Embed Size (px)
Citation preview

Esophagus DiseaseEsophagus Disease

AchalasiaAchalasia

AchalasiaAchalasiaAchalasia is a primary esophageal motility disorder characterized by failure of a hypertensive LES to relax and the absence of esophageal peristalsis. These abnormalities cause a functional obstruction at the
gastroesophageal junction.
Pathophysiology:
• LES pressure and relaxation are regulated by excitatory (eg, acetylcholine, substance P) and inhibitory (eg, nitric oxide, vasoactive intestinal peptide) neurotransmitters.
• Persons with achalasia lack nonadrenergic, noncholinergic, inhibitory ganglion cells, causing an imbalance in excitatory and inhibitory neurotransmission.
• The result is a hypertensive, nonrelaxed esophageal sphincter.
Causes:
The cause of achalasia is unknown.

Frequency:
In the US: The incidence of achalasia is approximately 1 per 100,000 people per year.
In the GB: About 6.000 people are affected
Age:
Achalasia typically occurs in adults aged 25 - 60 years. Fewer than 5% of cases occur in children.
AchalasiaAchalasia

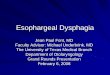
The specimen is the esophagus (27 cm), cardia, and a portion of stomach wall (10 x 10 cm). The organs have been laid open to display the mucosal surfaces.
The esophagus is narrowed at the cardia to approximately 2 cm in circumference. Above this constriction is dilated (maximum 10 cm).
There is patchy mucosal ulceration 7cm from the cardia. The diagnosis is of achalasia of the oesophagus.
This is example of a normal gastroesophageal junction showing the
transition from the esophagus to the stomach.
This is the very bottom of the esophagus, and compared to normal
gastroesophageal junction, this is very tightly shut - there is only a pinhole
opening. In patients with this condition, there is difficulty in swallowing food and it backs up into the esophagus.
AchalasiaAchalasia

Symptoms of AchalasiaSymptoms of Achalasia
The most frequent presenting symptoms are difficulty swallowing (dysphagia). It is insidious and intermittent in the beginning but tends to
become progressively worse. It is rare that it leads to an abrupt loss of ability to eat or drink.
The symptoms are subtle in its onset and most describe "fullness".
• Over 90% of patients have regurgitation of undigested foods. • Chest spasms or pains, resembling heart pain (angina), occur in 30-50% of patients. • Heartburn occurs in 25 to 45% of patients.• Coughing and lung infections from food particles trapped in bronchial tubes (aspiration of food) occur in 10% of patients. Some patients have coughing at night from food aspirating into the trachea from food in the esophagus. Elevating the head of the bed may often help these people. • Hoarseness, drooling, and belching may also occur.
Because of these symptoms, the diagnosis may often be missed.Because of these symptoms, the diagnosis may often be missed. Most commonly, many are misdiagnosed as having gastroesophageal reflux
disease or GERD.

Symptoms of AchalasiaSymptoms of Achalasia
Physical: Physical examination is noncontributory.
Lab Studies: Laboratory studies are noncontributory.
The patient's eating habits change by eating slower, chewing longer, arching the back or raising their arms to
swallowing by gravity. At this point, the esophagus is only a passive tube unable to contract.

Imaging Studies:
Barium swallow:• The esophagus appears
dilated, and contrast material
passes slowly into the
stomach as the LES opens
intermittently. The distal
esophagus is narrowed and
has been described as
resembling a bird's beaka bird's beak
• The test may show
esophageal dilatation
AchalasiaAchalasia

Other Tests:
Esophageal manometry findings include the following:• Incomplete relaxation of the LES in response to swallowing• High resting LES pressure• Absent esophageal peristalsis
Prolonged esophageal pH monitoring is important for the following reasons:• To rule out gastroesophageal reflux disease (GERD)• To determine if abnormal reflux is being caused by treatment
Procedures:
An esophagogastroduodenoscopy (EGD) is performed to rule out cancer of the
gastroesophageal junction or fundus. If a tumor is suspected, an endoscopic
ultrasound is performed at the same time.
AchalasiaAchalasia

Achalasia

Achalasia
"bird-beak" at LES on esophagram "bird-beak" at LES on esophagram

megaesophagus
AchalasiaAchalasia

Esophageal DiverticulaEsophageal Diverticula

Esophageal DiverticulaEsophageal Diverticula
1. Zenker's (pharyngeal, crycopharyngeal) diverticulum is a posterior outpouching of the mucosa and submucosa through the cricopharyngeal muscle. It probably results from incoordination between pharyngeal propulsion and cricopharyngeal relaxation.
2. Midesophageal (traditionally called traction) diverticula are either caused by traction from mediastinal inflammatory lesions or secondary to motor disorders.
3. Epiphrenic diverticulum, also probably of propulsive origin, occurs just above the diaphragm and usually accompanies an esophageal motor disturbance (achalasia, diffuse esophageal spasm).

A diverticulum is a pouch or sac that is created by herniation of a
muscle wall. Zenker’s diverticula are pouches that develop in the
pharynx just above the upper esophageal sphincter.
Zenker’s diverticula occur most often in northern European countries and
those whose heritage is northern European, including the US, Canada and
Australia. It is rare in Asia.
In the US: Fluoroscopic studies of the upper GI tract have shown that
the prevalence of Zenker diverticulum is 0.01-0.1%. They are present
in approximately 2% of patients with nonspecific dysphagia who are
referred for fluoroscopy.
Zenker’s diverticulaZenker’s diverticula

Surgical Picture of Zenker's Diverticulum
The excised diverticulum is opened and inspected
Zenker’s diverticula generally are categorized as small, intermediate, or
large in size.
They extend into the left side of the neck 90% of the time due to a slight convex shape
of the esophagus to that side and the presence of a potential space there.
Zenker’s diverticulaZenker’s diverticula

Killian's triangle is formed posteriorly between the junction of the cricopharyngeus muscle and the lower border of the inferior
constrictor muscle and is the site of origin of Zenker's diverticulum.
Zenker’s diverticulaZenker’s diverticula

Radiograph demonstrating a Zenker's diverticulum. The barium filling the diverticular
pouch.
Upper esophageal sphincter area. Killian's area is located between the inferior
pharyngeal muscle superiorly and the cricopharyngeal muscle inferiorly.
Zenker’s diverticulaZenker’s diverticula

Symptoms of Zenker’s Diverticulum:The combination of the following symptoms is nearly pathognomonic for ZD:
• Dysphagia • Regurgitation of undigested food hours after eating • Sensation of food sticking in the throat • Special maneuvers to dislodge food • Coughing after eating • Aspiration of organic material • Unexplained weight loss • Fetor ex ore • Borborygmi in the neck
Symptoms may last from months to years.
The most dangerous symptom is aspiration (30% of patients). If the diverticula spread into a major vessel, obstruction of the esophagus or trachea can occur. They can cause massive bleeding. Very rarely, squamous cell carcinoma within diverticulum occur (< 0,5% of patients).
Zenker’s diverticulaZenker’s diverticula

Diagnostic Procedures: • Flexible endoscopic evaluation of swallowing (FEES) provides information that may suggest the presence of a ZD, but this test has not supplanted the barium swallow in most surgeons' practices.• Rigid or flexible esophagoscopy is essential before surgical management to assess the nature of the mucosa of the ZD and to exclude the presence of SCC or carcinoma in situ.
Imaging Studies:
• The criterion standard of confirmatory evaluations is the barium swallow with videofluoroscopy.
• This study provides information about size, location, and character of the mucosal lining of the ZD.
• CT and MRI are not routinely used to either confirm or exclude Zenker’s diverticulum
Zenker’s diverticulaZenker’s diverticula

• The fluoroscopic barium esophagram is the primary tool for the diagnosis of Zenker diverticulum.
• The diverticulum appears as an outpouching arising from the midline of the posterior wall of the distal pharynx near the pharyngoesophageal junction.
• This is best identified during swallowing and is best seen on the lateral view, on which the diverticulum is typically noted at the C5-6 level.
• When the diverticulum is large enough to protrude laterally, it protrudes to the left in 90% of the cases.
• After the contrast agent bolus passes the upper esophagus, the diverticulum is typically seen extending posterior to the cricopharyngeus muscle, and contrast material that was trapped within the diverticulum may be regurgitated back into the hypopharynx. www.radiology.vcu.edu
Zenker’s diverticulaZenker’s diverticula

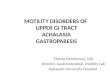
73-year-old man with remnant diverticulum after endoscopic stapling diverticulotomy for dysphagia.
Steep oblique view from preoperative barium study shows 3-cm Zenker's diverticulum (white arrow) above prominent cricopharyngeus (black arrow).
Radiographic Findings and Complications After Surgical or Endoscopic Repair of Zenker's Diverticulum in 16 Patients Am. J. Roentgenol. Sydow et al. 177 (5): 1067.
Zenker’s diverticulaZenker’s diverticula

• A Valsalva maneuver may be helpful in visualizing the diverticulum after swallowing.
• Occasionally, a patient may aspirate contrast material from the diverticulum.
• Pay attention to the lumen of the diverticulum because irregularities or filling defects within the diverticulum may indicate the rare complication of squamous cell carcinoma.
Zenker’s diverticulaZenker’s diverticula

Diverticula of the Diverticula of the esophageal bodyesophageal body

Diverticula of the esophageal body Diverticula of the esophageal body
Midesophageal (traction) diverticula:
caused by traction from mediastinal inflammatory lesions or secondary to motor disorders
Epiphrenic (supradiaphragmatic) diverticula:
Diverticula that occur in the distal esophagus, in the lower 6-10 cm, are termed epiphrenic diverticula.
Epiphrenic diverticulum, probably of propulsive origin usually accompanies an esophageal motor disturbance (achalasia, diffuse esophageal spasm).

Developmental diverticulum
Traction diverticulum
Diverticula of the esophageal body Diverticula of the esophageal body

Midesophageal diverticulum
Diverticula of the esophageal body Diverticula of the esophageal body

Midesophageal and epiphrenic diverticula
Diverticula of the esophageal body Diverticula of the esophageal body

Roentgenogram of esophagus showing a typical pulsion diverticulum of lower part. Such diverticula usually present on the right in the lower 10 cm of thoracic portion of esophagus.
(From Payne WS, and Clagett OT: Pharyngeal and esophageal diverticula. Curr Probl Surg April: 1-31, 1965.)
Esophagus with huge epiphrenic diverticulum occupying approximately half of the right thorax. Note associated
sliding esophageal hiatal hernia. (From Payne WS : Esophageal diverticula. In Shields TW (ed.), General Thoracic Surgery Second Edition. Philadelphia: Lea &
Febiger, 1983, pp. 859-872).
Epiphrenic diverticulum
Diverticula of the esophageal body Diverticula of the esophageal body

Epiphrenic diverticulum
Diverticula of the esophageal body Diverticula of the esophageal body

Caustic Burns of the Caustic Burns of the EsophagusEsophagus

Caustic Burns of the EsophagusCaustic Burns of the Esophagus
• Alkaline caustics and acids are the commonest chemicals implicated in caustic burns.
• Burns from ingestion of such agents may include the oral, pharynx, larynx, esophagus and stomach. Destruction of tissues or of these organs may lead to complications, of which respiratory compromise, esophageal and gastric perforation, septicemia, or even death might occur.
• Patients with ulceration, blisters, even areas of extensive necrosis always tended to develop esophageal strictures with inability to swallow food.
• Repeated dilations to maintain an adequate lumen diameter are performed in patients with chronic strictures.
A barium-swallow esophagogram is performed before the dilatations (i.e., first time in two weeks after ingestions) to evaluate the sites of lesions,
degree of the stenosis and motor function of the esophagus.

Caustic Burns of the EsophagusCaustic Burns of the EsophagusRadiographic findings:
•esophagus tapered throughout its path
•area of narrowing
•irregular contours
•loss of the mucosal pattern
•reduced peristalsis
•rigidity

Esophageal VaricesEsophageal Varices

Esophageal VaricesEsophageal Varices
Most esophageal varices are a result of portal hypertension resulting from cirrhosis.
• The leading cause of cirrhosis in the Western world is alcoholic liver disease, closely followed by viral hepatitis.
• Outside the Western world, the leading causes of cirrhosis are hepatitis B and hepatitis C.
• The lifetime incidence of esophageal varices is approximately 50% for all patients with cirrhosis.
• The annual risk of developing varices is 5-15%.

Esophageal VaricesEsophageal Varices
• The mortality rate for each bleeding episode is approximately 30%.
• If underlying etiology remains untreated, as many as 70% of patients who develop hemorrhage die within 1 year of the initial bleeding episode.
• Bleeding from esophageal varices accounts for approximately 10% of episodes of upper GI bleeding.
Diagnosing varices is critical to prevent the first episode Diagnosing varices is critical to prevent the first episode of hemorrhage. of hemorrhage.
Hemorrhage is a major complication in patients with
esophageal varices, occurring in approximately one third of
patients.

Esophageal VaricesEsophageal Varices

Although endoscopy is the criterion standard in diagnosing and grading esophageal varices, the anatomy outside of the esophageal mucosa cannot be evaluated with this technique.
Therefore, imaging modalities such as barium swallow, CT, MRI, and EUS are also performed for a more complete evaluation.
Grossly, esophageal varices appear as tortuous, dilated, blue veins
running along the long axis of the esophagus.
Esophageal VaricesEsophageal Varices

Imaging Studies
Barium study
Barium swallow examination is not a sensitive test, and it must be
performed carefully with close attention to the amount of barium used and
the degree of esophageal distension. Barium swallow images may help in
detecting only 50% of varices.
However, according to American Academy of Family Physicians, barium
swallow is the imaging modality of choice for demonstrating esophageal
varices.
Esophageal VaricesEsophageal Varices

Barium study
may be of benefit if the patient has a contraindication to endoscopy or if endoscopy is not available.
The procedure should be performed with the patient in the supine or slight Trendelenburg position.
These positions enhance gravity-dependent flow and engorge the vessels.
The patient should be situated in an oblique projection.
This positioning prevents overlap with the spine and further enhances venous flow.
Barium swallow demonstrates multiple serpiginous filling defects primarily involving
the lower one third of the esophagus
Esophageal VaricesEsophageal Varices

Esophageal varices appear as tortuous, serpiginous, longitudinal filling defects projecting into the lumen of the esophagus.
These defects are seen best on relief projections of the esophagus.
Barium study
Esophageal VaricesEsophageal Varices

CT scans
• CT scanning is an excellent method for detecting moderate-to-large
esophageal varices and for evaluating the entire portal venous system.
• CT is a minimally invasive imaging modality that involves the use of only
a peripheral intravenous line; therefore, it is a more attractive method
than angiography or endoscopy in the evaluation of the portal venous
system.
• CT scans also help in evaluating the liver, other (than left gastric vein and
the venous plexus of the esophagus) venous collaterals, details of other
surrounding anatomic structures, and the patency of the portal vein.
Esophageal VaricesEsophageal Varices

• On nonenhanced studies, esophageal varices may not be
depicted well.
• On contrast-enhanced images, esophageal varices appear On contrast-enhanced images, esophageal varices appear
as homogeneously enhancing tubular or serpentine as homogeneously enhancing tubular or serpentine
structures projecting into the lumen of the esophagus. structures projecting into the lumen of the esophagus.
Esophageal VaricesEsophageal VaricesCT findings

CT findings
post contrast axial and coronal reconstructed images
esophageal varices and splenomegaly
From: http://home.earthlink.net/~radiologist/tf/120604.htm
Esophageal VaricesEsophageal Varices

CT findings
enhancing paraesophageal varices splenomegay, dilated paraumbilical veins
Esophageal VaricesEsophageal Varices

• MRI is an excellent noninvasive method for imaging the portal venous system and esophageal varices.
• MRI is becoming a more common examination in pre-TIPS and pretransplantation evaluations.
• The only major disadvantages of MRI compared with CT are its limited availability and cost
MRI
From: www.medical.philips.com
Maximum intensity projection MRI of the portal venous system demonstrates
esophageal varices
Esophageal VaricesEsophageal Varices
• Varices appear as flow voids on conventional T1- and T2-weighted images.
• Esophageal varices and other portosystemic collaterals are demonstrated as serpiginous contrast-enhanced vessels in the portal venous phase.

Hiatal HerniaHiatal Hernia

Hiatal HerniaHiatal Hernia
A hiatal hernia occurs when a portion of the stomach prolapses through the diaphragmatic
esophageal hiatus.
Hiatal hernias are more common in Western countries. The frequency of hiatus hernia increases with age, from 10% in patients younger than 40 years to 70% in patients older than 70 years.
Most hiatal hernias are found incidentally and usually are discovered on routine chest radiographs or CT scans performed for unrelated symptoms. When symptomatic, patients may experience:
• heartburn
• dyspepsia
• epigastric pain
Gastroesophageal reflux disease is a common finding in patients with hiatal hernia

Diaphragmatic hernias may be congenital or acquired.
Acquired hiatal hernias are divided further into nontraumatic and traumatic hernias. The most common types of hernias are those acquired in a nontraumatic fashion.
Hernias acquired in a nontraumatic fashion are divided into 2 types:
1. sliding hiatal hernia
2. paraesophageal hiatal hernia.
A mixed variety is possible.
Approximately 99% of hiatal hernias are sliding, and the remaining 1% are paraesophageal.
Hiatal HerniaHiatal Hernia

From: http://www.gastrointestinalatlas.com/index.html
1. Sliding hiatal hernia is the most
common type of hiatal hernia.
• It occurs when the
gastroesophageal junction, along
with a portion of the stomach,
migrates into the mediastinum
through the esophageal hiatus.
• The majority of patients with
demonstrated hiatal hernias are
asymptomatic.
Hiatal HerniaHiatal Hernia

2. In paraesophageal hernia, also called rolling-type hiatal hernia, the
widened hiatus permits the fundus of the stomach to protrude into the
chest, anterior and lateral to the body of the esophagus; however, the
gastroesophageal junction remains below the diaphragm.
PParaesophageal hernias are potentially life threatening because of araesophageal hernias are potentially life threatening because of
the risk of volvulus and incarceration. the risk of volvulus and incarceration.
No clear correlation exists between the size of a hiatal hernia and the severity of the symptoms. A very large hiatal hernia may be present with no
symptoms at all.
Hiatal HerniaHiatal Hernia

Hiatal HerniaHiatal Hernia

Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging StudiesAn upper GI barium series is the definitive method of diagnosing hiatal hernias.
The lower esophageal sphincter (LES)
Ampulla phrenica
Epiphrenic esophageal dilatation
Normal anatomy of gastroesophageal junction
stomach
esophagus

Upper GI barium series • A single-contrast barium swallow performed with the patient in the prone position is more likely to demonstrate a sliding hiatal hernia than an upright double-contrast examination.
• The A-ring is an indentation sometimes seen on barium studies, and it marks the upper part of the LES. Just below this is a slightly dilated part of the esophagus, forming the vestibule.
• A second ring, the B-ring, may be seen just distal to the vestibule
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

A sliding hiatal hernia
Symptomatic lower esophageal mucosal ring (B-ring) that cause dysphagia is termed Schatzki ring.
The presence of a B-ring more than 1-2 cm
above the diaphragmatic
impression confirms the diagnosis of a
sliding hiatal hernia
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging StudiesUpper GI barium series • A single-contrast barium swallow performed with the patient in the prone position is more likely to demonstrate a sliding hiatal hernia than an upright double-contrast examination.

Upper GI barium series • The hernia can often be recognized by the demonstration of mucosal gastric folds within the hernia. • On a dynamic study, the esophageal peristaltic wave ceases above the hiatus; thus, the end of a peristaltic wave delineates the esophagogastric junction.
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

Upper GI barium series
Esophagogram shows that a portion of stomach lies above the diaphragm.
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

Upper GI barium series
A paraesophageal hiatal hernia is diagnosed by the position of the gastroesophageal junction. The cardia of the stomach - esophagogastric junction usually remains in the normal position below the diaphragmatic hiatus, and only the stomach herniates into the thorax, adjacent to the normally placed gastroesophageal junction.
Esophagogram depicts elevated gastric fundus extending through the widened esophageal hiatus to
the thoracic cavity (arrows).
The intra-abdominal position of the gastroesophageal junction
(open arrow) is normal.
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

Upper GI barium series
Paraesophageal Hernia
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

Plain radiography • Most hiatal hernias are found incidentally on routine chest radiographs. • The hernia may be seen as a retrocardiac mass with or without an air-fluid level. • The hernia usually is positioned to the left of the spine
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

Plain radiography
• The air-fluid level in the lateral projection
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

Plain radiography • The two air-fluid levels; one in the stomach and the other in the esophagus • Inhomogeneous cardiac density • Retrocardiac density
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

CT Findings
• Hiatal hernias often are seen incidentally on CT scans obtained for other indications. • A hiatal hernia appears as a retrocardiac mass with or without an air-fluid level. The mass usually can be traced into the esophageal hiatus on sequential cuts. • Herniation of omentum through the esophageal hiatus may result in an increase in the fat surrounding the lower esophagus.
Mediastinal window of enhanced CT scan obtained at the level of the
suprahepatic inferior vena cava shows that the thorax contains a portion of
stomach (arrows). The aorta is displaced to the right
Sliding hiatal hernia
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

A totally intrathoracic stomach is not a true hiatal hernia because herniation occurs through a defect in the central tendon of the diaphragm.
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

Diaphragmatic herniation is a rare complication of thoracic and abdominal surgery
The barium swallow radiograph An incarcerated barium-filled stomach in
the chest
Lateral view of magnetic resonance imaging A rupture of the diaphragm and intrathoracic stomach show a rupture of the diaphragm.
From: Interactive Cardiovascular and Thoracic Surgery 2:544-546(2003)
Hiatal Hernia - Hiatal Hernia - Imaging StudiesImaging Studies

Peptic UlcerPeptic Ulcer

Peptic Ulcer• Peptic ulcers are mucosal breaks of 3 mm or larger.
• Gastric ulcers account for about one third of peptic ulcers, and duodenal ulcers account for the rest.
• Because a small percentage (<5%) of gastric ulcers are due to ulcerated gastric carcinomas, all gastric ulcers must be carefully assessed to differentiate benign lesions from malignant lesions.
Helicobacter pylori infection and the use of nonsteroidal anti-inflammatory drugs (NSAIDs) are the 2 main factors in the pathogenesis of peptic ulcers.
H. pylori infection occurs in 75% of gastric ulcers and 90% of duodenal
ulcers.
This photo taken with a high powered electron microscope shows the tiny H. pylori bacteria (pink) attacking the gastric cells which line the inside of the stomach. This is the "ulcer bacteria" that was re-discovered by Dr. Barry Marshall in Australia in 1982. Each year, over 7 million Americans suffer from H. pylori related disease

Gastric UlcerGastric Ulcer

Gastric UlcerGastric UlcerFrequency: In the US: Approximately 15% of the US population has evidence of a peptic ulcer at some time. Of these, about 5% are gastric ulcers, and the rest are duodenal ulcers. Overall, the incidence of gastric ulcers has been decreasing over the past 3-4 decades. In contrast to duodenal ulcers that occur in adults of all ages, gastric ulcers occur mainly in adults older than 40 years. • About 1 in 10 Americans develop at least one ulcer during their lifetimes. • Ulcers affect about 5 million people each year. • More than 40,000 people a year have surgery because of persistent symptoms or problems from ulcers. • Each year about 6,000 people die of ulcer-related complications.
Internationally: The annual incidence of gastric ulcers varies from approximately 1 case per 1000 population in Japan to 2.7 cases per 1000 population in Scotland.
People with low socioeconomic status are more likely to acquire H. pylori infection. Infected individuals are 3 times more likely to develop gastric ulcer compared to those
unexposed to the bacteria.
Stomach ulcer at endoscopy Surgical specimen

Preferred Examination:
• Begin the evaluation with history taking and physical examination. • Perform blood tests, including a full blood count and liver function tests. • Inspect the stool, and test it for the presence of occult blood. • Perform either fiberoptic endoscopy or a double-contrast barium study of
the upper GI tract. • Endoscopy has become the diagnostic procedure of choice for
patients with suspected duodenal ulcer. • Double-contrast examinations of the upper GI tract remain a useful
alternative to endoscopy but have a lower sensitivity especially in the
detection of small duodenal ulcers. • Test for the presence of H. pylori infection. This is essential in all
patients with peptic ulcers.
Gastric UlcerGastric Ulcer

Endoscopy with biopsy has a sensitivity of 95%.
However, endoscopy is more invasive and costly
than a double-contrast study and multiple biopsy
samples are needed to avoid sampling errors.
Single-contrast barium studies have an overall sensitivity of 75%, but
double-contrast barium examinations have a sensitivity of as high as 95% in
the detection of gastric cancer. These results are comparable to those of
endoscopy, and double-contrast barium examination remains a useful
alternative to endoscopy.
Barium studies have a disadvantage in that biopsy specimens of the lesion
cannot be obtained to test for H. pylori infection or to evaluate for the
presence of malignancy.
Preferred Examination:
Gastric UlcerGastric Ulcer

Radiologic features
• Gastric ulcers are usually seen as
round or ovoid collections of
barium, but they can also be linear,
rod or star shaped. Linear ulcers are
often observed in the healing
stages. • Ulcers smaller than 5 mm may not
be detected on barium studies. • Ulcers may vary from 3 mm to more
than 5 cm in diameter. Giant ulcers
(>3 cm) have a greater risk of
complications such as bleeding and
perforation.
Gastric UlcerGastric Ulcer

Radiologic features
• Most benign ulcers are
located in the lesser curvature
or posterior wall of the antrum
or body of the stomach.
• Only about 5% of benign
ulcers are located in the
anterior wall or greater
curvature.
Gastric UlcerGastric Ulcer

Radiologic features
Hampton lines, ulcer collars, and ulcer mounds are classic features of benign
gastric ulcers, but they are observed in only a minority of lesser-curve ulcers.
The smooth, round, or oval ulcer crater projects beyond the contour of the adjacent gastric wall.
Areae gastricae adjacent to the ulcer may be enlarged because of edema.
Gastric UlcerGastric Ulcer

Radiologic features
Undermining of the mucosa in the base of the ulcer results in the appearance of a thin radiolucent line called the Hampton line that divides the barium in the ulcer crater from that in the body of the stomach.
spot radiograph
Gastric UlcerGastric Ulcer

Radiologic features
If the rim of mucosa becomes edematous, a wider radiolucent band or ulcer collar may be observed.
Posterior-wall ulcer - an ulcer collar is seen as a radiolucent halo surrounding the ulcer
Lesser-curve ulcer - spot radiograph
Gastric UlcerGastric Ulcer

Radiologic features
Less commonly, the edema and swelling around the ulcer may produce an ulcer mound with poorly defined outer borders.
the ulcer (U) gastric mucosa (M) large arteries at the base of the ulcer (A).
Gastric UlcerGastric Ulcer

Radiologic features
Retraction of the gastric wall adjacent to lesser-curve ulcers may lead to the
formation of smooth, symmetric folds that radiate from the ulcer crater
radiating mucosal folds (arrows)
The gastric mucosal folds tend to radiate outwards from the margin of the ulcer - this is the result of the fibrosis which occurs in the base of a long
standing chronic ulcer.
Gastric UlcerGastric Ulcer

Radiologic features
A rare cause of peptic ulcers is Zollinger-Ellison syndrome (ie, gastrinoma).
The hallmark of Zollinger-Ellison syndrome is the profound hypersecretion of gastric acid.
Significant disruption of the mucosal integrity often results in multiple duodenal and gastric ulcers.
Gastric UlcerGastric Ulcer

spot radiograph
Radiologic features - healing and scarring
Ulcer healing is demonstrated as a decrease in ulcer size and, often, a change in shape from round to linear at follow-up studies.
Complete healing, or disappearance of the ulcer, is usually observed 8 weeks after medical treatment
Gastric UlcerGastric Ulcer

"Hourglass" stomachDue to chronic peptic ulceration there is fibrosis and contracture of the stomach leading to an hourglass shape as well as altered mobility.
Radiologic features - healing and scarring
„The hypothesis is proposed that hour-glass stomach is produced by gross scarring around a severe benign chronic gastric ulcer under the influence of prolonged exposure to aspirin.”
From: Med J Aust. 1976 Oct 30;2(18):674-6. Hour-glass stomach: an explanation. Floate DA, Duggan JM.
Gastric UlcerGastric Ulcer

Appearances suggestive of a benign ulcer
• About 95% of gastric ulcers are benign. • The double-contrast technique allows differentiation of benign and
malignant gastric ulcers in most cases.
The following features are associated with a benign ulcer: • The ulcer projects beyond the healthy lumen on the profile view.• The margin of the ulcer crater is sharply defined and smooth en face. • Any filling defect that surrounds the ulcer, as a result of edema, is smooth
and symmetric and merges with the healthy mucosa. • The mucosal folds radiate to the edge of the ulcer.
Benign ulcers that do not have these typical features are classed as indeterminate, and endoscopy and biopsy are required, as they are for
ulcers that appear malignant.
Gastric UlcerGastric Ulcer

Appearances suggestive of malignancy
The following features are associated with a malignant ulcer:
• The ulcer crater has an intraluminal location. Exceptions are ulcers in the
antrum or greater curvature, where benign ulcers are often drawn inward
because of muscle spasm in the adjacent stomach wall. • The margins of the ulcer crater may be irregular and nodular. • The ulcer crater is surrounded by an asymmetric mass that has an abrupt
outer border with the healthy mucosa. • Clubbed mucosal folds terminate short of the ulcer crater.• Ulcers in the fundus are rare, and almost all are malignant.
There are no malignant ulcers; there are ulcerating malignancies.
The radiologic differentiation between benign and malignant ulcers may be difficult.
Gastric UlcerGastric Ulcer

CAT Scan
CT has no part in the primary detection of gastric ulcers.
It has a role in the detection of subphrenic and other collections that may occur after a perforation of a gastric ulcer
68-year-old man with perforated duodenal ulcer (solid arrow), severe epigastric pain, and diffuse peritoneal signs. CT scan shows free air and
extravasated contrast material in periphepatic space (open arrow).
From: AJR 2000; 174:901-913 Helical CT in the Evaluation of the Acute Abdomen. Richard M. Gore et al.
Gastric UlcerGastric Ulcer

30-year-old man with suspected pancreatitis. CT scan reveals benign gastric ulcer in lesser curvature (arrow).
From: AJR 2000; 174:901-913 Helical CT in the Evaluation of the Acute Abdomen. Richard M. Gore et al.
CAT Scan
Gastric UlcerGastric Ulcer

DuodenalDuodenal Ulcer Ulcer

Duodenal UlcerDuodenal Ulcer
Frequency:
In the US: The prevalence of duodenal ulcer is estimated to be 6-15% in the general
population. Most individuals do not have clinically significant ulcer disease. The prevalence
is linked to the presence of H pylori.
Approximately 10% of young men have H pylori, and the proportion of people with the
infection increases steadily with age.
Approximately 10% of the US population has evidence of a duodenal ulcer at some time. Of
those infected with H pylori, the lifetime prevalence is approximately 20%.
More than 95% of duodenal ulcers are found in the first part of the duodenum; most are less than 1 cm in diameter.
Duodenal ulcer is a common condition characterized by the presence of a well-demarcated break in the mucosa that may extend into the muscularis
propria of the duodenum.

Endoscopy• Esophagogastroduodenoscopy (EGD) is the most sensitive test available to detect duodenal ulcer. It has a sensitivity greater than 95%.• With EGD, the ulcer can be visualized, a biopsy specimen can be obtained, and, if required, bleeding ulcers can be treated directly. • EGD is a more invasive test and requires conscious sedation in many patients.
Imaging Studies• Single-contrast barium radiography can detect 70-80% of duodenal ulcers. • The sensitivity increases to greater than 90% when double contrast radiography is performed
and evaluated by an experienced radiologist.
Test for the presence of H. pylori infection. This is essential in all patients
with peptic ulcers.
Duodenal UlcerDuodenal Ulcer

A 1 cm irregular ulcer crater in the duodenal bulb on air contrast spot films with patient in the right posterior
oblique position
The specimen includes the distal part of the gastric antrum, the pylorus and
proximal duodenum.
On the posterior wall of the duodenum there is an ulcer 3 cm in greatest
diameter.
1. small, round/ovoid/linear ulcer niche
Radiologic features
Duodenal UlcerDuodenal Ulcer

1. small, round/ovoid/linear ulcer niche
Radiologic features
This is a 76 y.o. man with nausea and abdominal pain who underwent a barium study shown above.
The series reveals a small, ovoid ulcer in the duodenal bulb (retained barium in the ulcer crater).
The majority of gastric and duodenal ulcers are single.
Duodenal UlcerDuodenal Ulcer

2. "kissing ulcers": ulcers opposite from each other
Multiple duodenal ulcers A spot film of the duodenum without abdominal compression shows no evidence of deformity
of the duodenal bulb
A spot film of the duodenum with compression reveals two typical crater-form ulcers and symmetric folds that radiate from the ulcers
Radiologic features
When multiple ulcers are found, Zollinger-Ellison
syndrome should be suspected.
Duodenal UlcerDuodenal Ulcer

3. "clover-leaf deformity„ of the duodenal bulb
Radiologic features
Duodenal ulcers usually occur in the posterior wall of the bulb.
Because of its recurrent course, the resulting scarring will produce a typical cloverleaf deformity in response to constriction around the ulcer.
Duodenal UlcerDuodenal Ulcer

This study reveals a small duodenal ulcer crater on the
inferior aspect of the bulb with a moderately severe
cloverleaf deformity of the bulb.
Radiologic features
Marked deformity with a large pseudodiverticulum at the top (the
duodenal lumen is toward the bottom)
Duodenal UlcerDuodenal Ulcer

Complications of Peptic Complications of Peptic UlcerUlcer

Complications of Peptic UlcerComplications of Peptic Ulcer
• Bleeding
• Gastric outlet obstruction
• Perforation occurs
• Penetration

Bleeding is slightly more common in the duodenum than the stomach
• Hemorrhage occurs in 20-30% of ulcers • A filling defect in the ulcer crater may represent a blood clot
Complications of Peptic UlcerComplications of Peptic Ulcer

Gastric outlet obstruction is less common than bleeding (5%)
• It is most common in duodenal ulcers, but it also occurs in antral
or pyloric-channel ulcers
• Benign ulcer disease at pylorus is a more likely to cause gastric
outlet obstruction than ca
Complications of Peptic UlcerComplications of Peptic Ulcer

Barium upper GI studies are very helpful because they can delineate the gastric silhouette and demonstrate the site of obstruction.
An enlarged stomach with a narrowing of the pyloric channel or first portion of the duodenum helps differentiate GOO from gastroparesis.
Gastric outlet obstruction
Contrast study demonstrating a grossly distended stomach with absence of distal intestinal gas
due to outlet obstruction
Complications of Peptic UlcerComplications of Peptic Ulcer

Gastric outlet obstruction
Endoscopy, CT abdomen and barium study are suggestive of gastric outlet obstruction
Complications of Peptic UlcerComplications of Peptic Ulcer

Perforation occurs in as many as 10% of patients with peptic ulcer disease
but is less common in gastric ulcers
• Most perforations arise from ulcers in the anterior aspect of the duodenal
cap and, less commonly, from the anterior aspect of the lesser curve of the
stomach
• Free air is not detected by x-ray in 25-35% of perforated duodenal ulcers
Penetration is the extension of the ulcer beyond the serosa in to adjacent
structures
• Pancreas is most common site (in two thirds of cases), but also biliary
tree, colon
• An abscess may form in the lesser sac and liver
Complications of Peptic UlcerComplications of Peptic Ulcer