Embed Size (px)
Citation preview
Estimations of radiation-induced risks from low doses
and how to communicate these risks
Sören Mattsson
Medical Radiation Physics, Lund University and
Skåne University Hospital Malmö, Sweden
Medical Physics in the Baltic States
11th Conference & Workshop
10-12 October 2013
Malmö
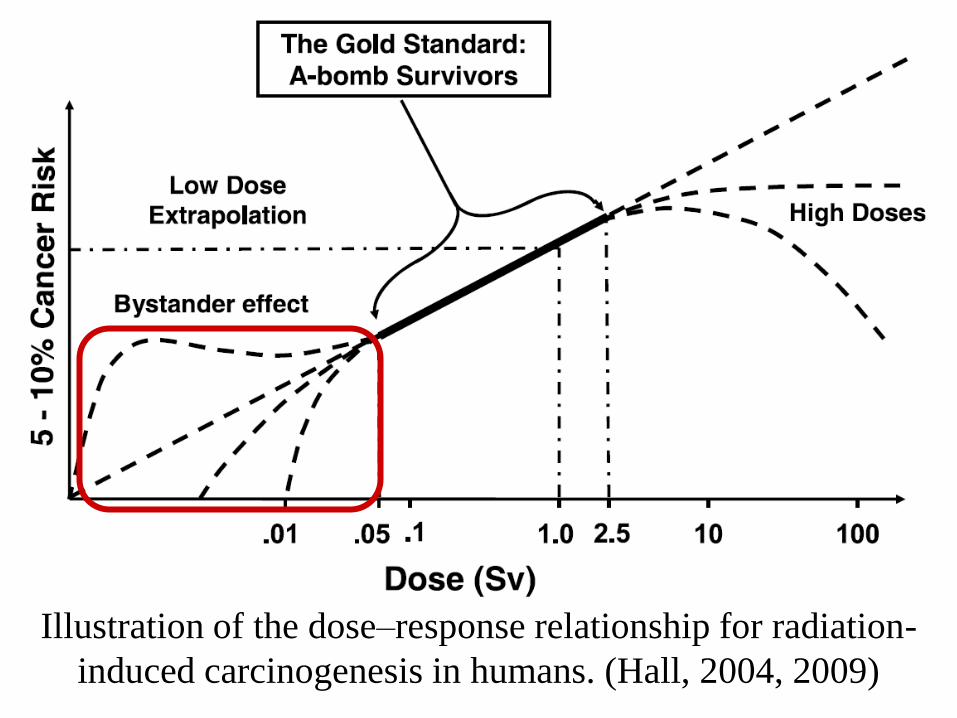
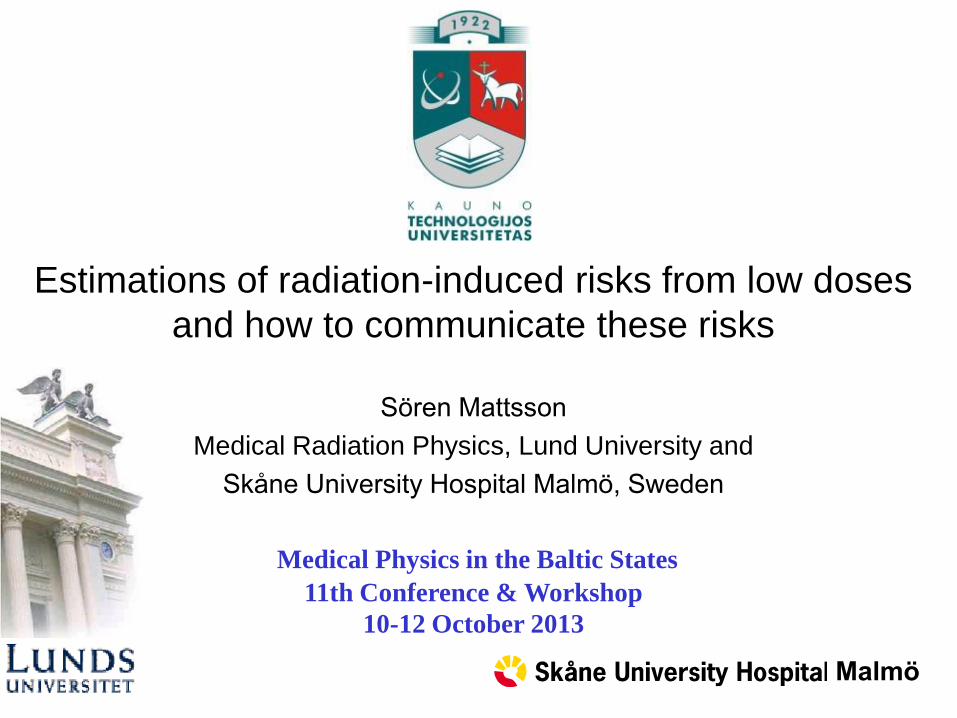
Illustration of the dose–response relationship for radiation-
induced carcinogenesis in humans. (Hall, 2004, 2009)
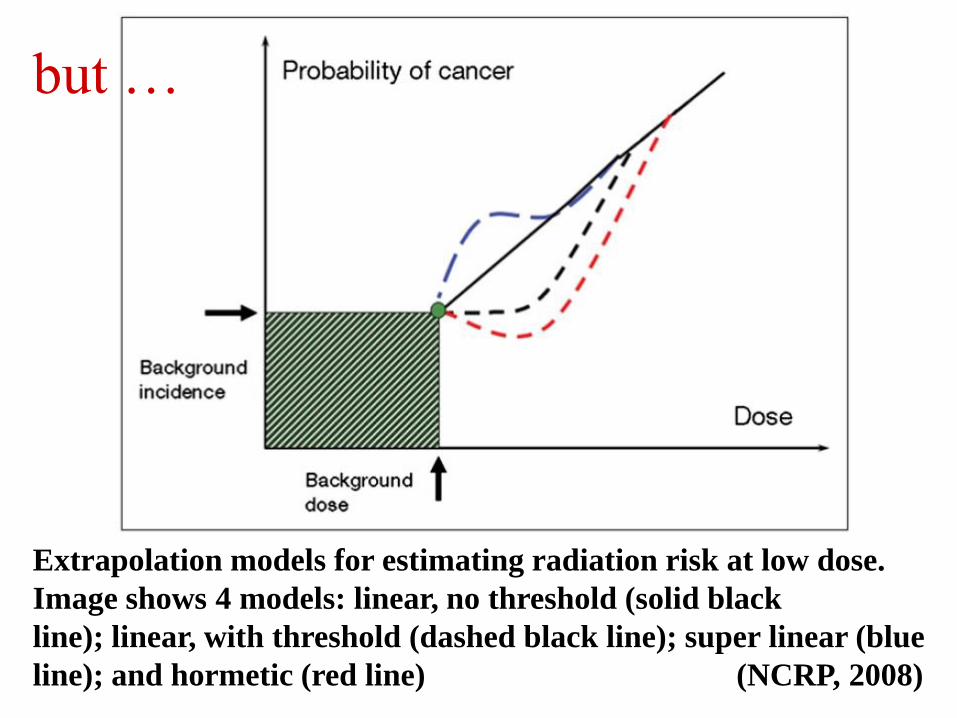
Extrapolation models for estimating radiation risk at low dose.
Image shows 4 models: linear, no threshold (solid black
line); linear, with threshold (dashed black line); super linear (blue
line); and hormetic (red line) (NCRP, 2008)
but …
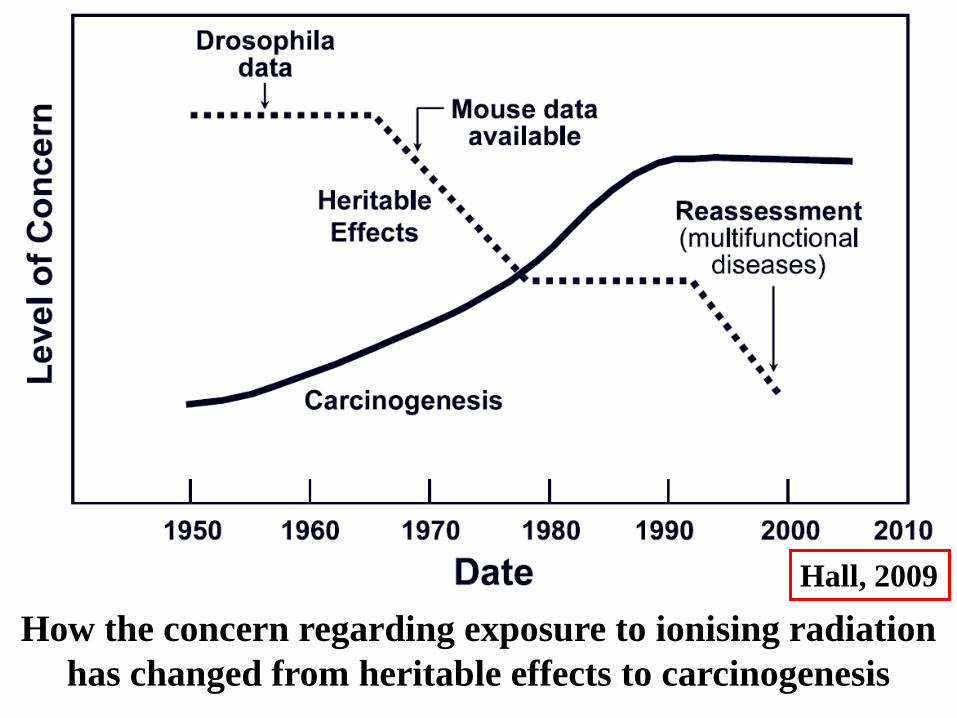
How the concern regarding exposure to ionising radiation
has changed from heritable effects to carcinogenesis
Hall, 2009

Radiation-induced cancer: Scientific basis for current radiation
protection. Epidemiology
• Survivors of Hiroshima and Nagasaki • Patients in health care (radiation
therapy, repeated diagnostic radiology, CT investigations of children)
• Occupationally exposed persons • Environmental exposures
Animal experiments
Cell research

Epidemiology: All cancers – All ages
Deviation of cancer mortality from the average (0/00)
in 1996-2005 (SEER-USA) and radiation effects (ICRP)

Hiroshima/Nagasaki 1945
86 572 persons

Solid cancers

Solid cancers

Solid cancers
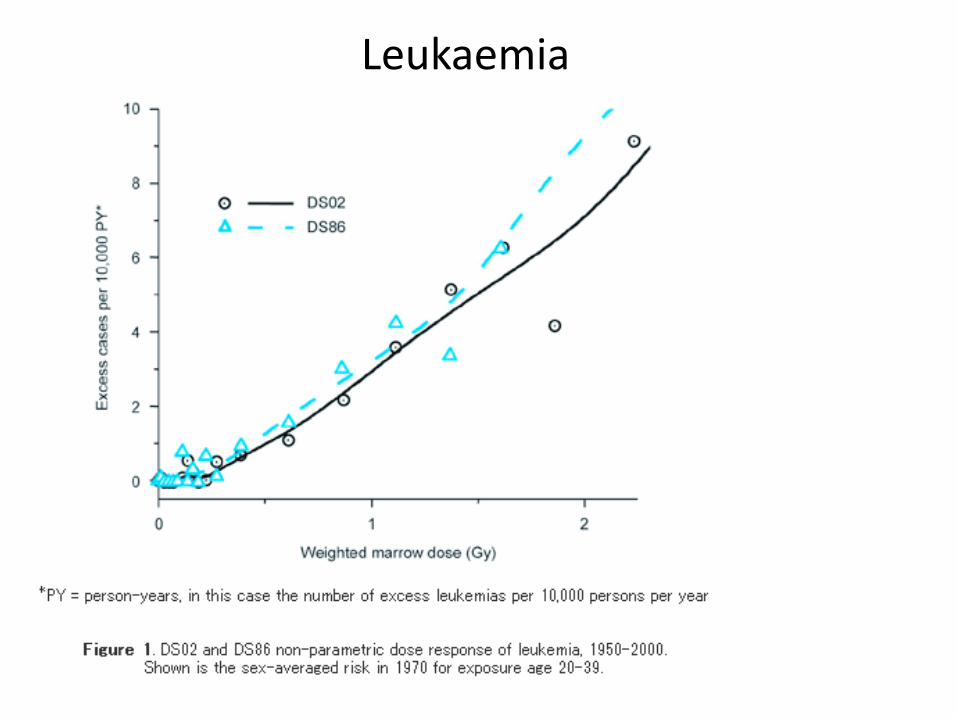
Leukaemia
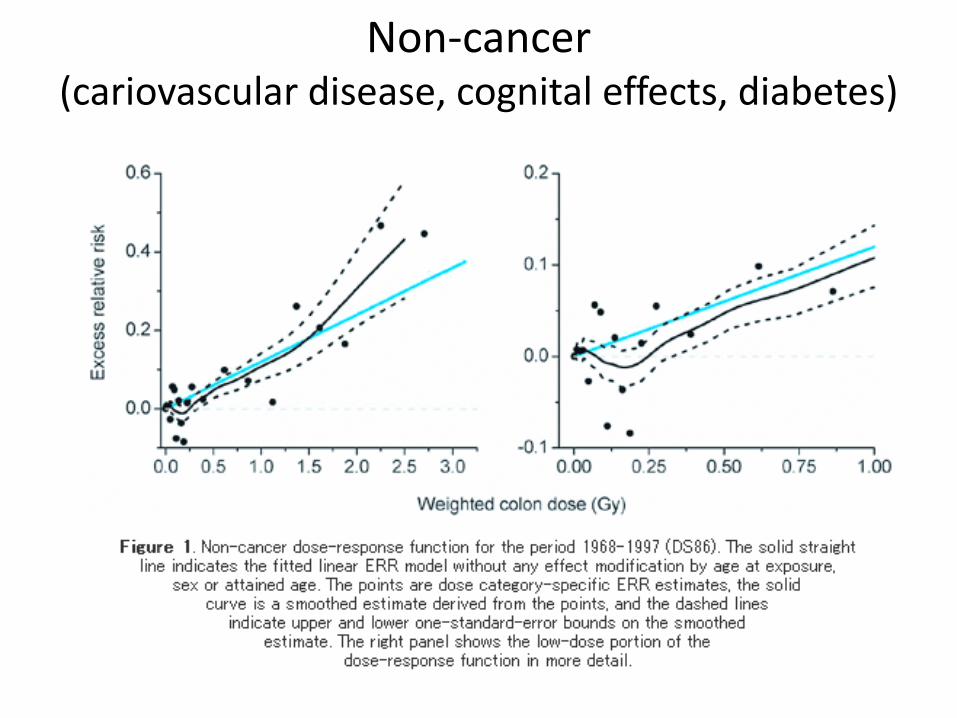
Non-cancer (cariovascular disease, cognital effects, diabetes)

Patients in healthcare • External radiotherapy • Haemangioma treatment with 226Ra • Chest radiograph at TBC - dose to the breast • Thyroid diagnostics with 131I • In utero diagnostic x-rays • Children who were examined with CT
Occupationally exposed persons • Medical staff • Chernobyl emergency and recovery workers • Participants in nuclear weapons tests • Workers in the nuclear weapons and power
industries • Underground miners • Radium dial painters
Environmental exposures • Radon in homes • Chernobyl contaminated areas • Mayak, Techa river, Kyshtym

Cancer risk
• UNSCEAR, lethal solid cancer: 11% Sv –1 (men 9%, women 13%)
• Reduce with a factor of 2 at low doses or dose-rates, which means a risk of about 5% Sv–1 (uncertainty interval: 1%-9%)
• Risk for fatal leukemia: 1% at 1 Sv; 0,05% at 0,1 Sv

Equivalent dose, Sv Effective dose, Sv
Risk of dying from radiation-induced cancer later in life (population average) according to ICRP
5% per Sv (1-9%)
10% per Sv
?

Base for information about radiation risks of low-dose radiation exposure - Health effects of low dose radiation exposure (5, 10, 20 mSv)? - Results from epidemiology in general - Results from epidemiology related to specific age groups - Biophysical arguments - The linear non-threshold (LNT) - model

What happens at lower doses
of radiation? There are data to support the hypothesis
that there is a risk also at lower doses
- Increased risk of cancer during child-
hood after X-ray in utero with 6-10 mSv
(mean 1 electron / cell)
- Biophysical argument
If the dose is reduced, we get fewer
electron tracks and fewer hits of cells.
The cells that are hit suffer the same
type of injury and the same biological
process is initiated.
- Increased risk of cancer after CT-
investigations during childhood.
Pelvimetry or obstetric abdominal examination
Average absorbed dose: 6 mSv
80 kV x-rays
Equivalent to about 1 electron
per nucleus
Alice Stewart (1906-2002)

The base of the biophysical argument for a linear relationship between dose and effect
at low doses: Track structure at 1000, 10 and 1 mSv

Risk varies with age
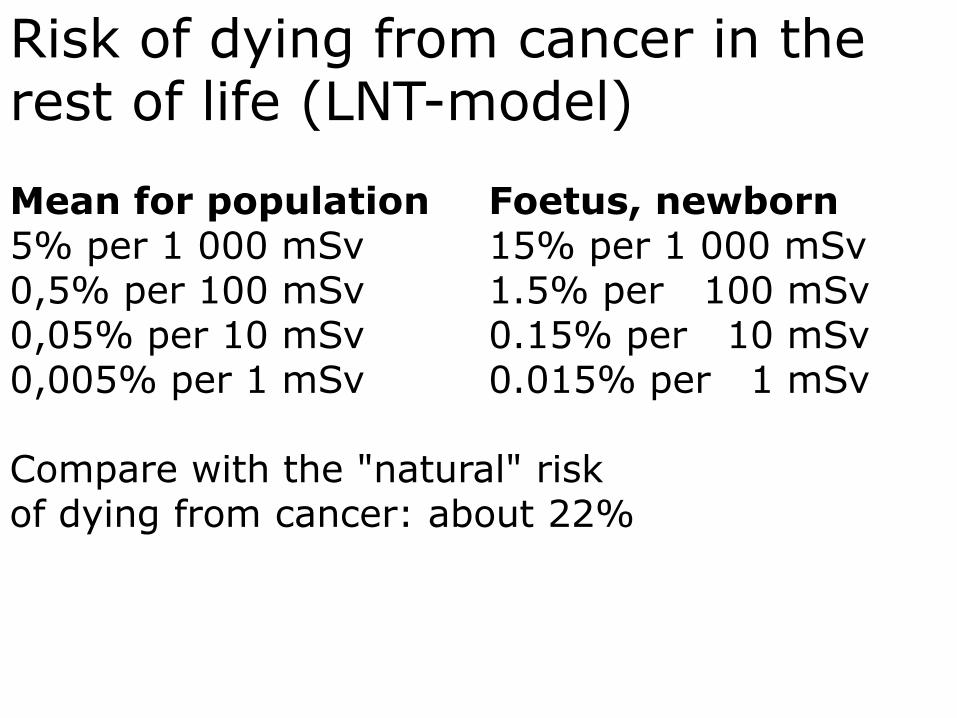
Risk of dying from cancer in the rest of life (LNT-model) Mean for population Foetus, newborn 5% per 1 000 mSv 15% per 1 000 mSv 0,5% per 100 mSv 1.5% per 100 mSv 0,05% per 10 mSv 0.15% per 10 mSv 0,005% per 1 mSv 0.015% per 1 mSv Compare with the "natural" risk of dying from cancer: about 22%

Remaining questions • Cancer The effect of low doses and dose-rates The effect of different types of radiation Extrapolations over time and between countries The importance of factors that may modify the risk Age Sex Genetically determined differences in radiosensitivity Environmental factors • Non-cancer effects Cardiovascular effects at low doses and dose rates Cognitive effects Diabetes

Some leading principles for all information 1. Transparency, openness. Tell the truth 2. Ask whether you are being understood 3. The listener must thrust on you 4. Initiative and speed 5. Quality
Communication about radiation risks The respect and fear of radioactivity and radiation is very deep. In other contects the risks have been/still are neglected. Communication of radiological risks is not an easy task. Different in medicine and health-care than in the society after an accident .

Transparency, openness. Tell the truth.
“Never underestimate people's talents,
but do not overestimate their knowledge”.
Take each question seriously-It is a chance to teach. Communicate therefore, openly and clearly.
The listener must
thrust you
Requires transparency.
Avoid ”double messages”. No danger
Dagens Nyheter 2/5 1986

It is also important how to convey the information Example: Activity levels in food. It is perceived very differently if you say that the limit for Cs-137 in foodstuff is 300 Bq/kg or you say that you have to eat 75 000 Bq to get a dose of 1 mSv. As it was perceived, 300 Bq/kg was by many considered as a toxic limit. Concentration (Bq/kg)- and doserate (mSv/hr) values that are supposed to be tolerated for a long time will be perceived as absolute limits.
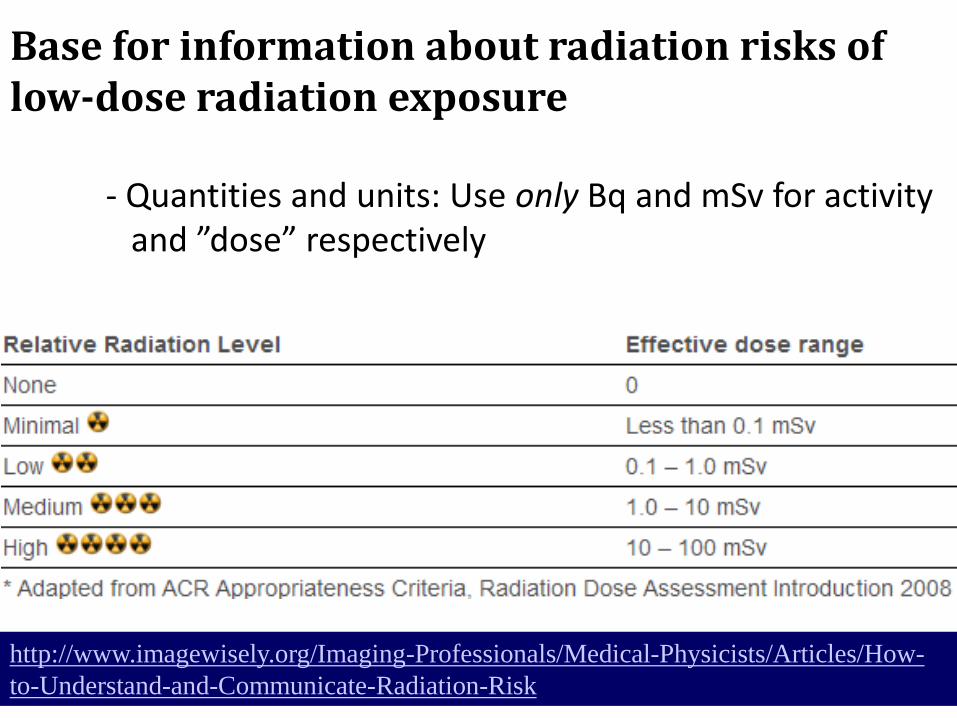
Base for information about radiation risks of low-dose radiation exposure - Quantities and units: Use only Bq and mSv for activity and ”dose” respectively
http://www.imagewisely.org/Imaging-Professionals/Medical-Physicists/Articles/How-
to-Understand-and-Communicate-Radiation-Risk



Comparison of dose contributions with the natural effective dose

What to tell the radiologist and the general practitioner
Any added risk, however small, is not acceptable if it does not benefit the patient. Justification and optimization of a procedure are absolutely essential. Diagnostic reference levels should be used to reduce variations from one center to another and to promote optimal dose indicator ranges for medical imaging protocols. The basic principles of radiation protection need to be respected to help counteract the unjustified explosion in the number of procedures now being performed.

… thank you for listening [email protected] Telephone +46 40 331374


Verdun et al., 2008

A 10 year old who gets 4 mSv effective dose (Ex: CT abdomen,
bone scan). Risk of dying from radiation-induced cancer in the rest
of life: 10% per Sv. 0.004 Sv x 10% per Sv gives a risk of 0.0004 or
1 per 2 500 (the star in the picture).
Example of a risk comparison
Of 2 500 10 year old
children, 550 will die from
cancer for reasons other
than man-made sources of
ionizing radiation