Embed Size (px)
Citation preview

Infectious complications of the aorta-
how to approach
Olaf Richter
Ev. Diakonissenkrankenhaus LeipzigDept. of Vascular Surgery
Ev. Diakonissenkrankenhaus LeipzigAkademisches Lehrkrankenhaus der Universität Leipzig
Ev. Diakonissenkrankenhaus LeipzigAkademisches Lehrkrankenhaus der Universität Leipzig
Eine Einrichtung der edia.con-Gruppe

Disclosure
Speaker name:
Olaf Richter, MD
I have the following potential conflicts of interest to report:
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interestX
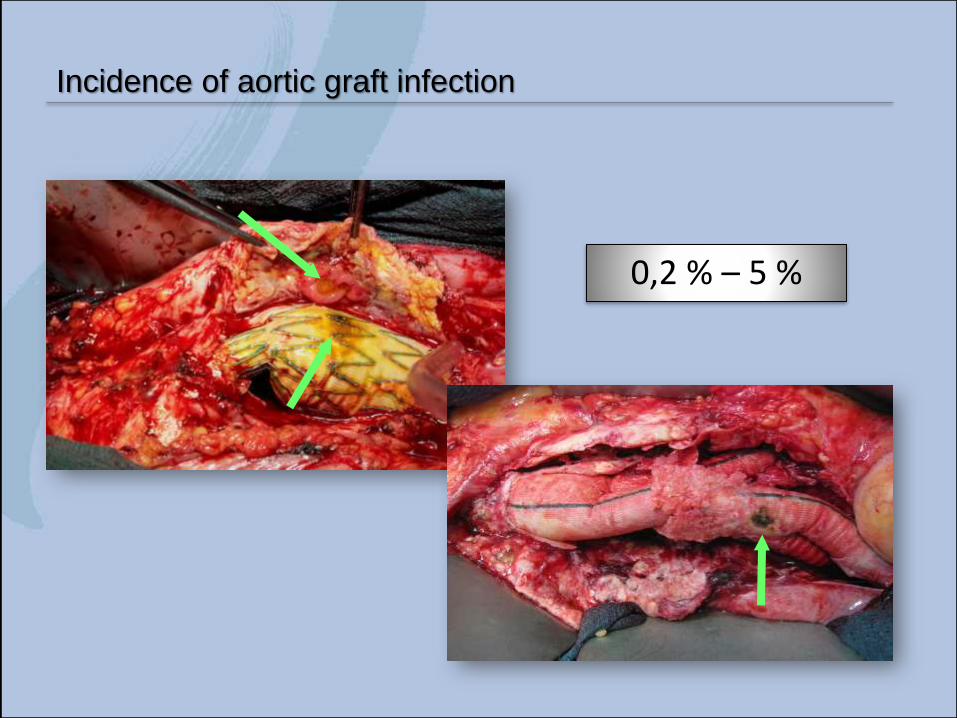
Incidence of aortic graft infection
0,2 % – 5 %

Therapeutic options
Long-term AntibiosisTerpling et al., Scand J Infect Dis. 2006;38(5):388-92Turgut et al., BMC Infect Dis. 2005 Oct 21;5:91Treitl M et al, Cardiovasc Intervent Radiol. 2011 Jun;34(3):642-6
Drainage Raffatto et al., J Vasc Surg. 2004 Oct;40(4):826-9.
LavageVoboril et al., Ann Vasc Surg. 2004 May;18(3):372-5.Francois et al., Ann Vasc Surg. 1991 Mar;5(2):199-201.
Muscle FlapSeify et al., Plast Reconstr Surg. 2006 Apr;117(4):1325-33.Mitra et al., Chest. 2005 Aug;128(2):1040-3.Schutzer et al., Vasc Endovascular Surg. 2005 Mar-Apr;39(2):159-62.
Cutis Flap Nenezic et al., Srp Arh Celok Lek. 2005 Jan-Feb;133(1-2):69-71.
Omentum plastic
Van Krunckelsven et al., Eur J Vasc Endovasc Surg. 1995 Aug;10(2):256-7.Krabatsch et al., Eur J Cardiothorac Surg. 1995;9(4):223-5.Shah S, Sinno S, Vandevender D, Schwartz J., Ann Plast Surg. 2013 Jun;70(6):680-3
Bovine Pericardium Lutz et al., Ann Vasc Surg. 2017;41:118-26
Vacuum TherapyDosluoglu et al., J Vasc Surg. 2005 Volume 42 (5):989-992Mayer D, Hasse B, Koelliker J, Enzler M, Veith FJ, Rancic Z, Lachat M., Ann Surg. 2011 Nov;254(5):754-59
Adhesive Dressing Aksoy et al., Surg Today. 2006;36(1):52-6.
Vein Da Gama et al., Rev Port Cir Cardiotorac Vasc. 2004 Apr-Jun;11(2):101-5.Daenens et al., Eur J Vasc Endovasc Surg. 2003 Mar;25(3):240-5.Toursarkissian et al., Vasc Surg. 2001 Mar-Apr;35(2):157-61.
Silver prosthesisBisdas T et al, J Vasc Surg. 2010 Aug; 52(2):323-30.Batt M et al, J Vasc Surg. 2003 Nov; 38(5):983-9.
Antibiotic prosthesisAboshady I, Raad I, Shah AS, Vela D, Dvorak T, Safi HJ, Buja LM, Khalil KG., J Vasc Surg. 2012 Sep;56(3):794-801Lew W, Moore W., Semin Vasc Surg. 2011 Dec;24(4):211-9
Arterial transplantationKieffer et al., J Vasc Surg 2004, 1009-1017Harlander-Locke et al., J Vasc Surg 2014, 669-74

Ideal Treatment:
Complete endograft excision
Extensive debridement of the arterial bed
Arterial reconstruction in a noninfected field
Infect-resistant vascular replacement
„Surgical treatment of infected descending thoracic aortic grafts is extremly
invasive and burdened with high mortality rates and usually poor conditions
of the patients.“
Experience in 26 pts./23a, mean 16 ± 18 months post implant
Patient survival 50 % @ 58±28 months
How to best treat infectious complications of open and
endovascular thoracic aortic repairs
Kahlberg et al.Sem Vasc Surg. 2017 (30):95-102

Treatment and outcomes of aortic endograft infection
Endograft infection in 206 pts., mean 22 months post implant
EVAR, n=180; TEVAR, n=26
Multicenter study
In situ replacement 90%
30-d-mortality 11 %
Patient survival 70 % @1a, 51 % @5a
Smeds MR et al.,J Vasc Surg. 2016 Feb;63(2):332-40

Treatment and outcomes of aortic endograft infection
Smeds MR et al.,J Vasc Surg. 2016 Feb;63(2):332-40
Management should be surgical
Autogeneous reconstruction (cryograft / deep femoral vein)
If it is not an option, antibiotic soaked prosthesis

Allograft replacement for infrarenal aortic graft infection: Early and late results in 179 patients (1988 – 2002)
Mean follow up 46.0 42.1 months (1 - 148 m)
111 x fresh allograft (until 1996)
68 x cryopreserved allograft
Results: 30-d-mortality 20 %
Late mortality 26 %
Rare specific complications (rupture, dilatation)
Late iliofemoral complications (63 x, most occlusive)
Complications reduced by using cryopreserved and
no thoracic aortal allografts
Kieffer et al., J Vasc Surg 2004, 1009-1017
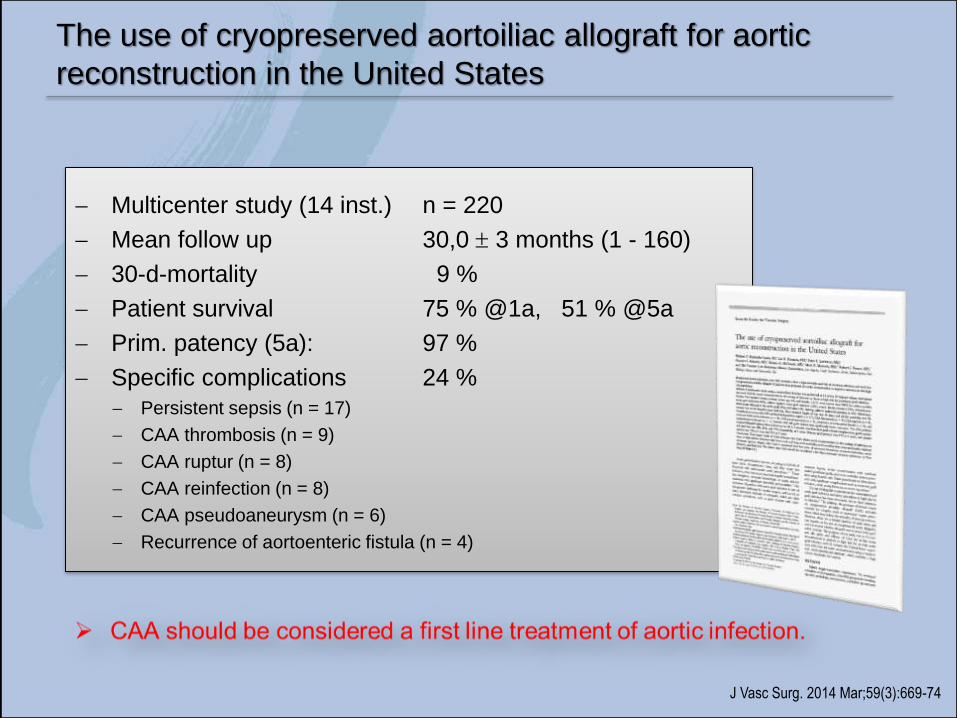
The use of cryopreserved aortoiliac allograft for aortic
reconstruction in the United States
Multicenter study (14 inst.) n = 220
Mean follow up 30,0 3 months (1 - 160)
30-d-mortality 9 %
Patient survival 75 % @1a, 51 % @5a
Prim. patency (5a): 97 %
Specific complications 24 %
Persistent sepsis (n = 17)
CAA thrombosis (n = 9)
CAA ruptur (n = 8)
CAA reinfection (n = 8)
CAA pseudoaneurysm (n = 6)
Recurrence of aortoenteric fistula (n = 4)
J Vasc Surg. 2014 Mar;59(3):669-74
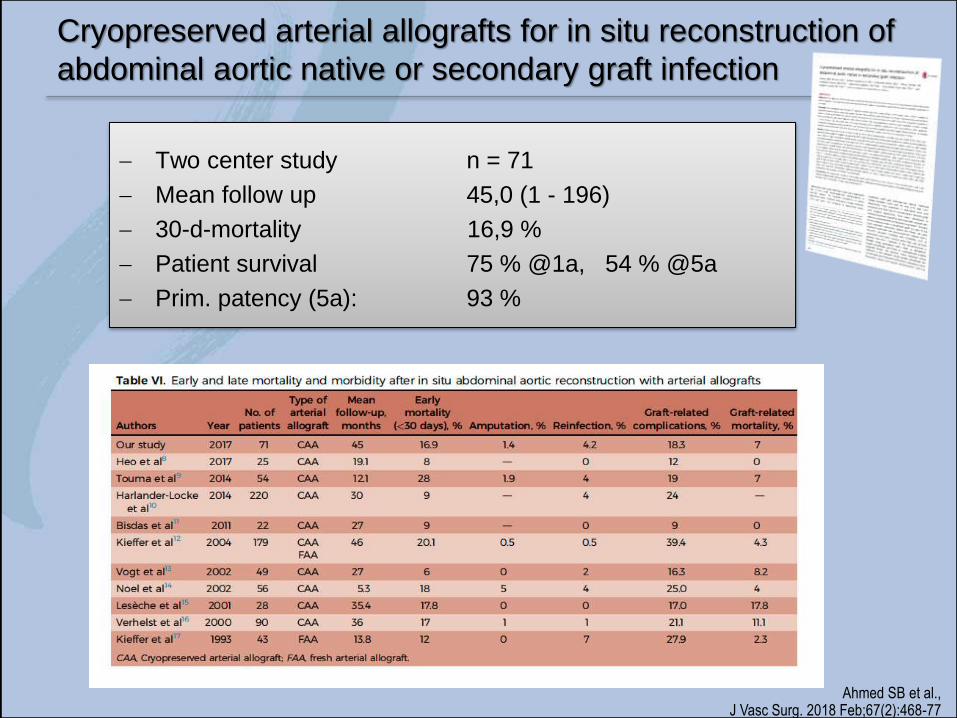
Cryopreserved arterial allografts for in situ reconstruction of
abdominal aortic native or secondary graft infection
Two center study n = 71
Mean follow up 45,0 (1 - 196)
30-d-mortality 16,9 %
Patient survival 75 % @1a, 54 % @5a
Prim. patency (5a): 93 %
Ahmed SB et al.,J Vasc Surg. 2018 Feb;67(2):468-77

Cryopreserved arterial allografts for in situ reconstruction of
abdominal aortic native or secondary graft infection
Two center study n = 71
Mean follow up 45,0 (1 - 196)
30-d-mortality 16,9 %
Patient survival 75 % @1a, 54 % @5a
Prim. patency (5a): 93 %
Ahmed SB et al.,J Vasc Surg. 2018 Feb;67(2):468-77

Own experience in arterial transplantation (n = 149 patients)
Vascular transplantation program 11/2000 – 02/2010 (University of Leipzig - UKL)
“Bridging“-OP
n = 80
Fresh homografts and immunosuppression
be terminated by „Gewebegesetz“ (7/2007 – federal law)
Vascular transplantation program 05/2010 until now(Diakonissen-Hospital Leipzig - DKL)
n = 69
Cryopreserved allografts
No immunosuppression

Aortic reconstruction
DKL
Period 05/2010 - 01/2018
Follow up 26 (0 – 89) months
Patients 43
Sex ♂ 33
♀ 10
Age 64,2 (46,5 – 83,6)
Allograft Cryopreserved
n=39 prosthetic graft
n=3 EVAR
n=1 Viabahn

Aortic reconstruction
DKL
Aortic tube 0
Aorto-biiliacal graft 4
Aorto-bifemoral graft 24
Aorto-monofemoral graft 3
Aorto-monoiliakal graft 1
Bifurcationgraft aortoiliako and aortofemoral 2
Bifurcationgraft aortofemoro and aortopopliteal 2
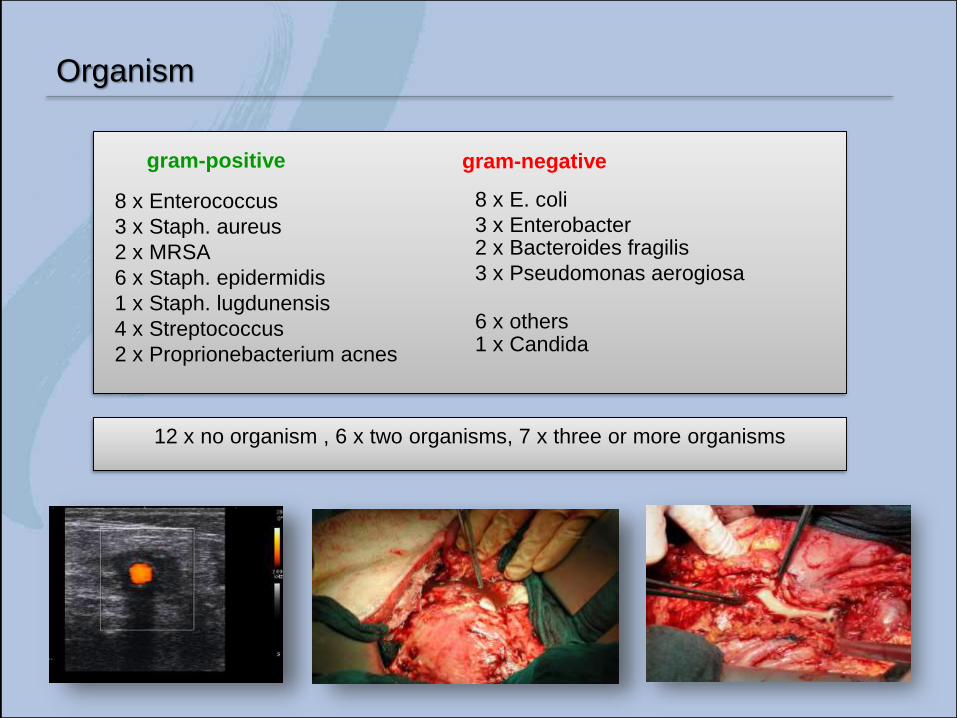
Organism
gram-positive gram-negative
8 x Enterococcus
3 x Staph. aureus
2 x MRSA
6 x Staph. epidermidis
1 x Staph. lugdunensis
4 x Streptococcus
2 x Proprionebacterium acnes
8 x E. coli
3 x Enterobacter2 x Bacteroides fragilis
3 x Pseudomonas aerogiosa
6 x others1 x Candida
12 x no organism , 6 x two organisms, 7 x three or more organisms

Gastroscopy
Gastroscopy Dr. Stephan
Dres. med. Bayer, Schmidt, Steinecke, Englisch, Neubauer, Löbe, Schneider, Häntschel, Scholle, Schäfer
by courtesy of
Results
Mortality < 30 d n = 6 (13,9 %)d - 0, 0, 1, 2, 13, 17
Mortality > 30 d n = 8 (18,6 %)

Results
Graft related complications
Bypass thrombectomy 4
Chronic bypass occlusion 0
Ureteroiliac fistula 3
Graftinfection 1
Rejection 0
Stenosis 0
Aneurysm 1
Σ complications 9 x ( 20,9 %)
Mortality < 30 d n = 6 (13,9 %)d - 0, 0, 1, 2, 13, 17
Mortality > 30 d n = 8 (18,6 %)

Results
Mortality < 30 d n = 6 (13,9 %)d - 0, 0, 1, 2, 13, 17
Mortality > 30 d n = 8 (18,6 %)
Graft related complications
Bypass thrombectomy 4
Chronic bypass occlusion 0
Ureteroiliac fistula 3
Graftinfection 1
Rejection 0
Stenosis 0
Aneurysm 1
Rupture /Bleeding 8
Σ complications 17 (39,5 %)

Patient survival
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 10 20 30 40 50 60 70 80 90
month
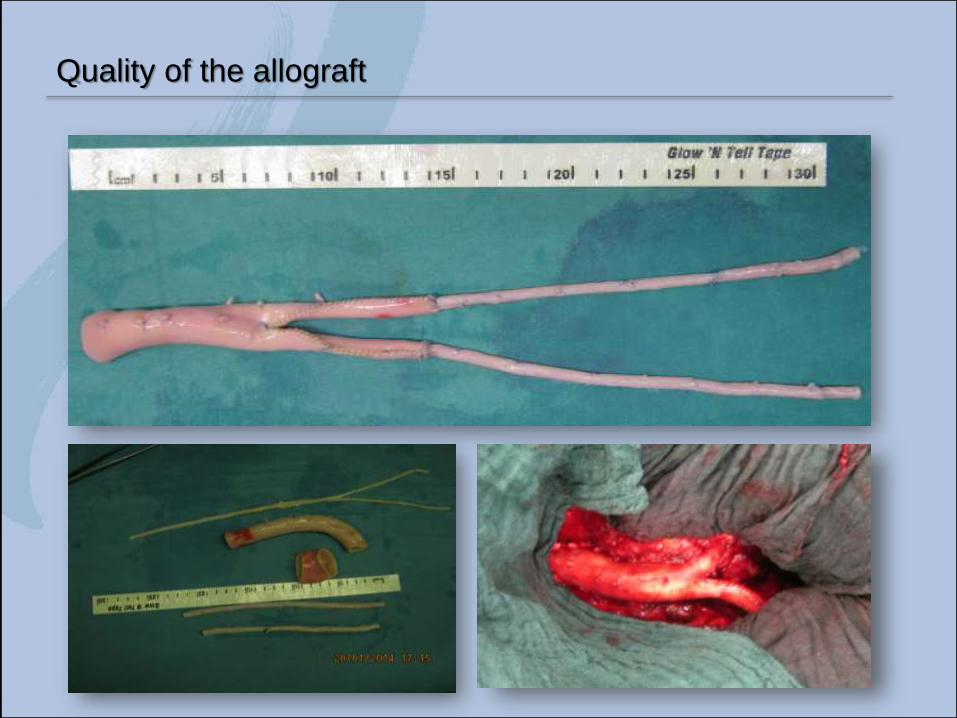
Quality of the allograft

Conclusions
Management of an infected prosthetic graft should be surgical.
Cryopreserved allografts can be used for in situ replacement.
Allograft related mortality rate is reasonable.
Graft related complications are high but were successfully treated in
each case.
Most complications in the early postop. periode (persistent infection)

Infectious complications of the aorta-
how to approach
Olaf Richter
Ev. Diakonissenkrankenhaus LeipzigDept. of Vascular Surgery
Ev. Diakonissenkrankenhaus LeipzigAkademisches Lehrkrankenhaus der Universität Leipzig
Ev. Diakonissenkrankenhaus LeipzigAkademisches Lehrkrankenhaus der Universität Leipzig
Eine Einrichtung der edia.con-Gruppe