and Spectrum Laborato-ries.d A recent study evaluating the reliability ofcanine SAT from several laboratories revealed up-wards of 30% false-positive reactions detected from
canine IgE free samples and samples from non-al-lergic dogs.20 As well, background (non-specific)binding, lack of standardization among the variouscompany protocols, allergenic extract preparation,incubation, washing, and blocking steps may resultin aberrant reactions.
At this time, the author is investigating the use ofconcurrent IDT and SAT techniques but relies pri-marily on the findings of the IDT, in conjunctionwith the historical evaluation, to determine whichantigens to include in a patient’s allergen specificimmunotherapy set.
6. Intradermal Allergy Testing: The Procedure
Before allergy testing, the author prefers the follow-ing withdrawal periods from anti-inflammatorymedications.
1. Essential fatty acids, antihistamines, andtopical steroids—14 days.
2. Oral glucocorticoids�28 days.
Although appropriate withdrawal seems almost es-sential in dogs and cats to obtain reactions to testallergens, testing horses on shorter to no with-drawal times has, in most cases, still produced sig-nificant findings.
The IDT is typically performed under sedationusing detomidine.e An area for testing is shaved onthe neck tailored to the amount of allergens beingtested for the specific geographic region. Horseswith short, summer coats may be circumvented ifthe owners are concerned about appearances duringthe show season. Allergens from a typical dog/catprofile along with several other insects and outdoorallergens are injected intradermally in a grid pat-tern avoiding any primary or secondary existing le-sions. Skin test reactions are then assessed at 30min and 4 h after inoculation. Reactions are com-pared with a positive and negative control based onthe size and turgidity of wheals. Erythema as acriterion is limited to those horses with white skinon the neck.
As allergies become a more common presentingcomplaint in equine medicine and long-term controlof symptoms using anti-inflammatory medicationcarries side effects, costs, and drug-testing liabili-ties, offering intradermal allergy testing and devel-opment of allergen-specific immunotherapy shouldbe a serious consideration for large equine groups/centers. False positive/negative reactions can beminimized by the expertise of the allergist.
References and Footnotes1. Rufenacht S, Marti E, von Tscharner C, et al. Immuno-
globulin E-bearing cells and mast cells in skin biopsies ofhorses with urticaria. Vet Dermatol 2005;16:94–101.
2. van der Haegen A, Griot-Wenk M, Welle M, et al. Immuno-globulin-E-bearing cells in skin biopsies of horses with insectbite hypersensitivity. Equine Vet J 2001;33:699–706.
Fig. 4. Horse with severe atopic dermatitis housed in a highallergen load environment exhibiting classic secondary lesions(alopecia and excoriation) and distribution pattern including thechest.
468 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

3. van der Haegen A, Kunzle F, Gerber V, et al. Mast cells andIgE-bearing cells in lungs of RAO-affected horses. Vet Im-munol Immunopathol 2005;108:325–334.
4. Cordeau ME, Joubert P, Dewachi O, et al. IL-4, IL-5 andIFN-gamma mRNA expression in pulmonary lymphocytesin equine heaves. Vet Immunol Immunopathol 2004;97:87–96.
5. Kolm-Stark G, Wagner R. Intradermal skin testing in Ice-landic horses in Austria. Equine Vet J 2002;34:405–410.
6. Lorch G, Hillier A, Kwochka KW, et al. Comparison of im-mediate intradermal test reactivity with serum IgE quanti-tation by use of a radioallergosorbent test and two ELISA inhorses with and without atopy. J Am Vet Med Assoc 2001;218:1314–1322.
7. Lorch G, Hillier A, Kwochka KW, et al. Results of intrader-mal tests in horses without atopy and horses with chronicobstructive pulmonary disease. Am J Vet Res 2001;62:389–397.
8. Lorch G, Hillier A, Kwochka KW, et al. Results of intrader-mal tests in horses without atopy and horses with atopicdermatitis or recurrent urticaria. Am J Vet Res 2001;62:1051–1059.
9. Jose-Cunilleras E, Kohn CW, Hillier A, et al. Intradermaltesting in healthy horses and horses with chronic obstructivepulmonary disease, recurrent urticaria, or allergic dermati-tis. J Am Vet Med Assoc 2001;219:1115–1121.
10. Lebis C, Bourdeau P, Marzin-Keller F. Intradermal skintests in equine dermatology: a study of 83 horses. EquineVet J 2002;34:666–671.
11. Fadok VA. Update on equine allergies. J Vet Allergy ClinImmunol 1997;5:68–76.
12. Scott DW, Miller WM. Skin immune system and allergicskin diseases. In: Scott DW, Miller WM, eds. Equine der-matology. Philadelphia: W.B. Saunders, 2003;436–448.
13. Wong D, Manning T. Equine skin: structure, immunologicfunction, and methods of diagnosing disease. Compend ContEduc Pract Vet 2005;27:463–473.
14. Cannon A. Clinical signs of allergy, in Proceedings. 21stNorth American Veterinary Dermatology Forum 2006;59–61.
15. White SD. Advances in equine atopic dermatitis, serologicand intradermal allergy testing. Clin Tech Equine Pract2005;4:311–313.
16. Tallarico NJ, Tallarico CM. Results of intradermal allergytesting and treatment by hyposensitization of 64 horses withchronic obstructive pulmonary disease, urticaria, headshak-ing, and/or reactive airway disease. J Vet Allergy Clin Im-munol 1998;6:25–35.
17. Halliwell REW, McGorum BC, Irving P, et al. Local andsystemic antibody production in horses affected with chronicobstructive pulmonary disease. Vet Immunol Immuno-pathol 1993;38:201–215.
18. Schmallenbach KH, Rahman I, Sasse HH, et al. Studies onpulmonary and systemic Aspergillus fumigatus-specific IgEand IgG antibodies in horses affected with chronic obstruc-tive pulmonary disease (COPD). Vet Immunol Immuno-pathol 1998;66:245–256.
19. Morris DO, Lindborg S. Determination of ‘irritant’ thresh-old concentrations for intradermal testing with allergenicinsect extracts in normal horses. Vet Dermatol 2003;14:31–36.
20. DeBoer DJ, Verbrugge MJ. Results of canine serum aller-gen-specific IgE determinations performed by commerciallaboratories on canine IgE-free samples and on samples fromnonallergic dogs, in Proceedings. 20th Annual North Amer-ican Veterinary Dermatology Forum 2005;191.
aHeska Corporation, Fort Collins, CO 80525.bGreer Laboratories, Lenoir, NC 28645.cBiomedical Laboratory, Austin, TX 78712.dSpectrum Laboratories, Tempe, AZ 85281.eDormosedan, Pfizer, Exton, PA 19380.
Treatment of Equine Allergies
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
One trend that is coming to light is the fact thathorses, as well as humans, dogs, and cats, commonlyhave combination allergies (i.e., insect allergies,atopy, and drug and food hypersensitivities). It is,therefore, important to keep in mind key conceptssuch as “allergic threshold” and “summation of ef-fect” when diagnosing and treating equine allergicdermatoses. That is, a successful therapeutic pro-tocol must encompass the patient’s pre-disposing/environmental influences along with treating thesecondary perpetuating factors (bacteria andMalassezia), all while specifically targeting the pri-mary etiology. Regardless of which combination oftherapeutic options is selected for the horse, theclient must be educated regarding the chronicity ofequine allergies, the workload involved in multimo-dal therapy, and the realistic expectations for con-trol of the condition.
2. Environmental Control
Avoidance or reduced allergen exposure is the besttreatment for all allergic forms. Although this op-tion if often impractical, it must be offered and con-sidered as an adjunct to systemic therapy by theowner in lieu of lifelong anti-inflammatory therapy.There are many recommendations of how to reduce/avoid allergen exposure.
1. Move from the current environment, whichmay include moving to a different part of thecountry, moving down the road, moving to adifferent barn (bank barn versus open air), orrestricting indoor/outdoor activity dependingon allergic reactions (put horses with moldspore and dust allergies to pasture and keephorses with summer pasture associated al-lergies indoors).
2. Minimize dust exposure in the barn, whichmay include switching to rubber mats and/orminimum dust generating bedding,1–4 orswitching to grass silage, hydroponic or wetdown hay, and/or pelleted rations.
3. Control insects in the environment by mov-ing horses away from standing water, ma-nure piles, compost, and cattle, stablingbefore dusk until after dawn, using fly sheetsor masks sprayed with permethrin repellant,using a �32 � 32 per 2.5-cm grid meshing,placing box fans within the stall, using time-release insecticide sprays, or placing flywasps in compost and manure areas and fishin ponds.
4. Use dietary trials to diagnose food hypersen-sitivity or intolerance. Current recommen-dations consist of a 4- to 6-wk trial usingnovel food sources like timothy, rolled oats,
AAEP PROCEEDINGS � Vol. 52 � 2006 469
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
alfalfa, or barley if not routinely fed. Previ-ous alfalfa exposure through medications,treats, or hay cubes should be investigated,and unnecessary supplements, vitamins, andother drugs should be discontinued. To re-challenge, add one item back into feedingevery 7 days; exacerbation of clinical signsusually occurs within 24–72 h.
5. Other allergens that owners might overlookinclude laundry detergent for the blanket/saddle pad/leg bandages, topically appliedwound ointments, sprays, and powders, andregular dewormers and vitamin supple-ments.
In a study evaluating the positive effects of environ-ment versus environment and anti-inflammatorytherapy, a simple change to wood shavings and apelleted diet for 2 wk from straw and hay resulted inimprovement of recurrent airway obstruction (RAO)in 12 horses within 3 days and continued to 7 days.1
The addition of steroids in a crossover study induceda more rapid reduction in airway inflammation butnot a more rapid improvement in airway function,which is most likely attributable to the use of pred-nisone (decreased bioavailability) versus pred-nisolone or dexamethasone. Overall, airwayfunction was best after 30 days at pasture. Thenotable improvement in lung function within 3 daysof an environmental modification emphasizes theneed for allergen reduction as the cornerstone oftreatment of RAO.1,4
An investigation of various peat-moss compositesrevealed fungi in sphagnum peat, various levels ofendotoxin pending storage conditions, and the pres-ence of thermophilic actinomycetes and Aspergillusfumigatus in few flowered peat materials.2 Theconcentrations of inhalable dust were smaller in thefew flowered peats (C-D) than in the sphagnumpeats (A-B). It was concluded that there are differ-
ences in the dustiness and hygienic quality of peatbedding.
Another study evaluated shredded cardboard asan appropriate minimum dust bedding. Pulmo-nary function tests (ventilatory mechanics, arterialblood gases, airway inflammation scoring, and bron-choalveolar cytology) were significantly differentfrom those recorded in poor hygienic conditions.3
On basis of the in vitro and in vivo results, it wasconcluded that cardboard bedding, used in conjunc-tion with low dust forage, might be appropriate inthe provision of minimum dust management ofheaves affected horses (Table 1).
Food allergens are another route by which clini-cians can help minimize/eliminate allergen load byavoidance alone. In a study of 22 cases of recurrentor chronic urticaria in Thoroughbred racehorsesduring training season, food allergy seemed to exac-erbate the clinical symptoms.5 Intradermal skintests with fresh allergenic food potentiated syn-dromic reactions in some horses, and elimination ofthe suspect allergen brought about resolution ofclinical signs such as urticaria and enteritis. Ingeneral, an elimination trial of high protein fooditems, supplements, flavored medications, and anymolasses-containing products for a minimum of 4–6wk is worthwhile when attempting to minimize thepatient’s allergen load.
3. Topical Control
When treating horses with allergies, patient fly con-trol is a mandatory part of any therapeutic regimen.A spray containing permethrin and an insect growthregulator (pyriproxyfen; Knockout L.A.,a) was effec-tive in treating horses with Culicoides spp. hyper-sensitivity.6 Other recommended repellantsinclude Avon Skin-So-Soft Bath Oil diluted 50:50with water and Skin-So-Soft Bug Guard PlusIR3535 lotion with sunscreen or an aqueous DEET(N,N-diethyl-m-toluamide) solution at a concentra-
Table 1. Respirable Dust and Mold Spores in a Variety of Feed and Bedding
Feed/beddingRespirable Dust
(particles � 103/l)A. fumigatus
(CFU/l)F. rectivirgula
(CFU/l)T. vulgaris
(CFU/l)
Good hay 63.0 (30.0) 20.1 (5.6) 3.1 (1.2) 3.3 (1.2)Silage 78% D.M. 8.8 (2.5) 11.5 (6.5) 1.7 (1.2) 2.2 (0.7)Silage � 50% D.M. 4.5 (1.9) 4.5 (4.2) 0.4 (0.2) 1.2 (0.8)Alfalfa pellets 9.5 (4.4) 2.6 (2.5) 0.1 (0.0) 0.4 (0.2)Wood shavings 31.5 (12.9) 16.7 (2.9) 1.2 (0.7) 1.9 (1.4)Cleanbox wood shavings 6.2 (0.1) 0.04 (0.05) 0.02 (0.04) 0.15 (0.09)Good straw 11.6 (4.9) 9.5 (5.0) 0.4 (0.4) 0.8 (0.4)Flax straw 9.3 (1.8) 2.4 (0.5) 0.2 (0.2) 1.4 (0.3)Ecobed cardboard 5.7 (1.6) 0.03 (0.05) 0 (0) 0 (0.01)Rolled grains 120.3 (30.6) 10.2 (0.6) 1.8 (1.6) 1.1 (1.1)Whole grains 4.1 (0.9) 4.5 (1.5) 0.1 (0.0) 1.0 (0.1)Mollassed concentrates 2.1 (0.6) 0.8 (0.3) 0.3 (0.2) 3.0 (1.8)
Material was agitated in an air stream and particulates expressed per liter of air.Adapted from Robinson NE. Recurrent airway obstruction (heaves). In Lekeux P (ed.) Equine Respiratory Diseases. Ithaca:
International Veterinary Information Service; 2001.
470 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
tion of 16.6% (a previously approved but recentlydiscontinued equine product is Ceratexb).6–10 Ap-plication frequency will depend on the product se-lection, geographic insect distribution, season of theyear, and severity of the patient’s condition.
Shampoo therapy should not be overlooked in thetreatment of equine allergies. The simple act ofbathing with cool water rehydrates the skin, im-proves the integrity of the epidermal barrier, resultsin the vasoconstriction that decreases delivery ofinflammatory mediators to the skin, helps to mini-mize percutaneous absorption of allergens, and fi-nally, with appropriate ingredient selection,addresses secondary superficial infections. The se-lection of shampoos should be based on the patient’sskin condition and may include colloidal oatmealproducts (shampoos, conditioners, and bath treat-ments) with or without a local anesthetic (pramox-ine HCl) or corticosteroids for pruritic dermatoses,sulfur/salicylic acid shampoos for horses with excessscale, antimicrobial shampoos (benzoyl peroxide,chlorhexidine or imidazoles) if secondary infectionshave been identified, or a combination of one or moreof the above.
Lime sulfur (LymDypc) is a very effective multi-modal topical therapeutic, because it provides notonly ectoparasitic activity but also antipruritic, an-tiseborrheic, and antimicrobial effects in all ani-mals. Although off label, it is a safe and proventreatment option that can be applied as a dip orspray on horses.
Topical steroids have also shown good efficacywhen treating small animal patients. Unfortu-nately, most of these products are not labeled for usein equine medicine. I have used several topicalsteroid products for treatment of localized lesions.
Resicortd is a mild 1% hydrocortisone, leave-onconditioner in a non-irritating base.
Steroid ointments or creams (Aclovatee [alclo-metasone 0.05%] or Eloconf [mometasone 0.1%])have different potencies (mild-moderate andhigh, respectively).
Genesis Topical Sprayg is a 0.015% triamcinolonespray.
When choosing a topical steroid, one must strive forproducts with minimal side effects (i.e., minimal tono hematological and biochemical changes, suppres-sion of the adrenal axis, and local cutaneous alter-ations [atrophy, alopecia, comedone formation, andsecondary infections]).
4. Systemic Therapy
Along with the traditional immunoglobulin E (IgE)-mediated allergic reactions, it seems that theT-helper-1/T-helper-2 paradigm, along with all itscytokine alterations, exists in some form in the lungof horses with RAO.10–12 Similar to other domesticspecies, our focus on treatment of allergies should bedirected at reestablishing the balance of T-cell inter-
actions, thus minimizing the production of interleu-kin (IL)-4, IL-5, and other inflammatory mediators,such as chemokines, and of course, the traditionalproducts of IgE mediated mast-cell degranulation.
5. Allergen Specific Immunotherapy
Allergen specific immunotherapy (ASIT) is a usefulnon-steroidal long-term treatment alternative inequine veterinary dermatology. It has been used tocontrol insect hypersensitivities, urticaria second-ary to atopy, and allergen induced RAO in horseswith anticipated improvement in some cases asearly as 2 mo.13 However, a minimum of 12 mo isnecessary to determine ASIT’s efficacy in an allergicpatient. ASIT may also be a consideration whentreating allergy induced head shaking andlaminitis.14
Although the mechanism of action of immunother-apy is not clearly defined, there are several theoriesthat have been proposed.
1. Induces immunoglobulin G (IgG) blockingantibody production in secretions, serum,and tissue.15,16
2. Decreases circulating IgE by stimulating Tregulatory cells.16
3. Decreases the number of mast cells and/ormast cell response to antigen.17
When selecting allergens for inclusion into ASIT,historical correlation with the allergy test findingsalong with likelihood of allergen exposure is key.ASIT has shown mixed results for treatment of in-sect hypersensitivity, urticaria secondary to atopy,and RAO ranging from 16% to 90% effica-cy.10,11,13,18–23 A recent report reflected the cur-rent concensus that �60–70% of atopic horsesimprove with ASIT.11 Although the exact reasonsfor inconsistencies in response to ASIT may becaused by individual response, a number of factorsmay contribute to the variable responses.
● Lack of allergen standardization.● Selection of antigen (was it based on intradermal,
serologic, or both) for allergen concentrations.● Incorporation of non-specific immunostimu-
lants (e.g., mycobacterial cell wall).● Induction of immunotherapy and maintenance
protocols.● Administration of allergen (dose and route;
i.e., SC or intradermal).● Use of post-induction aftercare.● Lack of objective data in a controlled environ-
ment.
Further studies with the standards set forth by theCanine Atopic Task Force24 need to be performed toreliably assess the efficacy of this treatment modal-ity in horses.
However, based on the positive responses, mini-mal side effects (local injection reaction), decreased
AAEP PROCEEDINGS � Vol. 52 � 2006 471
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
dosing frequency/workload for the owner, and costefficacy (weight independent dosing), ASIT in horsesis a viable therapeutic modality for long-term con-trol of insect hypersensitivity, recurrent urticaria/pruritus, and RAO. Even in competitive trial andshow horses where concerns about the use of medi-cation and drug testing arise, hyposensitization pro-vides an alternative treatment modality that mayallow the horse to return to performance standardsand not compromise the rider’s ethics.
5. Polyunsaturated N-3 and N-6 Fatty Acids
Most mammalian cell membranes incorporate poly-unsaturated N-3 and N-6 fatty acids (PUFAs), andthey are thought to create a shift in the production ofpro-inflammatory mediators to non- or anti-inflam-matory mediators in the arachidonic acid cascade.Other possible mechanisms by which PUFAs exerttheir positive clinical benefit in atopic dermatitis arestill under investigation. Fatty acid supplementshave shown variable reported responses in hors-es.25–28 The difference in results is most likely at-tributable to the variability of the researchparameters.
1. Source and dose of fatty acid being given andin food (linseed oil and flaxseed meal versusoil and marine fish oils).
2. Type of allergic reaction being evaluated (in-sect allergy versus atopy versus other).
3. Parameters being evaluated (intradermal testreaction versus circulating plasma fatty acid orinflammatory mediator concentrations).
4. Length of the study.5. Number of horses in the study.6. Study design (randomized double-blind pla-
cebo controlled � crossover and 6-wkwashout).
7. Geographic location of the studies (Florida,Oregon, United Kingdom, and Canada).
Currently, it is difficult to make any conclusions onthe efficacy of the essential fatty acids based oncurrent equine studies. Our knowledge of clinicalbenefits of PUFAs in recent canine atopic dermatitisstudies along with the lack of significant adversereactions (mainly diarrhea) would prescribe its usein equine dermatology as adjunct to any long-termanti-inflammatory protocol. Typically, improve-ment in pruritus and/or skin condition should benoted within 2–8 wk after initiating therapy.10
A variety of PUFAs exist on the veterinary marketand are typically administered at their labeled dose(Derm Caps 100s;h 1 capsule per 100 lbs dividedtwice daily).
7. Antihistamines and Tricyclic Antidepressants
Antihistamines and tricyclic antidepressants (TCA)provide a non-steroidal alternative for long-termcontrol of allergic reactions in horses. The H1-re-ceptor antagonist activity of these drugs is some-
times complemented by other mechanisms of actionincluding anti-serotonin/serotonin re-uptake inhibi-tion. Exact dosing and recent pharmacokineticstudies are lacking in the horse.29–32 The followingare the antihistamines and TCAs that are beingprescribed to horses (in my personal order of prefer-ence).33
1. Hydroxyzine hydrochloride or pamoate (0.5–1.0 mg/kg, q 8 h).
2. Doxepin hydrochloride (0.5–0.75 mg/kg, q12 h).
3. Amitriptyline (1–2 mg/kg, q 12 h).4. Chlorpheniramine (0.25 mg/kg, q 12 h).5. Diphenhydramine (0.75–1 mg/kg, q 12 h).6. Pyrilamine maleate (1 mg/kg, q 12 h).
Similar to humans and other domestic species, thereis tremendous variation in response to antihista-mines/TCAs. It is sometimes necessary to try sev-eral different classes of antihistamines at 2-wkintervals before finding the most effective option.Despite the paucity of synergism between antihista-mines/TCAs and other anti-inflammatory therapiesin the horse, it is worthwhile to combine therapiesbased on the numerous positive studies in dogs andcats. Although antihistamines and TCAs havefewer reported side effects (light sedation and occa-sional personality changes) than corticosteroids, onemust always keep in mind the anticholinergic prop-erties of these medications, particularly in patientswith glaucoma, gastrointestinal atony, cardiac ar-rhythmias, or urinary retention problems. Lastly,advise owners to contact show authorities regardingdrug restrictions/withdrawals at least 14 days be-fore the event.
8. Phosphodiesterase Inhibitors
Pentoxifylline (PTX) is a synthetic xanthine deriva-tive related to caffeine and theophylline. Its phos-phodiesterase inhibition imparts three majortherapeutic benefits.34–42
1. It improves wound healing and connective-tissue disorders by increasing fibroblast col-lagenases, decreasing fibroblast collagen,fibroblast fibronectin, and fibroblast glycos-aminoglycans, and decreasing response totumour necrosis factor (TNF)-alpha.
2. Rheologic agents decrease platelet aggrega-tion and adhesion, increase red cell deform-ability, decrease vasoconstriction, increaseplasminogen activator, plasmin, and anti-thrombin III, and decrease fibrinogen, alpha2antiplasmin, alpha1 antitrypsin, and alpha2macroglobulin modulating effects.
3. Immunomodulators inhibit T- and B-cell ac-tivation and proliferation, increase leukocytedeformability and chemotaxis, decrease leu-kocyte adhesion and aggregation, decreaseneutrophil superoxide release and neutrophil
472 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

degranulation, decrease monocyte TNF-al-pha production, leukocyte response to TNF-alpha, lymphotoxin, and interferon-gamma,decrease production and leukocyte responseto IL-1 and IL-12, increased production ofIL-10 and PGE2, and decrease natural killercell activity.
By one or many of the mechanisms above, PTX po-tentiates the effectiveness of many medications in-cluding steroids (steroid sparing effect).43–48 Forthis reason as well as the fact that PTX’s rheologicactivity potentially minimizes the risk of laminitis,49
I tend to use pentoxifylline (8–10 mg/kg, q 12–24h)10,50 in conjunction with steroids. This provides anon-steroidal alternative with minimal side effects(hyperexcitability and sweats) for the purpose oftapering or eliminating the need for glucocorticoidsin immune-mediated and allergic dermatoses.This medication should not be used in conjunctionwith anticoagulants or in patients with hemorrhagicdisorders.
9. Corticosteroids
Corticosteroids have long been a standard therapyfor allergies in the horse. Corticosteroids work pri-marily by gene repression and inhibition of nuclearfactor kappa B, which directly or indirectly preventsthe production of cytokines, chemokines, cell adhe-sion molecules, complement factors, and prostaglan-din and leukotriene synthesis involved in theallergic response. Unfortunately, aggressive use ofcorticosteroids in horses may cause various adverseeffects, including steroid hepatopathy, laminitis,and iatrogenic hyperadrenocorticism.51–53 Individ-ual sensitivity to glucocorticoids may be directly re-lated to Type 1:Type 2 11-�-hydroxysteroiddehydrogenase ratio. Judicious use, appropriateamounts, and intervals are key to minimizing ad-verse reactions. The following are the two mostcommonly used glucocorticoids used for the short-term treatment of equine allergies.
1. Prednisolone: syrup compounded or tabletsat 0.5–1.5 mg/kg/day for 7–14 days and thentapering to 0.2–0.5 mg/kg, q 48 h over 2–5 wkfor maintenance. If cost is an issue, pred-nisone may be substituted for prednisolone;the latter has been shown to have greaterbioavailability in horses.54
2. Dexamethasone: powder or tablets. In-jectable dexamethasone solution given orallyis 60–70% bioavailable compared with the IVroute.11 The initial loading oral or IV pulsedose is 0.05–0.1 mg/kg daily for 3–7 days andthen tapering to 0.01–0.02 mg/kg every48–72 h for maintenance. This regime isparticularly helpful in more refractory cases.
Lastly, when addressing allergy induced RAO, theuse of locally dispersed steroids through metered-
dose inhalers (MDI) may help minimize concernsregarding glucocorticoid side effects while dispers-ing maximal concentration of drug at the effectorsites.55,56 Masks have been designed for use withMDIsi to improve drug delivery. Beclomethasonediproprionate and fluticasone propionate are bothefficacious and well tolerated by horses, but some-times these MDI steroids have a delayed response of�4 days; this necessitates combining them withfaster acting drugs such as bronchodilators and sys-temic corticosteroids. As well, MDI steroids havefew residual effects after treatment isdiscontinued.56
10. Cyclosporine
Cyclosporine has been used in the management ofhuman, feline, and canine atopic dermatitis. How-ever, the lack of pharmacokinetic data in horses andmoreover, the cost of the medication limits its use inequine medicine at this time.
11. Other Treatment Options
Methylsulfonylmethane (MSMj) can be used in con-junction with other anti-inflammatory therapies forits antioxidant properties. Controlled studies arelacking regarding its efficacy in equine allergies;however, because of the absence of significant sideeffects, I continue to use the product initially at10–12 gm/500 kg q 12 h and then taper to a oncedaily dose.
Some of the earlier and more recent research ofanti-inflammatory modalities is focused on receptorantagonists (platelet-activating factor receptor an-tagonist57 and eotaxin receptor [CCR3] antago-nists58), protein kinase-C inhibitors and itssubsequent effects on eosinophils,59 and monoclonalantibodies directed against cytokines (anti-IL-4monoclonal antibody [pascolizumab]60). With eachstudy, we hope to learn more about the pathogenesisof allergies and ultimately, find the key to turn offthe allergic response with minimal side effects andcost.
References and Footnotes1. Jackson CA, Berney C, Jefcoat AM, et al. Environment and
prednisone interactions in the treatment of recurrent airwayobstruction (heaves). Equine Vet J 2000;32:432–43 8.
2. Airaksinen S, Heiskanen ML, Heinonen-Tanski H, et al.Variety in dustiness and hygiene quality of peat bedding. AnnAgric Environ Med 2005;12:53–59.
3. Kirschvink N, Di Silvestro F, Sbai I, et al. The use of card-board bedding material as part of an environmental controlregime for heaves-affected horses: in vitro assessment ofairborne dust and aeroallergen concentration and in vivoeffects on lung function. Vet J 2002;163:319–325.
4. Leguillette R. Recurrent airway obstruction�heaves.Vet Clin North Am [Equine Pract] 2003;19:63–86.
5. Volland-Francqueville M, Sabbah A. Recurrent or chronicurticaria in Thoroughbred racehorses: clinical observations.Allerg Immunol (Paris) 2004;36:9–12.
6. Bourdeau PJ, Beis C, Chouilly C, et al. Evaluation of per-methrin and pyriproxyfen containing spray in the treatmentof sweet itch in 25 horses, in Proceedings. 15th AnnualMember’s Meeting of the American Academy of Veterinary
AAEP PROCEEDINGS � Vol. 52 � 2006 473
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
Dermatology/American College of Veterinary Dermatology1999;13–14.
7. Fadok VA. Update on equine allergies. J Vet Allergy ClinImmunol 1997;85:68–76.
8. Gortel K. Equine parasitic hypersensitivity: a review.Equine Pract 1998;20:14–16.
9. Rees C. Diagnosing and managing equine pruritus: insecthypersensitivity. Compend Cont Educ Pract Vet 2005;27:629–636.
10. Scott DW, Miller WM. Skin immune system and allergicskin diseases. In: Scott DW, Miller WM, eds. Equine der-matology. Philadelphia: W.B. Saunders, 2003;436–448.
11. White SD. Advances in equine atopic dermatitis, serologicand intradermal allergy testing. Clin Tech Equine Pract2005;4:311–313.
12. Cordeau ME, Joubert P, Dewachi O, et al. IL-4, IL-5 andIFN-gamma mRNA expression in pulmonary lymphocytes inequine heaves. Vet Immunol Immunopathol 2004;97:87–96.
13. Rees CA. Response to immunotherapy in six related horseswith urticaria secondary to atopy. J Am Vet Med Assoc2001;218:753–755.
14. Wagner IP, Rees CA, Dunstan RW, et al. Evaluation ofsystemic immunologic hyperreactivity after intradermal test-ing in horses with chronic laminitis. Am J Vet Res 2003;64:279–283.
15. Greenberger PA. Immunotherapy of IgE-mediated disor-ders. Immunol Allergy Clin North Am 1992;12:125–144.
16. Akdis M, Blaser K, Akdis CA. T regulatory cells in allergy:novel concepts in the pathogenesis, prevention, and treat-ment of allergic diseases. J Allergy Clin Immunol 2005:961–968.
17. Durham SR, Varney VA, Gaga M, et al. Grass pollen im-munotherapy decreases the number of mast cells in the skin.Clin Exp Allergy 1999;29:1490–1496.
18. Delger JM. Intradermal testing and immunotherapy inhorses. Vet Med 1997;92:635–639.
19. Anderson GS, Belton P, Jahren E, et al. Immunotherapytrial for horses in British Columbia with Culicoides (Diptera:Ceratopogonidae) hypersensitivity. J Med Entomol 1996;33:458–466.
20. Barbet J, Bevier D, Greiner EC. Specific immunotherapy inthe treatment of Culicoides hypersensitive horses: a double-blind study. Equine Vet J 1990;22:232–235.
21. Rosenkrantz WS, Griffin CE, Esch RE, et al. Response inhorses to intradermal challenge of insects and environmentalallergens with specific immunotherapy, in Proceedings. 3rdWorld Congress of Veterinary Dermatology 1996;191–200.
22. Tallarico NJ, Tallarico CM. Results of intradermal allergytesting and treatment by hyposensitization of 64 horses withchronic obstructive pulmonary disease, urticaria, headshak-ing, and/or reactive airway disease. Vet Allergy Clin Immu-nol 1998;6:25–35.
23. Wong D, Manning T. Equine skin: structure, immunologicfunction, and methods of diagnosing disease. Compend ContEduc Pract Vet 2005;27:463–473.
24. Griffin CE, Hillier A. The ACVD task force on canine atopicdermatitis (XXIV): allergen-specific immunotherapy. VetImmunol Immunopathol 2001;81:363–383.
25. O’Neill W, McKee S, Clarke AF. Flaxseed (Linum usitatis-simum) supplementation associated with reduced skin testlesional area in horses with Culicoides hypersensitivity.Can J Vet Res 2002;66:272–277.
26. Friberg CA, Logas D. Treatment of Culicoides hypersensi-tive horses with high-dose n-3 fatty acids: a double-blindedcross over study. Vet Dermatol 1999;10:117–122.
27. Craig JM, Lloyd DH, Jones RD. A double-blind placebo-controlled trial of an evening primrose and fish oil combina-tion vs. hydrogenated coconut oil in the management ofrecurrent seasonal pruritus in horses. Vet Dermatol 1997;8:177–182.
28. Hall JA, Van Saun RJ, Tornquist SJ, et al. Effect of type ofdietary polyunsaturated fatty acid supplement (corn oil orfish oil) on immune responses in healthy horses. J Vet IntMed 2004;18:880–886.
29. Foster AP, McKelvie J, Cunningham FM. Inhibition of an-tigen-induced cutaneous responses of ponies with insect hy-persensitivity by the histamine-1 receptor antagonistchlorpheniramine. Vet Rec 1998;143:189–193.
30. Wasfi IA, Abdel Hadi AA, Elghazali M, et al. Comparativepharmacokinetics of diphenhydramine in camels and horsesafter intravenous administration. Vet Res Commun 2003;27:463–473.
31. Torneke K, Ingvast-Larsson C, Pettersson K, et al. Pharma-cokinetics and pharmacodynamics of clemastine in healthyhorses. J Vet Pharmacol Ther 2003;26:151–157.
32. Manohar M, Goetz TE, Humphrey S, et al. H1-receptorantagonist, tripelennamine, does not affect arterial hypox-emia in exercising Thoroughbreds. J Appl Physiol 2002;92:1515–1523.
33. Yu AA. Equine urticaria: a diagnostic dilemma. Com-pend Cont Educ Pract Vet 2000;22:277–280.
34. Schmidt-Choudhury A, Furuta GT, Lavigne JA, et al. Theregulation of tumor necrosis factor-alpha production in mu-rine mast cells: pentoxifylline or dexamethasone inhibitsIgE-dependent production of TNF-alpha by distinct mecha-nisms. Cell Immunol 1996;171:140–146.
35. Rickards KJ, Page CP, Lees P, et al. In vitro and ex vivoeffects of the phosphodiesterase 4 inhibitor, rolipram, onthromboxane production in equine blood. J Vet PharmacolTher 2003;26:123–130.
36. Sykes BW, Furr MO. Equine endotoxaemia�a state-of-the-art review of therapy. Aust Vet J 2005;83:45–50.
37. Barton MH, Ferguson D, Davis PJ, et al. The effects ofpentoxifylline infusion on plasma 6-keto-prostaglandin F1alpha and ex vivo endotoxin-induced tumour necrosis factoractivity in horses. J Vet Pharmacol Ther 1997;20:487–492.
38. Barton MH, Moore JN, Norton N. Effects of pentoxifyllineinfusion on response of horses to in vivo challenge exposurewith endotoxin. Am J Vet Res 1997;58:1300–1307.
39. Weiss DJ, Richwagen K, Evanson OA. Effects of hematocritand erythrocyte deformability on pulmonary vascular pres-sures in perfused pony lungs. Am J Vet Res 1996;57:346–350.
40. Chilcoat CD, Rowlingson KA, Jones SL. The effects of cAMPmodulation upon the adhesion and respiratory burst activityof immune complex-stimulated equine neutrophils. Vet Im-munol Immunopathol 2002;88:65–77.
41. Zabel P, Entzian P, Dalhoff K, et al. Pentoxifylline in treat-ment of sarcoidosis. Am J Respir Crit Care Med 1997;155:1665–1669.
42. Leguillette R, Desevaux C, Lavoie JP. Effects of pentoxifyl-line on pulmonary function and results of cytologic examina-tion of bronchoalveolar lavage fluid in horses with recurrentairway obstruction. Am J Vet Res 2002;63:459–463.
43. Briggs WA, Eustace J, Mathew S, et al. Pentoxifylline po-tentiates in vitro lymphocyte suppression by glucocorticoidsand immunosuppressive drugs. J Clin Pharmacol 1998;38:561–566.
44. Entzian P, Zahringer U, Schlaak M, et al. Comparativestudy on effects of pentoxifylline, prednisolone and colchicinein experimental alveolitis. Int J Immunopathol Pharmacol1998;20:723–735.
45. Funk JO, Ernst M, Schonharting MM, et al. Pentoxifyllineexerts synergistic immunomodulatory effects in combinationwith dexamethasone or cyclosporin A. Int J ImmunopatholPharmacol 1995;17:1007–1016.
46. Baskett A, Barton MH, Norton N, et al. Effect of pentoxi-fylline, flunixin meglumine, and their combination on amodel of endotoxemia in horses. Am J Vet Res 1997;58:1291–1299.
47. Kasahara E, Yamagishi N, Tanaka M, et al. A child withsimple ulcer of the colon effectively treated with the combi-nation of prednisolone, azathioprine, and pentoxifylline. JGastroenterol 2002;37:745–749.
48. Kiku Y, Matsuzawa H, Ohtsuka H, et al. Effects of chlor-promazine, pentoxifylline and dexamethasone on mRNAexpression of lipopolysaccharide-induced inflammatory cyto-
474 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
kines in bovine peripheral blood mononuclear cells. J VetMed Sci 2002;64:723–726.
49. Ingle-Fehr JE, Baxter GM. The effect of oral isoxsuprineand pentoxifylline on digital and laminar blood flow inhealthy horses. Vet Surg 1999;28:154–160.
50. Crisman MV, Wilcke JR, Correll LS, et al. Pharmacokineticdisposition of intravenous and oral pentoxifylline in horses.J Vet Pharmacol Ther 1993;16:23–31.
51. Cohen ND, Carter GK. Steroid hepatopathy in a horse withglucocorticoid-induced hyperadrenocorticism. J Am VetMed Assoc 1992;200:1682–1684.
52. Vandenabeele SIJ, White SD, Affolter VK, et al. Pemphigusfoliaceus in the horse: a retrospective study of 20 cases.Vet Dermatol 2004;15:381–388.
53. Johnson PJ, Slight SH, Ganjam VK, et al. Glucocorticoidsand laminitis in the horse. Vet Clin North Am [EquinePract] 2002;18:219–236.
54. Peroni DL, Stanley S, Kollias-Baker C, et al. Prednisone peros is likely to have limited efficacy in horses. Equine Vet J2002;34:283–287.
55. Leguillette R. Recurrent airway obstruction—heaves.Vet Clin North Am [Equine Pract] 2003;19:63–86.
56. Lavoie JP. Heaves. In: Bertone J, Brown CM, eds. The 5minute veterinary consult—equine. Baltimore: Lippincott,Williams & Wilkins, 2002;478–479.
57. Foster AP, Lees P, Cunningham FM. Actions of PAF recep-tor antagonists in horses with the allergic skin disease sweetitch. Inflamm Res 1995;44:412–417.
58. Benarafa C, Collins ME, Hamblin AS, et al. Role of thechemokine eotaxin in the pathogenesis of equine sweet itch.Vet Rec 2002;151:691–693.
59. Greenaway EC, Sepulveda MF, Cunningham FM, et al.Protein kinase C (PKC) isotype profile in eosinophils fromponies with sweet itch and role in histamine-induced eosin-ophil activation. Vet Immunol Immunopathol 2003;96:53–63.
60. Hart TK, Blackburn MN, Brigham-Burke M, et al. Preclini-cal efficacy and safety of pascolizumab (SB 240683): a hu-manized anti-interleukin-4 antibody with therapeuticpotential in asthma. Clin Exp Immunol 2002;130:93–100.
aKnockout L.A., Virbac, Peakhurst, NSW 2210, Australia.bCeratex, Vet Genix, Coral Gables, FL 33134.cLymDyp, DVM Pharmaceuticals, Miami, FL 33137.dResicort, Virbac, Peakhurst, NSW 2210, Australia.eAclovate, GlaxoSmithKline Consumer Healthcare LP, Pitts-
burgh, PA 15230.fElocon, Schering Corporation, Kenilworth, NJ 07033.gGenesis Topical Spray, Virbac AH, Inc., Fort Worth, TX 76137.hDerm Caps 100s, DVM Pharmaceuticals, Miami, FL 33137.iEquine Aeromask, Trudell Medical International, London, ON,
Canada N5V 5G4.jMSM, Vita-Flex Nutrition Co, Council Bluffs, IA 51501.
II. Nodules, Lumps, and Bumps
Nodules—Infectious
Stephen D. White, DVM, Diplomate ACVD
1. Infectious
A serious yeast-caused disease is sporotrichosis(Sporothrix schenkii), which presents as a nodular toulcerative lymphatic cording disease (Fig. 1). Diag-nosis is made when the organism is detected onhistopathology, immunofluorescent antibody testingon affected tissues, impression smears, and/or cul-ture.1 This is a zoonosis, and therefore, care shouldbe taken in handling suspected samples. Success-ful therapy with a number of different systemic io-dine preparations (NaI or KI) has been reported.The organic iodides have proven to be superior inefficacy to the inorganic iodides in the treatment ofequine sporotrichosis, and ethylene diamine dihy-droiodide (organic iodide powdera or EDDI 20 Gr.Dextrose baseb) is the drug of choice. This productis in the form of a feed additive. It can be mixedwith a small amount of grain and administered at adosage of 1–2 mg/kg of the active ingredient once ortwice daily for the first week. The dosage is thenreduced to 0.5–1.0 mg/kg once daily for the remain-der of the treatment. In general, lesions will begin
to regress during the first month of treatment, andtreatment should be continued for at least 1 mobeyond the complete resolution of all cutaneous nod-ules and healing of any ulcerated lesions. Discon-tinuing therapy prematurely will invariably resultin an unnecessary relapse of the disease. Duringtreatment, the horse should be closely observed forany evidence of iodide toxicity (iodism), which in-cludes excess scaling and alopecia, a serous ocular ornasal discharge, excess salivation, anorexia, depres-sion, coughing, nervousness, or cardiovascular ab-normalities. Should any of these signs develop, thetreatment should be discontinued for 1 wk and re-sumed at three-quarters of the dosage at which theiodism was noted. In most instances, the treat-ment is subsequently well tolerated.2 Althoughboth itraconazole and terbinafine have been shownto be effective in vitro against the organism isolatedfrom a horse, the author is unaware of any clinicalreports in this species.3
Habronemiasis (summer sore) is a granulomatousdisease caused by the deposition of Habronema ma-jus, Habronema muscae, or Draschia megastomalarvae by flies at the site of wounds or natural bodymoisture (sheath or eyes).4,5 Diagnosis is based on
AAEP PROCEEDINGS � Vol. 52 � 2006 475
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
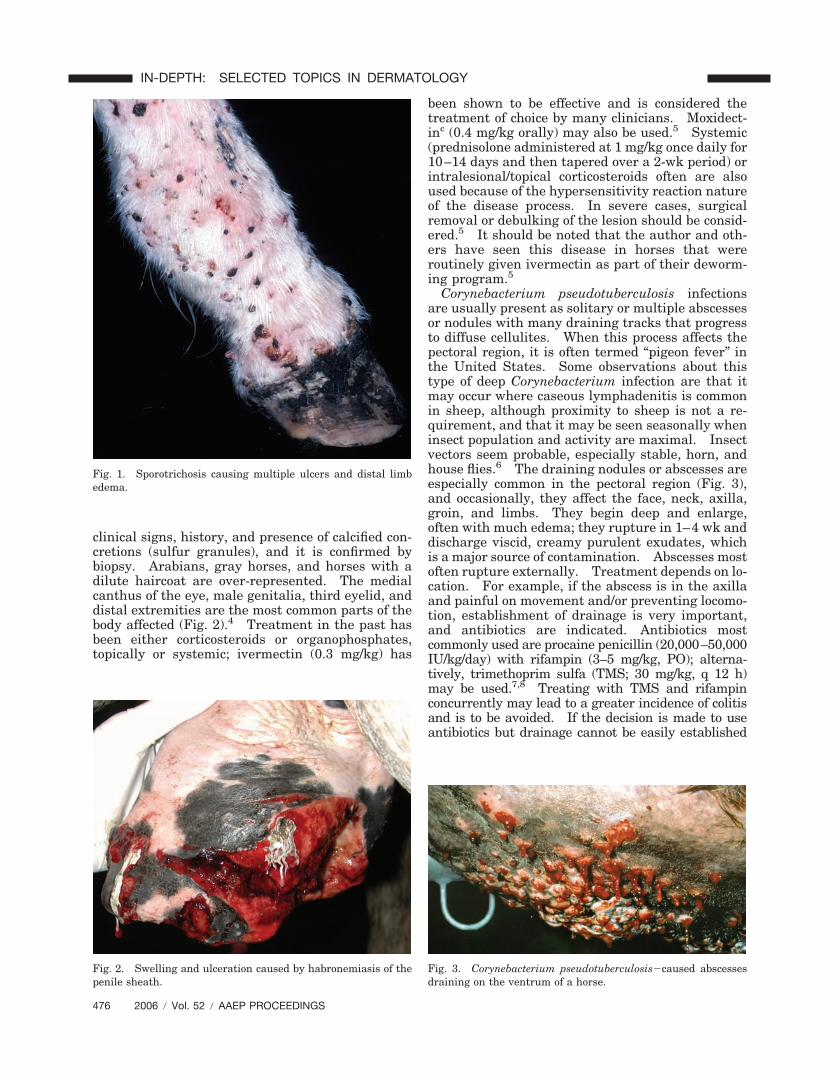
clinical signs, history, and presence of calcified con-cretions (sulfur granules), and it is confirmed bybiopsy. Arabians, gray horses, and horses with adilute haircoat are over-represented. The medialcanthus of the eye, male genitalia, third eyelid, anddistal extremities are the most common parts of thebody affected (Fig. 2).4 Treatment in the past hasbeen either corticosteroids or organophosphates,topically or systemic; ivermectin (0.3 mg/kg) has
been shown to be effective and is considered thetreatment of choice by many clinicians. Moxidect-inc (0.4 mg/kg orally) may also be used.5 Systemic(prednisolone administered at 1 mg/kg once daily for10–14 days and then tapered over a 2-wk period) orintralesional/topical corticosteroids often are alsoused because of the hypersensitivity reaction natureof the disease process. In severe cases, surgicalremoval or debulking of the lesion should be consid-ered.5 It should be noted that the author and oth-ers have seen this disease in horses that wereroutinely given ivermectin as part of their deworm-ing program.5
Corynebacterium pseudotuberculosis infectionsare usually present as solitary or multiple abscessesor nodules with many draining tracks that progressto diffuse cellulites. When this process affects thepectoral region, it is often termed “pigeon fever” inthe United States. Some observations about thistype of deep Corynebacterium infection are that itmay occur where caseous lymphadenitis is commonin sheep, although proximity to sheep is not a re-quirement, and that it may be seen seasonally wheninsect population and activity are maximal. Insectvectors seem probable, especially stable, horn, andhouse flies.6 The draining nodules or abscesses areespecially common in the pectoral region (Fig. 3),and occasionally, they affect the face, neck, axilla,groin, and limbs. They begin deep and enlarge,often with much edema; they rupture in 1–4 wk anddischarge viscid, creamy purulent exudates, whichis a major source of contamination. Abscesses mostoften rupture externally. Treatment depends on lo-cation. For example, if the abscess is in the axillaand painful on movement and/or preventing locomo-tion, establishment of drainage is very important,and antibiotics are indicated. Antibiotics mostcommonly used are procaine penicillin (20,000–50,000IU/kg/day) with rifampin (3–5 mg/kg, PO); alterna-tively, trimethoprim sulfa (TMS; 30 mg/kg, q 12 h)may be used.7,8 Treating with TMS and rifampinconcurrently may lead to a greater incidence of colitisand is to be avoided. If the decision is made to useantibiotics but drainage cannot be easily established
Fig. 3. Corynebacterium pseudotuberculosis�caused abscessesdraining on the ventrum of a horse.
Fig. 1. Sporotrichosis causing multiple ulcers and distal limbedema.
Fig. 2. Swelling and ulceration caused by habronemiasis of thepenile sheath.
476 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

(for example, an axillary abscess where the owner isunwilling to allow the veterinarian to use a trocar anddrain), the antibiotics must be used for a minimum of1 mo. If the abscess is solitary and not causing painor fever, antibiotics are usually not necessary, butbringing the abscess to a head with hot packs or heat-inducing agents (ichthammol) is important. Afterany abscess has drained, gentle cleaning with tamediodines or chlorhexidine is indicated.
2. Neoplasms
Mastocytosis (mast cell tumors) occurs in horses1–18 yr of age (mean � 9 yr), and there is no breedpredilection.9,10 A predilection for males has beenproposed but is not always substantiated. There isone report in a donkey.11 In addition, multiplemast cell tumors resembling urticaria pigmentosa ofhumans may occur in newborn foals; these sponta-neously appear and regress. Equine mastocytosisis usually solitary and occurs most commonly on thehead and trunk. Lesions are 0.5–20.0 cm in diam-eter, well to poorly circumscribed, firm to fluctuant,dermal or SC, and may or may not be alopecic,ulcerated, and hyperpigmented. Lesions on thelegs tend to be very firm and immovable.
Histology may vary from sheets of mast cells withfew eosinophils (presumably early lesions) to thoseshowing both the sheets of mast cells with numerouseosinophils and collagen degranulation. Ultra-structural features are similar to those noted inmast cell tumors of other species. Clinically, mostmast cell tumors in horses do not recur after beingexcised (22 of 25 in one study). The author knowsof one anecdotal case of metastasis from a tumor onthe muzzle to regional lymph nodes; the tumor andthe nodes were removed, and the horse was clini-cally sound 3 yr later. There is some debate as towhether equine mast cell tumors are benign neopla-sias or focal dysplasias of mast cells.
Melanocytic skin tumors of horses traditionallyhave been described in aging grey horses and on theventral tail, perineum, external genitalia, lip, udder,periocular, and parotid gland regions. They havebeen the subject of several classification schemes inattempt to correlate histopathologic appearancewith clinical behavior (i.e., is it benign or malig-nant?). One study distinguished three basic typesof melanocytic skin tumors.12
Melanocytic nevi (melanocytoma) occurs in thesuperficial dermis or at the epidermal-dermal junc-tion, and it frequently has epithelial involvementwith nests of relatively large, mildly to moderatelypleomorphic cells showing variable cytoplasmic pig-mentation and occasional mitoses (Fig. 4). Morethan 70% of these occur in horses �6 yr of age andmay occur in horses of any color (not just grey).Most of these tumors occurred in atypical locations.Of 28 melanocytic nevi, only one became invasive,and the rest exhibited benign behavior.
Dermal melanomas are found in the deep dermisand are composed of small homogeneous, indistinct
tumor cells, either round or dendritic, with no mito-ses. (If there are multiple, confluent dermal mela-nomas, this is referred to as dermal melanomatosis).Eighty percent of these tumors are in horses �6 yr ofage12 or between 5 and 15 yr,13 and it is much morecommon in grey horses. Most of these tumors oc-curred in typical locations. Of 14 cases availablefor follow-up in one study,12 8 had malignant behav-ior as shown by metastases.
In another study,14 the clinical and pathologicalcharacteristics of cutaneous melanomas occurring in83 Camargue-type gray-skinned horses showed thatthe tumors occurred most frequently underneath thetail (93.9%) and at high rates in the perianal region(43.0%), the lips (33.0%), and the eyelids (24.0%) butrarely in the vulva (3.8%). Microscopic examinationindicated that these tumors were composed mostly ofmelanocytes and numerous melanophages and thatthese cells manifested a remarkable cellular atypia.Early stages of the tumors occurred in close associa-tion with apocrine sweat glands but not at the dermal-epidermal junction.
A clinical study was conducted on 296 grayhorses of the Lipizzane breed.15 Of the 296horses, dermal melanomas were present in 148horses (50%), 68 of which were �15 yr of age; 51 ofthese were melanoma bearing. In 75.6% of cases,melanotic tumors were detected underneath thetail. None of the affected individuals sufferedany severe clinical effect or were handicapped inperformance. Seltenhammer et al.15 concludedthat in contrast to melanomas in solid coloredhorses characterized by early metastases, melano-mas in grey horses showed less malignancy. Af-fected individuals often had encapsulated nodulesor structures similar to human blue nevi. Prob-ably, this finding at least partially reflects confu-
Fig. 4. Melanocytoma on a young horse. (Courtesy of Dr. J.Traub-Dargatz.)
AAEP PROCEEDINGS � Vol. 52 � 2006 477
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

sion in terminology between true malignantmelanomas and dermal melanomas.
Anaplastic malignant melanomas were composedof sheets of extremely pleomorphic epithelioid cellswith poor pigmentation and many mitoses. Theseare usually seen in horses �20 yr of age and inhorses of any color.
In regard to treatment, one study reported goodsuccess with excising dermal melanomatosis fromthe perineal, perianal, perirectal, or ventral tailregions.16 In a study of three horses, cimetidine(2.5 mg/kg, q 8 h, PO) was shown to decrease thenumber and size of melanomas tumor growth.17
However, a more recent study of 10 horses foundthat cimetidine had no consistent effects on eitherthe number of tumors or tumor surface area overthe 16-wk treatment at a dose of 5mg/kg, q 12 h, PO.18
References and Footnotes1. Irizarry-Rovira AR, Kaufman L, Christian JA, et al. Diag-
nosis of sporotrichosis in a donkey using direct fluorescein-labeled antibody testing. J Vet Diag Invest 2000;12:180–183.
2. Rosser EJ Jr. Sporotrichosis. In: Robinson NE, ed. Cur-rent therapy in equine medicine, 5th ed. St. Louis: W.B.Saunders, 2003;213–214.
3. Kohler LM, Monteiro PC, Hahn RC, et al. In vitro suscep-tibilities of isolates of Sporothrix schenckii to itraconazoleand terbinafine. J Clin Microbiol 2004;42:4319–4320.
4. Pusterla N, Watson JL, Wilson WD, et al. Cutaneous andocular habronemiasis in horses: 63 cases (1988–2002). J Am Vet Med Assoc 2003;222:978–982.
5. Rees CA, Craig TM. Equine cutaneous habronemiasis.In: Robinson NE, ed. Current therapy in equine medicine,5th ed. Philadelphia: W.B. Saunders, 2003;195–197.
6. Spier SJ, Leutenegger CM, Carroll SP, et al. Use of a real-time polymerase chain reaction-based fluorogenic 5 nucleaseassay to evaluate insect vectors of Corynebacterium pseudo-tuberculosis infections in horses. Am J Vet Res 2004;65:829–834.
7. Farstvedt EG, Hendrickson DA, Dickenson CE, et al. Treat-ment of suppurative facial cellulitis and panniculitis causedby Corynebacterium pseudotuberculosis in two horses. J AmVet Med Assoc 2004;224:1139–1142.
8. Aleman M, Spier SJ, Wilson WD, et al. Corynebacteriumpseudotuberculosis infection in horses: 538 cases(1982–1993). J Am Vet Med Assoc 1996;209:804–809.
9. McEntee MF. Equine cutaneous mastocytomas: morphol-ogy, biological behavior and evolution of the lesion. J CompPathol 1991;104:171–178.
10. Whitler WA, Schmotzer WB, Huber MJ, et al. Equine mastcell tumor. Equine Pract 1994;16:16–21.
11. Kay G, Noursaid I, El Hamidi M, et al. Grade III mastocy-toma in a donkey. Vet Rec 2003;152:266–267.
12. Valentine BA. Equine melanocytic tumors: a retrospectivestudy of 53 horses (1988–1991). J Vet Int Med 1998;9:291–297.
13. Fleury C, Berard F, Leblond A, et al. The study of cutaneousmelanomas in Camargue-type gray-skinned horses (2): ep-idemiological survey. Pigment Cell Res 2000;13:47–51.
14. Fleury C, Berard F, Balme B, et al. The study of cutaneousmelanomas in Camargue-type gray-skinned horses (1): clin-ical-pathological characterization. Pigment Cell Res 2000;13:39–46.
15. Seltenhammer MH, Simhofer H, Scherzer S, et al. Equinemelanoma in a population of 296 grey Lipizzaner horses.Equine Vet J 2003;35:153–157.
16. Rowe EL, Sullins KE. Excision as treatment of dermal mel-anomatosis in horses: 11 cases (1994–2000). J Am VetMed Assoc 2004;225:94–96.
17. Goetz TE, Ogilvie GK, Keegan KG, et al. Cimetidine fortreatment of melanomas in three horses. J Am Vet MedAssoc 1990;196:449–452.
18. Bowers JR, Huntington PJ, Slocombe RF. Efficacy of cime-tidine for therapy of skin tumours of horses�10 cases. AustEquine Vet 1994;12:30–32.
aNeogen Corporation, Lexington, KY 40511.bEDDI 20 Gr. Dextrose base, Vedco Inc., St. Joseph, MO 64507.cQuest® Equine Gel, Fort Dodge Animal Health, Overland
Park, KS 66225-5945.
Sarcoids
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
Sarcoids are one of the most common causes of lo-cally aggressive, non-metastatic fibroblastic nodularneoplastic lesions in horses, and they account for35–90% of dermatological neoplasms.1–4
2. Proposed Viral Etiology
Papillomaviridae (animal and human viruses) infectepithelial cells and cause hyperproliferation, warts,papillomas, or condylomas. Bovine papillomavirus(BPV) is currently categorized into six subtypes andtwo groups (A or B). Subgroup A transforms fibro-blast and epithelial cells, whereas subgroup B trans-forms epithelial cells only. It is believed that BPVtypes 1 and 2 (subgroup A) are associated with thegenesis of sarcoid disease. Polymerase chain reac-tion methods have been able to detect viral DNA andRNA from most sarcoids and recently, expression ofthe major transforming oncoprotein, E5, of BPVtypes 1 and 2. BPV types 1 and 2 do not seem toproduce infectious virions but rather persistenceand disease pathogenesis by downregulating majorhistocompatibility complex (MHC) class I expression.5,6
3. Signalment
Sarcoids are more often noted in donkeys and mulesthan horses. Most affected individuals are geld-ings, and the age of onset is between 1 and 7 yr.Thoroughbreds, Warmbloods, and those horses thatoften work cattle, such as Appaloosas, Arabians, andQuarter Horses, seem predisposed to sarcoid forma-tion. Standardbreds seem unlikely to develop sar-coids, possibly because of a decreased expression ofthe MHC class II antigen W13 ELA alleles; however,the aforementioned breeds tend to have an in-creased expression.1
4. Clinical Findings
Multiple lesions are noted in 14–84% of affectedindividuals (Fig. 1). Sarcoids tend to occur in areasof previous trauma or irritation by insects or tack,including the chest, legs, girth, and base of the earsalong with areas of thin skin such as the periocular,muzzle, and ventral abdomen (Fig. 2). Geographi-cal variation seems to result in differing distribution(e.g., the trunk in the United Kingdom and Switzer-land) potentially associated with feeding patterns of
478 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
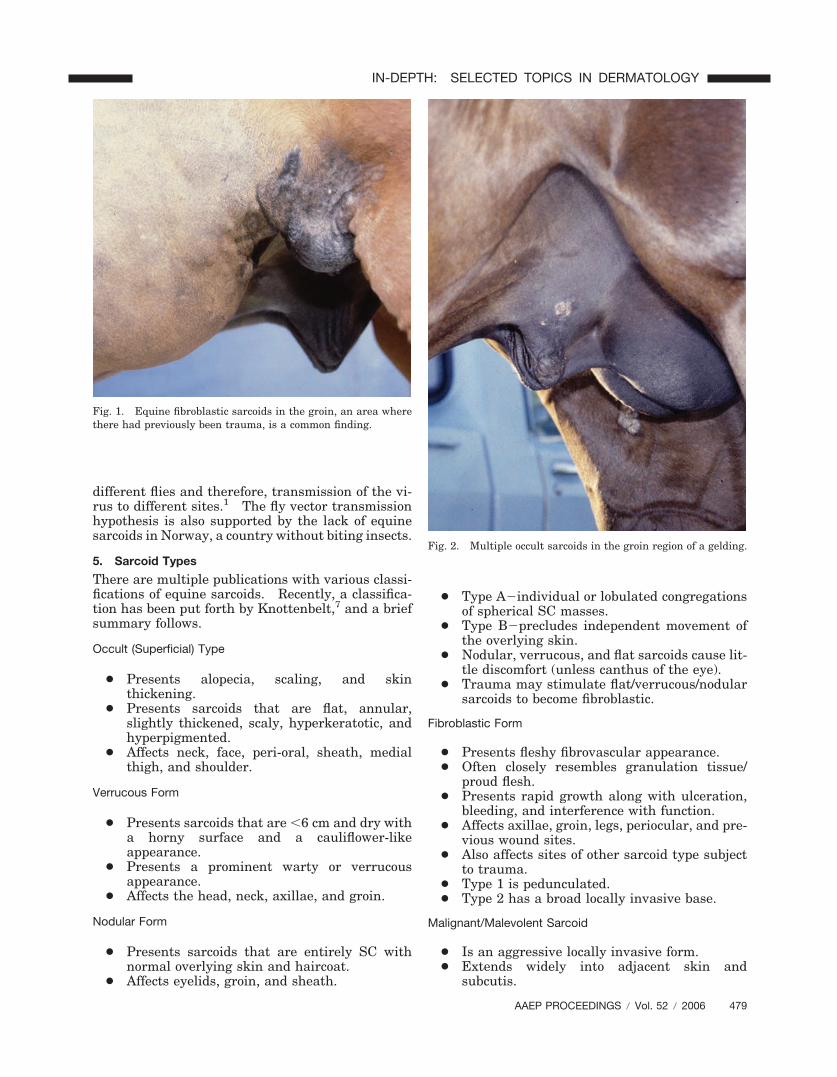
different flies and therefore, transmission of the vi-rus to different sites.1 The fly vector transmissionhypothesis is also supported by the lack of equinesarcoids in Norway, a country without biting insects.
5. Sarcoid Types
There are multiple publications with various classi-fications of equine sarcoids. Recently, a classifica-tion has been put forth by Knottenbelt,7 and a briefsummary follows.
Occult (Superficial) Type
● Presents alopecia, scaling, and skinthickening.
● Presents sarcoids that are flat, annular,slightly thickened, scaly, hyperkeratotic, andhyperpigmented.
● Affects neck, face, peri-oral, sheath, medialthigh, and shoulder.
Verrucous Form
● Presents sarcoids that are �6 cm and dry witha horny surface and a cauliflower-likeappearance.
● Presents a prominent warty or verrucousappearance.
● Affects the head, neck, axillae, and groin.
Nodular Form
● Presents sarcoids that are entirely SC withnormal overlying skin and haircoat.
● Affects eyelids, groin, and sheath.
● Type A�individual or lobulated congregationsof spherical SC masses.
● Type B�precludes independent movement ofthe overlying skin.
● Nodular, verrucous, and flat sarcoids cause lit-tle discomfort (unless canthus of the eye).
● Trauma may stimulate flat/verrucous/nodularsarcoids to become fibroblastic.
Fibroblastic Form
● Presents fleshy fibrovascular appearance.● Often closely resembles granulation tissue/
proud flesh.● Presents rapid growth along with ulceration,
bleeding, and interference with function.● Affects axillae, groin, legs, periocular, and pre-
vious wound sites.● Also affects sites of other sarcoid type subject
to trauma.● Type 1 is pedunculated.● Type 2 has a broad locally invasive base.
Malignant/Malevolent Sarcoid
● Is an aggressive locally invasive form.● Extends widely into adjacent skin and
subcutis.
Fig. 2. Multiple occult sarcoids in the groin region of a gelding.
Fig. 1. Equine fibroblastic sarcoids in the groin, an area wherethere had previously been trauma, is a common finding.
AAEP PROCEEDINGS � Vol. 52 � 2006 479
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

● Is invasive with infiltrated lymphatic vessels.● Has multiple cords of tumor mass.● Elbow and jaw.
Mixed FormsCommon with components of two or more types.
6. Diagnosis
Although it has been suggested that as high as50% of flat or verrucous type sarcoids that arebiopsied will transform into the more aggressivefibroblastic type, a recent roundtable discussion atthe North American Veterinary Dermatology Fo-rum (NAVDM) in 2006 among dermatologists anddermatopathologists from various parts of theworld recommended that biopsies be taken to con-firm your diagnosis so that appropriate therapycan be pursued. If transformation is noted (typ-ically within 2 wk), then consider applying imi-quimod to the affected lesion (see below) toprevent transformation and provide potential res-olution. Also, the attendees at the roundtable didnot find such a high incidence of transformation;however, it could be that the specialists are seeinga skewed population. That being said, when pos-sible, the entire tumor should be removed.
When sampling tissue for dermatohistopathologicevaluation, it is advised to take large (6–8 mm) anddeep biopsies, because small and superficial biopsiesmay read out as granulation tissue over the top of achronic ulcerated sarcoid. Also, some sarcoids mayinitially appear consistent with insect bites (eosino-phils with reactive appearing fibrosis) and are sub-sequently rebiopsied to be consistent with equinesarcoid. Perhaps these cases are truly insect bitesthat later become equine sarcoids. As a generalrule, all well differentiated spindle cell prolifera-tions appear very similar on histopathology. Thisincludes granulation tissue, equine sarcoid, amela-notic melanocytic tumors, nerve sheath tumors, andnon-transmissible, non-sarcoidal well differentiatedfibrosarcoma. Classic equine sarcoid is fairly rec-ognizable; however, it is not terribly dissimilar fromthe other listed differentials. The classic appear-ance consists of overlying epidermal hyperplasiaand perpendicular arrangement of some spindlecells with surface epithelium creating a picket fencepattern.1 Problems in diagnosis arise when thereis no surface epithelium, when the lesion is trauma-tized with overlying granulation tissue as men-tioned above, or when the mass is in the deep dermisto subcutis without the overlying typical changes.In cases where the dermatohistopathology does notsupport the clinical diagnosis, polymerase chain re-action analysis for BPV may be of value.
7. Management/Treatment
Lesions may progress if they are handled andrarely, may regress spontaneously. The generalrule of thumb is if it is flat, leave it alone, but if itis fibroblastic, treat aggressively or refer. To
date, there is no one treatment option that hasproved universally successful. Surgical excision,cryosurgery, carbon dioxide LASER, radiofre-quency hyperthermia, radiotherapy, chemother-apy, immunotherapy, or combinations thereof aresummarized below.
8. Surgical Approaches
Surgical excision8,9 alone has met with 50–64% re-currence within 6 mo. Thus, surgery is used moreoften to debulk the mass and improve combinationtreatment. Typically, 0.5–1 cm margins have beendescribed; however, in the NAVDF roundtable, thegroup felt that 3–10 cm margins were more appro-priate in an attempt to decrease recurrence. Sur-gical excision, therefore, should be performed undergeneral anesthesia (not local anesthesia) to performthorough extirpation. To close such a defect, pinchor split thickness graft can be used. One shouldanticipate increased healing time and excess gran-ulation tissue. In general, a cosmetic outcome canbe achieved.
Cryotherapy8–10 has achieved up to 70% successwith no recurrence. The procedure involves apply-ing probes cooled to �20–30°C directly on the sar-coid with 2–3 freeze/thaw cycles. Thermocoupleneedles are used to monitor depth and degree offreezing. Hyperemia, hemorrhage, swelling, andlocal edema follow, resulting in damaged epitheliumand viral particles at the site. Average healingtime is 2.4 mo. The hair follicles are damaged ordestroyed, and hair regrows white or not at all.Facial nerve paralysis, septic arthritis, loss of uppereyelid, and eviscerated globe are some of the com-plications to discuss with the owner before embark-ing on this treatment modality. Regression ofmultiple tumors (when only a select few are treated)has been reported inconsistently and is likely theresult of a cryoimmune response to sarcoid-cellcomponents.
Carbon dioxide LASER11–13 cuts and evaporatestumor tissue with accurate dissection and excellentcosmetic results. The advantages include de-creased to no post-operation swelling, no post-oper-ation pain on palpation, primary wound closure orsecond intention healing without hypergranulation,and superior cosmesis. It has been reported that81% of 59 horses with sarcoids treated by CO2 laserwere free from recurrence after 12 mo. In the samestudy, 60% of 35 horses in which sarcoids weretreated by cryosurgery and 64% of 14 horses inwhich sarcoids were treated by conventional surgerywere sarcoid free after 12 mo. The improved suc-cess rates may be caused by the extension of thethermal-killing effects and vaporization of viral par-ticles with CO2 LASER, thus extending the marginsand minimizing recontamination, respectively.Regardless of the technique, animals with multiplesarcoids were more predisposed to recurrence, anddonkeys showed a significantly lower recurrencerate than horses.
480 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

9. Intralesional Approaches
Radiofrequency (orthovoltage) current induced hy-perthermia1 involves heating sarcoids to 50°C for30 s (2 MHz current) with a thermoprobe every 1–3wk. Hyperthermia is often combined with radio-therapy, immunotherapy, and chemotherapy. Lim-ited reports on success of use in three cases resulted inregression with no recurrence 7–12 mo after the lasttreatment.
Interstitial brachytherapy4,14 using various iso-topes (e.g., permanently implanted seeds of radon-222 or gold-198, removable needles of radium-226,cobalt-60, or iridium-192, and 192Ir seeds using anafter loading technique) has been used to treatequine sarcoids. Responses range from 50% to100% sarcoid free for 1 yr, alone or in combinationwith surgical debulking and/or hyperthermia, espe-cially when the peri-orbital is involved. Fortu-nately, the treatment radiates the tumor locally andspares adjacent healthy tissue. Disadvantages in-clude exposure for the surgeon, need for specialequipment, size of the tumor limiting its application,poor local cosmesis (alopecia and leukotrichia), andpatient containment in a radiation safety approvedarea that increases costs.
Intratumoral cisplatin15–20 (an emulsion of 10 mgof powdered cisplatin, 1 ml of sterile saline, and 2 mlof patient’s serum, medical grade sesame or peanutoil [resultant solution contains 3.3 mg of cisplatinper milliliter], or aqueous cisplatin [Platinola at 1mg/ml]) has proven successful as a sole chemother-apeutic treatment or when performed after debulk-ing the tumor. The procedure involves pre-treatingthe area with local anesthetic and then injecting themixture into multiple planes no further than 0.6–1cm apart at the base of the tumor and surroundingtissue at a dose rate of 0.97 mg of cisplatin/cm2 oftissue every 2 wk through four injections using Luerlocked small gauge needles (22–25 gauge). It hasbeen reported that 87% of these horses have notrelapsed after one year. Disadvantages includeneed for safety precautions (chemotherapy gear,Luer lock syringes, latex gloves, protective eyewear,surgical masks, and biohazard disposal), potentialfor secondary peri-injectional infections, and oc-currence of some degree of tissue sloughing andperilesional swelling. A serious human healthconcern is the potential for carcinogenicity andteratogenicity of all those handling treated horses,including extruded drug and the patient’s sweat,urine, and/or feces. At this time, post-chemo-therapeutic treatment quarantine times have notbeen addressed. Recently, cisplatin injectionshave been combined with adjunctive therapies totry to improve responses. Thus far, the additionof a single high dose of interleukin-2 has not im-proved efficacy over cisplatin injections alone(�80%). However, cisplatin intralesional injec-tions followed by electropulsation (improves diffu-sion of chemotherapeutics through tumors) of
sarcoids resulted in regression after only two tothree electrochemotherapies in 100% of thetreated lesions. No adverse effect from the elec-tric pulses was observed, and no regrowth wasobserved in the 18-mo follow-up period.
10. Topical Cytotoxic Approach
XXTerra,b a caustic agent containing zinc chloride,has anecdotally had some benefit. The product alsocontains water and bloodroot (Sanguineria canaden-sis). XXTerra is proposed to alter the tumor anti-gens of sarcoids in vivo, apparently stimulating theimmune system to recognize them as foreign andmount a response quite similar to the host versusgraft rejection. It can become quite sore to thetouch, but this sensitivity lasts only a few days.According to the manufacturer, XXTerra has beeneffective in �95% of the sarcoids treated. Totalfailures have been observed in rare instances andhave been attributed to a non-functional immunesystem. XXTerra seems safe on normal skin. Theproduct is applied 0.125- to 0.25-in thick over af-fected areas and then covered with a non-adherentTelfa pad and bandage. The procedure is repeatedevery 4–6 days until the tumor is ready to slough(i.e., purulent debris and blood is noted). For sar-coids located where a bandage cannot be used, theproduct is topically applied daily for 4–6 days andthen repeated at 4-day intervals until the tumorsloughs.
AW–3–LUDES,21,c a topical proprietary ointmentcontaining a variety of heavy metals and the antim-itotic compounds 5-fluorouracil and thiouracil, is ad-ministered on successive or alternate days for 3–5treatments. Within 5–10 wk, preferential necrosisand sloughing of the sarcoid tissues should be noted.
11. Immunomodulatory Approach
Bacillus of Calmette and Guerin (BCG; Regressin-Vd),9,22 cell wall fractions of an attenuated strain ofMycobacterium bovis, acts as an immunomodulatorthat stimulates host lymphocyte and natural killercells. Optimal results are obtained if this productis used in an immunocompetent host with limitedtumor burden or post-debulking in the periocularregion. An 83.5% (10 of 12) rate of remission hasbeen achieved with periocular sarcoids, whereas useon all other body regions resulted in a 48.5% rate ofremission. After two or more injections, swellingoccurs within minutes or hours and may be exten-sive. Inflammation progresses to necrosis and ul-ceration of the tumor along with pyrexia,leukocytosis, non-fatal anaphylaxis, severe local in-flammatory reactions (including lymphangitis), sep-tic arthritis, and general malaise in some cases.Complete resolution of the process and tumor takesmonths (6 wk to 1 yr or more). Complications caninclude death from anaphylactic shock after two ormore injections. Therefore, pre-medication withflunixin meglumine and corticosteroids has beenrecommended. An advantage is tumor specificity
AAEP PROCEEDINGS � Vol. 52 � 2006 481
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

whereby only sarcoid cell necrosis is noted on his-topathologic post-BCG evaluation.
Similarly, Propionibacterium acnes is a non-spe-cific immunostimulant that may induce macrophageactivation and lymphokine production, increase nat-ural killer cell activity, and enhance cell mediatedimmunity against immunogenic components ofequine sarcoids. Protocols vary from intralesionalto IV injections once weekly for 6–8 wk. Susceptiblelesions generally show improvement after two to threetreatments, and eventually, they necrose and slough.
Autogenous vaccination,23 using autogenous poly-merized tumor tissue combined with tuberculin pu-rified protein derivative as an adjuvant, resulted incomplete regression in nine horses with refractorysarcoids. However, because the risks include tu-mor production and transmission of other diseases,this procedure should only be attempted in the mostrefractory of cases and with individual patientsknown to be negative for equine infectious anemia.
Imiquimod 5%g24 is an immune-response modifierthat was shown to have potent antiviral and antitu-mor activity in animal models and humans. Untilrecently, the successful use of topical imiquimod inthe treatment of equine sarcoids has been anecdot-ally reported. An open label study evaluating theefficacy of topically applied imiquimod 5% cream (3times per week) for the treatment of various equinesarcoids revealed a �75% reduction in tumor size in13 of 16 (81.3%) tumors in the study over 8–24 wk;9 of them (56.2%) showed complete resolution.The most common adverse effects included exudate,erythema, erosions, and alopecia, which were lim-ited to the tumor and adjacent areas. Based on theseresults, topical imiquimod seems to be a good thera-peutic option for the treatment of equine sarcoids andto prevent tumor transformation post-biopsy.
12. Future Therapeutic Direction
The positive response to the immunomodulator Al-dara supports the hypothesis of a viral component tothe etiology of sarcoids. Based on these findingsand the response to non-specific immunomodulatoryagents, perhaps we should focus our treatment di-rection toward specific anti-viral agents (e.g., riba-virin) and/or other specific anti-viral immune-response modifiers (e.g., interferon), as opposed totoxic chemotherapeutic agents and expensive surgi-cal extirpation.
13. Client Education
Prognosis depends on many variables such as site,size, aggressiveness, number of lesions, number oftreatment attempts, and location (legs and axillae �aggressive; periocular � vulnerable). Failure to re-solve the lesions frequently results in regrowth ofthe tumor, which may be more aggressive with exten-sive local infiltration and faster growth.8 Combinedtherapy may provide fewer chances of relapse. If sar-coids are noted on a pre-purchase examination, thelesion(s) should be recorded, and owners should be
made aware of their location along with the potentialrisk that even flat sarcoids may become malignant.
References and Footnotes1. Scott DW, Miller WH. Neoplastic and non-neoplastic
tumors�sarcoids. In: Scott DW, Miller WH, eds. Equinedermatology. St. Louis: W.B. Saunders, 2003;720–732.
2. Pascoe RRR, Knottenbelt DC. Manual of equine dermatol-ogy. Neoplastic conditions. London: W.B. Saunders,1999;241–267.
3. Goodrich L, Gerber H, Marti E, et al. Equine sarcoids.Vet Clin North Am [Equine Pract] 1998;14:607–621.
4. Foy JM, Rashmir-Raven AM, Brashier MK. Commonequine tumors. Compend Cont Educ Pract Vet 2002;24:242–252.
5. Chambers G, Ellsmore VA, O’Brien PM, et al. Association ofbovine papillomavirus with the equine sarcoid. J Gen Virol2003;84:1055–1062.
6. Chambers G, Ellsmore VA, O’Brien PM, et al. Sequencevariants of bovine papillomavirus E5 detected in equine sar-coids. Virus Res 2003;96:141–145.
7. Knottenbelt DC. A suggested clinical classification for theequine sarcoid. Clin Tech Equine Pract 2005;4:278–295.
8. Knottenbelt DC, Kelly DF. The diagnosis and treatment ofperiorbital sarcoid in the horse: 445 cases 1974 to1999. Vet Ophthalmol 2000;3:169–191.
9. Martens A, De Moor A, Vlaminck L, et al. Evaluation ofexcision, cryosurgery and local BCG vaccination for treat-ment of equine sarcoids. Vet Rec 2001;1:665–669.
10. Hanson RR. Cryotherapy for equine skin conditions.In: Robinson NE, ed. Current therapy in equine medicine,4th ed. Philadelphia: W.B. Saunders, 1997;370–372.
11. Carstanjen B, Jordan P, Lepage OM. Carbon dioxide laseras a surgical instrument for sarcoid therapy�a retrospectivestudy on 60 cases. Can Vet J 1997;38:773–776.
12. McCauley CT, Hawkins JF, Adams SB, et al. Use of a car-bon dioxide laser for surgical management of cutaneousmasses in horses: 32 cases (1993–2000). J Am Vet MedAssoc 2002;220:1192–1197.
13. Lucroy MD, Bartels KE. Using biomedical lasers in veteri-nary practice. Vet Med 2000;95(10):4–9.
14. Theon AP, Pascoe JR. Iridium-192 interstitial brachyther-apy for equine periocular tumors: treatment results andprognostic factors in 115 horses. Equine Vet J 1995;27:117–121.
15. Spoormakers TJ, Klein WR, Jacobs JJ, et al. Comparison ofthe efficacy of local treatment of equine sarcoids with IL-2 orcisplatin/IL-2. Cancer Immunol Immunother 2003;52:179–184.
16. Rols MP, Tamzali Y, Teissie J. Electrochemotherapy ofhorses. A preliminary clinical report. Bioelectrochemistry2002;55:101–105.
17. Theon AP. Intralesional and topical chemotherapy and im-munotherapy. Vet Clin North Am [Equine Pract] 1998;14:659–672.
18. Theon AP, Pascoe JR, Madigan JE, et al. Comparison ofintratumoral administration of cisplatin versus bleomycin fortreatment of periocular squamous cell carcinomas in horses.Am J Vet Res 1997;58:431.
19. Theon AP, Pascoe JR, Meagher DM. Perioperative intratu-moral administration of cisplatin for treatment of cutaneoustumors in equidae. J Am Vet Med Assoc 1994;205:1170–1176.
20. Theon AP, Pascoe JR, Carlson GP, et al. Intratumoral che-motherapy with cisplatin in oily emulsion in horses. J AmVet Med Assoc 1993;202:261–267.
21. Newton SA. Periocular sarcoids in the horse: three casesof successful treatment. Equine Vet Edu 2000;12:137–143.
22. Komaromy AM, Andrew SE, Brooks DE, et al. Periocularsarcoid in a horse. Vet Ophthalmol 2004;7:141–146.
23. Kinnunen RE, Tallberg T, Stenback H, et al. Equine sarcoidtumour treated by autogenous tumour vaccine. AnticancerRes 1999;19:3367–3374.
482 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
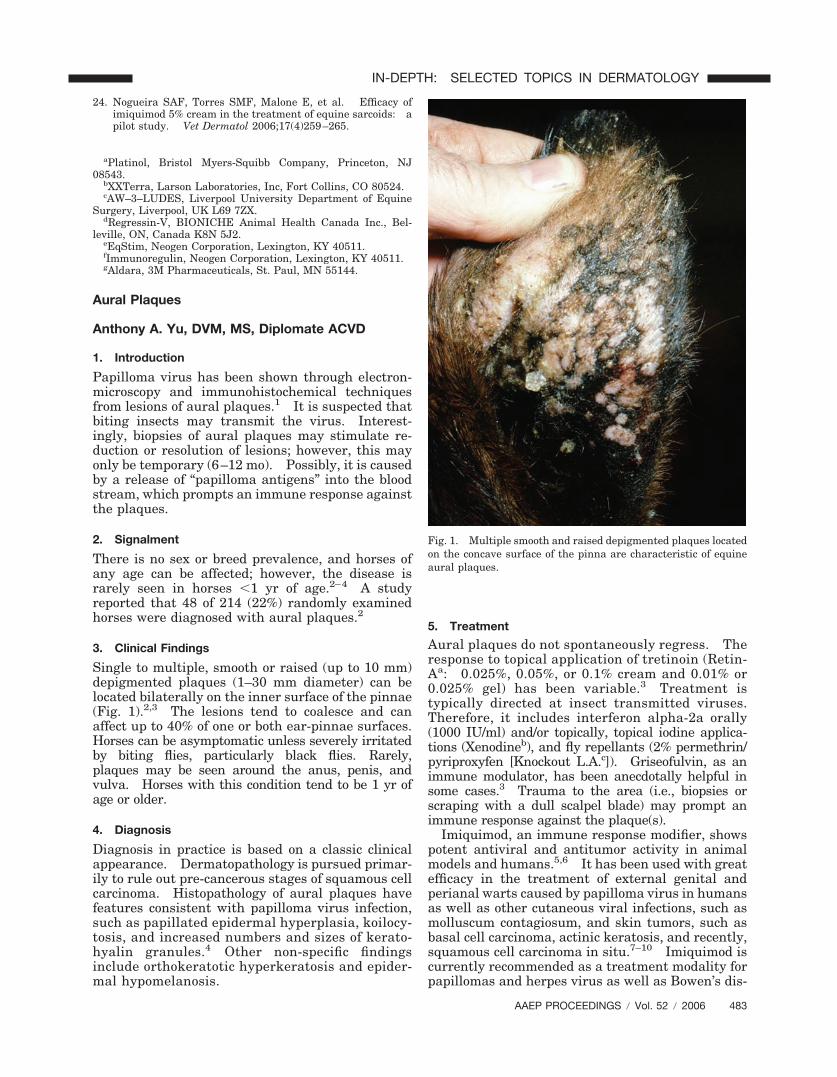
24. Nogueira SAF, Torres SMF, Malone E, et al. Efficacy ofimiquimod 5% cream in the treatment of equine sarcoids: apilot study. Vet Dermatol 2006;17(4)259–265.
aPlatinol, Bristol Myers-Squibb Company, Princeton, NJ08543.
bXXTerra, Larson Laboratories, Inc, Fort Collins, CO 80524.cAW–3–LUDES, Liverpool University Department of Equine
Surgery, Liverpool, UK L69 7ZX.dRegressin-V, BIONICHE Animal Health Canada Inc., Bel-
leville, ON, Canada K8N 5J2.eEqStim, Neogen Corporation, Lexington, KY 40511.fImmunoregulin, Neogen Corporation, Lexington, KY 40511.gAldara, 3M Pharmaceuticals, St. Paul, MN 55144.
Aural Plaques
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
Papilloma virus has been shown through electron-microscopy and immunohistochemical techniquesfrom lesions of aural plaques.1 It is suspected thatbiting insects may transmit the virus. Interest-ingly, biopsies of aural plaques may stimulate re-duction or resolution of lesions; however, this mayonly be temporary (6–12 mo). Possibly, it is causedby a release of “papilloma antigens” into the bloodstream, which prompts an immune response againstthe plaques.
2. Signalment
There is no sex or breed prevalence, and horses ofany age can be affected; however, the disease israrely seen in horses �1 yr of age.2–4 A studyreported that 48 of 214 (22%) randomly examinedhorses were diagnosed with aural plaques.2
3. Clinical Findings
Single to multiple, smooth or raised (up to 10 mm)depigmented plaques (1–30 mm diameter) can belocated bilaterally on the inner surface of the pinnae(Fig. 1).2,3 The lesions tend to coalesce and canaffect up to 40% of one or both ear-pinnae surfaces.Horses can be asymptomatic unless severely irritatedby biting flies, particularly black flies. Rarely,plaques may be seen around the anus, penis, andvulva. Horses with this condition tend to be 1 yr ofage or older.
4. Diagnosis
Diagnosis in practice is based on a classic clinicalappearance. Dermatopathology is pursued primar-ily to rule out pre-cancerous stages of squamous cellcarcinoma. Histopathology of aural plaques havefeatures consistent with papilloma virus infection,such as papillated epidermal hyperplasia, koilocy-tosis, and increased numbers and sizes of kerato-hyalin granules.4 Other non-specific findingsinclude orthokeratotic hyperkeratosis and epider-mal hypomelanosis.
5. Treatment
Aural plaques do not spontaneously regress. Theresponse to topical application of tretinoin (Retin-Aa: 0.025%, 0.05%, or 0.1% cream and 0.01% or0.025% gel) has been variable.3 Treatment istypically directed at insect transmitted viruses.Therefore, it includes interferon alpha-2a orally(1000 IU/ml) and/or topically, topical iodine applica-tions (Xenodineb), and fly repellants (2% permethrin/pyriproxyfen [Knockout L.A.c]). Griseofulvin, as animmune modulator, has been anecdotally helpful insome cases.3 Trauma to the area (i.e., biopsies orscraping with a dull scalpel blade) may prompt animmune response against the plaque(s).
Imiquimod, an immune response modifier, showspotent antiviral and antitumor activity in animalmodels and humans.5,6 It has been used with greatefficacy in the treatment of external genital andperianal warts caused by papilloma virus in humansas well as other cutaneous viral infections, such asmolluscum contagiosum, and skin tumors, such asbasal cell carcinoma, actinic keratosis, and recently,squamous cell carcinoma in situ.7–10 Imiquimod iscurrently recommended as a treatment modality forpapillomas and herpes virus as well as Bowen’s dis-
Fig. 1. Multiple smooth and raised depigmented plaques locatedon the concave surface of the pinna are characteristic of equineaural plaques.
AAEP PROCEEDINGS � Vol. 52 � 2006 483
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
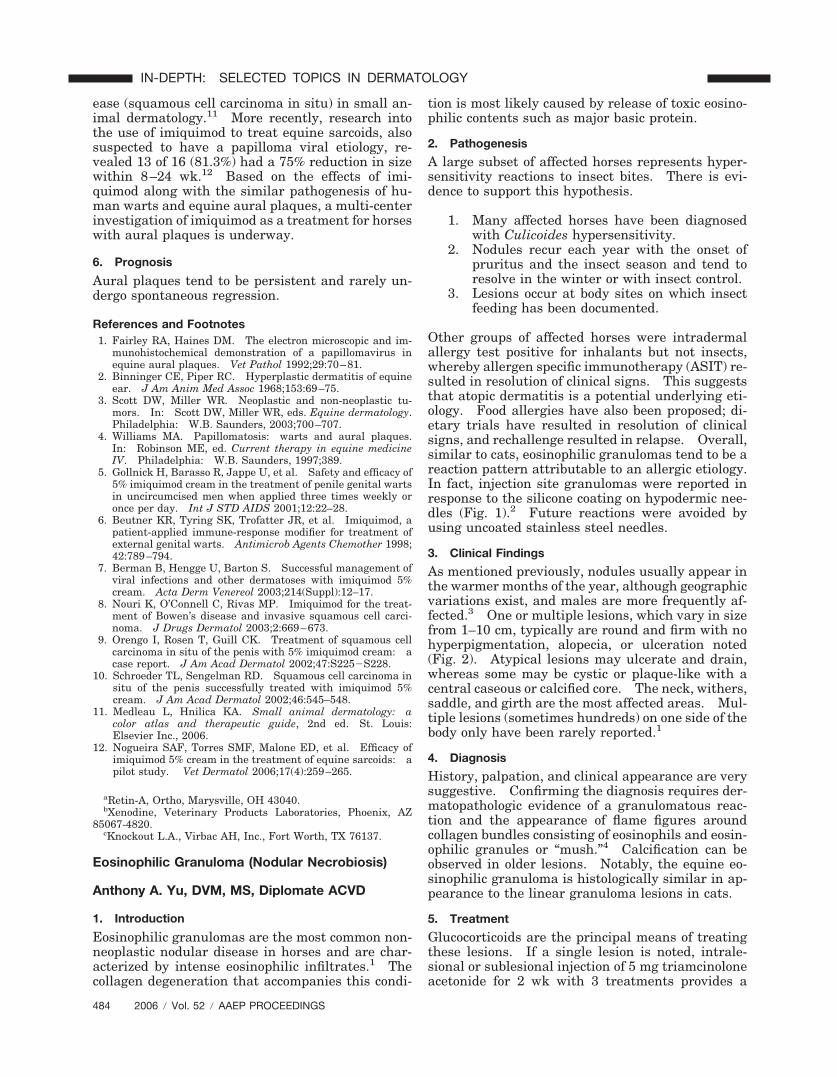
ease (squamous cell carcinoma in situ) in small an-imal dermatology.11 More recently, research intothe use of imiquimod to treat equine sarcoids, alsosuspected to have a papilloma viral etiology, re-vealed 13 of 16 (81.3%) had a 75% reduction in sizewithin 8–24 wk.12 Based on the effects of imi-quimod along with the similar pathogenesis of hu-man warts and equine aural plaques, a multi-centerinvestigation of imiquimod as a treatment for horseswith aural plaques is underway.
6. Prognosis
Aural plaques tend to be persistent and rarely un-dergo spontaneous regression.
References and Footnotes1. Fairley RA, Haines DM. The electron microscopic and im-
munohistochemical demonstration of a papillomavirus inequine aural plaques. Vet Pathol 1992;29:70–81.
2. Binninger CE, Piper RC. Hyperplastic dermatitis of equineear. J Am Anim Med Assoc 1968;153:69–75.
3. Scott DW, Miller WR. Neoplastic and non-neoplastic tu-mors. In: Scott DW, Miller WR, eds. Equine dermatology.Philadelphia: W.B. Saunders, 2003;700–707.
4. Williams MA. Papillomatosis: warts and aural plaques.In: Robinson ME, ed. Current therapy in equine medicineIV. Philadelphia: W.B. Saunders, 1997;389.
5. Gollnick H, Barasso R, Jappe U, et al. Safety and efficacy of5% imiquimod cream in the treatment of penile genital wartsin uncircumcised men when applied three times weekly oronce per day. Int J STD AIDS 2001;12:22–28.
6. Beutner KR, Tyring SK, Trofatter JR, et al. Imiquimod, apatient-applied immune-response modifier for treatment ofexternal genital warts. Antimicrob Agents Chemother 1998;42:789–794.
7. Berman B, Hengge U, Barton S. Successful management ofviral infections and other dermatoses with imiquimod 5%cream. Acta Derm Venereol 2003;214(Suppl):12–17.
8. Nouri K, O’Connell C, Rivas MP. Imiquimod for the treat-ment of Bowen’s disease and invasive squamous cell carci-noma. J Drugs Dermatol 2003;2:669–673.
9. Orengo I, Rosen T, Guill CK. Treatment of squamous cellcarcinoma in situ of the penis with 5% imiquimod cream: acase report. J Am Acad Dermatol 2002;47:S225�S228.
10. Schroeder TL, Sengelman RD. Squamous cell carcinoma insitu of the penis successfully treated with imiquimod 5%cream. J Am Acad Dermatol 2002;46:545–548.
11. Medleau L, Hnilica KA. Small animal dermatology: acolor atlas and therapeutic guide, 2nd ed. St. Louis:Elsevier Inc., 2006.
12. Nogueira SAF, Torres SMF, Malone ED, et al. Efficacy ofimiquimod 5% cream in the treatment of equine sarcoids: apilot study. Vet Dermatol 2006;17(4):259–265.
aRetin-A, Ortho, Marysville, OH 43040.bXenodine, Veterinary Products Laboratories, Phoenix, AZ
85067-4820.cKnockout L.A., Virbac AH, Inc., Fort Worth, TX 76137.
Eosinophilic Granuloma (Nodular Necrobiosis)
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
Eosinophilic granulomas are the most common non-neoplastic nodular disease in horses and are char-acterized by intense eosinophilic infiltrates.1 Thecollagen degeneration that accompanies this condi-
tion is most likely caused by release of toxic eosino-philic contents such as major basic protein.
2. Pathogenesis
A large subset of affected horses represents hyper-sensitivity reactions to insect bites. There is evi-dence to support this hypothesis.
1. Many affected horses have been diagnosedwith Culicoides hypersensitivity.
2. Nodules recur each year with the onset ofpruritus and the insect season and tend toresolve in the winter or with insect control.
3. Lesions occur at body sites on which insectfeeding has been documented.
Other groups of affected horses were intradermalallergy test positive for inhalants but not insects,whereby allergen specific immunotherapy (ASIT) re-sulted in resolution of clinical signs. This suggeststhat atopic dermatitis is a potential underlying eti-ology. Food allergies have also been proposed; di-etary trials have resulted in resolution of clinicalsigns, and rechallenge resulted in relapse. Overall,similar to cats, eosinophilic granulomas tend to be areaction pattern attributable to an allergic etiology.In fact, injection site granulomas were reported inresponse to the silicone coating on hypodermic nee-dles (Fig. 1).2 Future reactions were avoided byusing uncoated stainless steel needles.
3. Clinical Findings
As mentioned previously, nodules usually appear inthe warmer months of the year, although geographicvariations exist, and males are more frequently af-fected.3 One or multiple lesions, which vary in sizefrom 1–10 cm, typically are round and firm with nohyperpigmentation, alopecia, or ulceration noted(Fig. 2). Atypical lesions may ulcerate and drain,whereas some may be cystic or plaque-like with acentral caseous or calcified core. The neck, withers,saddle, and girth are the most affected areas. Mul-tiple lesions (sometimes hundreds) on one side of thebody only have been rarely reported.1
4. Diagnosis
History, palpation, and clinical appearance are verysuggestive. Confirming the diagnosis requires der-matopathologic evidence of a granulomatous reac-tion and the appearance of flame figures aroundcollagen bundles consisting of eosinophils and eosin-ophilic granules or “mush.”4 Calcification can beobserved in older lesions. Notably, the equine eo-sinophilic granuloma is histologically similar in ap-pearance to the linear granuloma lesions in cats.
5. Treatment
Glucocorticoids are the principal means of treatingthese lesions. If a single lesion is noted, intrale-sional or sublesional injection of 5 mg triamcinoloneacetonide for 2 wk with 3 treatments provides a
484 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
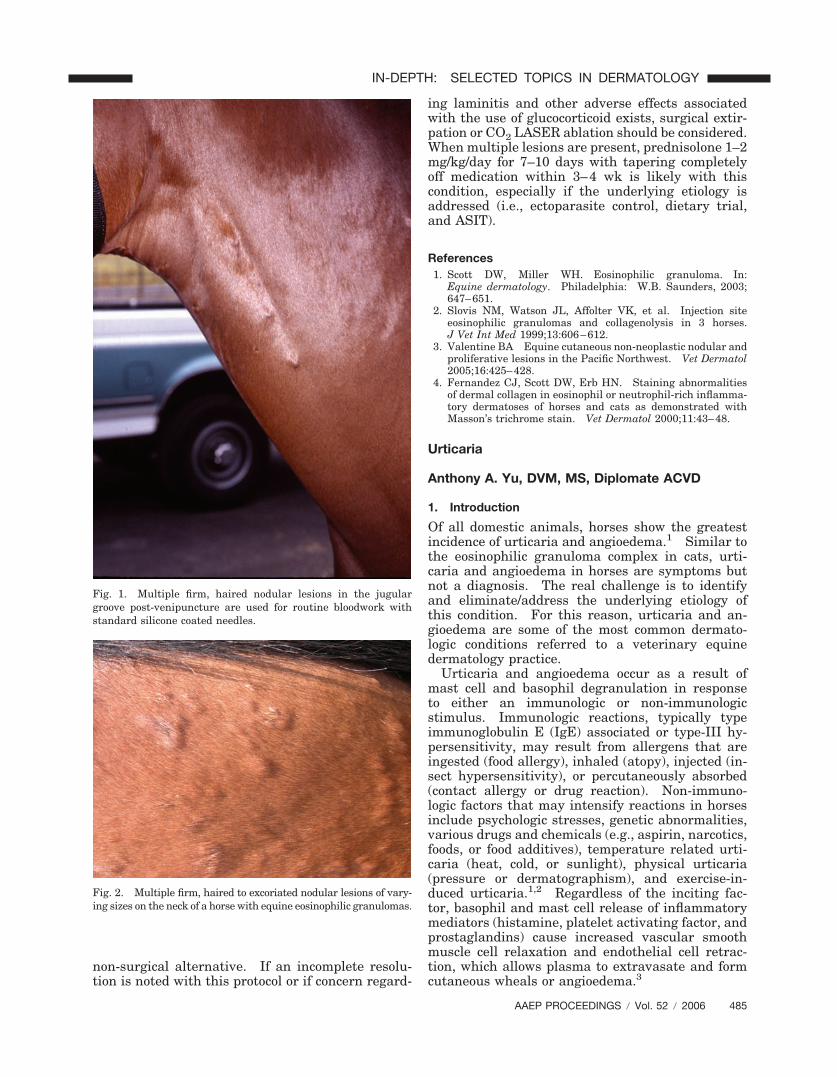
non-surgical alternative. If an incomplete resolu-tion is noted with this protocol or if concern regard-
ing laminitis and other adverse effects associatedwith the use of glucocorticoid exists, surgical extir-pation or CO2 LASER ablation should be considered.When multiple lesions are present, prednisolone 1–2mg/kg/day for 7–10 days with tapering completelyoff medication within 3–4 wk is likely with thiscondition, especially if the underlying etiology isaddressed (i.e., ectoparasite control, dietary trial,and ASIT).
References1. Scott DW, Miller WH. Eosinophilic granuloma. In:
Equine dermatology. Philadelphia: W.B. Saunders, 2003;647–651.
2. Slovis NM, Watson JL, Affolter VK, et al. Injection siteeosinophilic granulomas and collagenolysis in 3 horses.J Vet Int Med 1999;13:606–612.
3. Valentine BA Equine cutaneous non-neoplastic nodular andproliferative lesions in the Pacific Northwest. Vet Dermatol2005;16:425–428.
4. Fernandez CJ, Scott DW, Erb HN. Staining abnormalitiesof dermal collagen in eosinophil or neutrophil-rich inflamma-tory dermatoses of horses and cats as demonstrated withMasson’s trichrome stain. Vet Dermatol 2000;11:43–48.
Urticaria
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
Of all domestic animals, horses show the greatestincidence of urticaria and angioedema.1 Similar tothe eosinophilic granuloma complex in cats, urti-caria and angioedema in horses are symptoms butnot a diagnosis. The real challenge is to identifyand eliminate/address the underlying etiology ofthis condition. For this reason, urticaria and an-gioedema are some of the most common dermato-logic conditions referred to a veterinary equinedermatology practice.
Urticaria and angioedema occur as a result ofmast cell and basophil degranulation in responseto either an immunologic or non-immunologicstimulus. Immunologic reactions, typically typeimmunoglobulin E (IgE) associated or type-III hy-persensitivity, may result from allergens that areingested (food allergy), inhaled (atopy), injected (in-sect hypersensitivity), or percutaneously absorbed(contact allergy or drug reaction). Non-immuno-logic factors that may intensify reactions in horsesinclude psychologic stresses, genetic abnormalities,various drugs and chemicals (e.g., aspirin, narcotics,foods, or food additives), temperature related urti-caria (heat, cold, or sunlight), physical urticaria(pressure or dermatographism), and exercise-in-duced urticaria.1,2 Regardless of the inciting fac-tor, basophil and mast cell release of inflammatorymediators (histamine, platelet activating factor, andprostaglandins) cause increased vascular smoothmuscle cell relaxation and endothelial cell retrac-tion, which allows plasma to extravasate and formcutaneous wheals or angioedema.3
Fig. 1. Multiple firm, haired nodular lesions in the jugulargroove post-venipuncture are used for routine bloodwork withstandard silicone coated needles.
Fig. 2. Multiple firm, haired to excoriated nodular lesions of vary-ing sizes on the neck of a horse with equine eosinophilic granulomas.
AAEP PROCEEDINGS � Vol. 52 � 2006 485
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

2. Signalment
There seems to be no characteristic signalment as-sociated with the development of urticaria or angio-edema. Thoroughbred and Arabian horsesbetween 1 and 10 yr of age seem to be affectedfrequently because of their increased predispositionto allergic dermatitis.
3. Clinical Findings
Pitting edema is the key clinical feature of urticariaand angioedema, although some hives can be quitefirm on palpation. Inflammatory lesions, tumors,and fluid filled swellings do not pit on compression.The onset of clinical lesions can be acute or peracutewithin minutes to hours post challenge from expo-sure to the inciting factor. Pruritus is variable.The overlying skin is normal, and there is no alope-cia. Lesions vary in shape and size and maypresent as papular, annular, giant, or gyrate (ser-piginous, linear, or arciform) wheals (Figs. 1 and 2;Table 1). In cases with severe dermal edema, ooz-ing of serum from the skin surface and possibly,cracking and superficial sloughing of the hair andskin that resembles pyoderma and vasculitis may benoted.1 Angioedematous reactions are SC, local-ized to generalized, gravity dependent fluid swell-ings that are variably pruritic, and may have serumleakage or hemorrhage. The pattern of distribu-tion includes the head, extremities, and, ventral ab-domen and thorax. Angioedema may be acutaneous manifestation of systemic and/or seriousdisease.
4. Underlying Etiologies
Urticaria and angioedema are symptoms ratherthan specific disease entities. It is often seen justbefore races (perhaps psychogenic) or in associationwith insect or arthropod envenomation, various in-fections (strangles, dermatophytosis, dermatophilo-sis, dourine, babesiasis, surra, horse pox, or mal decaderas), intestinal parasitism (Cyathostomosis),topical applications (especially parasiticidal sprays,dips, and pour-ons), systemic medicaments (espe-cially trimethoprim potentiated sulfonamides,penicillin, phenylbutazone, ivermectin, aspirin,guaiphenesin, phenothiazine, streptomycin, oxytet-racycline, gas anesthesia, or iron dextrans), feed-stuffs (pasture plants or concentrates), contactants(saddle soaps, leather conditioners, or tack), variousbiologicals (strangles, encephalomyelitis, and salmo-nellosis vaccines or botulinum and tetanus toxoids),snake bites, hypodermiasis, erythema multiforme,inhalants (pollens, molds, or chemicals), purpurahemorrhagica, plants (stinging nettle), hematoma(especially hemophiliacs), lymphangitis, abscess/pyoderma, cellulitis, vasculitis (immune mediatedand photoactivated), lymphoreticular neoplasia,mast cell tumor, or amyloidosis.1,2,4–10
5. Diagnosis
Based on the extensive list of potential causes, aveterinarian’s task can seem ominous. Careful ex-amination of the horse’s history and environmentare key to establishing a possible etiology. For in-stance, the sudden onset of wheals associated withthe administration of a drug renders the causereadily apparent. A protracted history may bemore difficult to decipher, because eruptions waxand wane, environmental challenges occur daily,and medications are often used concurrently withfeed supplements.
Fig. 1. Conventional urticaria with mixed papular and wheallesions involving the face and neck of a pollen sensitive horse.
Fig. 2. Conventional urticaria with mixed papular and wheallesions involving the trunk of pollen sensitive horse in Fig. 1.
486 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

Physical urticaria (dermatographism) is easilydistinguished by drawing a pattern on the skin witha blunt object. Within 10–15 min, a positive reac-tion is denoted by marked edematous swelling of theinscribed pattern. Historical evidence of dermatog-raphism includes swelling involving areas of lightpressure such as under the saddle, bridle, or girth.Temperature sensitive urticaria will similarly de-velop edematous swelling within 15 min of cold (icecube) or heat (hot pack hand warmers) application tothe skin. Exercise-induced urticaria and cholin-ergic urticaria are easily confused. Cholinergic ur-ticaria results from an increase, either active(exercise related) or passive (hot bath), in body coretemperature, whereas exercise-induced urticaria re-quires the active stimulus of exercise.4,11
Skin scrapings, fungal cultures, impressionsmears, and serology are valuable diagnostic tools ifan infectious etiology is suspected. Biopsies mayhelp to rule out other potential etiologies. Biopsiesare recommended when the lesions are firmer thanexpected or when the disease has been ongoing (�2mo). A dermatopathologist with an interest inequine dermatology is advised, especially if second-ary self-inflicted trauma is involved. Typical his-topathologic findings of urticaria or angioedemavary from a simple vascular dilatation and edema inthe superficial and middle dermis to pure perivas-cular dermatitis with varying numbers of mononu-clear cells, neutrophils, mast cells, and eosinophils.2
In challenging cases, immunohistochemical evalua-tion of IgE bearing cells may distinguish betweencommon clinical differentials, such as insect bitehypersensitivity, and pemphigus.12 Laboratorytests may provide confusing results when evaluatingurticaria and angioedema. This is exemplified by acase of a Paso Fino stallion that was cultured der-matophyte positive (Trichophyton mentagrophytes)and histologically diagnosed with urticaria; how-
ever, the horse had negative findings on specialstains.4 Successful treatment was achieved withantifungal therapy for the dermatophytosis and IVdexamethasone for the urticaria. It was suspectedthat the ringworm infection resulted in an “id” reac-tion, an immunologic response of the skin to system-ically absorbed fungal antigens.
In this author’s opinion, allergy testing for urti-caria is warranted if the history coincides with aclinical case that is recurrent or persists for �8 wk.Allergy testing should not be used to diagnose atopy.Rather, it is a means of confirming your clinicalsuspicions and formulating a treatment plan involv-ing both avoidance and allergen specific immuno-therapy. Positive reactions indicate that antigenspecific IgE is present in the patient; it does notindicate that the antigen in question caused thedisease. Therefore, careful historical evaluationand correlation with reactions is important for hy-posensitization success. Serologic testing is avail-able through Greer Laboratories,a SpectrumLaboratories,b Heska Corporation,c and Bio-MedicalServices.d Serologic testing can be quite expensive;however, recent series of studies from the Ohio StateUniversity concurred with previous findings thatintradermal allergy testing is more reliable thanserologic testing.13–16
Intradermal allergy testing (IDT) does require se-dation, shaving, withdrawal from essential fatty ac-ids, antihistamines, and topical steroids for 7–14days, and withdrawal from oral/injectable glucocor-ticoids for 7–28 days. This author has performedIDT on cases that have received injectable diphen-hydramine and glucocorticoids shortly before allergytesting, and significant results were still obtained(Fig. 3). Therefore, withdrawal from anti-inflam-matory medications does not seem as crucial inhorses as it does in dogs and cats. A detailed re-view of the testing method has recently been re-viewed.13–16 The tests are tailored to specificgeographic regions using small animal test concen-trations/allergens with additional insects and out-door allergens to account for the horse’s exposure.This author tends to read test reactions at 30 minand 4 h after inoculation and omits the 24-m and48-h reactions because of the questionable value ofthe delayed responses for immunotherapy and fea-sibility in practice. Evaluating size and especiallyturgidity of the wheals is very important, and itrequires the expertise of an allergist to minimizefalse positive/negative reactions.17
Dietary trials are the only way to diagnose foodhypersensitivity or intolerance. The author’s cur-rent approach consists of a 4–6-wk trial with novelfood sources such as timothy, rolled oats, alfalfa, orbarley, if not routinely fed, because these items areeasily obtainable single source foods. Discontinua-tion of unnecessary supplements, vitamins, andother drugs is mandatory throughout the trial pe-riod. After the urticaria has resolved, confirmationof food allergy is achieved by challenging with one
Fig. 3. Intradermal allergy test in horse from Fig. 1 with posi-tive reactions to primarily pollens (trees, grasses and weeds).
AAEP PROCEEDINGS � Vol. 52 � 2006 487
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
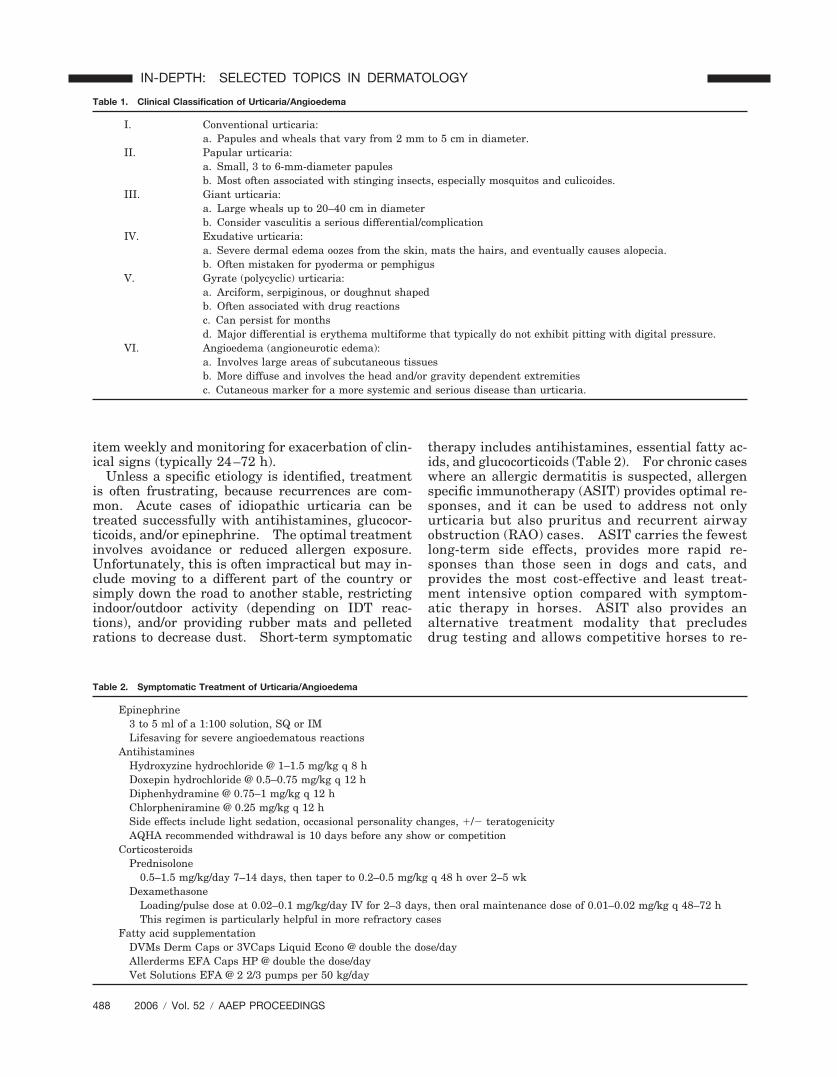
item weekly and monitoring for exacerbation of clin-ical signs (typically 24–72 h).
Unless a specific etiology is identified, treatmentis often frustrating, because recurrences are com-mon. Acute cases of idiopathic urticaria can betreated successfully with antihistamines, glucocor-ticoids, and/or epinephrine. The optimal treatmentinvolves avoidance or reduced allergen exposure.Unfortunately, this is often impractical but may in-clude moving to a different part of the country orsimply down the road to another stable, restrictingindoor/outdoor activity (depending on IDT reac-tions), and/or providing rubber mats and pelletedrations to decrease dust. Short-term symptomatic
therapy includes antihistamines, essential fatty ac-ids, and glucocorticoids (Table 2). For chronic caseswhere an allergic dermatitis is suspected, allergenspecific immunotherapy (ASIT) provides optimal re-sponses, and it can be used to address not onlyurticaria but also pruritus and recurrent airwayobstruction (RAO) cases. ASIT carries the fewestlong-term side effects, provides more rapid re-sponses than those seen in dogs and cats, andprovides the most cost-effective and least treat-ment intensive option compared with symptom-atic therapy in horses. ASIT also provides analternative treatment modality that precludesdrug testing and allows competitive horses to re-
Table 1. Clinical Classification of Urticaria/Angioedema
I. Conventional urticaria:a. Papules and wheals that vary from 2 mm to 5 cm in diameter.
II. Papular urticaria:a. Small, 3 to 6-mm-diameter papulesb. Most often associated with stinging insects, especially mosquitos and culicoides.
III. Giant urticaria:a. Large wheals up to 20–40 cm in diameterb. Consider vasculitis a serious differential/complication
IV. Exudative urticaria:a. Severe dermal edema oozes from the skin, mats the hairs, and eventually causes alopecia.b. Often mistaken for pyoderma or pemphigus
V. Gyrate (polycyclic) urticaria:a. Arciform, serpiginous, or doughnut shapedb. Often associated with drug reactionsc. Can persist for monthsd. Major differential is erythema multiforme that typically do not exhibit pitting with digital pressure.
VI. Angioedema (angioneurotic edema):a. Involves large areas of subcutaneous tissuesb. More diffuse and involves the head and/or gravity dependent extremitiesc. Cutaneous marker for a more systemic and serious disease than urticaria.
Table 2. Symptomatic Treatment of Urticaria/Angioedema
Epinephrine3 to 5 ml of a 1:100 solution, SQ or IMLifesaving for severe angioedematous reactions
AntihistaminesHydroxyzine hydrochloride @ 1–1.5 mg/kg q 8 hDoxepin hydrochloride @ 0.5–0.75 mg/kg q 12 hDiphenhydramine @ 0.75–1 mg/kg q 12 hChlorpheniramine @ 0.25 mg/kg q 12 hSide effects include light sedation, occasional personality changes, /� teratogenicityAQHA recommended withdrawal is 10 days before any show or competition
CorticosteroidsPrednisolone
0.5–1.5 mg/kg/day 7–14 days, then taper to 0.2–0.5 mg/kg q 48 h over 2–5 wkDexamethasone
Loading/pulse dose at 0.02–0.1 mg/kg/day IV for 2–3 days, then oral maintenance dose of 0.01–0.02 mg/kg q 48–72 hThis regimen is particularly helpful in more refractory cases
Fatty acid supplementationDVMs Derm Caps or 3VCaps Liquid Econo @ double the dose/dayAllerderms EFA Caps HP @ double the dose/dayVet Solutions EFA @ 2 2/3 pumps per 50 kg/day
488 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

turn to performance standards without jeopardiz-ing the owner’s ethics.
6. Prognosis
The prognosis for urticarial reactions is good, be-cause general health is not usually affected. Theprognosis for angioedema varies with the severityand location. Angioedematous reactions involvingthe nasal passages, pharynx, and larynx may befatal if not immediately addressed.
References and Footnotes1. Pascoe RRR, Knottenbelt DC. Manual of equine dermatology.
Immune-mediated/allergic diseases. London: Harcourt Braceand Company, 1999;156–160.
2. Scott, DW, Miller, WH. Skin immune system and allergicskin disease. In: Equine dermatology. London: W.B.Saunders, 2003;422–427.
3. Abbas AK, Lichtman AH, Pober JS. Cellular and molecularimmunology. Philadelphia: W.B. Saunders, 1991;294.
4. Fadok VA. Overview of equine papular and nodular derma-toses. Vet Clin North Am [Equine Pract] 1995;11:61–74.
5. Fadok VA. Update on equine allergies. J Vet Allergy ClinImmunol 1997;5:68–76.
6. Scott DW, Miller WH. Idiosyncratic cutaneous adverse drugreactions in the horse: literature review and report of 19cases (1990–1996). Equine Pract 1997;19:12–18.
7. Scott DW, Miller WH. Erythema multiforme in the horse:literature review and report of 9 cases (1988–1996). EquinePract 1998;20:6–9.
8. Bathe AP. An unusual manifestation of nettle rash in threehorses. Vet Rec 1994;134:11–12.
9. Matthews NS, Light GS, Sanders EA, et al. Urticarial re-sponse during anesthesia in a horse. Equine Vet J 1993;25:555–556.
10. Paul JW. Equine larval cyathostomosis. Compend ContEduc Pract Vet 1998;20:509–515.
11. Logas D, Kunkle GA, Calderwood-Mays MB, et al. Cholinergicpruritus in a horse. J Am Vet Med Assoc 1992;201:90–91.
12. Rufenacht S, Marti E, von Tscharner C, et al. Immuno-globulin E-bearing cells and mast cells in skin biopsies ofhorses with urticaria. Vet Dermatol 2005;16:94–101.
13. Delger JM. Intradermal testing and immunotherapy inhorses. Vet Med 1997;92:635–639.
14. Lorch G, Hillier A, Kwochka KW, et al. Comparison of im-mediate intradermal test reactivity with serum IgE quanti-tation by use of a radioallergosorbent test and two ELISA inhorses with and without atopy. J Am Vet Med Assoc 2001;218:1314–1322.
15. Lorch G, Hillier A, Kwochka KW, et al. Results of intrader-mal tests in horses without atopy and horses with chronicobstructive pulmonary disease. Am J Vet Res 2001;62:389–397.
16. Lorch G, Hillier A, Kwochka KW, et al. Results of intrader-mal tests in horses without atopy and horses with atopicdermatitis or recurrent urticaria. Am J Vet Res 2001;62:1051–1059.
17. Yu AA. Equine urticaria: a diagnostic dilemma. Com-pend Cont Educ Pract Vet 2000;22:277–280.
aGreer Laboratories, Lenoir, NC 28645.bSpectrum Laboratories, Mesa, AZ 85204.cHeska Corporation, Fort Collins, CO 80525.dBio-Medical Services, Austin, TX 78759.
AAEP PROCEEDINGS � Vol. 52 � 2006 489
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
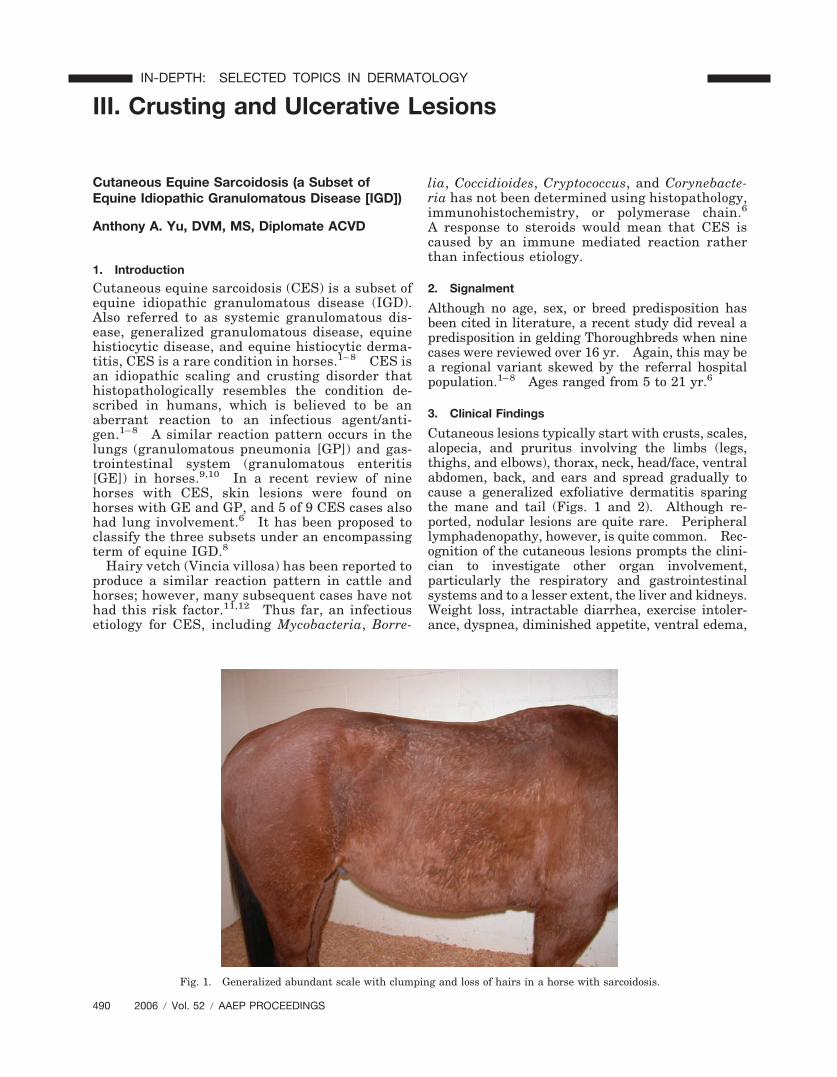
III. Crusting and Ulcerative Lesions
Cutaneous Equine Sarcoidosis (a Subset ofEquine Idiopathic Granulomatous Disease [IGD])
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
Cutaneous equine sarcoidosis (CES) is a subset ofequine idiopathic granulomatous disease (IGD).Also referred to as systemic granulomatous dis-ease, generalized granulomatous disease, equinehistiocytic disease, and equine histiocytic derma-titis, CES is a rare condition in horses.1– 8 CES isan idiopathic scaling and crusting disorder thathistopathologically resembles the condition de-scribed in humans, which is believed to be anaberrant reaction to an infectious agent/anti-gen.1– 8 A similar reaction pattern occurs in thelungs (granulomatous pneumonia [GP]) and gas-trointestinal system (granulomatous enteritis[GE]) in horses.9,10 In a recent review of ninehorses with CES, skin lesions were found onhorses with GE and GP, and 5 of 9 CES cases alsohad lung involvement.6 It has been proposed toclassify the three subsets under an encompassingterm of equine IGD.8
Hairy vetch (Vincia villosa) has been reported toproduce a similar reaction pattern in cattle andhorses; however, many subsequent cases have nothad this risk factor.11,12 Thus far, an infectiousetiology for CES, including Mycobacteria, Borre-
lia, Coccidioides, Cryptococcus, and Corynebacte-ria has not been determined using histopathology,immunohistochemistry, or polymerase chain.6
A response to steroids would mean that CES iscaused by an immune mediated reaction ratherthan infectious etiology.
2. Signalment
Although no age, sex, or breed predisposition hasbeen cited in literature, a recent study did reveal apredisposition in gelding Thoroughbreds when ninecases were reviewed over 16 yr. Again, this may bea regional variant skewed by the referral hospitalpopulation.1–8 Ages ranged from 5 to 21 yr.6
3. Clinical Findings
Cutaneous lesions typically start with crusts, scales,alopecia, and pruritus involving the limbs (legs,thighs, and elbows), thorax, neck, head/face, ventralabdomen, back, and ears and spread gradually tocause a generalized exfoliative dermatitis sparingthe mane and tail (Figs. 1 and 2). Although re-ported, nodular lesions are quite rare. Peripherallymphadenopathy, however, is quite common. Rec-ognition of the cutaneous lesions prompts the clini-cian to investigate other organ involvement,particularly the respiratory and gastrointestinalsystems and to a lesser extent, the liver and kidneys.Weight loss, intractable diarrhea, exercise intoler-ance, dyspnea, diminished appetite, ventral edema,
Fig. 1. Generalized abundant scale with clumping and loss of hairs in a horse with sarcoidosis.
490 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

and low-grade fever indicate multiple organinvolvement.9,10
4. Differential Diagnoses
Differentials based on clinical findings include mul-tisystemic eosinophilic epitheliotropic dermatitisand stomatitis, eosinophilic gastroenterocolitis anddermatitis, lymphocytic plasmacytic enterocolitis,dermatophilosis, recurrent airway obstruction, der-matophytosis, pemphigus foliaceus, contact derma-titis, drug eruptions, and toxicoses (arsenic oriodine), depending on the organs involved.
5. Diagnosis
Based on history, physical examination, lymph nodeaspirates, and dermatopathology, a diagnosis ofCES can be made. Typically, the complete bloodcount (CBC) and chemistry profile reveal a neutro-philia, hyperfibrinogenemia, and hyperproteinemiaconsistent with an inflammatory condition.13
Peripheral circulating eosinophilia is rarely seen.Bacterial and fungal cultures have classically beennegative. Dermatohistopathologic findings includeperifollicular mid-dermal sarcoid type granulomaswith many histiocytic cells, superficial dermal infil-trate of multinucleated histiocytic giant cells, and asmaller number of superficial dermal neutrophils,lymphocytes, and plasma cells.1–7
6. Treatment
Currently, as in human medicine, there is no universaleffective treatment for IGD/sarcoidosis (informationavailable online at http://www.nhlbi.nih.gov/health/public/lung/other/sarcoidosis). Immunosuppres-sive doses of steroids have been the mainstay withinconsistent results. Prednisolone (2.2–4.4 mg/kgdaily) or dexamethasone (0.1–0.2 mg/kg daily) for7–14 days with tapering doses when or if an improve-ment is noted tends to be the first line of treatment.
If malabsorption/GE is present, it is recommendedthat medications be given parenterally where possible.
Also included in my initial protocol are the use ofessential fatty acids, shampoo therapy, and pentoxi-fylline. Adding essential fatty acidsa at the recom-mended daily dose may help reduce the scaling byreplenishing the corneal lipid envelope and provid-ing membrane stabilizing effects. Shampoo ther-apy (Universal Medicated Shampoob or Seboluxc)enhances keratolysis and keratoplasty and providestopical antimicrobial protection. Pentoxifylline (10mg/kg, q 8–12 h) has rheologic activity that mayimprove drug delivery into granulomatous tissueand minimize the risk of laminitis while administer-ing steroids. Additionally, pentoxifylline has anti-inflammatory properties, namely anti-tumornecrosis factor-�, which potentially allows for a syn-ergistic tapering of steroids. Some cases of CEShave spontaneously resolved, and therefore, taper-ing of medications to the lowest dose possible or intotal is always advised.2,7
If minimal response is noted to the above protocol,adding azathioprine (3 mg/kg daily) for 30–60 daysand then tapering to every other day alternatingwith steroids may provide some benefit. Systemicantibiotics should always be considered in severegeneralized cases (trimethoprim sulfa, 15–30 mg/kg,q 12 h for 30 days) where a primary or secondaryinfection may be suspected.
7. Prognosis
The prognosis for cases limited to cutaneous involve-ment tends to be better (�12 yr) than those withconcurrent internal organ disease, especially if signsof weight loss/wasting exist.6 As spontaneous re-mission has been reported, treatment should be at-tempted in all cases.6,7 Most horses with internalinvolvement, however, tend to decline over severalmonths and are eventually humanely euthanized.
References and Footnotes1. Stannard T. Immunologic diseases. Vet Dermatol 2000;11:
163–178.2. Scott DW, Miller WH. Miscellaneous skin diseases. In:
Scott DW, Miller WH, eds. Equine dermatology. St. Louis:W.B. Saunders, 2003;647–697.
3. Heath SE, Bell RJ, Clark EG, et al. Idiopathic granuloma-tous disease involving the skin in a horse. J Am Vet MedAssoc 1990;197:1033–1036.
4. Sellers RS, Toribio RE, Blomme EA. Idiopathic systemicgranulomatous disease and macrophage expression of PTHrPin a miniature pony. J Comp Pathol 2001;125:214–218.
5. Axon JE, Robinson P, Lucas J. Generalised granulomatousdisease in a horse. Aust Vet J 2004;82:48–51.
6. Spiegel IB, White SD, Foley JE, et al. A retrospective studyof cutaneous equine sarcoidosis and its potential infectiousaetiological agents. Vet Dermatol 2006;17:51–62.
7. Loewenstein C, Bettenay SV, Mueller RS. A retrospectivestudy of equine sarcoidosis. Vet Dermatol 2004;15:67.
8. Petersen AD, Schott HC. Cutaneous markers of disordersaffecting adult horses. Clinical techniques in equine prac-tice. 2005;4:324–338.
9. Schumacher J, Edwards JF, Cohen ND. Chronic idiopathicinflammatory bowel diseases of the horse. J Vet Int Med2000;14(3):258–265.
Fig. 2. Close-up of horse in Fig 1. with sarcoidosis. Note thesheets of scale emanating from the skin and caught in the hairs,characteristic of an advanced case of sarcoidosis.
AAEP PROCEEDINGS � Vol. 52 � 2006 491
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

10. Pusterla N, Pesavento PA, Smith P, et al. Idiopathic gran-ulomatous pneumonia in seven horses. Vet Rec 2003;153:653–655.
11. Anderson CA, Divers TJ. Systemic granulomatous inflam-mation in a horse grazing hairy vetch. J Am Vet Med Assoc1983;183:569–570.
12. Woods LW, Johnson B, Hietala SK, et al. Systemic granu-lomatous disease in a horse grazing pasture containing vetch(Vicia sp.). J Vet Diag Invest 1992;4(3):356–360.
13. Lindberg R, Persson SG, Jones B, et al. Clinical and patho-physiological features of granulomatous enteritis and eosin-ophilic granulomatosis in the horse. Zentralbl Vet Med A1985;32:526–539.
aDermCaps Liquid Econo, DVM, Miami, FL 33169.bUniversal Medicated Shampoo, Vet Solutions, Fort Worth, TX
76137.cSebolux, Virbac AH, Inc., Fort Worth, TX 76137.
Pemphigus
Anthony A. Yu, DVM, MS, Diplomate ACVD
1. Introduction
Pemphigus foliaceus, first described in this speciesin 1981, is the most common autoimmune skindisease in the horse.1,2 Several forms of pemphi-gus exist including pemphigus foliaceus, pemphi-gus vulgaris (very rare), drug-induced pemphigus,and paraneoplastic pemphigus. The most com-monly reported form is that of pemphigus folia-ceus. Pemphigus foliaceus in humans is a resultof the production of autoantibodies directedagainst cell adhesion proteins, particularly thedesmosomal antigens (desmoglein 1 [DSG1] inpemphigus foliaceus and DSG3 in pemphigus vul-garis) of the stratified squamous epithelium. Theantibody antigen complex moves through multiple
pathways and then incites acantholysis.3 A sim-ilar pathway is hypothesized for the dog and horsebased on the detection of DSG1 in immunoblotting/immunoprecipitation studies.4,5 Several triggerfactors have been proposed including drugs, sys-temic disease, neoplasia, stressful situations, andlastly, allergies (foods, inhalants, insects) basedon the presence of case clusters and seasonality(Figs. 1–5).1,6
2. Signalment
Pemphigus presents in both adult horses (�5 yr ofage) and foals (�yr of age).7,8 This age dichotomymay not be obvious in all populations.6 Youngerhorses often carry a better prognosis and potentialfor spontaneous remission without relapses. Ofthe specific horse breeds, Appaloosas, QuarterHorses, and Thoroughbreds seem to be at greaterrisk, although this may have some geographic variabil-ity.1,6,7 At this time, there does not seem to be anyevidence of sex predilection. Pemphigus has beenknown to have a waxing and waning course, and theremay also be a seasonal incidence of the condition, poten-tially caused by allergen load (pollens, insects) and/or theincreased use of preventative medications (dewormers,vaccines, supplements, etc.).6,9
3. Clinical Signs
Classic clinical findings of vesicles and pustulesare rarely noted in the horse, because lesions ofpemphigus progress rapidly to crusts, exfoliation,erosions, alopecia, and scaling (Fig. 6). In fact,
Fig. 1. Equine pemphigus foliaceus with generalized crusts, exfoliation, erosions, alopecia, and scaling in a horse that was pruriticand responded poorly to treatment.
492 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
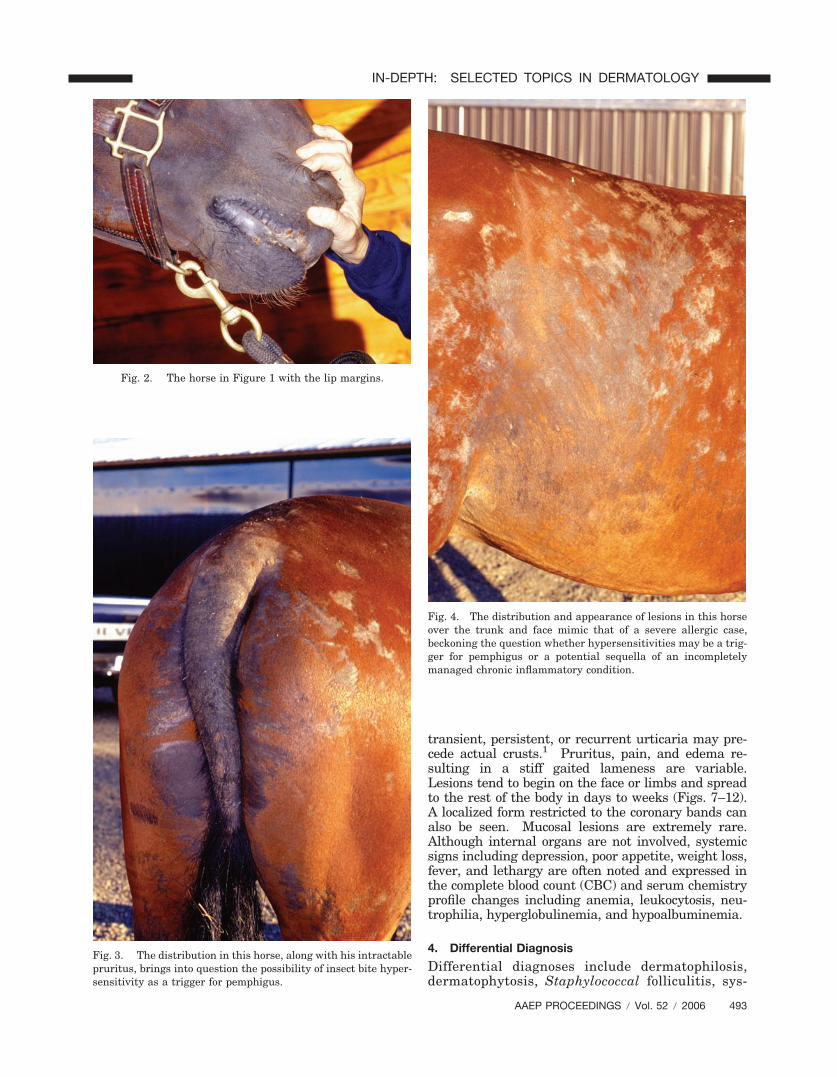
transient, persistent, or recurrent urticaria may pre-cede actual crusts.1 Pruritus, pain, and edema re-sulting in a stiff gaited lameness are variable.Lesions tend to begin on the face or limbs and spreadto the rest of the body in days to weeks (Figs. 7–12).A localized form restricted to the coronary bands canalso be seen. Mucosal lesions are extremely rare.Although internal organs are not involved, systemicsigns including depression, poor appetite, weight loss,fever, and lethargy are often noted and expressed inthe complete blood count (CBC) and serum chemistryprofile changes including anemia, leukocytosis, neu-trophilia, hyperglobulinemia, and hypoalbuminemia.
4. Differential Diagnosis
Differential diagnoses include dermatophilosis,dermatophytosis, Staphylococcal folliculitis, sys-
Fig. 2. The horse in Figure 1 with the lip margins.
Fig. 3. The distribution in this horse, along with his intractablepruritus, brings into question the possibility of insect bite hyper-sensitivity as a trigger for pemphigus.
Fig. 4. The distribution and appearance of lesions in this horseover the trunk and face mimic that of a severe allergic case,beckoning the question whether hypersensitivities may be a trig-ger for pemphigus or a potential sequella of an incompletelymanaged chronic inflammatory condition.
AAEP PROCEEDINGS � Vol. 52 � 2006 493
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
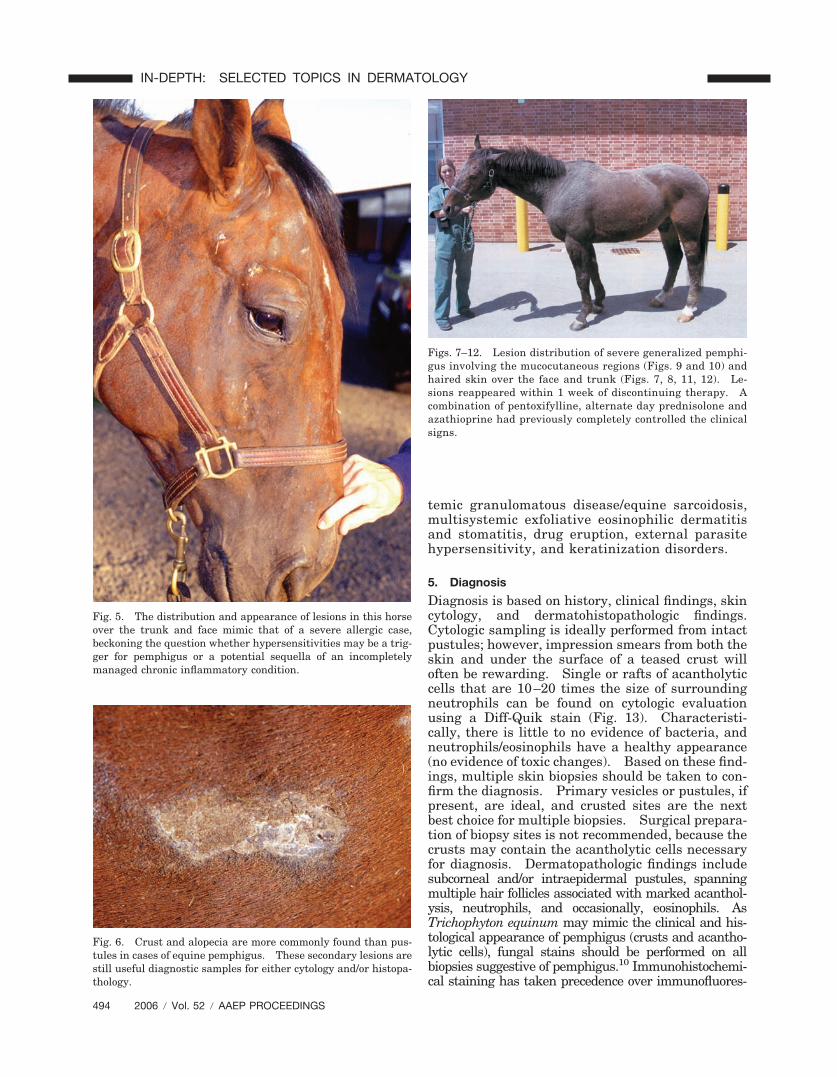
temic granulomatous disease/equine sarcoidosis,multisystemic exfoliative eosinophilic dermatitisand stomatitis, drug eruption, external parasitehypersensitivity, and keratinization disorders.
5. Diagnosis
Diagnosis is based on history, clinical findings, skincytology, and dermatohistopathologic findings.Cytologic sampling is ideally performed from intactpustules; however, impression smears from both theskin and under the surface of a teased crust willoften be rewarding. Single or rafts of acantholyticcells that are 10–20 times the size of surroundingneutrophils can be found on cytologic evaluationusing a Diff-Quik stain (Fig. 13). Characteristi-cally, there is little to no evidence of bacteria, andneutrophils/eosinophils have a healthy appearance(no evidence of toxic changes). Based on these find-ings, multiple skin biopsies should be taken to con-firm the diagnosis. Primary vesicles or pustules, ifpresent, are ideal, and crusted sites are the nextbest choice for multiple biopsies. Surgical prepara-tion of biopsy sites is not recommended, because thecrusts may contain the acantholytic cells necessaryfor diagnosis. Dermatopathologic findings includesubcorneal and/or intraepidermal pustules, spanningmultiple hair follicles associated with marked acanthol-ysis, neutrophils, and occasionally, eosinophils. AsTrichophyton equinum may mimic the clinical and his-tological appearance of pemphigus (crusts and acantho-lytic cells), fungal stains should be performed on allbiopsies suggestive of pemphigus.10 Immunohistochemi-cal staining has taken precedence over immunofluores-
Fig. 5. The distribution and appearance of lesions in this horseover the trunk and face mimic that of a severe allergic case,beckoning the question whether hypersensitivities may be a trig-ger for pemphigus or a potential sequella of an incompletelymanaged chronic inflammatory condition.
Fig. 6. Crust and alopecia are more commonly found than pus-tules in cases of equine pemphigus. These secondary lesions arestill useful diagnostic samples for either cytology and/or histopa-thology.
Figs. 7–12. Lesion distribution of severe generalized pemphi-gus involving the mucocutaneous regions (Figs. 9 and 10) andhaired skin over the face and trunk (Figs. 7, 8, 11, 12). Le-sions reappeared within 1 week of discontinuing therapy. Acombination of pentoxifylline, alternate day prednisolone andazathioprine had previously completely controlled the clinicalsigns.
494 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
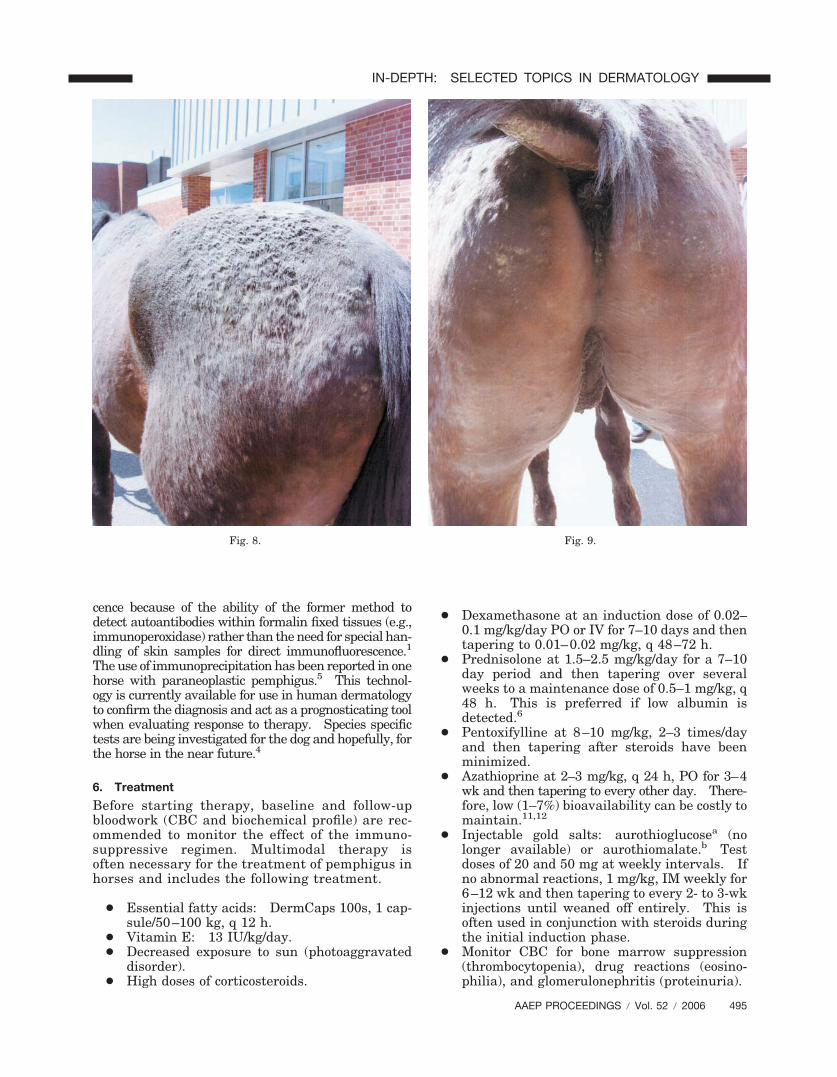
cence because of the ability of the former method todetect autoantibodies within formalin fixed tissues (e.g.,immunoperoxidase) rather than the need for special han-dling of skin samples for direct immunofluorescence.1
The use of immunoprecipitation has been reported in onehorse with paraneoplastic pemphigus.5 This technol-ogy is currently available for use in human dermatologyto confirm the diagnosis and act as a prognosticating toolwhen evaluating response to therapy. Species specifictests are being investigated for the dog and hopefully, forthe horse in the near future.4
6. Treatment
Before starting therapy, baseline and follow-upbloodwork (CBC and biochemical profile) are rec-ommended to monitor the effect of the immuno-suppressive regimen. Multimodal therapy isoften necessary for the treatment of pemphigus inhorses and includes the following treatment.
● Essential fatty acids: DermCaps 100s, 1 cap-sule/50–100 kg, q 12 h.
● Vitamin E: 13 IU/kg/day.● Decreased exposure to sun (photoaggravated
disorder).● High doses of corticosteroids.
● Dexamethasone at an induction dose of 0.02–0.1 mg/kg/day PO or IV for 7–10 days and thentapering to 0.01–0.02 mg/kg, q 48–72 h.
● Prednisolone at 1.5–2.5 mg/kg/day for a 7–10day period and then tapering over severalweeks to a maintenance dose of 0.5–1 mg/kg, q48 h. This is preferred if low albumin isdetected.6
● Pentoxifylline at 8–10 mg/kg, 2–3 times/dayand then tapering after steroids have beenminimized.
● Azathioprine at 2–3 mg/kg, q 24 h, PO for 3–4wk and then tapering to every other day. There-fore, low (1–7%) bioavailability can be costly tomaintain.11,12
● Injectable gold salts: aurothioglucosea (nolonger available) or aurothiomalate.b Testdoses of 20 and 50 mg at weekly intervals. Ifno abnormal reactions, 1 mg/kg, IM weekly for6–12 wk and then tapering to every 2- to 3-wkinjections until weaned off entirely. This isoften used in conjunction with steroids duringthe initial induction phase.
● Monitor CBC for bone marrow suppression(thrombocytopenia), drug reactions (eosino-philia), and glomerulonephritis (proteinuria).
Fig. 8. Fig. 9.
AAEP PROCEEDINGS � Vol. 52 � 2006 495
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
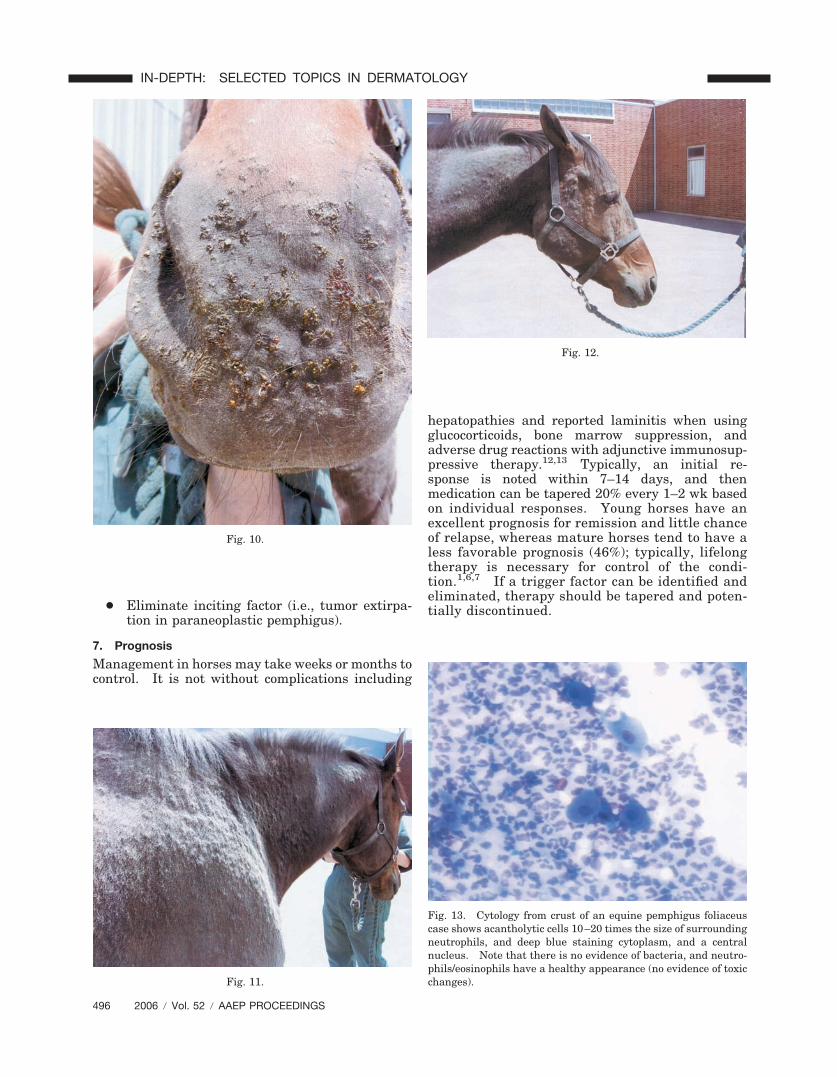
● Eliminate inciting factor (i.e., tumor extirpa-tion in paraneoplastic pemphigus).
7. Prognosis
Management in horses may take weeks or months tocontrol. It is not without complications including
hepatopathies and reported laminitis when usingglucocorticoids, bone marrow suppression, andadverse drug reactions with adjunctive immunosup-pressive therapy.12,13 Typically, an initial re-sponse is noted within 7–14 days, and thenmedication can be tapered 20% every 1–2 wk basedon individual responses. Young horses have anexcellent prognosis for remission and little chanceof relapse, whereas mature horses tend to have aless favorable prognosis (46%); typically, lifelongtherapy is necessary for control of the condi-tion.1,6,7 If a trigger factor can be identified andeliminated, therapy should be tapered and poten-tially discontinued.
Fig. 10.
Fig. 11.
Fig. 12.
Fig. 13. Cytology from crust of an equine pemphigus foliaceuscase shows acantholytic cells 10–20 times the size of surroundingneutrophils, and deep blue staining cytoplasm, and a centralnucleus. Note that there is no evidence of bacteria, and neutro-phils/eosinophils have a healthy appearance (no evidence of toxicchanges).
496 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
References and Footnotes1. Scott DW, Miller WH. Pemphigus foliaceus. In: Equine
dermatology. Philadelphia: W.B. Saunders, 2003;480–492.2. Johnson ME, Scott DW, Manning TO. A case of pemphigus
foliaceus in the horse. Equine Pract 1981;3(2):40–45.3. Jordon RE. Pemphigus. In: Fitzpatrick TB, Eisen AZ,
Wolff K, eds. Dermatology in general medicine, 2nd ed. NewYork: McGraw-Hill, 1979;310–317.
4. Iwasaki T, Shimizu M, Obata H, et al. Detection of caninepemphigus foliaceus autoantigen by immunoblotting. VetImmunol Immunopathol 1997;59:1–10.
5. Williams MA, Dowling PM, Angarano DW, et al. Paraneo-plastic bullous stomatitis in a horse. J Am Vet Med Assoc1995;207:331–334.
6. Vandenabeele SIJ, White SD, Affolter VK, et al. Pemphigusfoliaceus in the horse: retrospective study of 20 cases. VetDermatol 2004;15:381–388.
7. Zabel S, Mueller RS, Fieseler KV, et al. Review of 15 casesof pemphigus foliaceus in horses and a survey of the litera-ture. Vet Rec 2005;157:505–509.
8. Stannard AA. Stannard’s Illustrated Equine DermatologyNotes. Immunologic Diseases. 2000;11(3):163–178.
9. White SD, Carlotti DN, Pin D, et al. Putative drug-relatedpemphigus foliaceus in four dogs. Vet Dermatol 2002;13:195–202.
10. Scott DW. Marked acantholysis associated with dermato-phytosis due to Trichophyton equinum in two horses. VetDermatol 1994;5:105–110.
11. White SD, Maxwell LK, Szabo NJ. Pharmacokinetics of aza-thioprine following single-dose intravenous and oral admin-istration and effects of azathioprine following chronic oraladministration in horses. Am J Vet Res 2005;66:1578–1583.
12. White SD, Rosychuk RAW, Outerbridge CA, et al. Thiopu-rine methyltransferase in red blood cells of dogs, cats, andhorses. J Vet Int Med 2000;14:499–502.
13. Eyre P, Elmes PJ, Strickland S. Corticosteroid-potentiatedvascular responses of the equine digit: a possible pharma-cologic basis for laminitis. Am J Vet Res 1979;40:135–138.
aSolgonal, Schering, Kenilworth, NJ 07033.bMyochrysine, Merck, Whitehouse Station, NJ 08889.
Hereditary Diseases
Stephen D. White, DVM, Diplomate ACVD
1. Introduction
Epidermolysis bullosa (EB) includes a number ofdiseases typified in humans by the common findingof blister formation after minor trauma. Mostforms are congenital and apparent soon after birth.In animals and humans, subsets of EB are classifiedby the histologic location of the blister or cleft.These subtypes (and respective cleft locations) aretermed EB simplex (basal cell layer of the epider-mis), junctional EB (intralamina lucida or basal celllayer), and dystrophic EB (sublamina densa).
Junctional EB has been reported in Belgian foalsof both sexes as well as other breeds and a don-key.1–4 Lesions are usually noted within 3 days ofbirth and include multiple asymmetrical irregularskin erosions and ulcers that are often encrusted.Lesions may be especially prominent around thecoronary bands (causing the hoof to crack andslough) and on the oral, anal, and genital mucosa.Histology and ultrastructural findings point to acleft in the intralamina lucida of the basement mem-brane zone. This is presumably caused by a defect
in the anchoring filaments that connect the base-ment membrane to filaments in the superficial der-mis.2 A laminin-5 defect has been shown inBelgians and in two French draft breeds (Trait Bre-ton and Trait Comtois); the mutation is a cytosineinsertion in exon 10 of the LAMC2 gene.5–7 Be-cause of this knowledge, the Veterinary GeneticsLaboratory at the University of California at Davisoffers a diagnostic test to determine carrier status(available online at www.vgl.ucdavis.edu/service/horse/index.html) in Belgian Draft horses and re-lated breeds.
Clinical presentation and the age of the foal arehighly suggestive of the diagnosis. Histology andideally, electron microscopy are required to con-firm the diagnosis. There is no known treatment,and affected horses, as well as the sires and damsof affected horses, should not be bred; the mode ofinheritance is autosomal recessive.
This disease differs from epitheliogenesis imper-fecta (see below). At first, EB does not presentlarge areas of the skin are devoid of epidermis, butrather, the skin is later lost because of the fibrildefect.
Epitheliogenesis imperfecta (aplasia cutis) is aninherited, congenital discontinuity of squamous ep-ithelium. It is thought to be an autosomal reces-sive trait, and it has been reported in several breeds.Lesions are most common on the limbs, head, andtongue. Hooves may slough in severe cases.Clinical presentation is usually diagnostic.8 Inmoderately to severely affected animals, the diseaseis fatal within a few days, because the foal usuallydies of septicemia or other developmental abnormal-ities. Mildly affected areas may heal by scar for-mation. More recent reports would suggest thatsome of these horses with epitheliogenisis imper-fecta (Saddlebreds) may, in fact, have a conditionsimilar to the junctional EB common in Belgianfoals.9–11
Hereditary equine regional dermal asthenia(HERDA; “hyperelastosis cutis”) is a disease thatoccurs early in life in horses. Most affected horsesare Quarter Horses, but registered Paint Horses andAppaloosas with Quarter Horse lineage have beenafflicted with this disease.12,13 Many of the Quar-ter Horses are from high-quality cutting lines.The disease (or something very similar) has alsobeen reported in a cross-bred Arabian mare, a Thor-oughbred gelding, a Hanoverian foal, and a Haf-flinger horse.14–17
The working hypothesis is that these horses havea defect in their collagen fibers or in the way thosefibers are structurally organized in the mid to deepdermis. Typically, these areas are over the backand sides of the neck (Fig. 1). The skin in theseareas may seem to be easily torn or stretched, and itoften develops seromas and hematomas (“blisters”filled with either serum or blood) (Fig. 2). Healingper se is usually adequate but often leaves ratherunsightly scars. Diagnosis is often based on the
AAEP PROCEEDINGS � Vol. 52 � 2006 497
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY
clinical signs alone; histologic findings are some-times subtle, but “clumped” or poorly organized col-lagen fibers below the level of the hair follicles maybe seen. A zone of mid- to deep-dermal separationhas been reported in two horses, and it has beenpresent in some of the biopsy samples that the authorhas seen.13,18 “Poorly oriented” collagen fibers aresometimes seen on electron microscopy. There is noblood test to confirm the disease.
This condition is almost certainly present at birth;however, it is often not noticed until �2 yr of agewhen horses start being trained with tack, and thefriction/trauma of this induces the typical lesions.
As with many genetic diseases, there is no effectivetreatment or cure, but some of these horses havebeen maintained as “pasture pets.”
This disease follows an autosomal recessive modeof inheritance; therefore, for the foal to be affected,both the sire and the dam must carry the gene, andif they were bred again, there would be �25%chance that the next foal would also be affected.19
At the present time, there is no test available toverify carriers. Obviously, clinically affectedhorses with the disease should be removed frombreeding programs.
Progressive chronic lymphedema is the tentativeterm for a condition seen in Shires, Clydesdales, andBelgians. It is characterized by progressive swell-ing, hyperkeratosis (thickening), and fibrosis (hard-ening) of the skin on the lower legs. This chronicprogressive disease starts at an early age,progresses throughout the life of the horse, and of-ten ends in disfigurement and disability of the limbs.Inevitably, this condition leads to the horse’s pre-mature death. In the Belgian draft horse, it hasreduced the average life expectancy of a stallionfrom 20 to 6 yr.
The pathologic changes and clinical signs closelyresemble a condition known in humans as chroniclymphedema or elephantiasis nostras verrucosa.The lower leg swelling is caused by abnormal func-tioning of the lymphatic system in the skin, whichresults in chronic lymphedema (swelling), fibrosis, acompromised immune system, and subsequent sec-ondary infections of the skin. Based on prelimi-nary research, it seems that a similar pathogenic
Fig. 1. Stallion with hereditary equine regional dermal asthenia (HERDA).
Fig. 2. Dorsum of filly with HERDA.
498 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

mechanism is involved in the disease that affectsthese specific draft horse breeds.
The clinical signs of this disease are highly vari-able. The earliest lesions are characterized by skinthickening and crusting; both are often visible onlyafter clipping the long feathering. Secondary infec-tions develop very easily in these horse’s legs andusually consist of either chorioptic mange or bacte-rial infections. Both dark and white skin on thelower legs are equally affected. These lesions areconsistent with pastern dermatitis, which is cer-tainly seen in other breeds. In Shires, Clydesdales,and Belgians, however, these lesions do not respondwell to therapy.
As the disease progresses, 1–2 thick skin foldsand sometimes multiple small, well-demarcatedulcerations develop predominantly in the rear ofthe pastern region. The ulcerations are coveredwith adherent crusts. Manual removal of thecrusts and even movement during exercise resultsin bleeding. These small sores may seem to re-spond initially to various topical medications, butthey often reverse course, only to progress in se-verity and multiply in number. Small lesionstend to coalesce into larger and more intractable(resistant to cure) areas of skin ulceration. Overtime, the lesions extend up the leg, often affectingthe skin as high as the knees or hocks. Theselesions are, at the very least, irritating and both-ersome to the horses and at times, can be quitepainful. Severely affected individuals often ex-hibit generalized swelling in all four legs.
This condition is thought to be primarily a lymph-system disease, and the pastern dermatitis in thesedraft horses is a secondary result caused by thebody’s inability to properly supply fluids and oxygen-ate the skin of the lower leg. The lymphatics breakdown over time, and protein-rich fluid leaks into thetissues of the lower leg, which results in fibrosis ofthe tissues under the skin and thickening of the skinitself. The tissue fibrosis leads to even more block-age of fluid within the legs, thereby inhibitingproper circulatory flow. This results in neovascu-larization; this is a process by which the body devel-ops new blood vessels in a futile attempt to provideoxygen to its tissues.
Researchers suspect that a deficiency or abnor-mality in a connective tissue component known aselastin is the underlying element and perhaps, thecause of the lymphatic degeneration in these horses.In affected animals, the lymph vessels and deeptissues of the skin do not have sufficient amounts orproper configuration of elastin. The lack of thiscritical tissue element apparently instigates the pro-gression of disease and the chronic progression ofclinical signs.
As the condition becomes more chronic, the lowerleg enlargement becomes permanent, and the swell-ing is firm on palpation. More thick skin folds andlarge, poorly defined, firm nodules develop. Thenodules may become quite large and are often de-
scribed as “golf ball” or even “baseball” in size.Both skin folds and nodules first develop in the backof the pastern area. With progression, they mayextend and encircle the entire lower leg. The nod-ules become a mechanical problem, because theyinterfere with free movement and are frequentlyinjured during exercise. This disease oftenprogresses to include massive secondary infectionsthat produce copious amounts of foul-smelling exu-dates, generalized illness, debilitation, and evendeath.20,21
In a recent report on what may be the same con-dition in several draft breeds, the authors found aperivascular dermatitis dominated by T lympho-cytes with an increase in major histocompatibilitycomplex (MHC) class II�positive dendritic-likecells. Immunohistochemical labeling for cytokera-tins (CK) 5/6, CK10, and CK14 indicated a change intheir expression pattern. This correlated with thedegree of epidermal hyperplasia, indicating abnor-mal differentiation of keratinocytes. There was astatistically significant correlation between theseverity of skin lesions and several other factorsincluding increasing age, increasing cannon circum-ference, prominence of anatomical structures suchas fetlock tufts of hairs, ergots, and chestnuts, andbulges in the fetlock region.22
References1. Frame SR, Harrington DD, Fessler J, et al. Hereditary junc-
tional mechanobulluous disease in a foal. J Am Vet MedAssoc 1988;193:1420–1424.
2. Johnson GC, Kohn CW, Johnson CW, et al. Ultrastructureof junctional epidermolysis bullosa in Belgian foals. J CompPathol 1988;98:331–336.
3. Kohn CW, Johnson GC, Garry F, et al. Mechanobullousdisease in two Belgian foals. Equine Vet J 1989;21:297–301.
4. Sloet van Oldruitenborgh-Oosterbaan M, Boord M. Equinedermatology workshop. In: Thoday KL, Foil CS, Bond R,eds., Advances in veterinary dermatology, vol. 4. Oxford,UK: Blackwell Science, 2002;286–290.
5. Linder KE, Olivry T, Yager JA, et al. Mechanobullous dis-ease of Belgian foals resembles lethal (Herlitz) junctionalepidermolysis bullosa of humans and is associated with fail-ure of laminin-5 assembly. Vet Dermatol 2000;11(Suppl 1):24.
6. Spirito F, Charlesworth A, Linder K, et al. Animal modelsfor skin blistering conditions: absence of laminin 5 causeshereditary junctional mechanobullous disease in the Belgianhorse. J Invest Dermatol 2002;119:684–691.
7. Milenkovic D, Chaffaux S, Taourit S, et al. A mutation inthe LAMC2 gene causes the Herlitz junctional epidermolysisbullosa (H-JEB) in two French draft horse breeds. Genet SelEvol 2003;35:249–256.
8. Crowell WA, Stephenson C, Gosser HS. Epitheliogenesisimperfecta in a foal. J Am Vet Med Assoc 1976;168:56–58.
9. Dubielzig RR, Wilson JW, Beck KA, et al. Dental dysplasiaand epitheliogenesis imperfecta in a foal. Vet Pathol 1986;23:325–327.
10. Lieto LD, Swerczek TW, Cothran EG. Equine epitheliogen-esis imperfecta in two American Saddlebred foals is a laminalucida defect. Vet Pathol 2002;39:576–580.
11. Lieto LD, Cothran EG. The epitheliogenesis imperfecta lo-cus maps to equine chromosome 8 in American Saddlebredhorses. Cytogenet Genome Res 2003;102:207–210.
AAEP PROCEEDINGS � Vol. 52 � 2006 499
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY

12. Hardy MH, Fisher KR, Vrablic OE et al. An inherited con-nective tissue disease in the horse. Lab Invest 1988;59:253–262.
13. White SD, Affolter V, Bannasch DL, et al. Hereditaryequine regional dermal asthenia (HERDA; ‘Hyperelastosiscutis’) in 50 horses: clinical, histologic and immunohisto-logic findings. Vet Dermatol 2004;15:207–217.
14. Solomons B. Equine cutis hyperelastica. Equine Vet J1984;16:541–542.
15. Gunson DE, Halliwell RE, Minor RR. Dermal collagen degra-dation and phagocytosis. Occurrence in a horse with hyperex-tensible fragile skin. Arch Dermatol 1984;120:599–604.
16. Witzig P, Suter M, Wild P, et al. Dermatosparaxis in a foaland a cow�a rare disease? Schweiz Arch Tierheilkd 1984;126:589–596.
17. Scott DW, Miller WH Jr. Equine dermatology. St. Louis:W.B. Saunders, 2003;640.
18. Brounts SH, Rashmir-Raven AM, Black SS. Zonal dermalseparation: a distinctive histopathological lesion associated
with hyperelastosis cutis in a Quarter Horse. Vet Dermatol2001;12:219–221.
19. Tryon RC, White SD, Famula TR, et al. Inheritance ofhereditary equine regional dermal asthenia (HERDA) inthe American Quarter Horse. Am J Vet Res 2005;66:437–442.
20. de Cock HE, Affolter VK, Wisner ER, et al. Lymphoscinti-graphy of draught horses with chronic progressive lympho-edema. Equine Vet J 2006;38:148–151.
21. De Cock HE, Affolter VK, Wisner ER, et al. Progressiveswelling, hyperkeratosis, and fibrosis of distal limbs inClydesdales, Shires, and Belgian draft horses, suggestiveof primary lymphedema. Lymphat Res Biol 2003;1:191–199.
22. Geburek F, Ohnesorge B, Deegen E, et al. Alterations ofepidermal proliferation and cytokeratin expression in skinbiopsies from heavy draught horses with chronic pasterndermatitis. Vet Dermatol 2005;16:373–384.
500 2006 � Vol. 52 � AAEP PROCEEDINGS
IN-DEPTH: SELECTED TOPICS IN DERMATOLOGY