Embed Size (px)
Citation preview

Ultrasound in Med. & Biol., Vol. 36, No. 10, pp. 1756–1761, 2010Copyright � 2010 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/$ - see front matter
asmedbio.2010.05.013
doi:10.1016/j.ultrd Clinical Note
EVALUATION OF CORONARY FLOW VELOCITY RESERVE IN HOMOZYGOUSFAMILIAL HYPERCHOLESTEROLEMIA BY TRANSTHORACIC DOPPLERECHOCARDIOGRAPHY AND DUAL-SOURCE COMPUTED TOMOGRAPHY
YA YANG,* XIAOSHAN ZHANG,* RONGJUAN LI,* HONGYAN REN,* ZHENG WANG,* ZHIAN LI,* JIE LIN,y
LUYA WANG,y WEI YU,z and ZHAOQI ZHANGz
*Department of Ultrasound, Beijing Anzhen Hospital, Capital Medical University, Beijing, P. R. China; yBeijing Instituteof Heart Lung and Blood Vessel Diseases, Beijing, P. R.China; and zDepartment of Radiology, Beijing Anzhen Hospital,
Capital Medical University, Beijing, P. R. China
(Received 15 October 2009; revised 8 May 2010; in final form 14 May 2010)
Asound100029
Abstract—Homozygous familial hypercholesterolemia (HoFH) is a rare disorder characterized by the early onsetof atherosclerosis and usually occurs at the ostia of coronary arteries. In this study, we used transthoracic Dopplerechocardiography (TTDE) to evaluate the dynamic changes of coronary flow in HoFH patients and to detect aorticand coronary atherosclerosis by dual-source computed tomography (DSCT). We studied 20 HoFH patients(12 females, 8 males, mean age 13.1 ± 5.3 years, with a mean low density lipoprotein (LDL) cholesterol of 583 ±113 mg/dL) and 15 control patients (8 females, 7 males, mean age 15.2 ± 6.9 years, with a mean LDL cholesterol128 ± 71 mg/dL) using TTDE and DSCT. None of the patients showed evidence of ischemia with standard exercisetesting. Though the baseline coronary flow was similar between HoFH patients and normal controls, the hyperemicflow velocities and, thus, the coronary flow velocity reserve (CFVR) were significantly lower in those with HoFH. AllHoFH patients had aortic plaques, nine of them with the coronary artery ostia simultaneously, who had significantlyhigher LDL-cholesterol and lower CFVR than those without ostia plaques. Our data demonstrated that TTDEtogether with DSCT could be a useful noninvasive method for detection of coronary flow dynamics and atheroscle-rosis specifically in HoFH subjects with coronary ostia. (E-mail: [email protected]) � 2010 WorldFederation for Ultrasound in Medicine & Biology.
Key Words: Homozygous familial hypercholesterolemia, Coronary blood flow velocity reserve, TransthoracicDoppler echocardiography, Dual-source computed tomography.
INTRODUCTION
Familial hypercholesterolemia (FH) is a monogenic
disorder due to a mutation in the low density lipoprotein
receptor (LDL-R) gene (Kraft et al. 2000; Marais 2004).
It has been estimated to have a prevalence of 1/500
for the heterozygous form (HeHF) and, therefore,
a prevalence of about 1/1,000,000 for the homozygous
form (HoHF) (Marais 2004; Santos et al. 2008; Awan
et al. 2008). Individuals with this mutation have high
levels of low density lipoprotein (LDL) cholesterol in
plasma starting in childhood, early atherosclerosis and
a high incidence of coronary artery disease (Wiegman
et al. 2003; Civeira et al. 2005). Since atherosclerosis often
ddress correspondence to: Zhian Li, M.D., Department of Ultra-Beijing, Anzhen Hospital, Capital Medical University, Beijing,
P. R. China. E-mail: [email protected]
1756
happens at the ostia of coronary arteries, if untreated, the
prognosis is poor due to sudden death, which is oftscribed
to acute myocardial infarction before age 30.
Hypercholesterolemia is a major risk factor for coro-
nary artery disease. Deterioration of left ventricular (LV)
function has mainly been attributed to coronary insuffi-
ciency secondary to formation of atherosclerotic lesions
in epicardial coronary arteries that reduce blood flow at
rest or in response to increased demands. Hypercholester-
olemia also reduces coronary flow reserve and induces
microvascular dysfunction that may contribute to my-
ocardial ischemia and LV dysfunction. Patients with
syndrome X have myocardial ischemia without stegnotic
coronary artery lesions based on microvascular endothe-
lial dysfunction.
The objective of this study was to measure coronary
flow velocity reserve (CFVR) of HoFH patients by TTDE
and combine dual-source computed tomography (DSCT)
to evaluate the changes of coronary flow dynamics.

Evaluation of coronary flow velocity reserve d Y. YANG et al. 1757
MATERIALS AND METHOD
Study subjectsTwenty patients with HoFH but no history of ischemic
heart disease (8 men and 12 women; mean age 13.1 6 5.36
years) and 15 control subjects (7 men and 8 women; age
15.2 6 6.91 years) were studied. HoFH was diagnosed ac-
cording to the following criteria: (1) plasma cholesterol
concentration above 600 mg/dL or LDL cholesterol concen-
tration above 500 mg/dL; (2) occurrence of tendon xan-
thoma before age 20; and (3) having both parents who
were heterozygous familial hypercholesterolemia (Santos
et al. 2008; Faccenda et al. 1990). All patients satisfied
the aforementioned three criteria. Fifteen asymptomatic
subjects with normo-lipidemia, normo-glycemia, also the
siblings of HoFH patients, were selected as the control
group. Exclusion criteria were LV wall-motion abnor-
mality, previous myocardial infarction, LV hypertrophy,
previous cardiac surgery, atrial fibrillation, significant
valvular heart disease and unstable angina. All the study
subjects were prohibited to consume tea, coffee and other
caffeinated beverages during adenosine stress echocardi-
ography 12 hours prior to the study. The study was
approved by the Institutional Review Board of our institu-
tion and all study subjects gave informed consent prior to
the study. If the patients were children, appropriate parent or
guardian signatures were obtained on the informed
consents.
Dual-source computed tomographyAll of computed tomography (CT) scans were per-
formed on a DSCT (SOMATOM Definition; Siemens
Medical Solutions, Forchheim, Germany). The detector
collimation was 2 3 32 3 0.6 mm and acquisition colli-
mation was 2 3 32 3 0.6 mm by means of z-flying focal
spot. Gantry rotation time was 330 ms and pitch was 0.3–
0.45 adapted to heart rate (HR). DSCT angiography was
acquired using a retrospective gating with tube current
modulation scan protocol in the craniocaudal direction.
Full tube current was given during 30%–80% R-R
window. Bolus tracking was performed with a region-
of-interest placed in the root of ascending aorta and image
acquisition was automatically started 6 s after the signal
attenuation reached the predefined threshold of 100 HU.
The scanning range extended from the tracheal bifurcation
to just below the diaphragm.
The contrast medium injection used an 18-gauge
intravenous needle through right antecubital vein and
a dual-head power injector (Stellant D; Medrad, Indianola,
PA, USA). A two-phase protocol was used as a contrast
medium injection. According to scan time 50–70 mL,
contrast medium (Ultravist, 370 mgI/mL iopromide;
Bayer, Wayne, NJ, USA) was injected, followed by
30 mL saline (0.9% sodium chloride) as bolus chaser.
The injection rate for all phases was 4–4.5 mL/s.
The coronary tree was divided into segments accord-
ing to the modified American Heart Association classifica-
tion: left main and proximal mid and distal segments of the
left anterior descending artery, left circumflex, first and
second marginal branches and right coronary artery.
Transthoracic Doppler echocardiographyEchocardiographic examinations were performed
with a General Electronics Medical System (Vivid 7
dimension digital ultrasound system; General Electronics
Medical System, Waukesha, WI) with a harmonic probe at
a frequency of 4 MHz. Patients were examined in the left
lateral position using a modified left parasternal window.
Echocardiographic images were obtained from the
acoustic window around the midclavicular line in the
fourth and fifth intercostal spaces. After the lower portion
of the interventricular sulcus had been located in the long-
axis cross-section, the ultrasound beam was rotated
laterally, visualizing the distal portion of the left anterior
descending artery (LAD) under color flow-mapping guid-
ance. Color flow imaging was visualized using a high
frequency color Doppler technique. Blood flow velocity
was measured by pulsed-wave Doppler echocardiog-
raphy, using a sample volume (1.5–2.0 mm) placed on
the color signal in the distal LAD. After obtaining coro-
nary flow velocity at the baseline, adenosine was infused
into the peripheral arm vein at a rate of 140 mg/kg per min
for a total of 3 min. During the infusion, heart rate, blood
pressure and ECG were recorded and monitored at base-
line, every minute during adenosine infusion and for the
first 5 min after the infusion. An experienced operator
who was blinded to the patient’s data measured coronary
flow velocities. Both mean and peak diastolic flow veloc-
ities at baseline and at peak hyperemia were measured
manually by tracing the contour of the spectral Doppler
signals using analysis software incorporated into the
ultrasound system. Averages of the measurements were
obtained in three cardiac cycles. Peak diastolic velocity
(PDV) and mean diastolic velocity (MDV) were measured
off-line. The coronary flow velocity reserve (CFVR) was
calculated as the ratio of hyperemic to basal mean diastolic
flow velocities.
Intraobserver and interobserver variabilityIntraobserver and interobserver coefficient of varia-
tion for MDV and PDV measurements were analyzed, first
by one operator on two different occasions for validation
of intraobserver variability, and then by a second operator
for evaluation of interobserver variability.
Statistical analysisData are presented as mean 6 standard deviation and
compared with the two sample t-test. Data was analyzed
using SAS 9.0 (SAS Institute Inc., Cary, NC, USA)

1758 Ultrasound in Medicine and Biology Volume 36, Number 10, 2010
and p , 0.05 was considered statistically significant.
Intra- and interobserver variability was calculated using
intraclass correlation coefficients (ICC).
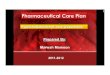
Fig. 1. An oblique coronal view in two-dimensional (2-D) mul-tiplanar reformatted image of hypercholesterolemia (HoFH)patient atherosclerotic plaques compromising the coronary
artery ostia.
RESULTS
Table 1 shows age, plasma lipid concentrations and
coronary flow parameters for the two study groups.
HoFH patients were similar to control subjects in age
and plasma triglyceride concentrations but had plasma
LDL concentrations higher than fourfold. Mean and
peak diastolic velocities in the LAD were not significantly
different in the two groups under basal conditions. When
vasodilator of the coronary arteries was induced with
adenosine, the increase in mean and peak diastolic veloc-
ities in the HoFH group was significantly lower than those
of the control group. As consequence of this inability to
achieve a normal increase in velocity during vasodilator
infusion, coronary flow velocity reserve was also signifi-
cantly lower in HoFH than in control subjects (3.36 vs.
1.92 respectively, p , 0.0001).
Aortic and coronary plaquesAll HoFH patients had aortic plaques and nine
patients had aortic plaques compromising the coronary
ostia (Fig. 1). In four patients, both the left and right coro-
nary artery ostia were involved. Five patients presented
coronary artery calcification. All patients had no signifi-
cant coronary artery stenosis (Table 2).
Table 3 listed lipid and coronary flow parameters of
HoFH subjects with and without plaques compromising
the coronary artery ostia. LDL cholesterol was signifi-
cantly higher in coronary artery ostia with plaques
subjects than those without. Coronary flow velocity
reserve was significantly lower.
Table 1. Blood lipid and coronary flow dynamics data inpatients with HoFH and control group
Control (n 5 15) HoFH (n 5 20) p
Age (years) 15.2 6 6.91 13.1 6 5.36 0.5772TC (mg/dL) 201.59 6 54.71 679.00 6 87.82 ,0.0001*LDL-C (mg/dL) 128.01 6 71.33 583.59 6 113.74 ,0.0001*TG (mg/dL) 105.12 6 48.96 106.22 6 43.43 0.9522
MDVb 23.60 6 5.58 27.82 6 7.72 0.1438PDVb 36.00 6 6.93 35.65 6 7.38 0.9034MDVh 77.96 6 18.12 51.88 6 11.78 ,0.0001*PDVh 91.60 6 15.09 69.76 6 13.91 0.0008*CFVR 3.36 6 0.61 1.92 6 0.40 ,0.0001*
Data are presented by mean 6 standard deviation.TC 5 total serum cholesterol; LDL-C 5 low-density lipoprotein
cholesterol; TG 5 triglyceride; MDVb 5 mean diastolic velocity at base-line; PDVb 5 peak diastolic velocity at baseline; MDVh 5 mean dia-stolic velocity in hyperemia; PDVh 5 peak diastolic velocity inhyperemia; CFVR 5 coronary flow velocity reserve.
* p , 0.05 marks statistical significance.
Intra- and interobserver variabilityTable 4 showed intra- and interobserver repeated
measure analysis using intraclass correlation coefficients
in the MDVb and MDVh.
DISCUSSION
Although HoFH is a rare disease, the mortality is
high due to the high prevalence of cardiovascular events.
It has been previously shown that sudden death and heart
failure are frequent causes of death in HoFH. Angina is
also a feature of HoFH since atherosclerosis may occur
on both aortic plaques and the coronary ostia.
A number of imaging techniques can be used to assess
coronary function and each has both advantages and disad-
vantages. Angiography is able to observe aortic and coro-
nary artery lumens and the degree of stenosis can be judged
directly. However, this method is invasive and cannot
accurately identify information about the vessel wall.
Magnetic resonance imaging (MRI) and CT, as noninva-
sive examinations, can detect early coronary atheroscle-
rosis in patients with HoFH and visualize plaque in both
the aorta and coronary artery but it is unable to evaluate
coronary hemodynamics (Santos et al. 2008; Summers
et al. 1998). Several tools have already been used to
measure coronary flow and coronary flow reserve (CFR)
for decades, including coronary sinus thermodilution,
cardiac nuclear imaging, cardiac magnetic resonance and
intracoronary Doppler flow wire. However, these
methods, mainly used research, have major limitations
on clinical analysis because of being complex, time-
consuming, expensive, invasive and not easily available.
TTDE can measure coronary flow and CFR and it is nonin-
vasive, easily available at bedside, not expensive and

Table 2. Aortic and coronary artery atherosclerosis
Patients
Aortic plaquesadjacent to
coronary ostia Aortic plaques compromising the coronary ostiaCoronary artery
calcification Affected artery
1 Yes compromising the left coronary ostia No None2 Yes Compromising the left coronary ostia Yes Mid LAD3 Yes compromising the left and right coronary ostia No None4 Yes compromising the left coronary ostia No None5 Yes compromising the left coronary ostia Yes Left main6 Yes compromising the left and right coronary ostia Yes Mid RCA7 Yes compromising the left coronary ostia Yes Left main8 Yes compromising the left and right coronary ostia Yes Left main and mid RCA9 Yes compromising the left and right coronary ostia No None
Evaluation of coronary flow velocity reserve d Y. YANG et al. 1759
without radiation exposure with multiple potential clinical
applications.
Using the noninvasive technique, TTDE, we found
a significant decrease in coronary flow velocity reserve
in the HoFH patients. In this study, TTDE and DSCT
were used to detect coronary flow dynamics and athero-
sclerosis in HoFH subjects. The most striking finding
was that CFVR was significantly lower in coronary artery
ostia with plaques subjects than those without. These
results suggest that TTDE assessment of CFVR might
be used in HoFH patients to assess their coronary artery
hemodynamics.
We used the ratio of hyperemic to rest coronary flow
velocity to calculate the CFVR, which is an important
index of coronary hemodynamics. CFR is defined as the
ratio of coronary flow under maximal coronary vasodila-
tion to coronary flow in resting condition. Intracoronary
Doppler and simultaneous angiography were used to deter-
mine CFR itself. However, this method is invasive and
costly and its clinical use is restricted. If coronary artery
cross-sectional area is similar during basal and hyperemic
conditions, CFVR can be used to represent CFR (Erbel
et al. 1996). TTDE can measure CFVR as a noninvasive
way. Average peak velocity, measured by TTDE, had
been found to correlate well with that measured invasively
Table 3. Lipid and hemodynamic parameters inhomozygous familial hypercholesterolemia patients withand without aortic plaques combined with the coronary
ostia
Aortic plaquescompromising the
coronary ostia
No aortic plaquescompromising the
coronary ostia p
CFVR 1.72 6 0.32 2.15 6 0.38 0.0029*TC (mg/dL) 714.67 6 105.57 638.88 6 37.60 0.0710LDL-C (mg/dL) 634.63 6 119.05 526.18 6 79.08 0.0455*TG (mg/dL) 95.45 6 37.62 118.33 6 48.75 0.2925
Data are presented by mean 6 standard deviation.CFVR 5 coronary flow velocity reserve; TC 5 total serum choles-
terol; LDL-C 5 low-density lipoprotein cholesterol; TG 5 triglyceride.* p , 0.05 marks statistical significance.
by intracoronary Doppler (Bartel et al. 1999; Murata et al.
2006). However, coronary artery flow velocity was
lower in the systolic, especially during the baseline; flow
spectrum can not be displayed completely in some
patients at the systolic. Nevertheless, flow spectrum can
be displayed thoroughly in the systolic either in the
baseline or in hyperemic. As a result, MDV was used to
calculate CFVR in this study.
All the patients were successfully measured with
CFVR in current study since all the patients were
children. Although no significant difference between
HoHF patients and controls was seen in MDV and PDV
at baseline, MDV and PDV were significantly decreased
in HoHF patients compared with controls during hyper-
emia (Figs. 2 and 3). All HoFH patients had aortic
plaques by DSCT and nine patients had aortic plaques
combined with the coronary ostia. In four patients,
both the left and right coronary artery ostia were
compromised while all patients had no significant
coronary artery stenosis. CFVR was impaired in HoFH
patients probably because the high serum cholesterol led
to an increase in coronary resistance (Kaufmann et al.
2000; Yokoyama et al. 1996; Awan et al. 2008). A
typical characteristic of HoFH is aortic plaques. CFVR
was lower and LDL-C concentration was increased signif-
icantly in the aortic plaques compromising the coronary
ostia compared with the group without compromising
the coronary ostia. Decrease of coronary artery flow perfu-
sion due to plaques compromising the coronary artery ostia
and coronary artery calcification would explain the signif-
icant decrease in CFVR seen in HoHF patients with aortic
Table 4. Intra- and interobserver ICC
MDVb MDVh
intraobserver interobserver intraobserver interobserver
r 0.987 0.989 0.992 0.990
MDVb 5 mean diastolic velocity at baseline; MDVh 5 mean diastolicvelocity in hyperemia.

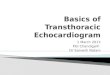
Fig. 2. Transthoracic color Doppler echocardiography demon-strating coronary blood flow in the distal left anterior descending
artery (LAD) when basal.
1760 Ultrasound in Medicine and Biology Volume 36, Number 10, 2010
plaques compromising the coronary ostia (Beppu et al.
1983).
CONCLUSION
TTDE together with DSCT could be used to detect
both coronary and aortic atherosclerosis in HoFH subjects.
Noninvasive CFVR measurement using TTDE may be
useful to evaluate coronary hemodynamics. CFVR is
impaired in patients with HoFH due to existence of
coronary atherosclerosis. It is further impaired in HoFH
patients with aortic plaques compromising the coronary
ostia.
Study limitationsMurata et al. measured CFVR using TTDE in three
major coronary arteries. They defined CFVR , 2.0 in at
least one vessel as being positive for myocardial ischemia
and, then, compared TTDE results with single photon
Fig. 3. Transthoracic color Doppler echocardiography demon-strating coronary blood flow in the distal left anterior descending
artery (LAD) when hyperemic.
emission computed tomography (SPECT). The sensitivity
and specificity of CFVR , 2.0 in at least one coronary
vessel were 86% and 89%, respectively. However, it
was more difficult to measure CFVR in the posterior de-
scending artery or the lateral circumflex artery than in
the LAD (Murata et al. 2006). In the present study,
CFVR was only calculated in the LAD. DSCT angiog-
raphy can identify coronary plaques but the hemodynamic
significance of these is uncertain as most operators are
only able to report .50% stenosis and unable to distin-
guish hemodynamically significant disease.
Acknowledgments—This work was supported by the research grants fromNational Natural Science Foundation of China Research Grants30772356, the Natural Science Foundation of Beijing, China (Grant7062010).
REFERENCES
Awan Z, Alrasadi K, Francis GA, Hegele RA, McPherson R, Frohlich J,Valenti D, Varennes BD, Marcil M, Gagne C, Genest J, Couture P.Vascular calcifications in homozygote familial hypercholesterol-emia. Arterioscler Thromb Vasc Biol 2008;28:777–785.
Bartel T, Muller S, Baumgart D, Mathew B, Haude M, Erbel R.Improved high frequency transthoracic flow velocity measurementin the left anterior descending coronary artery after intravenousperipheral injection of Levovist. J Am Soc Echocardiogr 1999;12:252–256.
Beppu S, Minura Y, Sakakibara H, Nagata S, Park YD, Nambu S,Yamamoto A. Supravalvular aortic stenosis and coronary ostialstenosis in familial hypercholesterolemia: Two-dimensional echocar-diographic assessment. Circulation 1983;67:878–884.
Civeira F, Castillo S, Alonso R, Merino Ibarra E, Cenarro A,Artied M, Martin Fuentes P, Ros E, Pocovi M, Mata P. Tendonxanthomas in familial hypercholesterolemia are associated withcardiovascular risk independently of the low-density lipoproteinreceptor gene mutation. Arterioscler Thromb Vasc Biol 2005;25:1960–1965.
Erbel R, Ge J, Bockisch A, Kearney P, GOrge G, Haude M, Schumann D,Zamorano J, Rupprecht HJ, Meyer J. Value of intracoronary ultra-sound and Doppler in the differentiation of angiographically normalcoronary arteries: A prospective study in patients with angina pecto-ris. Eur Heart J 1996;17:880–889.
Faccenda F, Rubba P, Gnasso A, Pauciullo P, Postiglione A, Cortese C,Mancini M. Noninvasive ultrasound evaluation of pressure gradientsin aortic root of homozygotes for familial hypercholesterolemia.Arteriosclerosis 1990;10:710–713.
Kaufmann PA, Gnecchi-Ruscone T, Schafers KP, Luscher TF,Camici PG. Low density lipoprotein cholesterol and coronary micro-vascular dysfunction in hypercholesterolemia. J Am Coll Cardiol2000;36:103–109.
Kraft HG, Lingenhel A, Raal FJ, Hohenegger M, Utermann G. Lipopro-tein(a) in homozygous familial hypercholesterolemia. ArteriosclerThromb Vasc Biol 2000;20:522–528.
Marais AD. Familial hypercholesterolemia. Clin Biochem Rev 2004;25:49–68.
Murata E, Hozumi T, Matsumura Y, Fujimoto K, Sugioka K,Takemoto Y, Watanabe H, Yamagishi H, Yoshiyama M, Iwao H,Yoshikawa J. Coronary flow velocity reserve measurement in threemajor coronary arteries using transthoracic Doppler echocardiog-raphy. Echocardiography 2006;23:279–286.
Santos RD, Miname MH, Martinez LC, Rochitte CE, Chacra AM,Nakandakare ER, Chen D, Schaefer EJ. Noninvasive detection ofaortic and coronary atherosclerosis in homozygous familial hyper-cholesterolemia by 64-slice multidetector row computed tomographyangiography. Atherosclerosis 2008;197:910–915.
Summers RM, Andrasko-Bourgeois J, Feuerstein IM, Hill SC, Jones EC,Busse MK, Wise B, Bove KE, Rishforth BA, Tucker E, Spray TL,

Evaluation of coronary flow velocity reserve d Y. YANG et al. 1761
Hoeg JM. Evaluation of the aortic root by MRI: Insights frompatients with homozygous familial hypercholesterolemia. Circula-tion 1998;98:509–518.
Wiegman A, Rodenburg J, de Jongh S, Defesche J, Bakker H,Kastelein JP, Sijbrands EG. Family history and cardiovascular risk
in familial hypercholesterolemia: Data in more than 1000 children.Circulation 2003;107:1473–1478.
Yokoyama I, Murakami T, Ohtake T, Momomura S, Nishikawa J,Sasaki Y, Omata M. Reduced coronary flow reserve in familialhypercholesterolemia. J Nucl Med 1996;37:1937–1942.