Embed Size (px)
Citation preview

Evaluation of Molecular Diagnostic Tests for TB (Option B Study)
Mary DeMartino, B.S., MT (ASCP) SM State Hygienic Laboratory-Iowa [email protected] 8th National Conference on Laboratory Aspects of Tuberculosis August 20, 2013
This presentation was supported by the Association of Public Health Laboratories and by the Cooperative Agreement Number U60HM000803 from the Centers for Disease Control and Prevention and/or Assistant Secretary for Preparedness and Response. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Association of Public Health Laboratories, the Centers for Disease Control and Prevention and/or Assistant Secretary for Preparedness and Response.
Request for Application: Performance Evaluation of Molecular Diagnostic Tests for Tuberculosis Option B Determining best practices for performing NAAT and the contribution of NAAT as it relates to the overall TB testing algorithm in the laboratory. Some examples include, number of diagnostic specimens receiving NAAT per patient (e.g., incremental yield in smear negatives), incremental yield of 1, 2, or 3 cultures inoculated per patient for diagnosis, or the need for confirmatory testing by another method when NAAT is positive.
SHL’s Objectives 1. Determine the number of smear negative
specimens from an individual patient on which NAAT should be performed in a low incidence population.
2. Determine how Rifampin resistance testing performs in a low prevalence setting. 3. Develop an algorithm indicating the number of NAATs to perform on smear negative specimens from patients based on suspicion for tuberculosis and risk factors.
Background • Iowa has between 35 and 40 new TB cases
per year • Protocol at the time:
o Perform naat on all new smear positive patients o Perform naat on smear negatives at the request
of the TB controllers oWe had been performing naat on up to three
specimens per smear negative patient if the first naat was negative-what our controllers expected
• Wanted to move towards limiting that to two specimens per smear negative patient
• IRB Approval • Purchase additional instrumentation and
supplies • Development of internal protocol • Determination of enrollment criteria • Development of enrollment process • Maintenance of Data Collection Sheet • Analyze data • Determine algorithm

IRB Approval
Purchase Equipment and Supplies
www.cepheid.com
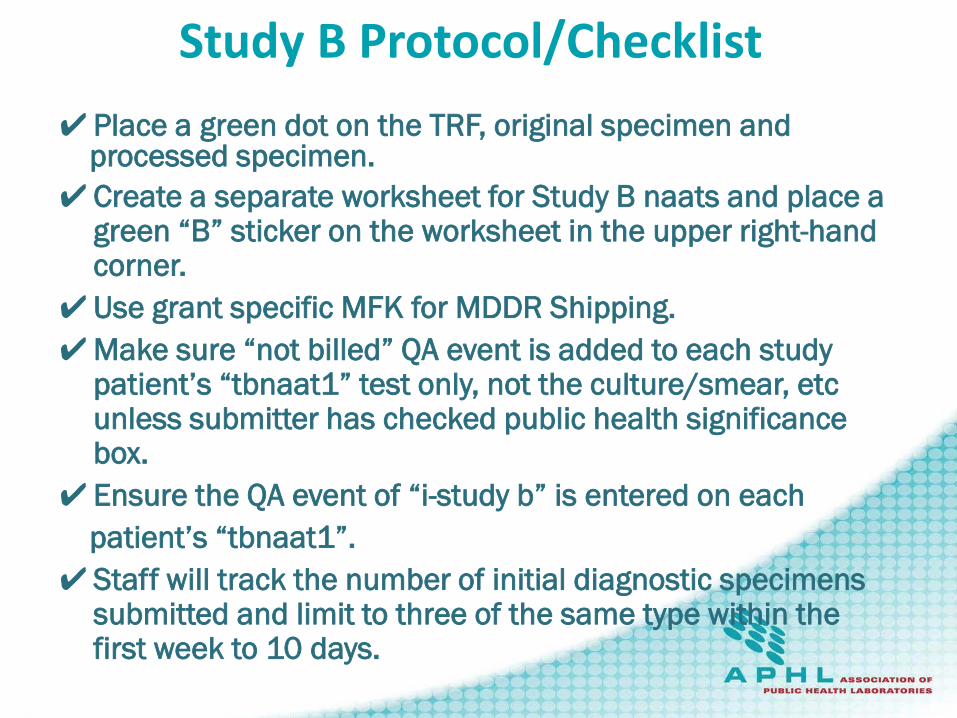
Study B Protocol/Checklist
✔Place a green dot on the TRF, original specimen and processed specimen. ✔Create a separate worksheet for Study B naats and place a
green “B” sticker on the worksheet in the upper right-hand corner.
✔Use grant specific MFK for MDDR Shipping. ✔Make sure “not billed” QA event is added to each study
patient’s “tbnaat1” test only, not the culture/smear, etc unless submitter has checked public health significance box.
✔Ensure the QA event of “i-study b” is entered on each patient’s “tbnaat1”. ✔Staff will track the number of initial diagnostic specimens
submitted and limit to three of the same type within the first week to 10 days.
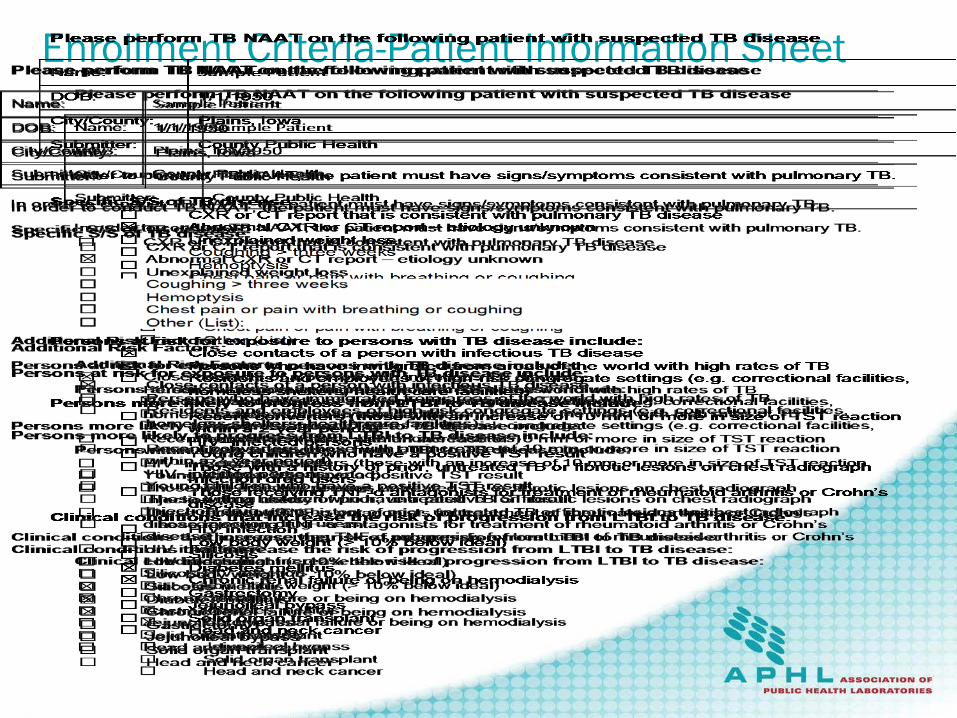
Enrollment Criteria-Patient Information Sheet

Enrollment Process
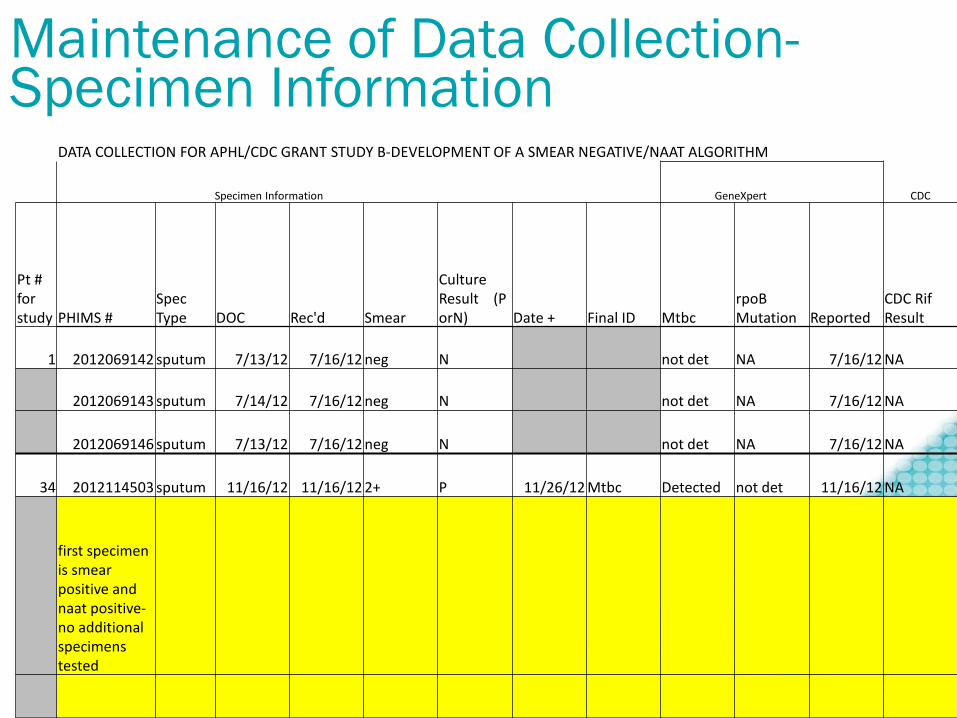
DATA COLLECTION FOR APHL/CDC GRANT STUDY B-DEVELOPMENT OF A SMEAR NEGATIVE/NAAT ALGORITHM
Specimen Information GeneXpert CDC
Pt # for study PHIMS #
Spec Type DOC Rec'd Smear
Culture Result (P orN) Date + Final ID Mtbc
rpoB Mutation Reported
CDC Rif Result
1 2012069142 sputum 7/13/12 7/16/12 neg N not det NA 7/16/12 NA
2012069143 sputum 7/14/12 7/16/12 neg N not det NA 7/16/12 NA
2012069146 sputum 7/13/12 7/16/12 neg N not det NA 7/16/12 NA
34 2012114503 sputum 11/16/12 11/16/12 2+ P 11/26/12 Mtbc Detected not det 11/16/12 NA
first specimen is smear positive and naat positive-no additional specimens tested
Maintenance of Data Collection-Specimen Information
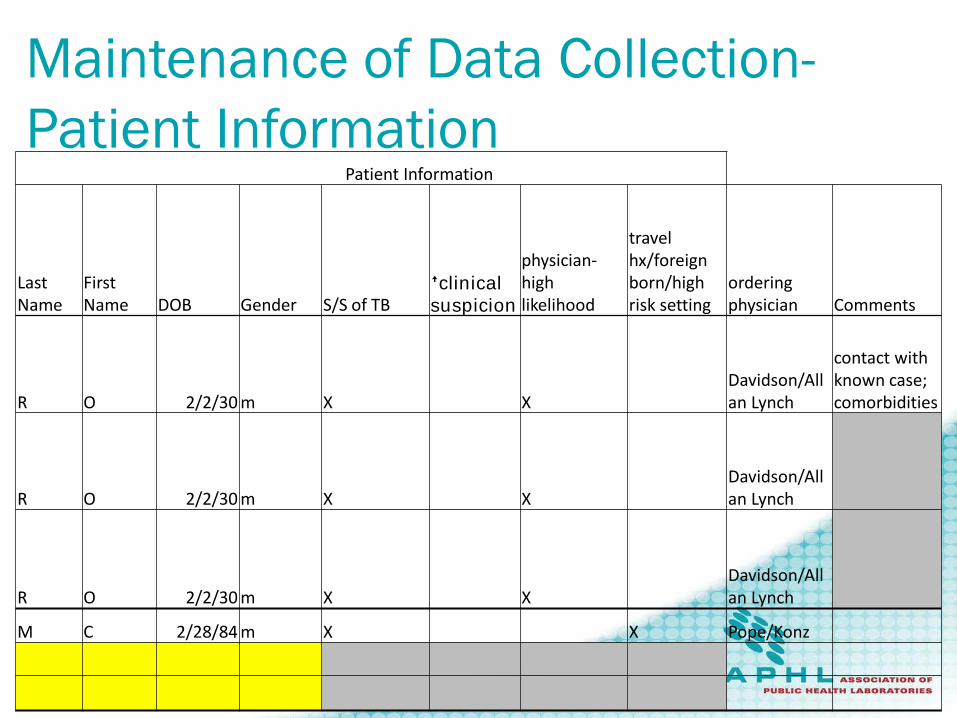
Patient Information
Last Name
First Name DOB Gender S/S of TB
ꜛclinical suspicion
physician-high likelihood
travel hx/foreign born/high risk setting
ordering physician Comments
R O 2/2/30 m X X Davidson/Allan Lynch
contact with known case; comorbidities
R O 2/2/30 m X X Davidson/Allan Lynch
R O 2/2/30 m X X Davidson/Allan Lynch
M C 2/28/84 m X X Pope/Konz
Maintenance of Data Collection-Patient Information
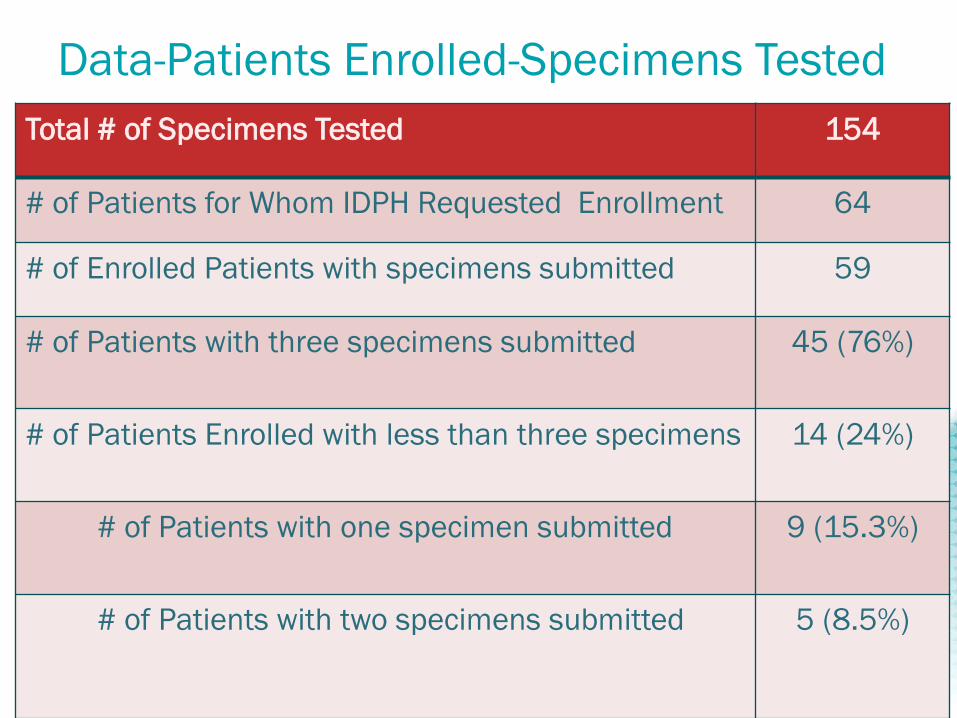
Total # of Specimens Tested 154
# of Patients for Whom IDPH Requested Enrollment 64
# of Enrolled Patients with specimens submitted 59
# of Patients with three specimens submitted 45 (76%)
# of Patients Enrolled with less than three specimens 14 (24%)
# of Patients with one specimen submitted 9 (15.3%)
# of Patients with two specimens submitted 5 (8.5%)
Data-Patients Enrolled-Specimens Tested
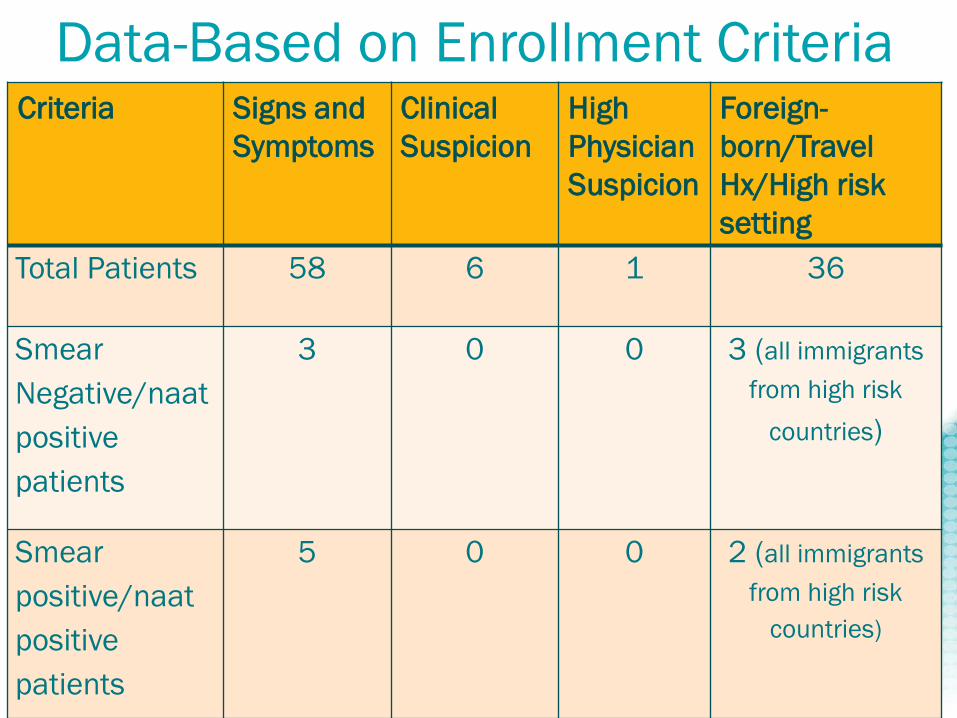
Criteria Signs and Symptoms
Clinical Suspicion
High Physician Suspicion
Foreign-born/Travel Hx/High risk setting
Total Patients 58 6 1 36
Smear Negative/naat positive patients
3 0 0 3 (all immigrants from high risk
countries)
Smear positive/naat positive patients
5 0 0 2 (all immigrants from high risk
countries)
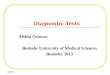
Data-Based on Enrollment Criteria

0
10
20
30
40
50
60
58
6 1
36
3 0 0 3 5 0 0 2
Total Patients
Smear Negative/NAAT Positivepatients
Smear Positive/NAAT Positivepatients
Data-Based on Enrollment Criteria
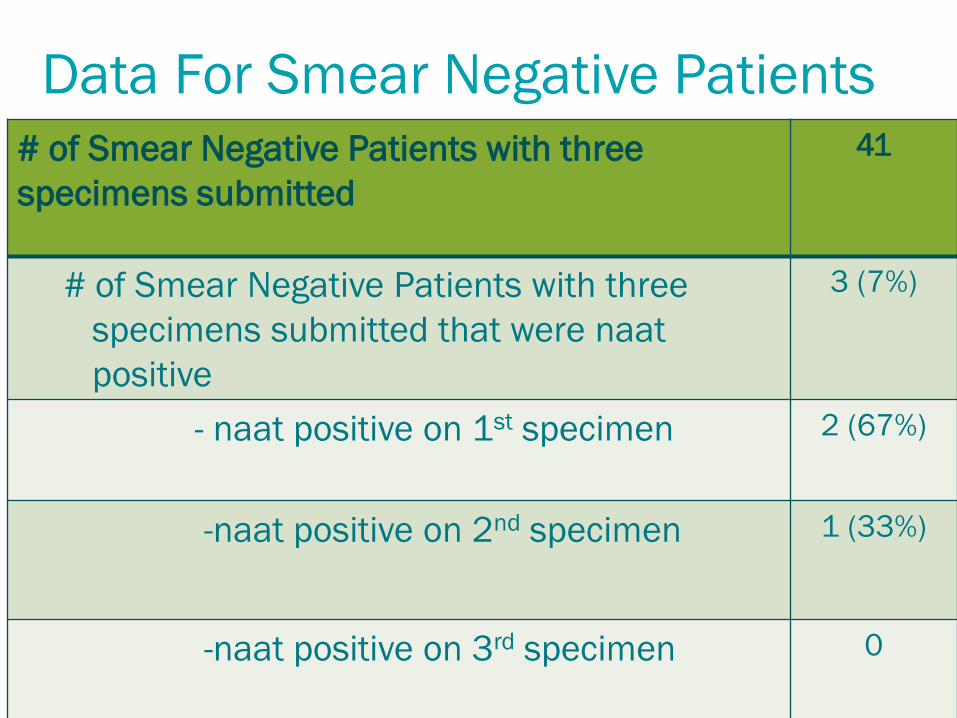
# of Smear Negative Patients with three specimens submitted
41
# of Smear Negative Patients with three specimens submitted that were naat positive
3 (7%)
- naat positive on 1st specimen 2 (67%)
-naat positive on 2nd specimen 1 (33%)
-naat positive on 3rd specimen 0
Data For Smear Negative Patients
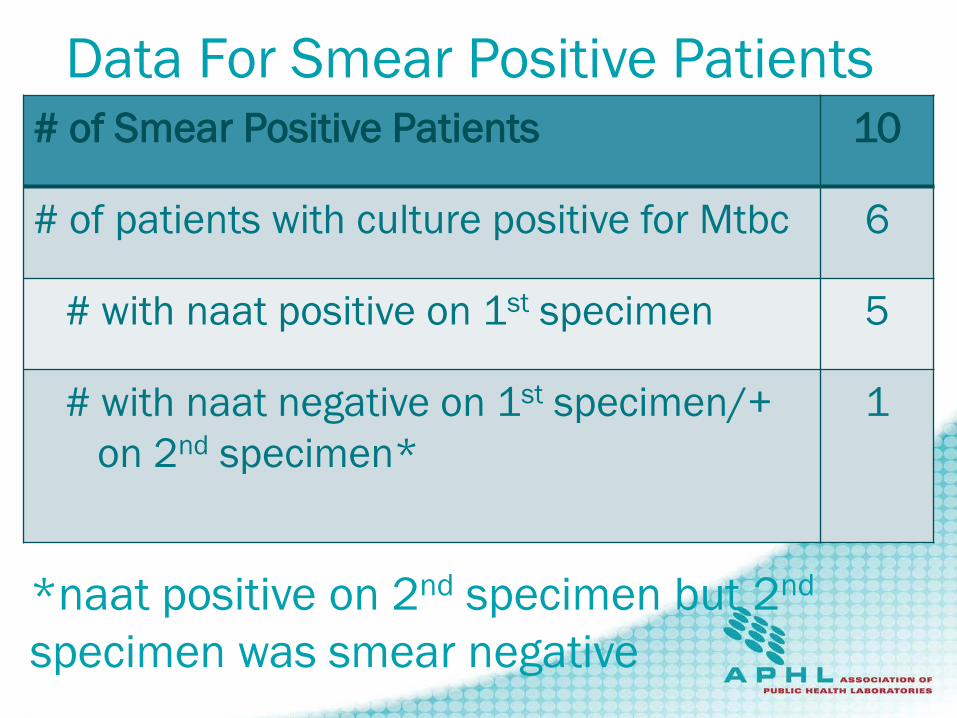
*naat positive on 2nd specimen but 2nd specimen was smear negative
# of Smear Positive Patients 10
# of patients with culture positive for Mtbc 6
# with naat positive on 1st specimen 5
# with naat negative on 1st specimen/+ on 2nd specimen*
1
Data For Smear Positive Patients
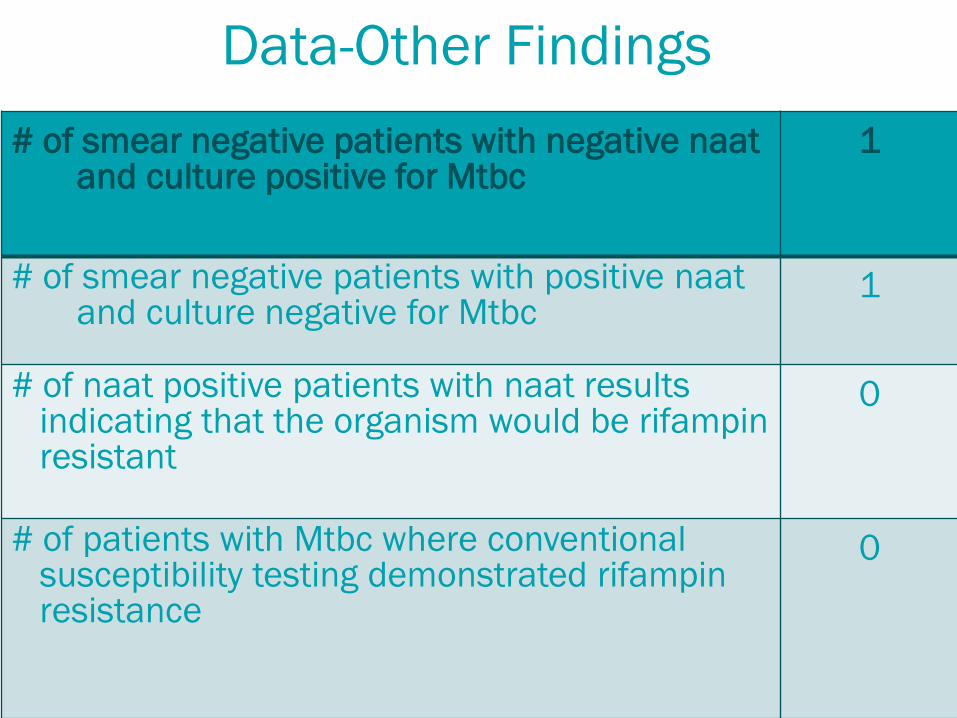
Data-Other Findings # of smear negative patients with negative naat and culture positive for Mtbc
1
# of smear negative patients with positive naat and culture negative for Mtbc
1
# of naat positive patients with naat results indicating that the organism would be rifampin resistant
0
# of patients with Mtbc where conventional susceptibility testing demonstrated rifampin resistance
0
Objective 1-Mostly Met
• Regardless of smear results patients who grew Mycobacterium tuberculosis complex (mostly) did not require more than two specimens to achieve a positive naat.
Objective 2-Not Met • We had no specimens that were Rifampin
resistant by the GeneXpert and no patients whose conventional susceptibility testing indicated rifampin resistance.
Conclusions on Risk Factors 58 (98%) of the 59 patients tested were
noted to have signs and symptoms of TB. 37 (63%) of the 59 patients tested were
noted as meeting the criteria of being foreign-born or having a history of travel to a high risk country or living in a high-risk setting.
Objective 3-Met 100% of the naat positive specimens,
regardless of smear results, were noted to have signs and symptoms of TB and immigrated from a high risk country. This indicates that presenting with
signs and symptoms of TB is the most important indicator when deciding if a patient should have a naat performed.
Naat identified 7% (3 out of 41) of smear negative patients who were M. tuberculosis complex positive within 24 hours of receipt of specimen.

Ensuring that the requested number of specimens recommended for initial diagnosis of tuberculosis were submitted.
Patients with inconsistent smear results and naat results for the three initial diagnostic specimens. There were two patients who had specimens
that were smear negative, naat negative and culture positive for Mycobacterium tuberculosis complex.
There was one patient whose first specimen was smear positive, naat negative and culture positive. Their second specimen was smear negative, naat positive and culture positive and their third specimen was smear negative, naat negative and the culture negative.
There was one patient with three specimens submitted. All three were smear negative and culture negative but the first specimen received was naat positive. The naat on each of the other two specimens was negative. TB Controllers indicate that this patient was reported as a verified case.
Ryan Jepson Bridget Konz Beth Albaugh Allan Lynch Jolynn Koehler Jennifer Elwood Bob Rotzoll Erin Nelson
Michael Pentella-CLIA Director SHL Staff IDPH TB Controllers