Embed Size (px)
Citation preview

Evaluating Use of and Application of MDDR Service by
U.S. TB Control Programs
Allison McAlister, MPH Microbiologist
DTBE Brown Bag
April 3, 2014
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination

BACKGROUND
Molecular Detection of Drug Resistance (MDDR) Service

MDDR Service
Began offering the service in September 2009 Provides rapid drug susceptibility results
Utilizes DNA sequencing to detect mutations associated with drug resistance
Turn around time ~1-2 days
From September 2009 to December 2014, 2,162 samples (isolates and clinical specimens) have been received.
Samples submitted from states and U.S. territories

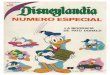
MDDR submissions by year
41
215
322
454
575 555
314
0
100
200
300
400
500
600
700
2009* 2010 2011 2012 2013 2014 2015**
*September-December only **January-May only; preliminary data only, may include duplicate patient samples

MDDR Workflow
Pre-
Analyt ic
• MDDR pre-submission request form is submitted by program or PHL • Approval provided and sample submitted by PHL • Reason for submission determines type of testing to be done
Analyt ic
• Sanger sequecing • Pyrosequencing • Growth-based DST (Agar Proportion Method and MGIT PZA Testing
Post-
Analyt ic
• Interim Report with molecular results is faxed to submitting PHL • Final report with growth-based DST results are sent when available

PURPOSE AND OBJECTIVES
Evaluating the MDDR Service

MDDR Evaluation Plan
Evaluate the service from a laboratory perspective Completed by Mitch Yakrus in 2013 Included quantitative analysis to measure discordance among the
molecular and phenotypic DST results.
Evaluate the service from a programmatic perspective Completed in January 2014
Evaluate the service from a clinical perspective Ivy Oyegun -In progress

Purpose and Objectives
• Determine the impact of the MDDR service on TB Control Programs
• Gain a better understanding of how TB controllers communicate with public health laboratories, how satisfied the programs are with the service, and the complexities with receiving and interpreting molecular drug susceptibility results.

STUDY DESIGN
Evaluating the MDDR Service from a Programmatic Perspective

Evaluation Approach
Investigate pre-analytical components Who is involved in the decision to make a request How are TB Programs involved in the sample referral process Are there factors that delay a request or submission
Investigate post-analytical components Who reviews the results How are the results interpreted Do programs compare molecular and growth-based results How are the results used Do the results impact the work of the TB control program

Study Population
TB Controllers in 60 U.S. health department jurisdictions that receive award through Cooperative Agreements 50 states 9 major U.S. cities (New York City, Los Angeles, San Diego, San
Francisco, Houston, Philadelphia, Chicago, Baltimore, Detroit) District of Columbia Who are the TB Controllers?
• Program Managers, Program officers, Division Directors, Branch Chiefs, State Epidemiologists, TB Coordinators, Nurse Consultants, others
http://intranet.cdc.gov/nchhstp/dtbe/directories/controlofficers.asp

Data Collection Instrument
Adobe Forms Central Easy to create PDF and web forms Easy to distribute-provides a hyperlink that can be embedded in
website or sent via email Data is automatically compiled in tables Sort and filter tables in real-time Automatically creates charts of your data Allows for skip logics
https://www.acrobat.com/formscentral/en/home.html

Approval Process
Non-human subjects research determination IRB exemption from the USF IRB board Paper Reduction Act (PRA) determination Office of Management and Budget (OMB) approval

RESULTS

Response Rate
Received 37 responses Excluded responses from four Microbiologists The final response rate was 54% (33/60)

Initiation of Requests

Initiation of Requests

Sample Referral Process
3%
0
3%
79%
3%
12%
Other. Please explain.
Not applicable.
Program consults with HCP then submitsrequest form
Program consults with PHL and labsends form
Program consults with PHL beforesubmitting the request form.
Program sends request form thencontacts PHLProgram sends form then contacts PHL
Program consults with PHL before submitting the request form
Program consults with PHL and lab sends form Program consults with HCP then submits request form Not Applicable. Program not involved in sample referral process.
Other.
If your TB program is involved in the process for submitt ing MDDR requests, what is the program’s role?

Sample Referral Process and Pre-submission Criteria

Sample Referral Process and Pre-submission Criteria

Delays in submission

Requests to Confirm In-house Molecular Assays
45% (15/33) have initiated a request to confirm results from another molecular assay 7 to confirm Cepheid Xpert MTB/RIF assay (Xpert) results 3 to confirm their own sequencing results 1 to confirm Xpert and Pyrosequencing results 4 to confirm unspecified molecular assay

Requests to Confirm In-house Molecular Assays

Comparison of molecular and growth-based DST results

Delivery of Molecular Results
70% (23/33) received the MDDR report from the PHL 21 within 1 business day 1 between 2-3 business days One Comment: They are not able to read the report form once it is faxed from CDC to local public health laboratory and then to the program. They would prefer CDC to send the report directly to the program.

The Interim Report
Result Interpretation (based on in-house evaluation of 550 clinical isolates)
No Mutation Probably Rifampin susceptible. (97% of RMP-R isolates in our in-house evaluation of 550 clinical isolates have a mutation at this locus.)
Mutation: TCGTTG; Ser531Leu
Rifampin resistant. (100% of isolates in our in-house evaluation of 550 clinical isolates with this mutation are RMP-R.)
Mutation: CTGCCG; Leu511Pro
Low-level but probably clinically relevant rifampin resistance has been linked to the Leu511Pro mutation detected in the rpoB locus; isolates with this mutation may test as susceptible by conventional techniques.
Silent Mutation: TTCTTT; Phe514Phe
The mutation detected is a synonymous (silent) single-nucleotide polymorphism (SNP) and does not result in an amino acid change and is not considered clinically significant.

Evaluation of Satisfaction With the Interim Report
Statement Percent Agreement
The format of the interim report is easy to interpret. 82%
The interim report does not provide enough information.
15%
The inclusion of the nucleot ide change is necessary for interpretat ion of the results.
36%
The inclusion of the amino acid change is necessary for interpretat ion of the results.
40%
The interpretat ion provided on the interim report is helpful for understanding the results.
79%
The interpretat ion provided on the interim report is difficult to understand.
27%
Further interpret ive comments are needed for less common mutat ions.
62%

Seeking help for interpreting MDDR results

Reporting Results to Healthcare Providers
91% consult with the health care provider most of the time and 3% only when contacted Of these,
• 93% agree that they are comfortable discussing the molecular results with healthcare providers
• 6% agree with having difficulty discussing molecular results with healthcare providers.
6% do not usually consult with health care providers.

Usability Of MDDR Results
Statement Percent Agreement
The program is confident about treatment decisions for TB case based primarily on molecular results. 76%
The program advises wait ing for growth-based DST results before making treatment decisions for TB cases.
15%
MDDR results have been useful in decision making with high profile situat ions, such as daycare facility, nursing home, correct ions facility, healthcare sett ing, or homeless shelters.
81%

MDDR and Treatment of Contacts to TB Case
Statement Percent Agreement
MDDR molecular results are useful when deciding how to treat contacts to a MDR-TB case. 94%
MDDR molecular results are useful when deciding how to treat contacts of drug-suscept ible TB case. 58%
DST results are essent ial for guiding treatment of contacts.
70%

MDDR Satisfaction
Statement Percent Agreement
I am sat isfied with turnaround t imes of molecular results. 94%
I am sat isfied with turnaround t imes of growth-based DST results. 61%
I am sat isfied with the test panel for second line drugs. 76%
I have found DTBE Laboratory Branch to be available when needed for consultat ion.
88%
I have found the information on CDC website to be useful. 58% I would like more training opportunit ies to better understand molecular results. 85%

CONCLUSIONS AND RECOMMENDATIONS

Conclusions
Overall, most were satisfied with the MDDR service. We received many positive comments about the service. We gained some insight about the program’s role in
requesting MDDR, the process, how many program’s receive the results and how they interpret and use the results.

What We Know
A need still exists for standardized reporting and clear interpretations, especially for less common mutations.
A need for educational opportunities or materials to ensure there is understanding of results and interpretations among laboratorians, TB controllers, consultants and healthcare providers.

What We Will Do
Continue to provide resources and training opportunities. Continue to work with APHL and other partners to develop
standardized reporting language Continue to evaluate our service and look for ways to
improve

Comments or Suggestions?

Acknowledgements
Angela Starks Mitch Yakrus
Awal Khan Dawn Tuckey
Beverly Metchock

Thank you. Any Questions?
For more information please contact Centers for Disease Control and Prevention 1600 Clifton Road NE, Atlanta, GA 30333 Telephone: 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348 Visit: www.cdc.gov | Contact CDC at: 1-800-CDC-INFO or www.cdc.gov/info The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of TB Elimination