Embed Size (px)
Citation preview
EVALUATING AND TREATING BALANCE IMPAIRMENTS IN STUDENTS WITH AUTISM SPECTRUM DISORDERSusan Ronan PT, DPT, PCS
New York Medical College
THANK YOU
Mary Paolillo PT
Giant Steps
Devereux Millwood Learning Center
Nicholas Manente PT, DPT
Lauren Perillo PT, DPT
Jovan Ramirez PT, DPT
Nicole Robell PT, DPT
Nicole Sproviero PT, DPT
Ellen Morello PT, DPT
Sara Butler PT, DPT
Carolyn Kirkup PT, DPT
DISCLOSURE
Financial: Susan Ronan receives an honorarium from Education Resources.
Non-financial: She has no relevant non-financial relationships to disclose.
Objectives
Compare the neurological differences between children with autism and those with typical development.
Apply the evidence for gross motor dysfunction to the clinical presentation of children with autism.
Identify interventions for children with autism based on the science and evidence.
TOPICS
Diagnosis
Systems Review
Neurological Evidence
Clinical Presentation
Intervention Evidence
Nutrition
What do I do tomorrow?
Conclusion
AUTISM
ASD?
TEMPLE GRANDIN
“I can remember the frustration of not being able to talk. I knew what I wanted to say, but I could not get the words out, so I would just scream.”
“A treatment method or an educational method that will work for one child may not work for another child. The one common denominator for all of the young children is that early intervention does work, and it seems to improve the prognosis.”
ASD: PREVALENCE1
Incidence: 1: 88
Boys: Girls::4:1 (1 in 54 boys)
Prevalence: 1% in Asia, Europe, and
North America "Increased Prevalence?” Increased awareness
Earlier diagnosis
Changes in diagnostic practice (screening)
ETIOLOGY
Unknown
Theories:
“Refrigerator Mother” 1970s
Infectious
Immunological deficiency
Environmental toxins
Gastric Inflammatory Disease
Genetic- multiple genetic factors
Sperm (older fathers)
AUTISM AND ASD
AUTISM 2
“A developmental disorder that appears by age three and that is variable in expression but is recognized and diagnosed by impairment of the ability to form normal social relationships, by impairment of the ability to communicate with others, and by stereotyped behavior patterns especially as exhibited by a preoccupation with repetitive activities of restricted focus rather than with flexible and imaginative ones.”
DIAGNOSIS3
Diagnostic and Statistical manual of Mental Disorders (V) (2013)
DIAGNOSTIC AND STATISTICAL MANUAL OF MENTAL DISORDERS (V)3
(A) Persistent deficits in social communication and social interaction across multiple contexts.
Including:
social-emotional reciprocity.
nonverbal communicative behaviors used for social interaction.
developing, maintaining, and understanding relationships.
DSM (V)
(B) RESTRICTED, REPETITIVE PATTERNS OF BEHAVIOR, INTERESTS, OR ACTIVITIES.
Stereotyped or repetitive motor movements, use of objects, or speech
Inflexible adherence to routines, or ritualized patterns or verbal nonverbal behavior
Highly restricted, fixated interests that are abnormal in intensity or focus interest).
Hyper- or hyporeactivity to sensory input or unusual interests in sensory aspects of the environment
DSM (V)3
C. Symptoms must be present in the early developmental period
D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay.
Questions
What are the main areas of impairment in the diagnosis of Autism?
EARLY DETECTIONWhen is the earliest time to detect autism?
WHEN CAN A DIAGNOSIS BE MADE?
“By 3 yrs.”
“As early as 18 mos.”
“12 mos.?”
“Earlier?”
PEDIATRICIANS
Pediatrician 82% routinely screening for general developmental delays, but only 8% screened for ASD.
Why? Insufficient time.
Lack of familiarity with screening tools
Reliance on referral to specialists.6
PARENTS
Early detection/ suspicion
Notice with peer interaction opportunities: Birthday part/ family event/ Play date
Medical professionals may disregard parental observations
Early detection/ suspicion
Notice with peer interaction opportunities: Birthday part/ family event/ Play date
Medical professionals may disregard parental observations
PRESENTATION
Social
Communication
Repetitive Behaviors/ play
Others
Sz (25- 33%)
Sensory- heightened sensory (smell/ taste?)
MR
PRESENTATION
Sleep difficulties
Self Injurious Behavior
Special Skills (Savant skills)
INDICATIONS7
Poor eye contact
Doesn't seem to know how to play with toys
Excessively lines up toys or other objects
Is attached to one particular toy or object
Doesn't smile
At times seems to be hearing impaired
BY 12 MOS.:
Red Flags: 10
Failure to orient to name
Lack of nonverbal showing
Lack of eye contact
Lack of initiative/ hypoactivity
Lack of emotional regulation
Poor social interaction
Orienting, smiling and vocalizing to objects.
Absolute Concern: 10
No babbling
No pointing/gesturing
Any loss of language
Any loss of social skills
SCREENING TOOLS
M-CHAT (toddlers)
Gilliam Autism Rating Scale 2 (GARS-2)
Autism Diagnostic Interview-Revised (ADI-R)
Autism Diagnostic Observation Schedule-Generic (ADOS)
Vineland Scale of Adaptive Behavior
EARLIER?
Dyadic interactions/ imitation
Emotional discrimination
Development of attachment11
Early asymmetry?12, 13
No early patterns identified14
Questions
Regarding the diagnosis of ASD
What would a parent report?
What would a teacher report?
ADDITIONAL CONSIDERATIONS
GI ISSUES
Constipation and Diarrhea, Chronic Abdominal pain15
Dysbiosis: Abnormal gastric flora
Abnormal gram-negative bacteria
Leaky Gut: increased intestinal permeability
Food Sensitivities/ Allergies15
Higher antigen specific antibodies for food proteins (IgA, IgG, IgM)
Glutens, Casein- may pass through the “leaky gut” and have neurological effects.
NUTRITIONAL DEFICIENCIES15
Omega -3 Fatty acids- lower in children with autism
Metabolism?

AUTOIMMUNITY15
Evidence for autoimmune antibodies
Cortex
Caudate nucleus (learning/ memory)
Cerebellum
Thalamic/ Hypothalamic
METABOLIC15
Impaired methylation
Increased oxidative stress
Lower antioxidants
Higher organic toxins/ heavy metals
Higher production of nitric acid (free radical)
HEAVY METAL TOXICITY15
Mercury
Thimerisol (Immunizations)
Do children with autism have an impairment in the ability to excrete mercury?
Not proved
Balance: NEUROLOGICAL EVIDENCE
NEUROANATOMICAL DIFFERENCES
Macrocephaly (first 2 years of life)
Enlarged
Frontal lobes
Amygdala (emotional learning, memory)
Cerebellar white matter
Underdevelopment
Cerebellar vermis (vestibular/ proprioception)

ASD: 3 PATHWAYS
Primary: frontal dysfunction
Second: brainstem dysfunction.
Tertiary: cerebellar dysfunction.
NEUROCHEMICAL
Alterations in16
Serotonergic (feelings of wellbeing)
Glutamatergic (cellular metabolism)
Cholinergic (PSN, SNS, Forebrain, Brainstem)
Gabaergic (inhibitory neurotransmitter)
Stress response
VISUAL SYSTEM
Normal retinal organization18
Visual Hyperacuity19*
Hypermetriopia (images reach the retina before focusing on the lens) 19
Astigmatism19
Strabismus/ optic disc Pallor19
Impaired oculomotor function19Difficulty with focusing on moving targets
Difficulty with skill acquisition
Communication
Social interaction
HYPERACUITY19
Individuals see all objects in the visual field with sharp resolution, making it difficult to focus on one.
Use of peripheral vision helps with selective attention to a visual target.
Head turn
HYPERACUSIS19
Decreased stapedial reflex
Results in:
Avoiding sounds
Covering ears
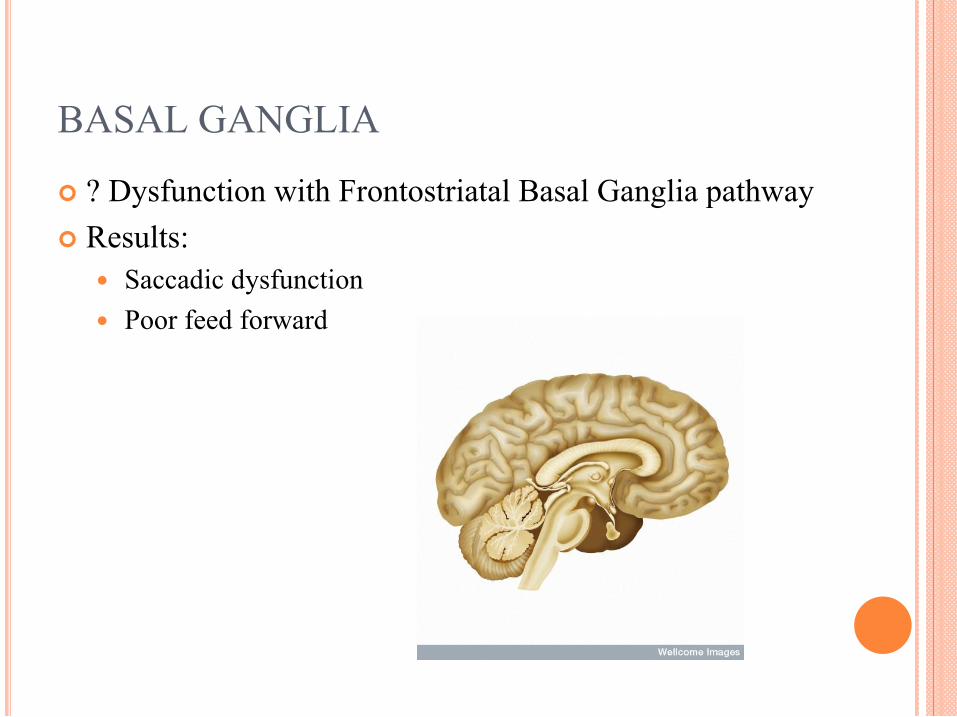
BASAL GANGLIA
? Dysfunction with Frontostriatal Basal Ganglia pathway
Results:
Saccadic dysfunction
Poor feed forward
SPECULATED LOSS OF PURKINJE CELLS
Purkinje Cells: Cortex of cerebellum
Control movement
GABA
Inhibitory- A decrease would decrease inhibition of the nerves
VESTIBULAR17
Semicircular canal deficits
Integration deficit between
Visual
Somatosensory
Vestibular system
Motor Planning20
Simple motor planning may be intact
Visual feedback, or external guidance is diminished
Difficulty with integration of visual and vestibular system
Decreases
Motor performance
Postural stability
Lack of effective sequencing
Question
What are the main motor impairments you have noticed in children with ASD?

CLINICAL PRESENTATION
POSSIBLE CLINICAL FINDINGS21
Low proximal tone
Delayed/ Poor postural reflexes
Poor integration of reflexes
Gross motor delays
Limited repertoire of play
Fine motor delays
Speech delays
POSSIBLE CLINICAL FINDINGS
Asymmetries
Difficulty crossing midline
Difficulty with visual tracking
Reliance on peripheral vision (Head posture?)
Difficulty with feed forward tasks (catching, kicking moving ball) Avoiding gaze
Echolalia
Movement Disorder
Dyspraxia
APRAXIA/ DYSPRAXIA21
Rinehart (2001): Children with autism ages 5- 19 yrs.: 22
Intact movement execution but atypical movement preparation.
Lack of anticipation
Related to motivation, and or attention?
Children with Asperger’s disorder:
Slower preparation (fronto striatal)
Oral:
Drooling
Open mouth at rest
Inability to pucker lips
Limb
Pen grasp, puzzle piece placement
ERRORS IN IMITATION23
Not related to memory or representing an action
Deficient activation of the mirror neuron cells
Deficit in mimicry
Visual attention- less attention to salient aspects of human interaction.
Difficulties perceiving biological motion.
STRENGTHS
Visual spatial perception
Better on tasks requiring acute visual perception
Visual search
SENSORY DYSFUNCTION24
Elevated sensory awareness.
Heightened sense of smell/ taste.
Gross Motor: 2 Theories25
Automatization Deficit Hypothesis:
Deficits in cerebellar function causes impairments skill learning/ and gaining automatic skills leading to poor motor and poor attention. (Visser 2003)
Disorder-Specific learning Theory:
Children who cannot cope with balance “threatening situations” (issues with motor learning and cerebellar function) develop anxiety. (Erez 2004)
Less Self Perceived Ability of Motor Performance?26
Deficits in:
Body Schema
Time/ Space awareness
Estimate Distance
Fear of intimate contact
Children with autism may view themselves as less capable than other children to perform gross motor tasks.

TYPICAL VESTIBULAR DEVELOPMENT27
Broad range of normal for children
Anatomically and functional at birth
VOR present in neonates and matures for the first 2 yrs of life.
Pursuit/ Optokinetic: 3-6 mos of age.
Same as an adult by 3-6 yrs of age.
VESTIBULAR SYSTEM28
Children with high functioning autism- normal post rotatory nystagmus in upright and with head tilt.
VESTIBULAR29
Vestibular processing is different for children with autism.
MOTOR STEREOTYPIES AND BALANCE
Suggestions that children with more severe motor stereotypies have worse balance.
Tested statically
? Dynamically
Radnovich KJ, Fournier KA, Hass CJ. (2013) Relationship between postural control and restricted, repetitive behaviors in autism spectrum disorders. Frontiers in Integrative Neuroscience. May, 7(28) pp 1-7.
BALANCE
Abnormal Proprioception.30,17
More difficulty with balance with eyes closed.17
Reliance on visual cues to reduce sway and maintain balance.17
Poor integration of visual, vestibular and somatosensory input for balance.17
GAIT
“Gait in children with autism: consistent with Cerebellar ataxia, difficulty walking on a line, variability in stride length and velocity, postural abnormalities in the head, trunk involvement in the fronto-striatial basal ganglia circuit.”31
GAIT CONTINUED
Increased stride length variability
No improvements with external cues (visual markers)
? Difficulty using environmental cues to modify movement once in action
Arm and head/ trunk posture asymmetries
TOE WALKING21
? Maybe
Related to: proprioception, kinesthesia, weight line shifted anterior in ambulation, difficulty with moving backward/ posterior in space.
INTERVENTION EVIDENCE
Supply and Demand of State EI programs (Respondents: 47 states, 4 territories)32
Services most used by children with ASD
Speech, OT
ABA
Psych/ Special Education
PT? not mentioned in study
Recommended Services: 25 or more services hrs./ week (National Research Council)
State EI: providing 5 hrs. (more than 1/ 2 states, with 4 statesproviding 20 hrs./ week)
Conclusion: EI does not have the resources for the increased demand
THE SEARCH
Physical Therapy, Physiotherapy, Gross Motor Skill, Gait, Balance, Vestibular System, SI, Autism, ASD, Asperger's, PDD, Motor Milestones, Developmental Reflexes, Gross Motor Function, Posture, Skill Acquisition.
SCOPUS, PEDro, CINAHL, OVID, Psych Info, PubMed, Specific Journals
Issues with Evidence- just to start
Lack of RCT
Small Sample sizes
Anecdotal
Non systematic
Did not quantify
Use of parental surveys
Use of child surveys
Heterogeneous population
Huge variety in function
Concurrent therapies/ treatments/ medications
Sackett’s Levels of Evidence33
1A = Systematic Review of Randomized
Controlled Trials (RCTs)
1B = RCTs with Narrow Confidence Interval
1C = All or None Case Series
2A = Systematic Review Cohort Studies
2B = Cohort Study/Low Quality RCT
2C = Outcomes Research
3A = Systematic Review of Case-Controlled
Studies
3B = Case-controlled Study
4 = Case Series, Poor Cohort Case Controlled
5 = Expert Opinion
Sensory Integration
Auditory Integration Training (AIT)
NDT
Vestibular Therapy
Brain Gym
Floor Time
Craniosacral
Greenspan
Brushing
Aquatic Therapy
“Traditional Therapy”
Massage
Interventions for Gross Motor Skills; WHERE IS THE EVIDENCE?
Sensory Integration
Most commonly used approach for individuals with autism34
Dr. Jean Ayres: Focus on processing of sensory information and the skill attainment. Hierarchical structure to development
Child centered approach
Just right challenge
Focus: Modulation
Integration

Sensory Integration:35
Meta Analysis
SI is as good as other therapies
May effect psychoeducational and motor skills
Ayers 1980:
Outcomes better for those with hyper sensory issues
Problems with literature:
Small sample size
Hard to differentiate effect of SI vs. other interventions
Characteristics of subjects heterogeneous and highly variable
Systematic approach
Anecdotal
Auditory Integration Training
Using headphones with music selected for different frequencies to improve attention, reticular activating and cerebellar performance.
Evidence:
Mixed findings
Weighted Vests36
Lack of well constructed studies
Treadmill training37
Article: Pitetti K, et al (2007) The Efficacy of a 9-Month Treadmill Walking Program on the Exercise Capacity and Weight Reduction for Adolescents with Severe Autism. Journal of Autism & Developmental Disorders, Jul, Vol. 37 Issue 6, p997-1006
Decreased BMI
Increased Exercise Capacity
Increased ability to walk on TM at a faster speed
AQUATIC THERAPY38
Benefits for children with Autism
Improved strength/ balance
Increased social participation
Vestibular stimulation
No studies
Massage
Calming effect
Improved responsiveness
Improved communication
Massage: Improves behavior/?Self regulation
Grandin’s Hug Machine
Decreased anxiety
Problems with literature:
Small sample size
NUTRITION: Socialization and language
NUTRITION15
Gluten/ Casein free diet (avoid for 60 days)
Changes in GI
Language
Socialization
SUPPLEMENTS15
Omega-3 Fatty Acids Improvements in reading
Probiotics Temporary results in GI (need more info)
Zinc ? Need more studies
Vitamin B6- ?
Multivitamin-?
OTHER INTERVENTIONS
Medications
Devices/ Orthotics/ Modifications:
Compression/ Weighted Vest
Foot orthotics
Communication Board/ Sign Language
“Wiggle seat”
THE CHALLENGE IN INTERVENTION:
Spectrum of abilities
Difficult to study because of a lack of homogeneity
No one intervention has been shown to be beneficial to balance
Studies tend to focus on children with higher functioning autism
WHAT DO I DO TOMORROW?
Learning strategies for children with autism39,40,41
Children with ASD: Focus on specific items in memory tasks rather than relational
processing or seeing the whole task.
Implicit learning is intact?
Children with Asperger's: Social Learning: SODA:
S: Stop; Where do I go to observe?
O: Observe; What is ___ doing?
D: Deliberate; What would I like to do?
A: Act; When I go to __ I plan
Plan/ Do/ Check/ Evaluate approach may be helpful with children who can participate
Sequencing, execution, using picture cards/ photos
CLINICAL QUESTION?
Do children with ASD have more difficulty with static or dynamic balance?
Suggestions from the evidence
Evaluate Eye tracking/ VOR
Functional use of vision
Test static vs. dynamic balance
Role of vision in balance
Vestibular/ Cerebellar training
Proprioceptive feedback
Feed forward activities (kicking a moving ball)
Sequencing activities
Bilateral integration
Proprioceptive/ Kinesthetic activities
Suggestions from the evidence
Aquatic Therapy
Increase self efficacy: gross motor tasks
Decrease fear of balance activities/ motor tasks
PILOT PROJECT
11 males: 9 - 20 years old
One subject excluded (n = 10)
Paraprofessional(s) were present
OTHER ASSESSMENTS
Romberg testing (tandem/ sharpened)
P-CTSIB
Eyes open
Eyes closed
Eyes open on foam pad
Eyes closed on foam pad.
BOTMP-2
Pediatric Balance Scale
Dynamic Gait Index
KEY FUNCTIONAL TASKS
Standing on one foot
Alternate step tapping
Turning to look over shoulder
What are you having success with?
CASE
GREG
Greg is 11 years old. He is receiving related services in 5th grade.
Greg is unable to stand still and will shift his weight back and forth whenever he is in standing. He requires a handrail to walk up and down stairs. He frequently miss steps when walking up or down a curb. He requires extra time to go up and down the steps of the bus.
Greg’s weight is shifted to the right in sitting and he has difficulty maintaining a midline position.
Greg frequently becomes distressed during the day and has a one on one para with him to assist with transitions and school activities.
CASE QUESTIONS
Evaluation:
What balance testing would be appropriate for Greg?
What kinds of functional activities would help to assess balance?
Intervention:
What approaches may be the most effective in working with Greg?
Case examples and problem solving
Psychosocial/ Environmental affordances and barriers
Systems review
Body structures/ functions
Strengths/ impairments
Activity
Participation
Coordination/ communication with others?
STG/ LTG
Create a treatment plan
Classroom instruction/ involvement
CONCLUSION
Team intervention is critical.
Each child and family must be approached on an individual basis.
Neuroanatomical/ functional differences in children with ASD may help guide intervention.
Functional assessment of balance may provide useful information
Consider dynamic vs. static control
THANK YOU!
Questions/ Comments?
REFERENCES
1. Kogen et al.(2007) Prevalence of Parent- Reported diagnosis of ASD Among Children in the US. Pediatrics 1124(4), 1-9.
2. Merriam-Webster (2013) Accessed September 27, 2013: http://www.merriam-webster.com/medical/autism.
3. Autism Speaks. DSM V Diagnostic Criteria: http://www.autismspeaks.org/what-autism/diagnosis/dsm-5-diagnostic-criteria accessed on 9/27/13
4. NIH: Rett’s Syndrome. Retrieved October 19, 2010. http://www.ninds.nih.gov/disorders/rett/detail_rett.htm
5. Mayo Clinic. (2010) Childhood disintegrative disorder. Retrieved October 19, 2010. http://www.mayoclinic.com/health/childhood-disintegrative-disorder/DS00801
6. Dosreis S, Weiner C, Johnson L, Newschaffer C. (2006) Autism spectrum disorder screening and management practices among general pediatric providers. Journal of Developmental and Behavioral Pediatrics, 27: 88-94.
7. NIH: ASD. 2010. Retrieved October 16, 2010. http://www.nimh.nih.gov/health/publications/autism/what-are-the-autism-spectrum-disorders.shtml
8. http://www.firstsigns.org/index.html. Retrieved October 10, 2010.
9. Robins et al. (2001) The MCHAT for Autism in Toddlers: An initial Study Investigating the Early detection of Autism and Pervasive Developmental Disorders. Journal of Autism and Developmental Disorder. 31(2); 131-144.
10. Nadel A, Poss J. (2007) Early detection of autism spectrum disorders: screening between 12 and 24 months of age. American Academy of Nurse Practitioners 19, 408-417.
11. Sigman M, Dijamco A, Gratier M, Rozga A. “Early Detection of Core deficits in Autism.” 2004. Mental Retardation and Developmental Disabilities Research Reviews 10: 221-233
12. Teitelbaum P, Teitelbaum O, Nye J, Fryman J, Maurer. (1998) Movement Analysis in infancy may be useful for early diagnosis. Proc. Ntl. Acad.Sci.USA 95: 13982-13987.
13. Esposito G, Venuti P, Maestro S, Muratori F. (2009) An exploration of symmetry in early autism spectrum disorders: Analysis of lying. Brain and Development31, 131-138.
14. Ozonoff S, Young G, Goldring S, Greiss-Hess L, Herrera A, Steele J, Macari S, Hepburn S, Rogers S. (2008) Gross Motor Development, Movement Abnormalities and Early Identification of Autism. Journal of Autism & Developmental Disorders. Vol. 38 Issue 4, 644-656.
15. Weber W. (2007) Complimentary and Alternative Medical Therapies for Attention-Deficit/ Hyperactivity Disorder and Autism. Pediatric Clinics of North America 54: 983-1006.
16. Anderson G. (2008) The Potential Role for Emergence in Autism. Autism Research 1: 18-30.
17. Molloy C, Dietrich K, Bhattacharya A. (2003) Postural Stability in Children with Autism Spectrum Disorder. Journal of Autism & Developmental Disorders. Dec, 33(6), 643-652.
18. Hadjikhani N, Chabris C, Joseph R, Clark J, Mc Grath L, Aharon I, Feczko E, Tager-Flusberg H, Harris G. (2001) Early visual cortex organization in autism: an fMRI study. Neurology Report 15(2): 267-270.
19. Gerrard S, Gordon R. (2009) Sensory Impairments and Autism: a Re-Examination of causal Modeling. Journal of Autism and Developmental Disorders. 39: 1449-1463
20. Baranek G. (2002) Efficacy of Sensory and Motor Interventions for Children with Autism. Journal of Autism and Developmental Disorders 32(5) 397- 422.
21. Ming X, Brimacombe M, Wagner G. (2007) Prevalence of Motor Development in ASD. Brain & Development.29; 565–570.
22. Rinehart N, Bradshaw J, Brereton A, Tonge B. (2001) Movement preparation in high- functioning autism and Asperger disorder: A serial choice reaction time task involving motor reprogramming. Journal of Autism and Developmental Disorders 31: 79-88.
23. Rogers S. (2007) Nature of motor imitation problems in school-aged males with autism. Developmental Medicine and Child Neurology 49: 5-5.
24. Rogers S, Hepburn S, Wehner. (2003) Parent Reports of Sensory Symptoms in Toddlers with Autism and Those with Other Developmental Disorders. Journal of Autism and Developmental Disorders. 33 (6); 631- 642.
25. Erez O, Gordon C, Sever J, Sadeh A, Mintz M. (2004) Balance dysfunction in child-hood anxiety: findings and theoretical approach. Journal of Anxiety Disorders; 18 341-356.
26. Eyck C, Bosscher R, Beek P, Doreleijers T. (2009) Gross motor performance and self-perceived motor competence in children with emotional, behavioral, and pervasive developmental disorder: a review. Developmental Medicine and Child Neurology. 51: 501-517.
27. Fife T, Tusa R, Furman J, Zee D, Frohman E, Baloh R, Hain T, Goebel J, Demer J, Eviatiar L. (2000) Assessment: Vestibular testing, techniques in adults and children. Neurology 55: 1431- 1441.
28. Goldberg M, Landa R, Lasker, A, Cooper L, Zee D. (2000) Evidence of Normal Cerebellar Control of Vestibulo-Ocular Reflex (VOR) in Children with High Functioning Autism. Journal of Autism and Developmental Disorders. 30(6) 519-524.
29. Kern J, Garver C, Grannemann B, Trivedi M, Carmody T, Andrews A, Mehta J. (2007) Response to Vestibular Sensory Events in Autism. Research in Autism Spectrum Disorders. 1 (1) 67-74.
30. Weimer A, Schatz A, Lincoln A, Ballantyne A, Trauner D. (2001) Motor impairment in Asperger Syndrome: evidence for a deficit in proprioception. Journal of Developmental and Behavioral Pediatrics. 22; 92-101.
31. Rhinehart N, Tonge B, Iansek R, et al. (2004) Gait function in newly diagnosed children wit autism: cerebellar and basal ganglia related motor disorder. Developmental Medicine and Child Neurology 48:819-24.
32. Wise M, Little A, Holliman J, Wise P, Wang J. (2010) Can State Early Intervention Programs Meet the Increased Demand of Children Suspected of having Autism Spectrum Disorders?” Journal of Developmental Behavior Pediatrics 31(6); 469- 472.
33. Sackett DL, Strauss SE, Richardson WS, et al. (2000) Evidence-Based Medicine: How to Practice and Teach EBM. Philadelphia, Pa: Churchill-Livingstone.
34. Hess K, Morrier M, Heflin LJ, Ivey M. (2008) Autism Treatment Survey: Services Received by Children with Autism Spectrum Disorders in the Public School System. Journal of Autism & Developmental Disorders, May, Vol. 38 Issue 5, p961-971
35. Vargas S, Camilli G. (1999) A meta-analysis of research on sensory integration treatment. American Journal of Occupational Therapy. 53(2): 189-198.
36. Stephenson J, Carter M. (2009) The Use of Weighted Vests with Children with Autism Spectrum Disorders and Other Disabilities. Journal of Autism & Developmental Disorders, Jan, Vol. 39 Issue 1, p105-114.
37. Pitetti K, Rendoff A, Grover T, Beets M. (2007)The Efficacy of a 9-Month Treadmill Walking Program on the Exercise Capacity and Weight Reduction for Adolescents with Severe Autism. Journal of Autism & Developmental Disorders, Vol. 37 Issue 6, p997-1006
38. Vonder Hulls D, Walker L, Powell J. (2006) Clinicians’Perceptions of the Benefits of Aquatic Therapy for young children with Autism: A Preliminary Study. Physical and Occupational Therapy in Pediatrics. 26(1/2) 13-22.
39. Bowler D, Motton L. (2009) Different Verbal Learning Strategies in Autism Spectrum Disorder: Evidence form the Rey Auditory Verbal Learning Test. Journal of Autism and Developmental Disorder. 39 : 910- 915.
40. Brown J, Aczel B, Jimenez L, Kaufman S, Grant K. (2010) Intact Implicit learning in Autism Spectrum Conditions. Quarterly Journal of Experimental Psychology. 63 (9), pp. 1789-1812
41. Bock M. (2007) The Impact of Social-Behavioral Learning Strategy Training on the Social Interaction Skills of Four Students with Asperger Syndrome. Focus on Autism and Other Developmental Disabilities. 22(2); 88-95.
42. Radnovich KJ, Fournier KA, Hass CJ. (2013) Relationship between postural control and restricted, repetitive behaviors in autism spectrum disorders. Frontiers in Integrative Neuroscience. May, 7(28) pp 1-7.
![journalofethics.ama-assn.org · as their more well-known Olympic counterpart [3]. The ethics of treating patients with a variety of physical impairments and disabilities is as complex](https://img.pdfslide.net/doc/110x75/5fa11d276b37d4615f46a9e1/as-their-more-well-known-olympic-counterpart-3-the-ethics-of-treating-patients.jpg)




























