Embed Size (px)
Citation preview

Everolimus in Advanced, Nonfunctional Neuroendocrine Tumors of
Lung or Gastrointestinal Origin: Efficacy and Safety Results from the
Placebo-Controlled, Double-blind, Multicenter, Phase 3 RADIANT-4 Study
James C. Yao, Nicola Fazio, Simron Singh, Roberto Buzzoni, Carlo Carnaghi, Edward Wolin, Jiri Tomasek, Markus Raderer, Harald Lahner, Maurizio Voi,
Lida Bubuteishvili Pacaud, Jeremie Lincy, Carolin Sachs, Juan W. Valle, Gianfranco Delle Fave, Eric Van Cutsem, Margot Tesselaar, Yasuhiro Shimada,
Do-Youn Oh, Jonathan Strosberg, Matthew H. Kulke, Marianne E. Pavel
On behalf of the RADIANT-4 Study Investigators

Background
• NET: Heterogeneous group of tumors with different anatomic locations
• Everolimus, an mTOR inhibitor, has shown antitumor efficacy in advanced NET of diverse origin in phase 2 and 3 studies1-5
Everolimus is one of the standard of care for advanced pancreatic NET6
RADIANT-2: Everolimus + octreotide LAR prolonged median PFS by 5.1 months in
patients with advanced NET and a history of carcinoid symptoms vs placebo +
octreotide LAR (although statistically not significant)3
• Effective therapeutic options for patients with advanced, progressive, nonfunctional NET of lung or GI are very limited
• RADIANT-4: First, large, placebo-controlled, phase 3 study to evaluate the efficacy and safety of everolimus in advanced, nonfunctional, progressive lung or GI NET
1. Yao JC et al. J Clin Oncol 2010;28:69-76. 2. Yao JC et al. J Clin Oncol 2008; 26:4311-18. 3. Pavel ME et al. Lancet 2011;378:2005-12. 4. Yao JC et al. N Engl J Med 2011;364:514-523. 5. Pavel ME et al. J Clin Oncol 2012;30. Abstract 4122. 6. Öberg et al. Ann Oncol 2012;23 (Supp 7): vii124–vii130.GI, gastrointestinal; LAR, long-acting repeatable; mTOR, mammalian target of rapamycin; NET, neuroendocrine tumors; PFS, progression-free survival.

RADIANT-4 Study Design
*Based on prognostic level, grouped as: Stratum A (better prognosis) appendix, caecum, jejunum, ileum, duodenum, and NET of unknown primary. Stratum B (worst prognosis) lung, stomach, rectum, and colon except caecum.Crossover to open-label everolimus after progression in the placebo arm was not allowed prior to the primary analysis.
Endpoints: • Primary: PFS (central)• Key Secondary: OS• Secondary: ORR, DCR, safety, HRQoL
(FACT-G), WHO PS, NSE/CgA, PK
Everolimus 10 mg/day N=205
Treated until PD, intolerable AE, or
consent withdrawal
Patients with well-differentiated (G1/G2), advanced, progressive, nonfunctional NET of lung or GI origin (N=302)
• Absence of active or any history of carcinoid syndrome
• Pathologically confirmed advanced disease
• Radiologic disease progression in ≤ 6 months
2:1
RANDOMIZE
Placebo N=97
Stratified by:•Prior SSA treatment (yes vs. no)•Tumor origin (stratum A vs. B)*•WHO PS (0 vs. 1)

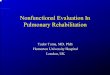
Primary Endpoint: PFS by Central Review
52% reduction in the relative risk of progression or death with everolimus vs placebo
HR = 0.48 (95% CI, 0.35-0.67); P < 0.00001
P-value is obtained from the stratified one-sided log-rank test; Hazard ratio is obtained from stratified Cox model.CI, confidence interval; HR, hazard ratio.
205 168 145 124 101 81 65 52 26 10 3 0 0
97 65 39 30 24 21 17 15 11 6 5 1 0Placebo
Everolimus
No.of patients still at risk
0 2 4 6 8 10 12 15 18 21 24 27 30
Months
0
10
20
30
40
50
60
70
80
90
100
Pro
bab
ility
of
Pro
gre
ssio
n-f
ree
Su
rviv
al (
%)
Kaplan–Meier mediansEverolimus: 11.0 months (95% CI, 9.23-13.31) Placebo: 3.9 months (95% CI, 3.58-7.43)
Censoring Times
Everolimus (n/N = 113/205)
Placebo (n/N = 65/97)

Consistent Investigator-Assessed PFS
P-value is obtained from the stratified one-sided log-rank test; Hazard ratio is obtained from stratified Cox model.CI, confidence interval; HR, hazard ratio.
Everolimus vs PlaceboHR = 0.39 (95% CI, 0.28-0.54); P < 0.00001
205 171 148 132 108 93 75 59 33 15 5 0
97 70 47 35 27 25 21 19 10 6 4 0Placebo
Everolimus
Time (Months)
0
10
20
30
40
50
60
70
80
90
100
Pro
bab
ility
of
Pro
gre
ssio
n-f
ree
Su
rviv
al (
%)
No.of patients still at risk
Kaplan–Meier mediansEverolimus: 14.0 months (95% CI, 11.24-17.71) Placebo: 5.5 months (95% CI, 3.71-7.39)
Censoring Times
Everolimus (n/N = 98/205)
Placebo (n/N = 70/97)
2 4 6 8 10 12 15 18 21 24 270 30
0
0

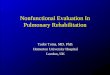
Interim Overall Survival Analysis
*P-value boundary for significance = 0.0002.P-value is obtained from the stratified one-sided log-rank test; Hazard ratio is obtained from stratified Cox model.CI, confidence interval; HR, hazard ratio; NS, not significant; OS, overall survival.
205 195 184 179 172 170 158 143 100 59 31 5 0
97 94 86 80 75 70 67 61 42 21 13 5 0Placebo
Everolimus
No. of patients still at risk
0 2 4 6 8 10 12 15 18 21 24 27 30
Months
0
10
20
30
40
50
60
70
80
90
100
Pro
bab
ility
of
Ove
rall
Su
rviv
al (
%)
Censoring Times
Everolimus (n/N = 42/205)
Placebo (n/N = 28/97)
Everolimus vs PlaceboHR = 0.64 (95 % CI, 0.40-1.05); P = 0.037 (NS)*
First interim OS analysis performed with 37% of information fraction favored the everolimus arm
Next interim analysis is expected in 2016

• RADIANT-4 demonstrated a statistically significant and clinically meaningful prolongation of PFS in patients with well-differentiated, advanced, progressive, nonfunctional NET of lung or GI origin
52% reduction in risk for progression or death; HR = 0.48, P < 0.00001
Central median PFS: 3.9 vs 11.0 months (∆ 7.1 months)
Local radiology review confirms the significant PFS benefit (∆ 8.5 months)
PFS improvement consistent across majority of the predefined subgroups
• First interim OS analysis favored everolimus
− HR = 0.64, statistically not significant− Next analysis expected in 2016
• Safety profile is consistent with known safety profile for everolimus
• Everolimus is the first targeted agent to show robust antitumor activity with acceptable tolerability across a broad spectrum of NET including those arising from the pancreas, lung, and GI tract
Summary and Conclusions

T. AsmisW. KochaD. RaysonJ. RuetherS. SinghL. SiderisH. Kennecke
P. FantaJ. YaoJ. StrosbergU. VermaS. LibuttiR. NataleR. PommierS. LubnerA. StarodubM. KulkeD. SigalB. PoliteC. LieuK. HandeD. Reidy-LagunesA. McCollumL. Forero
L. Vladimirova
M. PavelJ. BojungaP. MalfertheinerH. LahnerA. VogelM. WeberD. Horsch
Acknowledgments
J. ValleD. SarkerN. Reed J. CaveA. FrillingP. Corrie
T.W. KimY.S. ParkD.Y. OhM.A. LeeH.J. Choi
J. CapdevilaR. SalazarJ.J.R. Zoilo
T. ItoN. OkitaI. Komoto
J.S. ChenC.C. WuY.Y. ChenY. ChaoK. H. Yeh
B. JarzabM. Ruchala
V. SriuranpongS. Thongprasert
E. Van CutsemI. BorbathK. GeboesM. Peeters B. Melichar
E. SedlackovaJ. Tomasek
P. Ruff
G. Kaltsas
M.E.T. Tesselaar
M. RadererG. Pall
J. Wang L. ShenJ. XuJ. QianL. Jia
L.F. Maya
Z. PapaiM. Toth
C. Carnaghi G. LuppiN. FazioP. Tomassetti G. Delle Fave G. CartenìR. BuzzoniC. BaroneA. BerrutiD. GiuffridaG. TortoraF. Di Costanzo S. Tafuto
J. KattanA. Shamseddine
H. Raef
T. Salek
H. TurnaA. Sevinc
• The patients participating in this trial• The investigators and their teams• The independent data monitoring committee: Prof. K. Öberg, Dr. D. Haller, and Dr. D. Sargent• Medical editorial assistance: Rohit Kachhadiya and Bhavik Shah (Novartis Healthcare Pvt. Ltd.)
RADIANT-4 Study Investigators: