Embed Size (px)
Citation preview
Event Reporting, Disclosure, Sentinel
Events & Mock RCA – Grand Rounds
Eva M. Satori, B.A., CPHRM, FASHRMManager, Risk ServicesApril 2, 2015
2
• What Events should be reported in online Event Reporting System (ERS)
• Definition of Sentinel Events
• Disclosure of Adverse Events
• Definition Root Cause Analysis (RCA)
• Mock RCA
Objectives
3
• Event (incident, occurrence, notification): – Any unanticipated event that is not consistent with the routine care of a particular
patient and/or the routine operation of the facility. An event may be a potential or actual adverse event that involves a patient, guest, employee, volunteer, student or physician.
• Sentinel Event: – An unexpected event involving death or serious physical injury or psychological injury or
the risk thereof. Serious injury includes loss of limb or function. The phrase “or risk thereof” includes any process variation for which the recurrence would carry significant chance of serious adverse outcome.
• Disclosure: – Information regarding the results of a diagnostic test, medical treatment or surgical
intervention communicated to the patient, family and/or surrogate.
• Root Cause Analysis (RCA): – Is a process intended to help organizations delve deeper into processes (not people).
Definitions
4
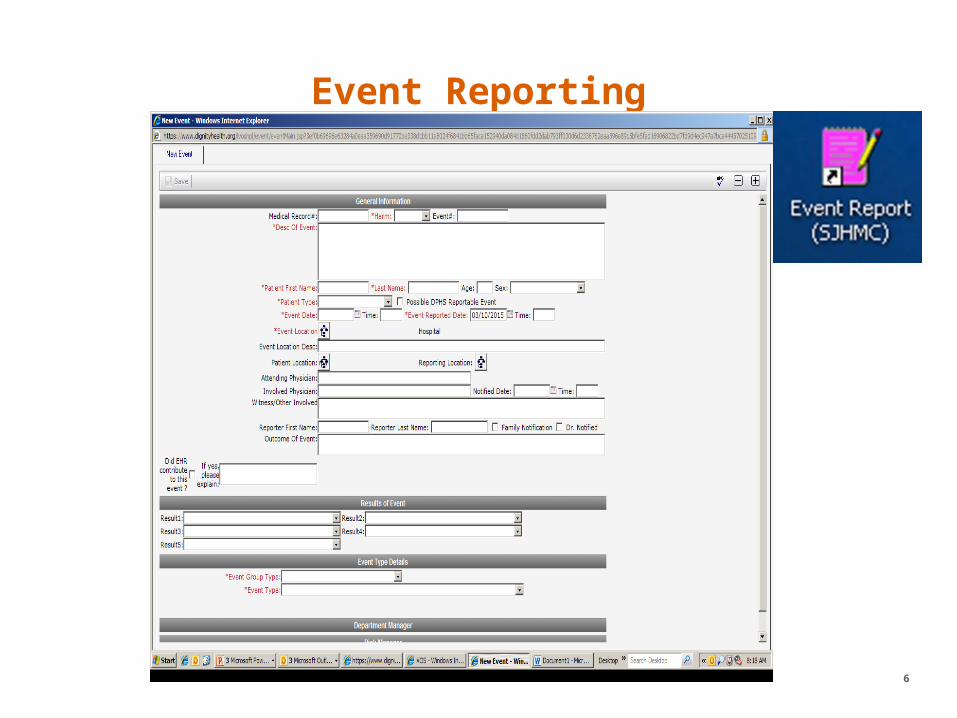
Event Reporting
Event Reporting
• An event/incident is any unanticipated event or any potential event that is not consistent with the routine care of a particular patient and/or routine operation of the facility.
– Be timely
– Be factual
– Provide details
– You may submit anonymously but it is always best if your name is provided for follow up
– Inform Attending MD, Program Directors or Chiefs
– Safe Harbor provision – report event within 48 hours in which employee involved.
5
Event Reporting
6
7
• Categorized and Routed to the involved Department/Director/Manager/Medical Staff
• Investigated and reviewed
• Improvement activities and follow up plans
• Serious events are quickly escalated to leadership for review and consideration of RCA.
What happens to Event Reports?
8
• Missed diagnosis or misdiagnosis
• Procedure or test done on wrong patient
• Reactions/complications to a medical test
• Patient death or serious injury associated with unsafe administration of blood products
• Hospital incurred trauma, injury or infection
• Patient or guest suicide or suicide attempt
• Death or permanent loss of function from a hospital acquired injury
• See “Think Pink handout” examples for further examples.
Examples of Events to be report in Event Reporting System (ERS)
9
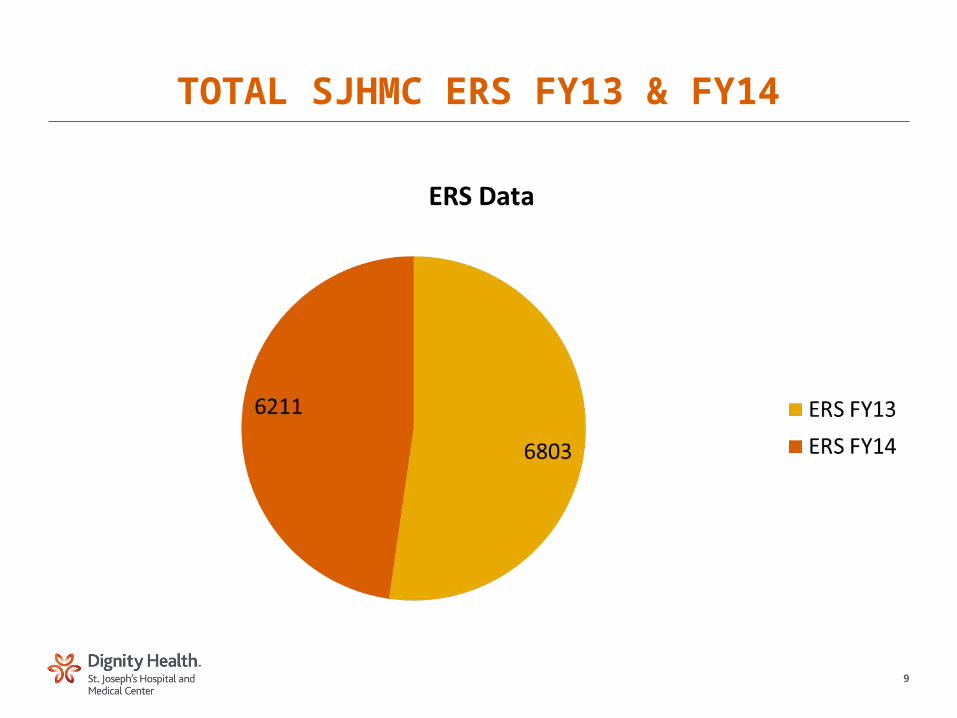
TOTAL SJHMC ERS FY13 & FY14
10
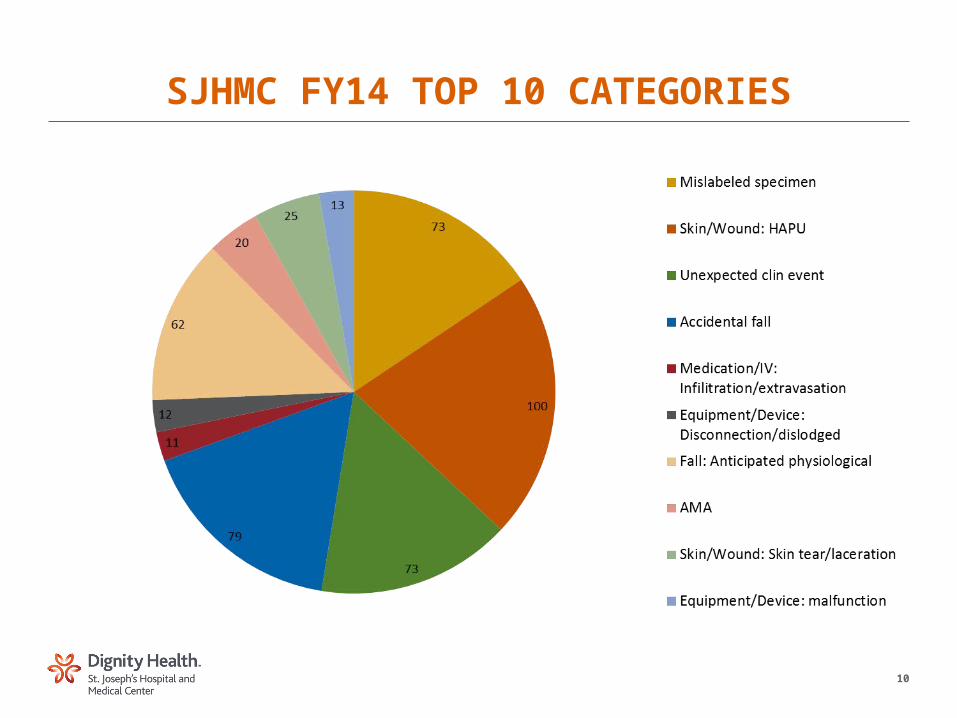
SJHMC FY14 TOP 10 CATEGORIES
11
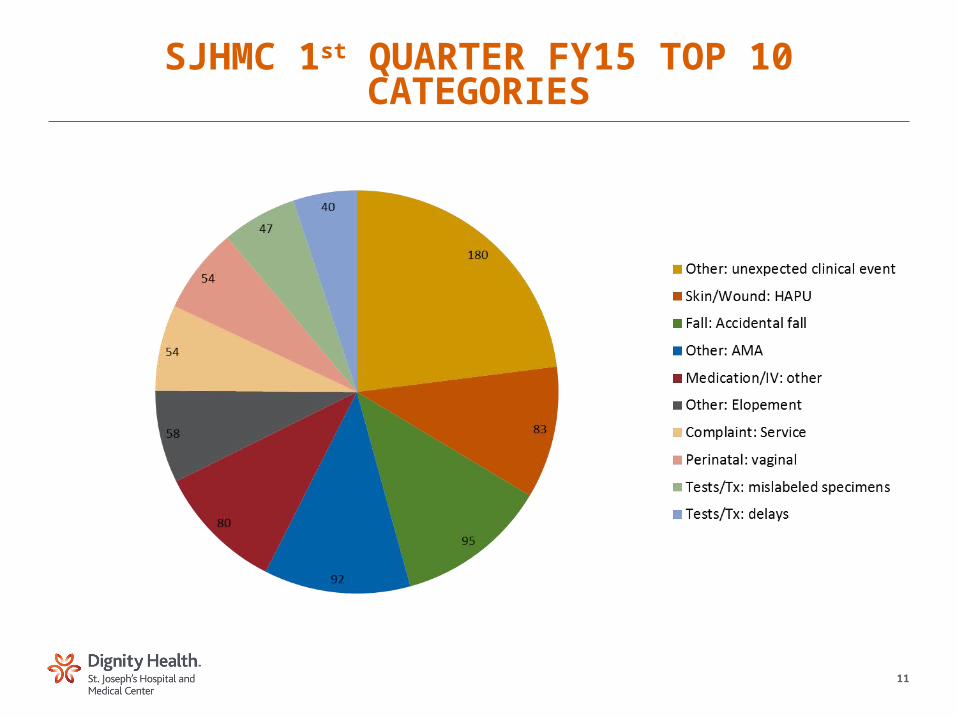
SJHMC 1st QUARTER FY15 TOP 10 CATEGORIES

12
Sentinel Events
13
• The Joint Commission (TJC) adopted a formal Sentinel Event Policy in 1996 to help hospitals that experience serious adverse events, improve safety and learn from those sentinel events.
• Definition of Sentinel Event: – Death
– Permanent Harm
– Severe Temporary Harm (critical, potentially life-threatening harm lasting for a limited time with no permanent residual, but requires transfer to higher level of care/monitoring for a prolonged period of time, transfer to higher level of care for a life-threatening condition, or additional major surgery, procedure, or treatment to resolve the condition.)
What is a Sentinel Event?
14
• An event is also considered sentinel if it is one of the following: – Suicide of any patient receiving care, treatment, and services in a staffed
around-the-clock care setting or within 72 hours of discharge, including from a hospital’s ED
– Unanticipated death of a full-term infant
– Discharge of an infant to the wrong family
– Abduction of any patient receiving care, treatment, and services
– Any elopement (that is, unauthorized departure) of a patient from a staffed around-the-clock care setting (including the ED), leading to a death, permanent harm, or severe temporary harm to the patient
– Hemolytic transfusion reaction involving administration of blood or blood products having major blood group incompatibilities (ABO, Rh, other blood groups)
What is a Sentinel Event? (cont)
15
– Rape, assault (leading to death, permanent harm, or severe temporary harm), or homicide of a staff member, licensed independent practitioner, guest, or vendor while on site at the hospital
– Invasive procedure, including surgery, on the wrong patient, at the wrong site, or that is the wrong (unintended) procedure
– Unintended retention of a foreign object in a patient after an invasive procedure, including surgery
– Severe neonatal hyperbilirubenemia (bilirubin >30 milligrams/deciliter)
– Prolonged fluroscopy with cumulative dose >1,500 rads to a single field or any delivery of radiotherapy to the wrong body region or >25% above the planned radiotherapy dose
– Fire, flame, or unanticipated smoke, heat or flashes occurring during an episode of patient care
– Any intrapartum (related to the birth process) maternal death or severe maternal morbidity
What is a Sentinel Event? (cont)
16
Disclosure
17
• Patients and their families will be informed about outcomes of treatment, including those that differ significantly from anticipated outcomes.
• The attending physician will lead the disclosure discussion. A representative from the hospital/Nursing, and Risk Manager will be present.
• Provide a factual explanation of the event and the impact on the patient’s treatment.
• A commitment to investigate the event in order to prevent like occurrences.
• Resources available to support and comfort the patient, family and/or surrogate.
• An apology or other expression of sympathy.
Disclosure
18
• Documentation in the medical record, should be completed by the physician or other designated individual participating in the disclosure and should contain: – A full description of facts of the event, without conjecture as to the cause
or attribution of fault/blame.
– Detailed disclosure discussions with the patient, family and/or surrogate.
– Identity of any interpreter used during the disclosure.
– Any follow-up discussions with the patient, family and/or surrogate.
– Complete an event report (if one not already completed). Do not refer to the event report in the patient’s medical record.
Disclosure – documentation in medical record
• Arizona Apology Law ARS 12-2605 (2005)– In any civil action that is brought against a health care provider…any
statement…expression apology…made by a health care provider…to the patient…that relates to discomfort, pain, suffering, injury, or death of the patient as a result of the unanticipated outcome of medical care is inadmissible as evidence of an admission of liability.
May I apologize?
19
20
Root Cause Analysis (RCA)
21
• Per The Joint Commission (TJC) and St. Joseph’s policy, an RCA is to be completed within 45 days of the event.
• Is a process for identifying the basic and causal factor(s) that underlying variation in performance, including the occurrence or possible occurrence of a sentinel event.
• Focuses primarily on systems and processes, not individual performance. • Addresses the appropriate elements from TJC “Minimum Scope of Review of
RCA”. • Set ground-rules:
• Safe, blame-free, protected• Structured retrospective analysis of events• Multidisciplinary• Focus on systems and processes, not individual performance• Identify and implement improvement actions to prevent recurrence
Root Cause Analysis (RCA)
22
• The Joint Commission (TJC) expects hospitals to identify and respond appropriate to all sentinel events:
• A formalized team response that stabilizes the patient, discloses the event to the patient and family, and provides support for the family as well as staff involved.
• Notification of hospital leadership.
• Immediate investigation.
• Completion of a comprehensive systematic analysis for identifying the causal and contributory factors.
• Corrective actions.
• Timeline for implementation of corrective actions.
• Systemic improvement.
Root Cause Analysis (RCA) (cont)
23
• Start the investigation• Gather data (e.g. staff involved, create a timeline)• Analyze the data• Identify root causes – A determination of the human and other factors most directly associated with
the sentinel event and the process(es) and systems related to its occurrence;
– Analysis of the underlying systems and processes through a series of “WHY?” questions to determine where redesign might reduce risk;
– Identification of risk points and their potential contributions to this type of event
• Create recommendations• Complete investigation and follow up on results
RCA process
24
• RCA action plan addressing the identified root causes, will identify the strategies than an organization intends to implement to reduce the risk of similar events occurring in the future. An appropriate action plan should demonstrate the following: – Identify changes that can be implemented to reduce risk, or formulates a
rationale for not undertaking such changes.
– Address responsibility for implementation, oversight, pilot testing as appropriate, timelines, and strategies for measuring the effectiveness of the actions.
RCA Action Plan
25
• Common Pitfalls
– Insufficient Organizational Support
– Reliance on the “Old View”
– Hindsight Bias
– Emphasis on “Work as Written”
– Failure to Reach True Root Causes
– Root Causes Unaddressed
– Insufficient Follow-Up, monitoring
• Guiding Principles
– Embrace Organizational Learning
– Address Root Causes
– Focus on “Work as Done”
– See Perspective of Staff
– Get into the Mindset
– Delve Deeply
– Develop Leading Indicators
RCA – Common Pitfalls and Strategies to Avoid them
26
• Patient RW– 64 YO male with new onset seizure-like activity with right hemiplegia,
altered mental status
– After consulting neurology, decided to get MRI with LP; MRI performed under general anesthesia due to deteriorating mental status
– MRI results inconclusive, so LP performed while patient still under general anesthesia
– Neurology reviews the MRI and adds additional recommendations which are text to the Medicine intern
– Next AM, patient RW is told that the LP studies looked normal. He hadn’t realized the LP was even performed and is angry about this fact.
– Neurology recommends additional LP to complete studies which weren’t done.
MOCK RCA
27
• Was there an error in RW’s care? – How would you classify the error(s)?
• Was there an adverse event? – If so, was it preventable?
• Should an Event Report be completed? – If so, by whom?
MOCK RCA (cont)
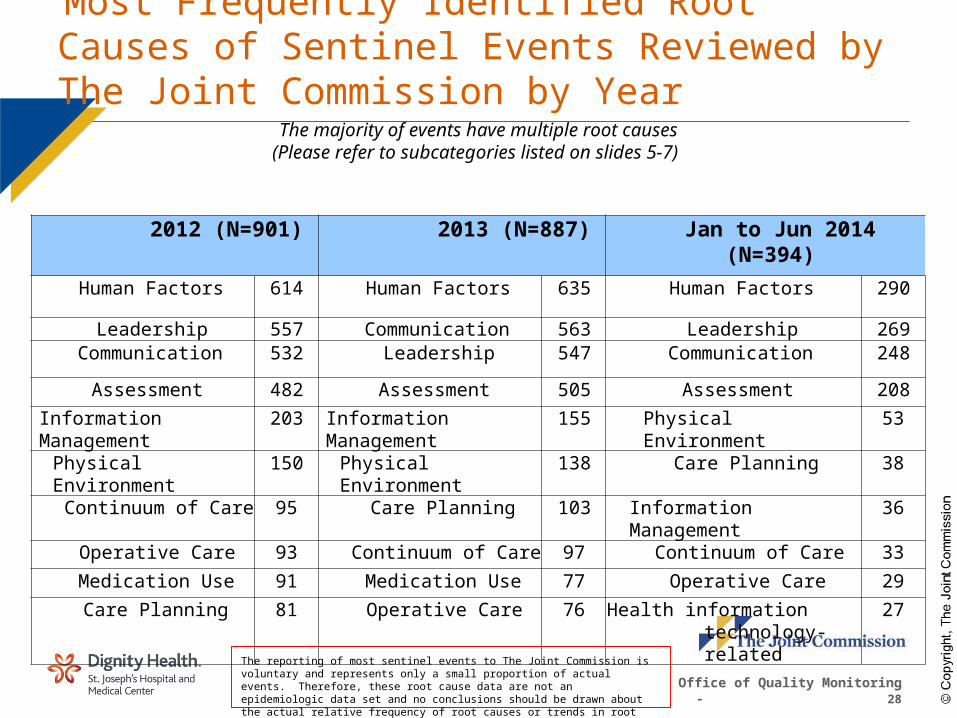
Most Frequently Identified Root Causes of Sentinel Events Reviewed by The Joint Commission by Year
The majority of events have multiple root causes (Please refer to subcategories listed on slides 5-7)
The reporting of most sentinel events to The Joint Commission is voluntary and represents only a small proportion of actual events. Therefore, these root cause data are not an epidemiologic data set and no conclusions should be drawn about the actual relative frequency of root causes or trends in root causes over time.
Office of Quality Monitoring - 28
2012 (N=901) 2013 (N=887) Jan to Jun 2014 (N=394)
Human Factors 614 Human Factors 635 Human Factors 290
Leadership 557 Communication 563 Leadership 269Communication 532 Leadership 547 Communication 248
Assessment 482 Assessment 505 Assessment 208
Information Management 203 Information Management 155 Physical Environment 53
Physical Environment 150 Physical Environment 138 Care Planning 38
Continuum of Care 95 Care Planning 103 Information Management 36
Operative Care 93 Continuum of Care 97 Continuum of Care 33
Medication Use 91 Medication Use 77 Operative Care 29
Care Planning 81 Operative Care 76 Health information technology- related
27
29
• Think Pink handout Sample Reportable Events (revised 11/18/14)
• AZ Service Area Policy Event Reporting Policy 2.011/10025.1 (effective 9/1/14)
• Dignity Health Patient Safety Event Reporting and Management Policy 100.5.006 (effective 6/26/14)
• St. Joseph’s Sentinel Event Identification/Investigation Policy 10027 (effective 12/27/06; last reviewed 8/1/12)
• Comprehensive Accreditation Manual for Hospitals (CAMH) (1/2015)
• Dignity Health Patient Safety Disclosure of Unanticipated or Adverse Outcome to Patients/Families (6/26/14)
• St. Joseph’s Medical Staff Disclosure Policy (10/17/14)
• Getting the Most out of RCAs (ECRI 2/10/15)
• Root Cause Analysis: How Incident Reports Lead to Improvements & Mock RCA (Matt Russell, M.D., Glenn Rosenbluth, M.D. UCSF 2014)
• What I Learned About Adverse Events from Captain Sully: It’s Not What You Think (Marjorie Podraza Stiegler, M.D. JAMA 1/27/15)
Resources
Thank You! Eva M. Satori, B.A., CPHRM, FASHRMManager Risk Services 602.406.6937 office602.746.4069 pager818.207.6535 cell